
Submitted:
20 January 2025
Posted:
20 January 2025
You are already at the latest version
Abstract
Objectives: To investigate recent research trends in biologics and small molecules for the treatment of inflammatory bowel disease (IBD), a bibliometric analysis was conducted on literature from the past decade. Methods: This cross-sectional study involved a bibliometric analysis of data retrieved from the Web of Science Core Collection (WoSCC) database to examine the evolution and thematic trends on biological agents and small molecular drugs for IBD conducted between January 1, 2014, and September 20, 2024. A total of 6,337 articles were analyzed for specific attributes, including publication year, journal, country/region, institution, author, references, and keywords. VOSviewer software was utilized to perform co-authorship, co-occurrence, co-citation, and network visualization analyses, and further discussions were conducted on significant sub-themes.Results: From 2014 to September 20, 2024, the annual number of global publications increased by 23%, from 442 to 544. The journal "Inflammatory Bowel Diseases" published the highest number of manuscripts (579 publications) and garnered the most citations (13,632 citations), followed by the "Journal of Crohn's & Colitis" (480 publications) and "Alimentary Pharmacology & Therapeutics" (250 publications). The United States emerged as the leading country in terms of productivity (1,943 publications, 66,320 citations), with the University of California, San Diego (291 publications, 23,017 citations) and the author Sandborn, Vermeire, Severine (180 publications, 10,383 citations) being the most prolific institution and author, respectively. The co-occurrence cluster analysis of the top 100 keywords resulted in the formation of six distinct clusters: (1) Disease, (2) Drug, (3) Surgery, (4) Therapeutic Drug Monitoring, (5) Mechanism Research, and (6) Others. Recent keywords such as biologics, vedolizumab, ustekinumab, tofacitinib, Janus kinase inhibitor, therapeutic drug monitoring, trough level, and pharmacodynamics highlight the emerging frontiers in IBD research. We have synthesized information on biologics and small molecules approved by the European Medicines Agency (EMA), the Food and Drug Administration (FDA), and regulatory bodies in China, focusing on therapeutic targets and the immunological mechanisms underlying these diseases. Further discussions are provided to aid researchers in identifying potential research subjects and directions. Conclusions: This study elucidates current trends, patterns of global collaboration, foundational knowledge, research hotspots, and emerging frontiers in the field of biologics and small molecules for IBD treatment. Current research hotspots include the management of therapeutic drug monitoring (TDM) and safety, as well as investigations into monotherapy or switch therapy.
Keywords:
inflammatory bowel disease
; biological product
; small molecules
; bibliometric study
1. Introduction
Inflammatory bowel disease (IBD) is a chronic inflammatory disorder of the gastrointestinal tract, distinct from typical acute gastroenteritis, and primarily encompasses ulcerative colitis (UC), Crohn’s disease (CD), and indeterminate colitis [1]. Ulcerative colitis is characterized by diffuse and continuous inflammation restricted to the colon, whereas Crohn’s disease can present with segmental lesions affecting any part of the gastrointestinal tract, from the oral cavity to the perianal area [2]. The principal aim in the management of IBD is to alleviate symptoms and mitigate inflammation, thereby decelerating disease progression and preventing complications.
Therapeutic strategies include both pharmacological and surgical interventions [3]. Currently approved pharmacotherapies comprise traditional agents such as mesalazine (a 5-aminosalicylic acid derivative), corticosteroids, and immunosuppressants like azathioprine; biologics, including anti-tumor necrosis factor-alpha agents, anti-interleukin IL12/23 inhibitors, and anti-integrin α4β7 monoclonal antibodies; as well as small molecule drugs such as Janus kinase inhibitors and S1P receptor modulators [4,5,6,7]. Up to 20% of patients with UC require a total colectomy, while 50% of those with CD undergo surgical intervention within ten years of diagnosis [8]. Presently, the surgical risk for individuals with IBD has decreased, likely due to the continuous improvement of pharmacological regimens, including biologics, as well as advancements in endoscopic imaging technology [9,10]. Figure 1 illustrates the approval timelines for various biologics and small molecules used in the treatment of IBD over recent years. Several biologics and small molecules with innovative mechanisms have transformed the management of UC and CD. Despite the approval of numerous new drugs, the indications and timing of approval differ. Typically, these drugs receive initial approval in the United States and the European Union, where there is the most experience, while China and other developing countries lag behind.
Bibliometric analysis can provide insights into the scope of a specific field, track emerging trends, and identify gaps by analyzing journals, articles, authors, and topics within the field [11]. The VOSviewer software can create a visual map depicting the co-occurrence of authors, research institutions, and keywords based on network data [12].
Despite the existence of numerous reviews on IBD with varying focuses [1], a comprehensive and visualized analysis of the evolution and trends in biologics and small molecules remains lacking. To address this gap, we employed bibliometric analysis to characterize the current state of research in these areas. Publications were sourced from the Web of Science Core Collection (WoSCC) covering the period from 2014 to September 20, 2024. Our analysis concentrated on the distribution of annual publications, as well as the contributions of countries, institutions, authors, source journals, keyword co-occurrence, and co-citation patterns. Additionally, we explored keyword clustering to facilitate a deeper understanding of the research landscape and to identify emerging issues and research opportunities. The aim is to provide valuable references for future research on mechanisms, the discovery of novel drugs, and strategies for combination therapy.
2. Results
2.1. The Trends in Annual Global Publications
As of our search date, 6, 337 articles related to biologics and small molecules for IBD were identified in the WoSCC. The strategy for data collection and retrieval is depicted in Figure 2a. Figure 2b illustrates the number of articles published on the use of biologics and small molecules in the treatment of patients with IBD from 2014 to 2024. The annual volume of publications serves as a critical metric for assessing the popularity and progression of research within a specific domain.
Overall, the volume of publications has demonstrated an upward trend, peaking in 2021-2022, followed by a slight decline in 2023, yet maintaining an overall upward trajectory. It remains uncertain whether 2024 will mark a turning point in the research enthusiasm within this field. This analysis underscores the increasing focus and importance placed by the global academic community on biologics and small molecule drugs for the treatment of IBD.
2.2. Distribution of Source Journals
The articles on biologics or small molecules for IBD were published across 855 journals. Table 1 lists the top 10 journals that published the most articles on this topic, accounting for 36.7% (2, 326 out of 6, 337) of the total publications. “Inflammatory Bowel Diseases” emerged as the most prolific journal with 579 publications, followed by the “Journal of Crohn’s & Colitis” with 480 publications, and “Alimentary Pharmacology & Therapeutics” with 250 publications.
2.3. Citation Analysis
A total of 6, 337 articles were cited 148, 141 times. Table 2 presents the top 10 most cited articles on biologics and small molecules for IBD. The citation count for these top 10 articles ranges from 667 to 1, 386. The article titled “3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical, ” published in the Journal of Crohn’s & Colitis in 2017, received the highest number of citations, totaling 1, 386.
2.4. Distribution and Co-Authorship of Countries/Regions
The exploration and therapeutic application of biologics and small molecules in the treatment of IBD have attracted global attention, involving research contributions from 93 countries/regions, as illustrated in Figure 3a. The distribution map of research hotspots clearly indicates that North America, particularly the United States and Canada, along with Western European countries such as Italy and France, exhibit significant interest in this research domain. Furthermore, China, with 6, 224 publications and 8, 336 citations, stands as a leading developing country in Asia, ranking fourth in scientific research contributions to this field, following the USA (1, 943 publications, 66, 320 citations), Canada (678 publications, 34, 707 citations), and Italy (655 publications, 25 166 citations).
Figure 3c illustrates other highly productive countries and regions that are ranked among the top 10 globally. A co-occurrence analysis of countries and territories was conducted using VOSviewer, revealing international collaboration networks within this field (Figure 3b). Out of the 93 countries analyzed, 52 have published 10 or more articles, which are organized into six clusters, each represented by a distinct color. The largest cluster, depicted in red, comprises 19 countries and is centered around Italy, Israel, and Denmark. The United States exhibited the highest number of collaborative partners (n = 51), followed by Italy (n = 50), Canada (n = 49), the United Kingdom (n = 49), Germany (n = 47), France (n = 47), and the Netherlands (n = 47).
2.5. Distribution and Co-Authorship of Institutions
A total of 7, 430 institutions have contributed to research on biologics and small molecules for IBD. The top 10 most prolific institutions are presented in Figure 4b, with the University of California, San Diego leading (291 publications, 23, 017 citations), followed by the Icahn School of Medicine at Mount Sinai (274 publications, 16, 595 citations) and Katholieke Universiteit Leuven (197 publications, 8, 373 citations).Upon setting the threshold for the minimum number of published articles by institutions at 50, a total of 54 institutions met the criteria. VOSviewer was employed to conduct a co-authorship analysis of these 54 prolific institutions (refer to Figure 4a). These institutions were categorized into six clusters, each represented by a unique color. The red cluster, comprising 15 institutions, prominently included the University of Tel Aviv, the University of Amsterdam, and the University of Calgary, and was identified as the largest cluster. The Icahn School of Medicine at Mount Sinai exhibited the highest number of collaborative partners (n = 50), followed by the Mayo Clinic (n = 48), the Medical University of Vienna (n = 48), and the University of Amsterdam (n = 47).
2.6. Distribution and Co-Authorship of Authors
A total of 28, 324 authors contributed to the publication of 6, 337 retrieved articles. Figure 5b illustrates the top 20 most productive authors. Vermeire, Severine, with 180 publications and 10, 383 citations, was the most prolific author, followed by Sandborn, William J, with 177 publications and 15, 117 citations, and Peyrin-Billet, Laurent, with 169 publications and 7, 029 citations. In the current study, VOSviewer was utilized to conduct a co-authorship analysis. A minimum threshold of 35 published articles per author was established. Among the 28, 324 authors analyzed, 58 met this criterion. Figure 5a illustrates the co-authorship network of these authors, who were organized into eight clusters, each represented by a different color. The red cluster comprises 12 authors, with Danese Silvio, D’haens Geert, and D’haens Geert R. at the center. Peyrin-Biroulet Laurent had the highest number of collaborative partners (n = 47), followed by Danese Silvio (n = 46), D’haens Geert (n = 46), and Vermeire Severine (n = 46).
2.7. Co-Citation Analysis
The 6, 337 publications retrieved cited a total of 86, 764 references. Table 3 presents the top 10 co-cited references, with citations ranging from 349 to 817. The most cited reference was the paper titled “Infliximab for Induction and Maintenance Therapy for Ulcerative Colitis, ” published in The New England Journal of Medicine in 2005, which received 817 citations.
2.8. The Co-Occurrence Analysis of the Top 100 Keywords
Keywords encapsulate the primary topics of publications, making high-frequency keywords particularly suitable for co-occurrence analysis. In this study, VOSviewer extracted and clustered the top 100 keywords. Figure 6a presents a network map visualization of the top 100 keywords, organized into six clusters based on their co-occurrence. The node labels denote the keywords, while the size of each node reflects the frequency of the keyword’s occurrence. Connections between nodes indicate co-occurrence relationships among the respective keywords.
Central to the network map are the keywords: inflammatory bowel disease (3, 707 occurrences), infliximab (3, 305), Crohn’s disease (3, 205), ulcerative colitis (2, 267), maintenance therapy (1, 744), and anti-TNFα (1, 262). Keywords with similar characteristics are grouped into six distinct clusters, which are visually differentiated by color: red (Cluster 1), green (Cluster 2), cerulean (Cluster 3), yellow (Cluster 4), purple (Cluster 5), and blue (Cluster 6). Specifically, Cluster 1 (red) pertains to disease, Cluster 2 (green) to drugs, Cluster 3 (cerulean) to surgery, Cluster 4 (yellow) to therapeutic drug monitoring, Cluster 5 (purple) to mechanism research for IBD and therapeutic drugs, and Cluster 6 (blue) encompasses various topics, including different populations, treatment types, complications, and precautions.
To examine the temporal progression of research topic trends, keywords extracted from publications are visualized using a VOSviewer overlay and are color-coded based on their average year of appearance (Figure 6b). Keywords represented in cooler hues denote those that emerged earlier, whereas those in warmer tones signify more recent occurrences. The most contemporary and frequently occurring keywords include biologics, vedolizumab, ustekinumab, tofacitinib, Janus kinase inhibitors, safety, therapeutic drug monitoring, biomarkers, cytokines, induction therapy, and gut microbiota.
3. Discussion
3.1. IBD and Immune Dysregulation
Dysregulation Immune dysregulation is a critical factor in the pathogenesis of IBD [13]. Under normal physiological conditions, the migration of T lymphocytes to the intestinal mucosa is stringently controlled. However, in pathological states, the integrity of the intestinal epithelial barrier is compromised, leading to increased permeability. This breach allows microorganisms or antigens to infiltrate the intestinal wall, initially causing aberrant T lymphocyte migration. This aberration triggers damage to the intestinal mucosa and further exacerbates its permeability. Consequently, this process stimulates the production of various inflammatory mediators. The body subsequently engages in an adaptive immune response, facilitating the differentiation of additional lymphocytes through pro-inflammatory cytokines. This exacerbates mucosal damage and results in the excessive release of cytokines, thereby amplifying the inflammatory cascade characterized by increased severity and duration of inflammation. Prolonged intestinal inflammation contributes to the chronicity of IBD and ongoing intestinal damage [14,15,16,17]. As the disease progresses, it may lead to subsequent complications such as intestinal fibrosis, strictures, abscesses, fistulas, malignancies, and extraintestinal manifestations [16].
Targeting lymphocyte migration to address inflammation caused by immune response dysfunction presents a promising therapeutic avenue for IBD. Current biologics and small molecule drugs, approved for this purpose, operate through this mechanism and are categorized based on their specific targets. These include anti-cytokine monoclonal antibodies targeting TNF-α and interleukins, anti-integrin monoclonal antibodies that inhibit activated lymphocyte surface receptors, and small molecule drugs targeting the JAK/STAT and S1P pathways. (Figure 7)

Table 4.
Administration strategies and trough level of approved biologics and small molecules for IBD.
Table 4.
Administration strategies and trough level of approved biologics and small molecules for IBD.
| Drug | Target | Indication | Induction therapy | Maintenance therapy | Trough level (ug/ml) | ||
| dose | by | dose | by | ||||
| infliximab | TNF-α | UC, CD |
5 mg/kg at 0, 2, 6wk | iv | 5 mg/kg q8w | iv | ≥5 [18]; 3-7 [24]; 5-10 [20]; 7-10 (I); 5-7(M) [22] |
| adalimumab | TNF-α | UC, CD |
160 mg day 1, 80 mg day 15 |
sc | 40 mg q2w | sc | ≥7.5 [18]; 4-8 [24]; 8-12 [20]; >10-12(I, M) [22] |
| golimumab | TNF-α | UC | 200 mg day 1, 100 mg day 15 |
sc | 100 mg q4 w; < 80 kg, 50 mg q4w; >80 kg, 100 mg q4w |
sc | >2.5 [19] |
| certolizumab | TNF-α |
CD | 400 mg 0, 2, 4 wk | sc | 400 mg q4w | sc | ≥20 [18] |
| vedolizumab | α4β7 Integrin | UC, CD |
300 mg at 0, 2, 6wk | iv | 300 mg q8w | iv | >33-37(6wk); >15-20(14wk); >10-15(M) [23] |
| natalizumab | α4 Integrin |
CD | 300 mg at 0, 4, 8, 12wk | iv | 300 mg, q4w | iv | |
| ustekinumab | IL-12/23 p40 | UC, CD |
<55 kg, 260 mg 55–85 kg, 390 mg >85 kg, 520 mg |
iv | 90 mg q8w | sc | >3-7(8wk); >1-3(maintenance) [23]; >11.1(I); >4.5(M) [22] |
| risankizumab | IL-23p19 | CD | 600 mg at 0, 4, 8 wk |
iv | 180 mg or 360 mg q8w | sc | NA |
| mirikizumab | IL-23p19 | UC | 300 mg at 0, 4, 8 wk |
iv | 200 mg at 12w, q4w | iv | |
| tofacitinib | JAK-1/2/3 | UC | 10 mg bid for 8 weeks |
po | 5 mg or 10 mg bid | po | |
| upadacitinib | JAK-1 | UC, CD |
45 mg daily for 8 weeks(UC) 12 weeks(CD) |
po | 15 mg or 30 mg qd | po | |
| filgotinib | JAK-1 | UC | 200 mg qd for 22 weeks |
po | 200 mg qd | po | |
| ozanimod | S1PR | UC | 0.23 mg qd, day 1–4 0.46 mg qd, day 5–7 |
po |
0.92 mg qd | po |
|
| etrasimod | S1PR | UC | 2mg qd | po | 2mg qd | po | |
3.2. Biologics for IBD
Although biologics are widely used in IBD management, approximately 30% of patients exhibit primary non-response, where the treatment is initially ineffective. Furthermore, up to 50% of patients may experience a secondary loss of response, where the treatment’s efficacy diminishes over time [25,26,27]. This loss of response is a complex phenomenon influenced by multiple factors. The following are potential reasons for non-response: One potential reason for non-response is the significant heterogeneity of IBD, as patients display diverse genetic profiles, immune responses, and disease phenotypes. If the primary causative factors are not effectively targeted by biological agents or involve other non-specific inflammatory pathways, this may lead to suboptimal responses to specific biological therapies in certain individuals [28]. Secondly, inadequate drug dosing or incorrect dosing intervals, along with individual variations in drug metabolism and clearance rates, can affect the concentration of medications in the body and, consequently, their therapeutic effectiveness. Thirdly, some biological agents are categorized as humanized or chimeric monoclonal antibodies. Although these are engineered to minimize immunogenicity, they may still elicit immune responses in patients. The production of anti-drug antibodies (ADAs) in the patient’s body can neutralize the drug and diminish its efficacy [29]. Fourthly, prolonged use of biologics may result in increased tolerance or adverse effects, contributing to a reduction in therapeutic efficacy. Potential side effects during biologic treatment include infections, malignancies, and immunogenic reactions, which could impact long-term treatment outcomes for patients [30].
In cases of unresponsive patients, therapeutic drug monitoring (TDM) can be utilized to evaluate serum drug trough concentrations and anti-drug antibody (ADA) levels alongside disease activity staging. Administration strategies and trough levels of approved biologics and small molecules for IBD are shown in Table 4. This methodology aids clinicians in determining the necessity of medication adjustments, optimizing treatment regimens, preventing adverse events, and improving recovery outcomes (Figure 8). However, neither the American Gastroenterological Association (AGA) nor the IBD guidelines from countries such as China have yet to define specific recommended some trough concentrations for various clinical outcomes, including symptom relief, mucosal healing, and perianal relief. As a result, standardized concentration benchmarks remain lacking.
3.3. Small Molecules for IBD
In contrast to biologics, small molecules such as Janus kinase (JAK) inhibitors and sphingosine-1-phosphate receptor (S1PR) modulators are non-immunogenic, convenient for oral administration, possess a short half-life, exert rapid effects, and demonstrate a linear dose-response relationship. Furthermore, they can serve as viable second-line treatment options for patients. The potential risks associated with these drugs, including thrombosis and infection, limit their clinical application. Therefore, it is essential to conduct comprehensive risk factor assessments—considering factors such as tumor presence, cardiovascular risk factors, age, and smoking habits—prior to selecting this class of medication. The FDA has explicitly indicated that Upatinib may lead to severe, potentially life-threatening adverse reactions, including serious infections, malignant tumors, major cardiovascular events, and thrombotic risks [31].
Despite these risks, these medications are prescribed for the treatment of various immune-mediated inflammatory diseases (IMIDs). When utilizing the same therapeutic strategy for different conditions, it is crucial to adjust the dosage accordingly. Upatinib, the only JAK1 inhibitor approved for the treatment of IBD in China, is also indicated for other IMIDs such as atopic dermatitis, rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis, with a recommended dosage of 15 mg once daily. However, for the induction phase of IBD treatment, the advised dosage is 45 mg once daily. Up to 50% of patients with IBD experience at least one extraintestinal manifestation [32], such as peripheral arthritis, episcleritis, stomatitis, and erythema nodosum, which are often associated with IBD flare-ups. Additionally, conditions such as ankylosing spondylitis, sacroiliitis, uveitis, pyoderma gangrenosum, and primary sclerosing cholangitis are closely related to IBD, though not necessarily linked to its activity. These typical extraintestinal manifestations are part of IMID) [33]. Consequently, IBD patients presenting with extraintestinal symptoms require a multidisciplinary approach for diagnosis and treatment to determine the appropriate medication dosage, thereby preventing ineffective therapy and disease progression.
S1PR modulators are associated with an increased risk of herpes zoster infection and transient cardiovascular events [31]. As dosages increase, the likelihood of adverse reactions and toxic side effects may also rise. The TDM of small molecules in IBD remains imperfect, and the AGA has not yet issued guidance on the clinical efficacy comparison and TDM of drugs with similar mechanisms. [34,35,36].
3.4. Natural Herbal Medicine
Moreover, drugs with potential therapeutic applications, such as berberine [37,38], Scutellaria baicalensis [39], curcumin [40], honeysuckle [41], and other plant-derived traditional Chinese medicines, have shown promising therapeutic effects on UC in animal studies. These traditional Chinese medicines have demonstrated efficacy in modulating gut microbiota, managing inflammatory responses, repairing intestinal mucosa, and alleviating diarrhea. The associated signaling pathways encompass PI3K/Akt, NF—κ B, JAK/STAT, MAPK, and Notch, among others. However, given that many of these treatments are compound and decoction formulations, further research is necessary to elucidate the specific mechanisms of action and identify the principal active ingredients of individual compounds [40,42,43,44].
4. Materials and Methods
4.1. Data Source and Strategy for Retrieval
In this cross-sectional study, all data were collected from the Science Citation Index (SCI) and Social Sciences Citation Index (SSCI) databases of the Web of Science Core Collection (WoSCC) on a single day (September 20, 2024). Set search formula: TS = [(Crohn disease “OR” ulcerative colitis “OR” inflammatory bowel disease “) AND (“biological product” OR “small molecules” OR “infliximab OR “adalimumab” OR “adalimumab” OR “vedolizumab” OR “ustekinumab” OR “upadacitinib” OR “golimumab” OR “determinolizumab pegol” OR “natalizumab” OR “riskizumab” OR “mirikizumab” OR “tofacitinib” OR “filmotinib”) OR “ozanimod” OR “etrasimod”]. The time span was from January 2014 to September 20, 2024, and the type was “article”. The specific data collection and retrieval strategies are detailed in the appendix.
4.2. Bibliometric Analysis and Visualization
By leveraging the technical tools and methodologies of information visualization, bibliometrics can effectively depict the research and development trajectory, current status, focal points, and emerging trends within a specific subject area. In this study, we utilized the online platform CNSknowal.com to create a distribution map that illustrates the countries and regions of publication for the articles analyzed. Subsequently, using VOSviewer (version 1.6.20), we conducted a visual analysis of authors, research institutions, countries/regions, citations, and keywords to explore the current research landscape and identify emerging hotspots within this academic domain.
5. Conclusions
Through bibliometric analysis and visualization techniques applied to keywords, our study reveals that biologics and small molecules are the primary focus of research and clinical application among current therapeutic drugs for IBD. The research emphasis has shifted from employing single induction therapies and maintaining remission with various biologics and small molecule drugs to the precise conversion of therapies or the use of drug combinations with differing mechanisms in cases of non-responsiveness.
The immunogenicity of biologics and the safety concerns associated with potential infections, thromboembolism, and the risk of malignant tumors linked to JAK inhibitors and S1P receptor modulators warrant significant attention [31,45,46]. Concurrently, addressing these immunogenicity challenges and safety concerns is crucial. A comprehensive evaluation of the efficacy and safety of current therapeutic drugs for monotherapy, combination therapy, and conversion therapy, alongside the development of novel drugs targeting various inflammatory pathways, will be pivotal in future research endeavors.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Search strategy; Table S1: Clusters of the top 100 Keywords.
Author Contributions
Conceptualization, L.HB.; methodology, L.H.B.; software, W.J.; validation, L.Y., and L.J.; formal analysis, L.J.; investigation, L.Y.; resources, L.H.B.; data curation, W.J. and H.Y.; writing—original draft preparation, W.J.; writing—review and editing, all authors.; visualization, W.J.; supervision, Z.RS.; project administration, Z.RS.; funding acquisition, L.HB., Z.Y.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Key Clinical Projects of Peking University Third Hospital, grant number BYSYZD2022022; Peking University Medicine Sailing Program for Young Scholars’ Scientific & Technological Innovation BMU2024YFJHPY040; Fund for Returned Overseas Talents of Peking University Third Hospital BYSYLXHG2024010.
Institutional Review Board Statement
Not applicable
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rosen, M.J.; Dhawan, A.; Saeed, S.A. Inflammatory Bowel Disease in Children and Adolescents. JAMA Pediatr 2015, 169, 1053–60. [Google Scholar] [CrossRef]
- Matsuoka, K.; Kobayashi, T.; Ueno, F.; Matsui, T.; Hirai, F.; Inoue, N.; Kato, J.; Kobayashi, K.; Kobayashi, K.; Koganei, K.; Kunisaki, R.; Motoya, S.; Nagahori, M.; Nakase, H.; Omata, F.; Saruta, M.; Watanabe, T.; Tanaka, T.; Kanai, T.; Noguchi, Y.; Takahashi, K.I.; Watanabe, K.; Hibi, T.; Suzuki, Y.; Watanabe, M.; Sugano, K.; Shimosegawa, T. Evidence-based clinical practice guidelines for inflammatory bowel disease. J Gastroenterol 2018, 53, 305–353. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Murphy, M.; Malter, L. A Review of Available Medical Therapies to Treat Moderate-to-Severe Inflammatory Bowel Disease. Am J Gastroenterol 2024, 119, 55–80. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, J.D.; Isaacs, K.L.; Schneider, Y.; Siddique, S.M.; Falck-Ytter, Y.; Singh, S. AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis. Gastroenterology 2020, 158, 1450–1461. [Google Scholar] [CrossRef]
- 5. Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; Biancone, L.; Bokemeyer, B.; Bossuyt, P.; Burisch, J.; Collins, P.; El-Hussuna, A.; Ellul, P.; Frei-Lanter, C.; Furfaro, F.; Gingert, C.; Gionchetti, P.; Gomollon, F.; González-Lorenzo, M.; Gordon, H.; Hlavaty, T.; Juillerat, P.; Katsanos, K.; Kopylov, U.; Krustins, E.; Lytras, T.; Maaser, C.; Magro, F.; Marshall, J.K.; Myrelid, P.; Pellino, G.; Rosa, I.; Sabino, J.; Savarino, E.; Spinelli, A.; Stassen, L.; Uzzan, M.; Vavricka, S.; Verstockt, B.; Warusavitarne, J.; Zmora, O.; Fiorino, G. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J Crohns Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, J.D.; Ho, E.Y.; Shmidt, E.; Singh, H.; Falck-Ytter, Y.; Sultan, S.; Terdiman, J.P. AGA Clinical Practice Guidelines on the Medical Management of Moderate to Severe Luminal and Perianal Fistulizing Crohn’s Disease. Gastroenterology 2021, 160, 2496–2508. [Google Scholar] [CrossRef]
- Raine, T.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; Eder, P.; Ellul, P.; Fidalgo, C.; Fiorino, G.; Gionchetti, P.; Gisbert, J.P.; Gordon, H.; Hedin, C.; Holubar, S.; Iacucci, M.; Karmiris, K.; Katsanos, K.; Kopylov, U.; Lakatos, P.L.; Lytras, T.; Lyutakov, I.; Noor, N.; Pellino, G.; Piovani, D.; Savarino, E.; Selvaggi, F.; Verstockt, B.; Spinelli, A.; Panis, Y.; Doherty, G. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment. J Crohns Colitis 2022, 16, 2–17. [Google Scholar] [CrossRef]
- Frolkis, A.D.; Dykeman, J.; Negrón, M.E.; Debruyn, J.; Jette, N.; Fiest, K.M.; Frolkis, T.; Barkema, H.W.; Rioux, K.P.; Panaccione, R.; Ghosh, S.; Wiebe, S.; Kaplan, G.G. Risk of surgery for inflammatory bowel diseases has decreased over time: a systematic review and meta-analysis of population-based studies. Gastroenterology 2013, 145, 996–1006. [Google Scholar] [CrossRef]
- Tsai, L.; Ma, C.; Dulai, P.S.; Prokop, L.J.; Eisenstein, S.; Ramamoorthy, S.L.; Feagan, B.G.; Jairath, V.; Sandborn, W.J.; Singh, S. Contemporary Risk of Surgery in Patients With Ulcerative Colitis and Crohn’s Disease: A Meta-Analysis of Population-Based Cohorts. Clin Gastroenterol Hepatol 2021, 19, 2031–2045.e11. [Google Scholar] [CrossRef]
- Singh, S.; Ananthakrishnan, A.N.; Nguyen, N.H.; Cohen, B.L.; Velayos, F.S.; Weiss, J.M.; Sultan, S.; Siddique, S.M.; Adler, J.; Chachu, K.A. AGA Clinical Practice Guideline on the Role of Biomarkers for the Management of Ulcerative Colitis. Gastroenterology 2023, 164, 344–372. [Google Scholar] [CrossRef]
- Ninkov, A.; Frank, J.R.; Maggio, L.A. Bibliometrics: Methods for studying academic publishing. Perspect Med Educ 2022, 11, 173–176. [Google Scholar] [CrossRef]
- Arruda, H.; Silva, E.R.; Lessa, M.; Proença, D., Jr.; Bartholo, R. VOSviewer and Bibliometrix. J Med Libr Assoc 2022, 110, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Guan, Q. A Comprehensive Review and Update on the Pathogenesis of Inflammatory Bowel Disease. J Immunol Res 2019, 2019, 7247238. [Google Scholar] [CrossRef] [PubMed]
- Nikolakis, D.; de Voogd, F.A.E.; Pruijt, M.J.; Grootjans, J.; van de Sande, M.G.; D’Haens, G.R. The Role of the Lymphatic System in the Pathogenesis and Treatment of Inflammatory Bowel Disease. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Coskun, M.; Vermeire, S.; Nielsen, O.H. Novel Targeted Therapies for Inflammatory Bowel Disease. Trends Pharmacol Sci 2017, 38, 127–142. [Google Scholar] [CrossRef]
- Neurath, M.F. Cytokines in inflammatory bowel disease. Nat Rev Immunol 2014, 14, 329–342. [Google Scholar] [CrossRef]
- Kim, D.H.; Cheon, J.H. Pathogenesis of Inflammatory Bowel Disease and Recent Advances in Biologic Therapies. Immune Netw 2017, 17, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Feuerstein, J.D.; Nguyen, G.C.; Kupfer, S.S.; Falck-Ytter, Y.; Singh, S. American Gastroenterological Association Institute Guideline on Therapeutic Drug Monitoring in Inflammatory Bowel Disease. Gastroenterology 2017, 153, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Harzallah, I.; Rigaill, J.; Williet, N.; Paul, S.; Roblin, X. Golimumab pharmacokinetics in ulcerative colitis: a literature review. Therap Adv Gastroenterol 2017, 10, 89–100. [Google Scholar] [CrossRef]
- Cheifetz, A.S.; Abreu, M.T.; Afif, W.; Cross, R.K.; Dubinsky, M.C.; Loftus, E.V., Jr.; Osterman, M.T.; Saroufim, A.; Siegel, C.A.; Yarur, A.J.; Melmed, G.Y.; Papamichael, K. A Comprehensive Literature Review and Expert Consensus Statement on Therapeutic Drug Monitoring of Biologics in Inflammatory Bowel Disease. Am J Gastroenterol 2021, 116, 2014–2025. [Google Scholar] [CrossRef] [PubMed]
- Ooi, C.J.; Hilmi, I.; Banerjee, R.; Chuah, S.W.; Ng, S.C.; Wei, S.C.; Makharia, G.K.; Pisespongsa, P.; Chen, M.H.; Ran, Z.H.; Ye, B.D.; Park, D.I.; Ling, K.L.; Ong, D.; Ahuja, V.; Goh, K.L.; Sollano, J.; Lim, W.C.; Leung, W.K.; Ali, R.A.R.; Wu, D.C.; Ong, E.; Mustaffa, N.; Limsrivilai, J.; Hisamatsu, T.; Yang, S.K.; Ouyang, Q.; Geary, R.; De Silva, J.H.; Rerknimitr, R.; Simadibrata, M.; Abdullah, M.; Leong, R.W.L. Best practices on immunomodulators and biologic agents for ulcerative colitis and Crohn’s disease in Asia. J Gastroenterol Hepatol 2019, 34, 1296–1315. [Google Scholar] [CrossRef]
- Rodríguez-Moranta, F.; Argüelles-Arias, F.; Hinojosa Del Val, J.; Iborra Colomino, M.; Martín-Arranz, M.D.; Menchén Viso, L.; Muñoz Núñez, F.; Ricart Gómez, E.; Sánchez-Hernández, J.G.; Valdés-Delgado, T.; Guardiola Capón, J.; Barreiro-de Acosta, M.; Mañosa Ciria, M.; Zabana Abdo, Y.; Gutiérrez Casbas, A. Therapeutic drug monitoring in inflammatory bowel diseases. Position statement of the Spanish Working Group on Crohn’s Disease and Ulcerative Colitis. Gastroenterol Hepatol 2024, 47, 522–552. [Google Scholar] [CrossRef] [PubMed]
- Restellini, S.; Afif, W. Update on TDM (Therapeutic Drug Monitoring) with Ustekinumab, Vedolizumab and Tofacitinib in Inflammatory Bowel Disease. J Clin Med 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Ooi, C.J.; Hilmi, I.; Banerjee, R.; Chuah, S.W.; Ng, S.C.; Wei, S.C.; Makharia, G.K.; Pisespongsa, P.; Chen, M.H.; Ran, Z.H.; Ye, B.D.; Park, D.I.; Ling, K.L.; Ong, D.; Ahuja, V.; Goh, K.L.; Sollano, J.; Lim, W.C.; Leung, W.K.; Ali, R.A.R.; Wu, D.C.; Ong, E.; Mustaffa, N.; Limsrivilai, J.; Hisamatsu, T.; Yang, S.K.; Ouyang, Q.; Geary, R.; De Silva, J.H.; Rerknimitr, R.; Simadibrata, M.; Abdullah, M.; Leong, R.W. Best practices on immunomodulators and biologic agents for ulcerative colitis and Crohn’s disease in Asia. Intest Res 2019, 17, 285–310. [Google Scholar] [CrossRef] [PubMed]
- Sparrow, M.P.; Papamichael, K.; Ward, M.G.; Riviere, P.; Laharie, D.; Paul, S.; Roblin, X. Therapeutic Drug Monitoring of Biologics During Induction to Prevent Primary Non-Response. J Crohns Colitis 2020, 14, 542–556. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Cheifetz, A.S.; Melmed, G.Y.; Irving, P.M.; Vande Casteele, N.; Kozuch, P.L.; Raffals, L.E.; Baidoo, L.; Bressler, B.; Devlin, S.M.; Jones, J.; Kaplan, G.G.; Sparrow, M.P.; Velayos, F.S.; Ullman, T.; Siegel, C.A. Appropriate Therapeutic Drug Monitoring of Biologic Agents for Patients With Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol 2019, 17, 1655–1668.e3. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Lichtenstein, L.; Assa, A.; Mazor, Y.; Weiss, B.; Levine, A.; Ron, Y.; Kopylov, U.; Bujanover, Y.; Rosenbach, Y.; Ungar, B.; Eliakim, R.; Chowers, Y.; Shamir, R.; Fraser, G.; Dotan, I.; Ben-Horin, S. Levels of drug and antidrug antibodies are associated with outcome of interventions after loss of response to infliximab or adalimumab. Clin Gastroenterol Hepatol 2015, 13, 522–530.e2. [Google Scholar] [CrossRef] [PubMed]
- Ashton, J.J.; Green, Z.; Kolimarala, V.; Beattie, R.M. Inflammatory bowel disease: long-term therapeutic challenges. Expert Rev Gastroenterol Hepatol 2019, 13, 1049–1063. [Google Scholar] [CrossRef]
- Vermeire, S.; Gils, A.; Accossato, P.; Lula, S.; Marren, A. Immunogenicity of biologics in inflammatory bowel disease. Therap Adv Gastroenterol 2018, 11, 1756283x17750355. [Google Scholar] [CrossRef] [PubMed]
- Larussa, T.; Basile, A.; Palleria, C.; Iannelli, C.; Vero, A.; Giubilei, L.; De Sarro, C.; Suraci, E.; Marasco, R.; Imeneo, M.; Russo, E.; Abenavoli, L.; De Sarro, G.; Luzza, F. Real-life burden of adverse reactions to biological therapy in inflammatory bowel disease: a single-centre prospective case series. Med Pharm Rep 2021, 94, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Solitano, V.; Vuyyuru, S.K.; MacDonald, J.K.; Zayadi, A.; Parker, C.E.; Narula, N.; Peyrin-Biroulet, L.; Danese, S.; Feagan, B.G.; Singh, S.; Ma, C.; Jairath, V. Efficacy and Safety of Advanced Oral Small Molecules for Inflammatory Bowel Disease: Systematic Review and Meta-Analysis. J Crohns Colitis 2023, 17, 800–1816. [Google Scholar] [CrossRef] [PubMed]
- Gordon, H.; Burisch, J.; Ellul, P.; Karmiris, K.; Katsanos, K.; Allocca, M.; Bamias, G.; Barreiro-de Acosta, M.; Braithwaite, T.; Greuter, T.; Harwood, C.; Juillerat, P.; Lobaton, T.; Müller-Ladner, U.; Noor, N.; Pellino, G.; Savarino, E.; Schramm, C.; Soriano, A.; Michael Stein, J.; Uzzan, M.; van Rheenen, P.F.; Vavricka, S.R.; Vecchi, M.; Zuily, S.; Kucharzik, T. ECCO Guidelines on Extraintestinal Manifestations in Inflammatory Bowel Disease. J Crohns Colitis 2024, 18, 1–37. [Google Scholar] [CrossRef]
- Rogler, G.; Singh, A.; Kavanaugh, A.; Rubin, D.T. Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management. Gastroenterology 2021, 161, 1118–1132. [Google Scholar] [CrossRef]
- Mitrev, N.; Vande Casteele, N.; Seow, C.H.; Andrews, J.M.; Connor, S.J.; Moore, G.T.; Barclay, M.; Begun, J.; Bryant, R.; Chan, W.; Corte, C.; Ghaly, S.; Lemberg, D.A.; Kariyawasam, V.; Lewindon, P.; Martin, J.; Mountifield, R.; Radford-Smith, G.; Slobodian, P.; Sparrow, M.; Toong, C.; van Langenberg, D.; Ward, M.G.; Leong, R.W. Review article: consensus statements on therapeutic drug monitoring of anti-tumour necrosis factor therapy in inflammatory bowel diseases. Aliment Pharmacol Ther 2017, 46, 1037–1053. [Google Scholar] [CrossRef] [PubMed]
- Dutt, K.; Vasudevan, A. Therapeutic Drug Monitoring for Biologic and Small-Molecule Therapies for Inflammatory Bowel Disease. Medicina (Kaunas) 2024, 60. [Google Scholar] [CrossRef] [PubMed]
- Dulai, P.S.; Singh, S.; Jairath, V.; Wong, E.; Narula, N. Integrating Evidence to Guide Use of Biologics and Small Molecules for Inflammatory Bowel Diseases. Gastroenterology 2024, 166, 396–408.e2. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Fan, C.; Lu, H.; Feng, C.; He, P.; Yang, X.; Xiang, C.; Zuo, J.; Tang, W. Protective role of berberine on ulcerative colitis through modulating enteric glial cells-intestinal epithelial cells-immune cells interactions. Acta Pharm Sin B 2020, 10, 447–461. [Google Scholar] [CrossRef]
- Dong, Y.; Fan, H.; Zhang, Z.; Jiang, F.; Li, M.; Zhou, H.; Guo, W.; Zhang, Z.; Kang, Z.; Gui, Y.; Shou, Z.; Li, J.; Zhu, R.; Fu, Y.; Sarapultsev, A.; Wang, H.; Luo, S.; Zhang, G.; Hu, D. Berberine ameliorates DSS-induced intestinal mucosal barrier dysfunction through microbiota-dependence and Wnt/β-catenin pathway. Int J Biol Sci 2022, 18, 1381–1397. [Google Scholar] [CrossRef]
- Li, M.X.; Li, M.Y.; Lei, J.X.; Wu, Y.Z.; Li, Z.H.; Chen, L.M.; Zhou, C.L.; Su, J.Y.; Huang, G.X.; Huang, X.Q.; Zheng, X.B. Huangqin decoction ameliorates DSS-induced ulcerative colitis: Role of gut microbiota and amino acid metabolism, mTOR pathway and intestinal epithelial barrier. Phytomedicine 2022, 100, 154052. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Wei, L.; Wang, N.; Li, X.; Miao, M. Efficacy and safety of adjuvant curcumin therapy in ulcerative colitis: A systematic review and meta-analysis. J Ethnopharmacol 2022, 289, 115041. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Ding, J.; Chen, S.; Chen, J.; Wang, C.; Li, J.; Shi, H.; Yin, X.; Wang, J.; Liu, J.; Song, H.; Zhou, Z.; Jiang, X.; Jiang, W.; Jiang, Y.; Cao, M.; Li, B.; Li, J.; Li, L.; Zhang, Y. Alleviation of colitis by honeysuckle MIR2911 via direct regulation of gut microbiota. J Control Release 2024, 376, 123–137. [Google Scholar] [CrossRef]
- Liu, Y.; Li, B.G.; Su, Y.H.; Zhao, R.X.; Song, P.; Li, H.; Cui, X.H.; Gao, H.M.; Zhai, R.X.; Fu, X.J.; Ren, X. Potential activity of Traditional Chinese Medicine against Ulcerative colitis: A review. J Ethnopharmacol 2022, 289, 115084. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Lin, S.; Feng, W.; Liu, Y.; Song, Z.; Pan, G.; Zhang, Y.; Dai, X.; Ding, X.; Chen, L.; Wang, Y. A potential therapeutic target in traditional Chinese medicine for ulcerative colitis: Macrophage polarization. Front Pharmacol 2022, 13, 999179. [Google Scholar] [CrossRef]
- Zheng, S.; Xue, T.; Wang, B.; Guo, H.; Liu, Q. Chinese Medicine in the Treatment of Ulcerative Colitis: The Mechanisms of Signaling Pathway Regulations. Am J Chin Med 2022, 50, 1781–1798. [Google Scholar] [CrossRef] [PubMed]
- Sedano, R.; Ma, C.; Jairath, V.; Feagan, B.G. Janus Kinase Inhibitors for the Management of Patients With Inflammatory Bowel Disease. Gastroenterol Hepatol (N Y) 2022, 18, 14–27. [Google Scholar]
- Parigi, T.L.; Solitano, V.; Peyrin-Biroulet, L.; Danese, S. Do JAK inhibitors have a realistic future in treating Crohn’s disease? Expert Rev Clin Immunol 2022, 18, 181–183. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Timeline of Regulatory Approvals for Biologics and Small Molecules in IBD. * IFX (infliximab), ADA (adalimumab), CZP (certolizumab pegol) GLM (golimumab), VDZ (vedolizumab), NTZ (natalizumab), UST (ustekinumab), RSK (risankizumab), MKZ (mirikizumab), TFN (tofacitinib), FGN (filgotinib), UPA(upadacitinib), OZM (ozanimod), ETM (etrasimod).
Figure 1.
Timeline of Regulatory Approvals for Biologics and Small Molecules in IBD. * IFX (infliximab), ADA (adalimumab), CZP (certolizumab pegol) GLM (golimumab), VDZ (vedolizumab), NTZ (natalizumab), UST (ustekinumab), RSK (risankizumab), MKZ (mirikizumab), TFN (tofacitinib), FGN (filgotinib), UPA(upadacitinib), OZM (ozanimod), ETM (etrasimod).
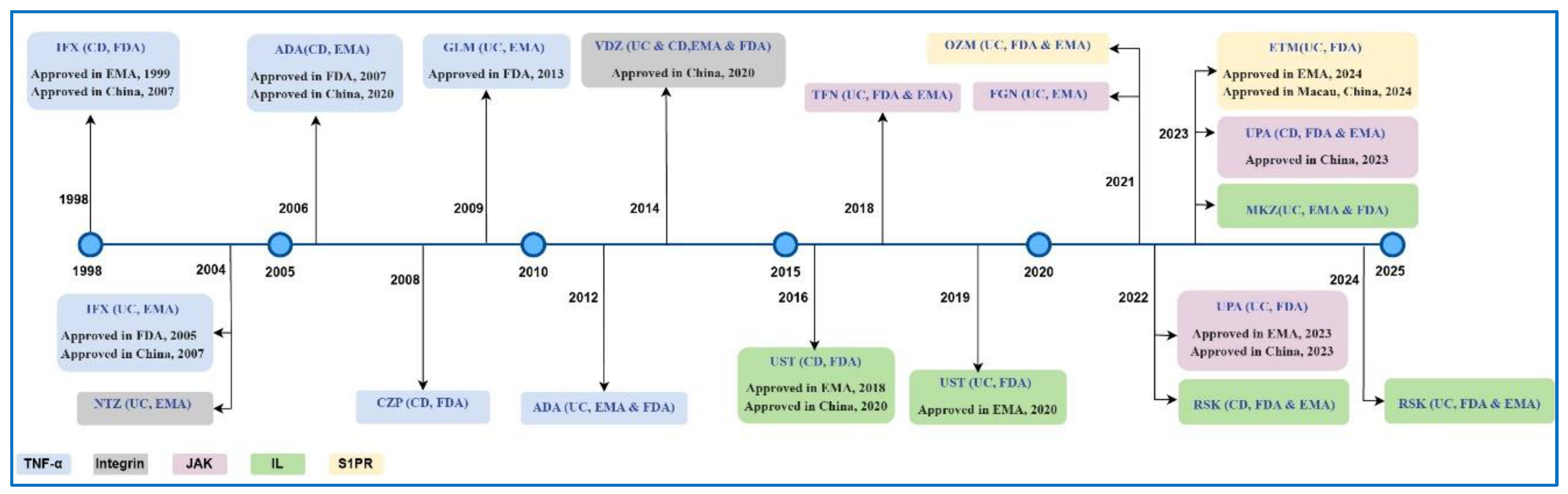
Figure 2.
(a)The data collection and retrieval methodology. (b). The number of articles on biologics and/or small molecules in treating patients with IBD from 2014 to 2024.
Figure 2.
(a)The data collection and retrieval methodology. (b). The number of articles on biologics and/or small molecules in treating patients with IBD from 2014 to 2024.
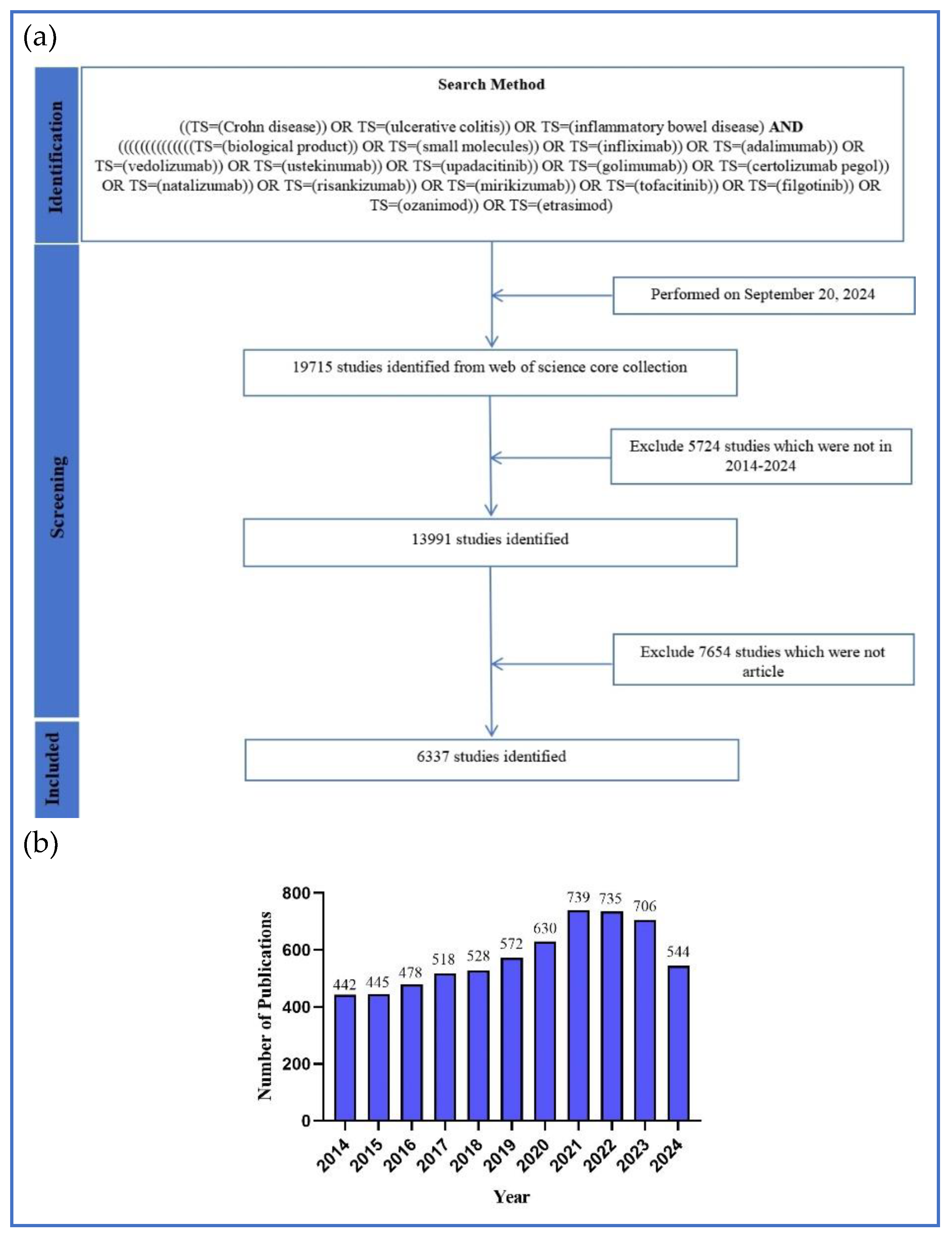
Figure 3.
(a)Distribution of countries/regions. (b)The co-authorship network of countries/regions. (c)The top 10 productive countries/regions.
Figure 3.
(a)Distribution of countries/regions. (b)The co-authorship network of countries/regions. (c)The top 10 productive countries/regions.
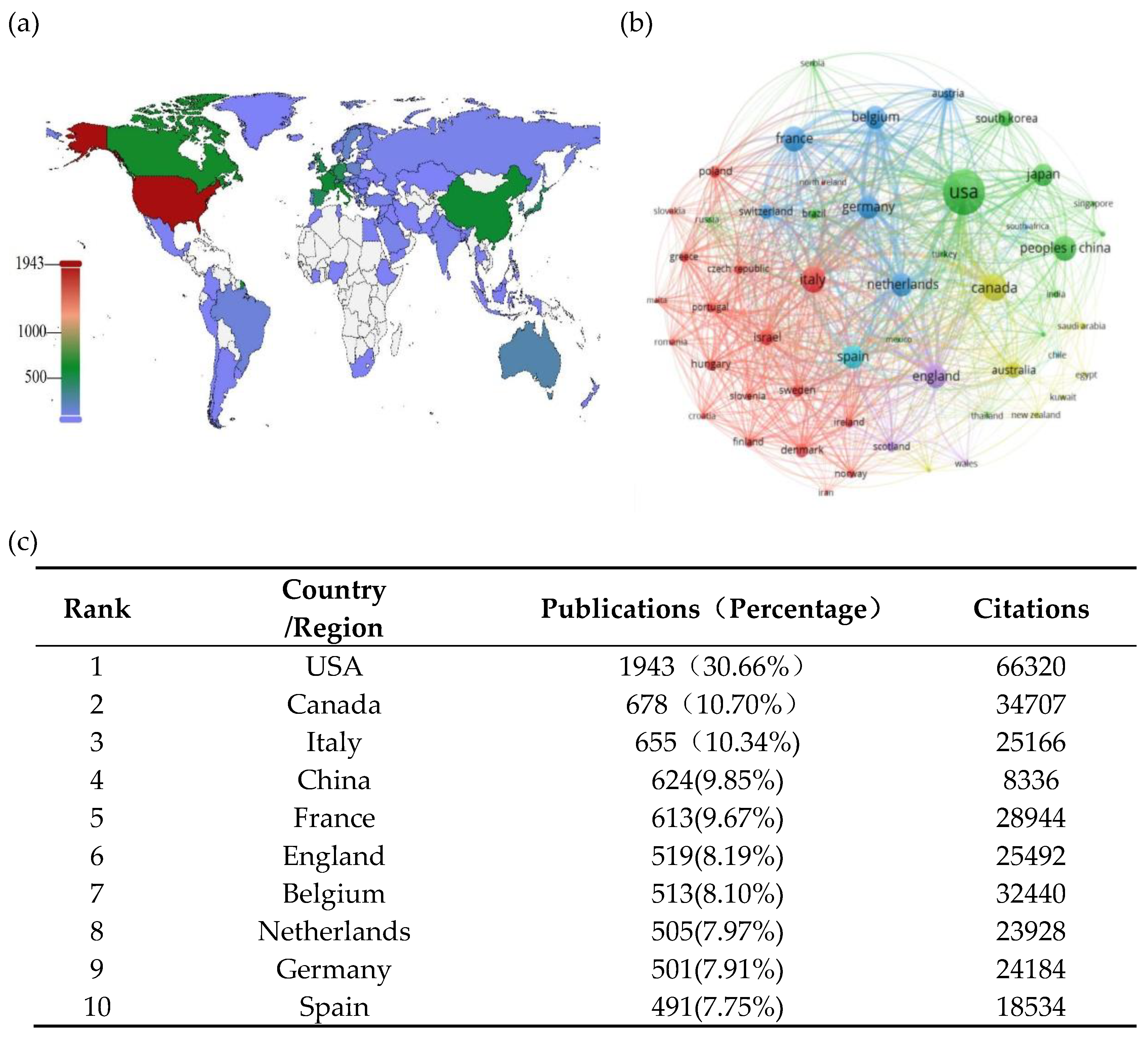
Figure 4.
(a)The co-authorship network of institutions. (b)The top 10 productive institutions.
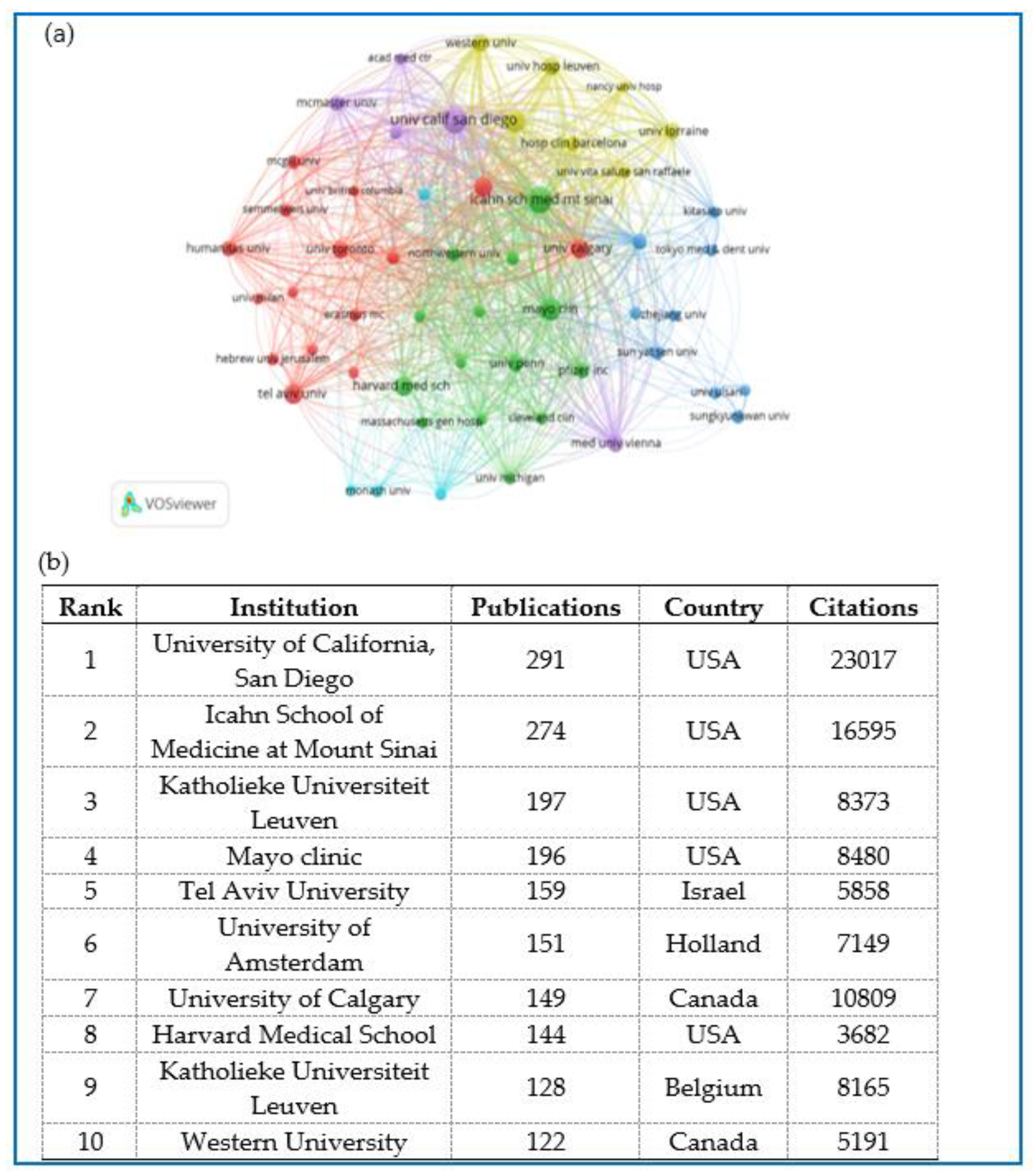
Figure 5.
(a)The co-authorship network of authors. (b)The top 20 productive authors.
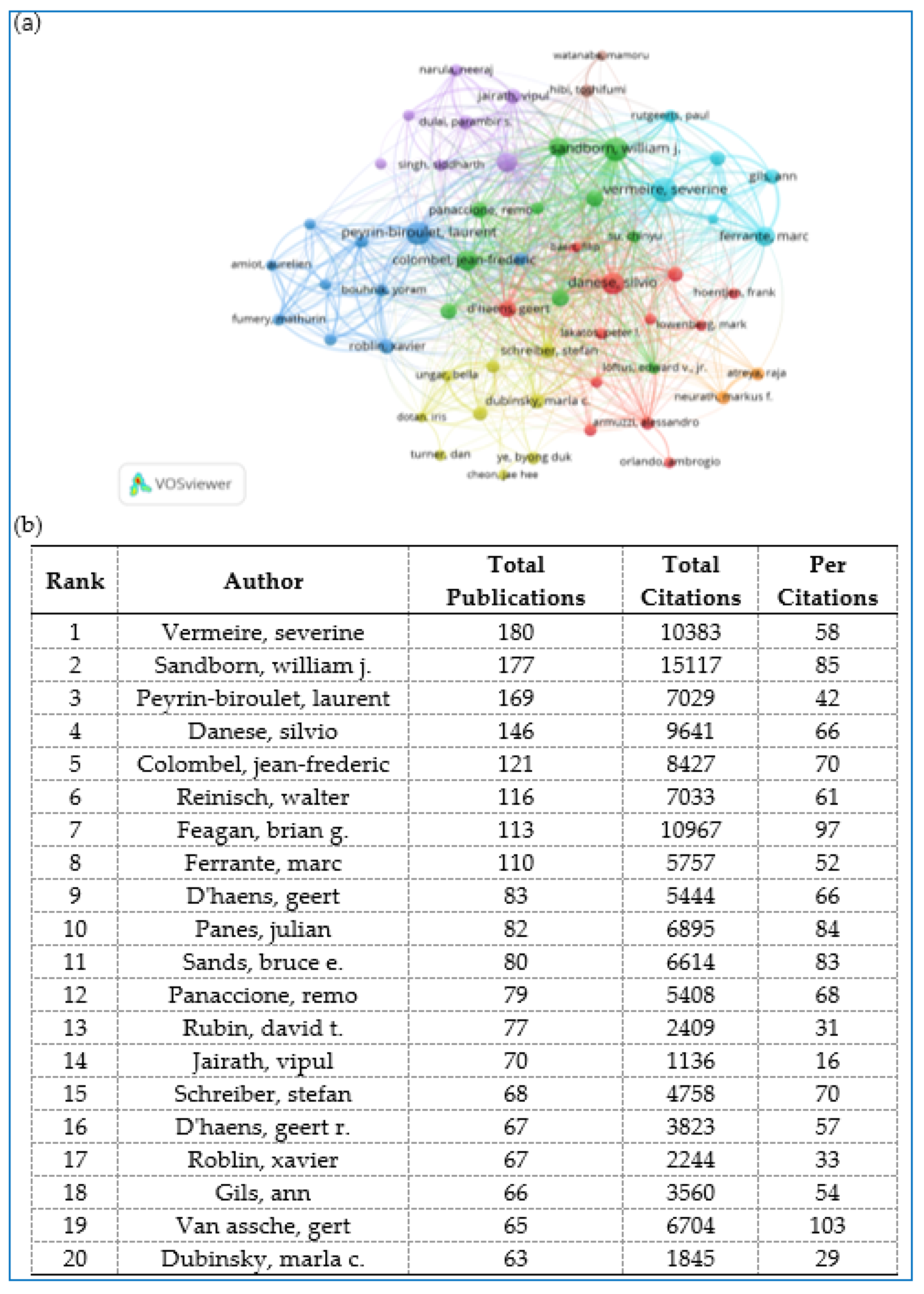
Figure 6.
(a)The co-occurrence and cluster analysis of the top 100 keywords. (b)The overlay visualization of the top 100 Keywords.
Figure 6.
(a)The co-occurrence and cluster analysis of the top 100 keywords. (b)The overlay visualization of the top 100 Keywords.
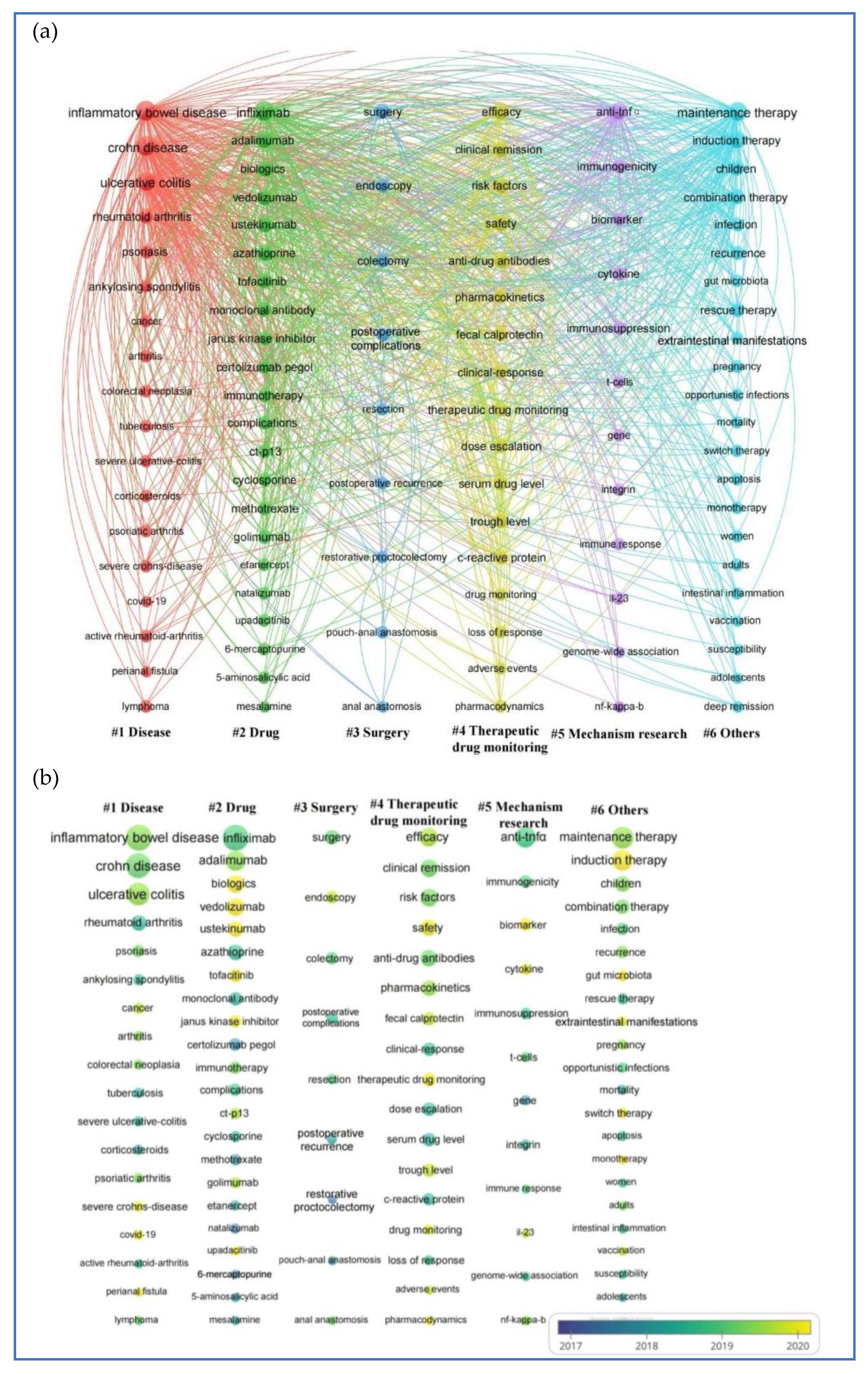
Figure 7.
Targets and IBD biologics and small molecules for IBD.
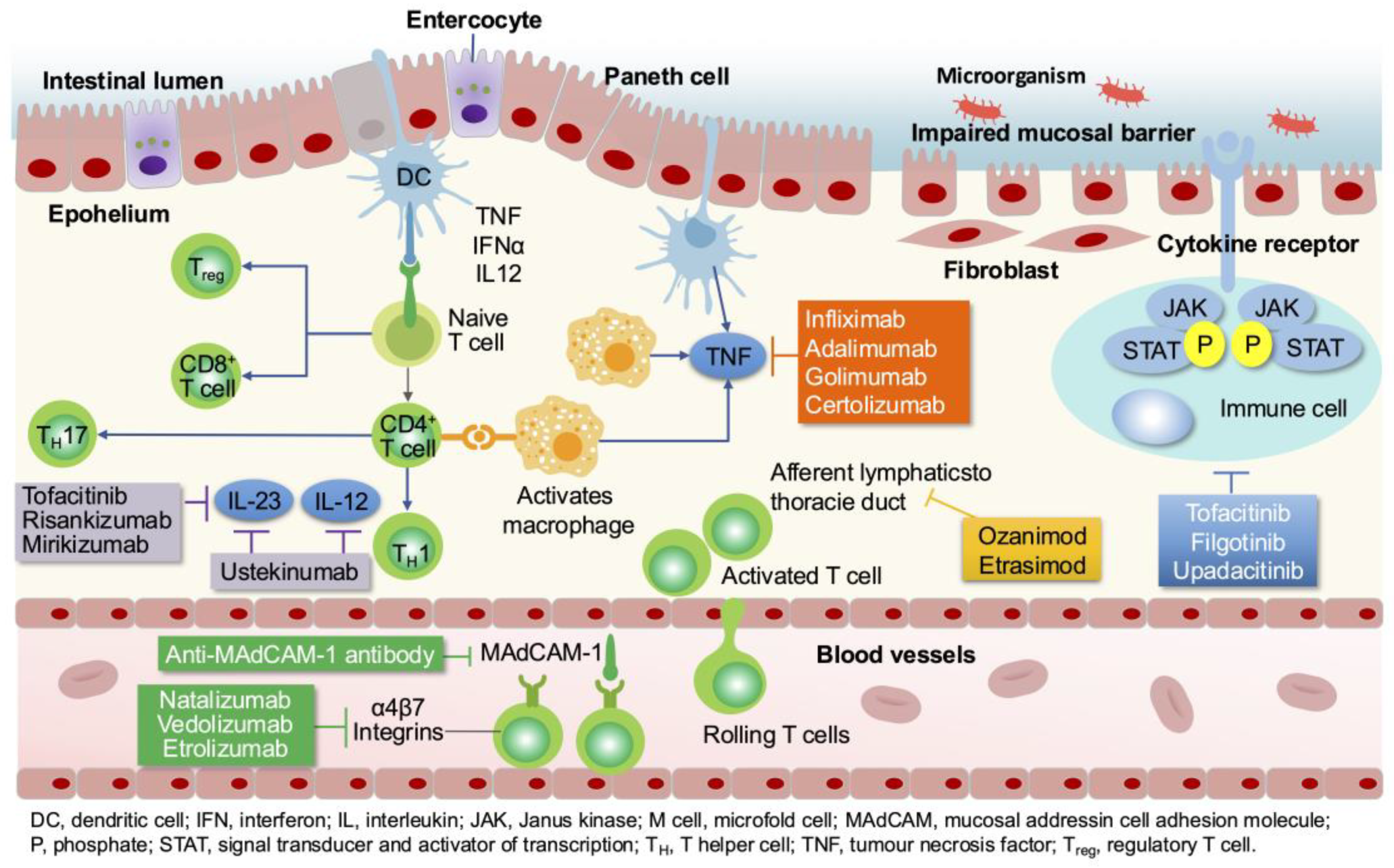
Figure 8.
Summary treatment strategy adjustment of anti-TNF-α drugs.
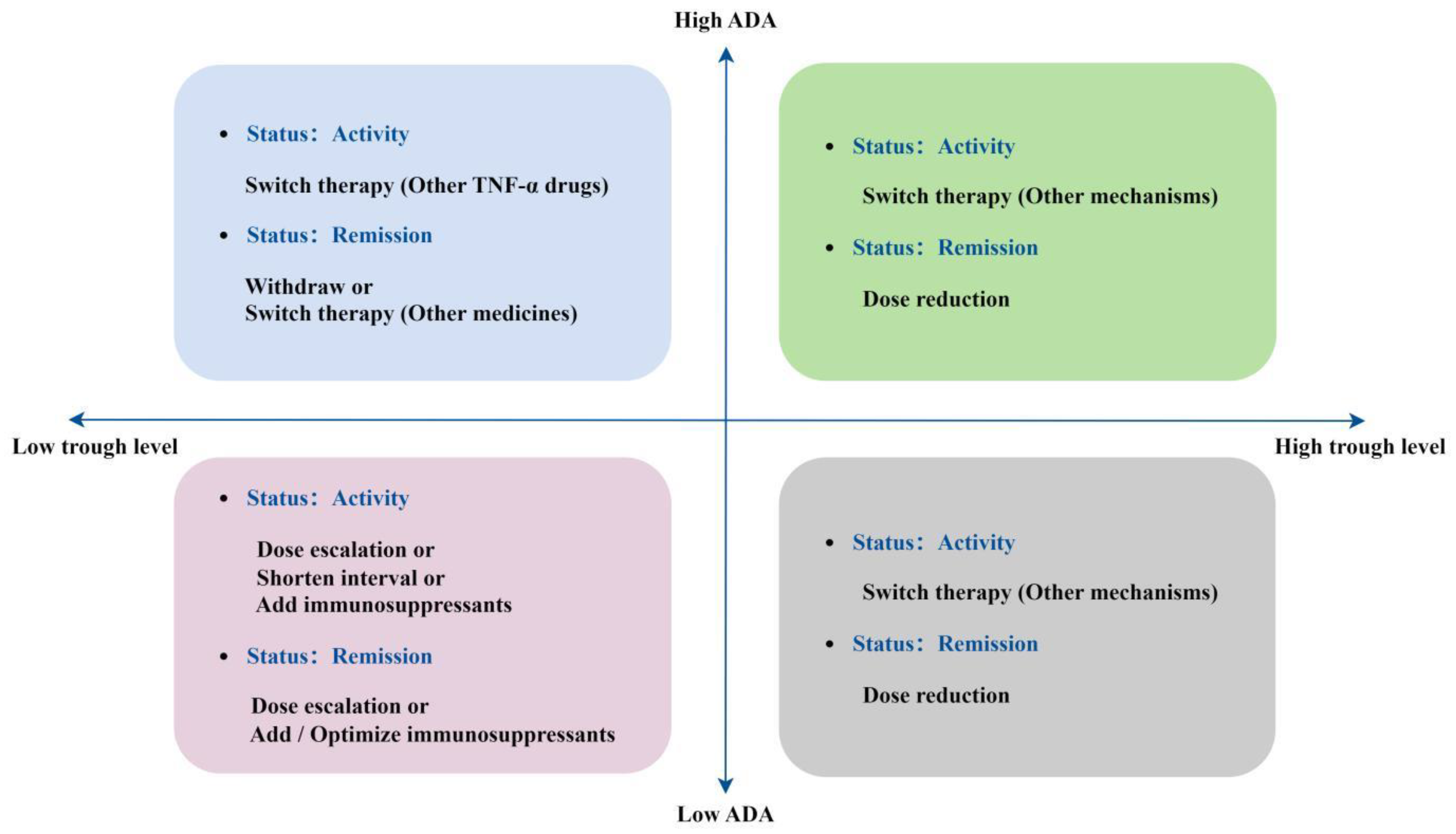
Table 1.
The top 10 journals that published the most articles.
| Rank | Source | Count (Percentage) |
Citations(n) |
|---|---|---|---|
| 1 | Inflammatory Bowel Diseases | 579 (9.14%) | 13632 |
| 2 | Journal of Crohns & Colitis | 480 (7.57%) | 17553 |
| 3 | Alimentary Pharmacology & Therapeutics | 250 (3.95%) | 9681 |
| 4 | Clinical Gastroenterology and Hepatology | 178 (2.81%) | 9260 |
| 5 | Digestive Diseases and Sciences | 177 (2.79%) | 2202 |
| 6 | Journal of Pediatric Gastroenterology and Nutrition | 159 (2.51%) | 2168 |
| 7 | Scandinavian Journal of Gastroenterology | 145 (2.29%) | 1855 |
| 8 | Digestive and Liver Disease | 126 (1.99%) | 1916 |
| 9 | World Journal of Gastroenterology | 117 (1.85%) | 2439 |
| 10 | European Journal of Gastroenterology & Hepatology | 115 (1.81%) | 1189 |
Table 2.
The top 10 highest cited articles.
| Rank | Title | Journal | Citations | PY | Doi |
|---|---|---|---|---|---|
| 1 | 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management | J Crohns Colitis | 1386 | 2017 | 10.1093/ecco-jcc/jjw168 |
| 2 | Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease | N Engl J Med | 1194 | 2016 | 10.1056/NEJMoa1602773 |
| 3 | Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis | N Engl J Med | 1121 | 2017 | 10.1056/NEJMc1707500 |
| 4 | ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment | J Crohns Colitis | 785 | 2020 | 10.1093/ecco-jcc/jjz180 |
| 5 | European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa | J Eur Acad Dermatol Venereol | 758 | 2015 | 10.1111/jdv.12966 |
| 6 | Consensus guidelines of ECCO/ESPGHAN on the medical management of pediatric Crohn’s disease | J Crohns Colitis | 737 | 2014 | 10.1016/j.crohns.2014.04.005 |
| 7 | Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn’s disease: a phase 3 randomised, double-blind controlled trial | Lancet | 706 | 2016 | 10.1016/S0140-6736(16)31203-X |
| 8 | Ustekinumab as Induction and Maintenance Therapy for Ulcerative Colitis | N Engl J Med | 702 | 2019 | 10.1056/NEJMoa1900750 |
| 9 | Combination Therapy With Infliximab and Azathioprine Is Superior to Monotherapy With Either Agent in Ulcerative Colitis | Gastroenterology | 677 | 2014 | 10.1053/j.gastro.2013.10.052 |
| 10 | Through Concentrations of Infliximab Guide Dosing for Patients With Inflammatory Bowel Disease | Gastroenterology | 667 | 2015 | 10.1053/j.gastro.2015.02.031 |
Table 3.
The top 10 most co-cited references.
| Rank | Year | Journal | Title | Citations | Doi |
|---|---|---|---|---|---|
| 1 | 2005 | N Engl J Med | Infliximab for induction and maintenance therapy for ulcerative colitis | 817 | 10.1056/nejmoa050516 |
| 2 | 2002 | Lancet | Maintenance infliximab for Crohn’s disease: the ACCENT I randomized trial | 801 | 10.1016/s0140-6736(02)08512-4 |
| 3 | 2010 | N Engl J Med | Infliximab, azathioprine, or combination therapy for Crohn’s disease | 785 | 10.1056/nejmoa0904492 |
| 4 | 2013 | N Engl J Med | Vedolizumab as induction and maintenance therapy for ulcerative colitis | 644 | 10.1056/nejmoa1215734 |
| 5 | 2013 | N Engl J Med | Vedolizumab as induction and maintenance therapy for Crohn’s disease | 596 | 10.1056/nejmoa1215739 |
| 6 | 2016 | Gastroenterology | Adalimumab for maintenance of clinical response and remission in patients with Crohn’s disease: the CHARM trial | 510 | 10.1053/j.gastro.2006.11.041 |
| 7 | 2016 | N Engl J Med | Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease | 437 | 10.1056/nejmoa1602773 |
| 8 | 2011 | Gastroenterology | Adalimumab induces and maintains clinical remission in patients with moderate-to-severe ulcerative colitis | 361 | 10.1053/j.gastro.2011.10.032 |
| 9 | 2005 | Gut | The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications | 357 | 10.1136/gut.2005.082909 |
| 10 | 1987 | N Engl J Med | Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study | 349 | 10.1056/nejm198712243172603 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



