Submitted:
17 January 2025
Posted:
17 January 2025
You are already at the latest version
Abstract
Patient nonadherence to drug usage is a major barrier to treating Tuberculosis (TB). Telemedicine has shown promise in treatment monitoring and evaluation. This paper aims to explore scientific evidence of telemedicine application in TB treatment to promote widespread adoption in areas that are remote, or with poor road networks from health facilities. Articles published from 2010 to 2023 on the adherence and outcomes in pulmonary tuberculosis with the use of telemedicine were reviewed. A scoping review of the studies was conducted by two authors independently, following the PRISMA guidelines to identify relevant articles. Telemedicine interventions have shown improvements in medication adherence, treatment completion, cure rates, and smear conversion among TB patients. The available evidence supports the beneficial effect of telemedicine in improving treatment adherence and outcomes in patients with pulmonary tuberculosis. However, the effect and outcomes varied across studies, indicating the need for further research and standardization of telemedicine interventions.
Keywords:
Treatment Adherence
; Outcomes
; Pulmonary tuberculosis
; Telemedicine
; Scoping review
; poor resource setting
1. Introduction
Globally, tuberculosis (TB) is a major communicable disease affecting millions of persons, and according to the World Health Organization (WHO) statistics, it is ranked among the first 10 causes of mortality globally with about 10 million cases yearly and about 1.4 million TB-related deaths in 2019.[1] A combination of antibiotics is used in treating TB over the course of a minimum period of 6 to 9 months. Directly Observed Treatment Short-course (DOTS) has been the standard treatment protocol, which involves the supervised administration of medications to ensure adherence.[1] However, this method, though strong among the other interventional strategies, has not proved efficient in the control of TB with the emergence of drug-resistant tuberculosis, including extensively drug-resistant (XDR) and multidrug-resistant (MDR) strains.[2]
Various strategies have been implemented globally to combat the spread of tuberculosis. WHO's End TB Strategy seeks to reduce TB fatalities, incidence, and out-of-pocket expenses associated with TB care by 2035.[3] The strategy emphasizes early diagnosis and treatment, expanding access to quality care, and confronting the social determinants of tuberculosis. Treatment adherence is a major obstacle to TB management because patients typically find the 6-month medication regimen too onerous, resulting in either delayed treatment beginning, treatment interruption, or treatment discontinuation (treatment default).[4] Each year, nonadherence increases the number of infectious days, heightens the risk of relapse, and contributes to the development of drug-resistant tuberculosis.[5]
Significant implementation obstacles exist for conventional directly observed therapy.[4] Adherence incurs ongoing non-monetary costs for patients and their families, even when TB medications themselves are free.[6] These costs include physical side effects, lost productivity, transportation expenses, social stigma, and a possible affront to patients' autonomy.[7] One enduring challenge is the fact that supervision and assistance often must be provided face-to-face; this is especially problematic in low-resource areas, where patients may be geographically dispersed and difficult to access.
Numerous adherence-enhancement solutions based on DOT have been explored to solve these issues. Reminder systems, defaulter action, education, and peer support are all examples of interventions that try to improve adherence but do not address the underlying motivation issue, with varying degrees of success.[8],[9] However, studies of monetary incentives reveal that patients who get material benefits are much more likely to complete TB treatment,[7] although these results were mostly found in wealthy nation settings.
Technology would play a crucial role in achieving the WHO’s objective of eradicating TB by 2035. Advanced diagnostic tools, treatment monitoring systems, data management solutions, telemedicine, and research innovations are crucial elements in the fight against TB. Harnessing the power of technology can improve TB detection, treatment outcomes, data-driven decision-making, and healthcare access, ultimately contributing to the goal of TB elimination. In achieving the objective of WHO, telemedicine could be at the forefront of leading the battle against TB.
In the context of this work, telemedicine is defined as using telecommunications technologies to support all kinds of medical treatment-related services in the management of PTB.[10] Telemedicine holds great promise for the treatment of TB.[11] It offers opportunities for remote consultations and expert advice, particularly in areas with limited access to specialized healthcare providers. Through videoconferencing and teleconsultation platforms, healthcare professionals can extend their expertise, support diagnosis, and guide TB management.[12] Telemedicine can help address the shortage of skilled healthcare workers and improve access to quality TB care in underserved regions.
Telemedicine allows healthcare providers to conduct remote consultations with TB patients, enabling access to specialized care even in areas with limited healthcare resources.[13] This approach is effective in improving patient outcomes and reducing the burden on healthcare facilities. By leveraging videoconferencing and digital platforms, telemedicine facilitates timely diagnosis, treatment monitoring, and adherence support for TB patients. Directly Observed Treatment (DOT) involves in-person observation of medication intake. However, telemedicine can enable remote DOT, where healthcare providers can visually verify patients' medication adherence through video calls or electronic pillboxes.[14] Remote DOT has shown promising results in improving treatment adherence and reducing costs associated with in-person visits. Through teleconsultation, healthcare professionals can discuss complex cases, receive recommendations for treatment adjustments, and access up-to-date medical knowledge.[15] This approach improves patient convenience, reduces healthcare costs, and allows for efficient allocation of resources.[16]
DiStefano and Schmidt[17] presented a framework to support the ethical planning, implementation, and evaluation of mobile health (mHealth) interventions for tuberculosis (TB) treatment adherence. They emphasized the potential of mHealth interventions, including mobile phone-based technologies, in improving TB treatment adherence. However, they also highlighted the importance of considering ethical implications throughout the development and implementation process. This review, therefore, aims to scope the existing literature on the adherence and treatment outcomes of pulmonary tuberculosis and latent TB patients treated through telemedicine.
2. Methodology
Literature searches were performed in relevant databases for studies assessing the impact of telemedicine DOT on treatment adherence and outcomes in latent TB in pulmonary TB patients. The telecommunication technologies specifically include VDOT, test messages, and reminders.
2.1. Inclusion Criteria:
- Articles published between 2010 and 2023.
- Full articles
- Articles on treatment adherence or outcome of PTB with the use of telemedicine.
- Articles published in the English language.
2.2. Exclusion Criteria:
- Only abstracts available.
- Articles outside the range of search
2.3. Search strategy and selection criteria
Using the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines,[18] data for this review were identified by searches of PubMed, and Google Scholar, from 2010 to 2023. The search terms include: “tuberculosis”, “treatment”, “outcome”, “medication adherence”, “treatment adherence”, “telemedicine”, “TB”, “tuberculosis patients”, “directly observed therapy”, “DOTs”, and “video DOTs”.
2.4. Data extraction, critical appraisal, and synthesis
There were 14,500 articles downloaded using the various online databases. The articles were independently reviewed by two authors. After the removal of duplicates and other irrelevant articles and abstracts, 374 articles were left. Emphasis was on telemedicine and pulmonary tuberculosis treatment adherence and outcomes. Therefore, all articles on other aspects of telemedicine and tuberculosis were excluded. Fifteen articles were left and eventually used for the scoping review. Data were extracted under the following headings: author, the year of publication, study location, sample size, intervention, and results/ findings.
3. Results
The studies highlighted here, as shown in Table 1, were reviewed for the effectiveness of telemedicine in the treatment of pulmonary tuberculosis. There were 12 Randomized Controlled Trial studies, 2 pilot studies, and only 1 retrospective study. Six studies utilized Video Directly Observed Therapy (VDOT), 3 studies used Text Message Reminders (TMR), while the remaining studies used other telemedicine-based interventions including combined VDOT and TMR, TMR and voice calls as reminders to monitor patients’ adherence.
The study conducted by Garfein et al.[19] showed that among the 27 patients who completed the study, 96% of observed therapy sessions were recorded and successfully transmitted. Burzynski et al.[20] demonstrated that electronic DOT was non-inferior to in-person DOT in terms of the percentage of completed doses. The study conducted by DeMaio et al.[21] demonstrated that telemedicine has the potential to enhance TB care by improving treatment adherence and patient satisfaction while reducing healthcare costs and logistical challenges associated with in-person observation.
Guo et al.[22] found high rates of treatment completion in both the VDOT and DOT groups, with no statistical differences between the two methods. Despite that, VDOT was associated with a significantly shorter time per observed dose compared to DOT, as well as lower costs. In India, Holzman et al.[23] (2019) suggested that vDOT is a feasible and acceptable method for TB treatment monitoring.
Manyasewal et al.[24] suggested that medication event reminder and monitor-observed therapy can improve health-related quality of life and reduce catastrophic costs in patients with TB compared to standard DOT. In a study conducted by Chuck et al.[25], treatment completion with VDOT was similar to that of in-person DOT but adherence to scheduled VDOT sessions was better compared with in-person DOT. Lam et al.[26] observed that treatment adherence was found to be high for patients with latent tuberculosis infection on 3-month Isoniazid and Rifapentine, with participants reporting an average adherence rate of 96% across the treatment period. Browne et al.[27] did not record any significant difference in adherence between the wirelessly observed therapy and DOT groups, with 85.5% and 82.8% of participants completing their treatment, respectively. Clinical response and adverse events did not differ significantly between the groups.
Liu et al.[28] concluded in their study that electronic reminders, such as SMS text messages or phone calls, were effective in improving medication adherence and treatment completion rates among TB patients. Chen et al.[29] concluded that using synchronous video-observed treatment (SVOT) as a method for medication adherence in LTBI patients provided an advantage in privacy protection while improving treatment adherence and completion rates. Mohammed et al.[30] concluded in their study that implementing a daily SMS medication reminder system significantly improved treatment outcomes for patients with TB. The use of SMS reminders increased treatment success, adherence, and patient engagement, thereby contributing to better TB treatment outcomes through its cost-effectiveness.
Farooqi et al.[31] concluded that mobile SMS reminders can play a significant role in improving medication compliance among patients receiving anti-TB treatment through the DOTS program. The use of SMS reminders proved to be an effective and feasible intervention in promoting adherence to the prescribed medication regimen, leading to higher treatment completion rates and improved treatment outcomes in TB patients. Guo et al.[32] (2020) concluded that the comprehensive app utilizing video-observed therapy for TB treatment management was well-received by the participants and demonstrated good usability. Belknap et al.[33] study concluded that self-administered once-weekly isoniazid and rifapentine treatment for LTBI was superior to DOT in terms of treatment completion. Johnston et al.[34] demonstrated that text message reminders significantly improved adherence to treatment for LTBI.
Figure 1.
PRISMA flowchart of study selection.
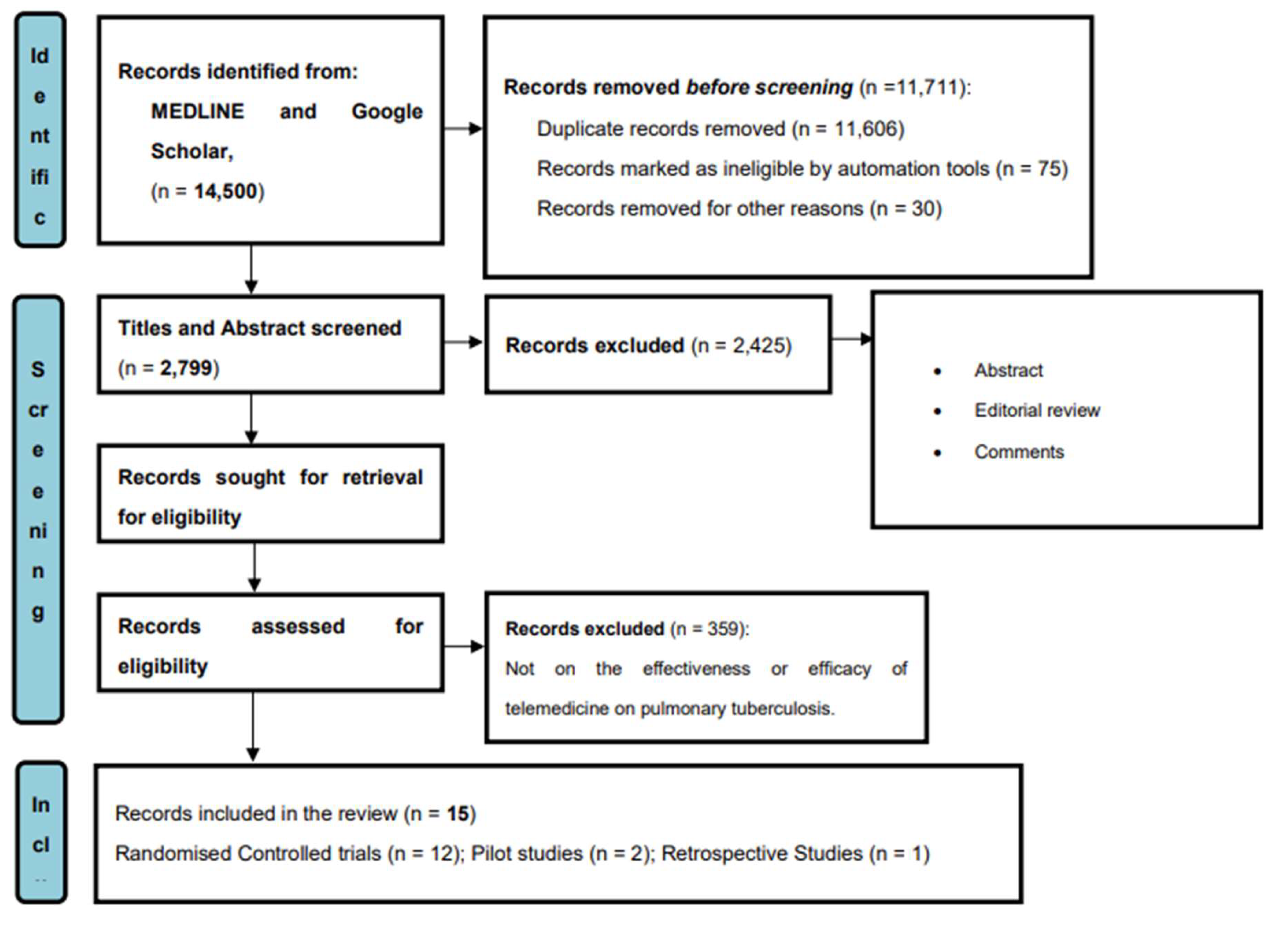

Table 1.
Summary of the treatment outcomes of pulmonary tuberculosis patients treated with telemedicine.
Table 1.
Summary of the treatment outcomes of pulmonary tuberculosis patients treated with telemedicine.
| SN | Author/ year/ Country |
Title | Goal/objective | Methodology | Sample size | Intervention | Result/findings |
|---|---|---|---|---|---|---|---|
| 1. | Lam et al.[26] (2018) USA |
“Using video technology to increase treatment completion for patients with latent tuberculosis infection on 3-month isoniazid and rifapentine: an implementation study” | Assessing the use of video technology on improving completion of treatment in patients undergoing a 3-month rifapentine and isoniazid regimen for latent tuberculosis infection (LTBI) | Randomized Controlled Trial | 116 | Scheduled VDOT session | Use of VDOT significantly improved treatment completion rates compared to historical controls |
| 2. | Burzvnski et al.[20] (2022) USA |
“In-person vs electronic directly observed therapy for tuberculosis treatment Adherence: A Randomized Noninferiority” | To determine if electronic directly observed therapy (DOT) for monitoring tuberculosis treatment can achieve a comparable treatment level to in-person DOT. | Randomized Crossover | 216 | Monitoring treatment of tuberculosis with electronic directly observed therapy (DOT) | This trial demonstrated that electronic DOT was non-inferior to in-person DOT in terms of the percentage of completed doses |
| 3. | DeMaio et al.[21] (2001) | “The application of telemedicine technology to a directly observed therapy program for tuberculosis: A pilot project” | To evaluate the feasibility and acceptability of using telemedicine technology programmed for tuberculosis (TB) in a directly observed therapy (DOT) | Pilot study | 23 | Video-conferencing equipment that allowed healthcare providers to remotely observe and monitor TB patients | Eighty -seven percent of the patients stated a positive experience with telemedicine and expressed satisfaction with the convenience and privacy it provided. The telemedicine-based DOT program demonstrated high adherence rates, with 91% of observed doses completed. |
| 4. | Garfein et al.[35] (2018) USA |
“Tuberculosis treatment monitoring by video directly observed therapy in 5 health districts, California, USA” | Examines the implementation and effectiveness of video directly observed therapy (VDOT) in five health districts in California, USA for monitoring tuberculosis (TB) treatment. | Retrospective Study | 467 | Video directly observed therapy (VDOT) | VDOT was particularly effective in improving treatment adherence among specific patient groups, including those with substance use disorders, homeless individuals, and patients with previous treatment non-adherence |
| 5. | Guo et al.[32] (2020) | “A comprehensive app that improves tuberculosis treatment management through video-observed therapy: usability study” | To evaluate the cost and clinical benefits of video-directly observed therapy (VDOT) in comparison to traditional directly observed therapy (DOT) for tuberculosis (TB) treatment. | Randomized Controlled Trial | 405 | Video directly observed therapy (VDOT) | High rates of treatment completion in both the VDOT and DOT groups, with no statistical differences between the two methods. VDOT was associated with a significantly shorter time per observed dose compared to DOT, as well as lower costs. Patients in the VDOT group reported better experiences and higher levels of satisfaction compared to those in the DOT group. They found VDOT to be convenient, and comfortable and expressed a willingness to recommend the method to other patients. |
| 6. | Holzman et al.[23] (2019) India |
“Use of smartphone-based video directly observed therapy (vDOT) in tuberculosis care: a single-arm, prospective feasibility study” | To assess its feasibility and acceptability for TB treatment monitoring | Pilot Study | 25 | Video-directly observed therapy (vDOT) | More than 90% of patients find it easy to make and upload videos. These findings suggest that vDOT is an acceptable and feasible method for the monitoring of TB treatment in India, expanding the evidence base for vDOT in resource-limited settings and firstly documenting the use of vDOT in India. |
| 7. | Manyasewal et al.[24] (2022) Ethiopia |
“Effect of digital medication event reminder and monitor-observed therapy vs standard directly observed therapy on health-related quality of life and catastrophic costs in patients with tuberculosis: A secondary analysis of a randomized clinical Trial” | Investigating the impact of a digital medication event reminder monitor (MERM)-observed therapy compared to traditional directly observed therapy (DOT) on catastrophic costs and health-related quality of life (HRQoL) in patients with tuberculosis (TB) in a resource-constrained setting | Randomized Clinical Trial | 109 | Digital medication event reminder monitor (MERM) | The median index value for EQ-5D-5L and HRQoL was significantly higher in the MERM-observed therapy group compared to the control group. Additionally, the intervention group had significantly lower median costs compared to the control group, resulting in potential cost savings. |
| 8. | Chuck et al.[25] (2016) USA |
“Enhancing Management of Tuberculosis Treatment with Video Directly Observed Therapy in New York City” | To evaluate the effectiveness of video-directly observed therapy (VDOT) in improving treatment outcomes for tuberculosis (TB) patients in New York City | Randomized Controlled Trial | 201 | Video directly observed therapy (VDOT) | High levels of satisfaction were reported by patients in the VDOT group with the technology and found it to be convenient and user-friendly. Healthcare providers also reported positive experiences with the VDOT system, finding it to be an effective tool for monitoring patients' medication adherence |
| 9. | Browne et al.[27] (2019) | “Wirelessly Observed Therapy Compared to Directly Observed Therapy to Confirm and Support Tuberculosis Treatment Adherence” | To compare wirelessly observed therapy (WOT) with directly observed therapy (DOT) in confirming and supporting adherence to tuberculosis (TB) treatment | Randomized Controlled Trial | 175 | Smartphone that was equipped with a video-based adherence system | Both WOT and DOT groups had high levels of treatment adherence, with mean adherence rates of 90.7% and 90.6%, respectively. There was no significant difference in adherence between the two groups. Treatment completion rates were also similar between the WOT and DOT groups, with 85.5% and 82.8% of participants completing their treatment, respectively. Clinical response and adverse events did not differ significantly between the groups. |
| 10. | Liu et al.[28] (2015) China |
“Effectiveness of Electronic Reminders to Improve Medication Adherence in Tuberculosis Patients” | To estimate the effectiveness of electronic reminders in improving medication adherence among tuberculosis (TB) patients. | Randomized Controlled Trial | 4,173 | Patients received electronic reminders in the form of phone calls or texts in short message service (SMS) | The intervention group, receiving electronic reminders, had a higher significance in treatment completion rate when compared to the normal control |
| 11. | Chen et al.[29] (2020) | “Advantage in privacy protection by using synchronous video observed treatment enhances treatment adherence among patients with latent tuberculosis infection” | To investigate the impact of synchronous video-observed treatment (SVOT) on adherence to treatment among latent tuberculosis infection (LTBI) patients. | Randomized Controlled Trial | 200 | Video call application to connect with healthcare providers | The SVOT group had significantly higher treatment adherence (98.2%) compared to the SAT group (89.0%). Furthermore, group SVOT had a higher treatment completion rate (92.0%) compared to the SAT group (81.0%). Patient satisfaction was also higher in the SVOT group, with 96.0% of participants expressing satisfaction with the SVOT intervention. |
| 12. | Mohammed et al.[30] (2016) | “Impact of a daily SMS medication reminder system on tuberculosis treatment outcomes” | To assess how effective a daily SMS medication reminder would improve treatment outcomes in tuberculosis (TB) patients | Randomized Controlled Trial | 200 | Daily SMS reminders | The intervention group had higher significance in treatment success (92.0%) and treatment adherence, with 94.0% of participants reporting good adherence when compared to patients in the control group with 78.0% and 79.0%, respectively. Additionally, the intervention group had a lower treatment failure rate and a lower loss to follow-up rate compared to the control group |
| 13. | Farooqi et al.[31] (2017) | “The role of mobile SMS-reminders in improving drug compliance in patients receiving anti-TB treatment from DOTS Program” | To assess the effectiveness of mobile SMS reminders in improving medication compliance among patients receiving anti-tuberculosis (TB) treatment through the Directly Observed Treatment Short-course (DOTS) program |
Randomized Controlled Trial | 300 | Mobile SMS reminders | The intervention group had significantly higher medication compliance when compared to patients in the control group. A lower proportion of missed doses was observed in the intervention group, indicating better adherence to the regime of prescribed medication. Furthermore, a higher treatment success rate and treatment completion rate were recorded in the intervention compared to the control group. Patient satisfaction with the SMS reminder system was also reported to be high |
| 14. | Johnston et al.[34] (2018) | “The effect of text messaging on latent tuberculosis treatment adherence: a randomized controlled trial” | To investigate the influence of text messaging on adherence to treatment for latent tuberculosis infection (LTBI). | Randomized Controlled Trial | 133 | Text Message Reminders | The group that received text messages had significantly higher adherence to LTBI treatment compared to the standard care group. Adherence rates were 87.5% in the text message group and 75.0% in the standard care group. The text message intervention also resulted in a higher treatment completion rate (92.3% vs. 81.3%) and greater participant satisfaction. When the occurrence of adverse events between the two groups was observed, there were no significant differences indicating that text messaging did not pose any additional risks |
| 15. | Guo et al. [22] 2020 |
Telemedicine Technologies and Tuberculosis Management: A Randomized Controlled Trial |
To assess the clinical and cost-benefit of video directly observed therapy (VDOT), compared with DOT service. | Randomized controlled trial | 405 participants from each study arm | Video directly observed therapy (VDOT) | VDOT enabled meaningful direct observation for TB patients through mobile devices, which was highly acceptable to patients and health care providers. It also saved time and is a cost-effective method, enabling the use of the saved money to other much-needed areas for TB. |
4. Discussion
A variety of studies were identified, with different designs, settings, and populations, which all focused on telemedicine DOT's impact on sputum conversion rates in pulmonary TB patients. While the exact interventions varied, all used some form of remote monitoring or video communication to observe patients’ medication intake. In this review, 15 studies published between 2010 and 2023 were examined. Most of the studies were conducted in developed nations. Very few studies on the treatment of tuberculosis with telemedicine in clinical trials were carried out in Africa where the prevalence of pulmonary TB is highest.[36] The treatment outcome of the studies indicated that there was a high adherence rate, and dose completion, with telemedicine being convenient and user-friendly, comfortable, cost-effective, and efficient in improving TB control outcomes. Most of the patients who used one or other form of telemedicine expressed their willingness to recommend the method to other patients.[37]
Most of the studies showed a significant difference in the outcome between VDOT and standard DOT in favor of VDOT. However, Guo et al.[32] used video-directly observed therapy (VDOT), Browne et al.[27] adopted a smartphone that was equipped with a video-based adherence system and Burzynski et al.[20] used electronic directly observed therapy (DOT) for monitoring tuberculosis treatment. They did not observe any significant difference in their studies. Despite this, they all agreed to the fact that VDOT was associated with a significantly shorter time per observed dose compared to DOT, as well as lower costs. Patients in the VDOT group reported better experiences and higher levels of satisfaction compared to those in the DOT group.
Most studies reported improved sputum conversion rates with the use of telemedicine DOT, indicating improved treatment effectiveness. However, inconsistencies between studies, including differing interventions, populations, and study designs, limit the ability to draw definitive conclusions. The importance of factors such as patient comfort with technology, privacy concerns, and technical support was also frequently noted.
5. Conclusion
The evidence synthesized from the reviewed studies underscores the effectiveness of telemedicine in improving treatment adherence and outcomes among patients with pulmonary tuberculosis (PTB). The diverse interventions, ranging from Video Directly Observed Therapy (VDOT) to Text Message Reminders (TMR), have demonstrated promising results in enhancing medication adherence, facilitating real-time monitoring, and providing personalized care for TB patients. Despite variations in study designs, settings, and populations, the consistent findings point towards the potential of telemedicine to address the challenges of patient nonadherence and treatment discontinuation, which have long been barriers to effective TB management. Moreover, telemedicine offers a convenient, accessible, and cost-effective approach to supporting patients in remote or underserved areas, bridging gaps in healthcare access and delivery.
However, it is important to acknowledge the limitations and gaps in the existing literature, including the predominance of studies conducted in developed nations and the scarcity of robust trials in resource-constrained settings, particularly in Africa. Future research should aim to address these disparities and generate more evidence on the scalability, feasibility, and sustainability of telemedicine interventions in diverse healthcare contexts. Moving forward, clear guidelines and protocols are needed to standardize telemedicine practices in TB treatment, ensuring ethical considerations, patient privacy, and data security. Additionally, investments in healthcare infrastructure, internet connectivity, and digital literacy are essential to enable widespread telemedicine adoption and maximize its potential impact on TB control efforts.
Overall, telemedicine represents a promising tool in the fight against tuberculosis, offering innovative solutions to enhance treatment adherence, improve patient outcomes, and ultimately contribute to the global goal of TB elimination by 2035. Through continued research, collaboration, and investment, telemedicine can play a pivotal role in shaping the future of TB care delivery and advancing towards a TB-free world.
6. Limitation of the review
While the strength of the review lies in its comprehensive examination of the existing literature on telemedicine's application in tuberculosis (TB) treatment, providing valuable insights into the effectiveness of various telemedicine interventions, the review also has some limitations that warrant consideration. Understanding and addressing these limitations are crucial for interpreting the findings accurately and guiding future research efforts aimed at optimizing telemedicine strategies for TB management.
- Geographical Bias: The majority of the studies included in this review were conducted in developed nations, leading to potential geographical bias. Limited representation from resource-constrained settings, particularly in Africa and other low-income regions, may restrict the generalizability of findings to diverse healthcare contexts.
- Study Design Variability: The studies encompassed a variety of designs, including Randomized Controlled Trials (RCTs), pilot studies, and retrospective analyses. While each design offers unique insights, the variability in methodologies makes it challenging to directly compare findings and draw definitive conclusions.
- Population Heterogeneity: The patient populations across the reviewed studies exhibited considerable heterogeneity in terms of demographic characteristics, TB severity, comorbidities, and socioeconomic status. This heterogeneity may introduce confounding variables that could influence treatment outcomes and adherence rates.
- Intervention Diversity: The telemedicine interventions evaluated in the studies varied widely, encompassing Video Directly Observed Therapy (VDOT), Text Message Reminders (TMR), and other telecommunication technologies. While this diversity reflects the evolving landscape of telemedicine, it also complicates the synthesis of results and limits the ability to identify optimal intervention strategies.
- Limited Longitudinal Data: Many of the reviewed studies provided short-term outcomes, such as treatment completion rates and adherence metrics. Longitudinal data on sustained treatment outcomes, relapse rates, and long-term patient follow-up were often lacking, limiting the assessment of telemedicine's durability and effectiveness over time.
7. Recommendation
- Clear guidelines and protocols need to be developed and implemented to ensure standardized and effective telemedicine practices in TB treatment. These guidelines should address issues such as patient selection criteria for telemedicine, data privacy, and security measures, and ethical considerations specific to telemedicine practice.
- Healthcare professionals, including nurses, should receive comprehensive training on telemedicine technologies, platforms, and best practices. Continued professional development opportunities and training programs should also be provided to ensure healthcare professionals remain updated on evolving telemedicine practices.
- Expanding internet access and ensuring reliable connectivity in remote regions will enable effective telemedicine implementation and bridge the digital divide, ensuring equal access to TB care, most especially in developing countries.
- Further research is needed to evaluate the long-term impact and effectiveness of telemedicine in TB treatment. Studies should focus on outcomes such as treatment adherence, treatment success rates, cost-effectiveness, patient satisfaction, and healthcare provider experiences. The findings from such studies will provide valuable insights and evidence to guide future telemedicine interventions and inform policy decisions.
- Collaboration among healthcare institutions, professional associations, and researchers is crucial for sharing best practices and experiences related to telemedicine in TB treatment.
- Efforts should be made to ensure equitable access to telemedicine services for all TB patients with special attention to vulnerable populations, such as those in rural or underserved areas, individuals with low socioeconomic status, and marginalized communities. Strategies like subsidized internet access or mobile data plans can help address access barriers and ensure inclusivity.
References
- Organization. WH. (2020). Global Tuberculosis Report 2020. Geneva: World Health Organization.
- https://www.who.int/publications/i/item/9789240013131. Global Tuberculosis Report 2020.
- https://www.who.int/teams/global-tuberculosis-programme/the-end-tb-strategy. Global Tuberculosis Programme.
- Adejumo OA, Daniel OJ, Otesanya AF, Salisu-Olatunj SO, Abdur-Razzaq HA. Evaluation of outcomes of tuberculosis management in private for profit and private-not-for profit directly observed treatment short course facilities in Lagos State, Nigeria. Nigerian Medical Journal: Journal of the Nigeria Medical Association. 2017, 58, 44. [Google Scholar] [CrossRef]
- Atif M, Anwar Z, Fatima RK, Malik I, Asghar S, Scahill S. Analysis of tuberculosis treatment outcomes among pulmonary tuberculosis patients in Bahawalpur, Pakistan. BMC Research Notes.
- Rabinovich L, Molton JS, Ooi WT, Paton NI, Batra S, Yoong J. Perceptions and Acceptability of Digital Interventions Among Tuberculosis Patients in Cambodia: Qualitative Study of Video-Based Directly Observed Therapy. J Med Internet Res. 2020, 22, e16856. [Google Scholar] [CrossRef]
- Abdulkader M, van Aken I, Niguse S, Hailekiros H, Spigt M. Treatment outcomes and their trend among tuberculosis patients treated at peripheral health settings of Northern Ethiopia between 2009 and 2014: a registry-based retrospective analysis. BMC Res Notes. 2019, 12, 786. [Google Scholar] [CrossRef]
- Tola A, Minshore KM, Ayele Y, Mekuria AN. Tuberculosis treatment outcomes and associated factors among TB patients attending public hospitals in Harar town, Eastern Ethiopia: a five-year retrospective study. Tuberculosis Research and Treatment, 2019.
- Adejumo OA, Daniel OJ, Adepoju VA, Femi-Adebayo T, Adebayo BI, Airauhi AO. Challenges of tuberculosis control in Lagos state, Nigeria: a qualitative study of health-care Providers' perspectives. Nigerian Medical Journal: Journal of the Nigeria Medical Association. 2020, 61, 37. [Google Scholar] [CrossRef]
- https://www.fcc.gov/general/telehealth-telemedicine-and-telecare-whats-what. Telehealth, Telemedicine, and Telecare: What's What? Assessed 9 May 2024;
- Parajuli R, Doneys P. Exploring the role of telemedicine in improving access to healthcare services by women and girls in rural Nepal. Telematics and Informatics. 2017, 34, 1166–1176. [Google Scholar] [CrossRef]
- Brauchli, K. Telemedicine for improving access to health care in resource-constrained areas: from individual diagnosis to strengthening health systems. University_of_Basel; 2006.
- Haleem A, Javaid M, Singh RP, Suman R. Telemedicine for healthcare: Capabilities, features, barriers, and applications. Sensors International, 1001.
- Mustopa R, Damris D, Syamsurizal S, Emawati M. Evaluation of M-Health On Medication Adherence In Tuberculosis Patients: A Systematic Review. Evaluation. 2023, 3, 1–29. [Google Scholar]
- Eisenstein E, Kopacek C, Cavalcante SS, Neves AC, Fraga GP, Messina LA. Telemedicine: a bridge over knowledge gaps in healthcare. Current Pediatrics Reports.
- O'Cathail M, Sivanandan MA, Diver C, Patel P, Christian J. The use of patient-facing teleconsultations in the national health service: scoping review. JMIR Medical Informatics. 2020, 8, e15380. [Google Scholar] [CrossRef] [PubMed]
- DiStefano MJ, Schmidt H. mHealth for tuberculosis treatment adherence: a framework to guide ethical planning, implementation, and evaluation. Global Health: Science and Practice. 2016, 4, 211–221. [Google Scholar]
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Garfein RS, Collins K, Muñoz F, et al. Feasibility of tuberculosis treatment monitoring by video directly observed therapy: a binational pilot study. The International Journal of Tuberculosis and Lung Disease. 2015, 19, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Burzynski J, Mangan JM, Lam CK, et al. In-person vs electronic directly observed therapy for tuberculosis treatment adherence: A randomized noninferiority trial. JAMA Network Open. 2022, 5, e2144210–e2144210. [Google Scholar] [CrossRef] [PubMed]
- DeMaio J, Schwartz L, Cooley P, Tice A. The application of telemedicine technology to a directly observed therapy program for tuberculosis: a pilot project. Clinical Infectious Diseases. 2001, 33, 2082–2084. [Google Scholar] [CrossRef]
- Guo P, Qiao W, Sun Y, Liu F, Wang C. Telemedicine technologies and tuberculosis management: a randomized controlled trial. Telemedicine and e-Health. 2020, 26, 1150–1156. [Google Scholar] [CrossRef]
- Holzman SB, Atre S, Sahasrabudhe T, et al. Use of Smartphone-Based Video Directly Observed Therapy (vDOT) in Tuberculosis Care: Single-Arm, Prospective Feasibility Study. JMIR Form Res. Aug 27 2019, 3, e13411. [Google Scholar] [CrossRef]
- Manyazewal T, Woldeamanuel Y, Fekadu A, Holland DP, Marconi VC. Effect of digital medication event reminder and monitor-observed therapy vs standard directly observed therapy on health-related quality of life and catastrophic costs in patients with tuberculosis: a secondary analysis of a randomized clinical trial. JAMA Network Open. 2022, 5, e2230509–e2230509. [Google Scholar] [CrossRef]
- Chuck C, Robinson E, Macaraig M, Alexander M, Burzynski J. Enhancing management of tuberculosis treatment with video directly observed therapy in New York City. The International Journal of Tuberculosis and Lung Disease. 2016, 20, 588–593. [Google Scholar] [CrossRef]
- Lam CK, Pilote KM, Haque A, Burzynski J, Chuck C, Macaraig M. Using video technology to increase treatment completion for patients with latent tuberculosis infection on 3-month isoniazid and rifapentine: an implementation study. Journal of Medical Internet Research. 2018, 20, e9825. [Google Scholar]
- Browne SH, Umlauf A, Tucker AJ, et al. Wirelessly observed therapy compared to directly observed therapy to confirm and support tuberculosis treatment adherence: a randomized controlled trial. PLoS M edicine. 2019, 16, e1002891. [Google Scholar]
- Liu X, Lewis JJ, Zhang H, et al. Effectiveness of electronic reminders to improve medication adherence in tuberculosis patients: a cluster-randomised trial. PLoS Medicine. 2015, 12, e1001876. [Google Scholar]
- Chen S-H, Wang I, Hsu H-L, et al. Advantage in privacy protection by using synchronous video observed treatment enhances treatment adherence among patients with latent tuberculosis infection. Journal of Infection and Public Health. 2020, 13, 1354–1359. [Google Scholar] [CrossRef]
- Mohammed S, Glennerster R, Khan AJ. Impact of a daily SMS medication reminder system on tuberculosis treatment outcomes: a randomized controlled trial. PloS One. 2016, 11, e0162944. [Google Scholar]
- Farooqi RJ, Ashraf S, Zaman M. The role of mobile SMS-reminders in improving drugs compliance in patients receiving anti-TB treatment from DOTS program. Journal of Postgraduate Medical Institute.
- Guo X, Yang Y, Takiff HE, et al. A comprehensive app that improves tuberculosis treatment management through video-observed therapy: usability study. JMIR mHealth and uHealth. 2020, 8, e17658. [Google Scholar] [CrossRef]
- Belknap R, Holland D, Feng P-J, et al. Self-administered versus directly observed once-weekly isoniazid and rifapentine treatment of latent tuberculosis infection: a randomized trial. Annals of Internal Medicine. 2017, 167, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Johnston JC, van der Kop ML, Smillie K, et al. The effect of text messaging on latent tuberculosis treatment adherence: a randomised controlled trial. European Respiratory Journal.
- Garfein RS, Liu L, Cuevas-Mota J, et al. Tuberculosis treatment monitoring by video directly observed therapy in 5 health districts, California, USA. Emerging Infectious Diseases. 2018, 24, 1806. [Google Scholar] [CrossRef]
- https://www.afro.who.int/health-topics/tuberculosis-tb.
- Sekandi JN, Buregyeya E, Zalwango S, et al. Video directly observed therapy for supporting and monitoring adherence to tuberculosis treatment in Uganda: a pilot cohort study. ERJ Open Research.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



