
Submitted:
20 January 2025
Posted:
22 January 2025
You are already at the latest version
Abstract
Background: As tobacco is the main risk factor for oral cancer, it is important to understand the burden of this disease after the Framework Convention on Tobacco Control. For MERCOSUR tobacco control is a topic of interest. The aim of this study was to describe MPOWER measures scores and to evaluate the trends of lip and oral cavity cancer (LOC) incidence, mortality and Disability-adjusted Life Years (DALYs), from 2005 to 2021, in MERCOSUR countries. Methods: This is an ecological descriptive study, where the MPOWER measures scores were extracted from the Global Health Observatory of World Health Organization, and the Age-standardized Rates (ASRs) of LOC for MERCOSUR countries were obtained from the Global Burden of Diseases 2021 results tool. The trends of LOC ASRs were obtained using the Prais-Winsten method. Results: Paraguay and Venezuela had lower MPOWER scores over time than Argentina, Brazil and Uruguay. These three last countries showed LOC trends decreasing for most indicators among males, while Paraguay and Venezuela showed increasing trends in incidence for both males and females, and no decreasing trends. Conclusion: This study suggests that MERCOSUR countries with a history of stronger tobacco control policies may be exhibiting more decreasing trends in LOC indicators.
Keywords:
Oral Cancer
; Tobacco Use
; Tobacco Control
; Latin American Countries
1. Introduction
The burden of oral cancer remains high worldwide, particularly in regions with lower sociodemographic development [1]. In 2019, lip and oral cavity cancer (LOC) ranked as the 13th leading cancer in terms of Disability-Adjusted Life Years (DALYs) globally, with an age-standardized DALY rate of 66.1 per 100,000 inhabitants [2]. Squamous cell carcinoma is the most common histological type, predominantly affecting men in their fifth decade of life. Key etiological factors include alcohol and tobacco, which act synergistically in the pathogenesis of this cancer [3,4]. Tobacco, containing numerous carcinogenic compounds, exhibits a dose-response relationship between packs smoked per year and the risk of developing oral cancer [5].
To address the substantial harm caused by the global tobacco epidemic, the World Health Organization (WHO) launched the Framework Convention on Tobacco Control (WHO-FCTC) in 2003, which came into force in 2005 [6]. In 2008, the MPOWER technical package was introduced to aid countries in reducing tobacco demand. MPOWER encompasses six measures: monitoring tobacco use and prevention policies; protecting people from tobacco smoke; offering help to quit tobacco use; warning about the dangers of tobacco; enforcing bans on tobacco advertising, promotion, and sponsorship; and raising taxes on tobacco products [7].
Despite progress, high DALY rates attributed to behavioral risk factors, including tobacco use, are observed in some Latin American countries [8]. However, tobacco-related LOC deaths are declining across the Americas as a whole [9]. Within the MERCOSUR bloc—comprising Argentina, Brazil, Paraguay, Uruguay, and Venezuela—tobacco control has been a priority since 2003, with the establishment of the Intergovernmental Commission for Tobacco Control. This initiative has been crucial in identifying and addressing priorities for tobacco control among member countries [10]. While these nations have adopted various WHO-recommended strategies, challenges such as socioeconomic and cultural diversity hinder the full implementation of MPOWER measures [11,12].
More than two decades after the launch of the WHO-FCTC, it is vital to assess the burden of non-communicable diseases in recent years. This study aims to describe MPOWER measure scores and evaluate trends in LOC incidence, mortality, and DALYs from 2005 (the year of WHO-FCTC implementation) to 2021 across MERCOSUR countries.
2. Materials and Methods
This ecological descriptive study evaluated the MPOWER measure scores and the trends in Lip and Oral Cavity Cancer (LOC) Age-Standardized Rates (ASRs) using a time series analysis. The units of analysis were the five MERCOSUR member countries.
2.1. MPOWER Scores
MPOWER scores were retrieved from the World Health Organization (WHO) Global Health Observatory database [13]. These scores began being attributed in 2007, with the exception of the "R" measure, which started in 2008. Since 2008, scores have been updated biennially. For this study, the MPOWER scores from 2007, 2008, 2010, 2012, 2014, 2016, 2018, and 2020 were included. The "M" score ranges from 1 to 4, while the "POWER" measures range from 1 to 5. A score of 1 indicates insufficient information regarding the measure in the country. Higher scores reflect better quality or intensity of the measure implemented [7].
2.2. Lip and Oral Cavity Cancer Rates
Data on LOC ASRs from 2005 to 2021 for MERCOSUR countries were obtained from the Global Burden of Diseases (GBD) 2021 Study results tool (Global Health Data Exchange – GHDx) [14]. The GBD employs advanced methodologies to estimate the distribution of diseases and injuries across 204 countries and territories, with input from a wide network of collaborators [1].
For this study, ASRs for incidence, mortality, and DALYs were analyzed. Data were stratified by sex due to the historically distinct epidemiological profiles of LOC between males and females [4]. The LOC sites included correspond to codes C00-C08 of the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) [1].
2.3. Statistical Analysis
MPOWER scores were descriptively analyzed, with medians and interquartile ranges calculated for each measure and for the total score. Time trends in LOC ASRs were assessed using the Prais-Winsten linear regression model, which corrects for first-order autocorrelation in time series data, as described by Antunes and Waldman [15].
The Annual Percent Change (APC) and its 95% confidence interval (95%CI) were calculated for each country. Trends were classified as: (1) decreasing, when the APC and the 95%CI are negative; (2) stationary, when the lower value of 95%CI is negative and the higher is positive (including zero in the interval); (3) increasing, when the APC and the 95%CI are positive. All analyses were conducted using SPSS version 20 and Stata version 13.1.3.
3. Results
3.1. MPOWER Scores
Figure 1 illustrates the distribution of scores over time for each MPOWER measure and the overall sum of all measures. Paraguay consistently displayed lower scores, particularly for the "W" (Warn about the dangers of tobacco) and "R" (Raise taxes on tobacco) measures, compared to other MERCOSUR countries throughout the study period. Venezuela showed lower scores for the "M" (Monitor tobacco use and prevention policies) and "E" (Enforce bans on tobacco advertising, promotion, and sponsorship) measures. Argentina began the study period with relatively low scores for the "P" (Protect people from tobacco smoke), "W," and "E" measures; however, these scores increased notably starting in 2012.
Table 1 provides a summary of these findings, presented as medians and interquartile ranges for each MPOWER measure and their overall sum. Paraguay recorded the lowest median scores across the measures, followed by Venezuela. In contrast, Brazil and Uruguay achieved the highest median scores, with Argentina close behind in overall performance.
3.2. LOC Trends
Table 2 summarizes the LOC trends for males and females across MERCOSUR countries. Among males, Argentina, Brazil, and Uruguay exhibited decreasing trends in almost all measures. The exception was Uruguay, where incidence remained stationary. Argentina demonstrated the most significant decreases in APCs among the countries. Among females, Argentina presented stationary trends across all measures. In Brazil, incidence trends were stationary, while mortality and DALYs showed decreases. Uruguay, on the other hand, displayed increasing incidence, stationary mortality, and decreasing DALYs trends. In contrast, Paraguay and Venezuela showed no decreasing trends for either sex. Both countries experienced increasing incidence trends for males and females, while the other measures remained stationary.
Figure 2 illustrates the trends in LOC ASRs for males from 2005 to 2021. Uruguay consistently recorded the highest incidence ASRs throughout the analyzed period. However, Brazil exhibited higher mortality and DALYs ASRs compared to Uruguay. Nevertheless, both mortality and DALYs rates in Brazil showed significant declines over time. In Argentina, ASRs for all indicators demonstrated marked decreases, contrasting with Paraguay, which initially had lower ASRs than Argentina but eventually surpassed it across all indicators. Meanwhile, Venezuela exhibited fluctuating ASRs for all indicators; however, over the last decade, these rates displayed an upward trend.
Figure 3 shows the trends in LOC ASRs for females from 2005 to 2021. The magnitude of ASRs was lower compared to males. Similar to the male scenario, Brazil’s incidence ASRs were lower than those in Uruguay, though mortality and DALYs were higher. Despite this, in recent years, these ASRs have been decreasing for females in Brazil, while in Uruguay they have fluctuated. Only in the last few years of the time series did Argentina show a decreasing trend for females. Similar to males, Venezuela’s ASRs fluctuated over time, but in the last decade, they demonstrated an increasing trend. Paraguay consistently reported the lowest ASRs across all indicators throughout the period, with a gradual and steady increase.
4. Discussion
In this study, Paraguay and Venezuela exhibit the lowest MPOWER scores within MERCOSUR and are the only countries that did not show any indicators of a decreasing trend in LOC from 2005 to 2021. In the other hand, Argentina, Brazil, and Uruguay demonstrated improvements in MPOWER scores and reductions in LOC ASRs, particularly for men. Among these top-performing countries, Uruguay exhibited an increasing trend in incidence rates for women, while all other indicators remained either decreasing or stable.
The influence of WHO-FCTC on the burden of oral cancer remains uncertain. Socioeconomic, cultural, and political factors play a significant role in this dynamic, impacting how tobacco control policies affect tobacco use prevalence [16]. Furthermore, socioeconomic status influences the distribution of oral cancer burden [17]. Studies reveal that in Latin American countries with weaker MPOWER implementations, smoking is more closely linked to higher oral cancer mortality rates [11]. Additionally, strong adoption of MPOWER measures could potentially prevent a significant number of tobacco-related deaths, particularly cancer-related cases [18, 19]. Thus, monitoring cancer trends is crucial for understanding whether tobacco control measures are beginning to show effects, or if alternative strategies need exploration. Recent time series analyses reveal differing patterns of oral cancer trends across MERCOSUR countries, depending on the analyzed period [11,12,20].
Herrera-Serna et al. [11] analyzed oral cancer mortality trends in Latin American countries, focusing on tobacco and alcohol consumption prevalence, as well as respective control policies. They found limited progress in tobacco and alcohol control in Paraguay, where mortality trends remained stationary for both men and women from 2000 to 2017. Venezuela also showed stationary trends for oral cancer mortality in men during the same period, although rates declined for women. Our study provides additional insights into incidence trends, which are increasing for both men and women in Paraguay and Venezuela. The scenario in these countries appears to be linked to slow implementation of tobacco control policies, emphasizing the urgent need for intensified measures. Paraguay, in particular, has low scores in the ‘raise taxes on tobacco’ measure, a critical component for effective tobacco control [16,21]. Venezuela must improve its tobacco monitoring and control policies, as they have deteriorated in recent years.
In this study, Argentina, Brazil and Uruguay presented better progress towards the MPOWER measures. Most of the trends among men for these countries were decreasing. Brazil has been reducing the prevalence of tobacco use largely in the past decades [11,22,23]. In this study, Brazil was the country with more decreasing indicators of LOC, with almost all trends decreasing, except for incidence of women, which was stationary. However, Argentina's APCs among men showed greater declines than in Brazil, suggesting that LOC reductions in Brazil, especially for incidence rates, do not appear to be reducing proportionately to what might be expected based on the large reduction in tobacco prevalence. Brazil is a very large country, with many particularities. In addition to the differences of tobacco control that could be happening over the country, other risk factors could be influencing the oral cancer burden, such as alcohol and, very importantly, socioeconomic factors [17, 24].
Argentina, Brazil, and Uruguay showed better progress towards MPOWER measures. Most indicators for these countries demonstrated decreasing trends among men. Brazil has been significantly reducing tobacco use prevalence over the past decades [11,22,23]. In this study, Brazil had the most notable reduction in LOC indicators, with nearly all trends decreasing except for the stationary incidence rates for women. However, Argentina’s APCs among men demonstrated greater declines than Brazil, suggesting that LOC reductions in Brazil, particularly for incidence rates, are not proportional to reductions in tobacco prevalence. Brazil, being a vast country with diverse regions, may experience variations in tobacco control efforts. Other risk factors, including alcohol consumption and socioeconomic disparities [17, 24], likely contribute to oral cancer burdens, particularly when considering Brazil’s high Gini index [12].
In South America, Brazil and Uruguay have one of the highest oral cancer mortality rates [1]. Although Brazil has shown decreasing ASRs for mortality and DALYs for men, there is a discrepancy when compared to Uruguay, which has lower incidence rates but higher mortality and DALYs ASRs. Socioeconomic inequalities are likely contributing to these differences, as higher oral cancer mortality rates are associated with socioeconomic disparities in Latin American countries [25]. This highlights the need to address such inequalities to improve health outcomes.
Uruguay has consistently achieved high MPOWER scores, with significant progress in reducing tobacco consumption. According to Abascal et al. [26], between 2005 and 2011, Uruguay reduced tobacco consumption per person by 4.3% annually. However, only men’s mortality and DALYs ASRs have been decreasing, while women’s incidence ASRs are increasing in recent years. This finding aligns with Herrera-Serna et al. [20], who identified similar trends, suggesting a need for further investigation. Additionally, Abascal et al. [26] noted that women students in Uruguay exhibited higher tobacco consumption than male students between 2001 and 2009, with a female-to-male ratio of 1.32, highlighting a critical area for future research.
Argentina, although initially lagging behind Brazil and Uruguay in MPOWER scores, has shown promise in recent years. Tobacco use has been decreasing in Argentina [27], contributing to the significant declines observed in LOC trends for men. Women’s trends were stationary, but rates showed a declining trend in recent years. Given these findings, Argentina’s trajectory for oral cancer appears promising for the next decade.
The illegal trade of tobacco remains a critical issue. MERCOSUR’s Intergovernmental Commission for Tobacco Control and WHO-FCTC have made eliminating illicit tobacco trade a priority [10,28]. In countries like Paraguay, which is a significant supplier of illegal cigarettes in Latin America [30], addressing this issue is essential for enhancing the effectiveness of tobacco control measures [29]. Illicit trade undermines tobacco control policies by increasing accessibility and reducing the cost of tobacco products [28].
Limitations. Studies based on secondary data face several limitations, including variability and reliability of data sources. However, GBD methodologies are continually refined, resulting in more accurate and representative estimates [31]. Another limitation is that oral cancer is influenced by various risk factors beyond tobacco use, such as alcohol consumption, diet, and socioeconomic level [32]. Despite the descriptive nature of this study, it provides a valuable exploratory analysis of the oral cancer scenario in MERCOSUR countries. MPOWER scores serve as reliable indicators of tobacco control effectiveness and represent countries’ dedication to tobacco regulation. While the timeline may still be short to assess the full impact of WHO-FCTC on oral cancer rates, it is essential to understand the distinct needs and circumstances of each country, especially in Latin America, where socioeconomic complexity plays a significant role.
5. Conclusions
The MERCOSUR countries with the highest MPOWER scores—Argentina, Brazil, and Uruguay—are demonstrating decreasing trends in certain indicators of lip and oral cavity cancer, particularly among men. On the other hand, Paraguay and Venezuela, which have the lowest MPOWER scores, have shown no decreasing trends in these cancer indicators. It is essential to recognize that MPOWER scores reflect the strength of tobacco control measures, but other factors also contribute to the burden of lip and oral cavity cancer in each country. Therefore, this study suggests that MERCOSUR countries with a history of more rigorous tobacco control policies may already be experiencing declining trends in the burden of lip and oral cavity cancer, though further research is needed to fully understand this relationship.
Author Contributions
Conceptualization, A.R.C., F.N.H. and J.M.A.; methodology, L.M.H., A.R.C., F.N.H. and J.M.A.; software, L.M.H. and A.R.C.; validation, F.N.H. and J.M.A.; formal analysis, L.M.H. and A.R.C.; investigation, L.M.H., F.J.M., A.R.C., F.N.H. and J.M.A.; writing—original draft preparation, L.M.H. and F.J.M.; writing—review and editing, A.R.C., F.N.H. and J.M.A.; supervision, A.R.C., F.N.H. and J.M.A.; project administration, J.M.A.; funding acquisition, L.M.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The author acknowledge to Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES-Brazil) for granting a scholarship to L.M.H.
Institutional Review Board Statement
Ethical review and approval were waived for this study because the data accessed were secondary, available in publicly accessible databases, and there was no identification of cases.
Data Availability Statement
The data used in this study are estimates resulting from the 2021 GBD study. They are available on the website of the Institute for Health Metrics and Evaluation [14], and can be publicly consulted and downloaded.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- GBD 2019 Lip, Oral, and Pharyngeal Cancer Collaborators. The Global, Regional, and National Burden of Adult Lip, Oral, and Pharyngeal Cancer in 204 Countries and Territories: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2023, 9, 1401–1416. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Cancer Collaboration. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019 A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef] [PubMed]
- Mello, F.W.; Melo, G.; Pasetto, J.J.; Silva, C.A.B.; Warnakulasuriya, S.; Rivero, E.R.C. The synergistic effect of tobacco and alcohol consumption on oral squamous cell carcinoma: a systematic review and meta-analysis. Clin. Oral. Invest. 2019, 23, 2849–2859. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Jethwa, A.R.; Khariwala, S.S. Tobacco-related carcinogenesis in head and neck cancer. Cancer Metastasis Rev. 2017, 36, 411–423. [Google Scholar] [CrossRef]
- World Health Organization. WHO Framework Convention on Tobacco Control. Geneva: World Health Organization; 2003. Available online: https://fctc.who.int/resources/publications (accessed on 14 December 2024).
- WHO report on the global tobacco epidemic, 2023: protect people from tobacco smoke. Available online: https://www.who.int/publications/i/item/9789240077164 (accessed on 14 December 2024).
- GBD 2019 Cancer Risk Factors Collaborators. The global burden of cancer attributable to risk factors, 2010–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 563–591. [Google Scholar] [CrossRef]
- Nocini, R.; Lippi, G.; Mattiuzzi, C. The worldwide burden of smoking-related oral cancer deaths. Clin Exp Dent Res. 2020, 6, 161–164. [Google Scholar] [CrossRef]
- Instituto Nacional de Câncer (INCA). Relatório Evolutivo da Comissão Intergovernamental para o Controle do Tabaco. Brasil: INCA, 2012. Available online: https://ninho.inca.gov.br/jspui/ (accessed on 10 January 2025).
- Herrera-Serna, B.Y.; Lara-Carrillo, E.; Toral-Rizo, V.H.; Amaral, R.C. Efecto de las Políticas de Control de Factores de Riesgo Sobre la Mortalidad por Cáncer Oral en América Latina. Rev Esp Salud Pública. 2019, 93, 1–14. [Google Scholar]
- Herrera-Serna, B.Y.; Lara-Carrillo, E.; Toral-Rizo, V.H.; Amaral, R.C.; Aguilera-Eguía, R.A. Relationship between the Human Development Index and its Components with Oral Cancer in Latin America. J Epidemiol Glob Hea. 2019, 9, 223–232. [Google Scholar] [CrossRef]
- WHO. The Global Health Observatory. Available online: https://www.who.int/data/gho (accessed on 31 November 2024).
- IHME. GHDx: GBD Results Tool. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 31 November 2024).
- Antunes, J.L.; Waldman, E.A. Trends and spatial distribution of deaths of children aged 12- 60 months in São Paulo, Brazil, 1980–1998. Bull World Health Organ. 2002, 80, 391–398. [Google Scholar]
- Flor, L.S.; Reitsma, M.B.; Gupta, V.; Ng, M.; Gakidou, E. The effects of tobacco control policies on global smoking prevalence. Nat Med. 2021, 27, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Conway, D.I.; Petticrew, M.; Marlborough, H.; Berthiller, J.; Hashibe, M.; Macpherson, L.M.D. Socioeconomic inequalities and oral cancer risk: a systematic review and meta-analysis of case-control studies. Int J Cancer. 2008, 122, 2811–2819. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.L.; Togawa, K.; Gilmour, S.; Leon, M.E.; Soerjomataram, I.; Katanoda, K. Projecting the impact of implementation of WHO MPOWER measures on smoking prevalence and mortality in Japan. Tob Control. 2022, 33, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, M.; Alhusseini, N.; Samhan, L.; Samhan, S.; Abbad, T. Tobacco control policies implementation and future lung cancer incidence in Saudi Arabia. A population-based study. Prev. Med. Rep. 2023, 36. [Google Scholar] [CrossRef]
- Herrera-Serna, B.Y.; Betancourt, J.A.O.; Soto, O.P.L.; Amaral, R.C.; Correa, M.P.C. Trends of incidence, mortality, and disability-adjusted life years of oral cancer in Latin America. Rev Bras Epidemiol. 2022, 25. [Google Scholar] [CrossRef]
- Sóñora, G.; Reynales-Shigematsu, L.M.; Barnoya, J.; Llorente, B.; Szklo, A.S.; Thrasher, J.F. Achievements, Challenges, Priorities and Needs to Address the Current Tobacco Epidemic in Latin-america. Tob Control. 2022, 31, 138–141. [Google Scholar] [CrossRef]
- GBD Study 2019 Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet. 2021, 397, 2337–2360. [Google Scholar] [CrossRef]
- Tam, J.; Jaffri, M.A.; Mok, Y.; Jeon, J.; Szklo, A.S.; Souza, M.C.; Holford, T.R.; Levy, D.T.; Cao, P.; Sánchez-Romero, L.M.; Meza, R. Patterns of Birth Cohort‒Specific Smoking Histories in Brazil. Am J Prev Med. 2023, 64, 63–71. [Google Scholar] [CrossRef]
- Freire, A.R.; Freire, D.E.W.G.; Araújo, E.C.F.d.; de Lucena, E.H.G.; Cavalcanti, Y.W. Influence of Public Oral Health Services and Socioeconomic Indicators on the Frequency of Hospitalization and Deaths due to Oral Cancer in Brazil, between 2002–2017. Int. J. Environ. Res. Public Health. 2021, 18, 238. [Google Scholar] [CrossRef]
- Freire, A.R.; Freire, D.E.W.G.; Araújo, E.C.F.; Carrer, F.C.A.; Pucca Júnior, G.A.; Sousa, S.A.; Lucena, E.H.G.; Cavalcanti, Y.W. Socioeconomic indicators and economic investments influence oral cancer mortality in Latin America. BMC Public Health. 2021, 21. [Google Scholar] [CrossRef]
- Abascal, W.; Esteves, E.; Goja, B.; Mora, F.G.; Lorenzo, A.; Sica, A.; Triunfo, P.; Harris, J.E. Tobacco control campaign in Uruguay: a population-based trend analysis. Lancet. 2012, 380, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- Salgado, M.V.; Mok, Y.; Jeon, J.; Jaffri, M.; Tam, J.; Holford, T.R.; Sánchez-Romero, L.M.; Meza, R.; Mejia, R. Smoking patterns by birth cohort in Argentina: an age-period cohort population-based modeling study. Lancet Reg Health Am. 2024, 36. [Google Scholar] [CrossRef] [PubMed]
- WHO Framework Convention on Tobacco Control. Protocol to Eliminate Illicit Trade in Tobacco Products. Available online: https://fctc.who.int/news-and-resources/publications (accessed on 10 January 2025).
- Ramos, A. Illegal trade in tobacco in MERCOSUR countries. Trends Organ Crim. 2009, 12, 267–306. [Google Scholar] [CrossRef]
- Masi, F.; Rodriguez-Iglesias, G.; Drope, J. Regional implications of the tobacco value chain in Paraguay. Tob Control. 2022, 31, 140–145. [Google Scholar] [CrossRef]
- GBD Study 2021 Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023, 403, 2133–2161. [Google Scholar] [CrossRef]
- Conway, D.I.; Purkayastha, M.; Chestnutt, I.G. The changing epidemiology of oral cancer: definitions, trends, and risk factors. Br Dent J. 2018, 225, 867–873. [Google Scholar] [CrossRef]
Figure 1.
MPOWER measures scores of MERCOSUR countries, in 2007, and then biennially, between 2008 and 2020.
Figure 1.
MPOWER measures scores of MERCOSUR countries, in 2007, and then biennially, between 2008 and 2020.
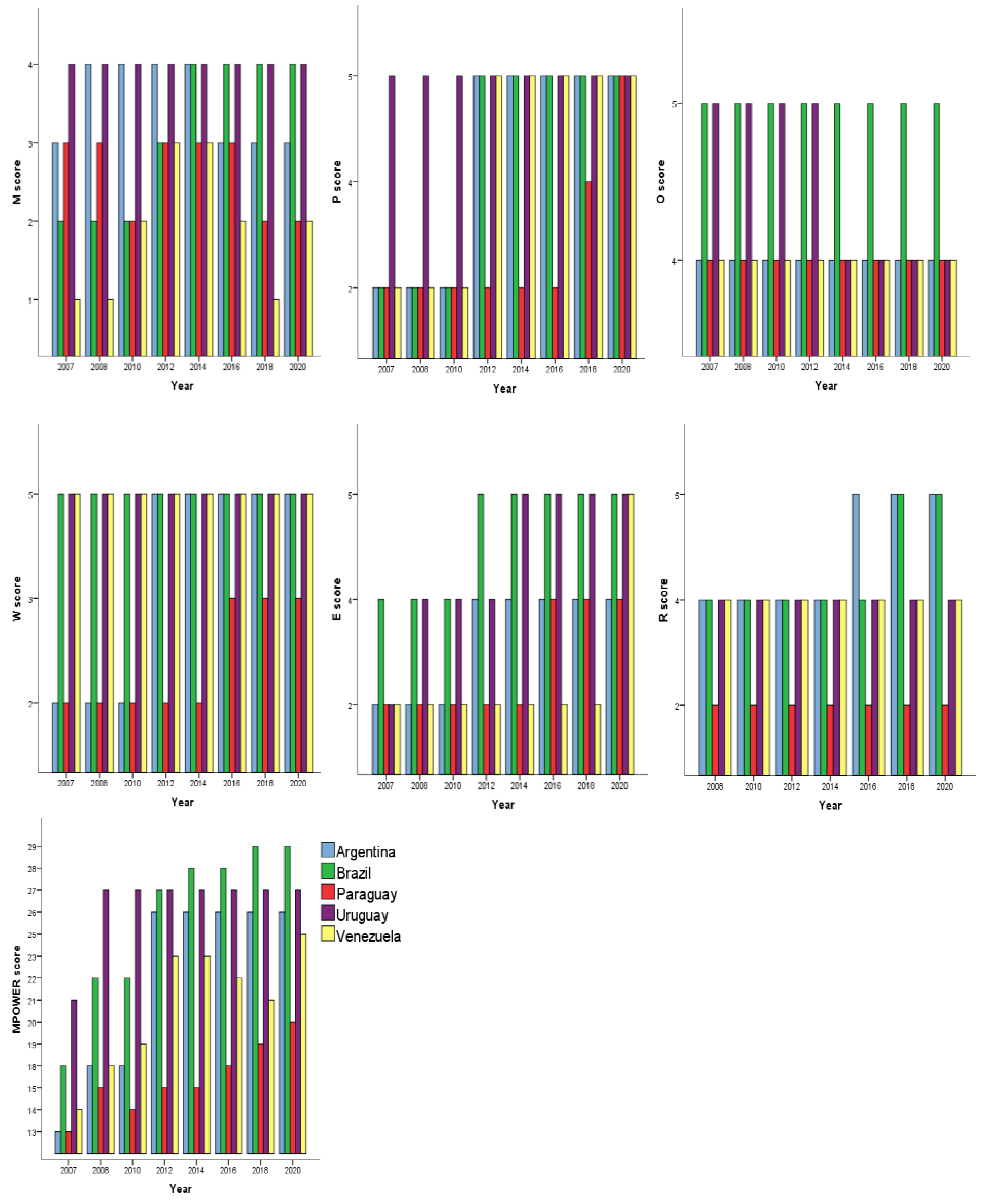
Figure 2.
Incidence, mortality and DALYs Age-standardized Rates of lip and oral cavity cancer among males in MERCOSUR countries between 2005 and 2021.
Figure 2.
Incidence, mortality and DALYs Age-standardized Rates of lip and oral cavity cancer among males in MERCOSUR countries between 2005 and 2021.
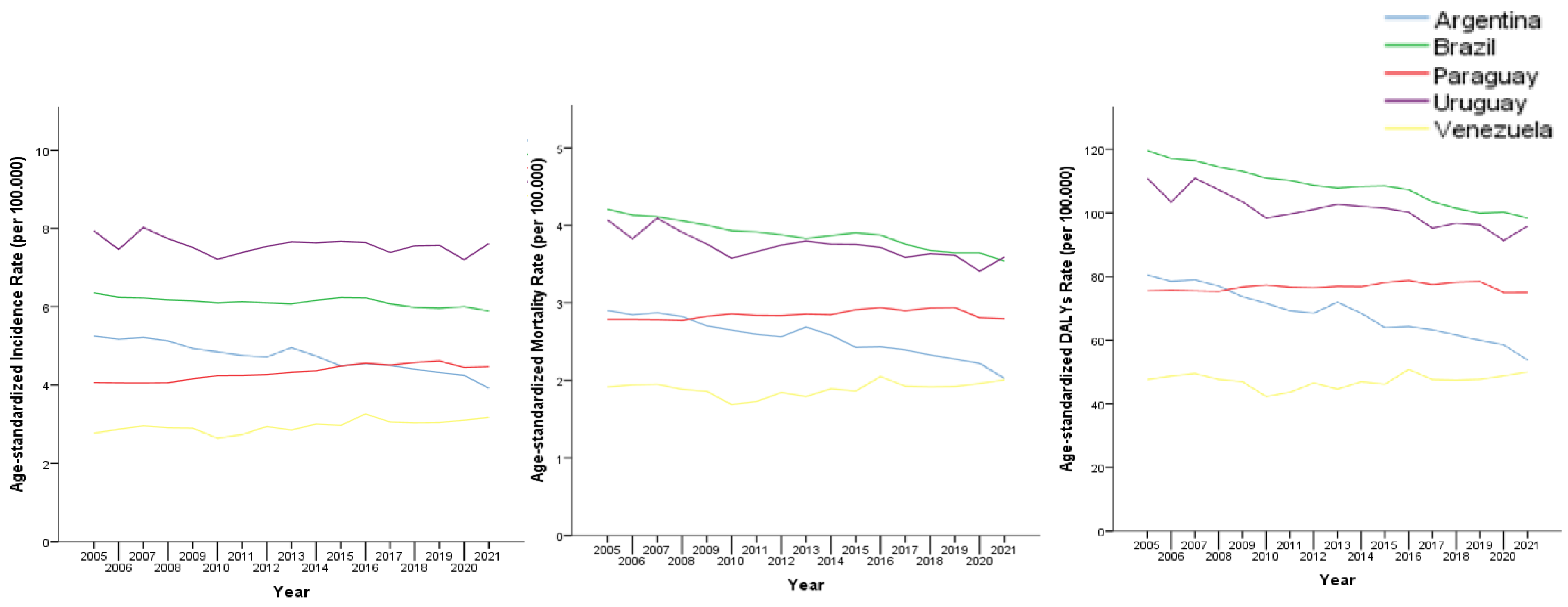
Figure 3.
Incidence, mortality and DALYs Age-standardized Rates of lip and oral cavity cancer among females in MERCOSUR countries between 2005 and 2021.
Figure 3.
Incidence, mortality and DALYs Age-standardized Rates of lip and oral cavity cancer among females in MERCOSUR countries between 2005 and 2021.
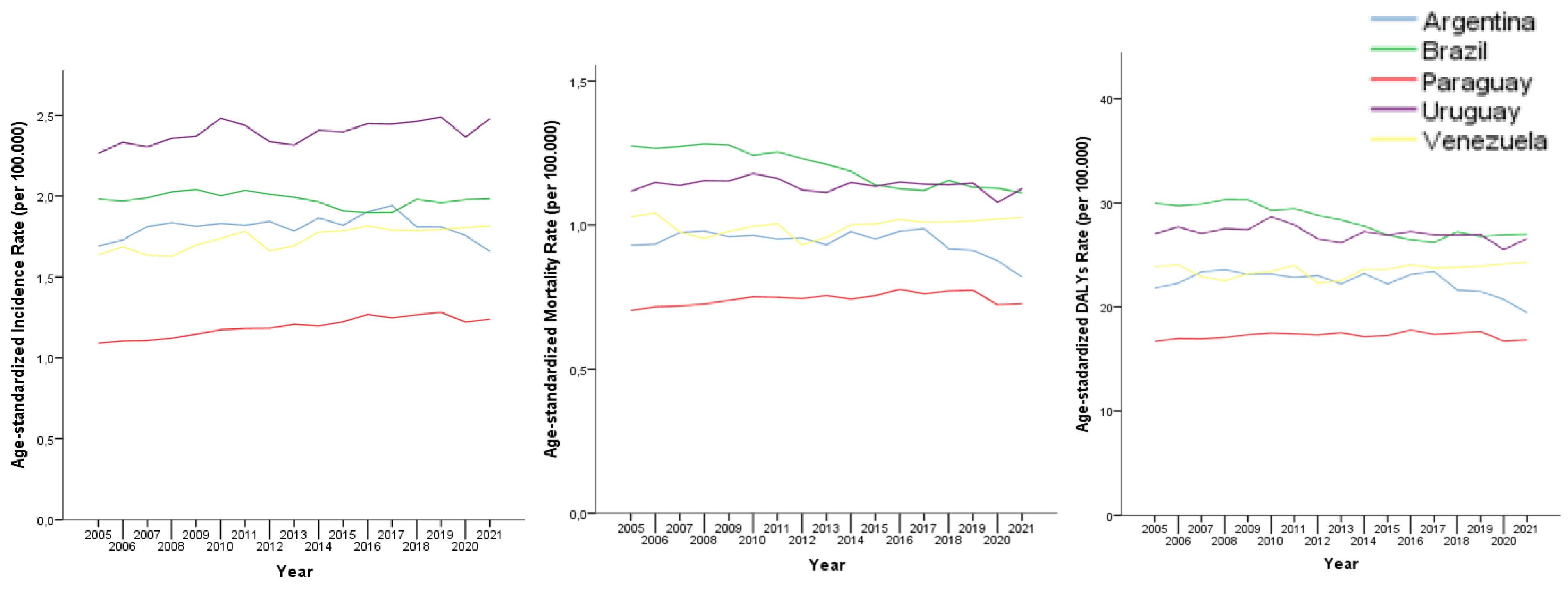

Table 1.
Median and interquartile range (IQR) of MPOWER scores of MERCOSUR countries.
| Countries | M | P | O | W | E | R | MPOWER |
|---|---|---|---|---|---|---|---|
| Argentina | 3.50 [3;4] | 5.0 [2;5] | 4.0 [4;4] | 5.0 [2;5] | 4.0 [2;4] | 4.5 [4;5] | 26.0 [18;26] |
| Brazil | 3.50 [2;4] | 5.0 [2;5] | 5.0 [5;5] | 5.0 [5;5] | 5.0 [4;5] | 4.0 [4;5] | 27.5 [22;28.3] |
| Paraguay | 3.0 [2;3] | 2 [2;2.5] | 4.0 [4;4] | 2.0 [2;3] | 2 [2;5] | 2.0 [2;2] | 15.0 [14.8;19;3] |
| Uruguay | 4.0 [4;4] | 5.0 [5;5] | 4.5 [4;5] | 5.0 [5;5] | 4.5 [4;5] | 4.0 [4;4] | 27.0 [27;27] |
| Venezuela | 2.0 [1;2.25] | 5.0 [2;5] | 4.0 [4;4] | 5.0 [5;5] | 2 [2;2] | 4.0 [4;4] | 21.5 [8.8;23] |
Table 2.
Incidence, mortality and DALYs ASR trends, Annual Percent Change (APC) and 95% Confidence Intervals (95%CI) of the time series (2005 to 2021).
Table 2.
Incidence, mortality and DALYs ASR trends, Annual Percent Change (APC) and 95% Confidence Intervals (95%CI) of the time series (2005 to 2021).
| Country | Sex | Incidence trend (APC [95%CI]) |
Mortality trend (APC [95% CI]) |
DALYs trend (APC [95%CI]) |
|---|---|---|---|---|
| Argentina | Male | Decreasing (-1.55[1.87;-1.24]) | Decreasing (-1.98[-2.39;-1.56]) | Decreasing (-2.24[-2.56;-1.92]) |
| Female | Stationary (-0.02[-0.76;0.74]) | Stationary (-0.65[-1.50;0.21]) | Stationary (-0.63[-1.40;0.14] | |
| Brazil | Male | Decreasing (-0.37[-0.59;-0.15]) | Decreasing (-0.98[-1.20;-0.76]) | Decreasing (-1.16[-1.34;-0.98]) |
| Female | Stationary (-0.10[-0.46;0.27]) | Decreasing (-0.95[-1.27;-0.63]) | Decreasing (-0.79[-1.22;-0.36]) | |
| Paraguay | Male | Increasing (0.74[0.39;1.09]) | Stationary (0.14[-0.18;0.46]) | Stationary (0.05[-0.22;0.33]) |
| Female | Increasing (0.91[0.58;1.24]) | Stationary (0.27[-0.16;0.71]) | Stationary (0.08[-0.18;0.34]) | |
| Uruguay | Male | Stationary (-0.21[-0.50;0.07]) | Decreasing (-0.72[-1.06;-0.38]) | Decreasing -0.89[-1.18;-0.59]) |
| Female | Increasing (0.40[0.14;0.66]) | Stationary (-0.13[-0.34;0.09]) | Decreasing (-0.27[-0.53;-0.02]) | |
| Venezuela | Male | Increasing (0.77[0.26;1.27]) | Stationary (0.31[-0.43;1.07]) | Stationary (0.24[-0.47;0.96]) |
| Female | Increasing (0.67[0.42;0.93]) | Stationary (0.12[-0.32;0.56]) | Stationary (0.21[-0.12;0.54]) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



