
Submitted:
13 January 2025
Posted:
14 January 2025
You are already at the latest version
Abstract
Major depressive disorder and bipolar disorders are prevalent mental health conditions that significantly impact quality of life and life expectancy. These mood disorders involve major depressive episodes (MDE), which pose a substantial burden for patients and their families. While psychopharmacological therapies are a first-line treatment for MDE, the response is often incomplete. New approaches focused on the human-nature relationship may potentially complement antidepressant treatments, thus reducing psychopharmacological needs. This study aims to evaluate whether green exposure affects depressive symptoms and inflammatory biomarker levels in patients with MDE. This prospective study examined the association between exposure to green environments such as woods, forests, large parks, and gardens for at least 45 minutes twice a week, depressive symptoms, and inflammatory biomarkers in 31 patients with an ongoing MDE. The findings suggest that exposure to greenness, together with the modification of antidepressant therapy, is associated with improved depressive symptoms, lower levels of inflammatory biomarker interleukin-6, and higher concentrations of adiponectin after six weeks of treatment. These results suggest that exposure to green environments may have a favorable impact both on mental health and on inflammatory processes, and thus represent a complementary therapeutic strategy. Such information could be relevant to clinicians and urban planners.
Keywords:
major depressive disorder (MDD)
; bipolar disorders (BD)
; mood disorders
; interleukin-6
; adiponectin
; human-nature interaction
; shinrin-yoku
; forest bathing
; augmentation strategies
; urban green environments
; urban park design
1. Introduction
In the 5th Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), mood disorders are defined as a group of psychiatric disorders characterized by the recurrence of clinically significant changes in mood state, energy, cognitive processes, sleep, or appetite [1]. Within this group, Major Depressive Disorder (MDD) and Bipolar Disorder (BD) are the most common conditions in the general population [1], with a prevalence of 5 and 1-2%, respectively (WHO, 2022). MDD is the second cause of years lived with disability and is expected to become the leading one by 2030 [2,3]; BD is currently the 27th [2]. Globally, both conditions are associated with significantly reduced quality of life (QoL) and life expectancy [4,5] and carry a particularly elevated risk of premature death from natural causes [6] and suicide [6,7,8,9]. Both MDD and BD share the presence of major depressive episodes (MDEs). MDEs consist of periods of two weeks or more during which there is a persistent change in the person’s usual level of functioning and are characterized by depressed mood, loss of interest, alterations in sleep and appetite, fatigue, difficulty concentrating and memory, feelings of guilt, and thoughts of death (DSM-5). Therapeutic strategies, such as antidepressant medication, are available to treat MDEs, although outcomes are suboptimal given that roughly half of the patients do not achieve complete remission [10,11,12,13]. Inadequate response to treatments represents a significant burden for patients and their families and a relevant economic and social cost due to lost working days, reduced productivity, and high utilization of healthcare services [14].
This lack of response to antidepressants may partially depend on the complex and poorly understood etiopathogenesis of mood disorders [15]. Recent research on the pathophysiological processes of depression focused on the alteration of the monoamine neurotransmitter systems, dysregulation of the hypothalamus-pituitary-adrenal axis (HPA) and the immune system, genetic susceptibility, maladaptive epigenetic modifications, oxidative stress-induced damage, and neurodevelopmental alterations [16,17,18,19,20,21,22,23,24].
In particular, MDD and BD are associated with altered stress-response [25] and chronic inflammation [26,27]. As concerns stress, an increased reactivity of the hypothalamic-pituitary-adrenal (HPA) was found in both mood disorders [28,29]. The HPA axis regulates cortisol secretion, which promotes allostasis by managing stress responses [30]. However, prolonged exposure to this hormone can lead to structural brain changes potentially contributing to the pathophysiology of MDD and BD [28,29]. As to inflammation, acute phase proteins, mainly C-reactive protein (CRP), are increased in patients with MDD and BD [2]. CRP has three primary functions: it promotes complement activation, opsonization, and the induction of phagocytosis [31]. Similarly to CRP, the complement system is critical in innate immune activity. Over 30 serum proteins are activated through three major pathways converging on the cleavage of the complement component C3 [32]. Elevated levels of this acute-phase protein [33,34,35,36], as well as of the C4 fraction [35,37], were found in patients with depression as compared to healthy controls. Complement activation may increase the permeability of the blood-brain barrier (BBB) and, consequently, promote neuroinflammation and the development of depressive symptoms [38]. Another relevant plasmatic marker of inflammation is interleukin-6 (IL-6) [39]. IL-6 is a multifunctional cytokine that participates in the transition from the acute phase to the chronic phase of inflammation [40]. This interleukin is elevated in patients with MDD [41] and BD [42] and might connect many pathological mechanisms sustaining mood disorders [41]. Higher levels of inflammation and metabolic alterations are frequent in MDD and BD [43]. Among cytokines, adipokines, i.e., the cytokines secreted from adipose tissue, are essential in linking metabolism and inflammation [43]. The two main adipokines are leptin and adiponectin [44]. Leptin regulates energy balance and appetite, has pro-inflammatory effects, and is augmented in obesity and chronic inflammation that cause leptin resistance and consequent hyperleptinemia [45,46]. Adiponectin is involved in glucose homeostasis and fatty acid oxidation, has anti-inflammatory properties, and is decreased in chronic inflammation [47,48,49]. Finally, brain-derived neurotrophic factor (BDNF), essential for neurogenesis and synaptic plasticity, particularly in the hippocampus [50,51], appears to be a fundamental link between inflammation and depression. Peripheral inflammation can compromise BBB integrity, increasing its permeability and allowing circulating cytokines’ entry into the brain [52]. Their neuroinflammatory action downregulates BDNF expression within the central nervous system (CNS), impairing neuroplasticity and contributing to cognitive and affective symptoms found in MDEs [52,53,54,55].
The high rate of patients who do not adequately respond to antidepressant therapies motivates the development of additional nonpharmacological treatments for MDEs in MDD and BD. Among them, there is a growing interest in multidisciplinary approaches that focus on human-nature interaction, such as frequenting natural green environments [56]. Indeed, green exposure reduces mental distress and promotes happiness, positive social interactions, and subjective well-being [56,57,58]. Some of these effects appear due to molecules released in green areas, i.e., terpenes -plant secondary metabolites- that display a broad spectrum of biological activities, particularly anti-inflammatory ones [59]. Living near green spaces reduces proinflammatory processes and chronic stress response and is associated with a lower risk of developing depression [60,61] and a longer life expectancy [62].
Therefore, the aim of this study is to evaluate whether exposure to natural green environments has a role in decreasing depressive symptoms and inflammatory biomarkers in patients with MDD or BD.
2. Results
2.1. Characteristics of the Sample at Baseline
Eighty-four subjects (53 patients, 31 HV) participated in the study. Twenty-two (41.5%) patients dropped out at follow-up; drop-outs did not show significant differences at baseline with patients who completed the study (Table 1). Most follow-up patients were female (71%), had a median age of 47, and had an education of 13 years. The median duration of illness was six years, and the median severity of the MDE was moderate [63].
2.2. Group Comparisons at Baseline and Follow-Up
At baseline, patients exposed to green during the study had lower IL-6, CRP, C3, C4, and leptin levels and higher adiponectin concentrations than nonexposed patients (Figure 1a; Table 2).
At follow-up, we found the same differences except for C4 (Figure 1b; Table 2). HV exposed to green had lower leptin levels than those nonexposed (Figure 1c; Table 2).
The comparison between patients and HV exposed to green did not show significant results either at baseline or at follow-up (Table 2).
2.3. Paired Sample Comparisons Within Exposed and Nonexposed Patients’ Groups
The paired sample comparisons showed that patients exposed to green had a reduction of depressive symptoms and IL-6 levels and an increase in adiponectin serum concentration at the six-week follow-up visit (Table 2; Figure 1f).
No significant differences in biomarkers and depressive symptoms were found in nonexposed patients (Table 2).
2.4. The Impact of Green Exposure on Depressive Symptoms and IL-6 and Adiponectin Plasmatic Levels
The regression models (Table 3) indicated that exposure to green environments was significantly associated with a reduction of depressive symptoms and IL-6 plasmatic levels and with an increase in adiponectin plasma concentrations.
3. Discussion
This paper evaluated the impact on depressive symptoms and inflammatory biomarkers of a six-week repeated green exposure as an additional treatment for patients experiencing an MDE. About two-thirds of our sample was exposed to green environments at least twice a week. This practice, in association with the modification of antidepressant therapy, contributed to symptom improvement, IL-6 reduction, and adiponectin increase.
The immersion into greenery proposed to our patients effectively fosters a human-nature solid connection, consistent with the so-called “biophilia hypothesis” [64]. Introduced in 1984, this theory posits that humans evolved with nature and, therefore, have an innate connection with it shaped by evolutionary forces [65]. According to this hypothesis, the human bond with the natural world is deeply rooted in our biology and contributes to our psychological well-being, reducing stress and enhancing cognitive function. This highlights that our affinity for nature supports mental and physical health, making incorporating natural elements into human environments essential for improved well-being [65]. Focusing on our results, we must note that our patients lived in urban areas, constantly exposed to stress-inducing stimuli typical of highly anthropized environments. Numerous studies have indeed shown that urban living is a significant risk factor for mental health disorders, including depression [66,67,68,69,70]. Immersing themselves in nature might have offered a reprieve from these stressors and contributed to the observed improvements in depressive symptoms. This agrees with a recent large meta-analysis that demonstrated a significant correlation between living in greener areas and reduced depression risk, with a 10% increase in green space associated with a 3.7% decrease in depression odds [71].
The positive effects of green exposure may depend on the sensory stimuli of immersion in a natural environment and the inhalation of terpenes. Studies on “Shinrin-yoku” -literally forest bathing- a Japanese practice of physical relaxation through forest aerosol showers with all senses [72,73,74], highlight how exposure to forest environments can lower cortisol levels, pulse rate, and blood pressure, promoting a sense of well-being [75]. Other studies indicate that visual exposure to greenery alone can elicit similar benefits. Even brief views of nature, such as looking at pictures, 3D images, videos, or virtual reality of green landscapes, have been associated with activating brain areas related to emotion regulation [76,77], stress reduction, and mood improvement [78,79]. An additional antidepressant mechanism of green exposure could be related to increased exposure to sunlight [80]. Being outdoors in green spaces during sunny days may promote antidepressant effects of sunlight related to visual exposure to light and activation of vitamin D [81]. A further study has demonstrated that olfactory stimuli, even more than visual ones, may reduce stress [82]. Among inhaled substances, terpenes, aromatic compounds released by many plants, including trees and shrubs, have been shown to have anxiolytic and anti-depressive effects [83]. Once inhaled, terpenes can interact with CNS by activating olfactory receptors or directly crossing the BBB. Following the first route, terpenes’ contact with the primary olfactory neurons transduces a signal to the glomerulus of the olfactory bulb, i.e., the relay between the peripheral and central olfactory systems. Then, olfactory information is transmitted to the secondary olfactory structures, mainly the piriform cortex. Finally, tertiary olfactory structures, including the thalamus, hypothalamus, amygdala, hippocampus, and orbitofrontal and insular cortices, are involved [84]. This direct connection between the olfactory and limbic systems may contribute in reducing stress and depressive symptoms following terpenes inhalation [85]. When crossing the BBB through the nasal epithelium, terpenes interact with specific receptors, influencing various neural pathways. For example, linalool, produced by several aromatic plants and flowers such as bay leaves, mint, citrus fruits, and lavender, binds to GABA-A receptors, exerting an anxiolytic effect and reducing depressive symptoms [86,87,88]. β-Caryophyllene, instead, is produced from various aromatic plants and spices such as rosemary, basil, and lavender. It is a full agonist of cannabinoid receptors 2 (CB2) that exerts an anti-inflammatory effect by reducing pro-inflammatory cytokines in the CNS, thus alleviating neuroinflammation [89,90,91]. Thanks to its permeability, high vascularization, and bypass of first-pass metabolism, the nasal epithelium is a promising route for needle-free drugs administration, which is reflected in several well-established drugs using this delivery strategy [92,93].
During a MDE, the CNS and the rest of the body establish a complex dialogue through cytokines, metabolism, and acute-phase proteins [94]. Patients experience a phase of emotional, cognitive, and inflammatory disruption, accompanied by acute psychological and physical stress, during which various systems (namely the psycho-neuro-endocrine-immune systems) interact closely, leading to homeostatic imbalances [95]. These systems communicate via signaling molecules like cytokines, hormones, and neurotransmitters, creating a dysfunctional feedback loop that negatively influences mood regulation, immune response, and stress adaptation [95]. Our results showed an inverse correlation between specific biological markers and green exposure. Indeed, compared to non-exposed patients, those who spent more time in green environments had lower baseline levels of IL-6, CRP, C3, C4, and leptin, and higher levels of adiponectin, showing that higher inflammatory levels at baseline were associated with lower engagement in green exposure. At follow-up, exposed patients demonstrated a reduction in IL-6 serum concentration and an increase in adiponectin, highlighting a possible anti-inflammatory role of green exposure.
Increased inflammatory markers, particularly IL-6, have been associated with specific symptoms of depression, such as hypersomnia, fatigue, leaden paralysis, and hyperphagia, which could negatively affect patients’ ability to move toward natural green environments [96,97,98]. This could account for our findings, showing that patients with higher levels of chronic inflammation markers at baseline are indeed the ones who experience more difficulty in attending green areas.
IL-6 is a biomarker of chronic inflammation that plays a crucial role in regulating immune responses, including neuroinflammation [99,100]. Heightened levels of IL-6 are linked to the activation of the HPA axis, the alteration of neurotransmitter metabolism, and more severe depressive symptoms [101]. Consequently, IL-6 may influence the onset and progression of depression [26]. We found increased IL-6 levels in patients at baseline. This agrees with previous studies that demonstrated this cytokine was elevated in MDD and BD patients with active MDE compared to patients during remission [102]. Moreover, our results show that IL-6 levels decreased at follow-up in patients exposed to green environments during the study. This effect might depend on the correlates of greenery, particularly terpenes inhalation and exposure to sunlight. Many previous studies reported the systemic anti-inflammatory activity of terpenes [103,104,105], which might be implied in the reduction of IL-6 that we found, while sunlight exposure has already demonstrated an anti-depressant and IL-6-reducing effect in depressed patients [80]. These effects of light exposure are probably exerted through the activation of the retina, which in turn modulates the activity of different limbic, thalamic, and hypothalamic structures, including the suprachiasmatic nucleus, the ventrolateral preoptic nucleus, orexin areas, the amygdala, the nucleus accumbens, the perihabenular nucleus, the left hippocampus, the ventral lateral geniculate nucleus, the intergeniculate leaflet, and the lateral habenula [106]. Adiponectin increased after green exposure. We suppose that the well-documented anti-inflammatory properties of exposure to nature might have reduced inflammation in depressed patients, creating a more favorable environment for adiponectin levels to rise. Once inflammation is lowered, this could, in turn, allow adiponectin to regain its regulatory role, contributing to improved metabolic and mood-related outcomes. Indeed, this adipokine is a pleiotropic adipocyte-secreted hormone; apart from its insulin-sensitizing role, it also has neurotrophic properties since it binds to receptors in both the hippocampus and medial PFC [107]. Remarkably, intracerebral injection of exogenous adiponectin in mice elicits an antidepressant response [107]. Moreover, studies demonstrated that exercise and environmental enrichment [108,109] in mice could also increase adiponectin levels, together with antidepressant effects’ induction and depression-like states’ prevention, respectively.
Our study has some limitations that must be acknowledged. Firstly, the observational design lacks the control of a randomized trial, which may introduce biases. Secondly, the sample size is limited, which may affect the generalizability of the findings. Additionally, the short follow-up period hinders assessing long-term effects on functioning and quality of life.
Despite these limitations, this study has notable strengths. It is pioneering as the first to examine green space exposure in patients with MDE in a real-world setting, showing that patients adhere to spending time in green spaces despite acute depression. We also show preliminary evidence of efficacy, with improvements in depressive symptoms and inflammatory balance linked to green space exposure. The clinical sample, which consists of patients with acute MDE, provides a unique insight into this population. Additionally, the study’s holistic approach considers not only depressive symptoms but also factors related to inflammation, stress, metabolism, and neurotrophic factors and focuses on the human-nature interaction in terms of exposure and immersion into green environments. Previous studies examined the relationship between green exposure and depressive symptoms in the general population; our study focused specifically on patients with MDD or BD during an acute depressive phase (MDE).
Future research directions include increasing the sample size to reach higher statistical power and extending the follow-up period to assess the long-term impacts of green exposure on patients’ functioning and quality of life. Moreover, evaluating neurocognitive functions and their relationships with MDE, inflammation, and exposure to green spaces could offer insights into the underlying mechanisms. Finally, studying epigenetic processes, such as miRNA transcription and histone modifications, could help clarify the role of green space exposure in regulating gene expression associated with depression and inflammation, further bridging the gap between environmental exposure and biological mechanisms.
In conclusion, exposure to natural green environments contributes to psychopharmacological therapy in accelerating the reduction of depressive symptoms and is associated with reduced inflammatory status. Information from this work could be relevant not only to psychiatrists dealing with depression but to all clinicians dealing with mental or neurological disorders who might benefit from the anti-inflammatory effect of exposure to green environments. Furthermore, these data indicate that designing and distributing urban greenery by giving space to large parks spread throughout the city fabric may positively impact the mental health of city dwellers.
4. Materials and Methods
4.1. Participants and Study Design
Participants were enrolled from May 2023 to March 2024 at the Struttura Complessa Psichiatria Universitaria, Dipartimento di Neuroscienze e Salute Mentale, Azienda Ospedaliero-Universitaria “Città della Salute e della Scienza di Torino”, Turin, Italy. Clinical assessment and venous blood sampling of all subjects were performed at this location.
The patients recruited were aged between 18 and 65 years, living in an urban area, and had a diagnosis of MDD or BD (DSM-5 criteria) with an ongoing MDE necessitating the initiation or modification of an antidepressant treatment. Exclusion criteria were neuropsychiatric comorbidities, assessed according to DSM-5 criteria, including neurodevelopmental disorders, alcohol and/or substance use disorder and major neurocognitive disorders, difficulties of mobility that impair access to green areas, and pregnancy.
Healthy volunteers (HV) were excluded if they had a positive history of head injury with loss of consciousness, neurological disease, current use of drugs with effects on the CNS, history of alcoholism or substance abuse in the last six months, pregnancy, and a positive personal and/or family history of psychiatric disorders.
The study had a prospective design: patients were assessed by a psychiatrist and taken a venous blood sample at baseline (t0), i.e., during the MDE when the antidepressant therapy was modified and after six weeks at the follow-up visit (t1).
At baseline, we suggested patients be exposed to natural green environments. We defined green environments as all those areas with low anthropization that allow patients to be in contact with nature while distancing themselves as much as possible from the urban environment. Therefore, we considered green environments to be forests, woodlands, and extensive urban gardens or parks that allowed patients an immersive greenery experience through sight, hearing, and smell. We suggested patients be exposed to green environments for 45-60 minutes three non-consecutive days a week until the follow-up visit. HV’s data collection and blood sampling were performed at one time point only.
Comprehensive information was provided on the procedures and goals of the study, and signed consent was obtained from all subjects. The study was designed in accordance with the Declaration of Helsinki and was approved by the Local Research Ethics Committee (Protocol number: 0010765).
4.2. Exposure to Green, Clinical, and Biological Markers Assessment
At the baseline, all participants were evaluated using a semi-structured interview to assess socio-demographic characteristics and to investigate the relationship with green in terms of time spent in green environments, including parks, gardens, and woods, in the six weeks before the interview. HV were interviewed to assess whether they met the exclusion criteria and were considered exposed to greenery if they stayed in green environments for at least 45 minutes on two non-consecutive days per week for the six weeks before enrollment and blood sampling.
The clinical characteristics of MDD or BD and the severity of depressive symptoms were assessed by two expert psychiatrists (C.B.; A.C.). Severity of symptoms was evaluated with the Hamilton Rating Scale for Depression (HAM-D) [110], where a higher score indicates greater severity.
After six weeks from baseline, patients performed the follow-up visit. They were reassessed with the HAM-D scale and asked whether they were exposed to green environments for at least 45 minutes on two non-consecutive days per week; according to their response, patients were considered exposed or non-exposed to green environments.
The nursing staff conducted venous sampling of all subjects at baseline and follow-up. In the serum, we dosed cortisol, IL-6, CRP, C3 and C4 complement fractions, leptin, and adiponectin at the Struttura Complessa Biochimica Clinica, Azienda Ospedaliero-Universitaria “Città della Salute e della Scienza”, Turin, Italy, and BDNF at “Neuroscience Institute Cavalieri Ottolenghi” laboratory in Orbassano.
The dosage of biomarkers in participants’ blood samples is described in supplementary methods.
4.3. Statistical Analysis
The normal distribution of the continuous variables was verified with the Shapiro-Wilk test. Variables were expressed as median and interquartile range. The Mann-Whitney test was employed for independent sample comparisons, and the Wilcoxon test for paired ones. The false discovery rate (FDR) was controlled with the Benjamini-Hochberg (BH) correction procedure [111].
The significant results of the Wilcoxon tests were used to perform linear regression models. Follow-up variables showing a significant variation from the baseline in the Wilcoxon tests were chosen as outcomes for the regression models. Exposure to green environments between baseline and follow-up was entered as the regressor in all regression models. The models were controlled for the diagnosis (MDD or BD) and the baseline variable that was significantly different in the Wilcoxon test. For example, if depressive symptoms were significantly different in the Wilcoxon test, we chose depressive symptoms at follow-up as the outcome while controlling for depressive symptoms at baseline.
Analyses were conducted with IBM Statistical Package for Social Science (SPSS) version 29.0 and Jasp version 0.18.3, with a critical p of 0.05.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Method M1: Biomarkers’ dosage.
Author Contributions
Conceptualization, A.V. and P.R.; methodology, G.P. and C.B.; software, G.P., C.B., and A.C.; validation, G.P., C.B., and A.C.; formal analysis, G.P. and G.M.; investigation, A.C., C.B; resources, A.V. and P.R.; data curation, G.P., C.B., and A.C.; writing—original draft preparation, G.P., C.B., and A.C.; writing—review and editing, G.P., C.B., M.B., A.C., F.C., G.M., R.S., A.V., and P.R.; supervision, M.B., A.V., and P.R.; project administration A.V. and P.R.; funding acquisition, A.V. and P.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research has been supported by “BANDO RICERCA TRASLAZIONALE” (Dept. Neuroscience, Univ. Turin) grant to A.V. and P.R. and Ministero dell’Università e della Ricerca—MUR projects “Dipartimenti di Eccellenza 2023–2027” to the Dept. of Neuroscience “Rita Levi Montalcini” of the University of Turin. G.P.’s research has been conducted with the support of Programma Operativo Nazionale Ricerca e Innovazione 2014-2020 (CCI2014IT16M2OP005), risorse FSE REACT-EU, Azione IV.5 “Dottorati su tematiche Green”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Local Research Ethics Committee (Protocol number: 0010765, 31/01/2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to the anonymity ensured in the informed consent documents at the time of data collection. These data are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mokhtari, A.; Porte, B.; Belzeaux, R.; Etain, B.; Ibrahim, E.C.; Marie-Claire, C.; Lutz, P.-E.; Delahaye-Duriez, A. The Molecular Pathophysiology of Mood Disorders: From the Analysis of Single Molecular Layers to Multi-Omic Integration. Prog. Neuropsychopharmacol. Biol. Psychiatry 2022, 116, 110520. [Google Scholar] [CrossRef] [PubMed]
- Organization, W.H. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization, 2017. [Google Scholar]
- Global Burden of Disease Study 2021 (GBD 2021) Burden and Strength of Evidence by Risk Factor 1990-2021 | GHDx. Available online: https://ghdx.healthdata.org/record/ihme-data/gbd-2021-burden-by-risk-1990-2021 (accessed on 15 October 2024).
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Koretz, D.; Merikangas, K.R.; Rush, A.J.; Walters, E.E.; Wang, P.S. National Comorbidity Survey Replication The Epidemiology of Major Depressive Disorder: Results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003, 289, 3095–3105. [Google Scholar] [CrossRef] [PubMed]
- P, C.; H, N.; E, K.; Ch, V.; A, C.; Ta, F. A Network Meta-Analysis of the Effects of Psychotherapies, Pharmacotherapies and Their Combination in the Treatment of Adult Depression. World Psychiatry Off. J. World Psychiatr. Assoc. WPA 2020, 19. [Google Scholar] [CrossRef]
- Costa, L. da S.; Alencar, Á.P.; Nascimento Neto, P.J.; dos Santos, M. do S.V.; da Silva, C.G.L.; Pinheiro, S. de F.L.; Silveira, R.T.; Bianco, B.A.V.; Pinheiro, R.F.F.; de Lima, M.A.P.; et al. Risk Factors for Suicide in Bipolar Disorder: A Systematic Review. J. Affect. Disord. 2015, 170, 237–254. [Google Scholar] [CrossRef] [PubMed]
- E, V.; M, B.; Tg, S.; Af, C.; T, S.; Jr, C.; K, G.; Kw, M.; I, G. Bipolar Disorders. Nat. Rev. Dis. Primer 2018, 4. [Google Scholar] [CrossRef]
- Miller, J.N.; Black, D.W. Bipolar Disorder and Suicide: A Review. Curr. Psychiatry Rep. 2020, 22, 6. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Chen, Y.; Li, L.; Chen, J.; Guo, Y.; Bian, Z.; Lv, J.; Yu, C.; Xie, X.; Huang, D.; et al. Factors Associated with Suicide Risk among Chinese Adults: A Prospective Cohort Study of 0.5 Million Individuals. PLoS Med. 2021, 18, e1003545. [Google Scholar] [CrossRef] [PubMed]
- Crisafulli, C.; Fabbri, C.; Porcelli, S.; Drago, A.; Spina, E.; De Ronchi, D.; Serretti, A. Pharmacogenetics of Antidepressants. Front. Pharmacol. 2011, 2, 6. [Google Scholar] [CrossRef]
- Rj, B.; Gh, V.; L, T. Bipolar Depression: A Major Unsolved Challenge. Int. J. Bipolar Disord. 2020, 8. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Rush, A.J.; Wisniewski, S.R.; Nierenberg, A.A.; Warden, D.; Ritz, L.; Norquist, G.; Howland, R.H.; Lebowitz, B.; McGrath, P.J.; et al. Evaluation of Outcomes with Citalopram for Depression Using Measurement-Based Care in STAR*D: Implications for Clinical Practice. Am. J. Psychiatry 2006, 163, 28–40. [Google Scholar] [CrossRef]
- Targum, S.D.; Schappi, J.; Koutsouris, A.; Bhaumik, R.; Rapaport, M.H.; Rasgon, N.; Rasenick, M.M. A Novel Peripheral Biomarker for Depression and Antidepressant Response. Mol. Psychiatry 2022, 27, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Mann, J.J. Depression. Lancet Lond. Engl. 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Orsolini, L.; Pompili, S.; Tempia Valenta, S.; Salvi, V.; Volpe, U. C-Reactive Protein as a Biomarker for Major Depressive Disorder? Int. J. Mol. Sci. 2022, 23, 1616. [Google Scholar] [CrossRef]
- Maes, M.; Yirmyia, R.; Noraberg, J.; Brene, S.; Hibbeln, J.; Perini, G.; Kubera, M.; Bob, P.; Lerer, B.; Maj, M. The Inflammatory & Neurodegenerative (I&ND) Hypothesis of Depression: Leads for Future Research and New Drug Developments in Depression. Metab. Brain Dis. 2009, 24, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.; Gomez, R.; Williams, G.; Lembke, A.; Lazzeroni, L.; Murphy, G.M.; Schatzberg, A.F. HPA Axis in Major Depression: Cortisol, Clinical Symptomatology and Genetic Variation Predict Cognition. Mol. Psychiatry 2017, 22, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Czarny, P.; Wigner, P.; Galecki, P.; Sliwinski, T. The Interplay between Inflammation, Oxidative Stress, DNA Damage, DNA Repair and Mitochondrial Dysfunction in Depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 80, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Gałecki, P.; Talarowska, M. Neurodevelopmental Theory of Depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 80, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Uchida, S.; Yamagata, H.; Seki, T.; Watanabe, Y. Epigenetic Mechanisms of Major Depression: Targeting Neuronal Plasticity. Psychiatry Clin. Neurosci. 2018, 72, 212–227. [Google Scholar] [CrossRef]
- Gałecki, P.; Talarowska, M. Inflammatory Theory of Depression. Psychiatr. Pol. 2018, 52, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, D.R.; Rapaport, M.H.; Miller, B.J. A Meta-Analysis of Blood Cytokine Network Alterations in Psychiatric Patients: Comparisons between Schizophrenia, Bipolar Disorder and Depression. Mol. Psychiatry 2016, 21, 1696–1709. [Google Scholar] [CrossRef] [PubMed]
- Nobis, A.; Zalewski, D.; Waszkiewicz, N. Peripheral Markers of Depression. J. Clin. Med. 2020, 9, 3793. [Google Scholar] [CrossRef] [PubMed]
- Osimo, E.F.; Pillinger, T.; Rodriguez, I.M.; Khandaker, G.M.; Pariante, C.M.; Howes, O.D. Inflammatory Markers in Depression: A Meta-Analysis of Mean Differences and Variability in 5,166 Patients and 5,083 Controls. Brain. Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef]
- Fiksdal, A.; Hanlin, L.; Kuras, Y.; Gianferante, D.; Chen, X.; Thoma, M.V.; Rohleder, N. Associations Between Symptoms of Depression and Anxiety and Cortisol Responses to and Recovery from Acute Stress. Psychoneuroendocrinology 2019, 102, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bidirectional Relationship of Depression and Inflammation: Double Trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef]
- Krishnadas, R.; Cavanagh, J. Depression: An Inflammatory Illness? J. Neurol. Neurosurg. Psychiatry 2012, 83, 495–502. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Mood Disorders and Allostatic Load. Biol. Psychiatry 2003, 54, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Protection and Damage from Acute and Chronic Stress: Allostasis and Allostatic Overload and Relevance to the Pathophysiology of Psychiatric Disorders - PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/15677391/ (accessed on 6 August 2024).
- Sapolsky, R.M.; Romero, L.M.; Munck, A.U. How Do Glucocorticoids Influence Stress Responses? Integrating Permissive, Suppressive, Stimulatory, and Preparative Actions. Endocr. Rev. 2000, 21, 55–89. [Google Scholar] [CrossRef] [PubMed]
- Du Clos, T.W. Function of C-Reactive Protein. Ann. Med. 2000, 32, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Zipfel, P.F.; Skerka, C. Complement Regulators and Inhibitory Proteins. Nat. Rev. Immunol. 2009, 9, 729–740. [Google Scholar] [CrossRef]
- Luo, X.; Fang, Z.; Lin, L.; Xu, H.; Huang, Q.; Zhang, H. Plasma Complement C3 and C3a Are Increased in Major Depressive Disorder Independent of Childhood Trauma. BMC Psychiatry 2022, 22, 741. [Google Scholar] [CrossRef]
- Pillai, A.; Bruno, D.; Nierenberg, J.; Pandya, C.; Feng, T.; Reichert, C.; Ramos-Cejudo, J.; Osorio, R.; Zetterberg, H.; Blennow, K.; et al. Complement Component 3 Levels in the Cerebrospinal Fluid of Cognitively Intact Elderly Individuals with Major Depressive Disorder. Biomark. Neuropsychiatry 2019, 1, 100007. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Dinan, T.; Leonard, B.E. Changes in Immunoglobulin, Complement and Acute Phase Protein Levels in the Depressed Patients and Normal Controls. J. Affect. Disord. 1994, 30, 283–288. [Google Scholar] [CrossRef]
- Shatri, H.; Purnamandala; Hidayat, R.; Sinto, R.; Widhani, A.; Putranto, R.; Purnamasari, R.D.; Ginanjar, E.; Jasirwan, C.O.M. The Correlation of Anxiety and Depression with C3 and C4 Levels and Systemic Lupus Erythematosus Activity. BMC Psychiatry 2023, 23, 785. [Google Scholar] [CrossRef]
- Wei, J.; Liu, Y.; Zhao, L.; Yang, X.; Ni, P.; Wang, Y.; Li, T.; Ma, X. Plasma Complement Component 4 Increases in Patients with Major Depressive Disorder. Neuropsychiatr. Dis. Treat. 2017, 14, 37–41. [Google Scholar] [CrossRef]
- Alexander, J.J. Blood-Brain Barrier (BBB) and the Complement Landscape. Mol. Immunol. 2018, 102, 26–31. [Google Scholar] [CrossRef]
- Rose-John, S. Interleukin-6 Signalling in Health and Disease. F1000Research 2020, 9, F1000. [Google Scholar] [CrossRef]
- Kaur, S.; Bansal, Y.; Kumar, R.; Bansal, G. A Panoramic Review of IL-6: Structure, Pathophysiological Roles and Inhibitors. Bioorg. Med. Chem. 2020, 28, 115327. [Google Scholar] [CrossRef] [PubMed]
- Ting, E.Y.-C.; Yang, A.C.; Tsai, S.-J. Role of Interleukin-6 in Depressive Disorder. Int. J. Mol. Sci. 2020, 21, 2194. [Google Scholar] [CrossRef]
- Solmi, M.; Suresh Sharma, M.; Osimo, E.F.; Fornaro, M.; Bortolato, B.; Croatto, G.; Miola, A.; Vieta, E.; Pariante, C.M.; Smith, L.; et al. Peripheral Levels of C-Reactive Protein, Tumor Necrosis Factor-α, Interleukin-6, and Interleukin-1β across the Mood Spectrum in Bipolar Disorder: A Meta-Analysis of Mean Differences and Variability. Brain. Behav. Immun. 2021, 97, 193–203. [Google Scholar] [CrossRef]
- Vuong, E.; Nothling, J.; Lombard, C.; Jewkes, R.; Peer, N.; Abrahams, N.; Seedat, S. Peripheral Adiponectin Levels in Anxiety, Mood, Trauma- and Stressor-Related Disorders: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2020, 260, 372–409. [Google Scholar] [CrossRef] [PubMed]
- Scotece, M.; Conde, J.; López, V.; Lago, F.; Pino, J.; Gómez-Reino, J.J.; Gualillo, O. Adiponectin and Leptin: New Targets in Inflammation. Basic Clin. Pharmacol. Toxicol. 2014, 114, 97–102. [Google Scholar] [CrossRef]
- Paz-Filho, G.; Mastronardi, C.; Franco, C.B.; Wang, K.B.; Wong, M.-L.; Licinio, J. Leptin: Molecular Mechanisms, Systemic pro-Inflammatory Effects, and Clinical Implications. Arq. Bras. Endocrinol. Metabol. 2012, 56, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Pérez, A.; Sánchez-Jiménez, F.; Vilariño-García, T.; Sánchez-Margalet, V. Role of Leptin in Inflammation and Vice Versa. Int. J. Mol. Sci. 2020, 21, 5887. [Google Scholar] [CrossRef] [PubMed]
- Ouchi, N.; Walsh, K. Adiponectin as an Anti-Inflammatory Factor. Clin. Chim. Acta Int. J. Clin. Chem. 2007, 380, 24–30. [Google Scholar] [CrossRef]
- Choi, H.M.; Doss, H.M.; Kim, K.S. Multifaceted Physiological Roles of Adiponectin in Inflammation and Diseases. Int. J. Mol. Sci. 2020, 21, 1219. [Google Scholar] [CrossRef]
- Robinson, K.; Prins, J.; Venkatesh, B. Clinical Review: Adiponectin Biology and Its Role in Inflammation and Critical Illness. Crit. Care 2011, 15, 221. [Google Scholar] [CrossRef] [PubMed]
- Leal, G.; Bramham, C.R.; Duarte, C.B. BDNF and Hippocampal Synaptic Plasticity. Vitam. Horm. 2017, 104, 153–195. [Google Scholar] [CrossRef] [PubMed]
- Kowiański, P.; Lietzau, G.; Czuba, E.; Waśkow, M.; Steliga, A.; Moryś, J. BDNF: A Key Factor with Multipotent Impact on Brain Signaling and Synaptic Plasticity. Cell. Mol. Neurobiol. 2018, 38, 579–593. [Google Scholar] [CrossRef]
- Porter, G.A.; O’Connor, J.C. Brain-Derived Neurotrophic Factor and Inflammation in Depression: Pathogenic Partners in Crime? World J. Psychiatry 2022, 12, 77–97. [Google Scholar] [CrossRef]
- Yang, T.; Nie, Z.; Shu, H.; Kuang, Y.; Chen, X.; Cheng, J.; Yu, S.; Liu, H. The Role of BDNF on Neural Plasticity in Depression. Front. Cell. Neurosci. 2020, 14, 82. [Google Scholar] [CrossRef] [PubMed]
- Correia, A.S.; Cardoso, A.; Vale, N. BDNF Unveiled: Exploring Its Role in Major Depression Disorder Serotonergic Imbalance and Associated Stress Conditions. Pharmaceutics 2023, 15, 2081. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, F.; Rossetti, A.C.; Racagni, G.; Gass, P.; Riva, M.A.; Molteni, R. Brain-Derived Neurotrophic Factor: A Bridge between Inflammation and Neuroplasticity. Front. Cell. Neurosci. 2014, 8, 430. [Google Scholar] [CrossRef] [PubMed]
- Banwell, N.; Michel, S.; Senn, N. Greenspaces and Health: Scoping Review of Studies in Europe. Public Health Rev. 2024, 45, 1606863. [Google Scholar] [CrossRef]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and Mental Health: An Ecosystem Service Perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef] [PubMed]
- Reklaitiene, R.; Grazuleviciene, R.; Dedele, A.; Virviciute, D.; Vensloviene, J.; Tamosiunas, A.; Baceviciene, M.; Luksiene, D.; Sapranaviciute-Zabazlajeva, L.; Radisauskas, R.; et al. The Relationship of Green Space, Depressive Symptoms and Perceived General Health in Urban Population. Scand. J. Public Health 2014, 42, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Song, B.; Cho, K.S.; Lee, I.-S. Therapeutic Potential of Volatile Terpenes and Terpenoids from Forests for Inflammatory Diseases. Int. J. Mol. Sci. 2020, 21, 2187. [Google Scholar] [CrossRef] [PubMed]
- Gonzales-Inca, C.; Pentti, J.; Stenholm, S.; Suominen, S.; Vahtera, J.; Käyhkö, N. Residential Greenness and Risks of Depression: Longitudinal Associations with Different Greenness Indicators and Spatial Scales in a Finnish Population Cohort. Health Place 2022, 74, 102760. [Google Scholar] [CrossRef]
- Bray, I.; Reece, R.; Sinnett, D.; Martin, F.; Hayward, R. Exploring the Role of Exposure to Green and Blue Spaces in Preventing Anxiety and Depression among Young People Aged 14-24 Years Living in Urban Settings: A Systematic Review and Conceptual Framework. Environ. Res. 2022, 214, 114081. [Google Scholar] [CrossRef]
- Beil, K.; Hanes, D. The Influence of Urban Natural and Built Environments on Physiological and Psychological Measures of Stress--a Pilot Study. Int. J. Environ. Res. Public. Health 2013, 10, 1250–1267. [Google Scholar] [CrossRef]
- Zimmerman, M.; Martinez, J.H.; Young, D.; Chelminski, I.; Dalrymple, K. Severity Classification on the Hamilton Depression Rating Scale. J. Affect. Disord. 2013, 150, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, M.P.; DeVille, N.V.; Elliott, E.G.; Schiff, J.E.; Wilt, G.E.; Hart, J.E.; James, P. Associations between Nature Exposure and Health: A Review of the Evidence. Int. J. Environ. Res. Public. Health 2021, 18, 4790. [Google Scholar] [CrossRef] [PubMed]
- Kellert, S.R.; Wilson, E.O. The Biophilia Hypothesis; Island Press, 1995. [Google Scholar]
- Lederbogen, F.; Kirsch, P.; Haddad, L.; Streit, F.; Tost, H.; Schuch, P.; Wüst, S.; Pruessner, J.C.; Rietschel, M.; Deuschle, M.; et al. City Living and Urban Upbringing Affect Neural Social Stress Processing in Humans. Nature 2011, 474, 498–501. [Google Scholar] [CrossRef]
- Xu, C.; Miao, L.; Turner, D.; DeRubeis, R. Urbanicity and Depression: A Global Meta-Analysis. J. Affect. Disord. 2023, 340, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Liu, N.; Polemiti, E.; Garcia-Mondragon, L.; Tang, J.; Liu, X.; Lett, T.; Yu, L.; Nöthen, M.M.; Feng, J.; et al. Effects of Urban Living Environments on Mental Health in Adults. Nat. Med. 2023, 29, 1456–1467. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, K. Urbanization and Mental Health. Ind. Psychiatry J. 2009, 18, 75–76. [Google Scholar] [CrossRef]
- Lecic-Tosevski, D. Is Urban Living Good for Mental Health? Curr. Opin. Psychiatry 2019, 32, 204–209. [Google Scholar] [CrossRef]
- Liu, Z.; Chen, X.; Cui, H.; Ma, Y.; Gao, N.; Li, X.; Meng, X.; Lin, H.; Abudou, H.; Guo, L.; et al. Green Space Exposure on Depression and Anxiety Outcomes: A Meta-Analysis. Environ. Res. 2023, 231, 116303. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. Int. J. Environ. Res. Public. Health 2017, 14, 851. [Google Scholar] [CrossRef] [PubMed]
- Li, D.Q. Shinrin-Yoku: The Art and Science of Forest Bathing. Penguin UK, 2018; ISBN 978-0-241-34696-9. [Google Scholar]
- Forest Medicine – Nova Science Publishers.
- Bj, P.; Y, T.; T, K.; T, K.; Y, M. The Physiological Effects of Shinrin-Yoku (Taking in the Forest Atmosphere or Forest Bathing): Evidence from Field Experiments in 24 Forests across Japan. Environ. Health Prev. Med. 2010, 15. [Google Scholar] [CrossRef]
- Kim, T.-H.; Jeong, G.-W.; Baek, H.-S.; Kim, G.-W.; Sundaram, T.; Kang, H.-K.; Lee, S.-W.; Kim, H.-J.; Song, J.-K. Human Brain Activation in Response to Visual Stimulation with Rural and Urban Scenery Pictures: A Functional Magnetic Resonance Imaging Study. Sci. Total Environ. 2010, 408, 2600–2607. [Google Scholar] [CrossRef]
- Kim, G.-W.; Jeong, G.-W.; Kim, T.-H.; Baek, H.-S.; Oh, S.-K.; Kang, H.-K.; Lee, S.-G.; Kim, Y.S.; Song, J.-K. Functional Neuroanatomy Associated with Natural and Urban Scenic Views in the Human Brain: 3.0T Functional MR Imaging. Korean J. Radiol. 2010, 11, 507–513. [Google Scholar] [CrossRef]
- Jo, H.; Song, C.; Miyazaki, Y. Physiological Benefits of Viewing Nature: A Systematic Review of Indoor Experiments. Int. J. Environ. Res. Public. Health 2019, 16, 4739. [Google Scholar] [CrossRef] [PubMed]
- Ikei, H.; Komatsu, M.; Song, C.; Himoro, E.; Miyazaki, Y. The Physiological and Psychological Relaxing Effects of Viewing Rose Flowers in Office Workers. J. Physiol. Anthropol. 2014, 33, 6. [Google Scholar] [CrossRef] [PubMed]
- Levandovski, R.; Pfaffenseller, B.; Carissimi, A.; Gama, C.S.; Hidalgo, M.P.L. The Effect of Sunlight Exposure on Interleukin-6 Levels in Depressive and Non-Depressive Subjects. BMC Psychiatry 2013, 13, 75. [Google Scholar] [CrossRef] [PubMed]
- Penckofer, S.; Kouba, J.; Byrn, M.; Ferrans, C.E. Vitamin D and Depression: Where Is All the Sunshine? Issues Ment. Health Nurs. 2010, 31, 385. [Google Scholar] [CrossRef]
- Hedblom, M.; Gunnarsson, B.; Iravani, B.; Knez, I.; Schaefer, M.; Thorsson, P.; Lundström, J.N. Reduction of Physiological Stress by Urban Green Space in a Multisensory Virtual Experiment. Sci. Rep. 2019, 9, 10113. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.S.; Lim, Y.-R.; Lee, K.; Lee, J.; Lee, J.H.; Lee, I.-S. Terpenes from Forests and Human Health. Toxicol. Res. 2017, 33, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Soudry, Y.; Lemogne, C.; Malinvaud, D.; Consoli, S.-M.; Bonfils, P. Olfactory System and Emotion: Common Substrates. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2011, 128, 18–23. [Google Scholar] [CrossRef]
- Lemke, H.; Probst, S.; Warneke, A.; Waltemate, L.; Winter, A.; Thiel, K.; Meinert, S.; Enneking, V.; Breuer, F.; Klug, M.; et al. The Course of Disease in Major Depressive Disorder Is Associated With Altered Activity of the Limbic System During Negative Emotion Processing. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2022, 7, 323–332. [Google Scholar] [CrossRef]
- dos Santos, É.R.Q.; Maia, J.G.S.; Fontes-Júnior, E.A.; Maia, C. do S.F. Linalool as a Therapeutic and Medicinal Tool in Depression Treatment: A Review. Curr. Neuropharmacol. 2022, 20, 1073–1092. [Google Scholar] [CrossRef]
- Harada, H.; Kashiwadani, H.; Kanmura, Y.; Kuwaki, T. Linalool Odor-Induced Anxiolytic Effects in Mice. Front. Behav. Neurosci. 2018, 12, 241. [Google Scholar] [CrossRef] [PubMed]
- Milanos, S.; Elsharif, S.A.; Janzen, D.; Buettner, A.; Villmann, C. Metabolic Products of Linalool and Modulation of GABAA Receptors. Front. Chem. 2017, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Machado, K. da C.; Islam, M.T.; Ali, E.S.; Rouf, R.; Uddin, S.J.; Dev, S.; Shilpi, J.A.; Shill, M.C.; Reza, H.M.; Das, A.K.; et al. A Systematic Review on the Neuroprotective Perspectives of Beta-Caryophyllene. Phytother. Res. PTR 2018, 32, 2376–2388. [Google Scholar] [CrossRef] [PubMed]
- Scandiffio, R.; Geddo, F.; Cottone, E.; Querio, G.; Antoniotti, S.; Gallo, M.P.; Maffei, M.E.; Bovolin, P. Protective Effects of (E)-β-Caryophyllene (BCP) in Chronic Inflammation. Nutrients 2020, 12, 3273. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Fan, M.; An, C.; Ni, F.; Huang, W.; Luo, J. A Narrative Review of Molecular Mechanism and Therapeutic Effect of Cannabidiol (CBD). Basic Clin. Pharmacol. Toxicol. 2022, 130, 439–456. [Google Scholar] [CrossRef]
- Rohrer, J.; Lupo, N.; Bernkop-Schnürch, A. Advanced Formulations for Intranasal Delivery of Biologics. Int. J. Pharm. 2018, 553, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Keller, L.-A.; Merkel, O.; Popp, A. Intranasal Drug Delivery: Opportunities and Toxicologic Challenges during Drug Development. Drug Deliv. Transl. Res. 2022, 12, 735–757. [Google Scholar] [CrossRef] [PubMed]
- Felger, J.C.; Lotrich, F.E. Inflammatory Cytokines in Depression: Neurobiological Mechanisms and Therapeutic Implications. Neuroscience 2013, 246, 199. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.W.; Kim, Y.K. Neuroinflammation and Cytokine Abnormality in Major Depression: Cause or Consequence in That Illness? World J. Psychiatry 2016, 6, 283–293. [Google Scholar] [CrossRef]
- Lamers, F.; Milaneschi, Y.; Smit, J.H.; Schoevers, R.A.; Wittenberg, G.; Penninx, B.W.J.H. Longitudinal Association Between Depression and Inflammatory Markers: Results From the Netherlands Study of Depression and Anxiety. Biol. Psychiatry 2019, 85, 829–837. [Google Scholar] [CrossRef]
- Lamers, F.; Milaneschi, Y.; de Jonge, P.; Giltay, E.J.; Penninx, B.W.J.H. Metabolic and Inflammatory Markers: Associations with Individual Depressive Symptoms. Psychol. Med. 2018, 48, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Ting, E.Y.-C.; Yang, A.C.; Tsai, S.-J. Role of Interleukin-6 in Depressive Disorder. Int. J. Mol. Sci. 2020, 21, 2194. [Google Scholar] [CrossRef]
- Erta, M.; Quintana, A.; Hidalgo, J. Interleukin-6, a Major Cytokine in the Central Nervous System. Int. J. Biol. Sci. 2012, 8, 1254–1266. [Google Scholar] [CrossRef] [PubMed]
- Kummer, K.K.; Zeidler, M.; Kalpachidou, T.; Kress, M. Role of IL-6 in the Regulation of Neuronal Development, Survival and Function. Cytokine 2021, 144, 155582. [Google Scholar] [CrossRef] [PubMed]
- Ting, E.Y.-C.; Yang, A.C.; Tsai, S.-J. Role of Interleukin-6 in Depressive Disorder. Int. J. Mol. Sci. 2020, 21, 2194. [Google Scholar] [CrossRef] [PubMed]
- Daray, F.M.; Grendas, L.N.; Arena, Á.R.; Tifner, V.; Álvarez Casiani, R.I.; Olaviaga, A.; Chiapella, L.C.; Vázquez, G.; Penna, M.B.; Hunter, F.; et al. Decoding the Inflammatory Signature of the Major Depressive Episode: Insights from Peripheral Immunophenotyping in Active and Remitted Condition, a Case–Control Study. Transl. Psychiatry 2024, 14, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Del Prado-Audelo, M.L.; Cortés, H.; Caballero-Florán, I.H.; González-Torres, M.; Escutia-Guadarrama, L.; Bernal-Chávez, S.A.; Giraldo-Gomez, D.M.; Magaña, J.J.; Leyva-Gómez, G. Therapeutic Applications of Terpenes on Inflammatory Diseases. Front. Pharmacol. 2021, 12, 704197. [Google Scholar] [CrossRef]
- Araruna, M.E.; Serafim, C.; Alves Júnior, E.; Hiruma-Lima, C.; Diniz, M.; Batista, L. Intestinal Anti-Inflammatory Activity of Terpenes in Experimental Models (2010-2020): A Review. Mol. Basel Switz. 2020, 25, 5430. [Google Scholar] [CrossRef]
- de las Heras, B.; Hortelano, S. Molecular Basis of the Anti-Inflammatory Effects of Terpenoids. Inflamm. Allergy Drug Targets 2009, 8, 28–39. [Google Scholar] [CrossRef]
- Maruani, J.; Geoffroy, P.A. Multi-Level Processes and Retina-Brain Pathways of Photic Regulation of Mood. J. Clin. Med. 2022, 11, 448. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Guo, M.; Zhang, D.; Cheng, S.-Y.; Liu, M.; Ding, J.; Scherer, P.E.; Liu, F.; Lu, X.-Y. Adiponectin Is Critical in Determining Susceptibility to Depressive Behaviors and Has Antidepressant-like Activity. Proc. Natl. Acad. Sci. USA 2012, 109, 12248–12253. [Google Scholar] [CrossRef] [PubMed]
- Herder, C.; Schmitt, A.; Budden, F.; Reimer, A.; Kulzer, B.; Roden, M.; Haak, T.; Hermanns, N. Longitudinal Associations between Biomarkers of Inflammation and Changes in Depressive Symptoms in Patients with Type 1 and Type 2 Diabetes. Psychoneuroendocrinology 2018, 91, 216–225. [Google Scholar] [CrossRef]
- Nicolas, S.; Veyssière, J.; Gandin, C.; Zsürger, N.; Pietri, M.; Heurteaux, C.; Glaichenhaus, N.; Petit-Paitel, A.; Chabry, J. Neurogenesis-Independent Antidepressant-like Effects of Enriched Environment Is Dependent on Adiponectin. Psychoneuroendocrinology 2015, 57, 72–83. [Google Scholar] [CrossRef]
- Hamilton, M. A Rating Scale for Depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
Figure 1.
Significant differences from group comparisons: (a) Green-exposed patients at baseline versus follow-up; (b) Nonexposed versus green-exposed patients at baseline; (c) Nonexposed versus green-exposed patients at follow-up; (d) Nonexposed versus exposed healthy volunteers; (e) Nonexposed healthy volunteers versus nonexposed patients at baseline; (f) Nonexposed healthy volunteers versus nonexposed patients at baseline at follow-up. PT: patients; E: exposed; nE: nonexposed; T0: baseline; T1: follow-up.
Figure 1.
Significant differences from group comparisons: (a) Green-exposed patients at baseline versus follow-up; (b) Nonexposed versus green-exposed patients at baseline; (c) Nonexposed versus green-exposed patients at follow-up; (d) Nonexposed versus exposed healthy volunteers; (e) Nonexposed healthy volunteers versus nonexposed patients at baseline; (f) Nonexposed healthy volunteers versus nonexposed patients at baseline at follow-up. PT: patients; E: exposed; nE: nonexposed; T0: baseline; T1: follow-up.
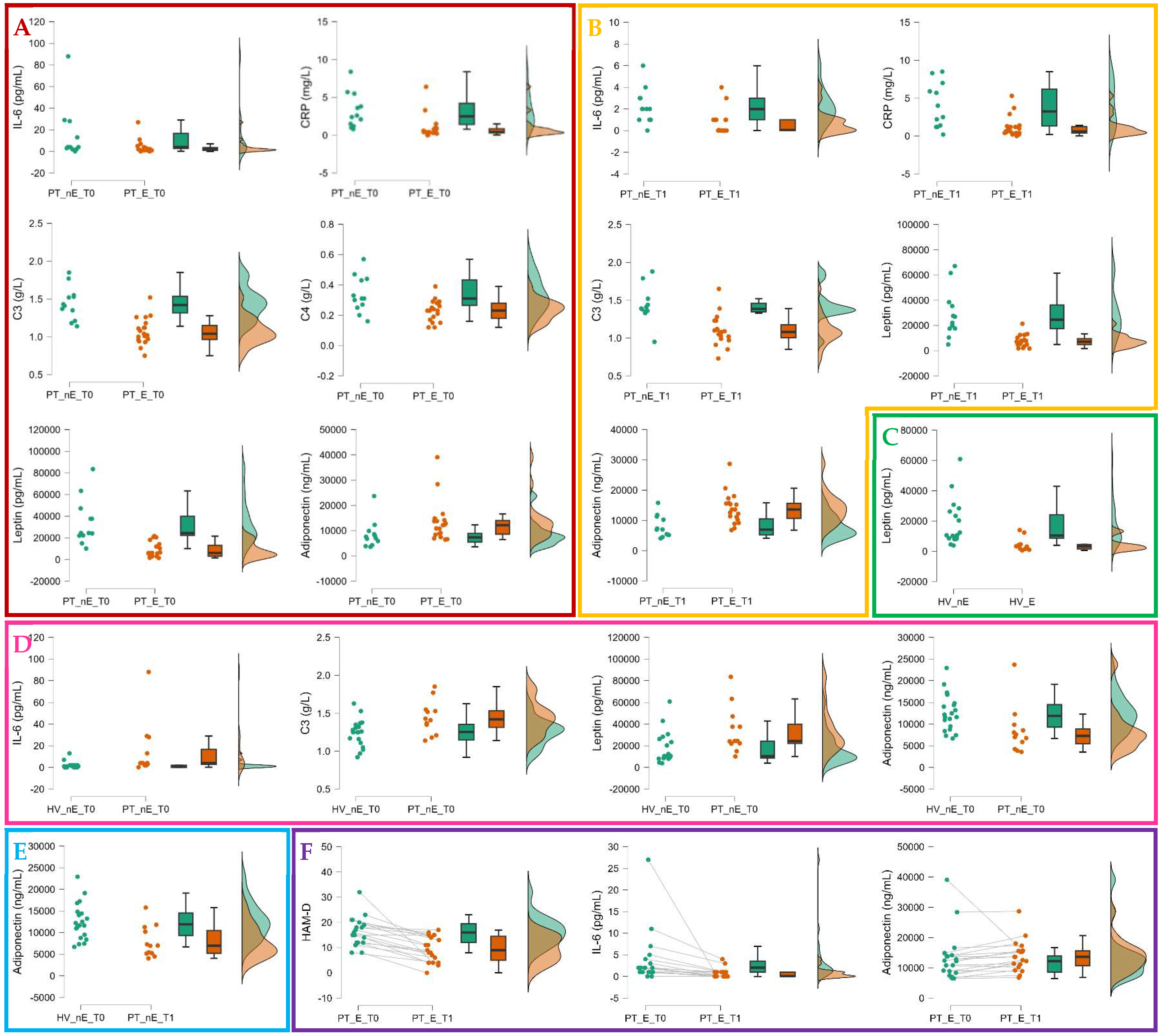

Table 1.
Characteristics of follow-up (n = 31) and drop-out (n = 22) patients at baseline and between-group comparison.
Table 1.
Characteristics of follow-up (n = 31) and drop-out (n = 22) patients at baseline and between-group comparison.
| Total sample of patients at t0 (n=53) |
Completers patients at t0 (n=31) | Drop-out patients (n=22) | Completers vs drop-out patients at t0 |
|
|---|---|---|---|---|
| p-FDR | ||||
| Sociodemographic variables | ||||
| Age, years | 48.0 [31.0; 56.0] | 47.0 [35.0; 59.5] | 49.5 [30.3; 55.0] | .848 |
| Sex, female | 36 (68%) | 22 (71%) | 14 (64%) | .464 |
| Education, years | 13.0 [13.0; 17.0] | 13.0 [13.0; 16.0] | 13.0 [11.5; 16.0] | .424 |
| Clinical variables | ||||
| Duration of illness, years | 6 [2; 14] | 5 [2; 13] | 8 [3; 14] | .718 |
| Numbers of hospitalization | 1 [1; 3] | 1 [1; 2] | 1 [1; 3] | .411 |
| HAM-D | 18 [13; 20] | 17 [12; 20] | 18 [16; 21] | .424 |
| Biological markers | ||||
| IL-6, pg/mL | 2.0 [1.0; 4.0] | 2.0 [1.0; 4.5] | 2.0 [1.0; 2.0] | .411 |
| CRP, mg/L | 0.9 [0.4; 2.1] | 0.9 [0.4; 2.5] | 0.8 [0.4; 1.6] | .810 |
| C3, g/L | 1.18 [1.02; 1.41] | 1.18 [1.02; 1.39] | 1.19 [1.04; 1.41] | .898 |
| C4, g/L | 0.29 [0.23; 0.35] | 0.26 [0.21; 0.31] | 0.32 [0.28; 0.41] | .150 |
| Cortisol, mcg/L | 109 [79; 153] | 105 [79; 127] | 136 [92; 158] | .424 |
| Leptin, pg/L | 10,423 [5,751; 24,111] | 14,202 [5,641; 23,196] | 9,349 [7,124; 22,372] | .999 |
| Adiponectin, ng/L | 8,575 [6,568; 12,303] | 9,087 [6,969; 13,283] | 7,367 [5,999; 11,246] | .411 |
| BDNF, pg/mL | 461.7 [305.5; 823.9] | 402.5 [273.2; 755.5] | 635.4 [427.4; 912.1] | .411 |
Continuous variables are expressed as median and interquartile range [Q1; Q3]; vs: versus; FDR: false discovery rate correction; HAM-D: Hamilton scale for Depression; CRP: C-Reactive Protein; C3: complement fraction 3; C4: complement fraction 4; BDNF: Brain-Derived Neurotrophic Factor.
Table 2.
Characteristics at baseline and six-week follow-up of green exposed and nonexposed patients and between-group and paired-sample comparisons.
Table 2.
Characteristics at baseline and six-week follow-up of green exposed and nonexposed patients and between-group and paired-sample comparisons.
| PT_E_t0 (n=19) |
PT_nE_t0 (n=12) |
PT_E_t1 (n=19) |
PT_nE_t1 (n=12) |
HV_E (n=10) |
HV_nE (n=21) |
PT_E_t0 vs PT_nE_t0 |
PT_E_t1 vs PT_nE_t1 |
HV_E vs HV_nE |
HV_E vs PT_E_t0 |
HV_E vs PT_E_t1 |
HV_nE vs PT_nE_t0 |
HV_nE vs PT_nE_t1 |
PT_E t0 vs t1 |
PT_nE t0 vs t1 |
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p-FDR | p-FDR | p-FDR | p-FDR | p-FDR | p-FDR | p-FDR | p-FDR | p-FDR | |||||||
| Sociodemographic variables | |||||||||||||||
| Age, years | 46.0 [28.0; 50.0] | 54.5 [38.0; 60.5] | - | - | 31.0 [25.0; 33.0] | 40.5 [31.0; 57.0] | .324 | - | .215 | .243 | - | .072 | - | - | - |
| Sex, female | 14 (74%) | 8 (67%) | - | - | 6 (60%) | 15 (71%) | .839 | - | .832 | .966 | - | .812 | - | - | - |
| Education, years | 13.0 [13.0; 17.0] | 13.0 [11.7; 13.7] | - | - | 18.0 [13.0; 18.0] | 13.0 [13.0; 18.0] | .324 | - | .577 | .628 | - | .048 | - | - | - |
| Biological markers | |||||||||||||||
| IL-6, pg/mL | 2.00 [1.00; 3.5] | 4.00 [2.75; 16.75] | 0.05 [0.01; 1.00] | 2.00 [1.00; 3.00] | 0.60 [0.01; 1.60] |
1.00 [0.01; 1.75] | .048 | .005 | .577 | .243 | .966 | .004 | .177 | .002 | .081 |
| CRP, mg/L | 0.4 [0.3; 0.8] | 2.5 [1.4; 4.2] | 0.6 [0.4; 1.2] | 3.2 [1.3; 6.2] | 0.5 [0.3; 1.8] | 0.9 [0.8; 1.5] | .002 | .005 | .324 | .656 | 1.00 | .065 | .094 | .542 | .906 |
| C3, g/L | 1.04 [0.96; 1.15] | 1.42 [1.31; 1.53] | 1.08 [1.00; 1.17] | 1.38 [1.35; 1.39] |
1.09 [1.02; 1.11] |
1.28 [1.16; 1.36] |
.002 | .002 | .075 | .735 | 1.00 | .048 | .052 | .542 | .906 |
| C4, g/L | 0.23 [0.18; 0.28] |
0.31 [0.26; 0.43] |
0.23 [0.18; 0.27] |
0.32 [0.22; 0.36] |
0.20 [0.18; 0.24] |
0.27 [0.22; 0.33] |
.021 | .095 | .215 | .735 | 1.00 | .228 | .431 | .777 | .290 |
| Cortisol, mcg/L | 105 [79; 129] |
110 [71; 125] |
136 [96; 168] |
97 [92; 133] |
125 [112; 144] |
100 [93; 112] |
.855 | .070 | .710 | .628 | .966 | .530 | .356 | .121 | .906 |
| Leptin, pg/L | 6,095 [3,112; 13,061] |
24,444 [22,211; 40,018] |
7,099 [4,871; 9,505] |
24,506 [17,572; 36,166] |
3,192 [1,525; 4,462] |
9,925 [8,554; 26,281] |
.002 | .002 | .004 | .243 | .248 | .017 | .094 | .551 | .290 |
| Adiponectin, ng/L | 12,182 [8,599; 13,960] |
7,309 [5,470; 13,503] |
13,599 [10,650; 15,642] |
6,968 [5,216; 10,479] |
13,141 [10,216; 17,288] |
11,626 [9,314; 14,832] |
.026 | .003 | .722 | .628 | 1.00 | .017 | .016 | .018 | .853 |
| BDNF, pg/mL | 396.7 [268.3; 591.2] |
416.8 [327.3; 1,032.4] |
535.0 [278.9; 1,058.7] |
772.6 [516.7; 1,026.4] |
429.1 [227.4; 712.0] |
234.8 [192.5; 561.7] |
.750 | .372 | .950 | .735 | .966 | .567 | .177 | .110 | .367 |
| Depressive symptoms | |||||||||||||||
| HAM-D, total score | 16.0 [12.0; 19.5] |
18.5 [11.5; 20.0] |
9.0 [5.0; 14.5] |
13.5 [8.7; 16.5] |
- | - | .855 | .188 | - | - | - | - | - | .002 | .855 |
Variables in bold showed a significant between-group difference; continuous variables are expressed as median and interquartile range [Q1; Q3]; vs: versus; PT_E: patients exposed to green between baseline and follow-up; PT_nE: patients nonexposed to green between baseline and follow-up; t0: baseline; t1: six-weeks follow-up; HV_E: healthy volunteers exposed to green for the six weeks before blood drawing; HV_nE: healthy volunteers nonexposed to green for the six weeks before blood drawing; FDR: False Discovery Rate correction; CRP: C-Reactive Protein; C3: Complement fraction 3; C4: Complement fraction 4; BDNF: Brain-Derived Neurotrophic Factor.
Table 3.
Regression models: contribution of the exposure to green environments to the follow-up outcomes.
Table 3.
Regression models: contribution of the exposure to green environments to the follow-up outcomes.
| Regressor | B | 95%CI of B | p | Outcomes at follow-up |
|---|---|---|---|---|
| Exposure to green environments between baseline and follow-up | -3.850 | -7.627; -.028 | .048 | Depressive symptoms (HAMD, total score) |
| -1.420 | -2.503; -.338 | .012 | IL-6, pg/mL | |
| 3,795 | 1,022; 6,567 | .009 | Adiponectin, ng/L |
CI: confidence interval; IL: interleukin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



