
Submitted:
11 January 2025
Posted:
13 January 2025
You are already at the latest version
Abstract
Objective: Liver cirrhosis (LC) progression induces intestinal microbiota abnormalities, such as small intestinal bacterial overgrowth (SIBO), and these changes lead to the inflow of gut pathogens and their degradation products into the vessels, causing cirrhotic complications such as hepatic encephalopathy (HE). Methods: To clarify the relationship between the development of overt HE and SIBO, we conducted a three-year observation after the assessment of SIBO in patients with LC. Results: In the analysis of 107 patients with a mean follow-up duration of 29.4 months, 31 were diagnosed with SIBO and 30 with covert HE. In the Cox multivariate regression analysis for prognosis, the Child-Pugh score, blood urea nitrogen level, and the Union for International Cancer Control (UICC) stage of hepatocellular carcinoma were derived using the following five factors: white blood cell count, blood urea nitrogen level, Child-Pugh score, UICC stage, and serum aspartate aminotransferase level (p = 0.001, hazard ratio [HR] 3.733, 95% confidence interval [CI] 1.592 – 8.754, p = 0.001, HR 1.076, 95% CI 1.030 – 1.123, and p < 0.001, HR 2.767, 95% CI 1.780 – 4.302, respectively). Furthermore, in the Cox multivariate regression analysis for overt HE development, covert HE and methane-producing SIBO were derived using the following four factors: methane-producing SIBO, UICC stage, covert HE, and serum ammonia level (p = 0.038, HR 5.008, 95% CI 1.096 – 22.892 and p = 0.006, HR 8.597, 95% CI 1.881 – 39.291, respectively). Conclusion: M-SIBO positivity was a significant predictor of overt HE.
Keywords:
small intestinal bacterial overgrowth
; hepatic encephalopathy
; liver cirrhosis
1. Introduction
Liver cirrhosis (LC), the ultimate stage of various hepatic conditions, is characterized by the presence of regenerative nodules with a fibrous septum in the whole liver [1]. Chronic viral hepatitis, steatotic liver disease, and autoimmune liver disease are common etiologies of LC. Because of recent advancements in antiviral therapy for viral hepatitis [2], the proportion of patients with LC due to steatotic liver disease, including alcoholic or metabolic-related variants, has significantly increased due to the decrease in the number of those with viral hepatitis [3].
The gut environment is altered by cirrhosis progression: small intestinal bacterial overgrowth (SIBO) [4], increased intestinal wall mucosa permeability [5], and dysfunction of the gut-associated lymphoid tissue immune system [6] occur in patients with LC. Furthermore, the interaction of these pathological gut conditions induces the inflow of gut pathogens and their degradation products, such as lipopolysaccharide, into the vessels, and causes cirrhotic complications, such as spontaneous bacterial peritonitis and hepatic encephalopathy (HE) [7]. Especially in alcohol-related and metabolic-associated steatotic liver diseases, the mechanisms of these pathological gut conditions are more important in the pathogenesis of hepatic inflammation and fibrosis [8,9].
A meta-analysis on the relationship between SIBO and LC revealed that the rate of SIBO positivity in patients with cirrhosis ranges from 34.8% to 47.1% and the odds of LC is 6.83 times higher in SIBO-positive patients. In addition, patients with decompensated cirrhosis complicated with SIBO had a higher frequency than those with compensated cirrhosis (50.5% vs. 31.2%; odds ratio: 2.56), therefore, the frequency of SIBO increases with the progression of LC [4]. We previously reported a cross-sectional study that concluded that the proportion of hydrogen-type SIBO is associated with LC progression [10]. While covert HE and hyperammonemia were previously identified as predictors of overt HE [11,12], we performed a three-year observation to reveal the relationship between overt HE onset and SIBO to assess the influence of the latter on overt HE complications and death.
2. Materials and Methods
2.1. Study Protocol
This was a prospective cohort study conducted at Niigata University. The study was approved by the ethical review board of Niigata University (Approval Number 2023-0209) and was performed as a follow-up study to a previous cross-sectional study [10]. We recruited the participants for the study between May 1, 2019 and December 31, 2020 in hospitalized patients because of LC complications and 121 patients agreed to participate in the study. All patients provided their written informed consent for the prospective observation at the time of case inclusion in the previous cross-sectional study. Physical assessments, including the breath test and number connection tests (NCTs), were performed after managing LC complications. Fourteen patients were excluded because of the administration of poorly absorbable antibiotics at the time of the breath test; therefore, we ended up with 107 participants in the study. After these assessments, we followed up on all 107 patients for three years. New inclusion and exclusion criteria were not established for the current study. The endpoints of the study were all-cause mortality and overt HE development.
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and the ethical guidelines for medical and biological research involving human subjects in Japan. The study protocol is presented in Figure 1.
2.2. Breath Test
The exhaled hydrogen and methane concentrations were measured using a BGA2000D (Laboratory for Expiration Biochemistry Nourishment Metabolism Co., Ltd., Nara, Japan). Fifty grams of glucose or 10 g of lactulose was used as the sugar substrate. Breath measurement was performed three times before the sugar substrate loading to determine the baseline, every 15 min after loading and up to 120 or 180 min.
The diagnostic criteria for SIBO are defined according to the North American consensus: a rise of ≥20 ppm from baseline in hydrogen by 90 min and a level of ≥10 ppm in methane [13]. Furthermore, patients with elevated hydrogen levels were defined as H-SIBO, whereas those with elevated methane levels were defined as M-SIBO, as previously reported [14].
2.3. Neuro-Psychological Tests
NCT-A and NCT-B were performed as the neuro-psychological tests. The NCTs are one of neuro-psychological tests that entails using an iPad to connect the displayed numbers and letters with the fingers for the diagnosis of covert HE. In this study, we used “Neuro-Psychological Tests (v2.1) For iPad” available on the website (https://www.jsh.or.jp/medical/guidelines/medicalinfo/otsuka.html) provided by Otsuka Pharmaceutical Co., Ltd. Patients performed the NCT-A and NCT-B tests, and covert HE was diagnosed based on the obtention of positive results of both NCT tests [15]. The cutoff values were based on a previous report for Japanese patients [16].
2.4. Statistical Analysis
SPSS (version 29.0.2.0; IBM, Armonk, NY, USA) was used to perform the univariate and multivariate Cox regression analyses, and GraphPad Prism Version 8.3.0 (GraphPad Software, Inc., Boston, MA, USA) was used to generate the Kaplan–Meier survival curve.
3. Results
The study cohort included 81 male and 26 female patients (n = 107), with a median age of 70 (40–86) years. Hepatocellular carcinoma (HCC) occurred as a complication in 77 (72.0%) patients. Thirty-one (29.0%) patients were diagnosed with SIBO using the breath test, and 30 (28.0%) patients were diagnosed with covert HE by the neuro-psychological tests. The mean observation period was 29.4 months in the cohort study. The characteristics of our study participants are summarized in Table 1.
First, the Cox regression analysis was performed to examine the relationship between each of the clinical characteristics and all-cause mortality. In this study, 72.0% of the patients had HCCs as mentioned above; thus, the clinical stage of HCC determined by the Union for International Cancer Control (UICC) or the Barcelona Clinic Liver Cancer (BCLC) was the most significant prognostic factor in the univariate analysis (p < 0.001, hazard ratio [HR] 2.323, 95% confidence interval [CI] 1.540–3.503, and p < 0.001, HR 2.259, 95% CI 1.480–3.446, respectively, Table 2). The high levels of total bilirubin (T-bil), aspartate aminotransferase (AST), blood urea nitrogen (BUN), and white blood cell (WBC) count were also associated with a poor prognosis, while the Child-Pugh grade was not significantly associated with the prognosis in the univariate analysis (p = 0.193, HR 1.701, 95% CI 0.764 – 3.790). T-bil is one of the components of the Child-Pugh Score, and the Child-Pugh score is significantly associated with poor prognosis. We performed the multivariate Cox regression analysis using these five factors: WBC, BUN, Child-Pugh score, UICC stage of HCC, and AST. As the result of the analysis, the Child-Pugh score, BUN, and UICC stage of HCC were found to be significantly associated with disease prognosis (p = 0.001, HR 3.733, 95% CI 1.592 – 8.754, p = 0.001, HR 1.076, 95% CI 1.030 – 1.123, and p < 0.001, HR 2.767, 95% CI 1.780 – 4.302, respectively; Table 2). Even if T-bil was used as a factor in the multivariate analysis, T-bil, BUN, and UICC stage of HCC also remained the same as they were in the analysis performed using the Child-Pugh score (Table S1).
Next, the Cox regression analysis was performed to examine the relationship between each of the clinical characteristics and overt HE. In the univariate analysis, M-SIBO positivity and UICC stage of HCC were identified as significantly associated factors (p = 0.010, HR 7.228, 95% CI 1.614 – 32.361 and p = 0.029, HR 2.046, 95% CI 1.076 – 3.889, respectively; Table 3). While covert HE and serum ammonia levels were not significantly associated with overt HE in the univariate analysis (p = 0.067, HR 4.058 95% CI 0.908 – 18.142 and p = 0.079, HE 1.016 95%CI 0.998 – 1.035), covert HE and hyperammonemia were previously identified as predictive factors for overt HE. Therefore, the multivariate Cox regression analysis was performed using four factors: M-SIBO, UICC stage, covert HE, and serum ammonia levels, and covert HE and M-SIBO were identified in the analysis (p = 0.038, HR 5.008, 95% CI 1.096 – 22.892 and p = 0.006, HR 8.597, 95% CI 1.881 – 39.291, respectively; Table 3). Furthermore, the multivariate analysis was performed using only two factors (M-SIBO and the UICC stage), that were significantly associated with overt HE in the univariate analysis, and only M-SIBO emerged as an independently associated factor in this analysis (Table S2).
Based on the results of the multiple Cox regression analysis, the patients were divided into four groups according to the presence or absence of covert HE and M-SIBO, and a cumulative incidence analysis was performed. The group of patients with neither covert HE nor M-SIBO had a cumulative three-year incidence rate of 5.9%, compared with 46.7% in the group of patients with both covert HE and M-SIBO (p = 0.017, Figure 2). Per our findings, both M-SIBO and covert HE are risk factors for overt HE development.
4. Discussion
In a previous cross-sectional study, we reported that H-SIBO was significantly associated with LC progression and covert HE [10]. Additionally, a meta-analysis reported that patients with decompensated cirrhosis complicated with SIBO with higher frequency than the patients with compensated cirrhosis [4]. In detail, only H-SIBO was measured in the meta-analysis, and it determined SIBO. Based on the results of the meta-analysis and our previous study, both the frequency of covert HE and the H-SIBO complication rate increased proportionately with LC progression. As a result, a statistically significant association was observed between H-SIBO and covert HE.
In the present observational study, H-SIBO had no significant relationship with the incidence of overt HE, whereas M-SIBO was a predictor of overt HE. Methane has been reported to decrease intestinal transit velocity in animal studies [17] and to be associated with constipation in humans, with the severity of constipation correlating with the methane concentration [18,19]. It is well-known that constipation is one of the triggers of overt HE [20]; therefore, M-SIBO-positive patients with LC are considered more constipated and more prone to encephalopathy than M-SIBO-negative patients. M-SIBO-positive patients exist regardless of their hepatic function; therefore, they are considered to have the potential to develop overt HE when their liver function deteriorates.
The key drugs for the treatment of overt HE and the prevention of recurrence in patients with LC are synthetic disaccharides and poorly absorbable oral antibiotics. Synthetic disaccharides, represented by lactulose, are expected to have a laxative effect and improve the gut microbiome and flora [21,22]. Synthetic disaccharides have been reported to improve not only HE but also the mortality rate of both liver-related and overall in patients with HE in a systematic review [23], and the agents are the treatment of first choice for overt HE in all the American Association for the Study of Liver Disease, the European Association for the Study of the Liver, and the Japan Society of Hepatology guidelines [24,25,26]. On the other hand, poorly absorbable oral antibiotics, such as rifaximin, are expected to inhibit ammonia-producing bacteria in the gut [27]. Rifaximin has been reported to prevent HE recurrence in a systematic review and may also improve the HE recovery and mortality rates [28]. Poorly absorbable oral antibiotics are also recommended by the guideline to use for patients with HE, the same as lactulose [26].
Rifaximin is also used in the treatment of SIBO, and its usefulness has already been reported with the improved rate of treatment with rifaximin for SIBO being 70% [29]. However, to the best of our knowledge, no reports were found that lactulose was administered for therapy in patients with SIBO in our literature survey. Therefore, for the treatment of patients with H-SIBO complicated by cirrhosis, poorly absorbable oral antibiotics may be more suitable. Methanobrevibacter smithii, the predominant methanogenic bacterium in the human gut, is resistant to many antibiotics; therefore, antibiotics are not considered effective for the treatment of M-SIBO [30,31,32]. Furthermore, lactulose is frequently used to treat constipation. Therefore, for the treatment of patients with H-SIBO complicated by cirrhosis, synthetic disaccharides may be more suitable. In addition, serum ammonia levels and neuro-psychological tests are considered to be performed more frequently to prevent the complication of overt HE in patients with M-SIBO.
5. Conclusions
M-SIBO positivity was a significant predictor of overt HE. In patients with M-SIBO, careful follow-up is needed to avoid complicating overt HE in patients with cirrhosis. While there is no evidence regarding drug selection for patients with SIBO and HE, and further studies are needed, poorly absorbable oral antibiotics for H-SIBO and synthetic disaccharides for M-SIBO may be more suitable by considering the pathophysiology of each SIBO.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. Cox regression analyses for the patient’s prognosis using total bilirubin levels. Table S2. Cox regression analyses for the onset of overt hepatic encephalopathy without serum ammonia levels and covert hepatic encephalopathy.
Author Contributions
Conceptualization, A.T., K.K., and J.Y.; methodology, A.S. and S.T.; formal analysis, A.S.; data curation, K.Y., H.Y., T.W., T.I., Y.K., K.T., and H.A.; writing—original draft preparation, A.S.; writing—review and editing, A.S.; visualization, A.S.; supervision, T.S. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Japan Agency for Medical Research and Development, grant number #24fk0210113h0003).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the ethical review board of Niigata University (Approval number, 2023-0209; Approval date, October 27, 2023).
Informed Consent Statement
Written informed consent was obtained from all patients involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| LC | Liver cirrhosis |
| SIBO | Small intestinal bacterial overgrowth |
| HE | Hepatic encephalopathy |
| H-SIBO | Hydrogen producing SIBO |
| M-SIBO | Methane producing SIBO |
| NCT | Number connection test |
| HCC | Hepatocellular carcinoma |
| UICC | Union for International Cancer Control |
| BCLC | Barcelona Clinic Liver Cancer |
| HR | Hazard ratio |
| CI | Confidence interval |
| T-bil | Total bilirubin |
| AST | Aspartate aminotransferase |
| BUN | Blood urea nitrogen |
| WBC | White blood cell |
References
- Schuppan, D.; Afdhal, N.H. Liver cirrhosis. Lancet 2008, 371, 838-851.
- Marshall, A.D.; Willing, A.R.; Kairouz, A.; Cunningham, E.B.; Wheeler, A.; O’Brien, N.; Perera, V.; Ward, J.W.; Hiebert, L.; Degenhardt, L.; et al. Direct-acting antiviral therapies for hepatitis c infection: Global registration, reimbursement, and restrictions. Lancet Gastroenterol Hepatol. 2024, 9, 366-382.
- Enomoto, H.; Akuta, N.; Hikita, H.; Suda, G.; Inoue, J.; Tamaki, N.; Ito, K.; Akahane, T.; Kawaoka, T.; Morishita, A.; et al. Etiological changes of liver cirrhosis and hepatocellular carcinoma-complicated liver cir-rhosis in japan: Updated nationwide survey from 2018 to 2021. Hepatol Res. 2024, 54, 763-772.
- Maslennikov, R.; Pavlov, C.; Ivashkin, V. Small intestinal bacterial overgrowth in cirrhosis: systematic review and meta-analysis. Hepatol. Int. 2018, 12, 567–576. [CrossRef]
- Nicoletti, A.; Ponziani, F.R.; Biolato, M.; Valenza, V.; Marrone, G.; Sganga, G.; Gasbarrini, A.; Miele, L.; Grieco, A. Intestinal permeability in the pathogenesis of liver damage: From non-alcoholic fatty liver disease to liver transplantation. World J. Gastroenterol. 2019, 25, 4814–4834. [CrossRef]
- Bernsmeier, C.; van der Merwe, S.; Périanin, A. Innate immune cells in cirrhosis. J. Hepatol. 2020, 73, 186–201. [CrossRef]
- Wiest, R.; Lawson, M.; Geuking, M. Pathological bacterial translocation in liver cirrhosis. J. Hepatol. 2014, 60, 197–209. [CrossRef]
- Ishikawa, M.; Uemura, M.; Matsuyama, T.; Matsumoto, M.; Ishizashi, H.; Kato, S.; Morioka, C.; Fujimoto, M.; Kojima, H.; Yoshiji, H.; et al. Potential Role of Enhanced Cytokinemia and Plasma Inhibitor on the Decreased Activity of Plasma ADAMTS13 in Patients with Alcoholic Hepatitis: Relationship to Endotoxemia. Alcohol. Clin. Exp. Res. 2010, 34, S25–S33. [CrossRef]
- Creely, S.J.; McTernan, P.G.; Kusminski, C.M.; Fisher f, M.; Da Silva, N.F.; Khanolkar, M.; Evans, M.; Harte, A.L.; Kumar, S. Lipopolysaccharide activates an innate immune system response in human adipose tissue in obesity and type 2 diabetes. Am. J. Physiol. Endocrinol. Metab. 2007, 292, E740-747.
- Yokoyama, K.; Sakamaki, A.; Takahashi, K.; Naruse, T.; Sato, C.; Kawata, Y.; Tominaga, K.; Abe, H.; Sato, H.; Tsuchiya, A.; et al. Hydrogen-producing small intestinal bacterial overgrowth is associated with hepatic en-cephalopathy and liver function. PLoS One 2022, 17, e0264459.
- Patidar, K.R.; Thacker, L.R.; Wade, J.B.; Sterling, R.K.; Sanyal, A.J.; Siddiqui, M.S.; Matherly, S.C.; Stravitz, R.T.; Puri, P.; Luketic, V.A.; et al. Covert hepatic encephalopathy is independently associated with poor sur-vival and increased risk of hospitalization. Am. J. Gastroenterol. 2014, 109, 1757-1763.
- Vierling, J.M.; Mokhtarani, M.; Brown, R.S.; Jr., Mantry, P.; Rockey, D.C.; Ghabril, M.; Rowell, R.; Jurek, M.; Coakley, D.F.; Scharschmidt, B.F. Fasting blood ammonia predicts risk and frequency of hepatic encephalopathy episodes in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2016, 14, 903-906.
- Quigley, E.M.; Abu-Shanab, A. Small intestinal bacterial overgrowth. Infect. Dis. Clin. N. Am. 2010, 24, 943-959.
- Suri, J.; Kataria, R.; Malik, Z.; Parkman, H.P.; Schey, R. Elevated methane levels in small intestinal bacterial overgrowth suggests delayed small bowel and colonic transit. Medicine 2018, 97, e10554. [CrossRef]
- Kato, A.; Tanaka, H.; Kawaguchi, T.; Kanazawa, H.; Iwasa, M.; Sakaida, I.; Moriwaki, H.; Murawaki, Y.; Suzuki, K.; Okita, K. Nutritional management contributes to improvement in minimal hepatic encephalopathy and quality of life in patients with liver cirrhosis: A preliminary, prospective, open-label study. Hepatol. Res. 2012, 43, 452–458. [CrossRef]
- Kawaguchi, T.; Konishi, M.; Kato, A.; Kato, M.; Kooka, Y.; Sawara, K.; Endo, R.; Torimura, T.; Suzuki, K.; Takikawa, Y. Updating the neuropsychological test system in Japan for the elderly and in a modern touch screen tablet society by resetting the cut-off values. Hepatol. Res. 2017, 47, 1335–1339. [CrossRef]
- Pimentel, M.; Lin, H.C.; Enayati, P.; Burg, B.v.D.; Lee, H.-R.; Chen, J.H.; Park, S.; Kong, Y.; Conklin, J. Methane, a gas produced by enteric bacteria, slows intestinal transit and augments small intestinal contractile activity. Am. J. Physiol. Liver Physiol. 2006, 290, G1089–G1095. [CrossRef]
- Chatterjee, S.; Park, S.; Low, K.; Kong, Y.; Pimentel, M. The Degree of Breath Methane Production in IBS Correlates with the Severity of Constipation. Am. J. Gastroenterol. 2007, 102, 837–841. [CrossRef]
- Kunkel, D.; Basseri, R.J.; Makhani, M.D.; Chong, K.; Chang, C.; Pimentel, M. Methane on Breath Testing Is Associated with Constipation: A Systematic Review and Meta-analysis. Dig. Dis. Sci. 2011, 56, 1612–1618. [CrossRef]
- Pantham, G.; Post, A.; Venkat, D.; Einstadter, D.; Mullen, K.D. A New Look at Precipitants of Overt Hepatic Encephalopathy in Cirrhosis. Dig. Dis. Sci. 2017, 62, 2166–2173. [CrossRef]
- Sharma, P.; Sharma, B.C.; Puri, V.; Sarin, S.K. An open-label randomized controlled trial of lactulose and probiotics in the treatment of minimal hepatic encephalopathy. Eur. J. Gastroenterol. Hepatol. 2008, 20, 506–511. [CrossRef]
- Malaguarnera, M.; Gargante, M.P.; Malaguarnera, G.; Salmeri, M.; Mastrojeni, S.; Rampello, L.; Pennisi, G.; Volti, G.L.; Galvano, F. Bifidobacterium combined with fructo-oligosaccharide versus lactulose in the treatment of patients with hepatic encephalopathy. Eur. J. Gastroenterol. Hepatol. 2010, 22, 199–206. [CrossRef]
- Gluud, L.L.; Vilstrup, H.; Morgan, M.Y. Nonabsorbable disaccharides for hepatic encephalopathy: A systematic review and meta-analysis. Hepatology 2016, 64, 908–922. [CrossRef]
- Easl clinical practice guidelines on the management of hepatic encephalopathy. J. Hepatol. 2022, 77, 807-824.
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [CrossRef]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Asaoka, Y.; Ueno, Y.; Ogawa, K.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for Liver Cirrhosis 2020. J. Gastroenterol. 2021, 56, 593–619. [CrossRef]
- Sama, C.; Morselli-Labate, A.M.; Pianta, P.; Lambertini, L.; Berardi, S.; Martini, G. Clinical effects of rifaximin in patientswith hepatic encephalopathy intolerant or nonresponsive to previous lactulose treatment: An open-label, pilot study. Curr. Ther. Res. 2004, 65, 413–422. [CrossRef]
- Kwok, R.; Tse, Y.K.; Wong, G.L.; Ha, Y.; Lee, A.U.; Ngu, M.C.; Wong, V.S. Systematic review with meta-analysis: non-invasive assessment of non-alcoholic fatty liver disease—The role of transient elastography and plasma cytokeratin-18 fragments. Aliment. Pharmacol. Ther. 2014;39, 254–269.
- Gatta, L.; Scarpignato, C. Systematic review with meta-analysis: rifaximin is effective and safe for the treatment of small intestine bacterial overgrowth. Aliment. Pharmacol. Ther. 2017, 45, 604–616. [CrossRef]
- Pimentel, M.; Chang, C.; Chua, K.S.; Mirocha, J.; DiBaise, J.; Rao, S.; Amichai, M. Antibiotic Treatment of Constipation-Predominant Irritable Bowel Syndrome. Dig. Dis. Sci. 2014, 59, 1278–1285. [CrossRef]
- Rezaie, A.; Pimentel, M.; Rao, S.S. How to test and treat small intestinal bacterial overgrowth: An evidence-based approach. Curr. Gastroenterol Rep. 2016, 18, 8.
- Low, K.; Hwang, L.; Hua, J.; Zhu, A.; Morales, W.; Pimentel, M. A Combination of Rifaximin and Neomycin Is Most Effective in Treating Irritable Bowel Syndrome Patients With Methane on Lactulose Breath Test. J. Clin. Gastroenterol. 2010, 44, 547–550. [CrossRef]
Figure 1.
Study protocol. LC, liver cirrhosis.
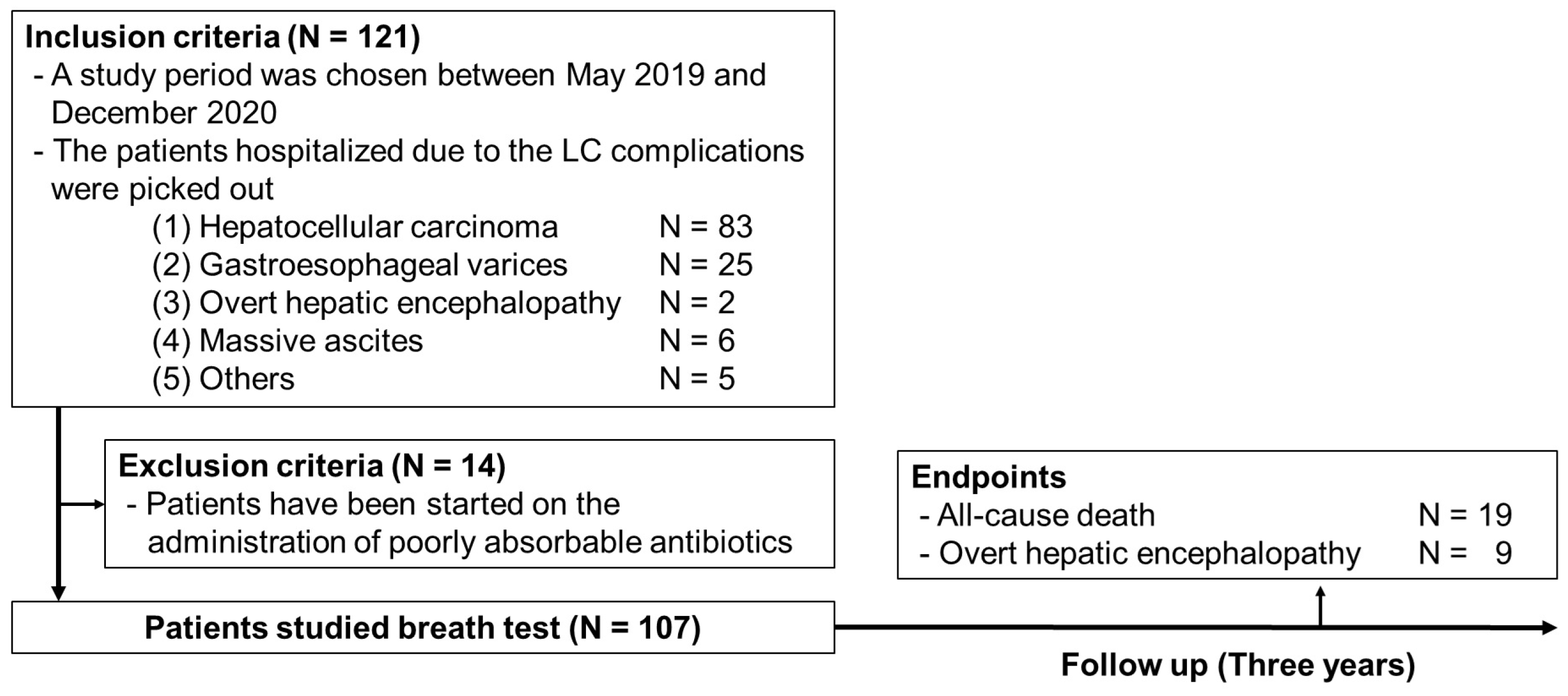
Figure 2.
Cumulative incidence curve of overt hepatic encephalopathy in at-risk patients. The patients were divided into four groups according to the presence or absence of covert HE and M-SIBO. The group of patients with neither covert HE nor M-SIBO had a cumulative three-year incidence rate of 5.9%, the group with covert HE without M-SIBO was 11.9%, the group with M-SIBO without covert HE was 19.8%, and the group of patients with both covert HE and M-SIBO was 46.7% (p = 0.017). M-SIBO, methane-producing small intestinal bacterial overgrowth; CHE, covert hepatic encephalopathy.
Figure 2.
Cumulative incidence curve of overt hepatic encephalopathy in at-risk patients. The patients were divided into four groups according to the presence or absence of covert HE and M-SIBO. The group of patients with neither covert HE nor M-SIBO had a cumulative three-year incidence rate of 5.9%, the group with covert HE without M-SIBO was 11.9%, the group with M-SIBO without covert HE was 19.8%, and the group of patients with both covert HE and M-SIBO was 46.7% (p = 0.017). M-SIBO, methane-producing small intestinal bacterial overgrowth; CHE, covert hepatic encephalopathy.
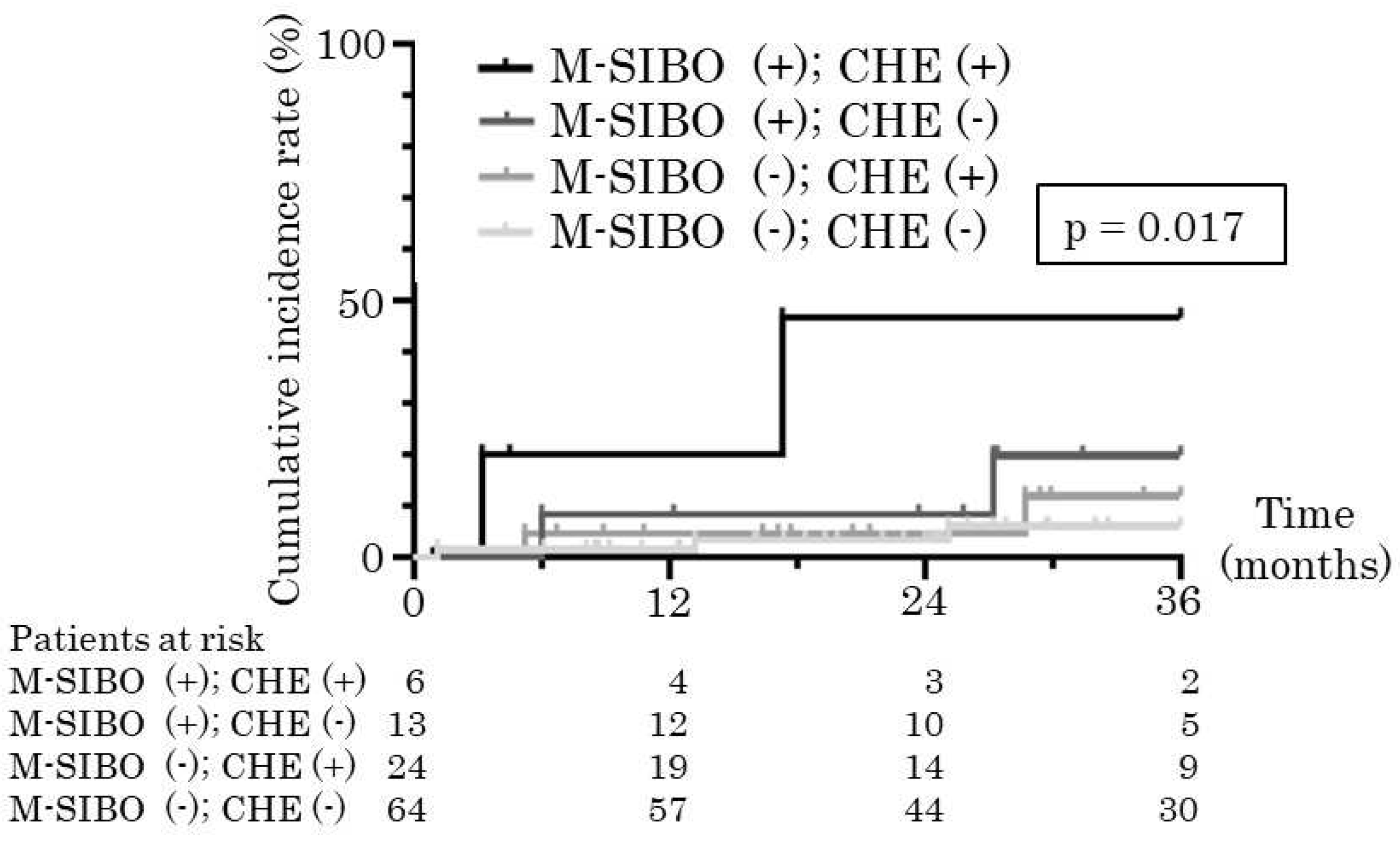

Table 1.
Characteristics of our study participants.
| median (min – max) | median (min – max) | ||
| or n (%) | N = 107 | or n (%) | N = 107 |
| Age, years | 70 (40 - 86) | Cholinesterase, U/L | 210 (47 – 484) |
| Gender | Albumin, g/dL | 3.8 (2.1 – 5.0) | |
| Males | 81 (75.7) | Total bilirubin, mg/dL | 0.9 (0.3 – 14.2) |
| Females | 26 (24.3) | Prothrombin time, % | 92 (25 - 131) |
| Body mass index, kg/m2 | 24.8 (12.6 - 47.7) | Ammonia, μg/dL | 64 (28 - 242) |
| The etiology of liver cirrhosis | Creatinine, mg/dL | 0.81 (0.45 – 3.31) | |
| Hepatitis B virus | 20 (18.7) | Blood urea nitrogen, mg/dL | 16 (5 – 61) |
| Hepatitis C virus | 23 (21.5) | White blood cell count, x103/µL | 4.3 (1.3 – 14.8) |
| Alcoholic liver disease | 31 (29.0) | Platelet count, x104/µL | 10.9 (2.6 – 26.3) |
| Non-alcoholic steatohepatitis | 23 (21.5) | Child-Pugh score | 5 (5 – 12) |
| Others | 10 ( 9.3) | Child Pugh grade (A/B/C) | 85 / 17 / 5 |
| PPI administration | 63 (58.9) | ALBI score | -2.45 (-0.47 – -3.32) |
| HCC complication | 77 (72.0) | mALBI grade (1/2a/2b/3) | 38 / 29 / 31 / 9 |
| UICC stage of HCC (I/II/III/IV) | 18 / 29 / 17 / 13 | Covert HE | 30 (28.0) |
| BCLC stage of HCC (I/II/III/IV) | 30 / 31 / 14 / 2 | SIBO | 31 (29.0) |
| Aspartate aminotransferase, U/L | 36 (12 – 209) | Hydrogen producing SIBO | 16 (15.0) |
| Alanine aminotransferase, U/L | 29 (10 – 217) | Methane producing SIBO | 19 (17.8) |
| Alkaline Phosphatase, U/L | 281 (64 – 3147) | Observation period, m | 29.4 (0.9 – 36.0) |
| Gamma-glutamyl transpeptidase, U/L | 68 (13 – 691) | ||
| PPI, proton pump inhibitor; HCC, hepatocellular carcinoma; UICC, Union for International Cancer Control; BCLC, Barcelona Clinic Liver Cancer; ALBI, Albumin-Bilirubin; mALBI, modified ALBI; HE, hepatic encephalopathy; SIBO, small intestinal bacterial overgrowth. | |||
Table 2.
Cox regression analyses for the patient’s prognosis.
| univariate analysis | multivariate analysis | |||
| p value | hazard ratio | p value | hazard ratio | |
| Age, years | 0.948 | 1.002 (0.956 – 1.049) | ||
| Gender | 0.210 | 0.392 (0.090 – 1.696) | ||
| Body mass index, kg/m2 | 0.431 | 1.031 (0.955 – 1.114) | ||
| The etiology of liver cirrhosis | ||||
| Hepatitis B virus | ||||
| Hepatitis C virus | ||||
| Alcoholic liver disease | ||||
| Non-alcoholic steatohepatitis | ||||
| Others | ||||
| PPI administration | 0.109 | 0.474 (0.191 – 1.181) | ||
| HCC complication | 0.102 | 3.399 (0.785 – 14.721) | ||
| UICC stage of HCC (0/I/II/III/IV) | < 0.001* | 2.323 (1.540 – 3.503) | < 0.001* | 2.767 (1.780 – 4.302) |
| BCLC stage of HCC (0/I/II/III/IV) | < 0.001* | 2.259 (1.480 – 3.446) | ||
| Aspartate aminotransferase, U/L | 0.037* | 1.013 (1.001 – 1.025) | 0.074 | |
| Alanine aminotransferase, U/L | 0.146 | 1.013 (0.996 – 1.030) | ||
| Alkaline Phosphatase, U/L | ||||
| Gamma-glutamyl transpeptidase, U/L | ||||
| Cholinesterase, U/L | ||||
| Albumin, g/dL | 0.424 | 0.712 (0.309 – 1.639) | ||
| Total bilirubin, mg/dL | 0.025* | 1.247 (1.028 – 1.513) | ||
| Prothrombin time, % | 0.768 | 1.004 (0.979 – 1.030) | ||
| Ammonia, μg/dL | 0.348 | 1.006 (0.993 – 1.020) | ||
| Creatinine, mg/dL | 0.316 | 1.587 (0.643 – 3.914) | ||
| Blood urea nitrogen, mg/dL | 0.009* | 1.047 (1.011 – 1.084) | 0.001* | 1.076 (1.030 – 1.123) |
| White blood cell count, x103/µL | 0.021* | 1.193 (1.027 – 1.385) | 0.626 | |
| Platelet count, x104/µL | 0.173 | 1.052 (0.978 – 1.131) | ||
| Child-Pugh score | 0.471 | 1.117 (0.827 – 1.508) | ||
| Child Pugh grade (A/B/C) | 0.193 | 1.701 (0.764 – 3.790) | 0.001* | 3.733 (1.592 – 8.754) |
| ALBI score | 0.392 | 1.448 (0.620 – 3.381) | ||
| mALBI grade (1/2a/2b/3) | 0.732 | 1.086 (0.676 – 1.747) | ||
| Covert HE | 0.479 | 1.418 (0.539 – 3.733) | ||
| SIBO | 0.483 | 1.414 (0.537 – 3.721) | ||
| Hydrogen producing SIBO | 0.130 | 2.348 (0.777 – 7.096) | ||
| Methane producing SIBO | 0.983 | 1.013 (0.295 – 3.479) | ||
| PPI, proton pump inhibitor; HCC, hepatocellular carcinoma; UICC, Union for International Cancer Control; BCLC, Barcelona Clinic Liver Cancer; ALBI, Albumin-Bilirubin; mALBI, modified ALBI; HE, hepatic encephalopathy; SIBO, small intestinal bacterial overgrowth. *: P value < 0.05. | ||||
Table 3.
Cox regression analyses for the onset of overt hepatic encephalopathy.
| univariate analysis | multivariate analysis | |||
| p value | hazard ratio | p value | hazard ratio | |
| Age, years | 0.631 | 0.982 (0.914 – 1.056) | ||
| Gender | 0.218 | 2.562 (0.573 – 11.458) | ||
| Body mass index, kg/m2 | 0.159 | 1.079 (0.971 – 1.199) | ||
| The etiology of liver cirrhosis | ||||
| Hepatitis B virus | ||||
| Hepatitis C virus | ||||
| Alcoholic liver disease | ||||
| Non-alcoholic steatohepatitis | ||||
| Others | ||||
| PPI administration | 0.310 | 0.460 (0.102 – 2.062) | ||
| HCC complication | 0.406 | 2.455 (0.295 – 20.423) | ||
| UICC stage of HCC (0/I/II/III/IV) | 0.029* | 2.046 (1.076 – 3.889) | 0.065 | |
| BCLC stage of HCC (0/I/II/III/IV) | 0.088 | 1.804 (0.917 – 3.551) | ||
| Aspartate aminotransferase, U/L | 0.065 | 1.017 (0.999 – 1.035) | ||
| Alanine aminotransferase, U/L | 0.587 | 1.009 (0.977 – 1.041) | ||
| Alkaline Phosphatase, U/L | ||||
| Gamma-glutamyl transpeptidase, U/L | ||||
| Cholinesterase, U/L | ||||
| Albumin, g/dL | 0.178 | 0.443 (0.135 – 1.449) | ||
| Total bilirubin, mg/dL | 0.189 | 1.202 (0.913 – 1.581) | ||
| Prothrombin time, % | 0.406 | 0.985 (0.949 – 1.021) | ||
| Ammonia, μg/dL | 0.079 | 1.016 (0.998 – 1.035) | 0.145 | |
| Creatinine, mg/dL | 0.476 | 1.719 (0.387 – 7.632) | ||
| Blood urea nitrogen, mg/dL | 0.338 | 1.036 (0.964 – 1.114) | ||
| White blood cell count, x103/µL | 0.391 | 0.804 (0.488 – 1.324) | ||
| Platelet count, x104/µL | 0.443 | 0.940 (0.803 – 1.100) | ||
| Child-Pugh score | 0.148 | 1.328 (0.904 – 1.952) | ||
| Child Pugh grade (A/B/C) | 0.165 | 2.270 (0.714 – 7.221) | ||
| ALBI score | 0.109 | 2.625 (0.806 – 8.551) | ||
| mALBI grade (1/2a/2b/3) | 0.129 | 1.826 (0.840 – 3.970) | ||
| Covert HE | 0.067 | 4.058 (0.908 – 18.142) | 0.038* | 5.008 (1.096 – 22.892) |
| SIBO | 0.015* | 7.610 (1.475 – 39.625) | ||
| Hydrogen producing SIBO | 0.131 | 3.553 (0.685 – 18.415) | ||
| Methane producing SIBO | 0.010* | 7.228 (1.614 – 32.361) | 0.006* | 8.597 (1.881 – 39.291) |
| HE, hepatic encephalopathy; PPI, proton pump inhibitor; HCC, hepatocellular carcinoma; UICC, Union for International Cancer Control; BCLC, Barcelona Clinic Liver Cancer; ALBI, Albumin-Bilirubin; mALBI, modified ALBI; HE, hepatic encephalopathy; SIBO, small intestinal bacterial overgrowth. *: P value < 0.05. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



