Submitted:
16 January 2025
Posted:
16 January 2025
You are already at the latest version
Abstract
Introduction: Maternal immunization (MI) has evolved over the past decade, protecting both mother and offspring from infectious diseases. In India, only one vaccine, tetanus toxoid (TT)/ tetanus and diphtheria (Td), is available under the Universal Immunization Programme (UIP) for pregnant women. However, the basket of MI can be expanded by introducing the additional maternal vaccines in the immunization schedule. The study aims to explore the potential predictors for the uptake of additional maternal vaccines under UIP.
Methodology: For the study, relevant data was extracted from the National Family Health Survey (NFHS-5) conducted during 2019-21. A cross-sectional sample of women aged 15-49 years who had given birth in the past 5 years was analyzed. Bivariate statistics and logistic regression analysis were employed to assess the predictors for pregnant women's interaction with healthcare workers (HCWs) during 3rd trimester of pregnancy using Stata 17 software. This measure was used as a proxy to gauge readiness for new vaccine introductions, like RSV, administered during the third trimester.
Results: Information from 174,483 women was included in the study. Of them, 59.3% went for four or more antenatal care (ANC) visits, and a significant proportion (83.8%) received tetanus injections. The number of antenatal visits and tetanus injections during pregnancy emerged as strong predictors, with higher ANC visit frequencies with increased odds of meeting with healthcare workers (HCWs) during the third trimester of pregnancy. Further, younger age (20-24 years), middle wealth index group, and residence in rural areas were identified as positive predictors while higher levels of education emerged as a negative predictor.
Conclusion: The study highlights the importance of ANC visits and tetanus vaccine uptake in engaging pregnant women with HCWs during the third trimester. These factors indicate readiness for potential interventions, like the RSV vaccine, and suggest leveraging ANC visits for introducing new maternal immunization vaccines.
Keywords:
maternal immunization
; tetanus vaccine
; antenatal care
; RSV vaccine
1. Introduction
Maternal immunization (MI) has gained significant recognition over the past decade as a critical public health strategy, offering dual protection to mothers and their infants against vaccine-preventable infectious diseases (Davies et al., 2023; Verma et al., 2016). The increasing body of evidence supporting the benefits of administering vaccines during pregnancy underscores its potential to boost maternal immunity while simultaneously conferring passive immunity to the newborn (Etti et al., 2022; Marshall et al., 2016). this dual protection plays a crucial role in reducing the incidence of morbidity and mortality associated with vaccine-preventable diseases (VPDs), protecting the disproportionately affected vulnerable populations (Etti et al., 2022). As global health priorities continue to evolve, maternal immunization has become an integral component of maternal and child health strategies, with vaccines like the flu vaccine and tetanus-diphtheria (Td) already recommended for pregnant women in many regions (Etti et al., 2022; Marshall et al., 2016).
Despite the widespread success of maternal immunization in many parts of the world, the landscape in India remains limited, as currently only tetanus and diphtheria (Td) vaccine is offered under the Universal Immunization Programme (UIP) for pregnant women (Khan & Raza, 2013; Verma et al., 2016). This limited coverage is concerning, especially given the nation’s ongoing challenges in maternal and infant health indicators (Sahoo et al., 2021). According to the latest National Family Health Survey (NFHS) report, India continues to struggle with high maternal and infant mortality rates, highlighting the urgent need for more comprehensive maternal health interventions (NFHS-5, 2022).
Recent developments in vaccine research have highlighted the potential for incorporating new vaccines for maternal immunization in the UIP (Adams & Gonik, n.d.; Beigi et al., 2014; Etti et al., 2022). One such promising maternal vaccine is the respiratory syncytial virus (RSV) vaccine which has shown significant potential to reduce respiratory infections caused by RSV in infants (Beigi et al., 2014; Quincer et al., 2024). Despite these promising developments, the integration of additional maternal vaccines into the existing immunization schedule faces significant challenges, particularly in a diverse and resource-constrained setting like India (Moniz & Beigi, 2014; Wallace et al., 2012).
Research indicates that various predictors can affect the uptake of maternal vaccines, including demographic, socio-economic, cultural, and healthcare-related factors, eliciting the need for a comprehensive understanding of the factors at play (Geoghegan, et al., 2022; Williams et al., 2019). Understanding these predictors is crucial to providing insights that can inform public policy decisions and programmatic strategies for improved acceptance of maternal vaccines. Therefore, the present study aims to explore the potential predictors for the uptake of additional maternal vaccines under the UIP in India.
2. Methodology
2.1. Data Source
This study utilized secondary data from the 5th round of the National Family Health Survey (NFHS) conducted from 2019-2021. The NFHS surveys are nationally representative cross-sectional surveys that provide reliable estimates of health and family welfare indicators, including maternal & child health, and reproductive health (Dhalaria, Kapur, Singh, Verma, et al., 2023). This survey was conducted by the International Institute for Population Sciences, Mumbai as the nodal agency, designated by the Ministry of Health and Family Welfare (MoHFW), Government of India, to help policymakers examine the improvement in health outcomes over the years (Dhalaria, Kapur, Singh, Priyadarshini, et al., 2023; Dhalaria, Kapur, Singh, Verma, et al., 2023). The survey employed a two-stage stratified sampling design to identify eligible respondents for collecting information on health indicators. In the first stage, a sample of primary sampling units (villages in rural areas and Census Enumeration Blocks in urban areas) was selected from the sampling frame with probability proportional to size (PPS). In the second stage, an equal number of households were selected within each PSU using systematic random sampling (Choudhary et al., 2019; Dhalaria, Kapur, Singh, Priyadarshini, et al., 2023). The survey collected data from 724,115 women aged 15-49 years from 636,699 households in 36 states/ union territories of India (PDF, n.d.). For the present study, we included data from 174,483 women aged 15-49 who had given birth in the past 5 years and had complete information on antenatal visits. (Figure 1)
2.2. Explanatory Variables
The NFHS-5 data contained information on the number of antenatal care visits (no antenatal visits, one visit, two visits, three visits, and four & above visits) and uptake of tetanus injections (no injection, one injection, or two and above injections) during pregnancy. These two measures served as the key explanatory variables. Additional predictor variables considered in the study were women’s age group (15-19 years, 20-24 years, 25-29, 30-34, 35-39, 40-44 and 45-49), women’s education level (no education, primary education, secondary education, or higher education), place of residence (urban or rural) and wealth index (poorest, poorer, middle richer, or richest).
2.3. Outcome Variable
The interaction of pregnant women with healthcare workers (HCWs) during the third trimester of pregnancy as part of the antenatal care (ANC) package was considered an outcome variable. This indicator was considered a proxy to gauge readiness for new maternal vaccine introductions, such as RSV, administered during the third trimester.
2.4. Statistical Analysis
Descriptive statistics were used to assess the characteristics of the sampled women. Bivariate analysis (chi-square test) to examine the association between the key explanatory variables (number of antenatal care visits and uptake of tetanus injections) and other predictor variables with the proxy indicator (interaction with HCWs during the third trimester of pregnancy) was done. Further, a multivariate logistic regression model was built to assess the association between pregnant women’s interaction with HCWs during 3rd trimester of pregnancy with the other predictor variables at a p-value < 0.05 using Stata 17 software.
3. Results:
3.1. Study Characteristics of the Sample
Table 1 shows the characteristics of the sampled women (n= 174,483) included in the study. Of the total sample, most women were in the 25–29 age group, resided in the rural area, completed secondary education, and belonged to the poorest wealth index group.
3.2. Antenatal Visits and Tetanus Vaccine Uptake by the Sample
Besides, the number of antenatal care visits and tetanus injections undertaken by the sampled women during pregnancy were evaluated. Among women aged 15-49, antenatal visits varied, with a significant proportion (59.3%) going for four or more antenatal care (ANC) visits, indicating the widespread utilization of antenatal care services (Table 1).
Also, a significant proportion of women (83.8%) received tetanus vaccines during pregnancy, which indicates a robust adherence to vaccine recommendations crucial for protecting against maternal and neonatal infections and establishes the potential touch points for the introduction of additional maternal vaccines (Table 1).
3.3. Predictors Associated with the Uptake of an Additional Maternal Vaccine Under the Immunization Programme in India
The proxy measure of pregnant women’s (aged 15–49) interaction with healthcare workers during the third trimester was estimated (n=174,483). A large proportion of women (69.0%) reported meeting healthcare workers during the third trimester of pregnancy, while a significant proportion (31.0%) did not meet the healthcare workers (Figure 2).
Figure 3, highlights the percentage distribution of women aged 15–49 meeting the healthcare workers during the third trimester of pregnancy. The findings reveal significant disparities across states, with states like Odisha (91.4%), Tamil Nadu (88.7%), and Puducherry (83.4%) showing high percentages of women meeting healthcare workers, indicating robust outreach and engagement. On the other hand, states such as Manipur (19.7%), Nagaland (25.5%), and Arunachal Pradesh (33.0%) reported much lower percentages, suggesting potential scope for improvement in healthcare delivery.
Further, the associations of the key explanatory variables (number of antenatal care visits and uptake of tetanus injections) and other predictor variables (age group, women’s education level, place of residence and wealth index) with the outcome variable (pregnant women meeting the HCWs during the third trimester) were assessed. The findings show significant associations of the outcome variable with the key explanatory and predictor variables included in the analysis (Table 2). Women with higher antenatal visits and uptake of more tetanus injections during pregnancy showed strong associations with meeting the healthcare workers during the third trimester of pregnancy, with 74.3% of those with four or more antenatal visits and 70.5% of those with two or more tetanus injections reporting such engagement. Younger women, particularly those aged 15-19 (72.4%), had higher engagement than older women aged 45-49 (57.4%). Additionally, women in rural areas (72.8%) and those in the middle wealth index (73.4%) had higher interaction rates with the healthcare worker during the third trimester of pregnancy than their urban and wealthier counterparts.
Table 3, shows the results from the multivariable logistic regression analysis for the pregnant women meeting the HCWs during the third trimester. Notably, the number of antenatal visits and tetanus injections during pregnancy emerge as strong predictors, with higher ANC visit frequencies (OR: 5.50, 95% CI: 5.26 - 5.74) and more tetanus vaccine uptake (OR: 2.00, 95% CI: 1.91 - 2.09) correlating with increased odds of meeting with HCWs.
Further, the younger age group (20-24 years) emerged as a positive predictor exhibiting the higher odds (OR: 1.10, 95% CI: 1.03 - 1.18), while older women, particularly those aged 35 and above, had lower odds of such interactions (Table 2). Another positive predictor was women residents of rural areas, associated with higher odds (OR: 1.69, 95% CI: 1.64 - 1.74) than the urban areas. Additionally, disparities were observed across wealth indices, with women in the middle wealth index group showing the highest odds (OR: 1.05, 95% CI: 1.01 - 1.09) of meeting with healthcare workers. On the other hand, women with higher education levels (OR: 0.92, 95% CI: 0.88 - 0.96) emerged as a negative predictor with slightly reduced odds of interaction with the HCW in the third trimester of pregnancy (Table 3).
The above findings underscored the multifaceted nature of factors influencing healthcare-seeking behaviors during pregnancy, highlighting the importance of targeted messaging to ensure equitable access to maternal healthcare services.
4. Discussion
The concept of maternal immunization has increasingly gained momentum over the past years. It has emerged as a promising strategy to protect the health of the mother and child against vaccine-preventable infectious diseases. The recent advancements show a strong potential for expanding the basket of maternal vaccines (such as the RSV vaccine) under the UIP. However, various predictors affecting the uptake of maternal vaccines have been highlighted in previous studies. This study aimed to explore the potential predictors for the uptake of additional maternal vaccines under the UIP in India, focusing on the interaction between pregnant women and healthcare workers (HCWs) during the third trimester as a proxy for readiness to receive new maternal vaccines.
The findings of this study exhibited a robust association between the number of antenatal visits and the likelihood of pregnant women interacting with HCWs during the third trimester. This aligns with the World Health Organization Model of Antenatal Care ANC (2016) which suggests a minimum of eight ANC visits with five contacts in the third trimester (WHO, 2016). Existing literature has emphasized the noteworthy improvement in the health outcomes of the mother and offspring with the increase in ANC visits including the reduction in disease burden (Bhat & Bhat, 2023). Also, there was a strong correlation between the uptake of the tetanus vaccine and increased interaction with the HCWs during the third trimester. This aligns with the previous studies where a high number of ANC visits were found to be significantly associated with the improved delivery of ANC services such as drugs or uptake of tetanus vaccine (Kumar et al., 2019; Yaya et al., 2019).
Furthermore, demographic factors also emerged as crucial predictors for the uptake of new maternal vaccines. Younger women, particularly those in the 20-24 age group, had higher odds of interacting with HCWs during the third trimester, while older women exhibited lower odds of interacting with healthcare workers. Earlier studies have also found an upward trend of full ANC services utilization in the age group of 15-19 years from 2005 to 2015 than in women over 40 years of age (Adedokun & Yaya, 2020; Rurangirwa et al., 2017).
Besides, geographical disparities influencing the uptake of maternal vaccines were noted. The study further underscored that rural women were more likely to meet with HCWs during pregnancy compared to their urban counterparts. Previous studies from India have also highlighted that younger women had a two-fold higher likelihood of utilizing maternal healthcare services in rural areas (Mishra et al., 2024). A study by Baht & Bhat (2023) revealed that women residents of urban areas received less information about delivery care than rural residents (Bhat & Bhat, 2023).
Wealth and education were other influential factors. Women from the middle wealth index group were more likely to interact with HCWs than the wealthier ones, as previous studies in India have also reported that younger women from the poorest wealth index were more likely to utilize ASHA services (Mishra et al., 2024). This may underscore the program’s efficacy in catering to previously underserved and marginalized populations while reducing disparities in access to critical healthcare services (Mishra et al., 2024).
Surprisingly, women with higher education levels had less likelihood of interacting with HCWs during the third trimester. This finding is intriguing, as it contradicts the common assumption that there is more likelihood of taking ANC services among women with higher levels of education (Yadav et al., 2021). This could be attributed to the lower satisfaction levels among women with higher education (Bhat & Bhat, 2023; Fantaye et al., 2018). However, this finding warrants the need to explore the underlying drivers further.
The findings from this study have several implications for maternal immunization programs in India. There is a strong potential to leverage existing maternal health services, particularly ANC services, to introduce new vaccines such as the respiratory syncytial virus (RSV) vaccine, which has demonstrated considerable promise in protecting infants from respiratory infections. Furthermore, strengthening the interaction between healthcare workers and pregnant women, especially in rural and underserved areas, could help increase vaccine uptake. Also, targeted interventions to increase awareness among women, especially the ones in the younger age group or belonging to wealthier backgrounds who might not perceive the need for healthcare worker engagement or maternal vaccines are crucial.
While this study offers valuable insights, it has a few limitations. Although, robust and representative, utilization of secondary data from the NFHS-5 may not have fully captured all nuances of healthcare-seeking behavior. Additionally, the proxy measure of interaction with healthcare workers during the third trimester does not directly capture maternal vaccine uptake. Consequently, an in-depth study is recommended to explore more direct measures of maternal vaccine uptake including the barriers and facilitators impacting maternal immunization in the future.
5. Conclusion
The uptake of maternal vaccines in India is influenced by a complex interplay of factors, including but not limited to antenatal care visits and socio-demographic characteristics. The present study highlights the importance of ANC visits and tetanus vaccine uptake in engaging pregnant women with HCWs during the third trimester. Leveraging these existing maternal health services could be an effective strategy for introducing new maternal immunization vaccines. Additionally, understanding these predictors will be crucial for designing effective and equitable maternal health strategies to achieve optimal outcomes.
References
- Adams, R. M., & Gonik, B. (n.d.). The Evolving Maternal Vaccine Platform. Retrieved 27 November 2024, from https://www.mdpi.com/2673-3897/5/3/14. [CrossRef]
- Adedokun, S. T. , & Yaya, S. (2020). Correlates of antenatal care utilization among women of reproductive age in sub-Saharan Africa: Evidence from multinomial analysis of demographic and health surveys (2010–2018) from 31 countries. Archives of Public Health. [CrossRef]
- Beigi, R. H. , Fortner, K. B., Munoz, F. M., Roberts, J., Gordon, J. L., Han, H. H., Glenn, G., Dormitzer, P. R., Gu, X. X., Read, J. S., Edwards, K., Patel, S. M., & Swamy, G. K. (2014). Maternal Immunization: Opportunities for Scientific Advancement. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America. [CrossRef]
- Bhat, B. A. , & Bhat, S. A. (2023). Do Increasing Number of Antenatal Care Visits Improve Quality of ANC Services in India.
- Choudhary, T. S. , Reddy, N. S., Apte, A., Sinha, B., Roy, S., Nair, N. P., Sindhu, K. N., Patil, R., Upadhyay, R. P., & Chowdhury, R. (2019). Delayed vaccination and its predictors among children under 2 years in India: Insights from the national family health survey–4. Vaccine, 37(17), 2331–2339. [CrossRef]
- Davies, B., Olivier, J., & Amponsah-Dacosta, E. (2023). Health Systems Determinants of Delivery and Uptake of Maternal Vaccines in Low- and Middle-Income Countries: A Qualitative Systematic Review. https://www.mdpi.com/2076-393X/11/4/869. [CrossRef]
- Dhalaria, P. , Kapur, S., Singh, A. K., Priyadarshini, P., Dutta, M., Arora, H., & Taneja, G. (2023). Exploring the Pattern of Immunization Dropout among Children in India: A District-Level Comparative Analysis. Vaccines. [CrossRef]
- Dhalaria, P. , Kapur, S., Singh, A. K., Verma, A., Priyadarshini, P., & Taneja, G. (2023). Potential impact of rotavirus vaccination on reduction of childhood diarrheal disease in India: An analysis of National Family Health Survey-5. Vaccine: X. [CrossRef]
- Etti, M. , Calvert, A., Galiza, E., Lim, S., Khalil, A., Le Doare, K., & Heath, P. T. (2022). Maternal vaccination: A review of current evidence and recommendations. American Journal of Obstetrics and Gynecology. [CrossRef]
- Fantaye, C. , Melkamu, G., & Makeda, S. (2018). Postnatal Care Service Utilization and Associated Factors among Mothers Who Delivered in Shebe Sombo Woreda, Jimma Zone, Ethiopia. International Journal of Women’s Health and Wellness. [CrossRef]
- Geoghegan, S., Shuster, S., Butler, K. M., & Feemster, K. A. (2022). Understanding Barriers and Facilitators to Maternal Immunization: A Systematic Narrative Synthesis of the Published Literature | Maternal and Child Health Journal. https://link.springer.com/article/10.1007/s10995-022-03508-0. [CrossRef]
- Khan, R. E. A. , & Raza, M. A. (2013). Maternal Health-Care in India: The Case of Tetanus Toxoid Vaccination. Asian Development Policy Review. [CrossRef]
- Kumar, G. , Choudhary, T. S., Srivastava, A., Upadhyay, R. P., Taneja, S., Bahl, R., Martines, J., Bhan, M. K., Bhandari, N., & Mazumder, S. (2019). Utilisation, equity and determinants of full antenatal care in India: Analysis from the National Family Health Survey 4. BMC Pregnancy and Childbirth. [CrossRef]
- Marshall, H. , McMillan, M., Andrews, R. M., Macartney, K., & Edwards, K. (2016). Vaccines in pregnancy: The dual benefit for pregnant women and infants. Human Vaccines & Immunotherapeutics. [CrossRef]
- Mishra, S. , Horton, S., Bhutta, Z. A., & Essue, B. M. (2024). Association between the use of Accredited Social Health Activist (ASHA) services and uptake of institutional deliveries in India. PLOS Global Public Health 4(1), e0002651. [CrossRef]
- Moniz, M. H. , & Beigi, R. H. (2014). Maternal immunization. Human Vaccines & Immunotherapeutics. [CrossRef]
- PDF. (n.d.). Retrieved 27 November 2024, from https://dhsprogram.com/pubs/pdf/FR375/FR375_II.pdf.
- Quincer, E. M. , Cranmer, L. M., & Kamidani, S. (2024). Prenatal Maternal Immunization for Infant Protection: A Review of the Vaccines Recommended, Infant Immunity and Future Research Directions. Pathogens. [CrossRef]
- Rurangirwa, A. A. , Mogren, I., Nyirazinyoye, L., Ntaganira, J., & Krantz, G. (2017). Determinants of poor utilization of antenatal care services among recently delivered women in Rwanda; a population based study. BMC Pregnancy and Childbirth. [CrossRef]
- Sahoo, K. C. , Negi, S., Patel, K., Mishra, B. K., Palo, S. K., & Pati, S. (2021). Challenges in Maternal and Child Health Services Delivery and Access during Pandemics or Public Health Disasters in Low-and Middle-Income Countries: A Systematic Review. Healthcare. [CrossRef]
- Verma, R., Khanna, P., & Dhankar, M. (2016). Full article: Vaccination during pregnancy: Today’s need in India. https://www.tandfonline.com/doi/full/10.1080/21645515.2015.1093265. [CrossRef]
- Wallace, A. S., Ryman, T. K., & Dietz, V. (2012). Experiences Integrating Delivery of Maternal and Child Health Services With Childhood Immunization Programs: Systematic Review Update | The Journal of Infectious Diseases | Oxford Academic. https://academic.oup.com/jid/article/205/suppl_1/S6/869196. [CrossRef]
- WHO, D. update. (2016). New guidelines on antenatal care for a positive pregnancy experience. https://www.who.int/news/item/07-11-2016-new-guidelines-on-antenatal-care-for-a-positive-pregnancy-experience.
- Williams, A. L. , Mitrovich, R., Mwananyanda, L., & Gill, C. (2019). Full article: Maternal vaccine knowledge in low- and middle-income countries—And why it matters. https://www.tandfonline.com/doi/full/10.1080/21645515.2018.1526589. [CrossRef]
- Yadav, A. K. , Sahni, B., Kumar, D., Bala, K., & Kalotra, A. (2021). Effect of Women’s and Partners’ Education on Maternal Health-care Services Utilization in Five Empowered Action Group States of India: An analysis of 13,443 Women of Reproductive Age. International Journal of Applied and Basic Medical Research. [CrossRef]
- Yaya, S. , Kota, K., Buh, A., & Bishwajit, G. (2019). Antenatal visits are positively associated with uptake of tetanus toxoid and intermittent preventive treatment in pregnancy in Ivory Coast. BMC Public Health 19(1), 1467. [CrossRef] [PubMed]
Figure 1.
Process of sample selection for the study from NFHS-5 survey.
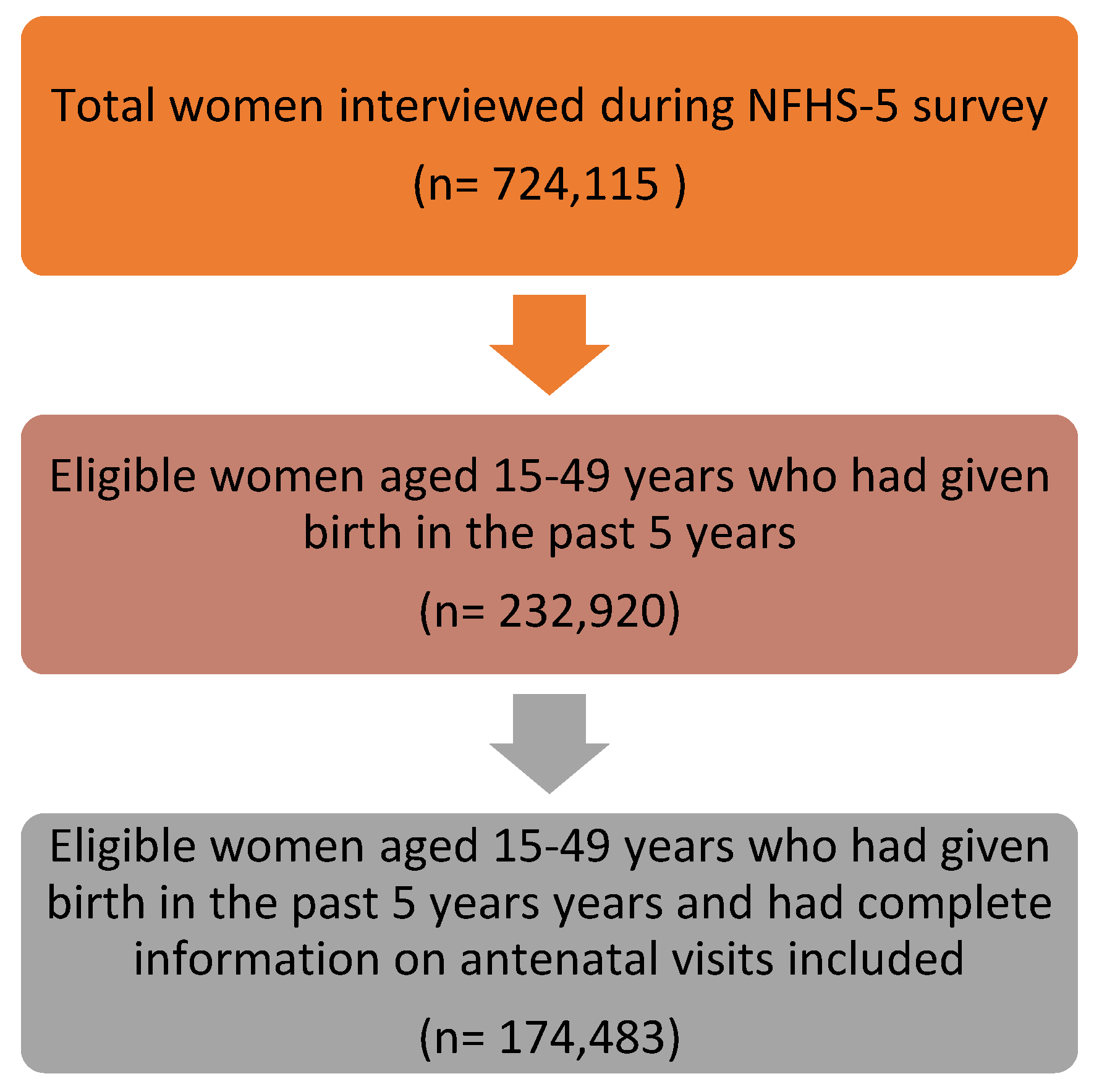
Figure 2.
Women in the age group of 15-49 years meeting Healthcare Workers during the third trimester of pregnancy (NFHS-5) (n=174,483).
Figure 2.
Women in the age group of 15-49 years meeting Healthcare Workers during the third trimester of pregnancy (NFHS-5) (n=174,483).
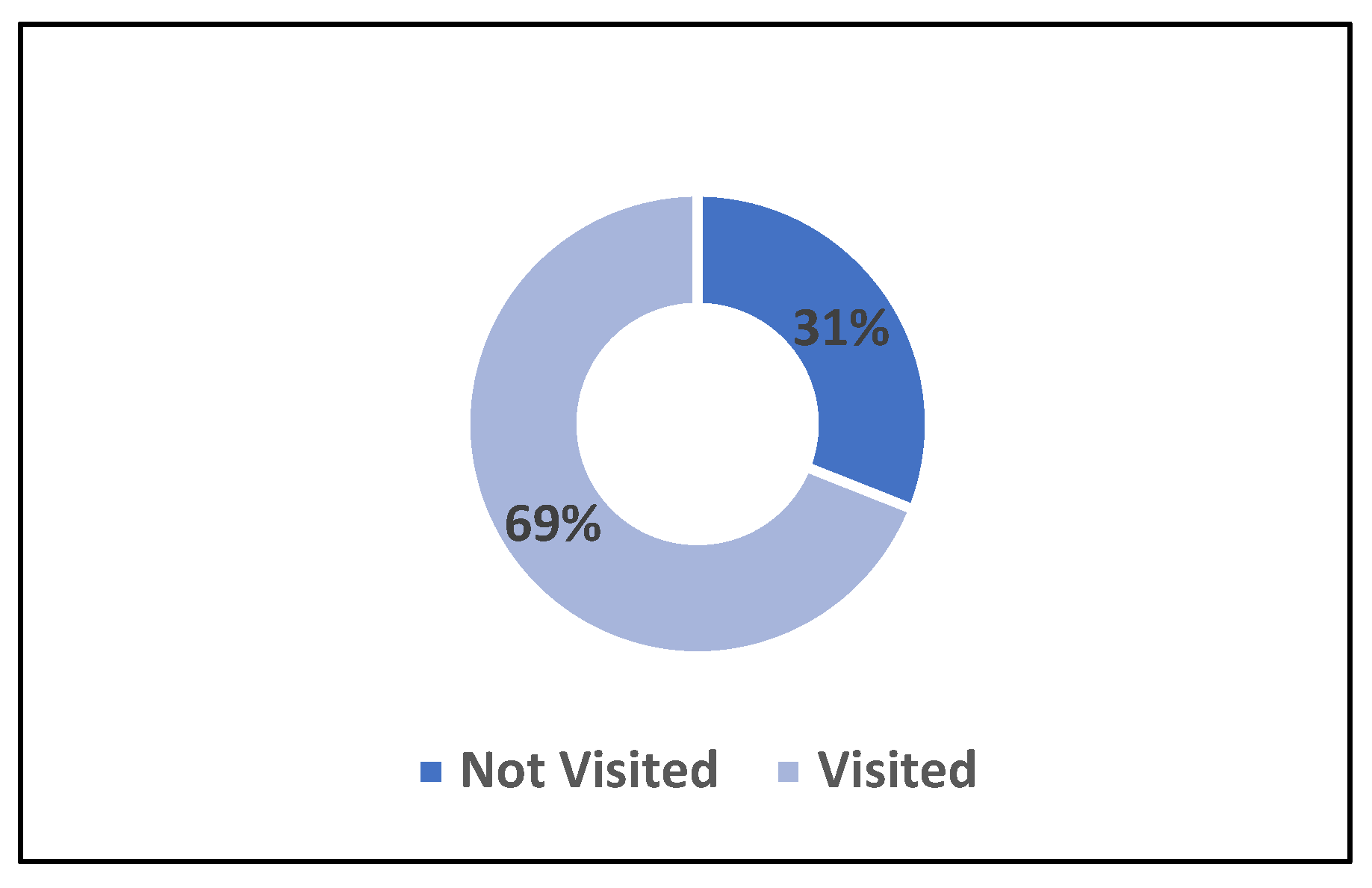
Figure 3.
State-wise Percentage Distribution of Women in the age group of 15-49 years meeting Healthcare Workers during the third trimester of pregnancy (NFHS-5) (n=174,483).
Figure 3.
State-wise Percentage Distribution of Women in the age group of 15-49 years meeting Healthcare Workers during the third trimester of pregnancy (NFHS-5) (n=174,483).
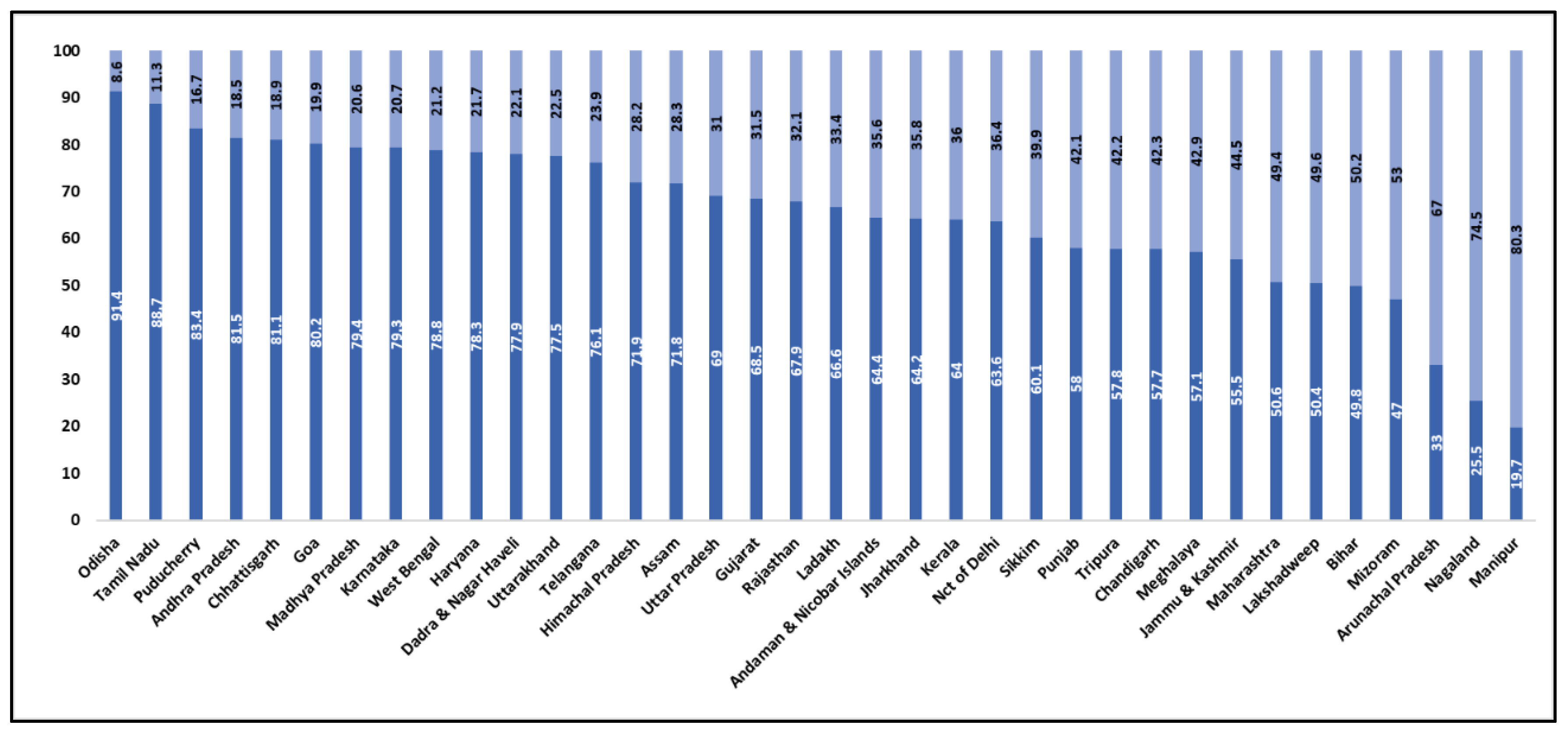

Table 1.
Study Characteristics of the sample.
| Variables | Percent (%) | Sample (N) |
|---|---|---|
| Antenatal Visits | ||
| No Visit | 6.2 | 11,462 |
| One Visit | 6.6 | 11,032 |
| Two Visits | 12.0 | 21,422 |
| Three Visits | 15.9 | 29,132 |
| Four And Above Visits | 59.3 | 1,01,435 |
| Tetanus Injection During Pregnancy | ||
| No Injection | 4.7 | 9,452 |
| One Injection | 11.6 | 20,492 |
| Two And Above Injections | 83.8 | 1,44,539 |
| Women Age Group | ||
| 15-19 | 3.1 | 4,817 |
| 20-24 | 29.2 | 48,160 |
| 25-29 | 38.8 | 66,884 |
| 30-34 | 19.6 | 35,785 |
| 35-39 | 7.2 | 14,331 |
| 40-44 | 1.6 | 3,540 |
| 45-49 | 0.4 | 966 |
| Women Education Level | ||
| No Education | 19.6 | 35,592 |
| Primary | 11.8 | 21,437 |
| Secondary | 51.4 | 91,314 |
| Higher | 17.2 | 26,140 |
| Place Of Residence | ||
| Urban | 28.1 | 37,392 |
| Rural | 71.9 | 1,37,091 |
| Wealth Index | ||
| Poorest | 22.8 | 44,314 |
| Poorer | 21.1 | 39,960 |
| Middle | 19.6 | 34,095 |
| Richer | 19.2 | 30,618 |
| Richest | 17.3 | 25,496 |
Table 2.
Chi-Square Analysis of Factors Associated with Women Meeting Healthcare Workers During the Third Trimester, 15–49 Age Group, NFHS-5.
Table 2.
Chi-Square Analysis of Factors Associated with Women Meeting Healthcare Workers During the Third Trimester, 15–49 Age Group, NFHS-5.
| Variables | No (%) | Yes (%) | Sample(N) | (p < .000) |
|---|---|---|---|---|
| Antenatal visits | 0.000 | |||
| No Visit | 62.7 | 37.3 | 11,462 | |
| One Visit | 42.2 | 57.9 | 11,032 | |
| Two Visits | 36.1 | 63.9 | 21,422 | |
| Three Visits | 29.8 | 70.2 | 29,132 | |
| Four And Above Visits | 25.7 | 74.3 | 1,01,435 | |
| Tetanus injection during pregnancy | 0.000 | |||
| No Injection | 48.9 | 51.1 | 9,452 | |
| One Injection | 34.4 | 65.6 | 20,492 | |
| Two And Above Injections | 29.5 | 70.5 | 1,44,539 | |
| Women age group | 0.000 | |||
| 15-19 | 27.6 | 72.4 | 4,817 | |
| 20-24 | 28.1 | 71.9 | 48,160 | |
| 25-29 | 30.4 | 69.6 | 66,884 | |
| 30-34 | 33.9 | 66.1 | 35,785 | |
| 35-39 | 36.6 | 63.4 | 14,331 | |
| 40-44 | 41.2 | 58.8 | 3,540 | |
| 45-49 | 42.6 | 57.4 | 966 | |
| Women Education level | 0.000 | |||
| No Education | 35.6 | 64.4 | 35,592 | |
| Primary | 28.6 | 71.4 | 21,437 | |
| Secondary | 27.8 | 72.2 | 91,314 | |
| Higher | 36.8 | 63.3 | 26,140 | |
| Place of residence | 0.000 | |||
| Urban | 40.7 | 59.3 | 37,392 | |
| Rural | 27.2 | 72.8 | 1,37,091 | |
| Wealth Index | 0.000 | |||
| Poorest | 31.1 | 68.9 | 44,314 | |
| Poorer | 27.5 | 72.5 | 39,960 | |
| Middle | 26.6 | 73.4 | 34,095 | |
| Richer | 29.7 | 70.3 | 30,618 | |
| Richest | 41.5 | 58.5 | 25,496 |
Table 3.
Logistic Regression Analysis of Factors Associated with women met with healthcare workers in the third Trimester, 15-49 age group, NFHS-5.
Table 3.
Logistic Regression Analysis of Factors Associated with women met with healthcare workers in the third Trimester, 15-49 age group, NFHS-5.
| Variables | Odds ratio | P>z | [95% Confidence interval] |
|---|---|---|---|
| Antenatal visits | |||
| No Visit® | |||
| One Visit | 2.748 | 0.000 | (2.6-2.905) |
| Two Visits | 3.202 | 0.000 | (3.049-3.363) |
| Three Visits | 4.051 | 0.000 | (3.863-4.248) |
| Four And Above Visits | 5.501 | 0.000 | (5.267-5.744) |
| Tetanus injection during pregnancy | |||
| No Injection® | |||
| One Injection | 1.732 | 0.000 | (1.643-1.825) |
| Two And Above Injections | 2.001 | 0.000 | (1.913-2.094) |
| Women age group | |||
| 15-19® | |||
| 20-24 | 1.110 | 0.002 | (1.038-1.188) |
| 25-29 | 1.047 | 0.177 | (0.979-1.119) |
| 30-34 | 0.928 | 0.034 | (0.867-0.994) |
| 35-39 | 0.793 | 0.000 | (0.737-0.853) |
| 40-44 | 0.721 | 0.000 | (0.655-0.793) |
| 45-49 | 0.622 | 0.000 | (0.536-0.722) |
| Women Education level | |||
| No Education® | |||
| Primary | 1.093 | 0.000 | (1.052-1.136) |
| Secondary | 1.060 | 0.000 | (1.029-1.092) |
| Higher | 0.922 | 0.000 | (0.885-0.961) |
| Place of residence | |||
| Urban® | |||
| Rural | 1.696 | 0.000 | (1.649-1.744) |
| Wealth Index | |||
| Poorest® | |||
| Poorer | 0.995 | 0.753 | (0.964-1.027) |
| Middle | 1.054 | 0.003 | (1.018-1.091) |
| Richer | 1.046 | 0.017 | (1.008-1.086) |
| Richest | 0.831 | 0.000 | (0.796-0.866) |
| Note: ®Reference Category; p < 0.05 (*), p < 0.01 (**), p < 0.001 (***) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



