
Submitted:
20 January 2025
Posted:
21 January 2025
You are already at the latest version
Abstract
Beals-Hecht (BH) syndrome is a rare autosomal dominant disorder caused by a mutation of the FBN2 gene that codifies for fibrillin-2 (FBN-2) and part of its nosology is congenital contractural arachnodactyly. There is no information in the literature on whether there is increased oxidative stress (OS) in these patients that could lead to a break-down in the redox balance. Therefore, the aim of this preliminary study was to evaluate the possible breakdown of redox homeostasis in the thoracic aortic aneurysm (TAA) in BH. We determinate OS markers such as malondialdehyde (MDA), total antioxidant capacity (TAC), carbonyl groups, glutathione (GSH), thiols and the nitrate/nitrite ratio (NO3−/NO2−) by spectrophotometry in homogenized TAA from controls subjects (CS) and BH. We also measured the activities of some of antioxidant enzymes such as GST, GPx, GR and TrxR. The super oxide dismutase (SOD) isoforms, catalase and peroxidase activities were evaluated by native polyacrylamide gels. The activities of the antioxidant enzymes GPx and TrxR were decreased (p≤0.04) and the OS markers NO3−/NO2−, TAC and thiols groups were decreased (p≤0.04). The results suggest an intricate system in the loss of redox homeostasis in BH syndrome patients that could contribute to the FBN2 instability.
Keywords:
Beals-Hecht syndrome
; Oxidative stress
; Redox homeostasis
; Antioxidant enzymes
; FBN-2
1. Introduction
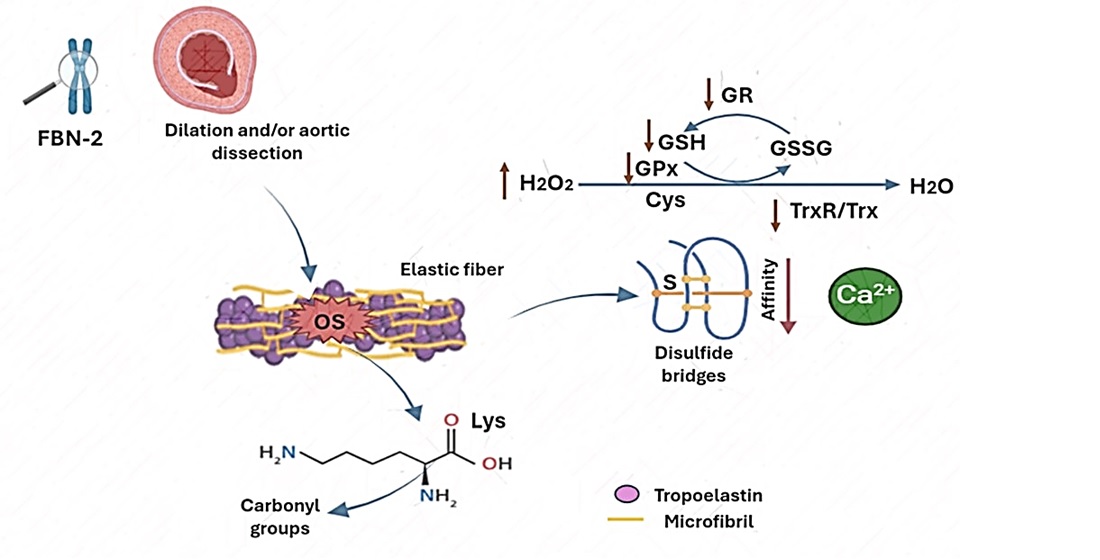
The Beals-Hecht (BH) syndrome is a pathology with an incidence of less than 1 case per 10,000 people, and it is manifested by congenital contractural arachnodactyly (CCA) [1]. It is an autosomal dominant disorder caused by a pathogenic variant of the fibrillin-2 (FBN-2) gene, that is located in chromosome 5q23.31. The fibrillin-2 (FBN-2) protein consists of five domains which are; bind calcium, epidermal growth factor (cbEGF), an EGF-like structural domain, a glycine-rich region, hybrid (hyb) domain, and an 8-cysteine repeat region [2]. The fibrillin’s are major constituents of the extracellular matrix (ECM) and provide connective tissue elasticity and mechanical force, which allows for the communication between cells through integrin receptors, and modulates the concentration, presentation, activation and bioavailability of transforming growth factor (TGFβ) and bone morphogenetic protein (BMP) complexes [3]. Fibrillin’s are extensively spread in organs and tissues and serve as templates for the deposition of elastin during elastic fibers (EF) formation. They are essential for maintaining the integrity of tissues such as skin, blood vessels, lungs and the ocular ligament [4]. The nosology caused by the FBN-2 mutation in patients with BH syndrome is characterized by flexion contractures of multiple joints including elbows, knees, hips, ankles, and with long spider-like fingers, CCA, camptodactyly, contracture of major joints, scoliosis, pectus deformities and crumpled ears. Occasionally, there may be cardiovascular signs as in the Marfan syndrome (MFS) and, rarely, aortic dissection [5]. The mutation in the FBN-2 gene is the only known one that is associated with CCA.
The nosology, the mutations of the FNB-2 gene in the patients with BH syndrome and the consequences present in patients who suffer from it have been described in the literature. However, to date, no basic research has addressed whether these patients may be experiencing oxidative stress (OS), as is present in MFS and Loeys-Dietz syndrome patients, who show increased reactive oxygen species (ROS) and depletion in the antioxidant enzymatic system [6,7].
On the other hand, the redox homeostasis is of vital importance to maintain the balance between ROS and the enzymatic and non-enzymatic antioxidant systems in humans. A disturbance in any of these systems can cause the alteration of the redox homeostasis leading to OS which is characterized by an increase in the ROS such as super oxide anion (O2–), hydrogen peroxide (H2O2), and hydroxyl groups (OH–) [8]. In this sense, the disturbance in redox homeostasis could favor a chronic systemic oxidative background in patients with BH leading to a positive feedback circuit, and fibrillin instability, thus contributing to the anatomical alterations present in these patients. Therefore, the objective of this preliminary study was to evaluate the possible break-down of redox homeostasis in TAA in BH syndrome patients.
2. Results
Table 1 describes the positive characteristics of the Ghent criteria in the three cases of the BH syndrome patients. The three cases included were men with an overall median age old of 38 (min 30 – max 66).
Table 2 describes the clinical and symptomatic characteristics of the three patients with BH and the three control subjects.
Table 3 shows the demographic characteristics, comorbidities, serum biochemistry and general characteristics of the aorta in the three patients with BH and the three CS positive.
OS markers of the non-enzymatic system components are shown in Figure 1. In this study we determined were NO3–/NO2– ratio, TAC, GSH and thiols groups which were decreased in patients with BH syndrome in comparison with CS (p<0.001 panel A, p=0.04 panel B, p=0.03 panel E and p=0.009 panel F respectively). The carbonyl groups did not show a statistical difference although it tended to decrease in the BH patients (p=0.08). The LPO-index were not significantly modified between both groups.
Figure 2 shows that the GPx and TxrR activities in the homogenized tissue from the TAA of HB patients was decreased in comparison with CS (p=0.04 and p=0.001, panel A and D respectively). However, the activities of the GR and GST did not change in BH in comparison with CS (panel C).
The activity of the SOD-1 was decrease (p=0.001 Figure 3A) but the -2 isoform did not change in BH in comparison with CS (Figure 3B). However, the peroxidases and catalase activities (Figure 4A, p=0.1 and B, p=0.05, respectively) showed a tendency and decrease respectively in BH in comparison with CS.
3. Discussion
The alteration of the redox homeostasis in the TAA in patients with MFS and in some of its variants such as the Loeys-Dietz syndrome has been previously demonstrated [10,11]. However, there is no information in the literature on the alteration of redox homeostasis linked to an increase in the oxidant background, in the patients with the BH syndrome which might perhaps be associated with the FBN-2 gene mutation. Therefore, the aim of this study was to demonstrate whether there is an alteration of redox homeostasis in patients with BH syndrome.
The MFS clinical identification is through the Ghent criteria or genetic mapping; however, there are only clinical data that guide the physician to suspect the diagnosis in the BH syndrome. In this series of cases, we were able to differentiate the patients from MFS with respect to BH syndrome through the scoring system proposed by Meerschaut et al. [9] for CCA which is one of the main characteristics of this syndrome. This scoring method allows for the classification and suspicion of the diagnosis with a sensitivity of 75% and specificity of 60%, when a genetic determination is not available [12]. The overlap of several clinical conditions in both syndromes can be explained because both present mutations in two homologous genes FBN-1 and FBN-2, with similar functions. Nevertheless, the altered gene the MFS for FBN-1 is located in chromosome 15q15-21.3 and the modified gene in patients with BH syndrome is in 5q23-31 and encodes for FBN-2 [13]. Both mutations have been related to skeletal, cardiovascular and aortic damage, and reports of cardiac abnormalities in BH syndrome have been going on for more than 4 decades. Mutations of both fibrillin’s have been found in a single patient and reported in the literature, a situation that can synergistically worsen cardiovascular manifestations and these patients also present other comorbidities [14]. In this sense, FBN-2 participates in the formation of the embryonic valve, and is pointed out as a molecular factor involved in this phase of bicuspid aortic valve complexity [15]. Also, patients with BH in this series of cases, have severe dilatation of the roots of both great arteries with aortic insufficiency [16].
Likewise, although patients with only CCA, as in BH syndrome seem to have a favorable prognosis. Nevertheless, cases have been identified that have shown an association of the presence of aortic dilation and aortic dissection with some polymorphisms in the FBN-2 gene [17]. In these cases, timely clinical detection and imaging studies make it possible to detect the possible aortic disease early, and FBN-2 genetic testing could be useful to identify them [17].
In this respect, ten novel mutations have been identified in the critical region of FBN-2 in patients with BH, indicating a 75% mutation detection rate in this limited region. Interestingly, none of these identified FBN-2 mutations alter amino acids in the calcium-binding consensus sequence in the EGF-like domains, whereas many of the FBN-1 mutations alter this consensus sequence. This indicates that patients with BH have aortic root dilatation and the vast majority lack evidence of congenital heart disease. In addition, the FBN-2 spans more than 28 kb and 65 exons. It is expressed early in development and is constrained to bone and cartilage matrices in adult tissues being essential in the EF formation. The pathogenic variant causes a decrease in the amount of FBN-2 protein available to form microfibrils; hence, the low levels of microfibril reduce the EF, resulting in the symptoms exhibited by patients with BH such as providing strength and flexibility to the connective tissue that sustains the body’s joints and organs [18]. These findings have led to a search for a better understanding of the molecular basis of CCA and the mechanisms of damage that interact through inflammatory status and oxidative dysregulation in particular in patients with BH syndrome [13].
On the other hand, EF assembly is a multistep process in which tropo-elastin (TE) monomers are secreted from elastogenic cells and self-assemble/coacervate to form microaggregates that interact with fibulin-4 (Fbln) and -5. This is a fundamental initial step for the generation of mature EF. In this process, the amino acids in TE could be susceptible to oxidative modifications and thus affect EF. In this sense, carbonyl formation by ROS on side chains of specific amino acids as Lys, Arg, Pro, and Thr may occurs resulting in an alteration of protein structure and function; for example, oxidative modifications to collagen cause a change in the elasticity of the skin, as well as stiffer and more brittle cartilage [19]. the above supports the theory that each protein interaction during assembly could actively participate together in the structural alteration observed in patients with aortic dilatation and dissection.
Our results only show a tendency to a decrease in the carbonyl groups in the patients with BH. A possible explanation could be because of the small sample of patients. However, the amino acids in TE are susceptible to oxidative modifications and this may favor the carbonylation which is associated with a decrease in TAC. In addition, another component of the EF is FBN-2 which contains two hyb domains composed of a TB/8-Cys-rich glycoprotein region with disulphide bridges between the Cys which are necessary for the temporal and hierarchical assembly of microfibrils and that are indispensables to sequester TGFβ [20]. The formation of intermolecular disulphide bond is also not suitable between a conserved extra Cys in domain hyb1 as an early part of the microfibril assembly process in cbEGF domains and may result in reduced calcium affinity, and destabilization of the linkage of the cbEGF domain [21,22,23].
The TrxR/Trx system is fundamental for the equilibrium of redox homeostasis and disulphide bond regeneration. TrxR reduces thioredoxin (Trx) through of the GSH oxidation in the presence of NADPH+, resulting in reduction of disulfide bridges (thiols groups) between Cys . It contributes to reduces the protein dysfunction, cellular receptor inactivity, and loss of enzyme activity caused by ROS [24]. Three TrxR isoforms (nuclear, mitochondrial and cytosolic) have been described in mammals and there are high and low expressions of Trx in the abdominal aorta aneurysms in the luminal and abluminal faces of arteries [25]. An efficient TrxR/Trx system contributes to decreases endothelial dysfunction and is associated with an anti-thrombotic and proinflammatory state. However, the loss of alteration of the TrxR/Trx system contributes to severe OS resulting in disturbances of redox homeostasis [7]. Our results show a decrease both in the TrxR activity and the concentration of thiol groups in the homogenized tissue from the TAA. These results suggest that the TrxR/Trx system is highly compromised in this syndrome and might contribute to decrease the EF maturation [26]. These changes could also be associated to the lack of disulphide bonds formed among TB/8-Cys-rich glycoprotein region of the FBN-2 [27]. In addition, the low TrxR activity could also contribute to OS which is favored, in part, by the increase in the ROS such as hydrogen peroxide (H2O2).
Moreover, one of the enzymes that uses H2O2 as a substrate in the presence of GSH is GPx. Our results showed a decrease in the activity of this enzyme. This suggest that this decrease could be due to the high concentration of intracellular H2O2 (enzymatic activity inhibition by substrate) [28]. GPx may regulates the H2O2 concentration, having a modulating effect on the TGF-β1 signaling pathways [28], GPx is also capable of acting as a peroxinitrite (ONOO–) reductase. A decrease in its activity could cause the accumulation of RNS in the aortic smooth muscle cells of this patients as has been described in MFS and contribute to TAA [29,30]. Furthermore, ONOO– affects the enzymatic activities by introducing tyrosine residues or oxidizing thiol groups thereby leading to 3-nitrotyrosine formation or formation of oxidized thiol groups in proteins. In this sense, the ONOO– is the result of the oxidation of the nitric oxide (NO) by O2– [31]. Our results show a decrease in the NO3–/NO2– ratio and this reduction could be in part due to the rapid oxidation of NO to ONOO–. The TE is susceptible to oxidative modifications by ONOO−, such as been shown in immunoblot analysis where TE is oxidatively by the ONOO− and hypochlorous acid activated by monocytes and macrophages. In this sense, a study in vitro elastic fiber assembly model, showed that oxidatively modified TE failed to form EF through of the cross-linking and interactions with other proteins required for EF assembly, including Fbln-4, -5, and FBN-2 [32]. These suggest that the ROS/RNS ratio can modify the TE and that these modifications affect EF assembly, such that OS is considered to influence structural and functional changes of EF under pathological conditions [32]. However, more studies are necessary for the confirmation of this hypothesis.
On the other hand, the tripeptide GSH inactivates ROS by itself and is a major thiol-disulfide redox buffer and antioxidant molecule that protects from overproduction of ROS under pathological conditions [33]. In addition, TxrR, GPx and GST require GSH as cofactor for ROS detoxification. This reaction converts to reduced GSH in oxidized GSSG [34]. Our results showed a GSH decrease, this result could suggest that the increased oxidative background in patients with BH may depleted this antioxidant molecule, contributing to the loss of the activity of TrxR and GPx and favoring the oxidative background. In this sense, the reduction of GSSG to GSH is catalyzed by GR. This enzyme acts as a control mechanism for the regeneration and re-establishment of the GSH concentration [35]. Our results show that the activity of GR tends to decrease in the patients with BH syndrome. This non- significant tendency could be due to the small sample size, but these results suggest that the chronic state of the OS may favor both the GSH oxidation by the loss of the by GR activity which may result in a decrease in the GSH regeneration [36].
Regarding the isoforms of SOD, catalase and peroxidases, which are enzymes that participate in a very important way in redox homeostasis it has been reported that they present alterations in MFS syndrome and contribute to OS [7,10]. The results show the presence of activity in the native polyacrylamide gels in SOD-1 (the manganese isoform which predominates in the mitochondria, and is very important in the muscular function to detoxicated the ROS) and catalase (an enzyme responsible for detoxifying H2O2) However, there were no changes in the activity of peroxidases, these results suggest that the patients with BH course with increase oxidative background in the TAA [7,10,11], that contribute in part to instability of the FBN-2 protein and EF.
4. Materials and Methods
4.1. Recruitment of the BH Patients and Control Subjects
This was an observational and comparative study between three BH patients versus three control subjects (CS) that attended in the aorta clinic of the National Institute of Cardiology Ignacio Chávez. The patients were classified with BH by the Ghent criteria. The research protocol was approved by the research and ethics committee of the National Institute of Cardiology Ignacio Chávez (protocol number 23-1366). Each BH and CS patient signed an informed consent form in accordance with the Helsinki Declaration, as amended by the Congress of Tokyo, Japan [37].
4.2. Ethical Considerations
An aortic tissue sample was obtained from BH patients for analysis during surgery. Patients were considered candidates for surgery when they had ≥ 5 cm dilation and had been previously presented and discussed in a medical-surgical session or when they had attended the Institute for the first time with dilation and/or aortic dissection. Inclusion criteria included patients who met the Ghent criteria evaluated by a rheumatology expert and that required surgical intervention of the thoracic aorta aneurysm (TAA), or another type of cardiovascular surgery, which was agreed upon consensus in a medical-surgical session. The patient’s age was of over 18 years old, and they belonged to any gender. The exclusion criteria were patients that did not agree to sign the informed consent form; patients who did not suspend oral nitrates, NSAIDs, statins, calcium antagonist; patients with β-blocker intake for 7 days prior to obtaining the samples; patients with neoplastic disease and/or associated infection; subjects with a smoking history in the last 4 years; patients with different phenotypic variants or phenotypes related to such as Shiprintzen–Goldberg, Ehler–Danlos, Alagille, Weill–Marchesani, Turner, Noonan, Marfan, MASS, and Loeys–Dietz (all its variants) syndromes, or with bicuspid aortic valve, or autosomal dominant polycystic, kidney disease. A segment of the ascending TAA was taken during the surgery procedure of Bentall and De Bono and stored at 4 °C [38].
The tissue used for the CS was obtained from patients that did not have aortic damage and did not undergo surgery for aortic stenosis, having had no syndrome pathology diagnosed. In these patients, there was no suspicion of inflammatory disease or the presence of a degenerative disorders such as thyroid and autoimmune diseases, hypertension or diabetes mellitus. Also, the drugs that could interfere with the outcome of the study such as NSAIDs or lipid-lowering agents were suspended in the perioperative period. Cases were dealt with cautiously, to avoid including patients undertaking treatment with allopurinol, antioxidants, or probable inhibitors of ROS production. Warfarin, aspirin, clopidogrel, anticoagulant, antiplatelet medications, and other similar drugs were suspended.
TAA, were obtained during surgery, samples of each tissue was sectioned into two portions, placed in tubes and transported under Liquid nitrogen and frozen at -70 °C until study. The studies requested during hospitalization for both BH patients and CS included the determination of triglycerides (TG), HDL, LDL, total cholesterol (CT), creatinine, and glucose. All assays on serum biochemical variables were made in duplicate.
4.3. Thoracis Aorta Homogenization
The segment from the TAA was homogenized under liquid nitrogen after adding KH2PO4 (2 mL) pH 7.3 in presence of 20 µL antiproteases inhibitors (1 mM PMSF, 2 μM pepstatin A, 2 μM leupeptin, and 0.1% aprotinin), and the preparation was kept in ice. The Bradford method was utilized to determine the protein concentration in the homogenates [39].
4.4. Oxidative Stress Markers
4.4.1. Determination of Malondialdehyde
Malondialdehyde (MDA) was read spectrophotometrically at 532 nm. A quantity of 100 μg of homogenized tissue from the TAA of BH patients and CS were used. Methanol with BHT at 4% (100 μL) plus KH2PO4 buffer pH 7.4 (1 mL) was added to sample and then it was incubated at 37 °C for 30 min after 2-thiobarbituric acid at 0.8 M (1.5 mL) was added. After that, the sample was incubated at 90 °C for 1 h. After, KCL at 5% (1mL) plus n-butanol (4 mL) were added and shaken for 30 s, and the sample was centrifuged at 4000 rpm (2 min). The butanol phase was extracted, and the absorbance was measured [6].
4.4.2. Evaluation of the Total Antioxidant Capacity
The total antioxidant capacity (TAC) was detected spectrophotometrically at 593 nm. 100 μg of homogenized tissue from the TAA of BH patients and CS were incubated in the presence of a mixture that contained C2H3O2 at 300 mM, FeCl3·6H2O at 20 mM, 2,4,6-tris-2pyridyl-s-triazine at 10 mM, HCL at 40 mM, at pH 3.6 (1.5 mL, at ratio of 10:1:1 v/v,). The samples were incubated at 37 °C for 15 min and the absorbance was measured [6].
4.4.3. Carbonylation
To evaluate the carbonyl groups, 100 μg of homogenized tissue from the TAA of BH patients and CS was mixed with HCL 2.5 M (500 μL) and in parallel, another sample was mixed with 2,4-dinitrophenylhydrazine (500 μL) and incubated in the dark at room temperature for one hour. At the end of the incubation, C2HCL3O2 at 20% was added (500 μL) and the samples were centrifuged at 15,000× g for 5 min. The bottom was recuperated, and it was washed two time, adding C2H5OH/C4H8O2 (1 mL). Then, the samples were incubated for 10 min and centrifuged at 15,000× g for 10 min. Finally, CH6CLN3 at 6 M in KH2PO4 at 20 mM and pH 2.3 (1 mL) was added and the mixture was incubated at 37 °C for 30 min. The absorbance was read spectrophotometrically at 370 nm [6].
4.4.4. GSH and Thiols
For the determination of GSH 100 μg of homogenized tissue from the TAA were used and GSH was detected spectrophotometrically at 412 nm, according to the Ellman’s method. Thiol groups were read spectrophotometrically at 415 nm. 50 µg of homogenized tissue form the cardiac valve BH patients and CS were used according to Erel and Neselioglu’s method [7].
4.4.5. NO3−/NO2− Ratio Determination
To evaluate the NO3−/NO2− ratio, 100 μg of homogenized tissue from the TAA of BH patients and CS previously deproteinized with 0.5 N, NaOH and 10%, ZnSO4 (100 μL) were used. Then, 10 μL of the cytochrome c reductase (NADPH) (Sigma Aldrich Cat# 24479) were added and the samples were incubated for 30 min at 37 °C. Sulfanilamide 1% and N-naphthyl-ethyldiamine 0.1% (200 µL respectively) were added and the total volume was adjusted with distilled water to 1 mL. The absorbance was measured at 540 [7].
4.4.6. Determinations of Antioxidant Enzymes that Employ GSH as a Substrate
To evaluate the activities of GST, GPx, GR and TrxR, 100 μg of homogenized tissue from the TAA of BH patients and CS, were used and treated as previously described [10]. The GR activity was expressed as μmol of reduced GSSG/min/mg of protein, with an extinction coefficient of 6220 M−1 cm−1. The GST activity was expressed as units of GS-TNB mol/min/mg of protein, with an extinction coefficient of 14,150 M−1 cm−1. The GPx activity was expressed as nmol of NADPH oxidized/min/mg of protein, with an extinction coefficient of 6220 M−1 cm−1 at 340 nm for NADPH. The samples were incubated and monitored at 340 nm for 6 min at 37 °C. The activity TrxR was determined after incubation and monitoring at 412 nm for 6 min at 37 °C. The TrxR activity was expressed as TNB nmol/min/mL of the serum, with an extinction coefficient of 13,600 M−1 cm−1 [8].
4.4.7. Determinations of Super Oxide Dismutase Isoforms, Catalase and Peroxidases Activities
The super oxide dismutase (SOD) isoforms, catalase and peroxidase activities were determined through non-denaturing gel electrophoresis [10]. 100 µg of homogenized tissue from the TAA of BH patients and CS were applied directly in non-denaturing 10% polyacrylamide gels. The electrophoresis was carried out at 120 volts for 4 h. For SOD isoforms activity, the gel was incubated with nitro blue tetrazolium at 2.45 mM for 20 min, then incubated with buffer of the KH2PO4 at 36 mM, EDTA at 28 mM, and riboflavin at 28 mM pH 7.8 (20 mL) and exposed for 10 min to UV light. For catalase activity the gel was incubated with a mixture of 1% K3Fe (CN)6 and 1% of FeCl3 6H2O for 10 min in the dark and then washed with distilled water to stop the reaction [12]. Purified SOD from bovine erythrocytes with a specific activity of 112 U/mg of protein (Sigma-Aldrich, St. Louis, MO, USA) and purified CAT from a bovine liver having a specific activity of 60 U/mg (Sigma-Aldrich) were used as positive control for calculating the activity of these enzymes. For the peroxidase activity, the gel was washed with distilled water three times, for 5 min, after being incubated with 3 mg/mL 3,3,5,5-tetramethylbenzidine dissolved in CH3-OH/CH3COOH/H2O (1:1:1 v/v) with H2O2 (300 μL) total volume 20 mL, for 10 min. A quantity of 35 μL of horseradish peroxidase was loaded to a final concentration of 178.5 μg as a standard. The activities in the SOD isoforms, catalase and peroxidase gels were analyzed using densitometry with a Kodak Image® 3.5 system. The samples were placed in a separate lane of the gel and run in parallel with the biological samples. The intensity of the signal from the controls was used as a reference to measure the enzymatic activity in the tissue samples. Therefore, the results are expressed as U of activity per mg of protein. The gels were analyzed by densitometry with image Sigma Scan Pro 5.1 software (Systat Software, Inc., San Jose, CA, USA).
4.5. Statistical Analysis
Continuous variables are expressed as median with minimum and maximum values. Categorical variables, such as frequencies and percentages, are reported. The results were normalized with natural logarithm and normality distribution was evaluated using the Shapiro-Wilk test, and Mann–Whitney according to the Gaussian distribution, were performed to detect significant independent variables The graphical results are shown as the median, first quartile, third quartile, and half dotted line. Sigma Plot® version 15 (Systat Software Inc., SanJose, CA 95131, USA, EE. 191 UU, North First Street, Suite 360, Jandel Corporation, San Jose, CA, USA) was used to generate the analysis and graphs. Differences were considered statistically significant when p ≤ 0.05.
5. Conclusions
The results of this preliminary study in this series of three patients with BH suggest a possible loss of redox homeostasis that may contribute to the alteration and instability of the FBN-2 protein, mainly due to the decrease in TrxR activity and the concentration of thiol groups.
Study Limitations
Collecting samples from BH syndrome patients, being a rare pathology where the prevalence is less than 1 in 10,000 cases, may seem a first limitation due to the low number of cases available for their study. However, this is really not so, because some of the results are clear as preliminary findings. Although several results did not reach a statistically significant difference, the trends are biologically relevant and important given the small "n" of cases. Furthermore, the low number of cases in this study indicates that the participation of OS is a mechanism that deserves attention for possible therapeutic targets. Therefore, since there exist no studies on this condition, and none have focused on elucidating the participation of OS or the presence of a state of the deregulation homeostasis redox this topic requires attention to further consider the adjuvant management of patients with antioxidant therapy in possible clinical trials. On the other hand, the control subjects that were selected for comparison with BH patients were intervened for aortic valve replacement and they underwent the same procedures as the subjects with BH. Although they are not healthy subjects, they might present alterations in redox homeostasis. However, the point of comparison lies in the presence and absence of BH.
Author Contributions
Conceptualization, I.P.-T., M.E-S.; methodology, L.M.-P.; writing—original draft preparation, I.P.-T., M.E-S.; V.G.-L.; writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
no applicable
Institutional Review Board Statement
The research protocol was approved by the research and ethics committee of the National Institute of Cardiology “Ignacio Chávez” (protocol number 23-1366).
Informed Consent Statement
Each BH patient signed an informed consent form in accordance with the Helsinki Declaration, as amended by the Congress of Tokyo. Informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request and available from the I.P.-T. and M.S.
Acknowledgments
Payment of open access publication was financed by Instituto Nacional de Cardiología Ignacio Chávez.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Abbreviations
| BH | Beals-Hecht |
| BMP | bone morphogenetic protein |
| cbEGF | epidermal growth factor |
| CCA | contractural arachnodactyly |
| CS | controls subjects |
| ECM | extracellular matrix |
| EF | elastic fibers |
| FBN-2 | fibrillin-2 |
| fibulin | Fbln |
| GPx | glutathione peroxidase |
| GR | glutathione reductase |
| GSH | glutathione |
| GST | glutathione-S-Transferase |
| H2O2 | hydrogen peroxide |
| LPO | Lipid peroxidation |
| MDA | malondialdehyde |
| MFS | Marfan syndrome |
| NO3−/NO2− | nitrate/nitrite ratio |
| O2– | super oxide anion |
| OH– | hydroxyl groups |
| ONOO– | peroxinitrite |
| OS | oxidative stress |
| ROS | reactive oxygen species |
| SOD | super oxide dismutase’s |
| TAA | thoracic aortic aneurysm |
| TAC | total antioxidant capacity |
| TE | tropo-elastin |
| TGFβ | transforming growth factor |
| Trx | thioredoxin |
| TrxR | Thioredoxin reductase |
References
- Li, A.L.; He, J.Q.; Zeng, L.; Hu, Y.Q.; Wang, M.; Long, J.Y.; Chang, S.H.; Jin, J.Y.; Xiang, R. Case report: Identification of novel <i>fibrillin-2</i> variants impacting disulfide bond and causing congenital contractural arachnodactyly. Front. Genet. 2023, 14, 1035887.
- Zhang, C.; Qiao, F.; Cheng, Q.; Luo, C.; Zhang, Q.; Hu, P.; Xu, Z. A Novel splice site mutation in the FBN2 Gene in a Chinese family with congenital contractural arachnodactyly. Biochem. Genet. 2024, 62, 2495–2503.
- Smaldone, S.; Ramirez, F. Fibrillin microfibrils in bone physiology. Matrix. Biol. 2016, 52-54, 191–197.
- Zodanu, G.K.E.; Hwang, J.H.; Mehta, Z.; Sisniega, C.; Barsegian, A.; Kang, X.; Biniwale, R.; Si, M.S.; Satou, G.M.; Halnon, N.; Grody, W.W.; Van Arsdell, G.S.; Nelson, S.F.; Touma, M. High-throughput genomics identify novel FBN1/2 variants in severe neonatal Marfan syndrome and congenital heart defects. Int. J. Mol. Sci. 2024, 25, 5469.
- Yang, S.; Li, Z. FBN2 pathogenic variants in congenital contractural arachnodactyly with severe cardiovascular manifestations. Connect. Tissue. Res. 2024, 65, 214–225.
- Zúñiga-Muñoz, A.M.; Pérez-Torres, I.; Guarner-Lans, V.; Núñez-Garrido, E.; Velázquez Espejel, R.; Huesca-Gómez, C.; Gamboa-Ávila, R; Soto, M.E. Glutathione system participation in thoracic aneurysms from patients with Marfan syndrome. Vasa. 2017, 46, 177–186.
- Pérez-Torres, I.; Soto, M.E.; Manzano-Pech, L.; Díaz-Diaz, E.; Soria-Castro, E.; Rubio-Ruíz, M.E.; Guarner-Lans, V. Oxidative stress in plasma from patients with Marfan syndrome is modulated by deodorized garlic preliminary findings. Oxid. Med. Cell. Longev. 2022, 2022, 5492127.
- Soto, M.E.; Pérez-Torres, I.; Manzano-Pech, L.; Soria-Castro, E.; Morales-Marín, A.; E.S.; Martínez-Hernández, H.; Herrera-Alarcón, V.; Guarner-Lans, V. Reduced levels of selenium and thioredoxin reductase in the thoracic aorta could contribute to aneurysm formation in patients with Marfan syndrome. Int. J. Mol. Sci. 2023, 24, 10429.
- Meerschaut, I.; De Coninck, S.; Steyaert, W.; Barnicoat, A.; Bayat, A.; Benedicenti, F.; Berland, S.; Blair, E.M.; Breckpot, J.; de Burca, A.; Destrée, A.; García-Miñaúr, S.; Green, A.J.; Hanna, B.C.; Keymolen, K.; Koopmans, M.; Lederer, D.; Lees, M.; Longman, C.; Lynch, S.A.; Male, A.M.; McKenzie, F.; Migeotte, I.; Mihci, E.; Nur, B.; Petit, F.; Piard, J.; Plasschaert, F.S.; Rauch, A.; Ribaï, P.; Pacheco, I.S.; Stanzial, F.; Stolte-Dijkstra, I.; Valenzuela, I.; Varghese, V.; Vasudevan, P.C.; Wakeling, E.; Wallgren-Pettersson, C.; Coucke, P.; De Paepe, A.; De Wolf, D.; Symoens, S.; Callewaert, B. A clinical scoring system for congenital contractural arachnodactyly. Genet. Med. 2020, 22, 124–131.
- Soto, M.E.; Soria-Castro, E.; Lans, V.G.; Ontiveros, E.M.; Mejía, B.I.; Hernandez, H.J.; García, R.B.; Herrera, V.; Pérez-Torres, I. Analysis of oxidative stress enzymes and structural and functional proteins on human aortic tissue from different aortopathies. Oxid. Med. Cell. Longev. 2014, 2014, 760694.
- Soto, M.E.; Manzano-Pech, L.G.; Guarner-Lans, V.; Díaz-Galindo, J.A.; Vásquez, X.; Castrejón-Tellez, V.; Gamboa, R.; Huesca, C.; Fuentevilla-Alvárez, G.; Pérez-Torres, I.; Oxidant/antioxidant profile in the thoracic aneurysm of patients with the Loeys-Dietz syndrome. Oxid. Med. Cell. Longev. 2020, 2020, 5392454.
- Pérez-Torres, I.; Roque, P.; El-Hafidi, M.; Diaz-Diaz, E.; Baños, G. Association of renal damage and oxidative stress in a rat model of metabolic syndrome. Influence of gender. Free. Rad. Res. 2009, 43, 761–771.
- Gupta, P.A.; Putnam, E.A.; Carmical, S.G.; Kaitila, I.; Steinmann, B.; Child, A.; Danesino, C.; Metcalfe, K.; Berry, S.A.; Chen, E.; Delorme, C.V.; Thong, M.K.; Ades. L.C.; Milewicz, D.M. Ten novel FBN2 mutations in congenital contractural arachnodactyly: delineation of the molecular pathogenesis and clinical phenotype. Hum. Mutat. 2002, 19, 39–48.
- Phokaew, C.; Sittiwangkul, R.; Suphapeetiporn, K.; Shotelersuk, V. Double heterozygous variants in FBN1 and FBN2 in a Thai woman with Marfan and Beals syndromes. Eur. J. Med. Genet. 2020, 63, 103982.
- Rueda-Martínez, C.; Lamas, O.; Mataró, M.J.; Robledo-Carmona, J.; Sánchez-Espín, G.; Moreno-Santos, I.; Carrasco-Chinchilla, F.; Gallego, P.; Such-Martínez, M.; de Teresa, E.; Jiménez-Navarro, M.; Fernández, B. Fibrillin 2 is upregulated in the ascending aorta of patients with bicuspid aortic valve. Eur. J. Cardiothorac. Surg. 2017, 51, 104-111.
- Bell, R.E.; Wheller, J.J. Cardiac defects in a patient with congenital contractural arachnodactyly. South. Med. J. 1985, 78, 742–743.
- Takeda, N, Morita H, Fujita D, Inuzuka R, Taniguchi Y, Imai Y, Hirata Y, Komuro I. Congenital contractural arachnodactyly complicated with aortic dilatation and dissection: Case report and review of literature. Am. J. Med. Genet. A. 2015, 167A, 2382–2387.
- Xu, P.; Li, R.; Huang, S.; Sun, M.; Liu, J.; Niu, Y.; Zou, Y.; Li, J.; Gao, M.; Li, X.; Xuan, Gao.; Yuan, Gao. A novel splicing mutation in the FBN2 gene in a family with congenital contractural arachnodactyly. Front. Genet. 2020, 11, 143.
- Deslee, G. Woods, J.C. Moore, C.M. Liu, L. Conradi, S.H. Milne, M. Gierada, D.S. Pierce, J. Patterson, A.; Lewit, R.A.; Battaile, J.T.; Holtzman, M.J.; Hogg, J.C.; Pierce, R.A. Elastin expression in very severe human COPD. Eur. Respir. J. 2009, 34, 324–331.
- Ramirez, F.; Sakai, L.Y. Biogenesis and function of fibrillin assemblies. Cell. Tissue. Res. 2010, 339, 71–82.
- Reinhardt, D.P.; Gambee, J.E.; Ono, R.N.; Bachinger, H.P.; Sakai, L.Y. Initial steps in assembly of microfibrils. Formation of disulfide-cross-linked multimers containing fibrillin-1. J. Biol. Chem. 2000, 275, 2205–2210.
- Downing, A.K.; Knott, V.; Werner, J.M.; Cardy, C.M.; Campbell, I.D.; Handford, P.A. Solution structure of a pair of calcium-binding epidermal growth factor-like domains: implications for the Marfan syndrome and other genetic disorders. Cell. 1996, 85, 597–605.
- Chupakhin, E.; Krasavin, M. Thioredoxin reductase inhibitors: Updated patent review (2017–present). Expert. Opin. Ther. Pat. 2021, 31, 745–775.
- Lu, J.; Holmgren, A. The thioredoxin antioxidant system. Free. Radic. Biol. Med. 2014, 66, 75–87.
- Kirsch, J.; Schneider, H.; Pagel, J.I.; Rehberg, M.; Singer, M.; Hellfritsch, J.; Chillo, O.; Schubert, K.M.; Qiu, J.; Pogoda, k., Kameritsch, P.; Uhl, B.; Pircher, J.; Deindl, E.; Müller, S.; Kirchner, T.; Pohl, U.; Conrad, M.; Beck. H.; Endothelial dysfunction, and a prothrombotic, proinflammatory phenotype is caused by loss of mitochondrial thioredoxin reductase in endothelium. Arterioscler. Throm. Vasc. Biol. 2016, 36, 1891–1899.
- Sakai, L.Y.; Keene, D.R.; Engvall, E. Fibrillin, a new 350-kD glycoprotein, is a component of extracellular microfibrils. J. Cell. Biol. 1986, 103, 2499–2509.
- Talot, T.; Conconi, M. T.; Di Liddo, R. Structural and functional failure of fibrillin-1 in human diseases (review). Int. J. Mol. Med. 2018, 41, 1213–1223.
- Lubos, E.; Loscalzo, J.; Handy, D.E. Glutathione peroxidase-1 in health and disease: from molecular mechanisms to therapeutic opportunities. Ant. Red. Sig. 2011, 15, 1957–1997.
- Soto, M.E.; Iturriaga-Hernández, A.V.; Guarner-Lans, V.; Zuñiga-Muñoz A.; Aranda-Fraustro A.; Velázquez-Espejel R.; Pérez-Torres, I. Participation of oleic acid in the formation of the aortic aneurysm in Marfan syndrome patients. Prost. Other. Lipid. Mediat. 2016, 123, 46–55.
- Bellinger, F.P.; Raman, A.V.; Reeves, M.A.; Berry, M.J. Regulation and function of selenoproteins in human disease. Biochem. J. 2009, 422, 11–22.
- Degendorfer, G.; Chuang, C.Y.; Mariotti, M.; Hammer, A.; Hoefler, G.; Hägglund, P.; Malle, E.; Wise, S.G.; Davies, M.J. Exposure of tropoelastin to peroxynitrous acid gives high yields of nitrated tyrosine residues, di-tyrosine cross-links and altered protein structure and function. Free. Radic. Biol. Med. 2018, 15, 219–231.
- Akhtar, K.; Broekelmann, T.J.; Miao, M.; Keeley, F.W.; Starcher, B.C.; Pierce, R.A.; Mecham, R.P.; Adair-Kirk, T.L. Oxidative and nitrosative modifications of tropoelastin prevent elastic fiber assembly in vitro. J. Biol. Chem. 2010, 285, 37396–37404.
- Lu, S.C. Regulation of glutathione synthesis. Mol. Aspects. Med. 2009, 30, 42–59.
- Deponte, M. Glutathione catalysis and the reaction mechanisms of glutathione-dependent enzymes. Biochim. Biophys. Acta. 2013, 1830, 3217–3266.
- Meister A. Glutathione metabolism and its selective modification. J. Biol. Chem. 1988, 263, 17205–17208.
- Enns, GM, Moore T, Le A, et al. Degree of glutathione deficiency and redox imbalance depend on subtype of mitochondrial disease and clinical status. PLoS. One. 2014, 9, e100001.
- Ndebele, P. The declaration of Helsinki, 50 years later. JAMA. 2013, 310, 2145–2146.
- Bentall, H.; De Bono, A. A technique for complete replacement of the ascending aorta. Thorax. 1968, 23, 338–339.
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254.
Figure 1.
Oxidative stress markers including NO3–/NO2– ratio (A), TAC (B), LPO levels (C), Carbonylation (D), GSH (E) and thiols groups (F) in homogenized tissue from the TAA of the BH syndrome patients and CS. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, BH= Beals-Hecht, LPO= Lipid peroxidation, TAC= Total antioxidant capacity, GSH= Glutathione and NO3–/NO2– = nitrate and nitrite.
Figure 1.
Oxidative stress markers including NO3–/NO2– ratio (A), TAC (B), LPO levels (C), Carbonylation (D), GSH (E) and thiols groups (F) in homogenized tissue from the TAA of the BH syndrome patients and CS. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, BH= Beals-Hecht, LPO= Lipid peroxidation, TAC= Total antioxidant capacity, GSH= Glutathione and NO3–/NO2– = nitrate and nitrite.
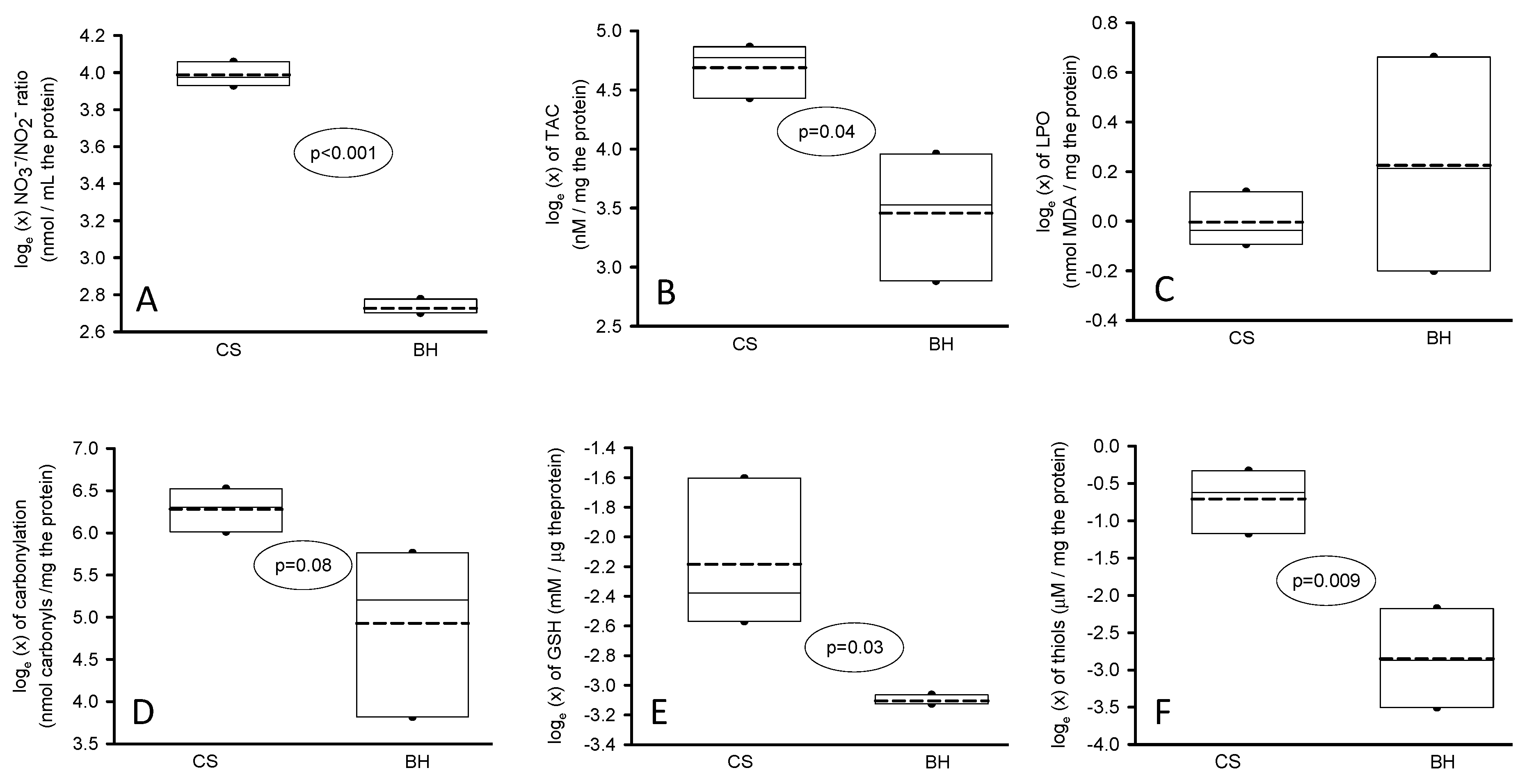
Figure 2.
Determinations of some antioxidant enzymes that utilize GSH as substrate including GR (A), GPx (B), GST (C) and TrxR (D) in homogenized tissue from the TAA of the BH syndrome patients and CS. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, BH= Beals-Hecht, GR= glutathione reductase, GPx= glutathione peroxidase, GST= glutathione-S-Transferase, TrxT= Thioredoxin reductase.
Figure 2.
Determinations of some antioxidant enzymes that utilize GSH as substrate including GR (A), GPx (B), GST (C) and TrxR (D) in homogenized tissue from the TAA of the BH syndrome patients and CS. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, BH= Beals-Hecht, GR= glutathione reductase, GPx= glutathione peroxidase, GST= glutathione-S-Transferase, TrxT= Thioredoxin reductase.
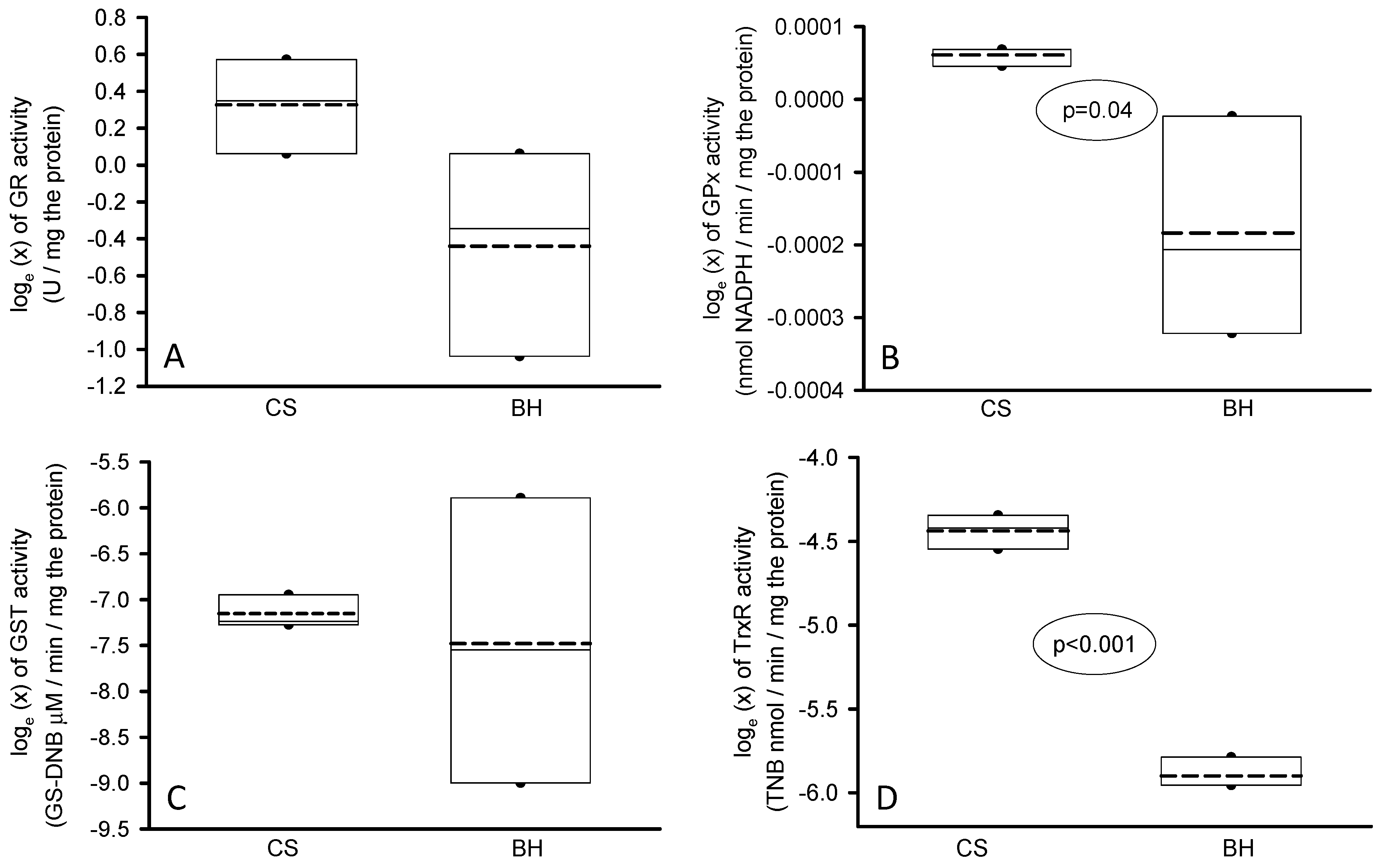
Figure 3.
SOD-1 (A) and SOD-2 (B) isoform activities in homogenized tissue from the TAA. The values are expressed as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, BH= Beals-Hecht, SOD= super oxide dismutase’s.
Figure 3.
SOD-1 (A) and SOD-2 (B) isoform activities in homogenized tissue from the TAA. The values are expressed as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, BH= Beals-Hecht, SOD= super oxide dismutase’s.
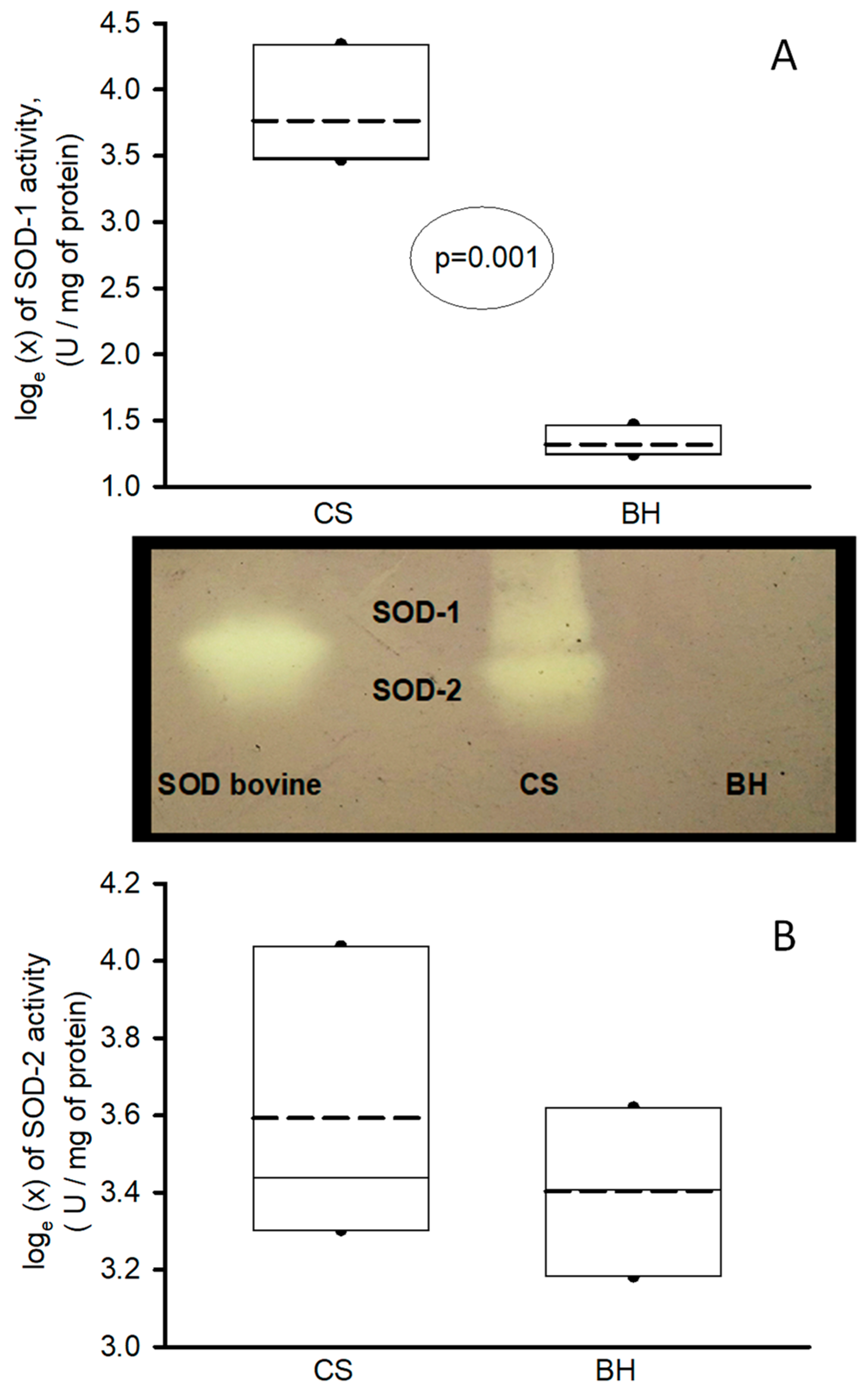
Figure 4.
Peroxidases (A) and catalase (B) activities in homogenized of the TAA. The values are expressed as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, BH= Beals-Hecht.
Figure 4.
Peroxidases (A) and catalase (B) activities in homogenized of the TAA. The values are expressed as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, BH= Beals-Hecht.
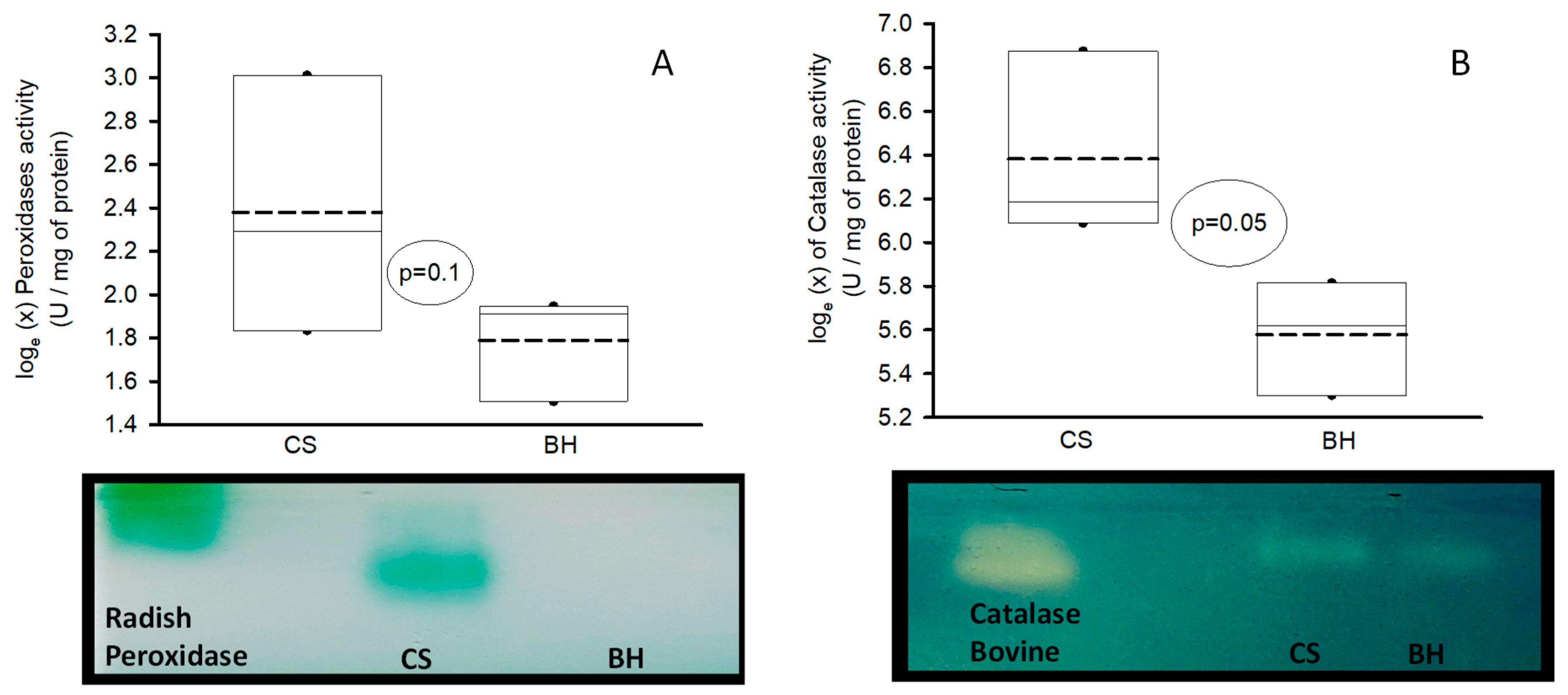

Table 1.
shows positive characteristics of the Ghent criteria in the patients with BH Syndrome.
| Case 1 | Case 2 | Case 3 | |
| Age at the time of diagnosis | 29 | 53 | 25 |
| Age (current post surgery and intervention) | 30 | 66 | 36 |
| Gender | Man | Man | Man |
| Ghent criteria > 2 is required for classification | |||
| 1) MFS family history | No | No | No |
| Aortic root dilation (mm) | 41 | 31 | 19 |
| Sinus of Valsalva dilation (mm) | 91 | 52 | 27 |
| Sino tubular junction dilation (mm) | 90 | 38 | 24.7 |
| Ascending aorta dilation (mm) | 46 | 37 | 28 |
| Abdominal Aorta | Without dilation | 33 | 36 |
| 2) Aortic dilatation | yes | yes | yes |
| 3) Lens dislocation | No | No | No |
| Systemic score | |||
| Facials | 1 | 1 | 1 |
| Steinberg and Walker Murdock sign | 0 | 0 | 3 |
| Pectus carinatum | 0 | 2 | 0 |
| Pectus excavatum or asymmetry of the thorax | 1 | 0 | 0 |
| Hollow foot | 0 | 0 | 0 |
| Normal or flat foot | 1 | 0 | 0 |
| Pneumothorax | 0 | 0 | 0 |
| Dural ectasia | 0 | 2 | 0 |
| Acetabular protrusion | 0 | 0 | 0 |
| US/UL Reduction or stroke/height ratio | 1 | 0 | 0 |
| Mild scoliosis | 0 | 0 | 0 |
| Thoracolumbar scoliosis or kyphosis | 1 | 1 | 0 |
| Reduction of elbow extension | 0 | 0 | 0 |
| Skin with stretch marks | 1 | 0 | 0 |
| Myopia> 3 diopters | 0 | 0 | 0 |
| Mitral valve prolapses | 0 | 0 | 0 |
| Total systemic score | 5 | 6 | 4 |
| 4) Positive systemic score (> 7) | No | No | No |
| 5) Positive genetic test for FBN-1 | No | No | No |
| 1 = 2, aortic dilatation | 2 = 2, aortic dilatation | 2 = aortic dilatation and in his mother | |
| Clinical suspicion of the BH syndrome by score system | |||
| Appearance of ear helix | Wrinkled (3) | Wrinkled (3) | Elf (3) |
| Highly arched palate | Yes (1) | Yes (1) | Yes (1) |
| Retrognathia | Yes (1) | Yes (1) | Yes (1) |
| Joint contractures | Hands and feet (3) | Hands and feet (3) | Hands and feet (3) |
| Arachnodactyly | no | no | Yes (3) |
| dolichostenomelia | Yes (2) | Yes (2) | no |
| Pectus deformity | Yes (2) | no | no |
| Kyphoscoliosis | Yes (1) | Yes (1) | no |
| Mutation FBN-2 | No done | No done | Positive |
| Total score system | 13 | 11 | 11+ mutation |
| Clinical Scoring System: In the absence of a pathogenic or likely pathogenic FBN-2 variant and in the absence of intellectual disability, progressive aortic root dilatation, and/or ectopia Lentis, a clinical score of ≥ 7/20 is suggestive for CCA (sensitivity 95.5%; specificity 17.1%) and a score of ≥11/20 makes the CCA diagnosis likely (sensitivity 75%; specificity 60% [9]. | |||
Table 2.
Description of the clinical and symptomatic characteristics of the patients with BH and CS.
Table 2.
Description of the clinical and symptomatic characteristics of the patients with BH and CS.
| BH case | Sex | Age | Description |
| 1 | Man | 30 | House painter by occupation. At the age of 28 he began to have dyspnea and chest tightness. He was evaluated by a cardiologist for recurrent oppressive chest pain, and was sent for evaluation to our center. On admission, at 29 years, he reported chest tightness. The echocardiographic study showed that he had aortic insufficiency, dilated left cavities, and decreased systolic function. The computed tomography also found severe destroxone convex scoliosis, aneurysm in the aortic root and ascending aorta. At the age of 30, he underwent Bentall and De Bono surgery. He was evaluated for suspected MFS; the only positive Ghent criterion was aortic dilation. He is currently alive, with 9 years of evolution. LVEF of 58%. |
| 2 | Man | 66 | A farmer, who began to have dyspnea when he was 53 years old and sought medical attention 6 years later. He was found to have a marfanoid habitus, aortic insufficiency attributed to aortic dilatation. A CT scan showed dilatation of the aortic root in the sinuses of Valsalva of 52 mm and an abdominal aortic aneurysm of 33 mm. He only met one of the Ghent criteria (aortic dilatation) and only met 6 of the systemic score. He had no other antecedents. His clinical characteristics showed a deep high-arched epicanthus palate, wrinkled ears, severe scoliosis and pectus carinatum. He underwent surgery using the Bentall and De bono technique. He is currently 66 years old and is stable. LVEF 62%. |
| 3 | A financial stockbroker who practices at Parco. At the age of 25, on a trip to Israel, he presented acute abdominal pain that radiated to the pelvic cavity. A CT scan showed an abdominal aneurysm, so he was treated with an endoprosthesis. He was evaluated for suspected MFS. The only relevant history was the death of his mother due to aortic rupture, but she died without a diagnosis. The patient only met one Ghent criterion (aortic dilatation) and was positive for mutation in the FBN-2 gene. The patient's clinical data included epicanthus, elf ears, CCA in the hands and feet, and a diagnosis of BH syndrome was concluded. Six years later, he presented a right femoral iliac dissection that was treated with an endoprosthesis. It was complicated by compartment syndrome treated with fasciotomy and finally had to be resolved with supracondylar amputation. Currently, his evolution is stable. LVEF 64% without aortic dilatation in the thorax. | ||
| CS | Sex | Age | Description |
| 1 | Man | 72 | Foreign farmer with no significant degenerative or cardiovascular history in 2014. At the age of 72 years, he began to have intense dominant pain, with straining and tenesmus. An ultrasound was performed in a private hospital, which showed an abdominal aneurysm. He was referred to our Institute and a CT scan was performed, which showed a ruptured infrarenal abdominal aneurysm with hemoperitoneum (Crawford-IV). Emergency surgery was performed. An 18 x 30 mm aortic graft was placed. The patient is alive and has a postoperative evolution of 10 years and two months. |
| 2 | Man | 52 | Foreign farmer with a history of arterial hypertension of 10 years of evolution dyslipidemia, alcoholism and positive smoking. His condition began at the age of 52. In 2015, after his work- day, he had intense precordial pain 7/10. In his place of origin, they performed a computed tomography that showed aortic dilatation and dissection. He was sent to our Institute and the MRI showed aortic dissection Stanford IIIB De DeBakey. Aortic dilatation of the descending thoracic abdominal aorta of 75 mm. The left ventricle showed concentric hypertrophy. Surgery was performed with aortic-thoracic abdominal replacement with revascularization of abdominal trunks. He died 24 hours later with refractory metabolic acidosis and acute kidney injury III. |
| 3 | Woman | 48 | Woman in housework occupation. In 2011 at the age of 40 she had dyspnea and was studied by a cardiologist who diagnosed her with significant aortic insufficiency and proposed aortic valve replacement. However, the patient postponed the surgery proposal. In 2016 the dyspnea had increased, she was found to have severe aortic insufficiency and a computed tomography found a bivalve aorta, dilation of the ascending aorta. Bentall and Bono surgery were performed. Current surgical survival is 8 years 4 months. |
Table 3.
Demographic characteristics of patients with BH and CS.
|
BH (n=3, median and min -max range) |
CS (n=3, median and min -max range) |
|
| Age (years) | 38 (30–66) | 52 (48–72) |
| BMI (weight/height2) | 25 (19–27) | 31 (30–34) |
| Comorbidities (%) | ||
| DM | 0 (0) | 1 (33.3) |
| SAH | 0 (0) | 2 (66.0) |
| Dyslipidemia | 0 (0) | 1 (33.3) |
| Smoking | 0 (0) | 1 (33.3) |
| Alcoholism | 0 (0) | 1 (33.3) |
| Serum biochemicals | ||
| Leukocytes (103/µL) | 6 (4.7–6.8) | 6.8 (0.9–9.0) |
| Lymphocytes (103/µL) | 1.9 (1.9–2) | 1.9 (1.6–2.2) |
| Neutrophils (103/µL) | 3.3 (2.2–4) | 5.9 (4.4–7.1) |
| Platelets (103/µL) | 194 (191–316) | 268 (158–307) |
| Hemoglobin (g/dL) | 15.9 (15.7–16.1)* | 11.4 (10.1–13.2) |
| Glucose (mg/dL) | 91 (90–100)* | 107 (80–264) |
| Creatinine (mg/dL) | 0.80 (0.75–0.88)* | 0.83 (0.70–1.5) |
| BUN (mg/dL) | 15.6 (11-4–20.6) | 17.3 (10.3–21.7) |
| Uric acid (mg/dL) | 6.4 (5.8–6.6) | 8.1 (6.2–8.4) |
| Albumin (mg/dL) | 4.3 (4–4.7)* | 3.6 (2.4–3.6) |
| CT (mg/dL) | 181 (167–188) | 124 (98–146) |
| LDL (mg/dL) | 120 (114–120) | 81 (54–95) |
| HDL (mg/dL) | 41 (34–49) | 29 (16–34) |
| TG (mg/dL) | 104 (92–218) | 92 (80–127) |
| CRP (mg/dL) | 0.58 (0.30–0.75)* | 81 (6.5–143) |
| General characteristics of the aorta (mm) | ||
| Aortic ring | 31 (21–41) | 25 (24–30) |
| Valsalva sinuses | 52 (28–91)* | 46 (30–48) |
| Sino tubular junction | 38 (27–90)* | 38 (28–56) |
| Ascending aorta | 37 (29–46) | 30 (30–82) |
| Descending aorta | 33 (21–33)* | 50 (26–54) |
| Mitral Regurgitation (%) | 50 (30–60) | 54 (52–55) |
| The values are expressed in median and minimum-maximum range. Abbreviations: BUN= Blood urea nitrogen, CT= Cholesterol total, CRP= C-reactive protein, LDL= Low density lipoprotein, HDL= High density lipoprotein, TG= Triglycerides, DM= Diabetes mellitus, SAH= Systemic arterial hypertension, TG= Triglycerides, BUN= Blood urea nitrogen BMI= Body Mass Index (weight/height2), p=0.01. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



