Submitted:
22 January 2025
Posted:
22 January 2025
You are already at the latest version
Abstract
Vitamin D deficiency was found to be associated with increased risks of infection, morbidity, and mortality in critically ill patients. However, current critical care guidelines do not recommend routine vitamin D supplementation. We conducted a literature search using Medline, Embase, Web of Science and Cochrane databases for randomized controlled trials published in the past five years on vitamin D supplementation in ICU patients. We analyzed data from 21 studies, reviewing dosing strategies, administration routes, baseline vitamin D levels, and clinical outcomes such as biomarker changes, mechanical ventilation duration, hospital length of stay, and mortality. Our results suggest that vitamin D supplementation may be safe and potentially beneficial in reducing ICU length of stay and time on mechanical ventilation. However, the impact on overall mortality remains uncertain. Our findings emphasize the need for individualized clinical decision-making regarding vitamin D supplementation in critically ill patients, considering baseline vitamin D levels, patient characteristics, severity of illness, and administration methods.
Keywords:
clinical outcomes
; vitamin D deficiency
; vitamin D replacement
; critically ill patients
; vitamin D doses
1. Introduction
It is reported that 40-70% of ICU patients present with vitamin D deficiency [1]. Vitamin D (calciferol) is a fat-soluble vitamin that endogenously forms in the skin from UV exposure or food or dietary supplementation. It hydroxylated in the liver to become 25-hydroxyvitamin D (calcidiol, D3/cholecalciferol is the supplement analogue), and hydroxylated again in the kidney into active metabolite 1,25-dihydroxyvitamin D(calcitriol, D2/ergocalciferol is the supplement analogue) [2]. Cholecalciferol, ergocalciferol and calcitriol are used for supplementation in clinical settings [3].
Previous studies have found that vitamin D also plays an important role in immune function that is crucial to recovery in critical illness. It is known that vitamin D regulates gene expression, cell proliferation, and apoptosis [4]. It also regulates the proliferation of T and B cells, modulates immunoglobulin production, and decreases proinflammatory cytokine levels [1,4,5]. Furthermore, vitamin D has been shown to upregulate cathelicidin and other antimicrobial peptides, which are essential to immune defense in critically ill patients [6]. Vitamin D deficiency leads to higher levels of inflammation in certain tissues, including nervous and lung tissues [7,8]. Studies found that vitamin D deficiency may also increase the risk of respiratory failure [9,10]. Vitamin D deficiency (25-hydroxyvitamin D<20 ng/mL) is associated with sepsis, infection, increased morbidity and mortality [10]. However, the benefit of vitamin D supplements in patients with critical illness remained unanswered. In fact, studies evaluating efficacy of vitamin D replacement in critically ill patients have demonstrated conflicting results. This review aimed to investigate the updated literature on the effects of vitamin D supplementation on clinical outcomes in adult intensive care unit (ICU) patients, as well as assessing the vitamin D doses used in various studies.
2. Materials and Methods
Two reviewers independently screened four databases (PubMed, Embase, and Cochrane, Web of Science) using predefined search terms: (vitamin D OR Cholecalciferol OR ergocalciferol OR calcitriol) AND (ICU OR intensive care OR critically- ill) to identify human studies meeting all following 4 criteria: 1) the study design must be a randomized clinical trials (RCT); 2) the study had to be performed in adult population (age ≥ 18 years); 3) the studies must have been published between 2019 to November 2024; and 4) the publications must have been written in full length and in the English language. 5) vitamin D is the only study variable for the clinical outcomes. Retrospective, observational studies and meta-analysis were excluded. Detailed information from each trial was extracted including baseline vitamin D levels, patient population, sample size included in analysis, vitamin D replacement routes and doses, duration of replacement, dose duration and study outcomes. Due to heterogeneous design of clinical trials, no quantitative statistical analysis was performed. Each eligible study was individually evaluated by authors.
3. Results
Out of 807 studies identified, 21 studies met the criteria and were included in this review, see Figure 1. For each included study, one author independently extracted the study details in Table 1. Two authors independently verified the extracted data for all trials.
Eight of the 21 trials included did not show clinical benefit of vitamin D replacement in critically ill patients. The remaining 13 trials demonstrated that replacement of vitamin D in ICU patients with vitamin D deficiency had a positive impact in certain clinical outcomes. Six of these 13 trials found that vitamin D supplementation led to a decreased ICU or hospital length of stay (LOS), three trials found an improvement in Sequential Organ Failure Assessment (SOFA) score, three trials found a decrease in mechanical ventilation (MV) duration, three trials found a decrease of 30-day mortality, two trials found positive outcomes in the Glasgow Coma Scale (GCS), and six trials found positive results in biomarkers. Table 1 summarizes the findings of the studies included in this systematic review. Table 2 highlights whether the study showed a statistically improved outcome of vitamin D replacement.
Various dosing replacement strategies have been used. Of the ones that showed benefit of vitamin D replacement, oral 50,000 International Units (IU) daily for 5 days; oral 120,000 IU single dose, oral 600,000 IU single dose, as well as IM dose 300,000 IU single dose are mostly commonly seen.
4. Discussion
Vitamin D to Improve Outcomes by Leveraging Early Treatment (VIOLET) trial conducted by The National Heart, Lung, and Blood Institute PETAL clinical trial group (2019) showed early administration of a single high-dose 540,000 IU of vitamin D3 enterally in critical-ill patients with vitamin D deficiency ( (25-hydroxyvitamin D level, <20 ng/ml) increases vitamin D serum level but did not demonstrate any clinical benefit over placebo in 90-day mortality or other nonfatal outcomes [8]. This group conducted an ancillary study, VIOLET Long-term Brain Outcomes in Vitamin D Deficient Patients (VIOLET-BUD) [17] . This study evaluated the same single enteral high dose of vitamin D vs placebo in vitamin D deficiency patients on their long-term cognitive outcomes at a median of 443 days (interquartile range, 390-482 days). Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) [25] was evaluated for long term cognitive outcomes and executive function (composite score derived from three Delis-Kaplan Executive Function System Subscales [26]). It concluded that a single high dose of enteral vitamin D did not improve long-term global cognition or executive function in critically ill patients with vitamin D deficiency.
Overall, conflicting results were demonstrated in the randomized controlled trials in the past 5 years regarding the clinical impact of vitamin D replacement on critically ill patients. Several studies showed vitamin D replacement has positive results in biomarkers such as procalcitonin, Cathelicidin LL-37, neutrophil-to-lymphocyte ratio(NLR) and platelet-to-lymphocyte ratio (PLR) levels [27]. Other studies demonstrated that vitamin D improved SOFA score, GCS score, post-op infection rate, duration of mechanical ventilation, and ICU and hospital length of stay [24]. On the contrary, studies also demonstrated no differences between the vitamin D replacement group and placebo group in regards to ICU and hospital LOS and duration of mechanical ventilation. In one of the biggest studies, with a cohort of 1078 patients, early administration of high-dose enteral vitamin D3 540,000 IU did not improve 90-day mortality and other clinical outcomes of vitamin D–deficient patients [8].
It was demonstrated that the vitamin D supplementation in ICU patients with low baseline vitamin D levels does not increase the serum 25-(OH)-D levels as much as expected [20]. This may be due to an increased distribution volume or an accelerated breakdown [20]. Additionally, vitamin D supplementation increased the serum level of 25-(OH)-D but there was no rise in 1, 25 (OH)2D, suggesting that 25-(OH)-D is not metabolized to the active hormone 1, 25 (OH)2D. It is speculated that CYP27B1 (also known as 1-alpha hydroxylase) is downregulated during critical illness, which compromises the conversion of 25OHD to 1, 25(OH)2D, and possibly shifts the metabolization of 25OHD to other compounds. Small rise in 24, 25 (OH)2D was also noticed, which might serve as a feedback mechanism of avoiding vitamin D toxicity. These findings could be part of an adaptive response to critical illness [20]. On the other hand, the vitamin D supplementation dose in the study of Ingels et al. is very low (loading dose of 8,000 IU and daily maintenance of 600 IU x10 days), compared to vitamin D doses in other studies. This could be the reason why Ingels et al did not find any significant benefit of vitamin D replacement in ICU patients.
The strategies to replace vitamin D also vary across studies. The dose and route of vitamin D replacement remains institutional and protocol-specific. In studies that show vitamin D replacement with positive clinical impacts, the vitamin D dose ranges from 5,000 IU to 540,000 IU as a single dose or multiple-day replacement. The vitamin D was given either via enteral or intramuscular route. In several studies, vitamin D was supplemented in patients who were found to have vitamin D deficiency; in other studies, the critically ill patients were supplemented with high dose vitamin D without knowing their baseline vitamin D level. The optimal timing of vitamin D replacement upon intubation is also unclear. Fortunately, no toxicity from vitamin D supplementation was reported in patients among all studies reviewed.
The promising role of vitamin D in patients with severe vitamin D deficiency has been identified and confirmed in several studies [5,7,10,12,13,18,19,22]. Even though in VITdAL-ICU, the use of vitamin D3 supplement did not show beneficial effects on duration of hospital stay or ICU stay as well as hospital mortality and 90-day mortality, one of the post-hoc study of VITDAL-ICU focused on the subgroup analysis on patients with severe vitamin D deficiency (defined as vitamin D level ≤ 12ng/ml) identified a significant reduction in 28-day mortality with the use of vitamin D3 supplements (HR 0.52, [0.30-0.89]) [28]. Bhattacharyya et al performed a subgroup analysis in regards to clinical effects of vitamin D3 supplements on patients with severe vitamin D deficiency (vitamin D levels <12 ng/mL) [4]. The results showed that vitamin D replacement significantly decreased the use of mechanical ventilation, as well as a trend in reducing 90-day mortality (HR 0.449, [0.198–1.017]). An ongoing trial VITDALIZE trial has specifically focused on the critically ill patients with severe vitamin D deficiency [29]. This study is designed to enroll 2400 patients with a primary endpoint of 28-day mortality. The outcome of this trial is expected to be reported in 2026, which may provide us with more robust evidence on vitamin D replacement in patients with severe vitamin D deficiency.
Of all trials included, Thampi et al, Sistanzid et al, and Naguib et al used synthetic vitamin D analogs as a vitamin D replacement form [3,6,18]. Thamp et al and Sistanzid et al used calcitriol in the sepsis population and no significant results were identified [3,6]. Naguib et al used alfacalcidol orally for patients scheduled for elective mechanical valve replacement surgery [18]. Although no significant difference in hospital mortality was identified, there was a significant reduction in ICU length of stay and postoperative infection rate. Generally, vitamin D analogs were not suitable for vitamin D replacement due to its narrow therapeutic range, lack of feedback control resulting in increased risk for hypercalcemia [30]. It is indicated for hypocalcemia, osteoporosis, and the prevention of corticosteroid-induced osteoporosis [31]. Given the high incidence of acute kidney injury in acute illness and high level of monitoring in ICU, it is arguable that active or partially active vitamin D analogs are more suitable for the critically ill population. Further studies should be designed to evaluate their efficacy and safety in this context.
Masbough et al. and Sharma et al. both investigated vitamin D in traumatic brain injury patients [7,13]. Surprisingly, both studies found a statistically increase in GCS scores. Sharma et al. reported improvement in biomarkers and shorter mechanical ventilation days. Similarly, Hansaloei et al. reported significant reduction in biomarkers, SOFAscore, duration of mechanical ventilation days and length of ICU stay in traumatic injury patients admitted to ICU [20]. The effect of preoperative vitamin D replacement was investigated by Hajimohammadebrahim-Ketabforoush et al and Naguib et al. for craniotomy for brain tumor resection and elective mechanical valve replacement surgery, respectively, both reported statistically significant reduction in ICU length of stay [18,19]. Low vitamin D level was associated with adverse outcomes with various surgical procedures [32]. With a relatively low patient population enrolled in these trials, the positive findings regarding GCS scores and reduced ICU length of stay suggest that this area could benefit from further exploration with larger patient enrollment to confirm these results and potentially identify a reduction in other outcomes in surgical patients.
Vitamin D deficiency in ICU patients is attributed to both pre-existing insufficiency and a decline in levels during acute illnesses [33,34]. Mechanisms contributing to reduced vitamin D levels during acute illness may include hemodilution, interstitial extravasation, decreased synthesis of binding proteins, and renal loss [35]. In addition, acute fluid resuscitation in ICU can significantly lower vitamin D level, which may take up to 24 hours to resolve [36]. Thus, interpretations of vitamin D level in acute illness should be performed with caution.
Absorption of vitamin D supplementation can vary in different patient populations. For example, higher BMI is linked to a smaller increase in serum 25(OH)D concentrations. Calcium intake and type of vitamin D (D2- ergocalciferol or D3-cholecalciferol) can affect the dose response of 25 (OH)D to vitamin D. Following oral intake, vitamin D is rapidly absorbed to reach a maximum level at around 24 hours. Levels of 25 (OH)D increase gradually to peak at 7-14 days depending on the dose. For studies that used only single dose vitamin D supplementation, it is questionable how the 25(OH)D concentrations played out. Patients with malabsorption issues such as gastrectomy or bariatric patients might need higher doses of vitamin D compared to others [37]. Lastly, baseline vitamin D levels reflect coexisting conditions, especially in critically ill patients, which could cause residual confounding effects when analyzing results [8].
The impact in clinical outcomes in vitamin D replacement in critically ill patients remains uncertain. High doses of vitamin D up to 540,000 IU have been used in studies to explore impact on duration of mechanical ventilation and length of stay. Given the wide therapeutic index of vitamin D, clinicians may feel comfortable with high dose vitamin D replacement even in absence of baseline vitamin D level. Vitamin D toxicity may occur when serum levels of 25(OH)D concentration are greater than 150 ng/mL, accompanied by normal or elevated values of 1,25(OH)2D concentration. The most common cause of vitamin D toxicity is excessive vitamin D supplementation without frequent monitoring of vitamin D levels. While most cases of vitamin D toxicity do not lead to serious complications or sequelae, it may cause hypercalcemia and acute renal failure, which are important considerations in critical care settings. If a high-dose vitamin D replacement is given, it is reasonable to consider monitoring vitamin D levels together with electrolytes and kidney functions. More studies need to be performed to determine the optimal dosing strategies to replace vitamin D in critically ill patients.
5. Limitations
This review has several limitations. First, no quantitative statistical analysis was conducted, resulting in reduced certainty and a potential for bias in the findings. Secondly, we did not perform meta-analysis on our review. It was previously discussed that vitamin D supplementation may be associated with a decrease in mortality rate and ICU admission [38]. Additionally, due to heterogeneity of the study design and the various vitamin D doses, the review is constrained by its approach of discussing each study individually.
6. Conclusions
Vitamin D supplementation is safe to be used in critically ill patients, even when their baseline vitamin D level is not known, because of rare incidence of vitamin D toxicity. The majority of clinical trials showed clinical benefits of vitamin D supplementation in ICU patients in shorter ICU or hospital length of stay, improvement of SOFA score, decrease in duration of mechanical ventilation or 28-day mortality. Therefore, Vitamin D supplementation deserves being considered in the ICU setting, especially with closely monitored vitamin D level.
Acknowledgments
We would like to express our sincere appreciation of Dr. Yongxia Zhang PhD for her assistance of literature search.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sistanizad, M.; Kouchek, M.; Miri, M.; Salarian, S.; Shojaei, S.; Moeini Vasegh, F.; Seifi Kafshgari, H.; Qobadighadikolaei, R. High Dose Vitamin D Improves Total Serum Antioxidant Capacity and ICU Outcome in Critically Ill Patients - A Randomized, Double-Blind Clinical Trial. Eur. J. Integr. Med. 2021, 42, 101271. [Google Scholar] [CrossRef]
- Institute of Medicine; Food and Nutrition Board; Committee to Review Dietary Reference Intakes for Vitamin D and Calcium Dietary Reference Intakes for Calcium and Vitamin D. Del Valle, H.B., Yaktine, A.L., Taylor, C.L., Ross, A.C., Eds.; National Academies Press: Washington, D.C., DC, 2011; ISBN 9780309163941.
- Sistanizad, M.; Salarian, S.; Kouchek, M.; Shojaei, S.; Miri, M.; Masbough, F. Effect of Calcitriol Supplementation on Infectious Biomarkers in Patients with Positive Systemic Inflammatory Response: A Randomized Controlled Trial. Ann. Med. Surg. (Lond.) 2024, 86, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, A.; Subramaniam, R.; Baidya, D.K.; Aggarwal, P.; Wig, N. Effect of Early Administration of Vitamin D on Clinical Outcome in Critically Ill Sepsis Patients: A Randomized Placebo-Controlled Trial. Indian J. Crit. Care Med. 2021, 25, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Bychinin, M.V.; Klypa, T.V.; Mandel, I.A.; Yusubalieva, G.M.; Baklaushev, V.P.; Kolyshkina, N.A.; Troitsky, A.V. Effect of Vitamin D3 Supplementation on Cellular Immunity and Inflammatory Markers in COVID-19 Patients Admitted to the ICU. Sci. Rep. 2022, 12, 18604. [Google Scholar] [CrossRef] [PubMed]
- Thampi, S.J.; Basheer, A.; Thomas, K. Calcitriol in Sepsis-A Single-Centre Randomised Control Trial. J. Clin. Med. 2024, 13, 3823. [Google Scholar] [CrossRef]
- Sharma, S.; Kumar, A.; Choudhary, A.; Sharma, S.; Khurana, L.; Sharma, N.; Kumar, V.; Bisht, A. Neuroprotective Role of Oral Vitamin D Supplementation on Consciousness and Inflammatory Biomarkers in Determining Severity Outcome in Acute Traumatic Brain Injury Patients: A Double-Blind Randomized Clinical Trial. Clin. Drug Investig. 2020, 40, 327–334. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute PETAL Clinical Trials Network; Ginde, A. A.; Brower, R.G.; Caterino, J.M.; Finck, L.; Banner-Goodspeed, V.M.; Grissom, C.K.; Hayden, D.; Hough, C.L.; Hyzy, R.C.; et al. Early High-Dose Vitamin D3 for Critically Ill, Vitamin D-Deficient Patients. N. Engl. J. Med. 2019, 381, 2529–2540. [CrossRef]
- Moromizato, T.; Litonjua, A.A.; Braun, A.B.; Gibbons, F.K.; Giovannucci, E.; Christopher, K.B. Association of Low Serum 25-Hydroxyvitamin D Levels and Sepsis in the Critically Ill. Crit. Care Med. 2014, 42, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Ashoor, T.M.; Abd Elazim, A.E.H.; Mustafa, Z.A.E.; Anwar, M.A.; Gad, I.A.; Mamdouh Esmat, I. Outcomes of High-Dose versus Low-Dose Vitamin D on Prognosis of Sepsis Requiring Mechanical Ventilation: A Randomized Controlled Trial. J. Intensive Care Med. 2024, 39, 1012–1022. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Singh, A.; Rastogi, A.; Puri, G.D.; Ganesh, V.; Naik, N.B.; Kajal, K.; Kahlon, S.; Soni, S.L.; Kaloria, N.; Saini, K.; et al. Therapeutic High-Dose Vitamin D for Vitamin D-Deficient Severe COVID-19 Disease: Randomized, Double-Blind, Placebo-Controlled Study (SHADE-S). J. Public Health (Oxf.) 2024, 46, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Masbough, F.; Kouchek, M.; Koosha, M.; Salarian, S.; Miri, M.; Raoufi, M.; Taherpour, N.; Amniati, S.; Sistanizad, M. Investigating the Effect of High-Dose Vitamin D3 Administration on Inflammatory Biomarkers in Patients with Moderate to Severe Traumatic Brain Injury: A Randomized Clinical Trial. Iran. J. Med. Sci. 2024, 49, 643–651. [Google Scholar] [CrossRef]
- Zamanian, M.; Javadfar, Z.; Salimi, Y.; Rahimi, M.A.; Rabieenia, E.; Rahimi, A. Effect of High-Dose Vitamin D on Mortality and Hospital Length of Stay in ICU Patients with COVID-19: A Randomized Clinical Trial. J. Kermanshah Univ. Med. Sci. 2024, 28. [Google Scholar] [CrossRef]
- Wang, A.-Y.; Yeh, Y.-C.; Cheng, K.-H.; Han, Y.-Y.; Chiu, C.-T.; Chang, C.-C.; Wang, I.-T.; Chao, A. Efficacy and Safety of Enteral Supplementation with High-Dose Vitamin D in Critically Ill Patients with Vitamin D Deficiency. J. Formos. Med. Assoc. 2024. [CrossRef]
- Domazet Bugarin, J.; Dosenovic, S.; Ilic, D.; Delic, N.; Saric, I.; Ugrina, I.; Stojanovic Stipic, S.; Duplancic, B.; Saric, L. Vitamin D Supplementation and Clinical Outcomes in Severe COVID-19 Patients-Randomized Controlled Trial. Nutrients 2023, 15, 1234. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Ginde, A.A.; Brown, S.M.; Baughman, A.; Collar, E.M.; Ely, E.W.; Gong, M.N.; Hope, A.A.; Hou, P.C.; Hough, C.L.; et al. Effect of Early High-Dose Vitamin D3 Repletion on Cognitive Outcomes in Critically Ill Adults. Chest 2021, 160, 909–918. [Google Scholar] [CrossRef]
- Naguib, S.N.; Sabry, N.A.; Farid, S.F.; Alansary, A.M. Short-Term Effects of Alfacalcidol on Hospital Length of Stay in Patients Undergoing Valve Replacement Surgery: A Randomized Clinical Trial. Clin. Ther. 2021, 43, e1–e18. [Google Scholar] [CrossRef] [PubMed]
- Hajimohammadebrahim-Ketabforoush, M.; Shahmohammadi, M.; Keikhaee, M.; Eslamian, G.; Vahdat Shariatpanahi, Z. Single High-Dose Vitamin D3 Injection and Clinical Outcomes in Brain Tumor Resection: A Randomized, Controlled Clinical Trial. Clin. Nutr. ESPEN 2021, 41, 153–159. [Google Scholar] [CrossRef]
- Ingels, C.; Vanhorebeek, I.; Van Cromphaut, S.; Wouters, P.J.; Derese, I.; Dehouwer, A.; Møller, H.J.; Hansen, T.K.; Billen, J.; Mathieu, C.; et al. Effect of Intravenous 25OHD Supplementation on Bone Turnover and Inflammation in Prolonged Critically Ill Patients. Horm. Metab. Res. 2020, 52, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Padhy, S.S.; Malviya, D.; Harjai, M.; Tripathi, M.; Das, P.K.; Rastogi, S. A Study of Vitamin D Level in Critically Ill Patients and Effect of Supplementation on Clinical Outcome. Anesth. Essays Res. 2020, 14, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Hasanloei, M.A.V.; Rahimlou, M.; Eivazloo, A.; Sane, S.; Ayremlou, P.; Hashemi, R. Effect of Oral versus Intramuscular Vitamin D Replacement on Oxidative Stress and Outcomes in Traumatic Mechanical Ventilated Patients Admitted to Intensive Care Unit. Nutr. Clin. Pract. 2020, 35, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Karsy, M.; Guan, J.; Eli, I.; Brock, A.A.; Menacho, S.T.; Park, M.S. The Effect of Supplementation of Vitamin D in Neurocritical Care Patients: RandomizEd Clinical TrIal oF hYpovitaminosis D (RECTIFY). J. Neurosurg. 2020, 133, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Miri, M.; Kouchek, M.; Rahat Dahmardeh, A.; Sistanizad, M. Effect of High-Dose Vitamin D on Duration of Mechanical Ventilation in ICU Patients. Iran. J. Pharm. Res. 2019, 18, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary Clinical Validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef]
- Shunk, A.W.; Davis, A.S.; Dean, R.S. TEST REVIEW: Dean C. Delis, Edith Kaplan & Joel H. Kramer, Delis Kaplan Executive Function System (D-KEFS), the Psychological Corporation, San Antonio, TX, 2001. $415.00 (complete Kit). Appl. Neuropsychol. 2006, 13, 275–227. [Google Scholar] [CrossRef]
- Akbas, E.M.; Gungor, A.; Ozcicek, A.; Akbas, N.; Askin, S.; Polat, M. Vitamin D and Inflammation: Evaluation with Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio. Arch. Med. Sci. 2016, 12, 721–727. [Google Scholar] [CrossRef]
- Martucci, G.; McNally, D.; Parekh, D.; Zajic, P.; Tuzzolino, F.; Arcadipane, A.; Christopher, K.B.; Dobnig, H.; Amrein, K. Trying to Identify Who May Benefit Most from Future Vitamin D Intervention Trials: A Post Hoc Analysis from the VITDAL-ICU Study Excluding the Early Deaths. Crit. Care 2019, 23, 200. [Google Scholar] [CrossRef]
- Amrein, K. The VITDALIZE Study: Effect of High-Dose Vitamin D3 on 28-Day Mortality in Adult Critically Ill Patients (VITDALIZE) Available online:. Available online: https://clinicaltrials.gov/study/NCT03188796 (accessed on 19 January 2025).
- Joshi, D. ; Jacqueline R Center; Eisman, J. A. Vitamin D Deficiency in Adults. Aust. Prescr. 2010, 33, 103–106. [Google Scholar] [CrossRef]
- Lung, B.E.; Mowery, M.L.; Komatsu, D.E.E. Calcitriol. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Iglar, P.J.; Hogan, K.J. Vitamin D Status and Surgical Outcomes: A Systematic Review. Patient Saf. Surg. 2015, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Papinutti, A.; Mathew, E.; Vila, G.; Parekh, D. Vitamin D and Critical Illness: What Endocrinology Can Learn from Intensive Care and Vice Versa. Endocr. Connect. 2018, 7, R304–R315. [Google Scholar] [CrossRef] [PubMed]
- Gomes, T.L.; Fernandes, R.C.; Vieira, L.L.; Schincaglia, R.M.; Mota, J.F.; Nóbrega, M.S.; Pichard, C.; Pimentel, G.D. Low Vitamin D at ICU Admission Is Associated with Cancer, Infections, Acute Respiratory Insufficiency, and Liver Failure. Nutrition 2019, 60, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Quraishi, S.A.; Camargo, C.A. , Jr Vitamin D in Acute Stress and Critical Illness. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.; Ochola, J.; Mundy, J.; Jones, M.; Kruger, P.; Duncan, E.; Venkatesh, B. Acute Fluid Shifts Influence the Assessment of Serum Vitamin D Status in Critically Ill Patients. Crit. Care 2010, 14, R216. [Google Scholar] [CrossRef]
- Ramasamy, I. Vitamin D Metabolism and Guidelines for Vitamin D Supplementation. Clin. Biochem. Rev. 2020, 41, 103–126. [Google Scholar] [CrossRef] [PubMed]
- Argano, C.; Mallaci Bocchio, R.; Natoli, G.; Scibetta, S.; Lo Monaco, M.; Corrao, S. Protective Effect of Vitamin D Supplementation on COVID-19-Related Intensive Care Hospitalization and Mortality: Definitive Evidence from Meta-Analysis and Trial Sequential Analysis. Pharmaceuticals (Basel) 2023, 16, 130. [Google Scholar] [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection based on inclusion and exclusion criteria [11].
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection based on inclusion and exclusion criteria [11].
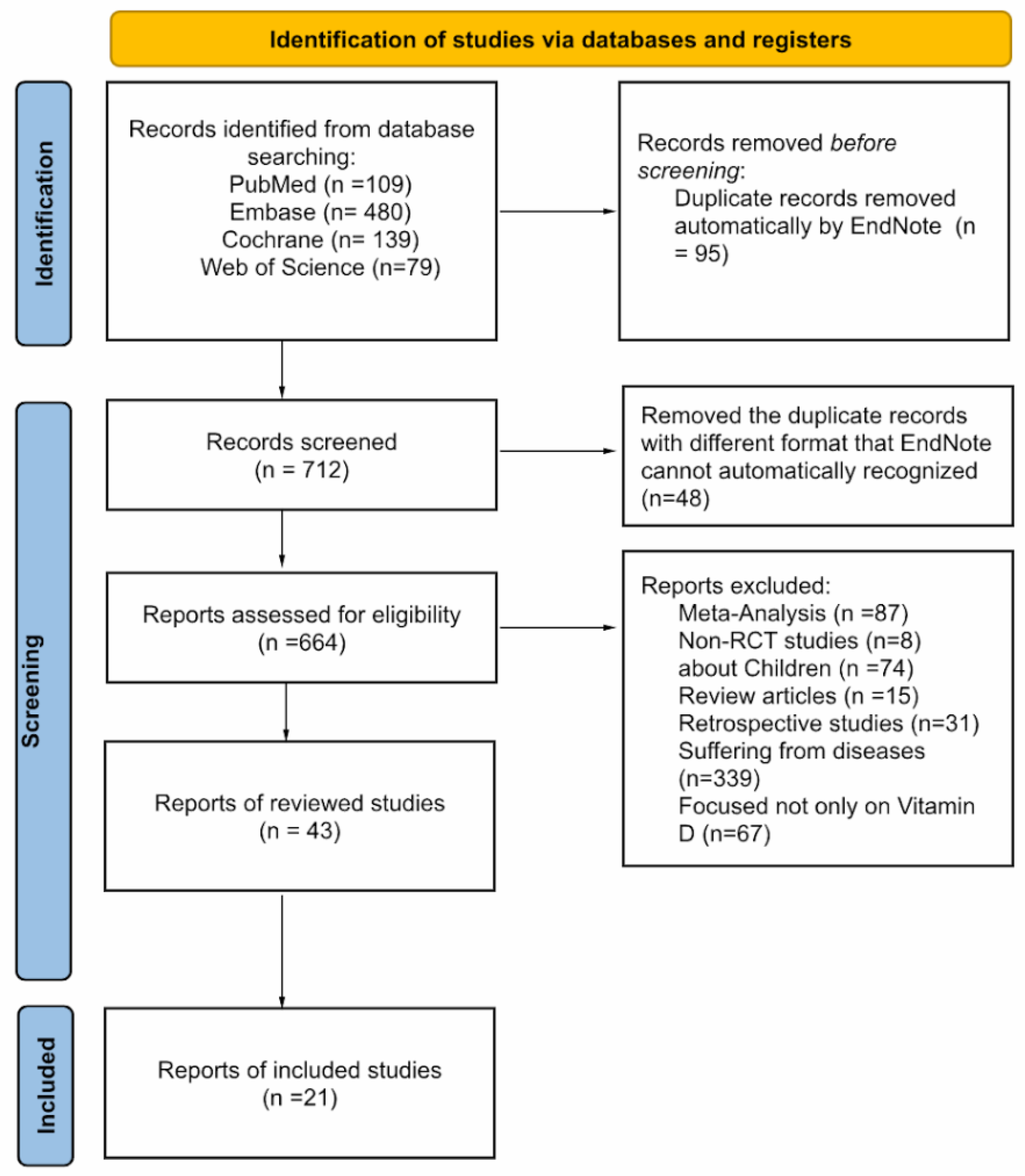

Table 1.
Summary of randomized clinical trials (RCT) from 2019 to 2024.
| Study | Year | Baseline vit D level (ng/mL) | Sample Size | Patient population | Vit D Replacement Dose | Duration | Notes |
|---|---|---|---|---|---|---|---|
| Ashoor et al [10] | 2024 | <20 | 80 | Sepsis on mechanical ventilation | HD: enteral 50,000IU/d vs LD: enteral 5,000IU/d | 5 days | Significant difference in procalcitonin, LL-37 reduction, improved SOFA and hospital LOS |
| Singh et al [12] | 2024 | 12 vs 13 | 90 | Covid-19 | Enteral 600,000IU | Once | Significantly improved SOFA score at Day 7 and 28 day mortality |
| Masbough et al [13] | 2024 | 15.95 vs 17.84 | 35 | Traumatic brain injury | IM 300,000IU | Once | Statistically significant increase in GCS scores, reduction in inflammatory markers; improvement in the GOS-E score; no difference in 28 day mortality, ICU LOS, MV needs |
| Thampi et al [6] | 2024 | Not reported | 152 | Sepsis | Calcitriol IM 300,000IU | Once | No significant difference in APACHE II scores, 28-day mortality, MV days, ICU LOS and hospital-acquired infections |
| Sistanizad et al [3] | 2024 | 11.37 vs 13.96 | 28 | Sepsis | Calcitriol IV 1 mcg/day | 3 days | No significant different in procalcitonin level, ICU LOS and 28-day mortality |
| Zamanian et al [14] | 2024 | 23.06 vs 25.68 | 61 | COVID-19 | IM 300,000IU | Once | No significant difference in mortality or hospital LOS |
| Wang et al [15] | 2024 | <20 | 61 | Vitamin D-deficient | Enteral 569,600IU | Once divided by 8 bottles | Less than half of the treatment group who achieved vit D level>30 ng/ml. They had significantly lower 30-day mortality than those who did not |
| Domazet Bugarin et al [16] | 2023 | 25.3 vs 27.3 | 155 | Covid-19 | Enteral 10,000IU vs placebo | Once | No statistically significant in MV days, secondary outcomes |
| Bychinin et al [5] | 2022 | 9.6 vs 11 | 110 | COVID-19 | PO 60,000IU weekly then 5,000IU/daily | During hospital stay | Significantly increased NK and NK T cell counts. No difference in mortality; need for MV or incidence of nosocomial infection |
| Sistanizad et al [1] | 2021 | <20 | 36 | ICU ventilated | IM 300,000IU vs placebo | Once | No statistically significant results identified due to small sample size |
| Bhattacharyya et al [4] | 2021 | 12.05 vs 15.47 | 126 | Sepsis | Enteral 540,000IU vs placebo | Once | No statistically difference in ICU LOS, hospital LOS, MV duration/requirements, or 90-day mortality |
| Han et al [17] | 2021 | 15.2 vs 13.1 | 95 | Vitamin D-deficient | Enteral 540,000IU | Once | No significant difference in long-term global cognition or executive function |
| Naguib et al [18] | 2021 | 21 vs. 19.1 | 86 | Elective mechanical valve replacement | Alfacalcidol 2 μg/day PO | Starting 2 days before surgery until the end of hospital stay | Statistically significant reduction in ICU LOS, postoperative infection rate. No significantly difference in hospital mortality |
| Sharma et al [7] | 2020 | 18.30 vs 15.15 | 35 | Traumatic brain injury | Enteral 120,000IU vs placebo | Once | Significant improvement in GCS score, MV duration and IL-6, TNF-ɑ |
| Hajimohammadebrahim-Ketabforoush et al [19] | 2020 | <20 | 60 | Craniotomy for brain tumor resection | IM 300,000IU | Once | Significantly reduction in ICU LOS and hospital LOS |
| Ingels et al [20] | 2020 | 6.8 vs. 9.2 | 24 | Prolonged ICU stay(>10 days) | 200μg loading dose once then 15μg/day | Loading dose then 10 days | No difference in SOFA score or MV duration |
| Padhy et al [21] | 2020 | ≤20 | 60 | Vitamin D-deficient, sepsis | G1: enteral 60,000IU once/wk; G2: 60,000IU twice/wk | During hospital stay | No difference was found in ICU LOS, duration of MV, and 28 day ICU mortality. Patients in group 2 required less inotropic support p=0.037 |
| Hasanloei et al [22] | 2020 | 10 - 30 | 72 | Ventilated, traumatic injury | G1: PO 50,000IU /day; G2: IM 300,000IU vs placebo | G1: 6 days; G2: once | Significant improvement in IL6, ESR, CRP, SOFA score, duration of MV, ICU LOS |
| Karsy et al [23] | 2020 | 14.6 vs 13.9 | 267 | Neurocritical care, vitamin D-deficient | PO 540,000IU vs placebo | Once | No statistically difference in hospital LOS or ICU LOS |
| Miri et al [24] | 2019 | 8.43 vs. 11.35 | 40 | ICU ventilated | IM 300,000IU vs placebo | Once | Significant reduction in 28-day mortality |
| PETAL group [8] | 2019 | 11.2 vs 11.0 | 1078 | Vitamin D- deficient | Enteral 540,000IU vs placebo | Once | No statistically difference in 90-day mortality and other clinical outcomes |
Table 2.
Summary of positive vs. negative clinical outcomes.
| Year | Author | Clinical results | Biomarkers | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICU LOS | Hospital LOS | SOFA score | MV duration | MV needs | 90-day mortality | 28-day mortality | 30-day mortality | GCS | Less inotropic support | |||
| 2024 | Ashoor et al [10] | HD | HD | HD: pct, IL-37 | ||||||||
| 2024 | Singh et al [12] | |||||||||||
| 2024 | Masbough et al [13] | IL-1b, IL-6 | ||||||||||
| 2024 | Thampi et al [6] | |||||||||||
| 2024 | Sistanizad et al [3] | pct | ||||||||||
| 2024 | Zamanian et al [14] | |||||||||||
| 2023 | Domazet Bugarin et al [16] | |||||||||||
| 2022 | Bychinin et al [5] | All-cause | NK, NKT, CRP, pct | |||||||||
| 2021 | Sistanizad et al [1] | |||||||||||
| 2021 | Bhattacharyya et al [4] | |||||||||||
| 2021 | Han et al [17] | BRANS score | ||||||||||
| 2021 | Naguib et al [18] | |||||||||||
| 2020 | Sharma et al [7] | IL-6, TNF-α | ||||||||||
| 2020 | Hajimohammadebrahim-Ketabforoush et al [19] | |||||||||||
| 2020 | Ingels et al [20] | CRP, WBC, IL-37, sCD163 | ||||||||||
| 2020 | Wang et al [15] | |||||||||||
| 2020 | Padhy et al [21] | |||||||||||
| 2020 | Hasanloei et al [22] | IL-6, ESR, CRP | ||||||||||
| 2020 | Karsy et al [23] | |||||||||||
| 2019 | Miri et al [24] | |||||||||||
| 2019 | PETAL group [8] | |||||||||||
1 Table 1 & Table 2: : Vitamin D showed statistically significant improvement; : Vitamin D showed no effects; : No trial has reported yet. HD: high-dose of vitamin D; LD: low-dose of vitamin D; G1: group 1; G2: group 2; LOS: length of stay; APACHE II: acute physiologic assessment and chronic health evaluation II; SOFA: sequential organ failure assessment; mNUTRIC: the modified Nutrition Risk in Critically ill; MV: mechanical ventilator; All-cause: all-cause mortality; pct: procalcitonin; CRP: C-reactive protein; NK: natural killer cell; NKT: natural killer T cell; ESR: erythrocyte sedimentation rate; WBC: white blood cell; IL: interleukin; TNF-α: tumor necrosis factor-alpha; GOS-E: Glasgow outcome scale-extended.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



