
Submitted:
10 January 2025
Posted:
13 January 2025
You are already at the latest version
Abstract
Every year, more than 150,000 cases of multiple myeloma (MM) are diagnosed worldwide, and over 100,000 deaths caused by this malignancy are recorded. MM incidence is increasing globally, particularly in high-income countries and in the male population aged ≥50. While advances in treatment strategies have led to improvement of survival over the past decades, MM remains incurable in a large percentage of cases. Importantly, about one third of patients diagnosed with MM are >75 years old and are characterized by relatively low fitness or frailty. These patients are more vulnerable to stressors and present a lower resistance to cancer and related treatment. Therefore, patients’ fitness and frailty should become part of standard assessment in MM, and flexible therapeutic options should apply. A careful review of studies investigating the management of frail patients with MM, strongly supports the use of a dynamic assessment of effectiveness and adverse events associated with current treatments in the context of patient-specific frailty and co-morbidities.
Keywords:
multiple myeloma
; frailty
; immunotherapy
; CAR-T
; bispecific antibodies
1. Introduction
Multiple myeloma (MM) is an aggressive hematologic malignancy, characterized by an excess of plasma cells (PCs) in the bone marrow (BM). Progression of this complex disease, occurs through a multistep process starting with a pre-malignant phase, the so called monoclonal gammopathy of undetermined significance (MGUS) [1], followed by an intermediate stage, the smouldering multiple myeloma (SMM), characterized by a higher disease burden than MGUS [2]. This pre-malignant, asymptomatic phase, may prelude to MM development (Figure 1).
Malignant transformation leading to MM clinical onset begins inside lymph nodes’ germinal centers [3], where B-lymphocytes undergo genetic and epigenetic alterations providing them with higher proliferation potential. Subsequently, they move to BM where they conclude their differentiation to PCs by interacting with the immune microenvironment [4]. Malignant PC produce serum immunoglobulins and activate osteoclasts, resulting in bone tissue demolition, and focal injuries leading to bone fractures [5].
From a genomic viewpoint, cytogenetic anomalies such as immunoglobulin heavy chain locus translocations and hyperdiploid karyotypes due to chromosomal trisomies, are already detectable in both MGUS and SMM [6]. However, although these alterations provide the bases of the neoplastic transformation of plasma cell clones, only 1% of MGUS cases do progress to MM [7], thereby suggesting that the switch to symptomatic disease may be due to sudden, very low frequency, randomly acquired genomic events [8].
While progression to SMM driven by the acquisition of additional oncogenic events does not usually produce end-organ damage [9], in some cases MM features might already be detectable [10]. Indeed, MM may be clinically suspected in the presence of malignant plasma cell levels>10% in the BM, and unusually large amounts of “M spike” serum proteins. The weakening of the immune system, anemia, bleeding disorders, hypercalcemia, kidney failure and bone lesions are some of the symptoms observed in advanced MM stages [11,12,13].
Samuel Solly was the first to describe MM more than 150 years ago. His two patients referred fatigue, bone pain and multiple fractures as main symptoms and only after their death, Solly discovered that their BM had been replaced by a “red substance” filled with distinctively looking large cells [14]. Notably, paleopathological investigations have traced this disease back to prehistoric era by documenting 25 ascertained cases of MM from 14 different countries worldwide dated from prehistory to modern times [15]
In 2014, the International Myeloma Working Group (IMWG) updated MM diagnostic criteria for MM to allow earlier diagnosis and initiation of treatment prior to the occurrence of organ damage. Important progress has been made since, with significant improvements in survival [12]. Nevertheless, further efforts and additional resources are needed to treat MM, particularly in unfit and frail patients, that do not tolerate and/or recover from systemic therapy, thereby requiring modifications of treatment protocols. Evaluation of functional health status of MM patients is as important as that of myeloma-related risk factors. Indeed, patients aged≥65 and those with long-term disabilities are known to be highly heterogeneous and to require proper assessment strategies to define their frailty profile and most appropriate treatments. Usually, they are not participating in clinical trials and are not eligible to receive treatments of choice, including hematopoietic stem cell transplantation, myeloablative chemotherapies and enhanced supportive care, but undergo unconventional therapies. To provide strategies of potential use in the selection of relevant therapeutic options, in this review we analyze treatment protocols recommended for "frail" and older MM patients.
2. Frailty: Definition, Categorization and Impact on Disease Outcomes
Aging is a gradual and progressive physiological process, associated with several modifications in vital organs and metabolism, and increased susceptibility to multiple vulnerabilities. About one third of newly diagnosed MM patients are >75 years old at diagnosis. Multiple comorbidities, frequently observed in older adults, including chronic kidney disease, osteoporosis, and iron/vitamin deficiencies may contribute to confound the clinical picture thereby delaying diagnosis, that is often reached when MM-related organ dysfunction is already present[16].
While different subgroups of older and frail patients may be identified based on specific characteristics, such as functional status, cognition, socio-economic factors, nutritional status, independence in daily activities, and fitness, they overall represent a poorly investigated population in clinical trials. Indeed, due to normal decline of organ and system functions, older adults are at higher risk of experiencing iatrogenic adverse events[17]. Therefore, extensive expertise and comprehensive geriatric assessment (GA) are required to correctly identify personalized management and therapy, and to predict tolerance and adverse outcomes[18].
Several GA scoring systems have been proposed. The IMWG has designed a tool to stratify patients considering age, comorbidities, cognitive and physical conditions[17,19]. The Freiburg Comorbidity Index (Initial Myeloma Comorbidity Index – I-MCI) is based on Karnofsky performance status, lung and renal impairment[20]. The Revised Myeloma Comorbidity Index (R-MCI) has extended its assessment to disease cytogenetics[21,22].Moreover, the Geriatric Assessment in Haematology (GAH), a 30-item scale directed to older patients diagnosed with haematological malignancies dedicates a special attention to psychometric evaluation, including, in addition to standard comorbidities, polypharmacy, gait speed, mood, daily activities, health status, nutrition, and mental status[20,23]. Additional GA tools and scoring systems have also been developed more recently[24,25,26].
The goal of personalized treatment in older patients should be to provide a therapy effectively prolonging survival without affecting patients’ quality of life. A balance between benefit on disease control and conservation of quality of life, physical independence and hospitalization should be pursued. A global assessment should also include palliative therapies and hospice care. On this line, multiple recommendations were formulated to guide the use of specific drugs[18,27]. As an example, dexamethasone plays a key role in MM treatment. However, despite its effectiveness, high-dose therapy may be associated with neurological and psychiatric disorders, iatrogenic diabetes mellitus, gastrointestinal bleeding, higher risk of infection, and glucocorticoid-induced osteoporosis [18]. The toxicity profile of this key player in MM treatment has led to the development of low-dose dexamethasone administration schedules intended for older and unfit patients. The formulation of fixed duration treatment schedules to reduce toxicity while preserving effectiveness is currently under investigation[18,28,29].
3. Choice of Treatment Regimen in Older MM Patients Ineligible to Receive Transplantation
Frailty status represents a key factor in the management of older patients with MM. Those above 75 years of age are immediately classified as intermediately fit or frail[30], since the use of aggressive treatments in these patients may lead to negative outcomes. Indeed, it has been demonstrated that frail older MM patients have a worse progression-free (PFS) and overall survival (OS) in comparison to fit individuals, and show higher rates of infection and treatment toxicity[22,31]. Therefore, personalized treatments should be administered according to the assigned frailty score. However, the use of different tools leads to a high variability in the definition of frailty in MM, withprevalence rates ranging between 17.2% and 66.0%[24], and treatment is usually determined on a case-by-case basis. Nevertheless, patients aged over 75 are typically deemed transplant ineligible.
The recognition of the importance of the frailty status has led to reconsiderations of MM treatment. Melphalan and prednisone with or without thalidomide (MPT or MP) previously represented the standard of care for these patients[20]. The addition of the anti-CD38 monoclonal antibody (mAb) daratumunab to these drug combinations has led to the achievement of good and long-lasting responses in several patient groups. Following the introduction of frailty assessments, current first-line treatments used in patients with newly diagnosed MM are represented by triplet or quadruplet therapy including VRd (bortezomib/lenalidomide/dexamethasone), DRd (daratumunab/lenalidomide/dexamethasone) and D-VMP (daratumumab, plusbortezomib, melphalan, and prednisone)[12,16]. A longer than 4/5-year survival may be achieved upon treatment with such regimens[32].
VRd has been approved by EMA based on the results of the SWOG S0777 trial. In this phase 3 study, VRd and Rd treatments were compared and addition of bortezomib to lenalidomide/dexamethasone for induction therapy resulted in improved PFS and OS, irrespective of age[33,34]. These results were also confirmed by O’Donnell and colleagues, who reported that in patients older than 75 years, requiring a reduction in the intensity of the VRd regimen, modifications of doses and schedules did not compromise treatment effectiveness[35]. Indeed, their data, obtained from a phase 2 study, underline that the modified VRd regimen was not only well-tolerated and highly effective, but also more appropriate for older patients[36].
Moreover, in a phase 3 trial (IMROZ ClinicalTrials.gov number, NCT03319667), Facon et al. demonstrated that also the addition of the anti-CD38 monoclonal antibody isatuximab to the VRd regimen would be able in slowing the progression of disease in 18 to 80 years of age MM patients. Comparing isatuximab plus VRd and VRd alone, a better PFS was in fact, highlighted in the isatuximab-VRd group than in the VRd group (63.2% vs 45.2%) and a similar safety profile[37].
DRd and D-VMP can also be recommended as initial therapy for elderly and/or frail patients. A phase 3 clinical trial supported the first-line use of DRd for patients with MM ineligible for transplantation, regardless of frailty status[38]. Moreover, a further subgroup analysis, including fit, intermediate, and frail patients, has demonstrated that treatment with DRd results in improved PFS, OS and minimal/measurable residual disease (MRD) , as compared to Rd alone, regardless of age and frailty[39,40]. Remarkably, approval of subcutaneous daratumumab, which is considered non-inferior to intravenous formulation in terms of efficacy and pharmacokinetics and provides an improved safety profile also in relapsed/refractory MM patients, has marked a turning point in the management of frail patients with MM[41] with positive effects on the patients’ quality of life, as well [42]. Other studies have also underlined both a prolonged OS [43]and a 4-fold higher MRD-negativity rate in patients treated with D-VMP compared to those treated with VMP alone even in a frail subgroup[44,45,46].
Notably, however, the use of multiple agent treatment in MM patients over 75 has also been shown to associate with a higher toxicity[47]. Within this context, it is important to consider that high-dose dexamethasone, included since almost 40 years in several drug-combinations for MM treatment [48], is associated with a variety of adverse effects, including neurological disorders, secondary diabetes mellitus, and increased susceptibility to infections[49,50]. Therefore, to allow older, intermediately fit patients to receive and tolerate sufficiently prolonged dexamethasone treatments, dose-adjustment based on the clinical, functional status and comorbidities have been proposed, aimed at managing potentially occurring adverse events [39]. In this context, Stege and colleagues [51] have reported that in frail patients with a median age of 81 years a low dose dexamethasone treatment of up to 10 mg every 2/4 weeks had potential advantages and was not less effective. Moreover, in these patients short-term treatments would be preferable [49,50], as also demonstrated by a randomized phase 3 study where a dose/schedule-adjusted Rd treatment without dexamethasone was used in the maintenance (Rd-R) of intermediately fit patients [28]. Other trials are underway aimed at determining the possibility to omit dexamethasone in older and frail patients. Preliminary data from IFM 2017_03 trial anticipate that in frail NDMM patients, early discontinuation of dexamethasone (after 2 cycles) in the context of daratumumab and lenalidomide treatment is associated with effective and durable responses with a manageable safety profile [18].
Choice of treatment for relapsing elderly patients is even more challenging. A series of factors, including front-line treatment, patient age, long-term side effects, comorbidities, and presence of cytogenetic alterations need to be considered [52,53]. Data from relapsed/refractory MM frail patients enrolled in CANDOR trial have shown that daratumumab in combination with Kd56 (D-Kd) is effective and safe and results in improved PFS without additional toxicity[54]. Importantly, cardiac failure has been shown to occur less frequently in frail patients treated with dexamethasone[54].
Altogether, data available from real world practice regarding older and frail patients are far from optimal. A retrospective analysis on real-world outcomes in about 5000 MM European patients, has underlined that only 61% of these patients reach second line treatment and only 38% the third line [55]. Fact is that patients aged ≥70 years remain at the highest risk for early mortality in the presence of a variety of aging-related vulnerabilities, resulting in a highly heterogeneous population with diverse clinical outcomes. Therefore, tailored therapeutic approaches are required, carefully balancing effectiveness and burden of treatment.
4. CAR T-Cell Therapy in Older Patients
Most recently, MM treatment is being revolutionized by the application of targeted therapies, including those with chimeric antigen receptor (CAR) T cells currently also used in relapsed or refractory MM[56]. Data from the phase 3 CARTITUDE-4 clinical trial have shown that the administration of CAR-T cells targeting the B-cell maturation antigen (BCMA) reduces the risk of disease progression or death by 74% compared to two standard-of-care regimens in relapsed and lenalidomide-refractory MM patients who have previously received one to three lines of treatment [57].
Safety and effectiveness of CAR-T has also been evaluated in elderly patients with R/R MM [57]. Tolerable safety and reasonable effectiveness were observed[58], although frailer patients had a higher treatment-related mortality. Moreover, all grades of immune effector cell-associated neurotoxicity syndrome (ICANS) were slightly higher in the elderly population, even if no differences in grade 3 or higher ICANS were observed [57].Nevertheless, reports on the use of CAR Tcell therapies in older patients are still scarce, the most relevant question being “how old is too old for CAR-T cell therapies in multiple myeloma?”[58]. Clearly, although age per se should not automatically exclude patients from such treatments, related toxicities have to be considered, including not only the most severe events but also low grade ones impacting on quality of life and clinical outcome.
As underlined by Rajeeve and Usmani[59],to correctly manage treatment related toxicities it is critically important to define a right sequence of therapies. However, to be eligible for CAR-T clinical trials, patients have to meet strict criteria of performance status and homeostasis regulation which were established to de-risk the development of treatment-related toxicities. Unfortunately, very few elderly patients meet these requirements. Accordingly, the oldest patients included in two important CAR-T phase 2 clinical trials, namely KarMMa[60] and CARTITUDE-1[61],were78 and 70 years old, respectively. Since the median age at MM diagnosis is of 69 years while the median age of patients admitted in phase 2 clinical trials is of 61 years, clearly older patients tend to be excluded from CAR-T therapy. However, interestingly, retrospective meta-analyses underline that anti-BCMA CAR-T cell therapy in older patients with relapsed MM is as safe and effective as in younger patients[62]. Consistently, in a cohort of 83 patients, including 22 ≥70 years old, Reyes et al have observed that CRS and ICANS rates, days to absolute neutrophil count recovery and incidence of hypogammaglobulinemia were comparable in older and younger patients, without specific geriatric complications[63]. An optimistic view of CAR-T cell therapy in older patients also emerges from a post-hoc analysis of the ZUMA-1 trial, documenting similar clinical effectiveness and safety as in younger patients [64].
On the other hand, Davis et al. have reported that although older/frail patients with RRMM treated with CAR-T cell therapy in a real-world setting do not show excess high-grade toxicities, however, therapy is associated with lower efficacy as compared to non-frail patients [58].
Taken together these data support the concept that advanced chronological age, per se, cannot represent an absolute contraindication for CAR-T cell therapy and that physiologic age should rather be assessed as in defined US therapy programs. As an example, Yates et al. have used a geriatric assessment-guided multidisciplinary clinic (GA-MDC) as a tool to evaluate and select older adults for CAR-T cell therapy, and to provide an effective risk stratification[65]. Therefore, it would be desirable to enclose the geriatric assessments and frailty scores into cellular therapy risk assessment to standardize the selection processes, thereby possibly increasing the number of older patients with MM eligible for CAR-T cell therapy.
5. Bispecific Antibodies
BsAbs are also part of the ongoing revolution in targeted MM therapy and are effectively used in RRMM treatment to enhance the interaction between MM and immune effector cells and facilitate the elimination of malignant cells[66].Bispecific T cell engagers (BiTEs) and DuoBodies have been developed. BiTEs combine into one molecule specificities of a mAb that binds a tumor-associated surface antigen and another,bindingCD3 expressed on the T cell surface, in the absence of an Fc fragment. BiTEs mainly trigger (Figure 2) CD8+ T cell cytotoxic activity resulting in highly efficient lysis of targeted tumor cells[66].
However, although BiTEs easily penetrate tumors thanks to their small size, they are characterized by a short half-life, requiring frequent/continuous infusions[67]. DuoBodies represent evolutions of BiTEs and include two different single-chain variable fragments linked by an Fc domain. Due to their higher molecular size, and binding to neonatal Fc receptor (FcRn), which recycles IgG, their half-life is increased, allowing intermittent dosing. Moreover Fc receptors’ binding also promotes antibody-dependent cytotoxicity (ADCC), phagocytosis and complement-dependent cytotoxicity[68]. BCMA, G protein-coupled receptor class C group 5 member D (GPRC5D), and Fc receptor-like 5 (FcRH5) are the main MM targets (Table 1).
These T cell redirecting therapies are associated with>60% ORR and a median PFS of around 1 year [68]. However, even if first reports are encouraging, the use of BsAbs requires a careful examination of patients >75 years old, particularly because of potential immune adverse events due to excessive cytokine production. Indeed, Dieterle et al. successfully used teclistamab, a humanized BCMAxCD3 IgG-like BsAb, characterized by Fc mutations that stabilize and minimize its immunological effector functions, in octogenarian patients with RRMM, with promising efficacy and reasonable safety[69]. However, the frequent infectious events evidenced in clinical trials, negatively impact patient management[70], and preventive measures are required to mitigate this risk particularly in frail and elderly patients.
6. Treatment of Complications and Adverse Events
Frailty often results in a high incidence of adverse events and treatment discontinuation. Therefore, supportive care, prevention and early identification of complications are crucial for treatment success. Bone disease should be conservatively managed with calcium and vitamin D supplementation, bisphosphonates, and anti-RANKL antibodies, such as denosumab, but may require radiotherapy or orthopaedic surgery[16,27].Infections are a major cause of death among MM older patients due to multiple factors, including disease itself, corticosteroid and treatment-related immunosuppression, and neutropenia. Vaccine prophylaxis against influenza, pneumococcal, and varicella-zoster-virus infections, and pharmacological prophylaxis should be judiciously added to the ongoing treatment. Anemia, present as prior comorbidity or MM-related, could also affect quality of life and impact on old and frail patient equilibrium. This condition may worsen with the initiation of chemotherapy and should be managed by supporting patients with iron supplementation in case of deficiency, erythropoietin-stimulating agents, and red cell transfusions [28].
Clinical signs and symptoms of pain and neuropathy should be carefully evaluated in MM patients. After the initial assessment, pain might represent a warning sign because of its relationship with disease progression or drug-related adverse events [71]. In particular, pain might present in acute and/or chronic form. Its etiology is often multifactorial, and associated with bone disease, fractures, nerve compression, peripheral neuropathy, and infectious [VZV] neuralgias. The management of this disabling condition should be patient and symptom tailored, considering patient’s characteristics and comorbidities, such as chronic kidney disease. In 2018, guidelines for the management of pain in cancer patients (https://www.who.int/publications/i/item/9789241550390) were provided by World Health Organization. Depending on its etiology, pain could be treated pharmacologically with corticosteroids, acetaminophen, neuromodulators, including pregabalin and gabapentin, and opioids. Tricyclic antidepressants, such as serotonin uptake inhibitors, and local anesthetics, including lidocaine and capsaicin, could also be of use[16,71,72]. More specifically, bone active agents, including bisphosphonates or denosumab, or interventional procedures, such as radiotherapy, vertebroplasty, neurolysis, radiofrequency neurotomy, and spinal cord decompression, should be evaluated [73]. Most importantly, frailty and fitness in patients with MM should be considered as dynamic features potentially modified by the initiation of treatment and supportive care [74,75]. Therefore, a flexible approach should be adopted to face treatment modification and to warrant a patient-tailored management [17]. Notably, ongoing prospective clinical trials are analyzing the clinical significance of the application of a dynamic frailty assessment to guide therapeutic decisions [76] (https://classic.clinicaltrials.gov/ct2/show/NCT06099912).
7. Conclusions
The analysis of published studies suggests that, at least in intermediately-fit, elderly, newly diagnosed MM patients, treatment intensity during continuous therapy can be deescalated without a negative impact on outcome. However, in subsequent phases, the choice of best therapeutic options, permitting to reduce treatment-related toxicities and preserve a good quality of life, is more difficult since treatment effectiveness may indeed be affected by the presence of co-morbidities, often related to advanced age, and by defective compliance [59]. As a result, few older and frail patients are currently enrolled in pivotal clinical trials and little data is presently available on appropriate management (Table 2).
Within this context it is remarkable that in a large majority of clinical studies analysis of potential patients frailty is limited to age report, without mentioning the use of available, though imperfect evaluation tools.
On the other hand, emerging targeted treatments, including CAR-T cells and BsAbs, are powerfully expanding the range of available MM therapeutic options, with increasing effectiveness. However, their application is also accompanied by the occurrence of specific adverse events [96], with potentially higher impact on frail and older patients. A safer use of these treatments urgently requires standardized frailty assessments based not only on clinical scoring, but, possibly, also on the characterization of innovative markers and laboratory tests[97]. In their absence, dynamic assessments and patient-tailored treatments should be recommended.
Author Contributions
All authors contributed to gathering of data, writing, editing, and revising of the manuscript
Funding
Not applicable
Acknowledgments
GS is supported by the Italian Association for Cancer Research (AIRC), Investigator Grant (IG) 2020-24440 and National Operational Program (PON), Ministry of the University and Research (MUR)-EU.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Kyle, R.A.; Greipp, P.R. Smoldering Multiple Myeloma. N. Engl. J. Med. 1980, 302, 1347–1349. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Kyle, R.A.; Pfeiffer, R.M.; Katzmann, J.A.; Caporaso, N.E.; Hayes, R.B.; Dispenzieri, A.; Kumar, S.; Clark, R.J.; Baris, D.; et al. Monoclonal gammopathy of undetermined significance (MGUS) consistently precedes multiple myeloma: a prospective study. Blood 2009, 113, 5412–5417. [Google Scholar] [CrossRef] [PubMed]
- Morgan, G.J.; Walker, B.A.; Davies, F.E. The genetic architecture of multiple myeloma. Nat. Rev. Cancer 2012 125 2012, 12, 335–348. [Google Scholar] [CrossRef]
- Tricot, G. New insights into role of microenvironment in multiple myeloma. Lancet 2000, 355, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Antoine-Pepeljugoski, C.; Braunstein, M.J. Management of Newly Diagnosed Elderly Multiple Myeloma Patients. Curr. Oncol. Rep. 2019, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bolli, N.; Martinelli, G.; Cerchione, C. The Molecular Pathogenesis of Multiple Myeloma. Hematol. Reports 2020, 12, 9054. [Google Scholar] [CrossRef]
- Kyle, R.A.; Therneau, T.M.; Rajkumar, S.V.; Offord, J.R.; Larson, D.R.; Plevak, M.F.; Melton, L.J. A Long-Term Study of Prognosis in Monoclonal Gammopathy of Undetermined Significance. N. Engl. J. Med. 2002, 346, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Kyle, R.A.; Buadi, F.; Vincent Rajkumar, S. Management of Monoclonal Gammopathy of Undetermined Significance (MGUS) and Smoldering Multiple Myeloma (SMM). Oncology (Williston Park). 2011, 25, 578. [Google Scholar] [PubMed]
- da Vià, M.C.; Ziccheddu, B.; Maeda, A.; Bagnoli, F.; Perrone, G.; Bolli, N. A Journey Through Myeloma Evolution: From the Normal Plasma Cell to Disease Complexity. HemaSphere 2020, 4, e502. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V.; Dimopoulos, M.A.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P.; et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014, 15, e538–e548. [Google Scholar] [CrossRef]
- Bolli, N.; Maura, F.; Minvielle, S.; Gloznik, D.; Szalat, R.; Fullam, A.; Martincorena, I.; Dawson, K.J.; Samur, M.K.; Zamora, J.; et al. Genomic patterns of progression in smoldering multiple myeloma. Nat. Commun. 2018 91 2018, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V.; Kumar, S. Multiple Myeloma: Diagnosis and Treatment. Mayo Clin. Proc. 2016, 91, 101–119. [Google Scholar] [CrossRef]
- Rajkumar, S.V. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am. J. Hematol. 2022, 97, 1086–1107. [Google Scholar] [CrossRef] [PubMed]
- Solly, S. Remarks on the pathology of mollities ossium; with cases. Med. Chir. Trans. 1844, 27, 435–461. [Google Scholar] [CrossRef]
- Riccomi, G.; Fornaciari, G.; Giuffra, V. Multiple myeloma in paleopathology: A critical review. Int. J. Paleopathol. 2019, 24, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Kaweme, N.M.; Changwe, G.J.; Zhou, F. Approaches and Challenges in the Management of Multiple Myeloma in the Very Old: Future Treatment Prospects. Front. Med. 2021, 8, 612696. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Moreau, P.; Terpos, E.; Mateos, M. V.; Zweegman, S.; Cook, G.; Delforge, M.; Hájek, R.; Schjesvold, F.; Cavo, M.; et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 309–322. [Google Scholar] [CrossRef]
- Mina, R.; Bringhen, S.; Wildes, T.M.; Zweegman, S.; Rosko, A.E. Approach to the Older Adult With Multiple Myeloma. Am. Soc. Clin. Oncol. Educ. B. 2019, 500–518. [Google Scholar] [CrossRef]
- Facon, T.; Leleu, X.; Manier, S. How I treat multiple myeloma in geriatric patients. Blood 2024, 143, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Bringhen, S.; Mateos, M.V.; Larocca, A.; Facon, T.; Kumar, S.K.; Offidani, M.; McCarthy, P.; Evangelista, A.; Lonial, S.; et al. Geriatric assessment predicts survival and toxicities in elderly myeloma patients: an International Myeloma Working Group report. Blood 2015, 125, 2068–2074. [Google Scholar] [CrossRef]
- Kleber, M.; Ihorst, G.; Terhorst, M.; Koch, B.; Deschler, B.; Wäsch, R.; Engelhardt, M. Comorbidity as a prognostic variable in multiple myeloma: comparative evaluation of common comorbidity scores and use of a novel MM–comorbidity score. Blood Cancer J. 2011 19 2011, 1, e35–e35. [Google Scholar] [CrossRef] [PubMed]
- Engelhardt, M.; Domm, A.S.; Dold, S.M.; Ihorst, G.; Reinhardt, H.; Zober, A.; Hieke, S.; Baayen, C.; Müller, S.J.; Einsele, H.; et al. A concise revised Myeloma Comorbidity Index as a valid prognostic instrument in a large cohort of 801 multiple myeloma patients. Haematologica 2017, 102, 910–921. [Google Scholar] [CrossRef]
- Engelhardt, M.; Dold, S.M.; Ihorst, G.; Zober, A.; Möller, M.; Reinhardt, H.; Hieke, S.; Schumacher, M.; Wäsch, R. Geriatric assessment in multiple myeloma patients: validation of the International Myeloma Working Group (IMWG) score and comparison with other common comorbidity scores. Haematologica 2016, 101, 1110–1119. [Google Scholar] [CrossRef]
- Bonanad, S.; De la Rubia, J.; Gironella, M.; Pérez Persona, E.; González, B.; Fernández Lago, C.; Arnan, M.; Zudaire, M.; Hernández Rivas, J.A.; Soler, A.; et al. Development and psychometric validation of a brief comprehensive health status assessment scale in older patients with hematological malignancies: The GAH Scale. J. Geriatr. Oncol. 2015, 6, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Mian, H.S.; Wildes, T.M.; Fiala, M.A. Development of a Medicare Health Outcomes Survey Deficit-Accumulation Frailty Index and Its Application to Older Patients With Newly Diagnosed Multiple Myeloma. JCO Clin. Cancer Informatics 2018, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wildes, T.M.; Tuchman, S.A.; Klepin, H.D.; Mikhael, J.; Trinkaus, K.; Stockerl-Goldstein, K.; Vij, R.; Colditz, G. Geriatric Assessment in Older Adults with Multiple Myeloma. J. Am. Geriatr. Soc. 2019, 67, 987–991. [Google Scholar] [CrossRef]
- Rosko, A.E.; Huang, Y.; Benson, D.M.; Efebera, Y.A.; Hofmeister, C.; Jaglowski, S.; Devine, S.; Bhatt, G.; Wildes, T.M.; Dyko, A.; et al. Use of a comprehensive frailty assessment to predict morbidity in patients with multiple myeloma undergoing transplant. J. Geriatr. Oncol. 2019, 10, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, H.; Delforge, M.; Facon, T.; Einsele, H.; Gay, F.; Moreau, P.; Avet-Loiseau, H.; Boccadoro, M.; Hajek, R.; Mohty, M.; et al. Prevention and management of adverse events of novel agents in multiple myeloma: a consensus of the European Myeloma Network. Leuk. 2018 327 2018, 32, 1542–1560. [Google Scholar] [CrossRef]
- Larocca, A.; Bonello, F.; Gaidano, G.; D’Agostino, M.; Offidani, M.; Cascavilla, N.; Capra, A.; Benevolo, G.; Tosi, P.; Galli, M.; et al. Dose/schedule-adjusted Rd-R vs continuous Rd for elderly, intermediate-fit patients with newly diagnosed multiple myeloma. Blood 2021, 137, 3027–3036. [Google Scholar] [CrossRef]
- Manier, S.; Corre, J.; Hulin, C.; Laribi, K.; Araujo, C.; Pica, G.-M.; Touzeau, C.; Godmer, P.; Slama, B.; Karlin, L.; et al. A Dexamethasone Sparing-Regimen with Daratumumab and Lenalidomide in Frail Patients with Newly-Diagnosed Multiple Myeloma: Efficacy and Safety Analysis of the Phase 3 IFM2017-03 Trial. Blood 2022, 140, 1369–1370. [Google Scholar] [CrossRef]
- Larocca, A.; Cani, L.; Bertuglia, G.; Bruno, B.; Bringhen, S. New Strategies for the Treatment of Older Myeloma Patients. Cancers 2023, 15, 2693. [Google Scholar] [CrossRef] [PubMed]
- Hulin, C.; Facon, T.; Rodon, P.; Pegourie, B.; Benboubker, L.; Doyen, C.; Dib, M.; Guillerm, G.; Salles, B.; Eschard, J.P.; et al. Efficacy of melphalan and prednisone plus thalidomide in patients older than 75 years with newly diagnosed multiple myeloma: IFM 01/01 trial. J. Clin. Oncol. 2009, 27, 3664–3670. [Google Scholar] [CrossRef] [PubMed]
- Durie, B.G.M.; Hoering, A.; Abidi, M.H.; Rajkumar, S.V.; Epstein, J.; Kahanic, S.P.; Thakuri, M.; Reu, F.; Reynolds, C.M.; Sexton, R.; et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. Lancet 2017, 389, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Durie, B.G.M.; Hoering, A.; Sexton, R.; Abidi, M.H.; Epstein, J.; Rajkumar, S.V.; Dispenzieri, A.; Kahanic, S.P.; Thakuri, M.C.; Reu, F.J.; et al. Longer term follow-up of the randomized phase III trial SWOG S0777: bortezomib, lenalidomide and dexamethasone vs. lenalidomide and dexamethasone in patients (Pts) with previously untreated multiple myeloma without an intent for immediate autologous stem cell transplant (ASCT). Blood Cancer J. 2020 105 2020, 10, 1–11. [Google Scholar] [CrossRef]
- O’Donnell, E.K.; Laubach, J.P.; Yee, A.J.; Chen, T.; Huff, C.A.; Basile, F.G.; Wade, P.M.; Paba-Prada, C.E.; Ghobrial, I.M.; Schlossman, R.L.; et al. A phase 2 study of modified lenalidomide, bortezomib and dexamethasone in transplant-ineligible multiple myeloma. Br. J. Haematol. 2018, 182, 222–230. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, E.K.; Laubach, J.P.; Yee, A.J.; Redd, R.; Huff, C.A.; Basile, F.; Wade, P.M.; Paba-Prada, C.E.; Ghobrial, I.M.; Schlossman, R.L.; et al. Updated Results of a Phase 2 Study of Modified Lenalidomide, Bortezomib, and Dexamethasone (RVd-lite) in Transplant-Ineligible Multiple Myeloma. Blood 2019, 134, 3178–3178. [Google Scholar] [CrossRef]
- Facon, T.; Dimopoulos, M.-A.; Leleu, X.P.; Beksac, M.; Pour, L.; Hájek, R.; Liu, Z.; Minarik, J.; Moreau, P.; Romejko-Jarosinska, J.; et al. Isatuximab, Bortezomib, Lenalidomide, and Dexamethasone for Multiple Myeloma. N. Engl. J. Med. 2024. [Google Scholar] [CrossRef]
- Facon, T.; Kumar, S.K.; Plesner, T.; Orlowski, R.Z.; Moreau, P.; Bahlis, N.; Basu, S.; Nahi, H.; Hulin, C.; Quach, H.; et al. Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 1582–1596. [Google Scholar] [CrossRef] [PubMed]
- Facon, T.; Cook, G.; Usmani, S.Z.; Hulin, C.; Kumar, S.; Plesner, T.; Touzeau, C.; Bahlis, N.J.; Basu, S.; Nahi, H.; et al. Daratumumab plus lenalidomide and dexamethasone in transplant-ineligible newly diagnosed multiple myeloma: frailty subgroup analysis of MAIA. Leuk. 2021 364 2022, 36, 1066–1077. [Google Scholar] [CrossRef] [PubMed]
- Durie, B.G.M.; Kumar, S.K.; Usmani, S.Z.; Nonyane, B.A.S.; Ammann, E.M.; Lam, A.; Kobos, R.; Maiese, E.M.; Facon, T. Daratumumab-lenalidomide-dexamethasone vs standard-of-care regimens: Efficacy in transplant-ineligible untreated myeloma. Am. J. Hematol. 2020, 95, 1486–1494. [Google Scholar] [CrossRef] [PubMed]
- Mateos, M.V.; Nahi, H.; Legiec, W.; Grosicki, S.; Vorobyev, V.; Spicka, I.; Hungria, V.; Korenkova, S.; Bahlis, N.; Flogegard, M.; et al. Subcutaneous versus intravenous daratumumab in patients with relapsed or refractory multiple myeloma (COLUMBA): a multicentre, open-label, non-inferiority, randomised, phase 3 trial. Lancet Haematol. 2020, 7, e370–e380. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.C.; Landgren, O.; Arend, R.C.; Chou, J.; Jacobs, I.A. Humanistic and economic impact of subcutaneous versus intravenous administration of oncology biologics. Futur. Oncol. 2019, 15, 3267–3281. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, R.; Facon, T.; Hashim, M.; Nair, S.; He, J.; Ammann, E.; Lam, A.; Wildgust, M.; Kumar, S. Impact of Treatment Sequencing on Overall Survival in Patients with Transplant-Ineligible Newly Diagnosed Myeloma. Oncologist 2023, 28, e263–e269. [Google Scholar] [CrossRef] [PubMed]
- Mateos, M.-V.; Dimopoulos, M.A.; Cavo, M.; Suzuki, K.; Jakubowiak, A.; Knop, S.; Doyen, C.; Lucio, P.; Nagy, Z.; Kaplan, P.; et al. Daratumumab plus Bortezomib, Melphalan, and Prednisone for Untreated Myeloma. N. Engl. J. Med. 2018, 378, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Mateos, M.V.; Dimopoulos, M.A.; Cavo, M.; Suzuki, K.; Knop, S.; Doyen, C.; Lucio, P.; Nagy, Z.; Pour, L.; Grosicki, S.; et al. Daratumumab Plus Bortezomib, Melphalan, and Prednisone Versus Bortezomib, Melphalan, and Prednisone in Transplant-Ineligible Newly Diagnosed Multiple Myeloma: Frailty Subgroup Analysis of ALCYONE. Clin. Lymphoma Myeloma Leuk. 2021, 21, 785–798. [Google Scholar] [CrossRef] [PubMed]
- San-Miguel, J.; Avet-Loiseau, H.; Paiva, B.; Kumar, S.; Dimopoulos, M.A.; Facon, T.; Mateos, M.V.; Touzeau, C.; Jakubowiak, A.; Usmani, S.Z.; et al. Sustained minimal residual disease negativity in newly diagnosed multiple myeloma and the impact of daratumumab in MAIA and ALCYONE. Blood 2022, 139, 492–501. [Google Scholar] [CrossRef]
- Mateos, M.V.; Cavo, M.; Blade, J.; Dimopoulos, M.A.; Suzuki, K.; Jakubowiak, A.; Knop, S.; Doyen, C.; Lucio, P.; Nagy, Z.; et al. Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): a randomised, open-label, phase 3 trial. Lancet 2020, 395, 132–141. [Google Scholar] [CrossRef]
- Barlogie, B.; Smith, L.; Alexanian, R. Effective Treatment of Advanced Multiple Myeloma Refractory to Alkylating Agents. N. Engl. J. Med. 1984, 310, 1353–1356. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V.; Blood, E.; Vesole, D.; Fonseca, R.; Greipp, P.R. Phase III Clinical Trial of Thalidomide Plus Dexamethasone Compared With Dexamethasone Alone in Newly Diagnosed Multiple Myeloma: A Clinical Trial Coordinated by the Eastern Cooperative Oncology Group. J. Clin. Oncol. 2006, 24, 431–436. [Google Scholar] [CrossRef]
- Facon, T.; Mary, J.Y.; Pégourie, B.; Attal, M.; Renaud, M.; Sadoun, A.; Voillat, L.; Dorvaux, V.; Hulin, C.; Lepeu, G.; et al. Dexamethasone-based regimens versus melphalan-prednisone for elderly multiple myeloma patients ineligible for high-dose therapy. Blood 2006, 107, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Stege, C.A.M.; Nasserinejad, K.; van der Spek, E.; Bilgin, Y.M.; Kentos, A.; Sohne, M.; van Kampen, R.J.W.; Ludwig, I.; Thielen, N.; Durdu-Rayman, N.; et al. Ixazomib, Daratumumab, and Low-Dose Dexamethasone in Frail Patients With Newly Diagnosed Multiple Myeloma: The Hovon 143 Study. J. Clin. Oncol. 2021, 39, 2758–2767. [Google Scholar] [CrossRef] [PubMed]
- Chim, C.S.; Kumar, S.K.; Orlowski, R.Z.; Cook, G.; Richardson, P.G.; Gertz, M.A.; Giralt, S.; Mateos, M. V.; Leleu, X.; Anderson, K.C. Management of relapsed and refractory multiple myeloma: novel agents, antibodies, immunotherapies and beyond. Leuk. 2018 322 2017, 32, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, P. Management of multiple myeloma in the relapsed/refractory patient. Hematology 2017, 2017, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Quach, H.; Nooka, A.; Samoylova, O.; Venner, C.P.; Kim, K.; Facon, T.; Spencer, A.; Usmani, S.Z.; Grosicki, S.; Suzuki, K.; et al. Carfilzomib, dexamethasone and daratumumab in relapsed or refractory multiple myeloma: results of the phase III study CANDOR by prior lines of therapy. Br. J. Haematol. 2021, 194, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Yong, K.; Delforge, M.; Driessen, C.; Fink, L.; Flinois, A.; Gonzalez-McQuire, S.; Safaei, R.; Karlin, L.; Mateos, M.V.; Raab, M.S.; et al. Multiple myeloma: patient outcomes in real-world practice. Br. J. Haematol. 2016, 175, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Qiu, L.; Usmani, S.; et al. Consensus guidelines and recommendations for the management and response assessment of chimeric antigen receptor T-cell therapy in clinical practice for relapsed and refractory multiple myeloma: a report from the International Myeloma Working Group Immunotherapy Committee. Lancet Oncol. Erratum in: Lancet Oncol. 2024, 25, e336. 10.1016/S1470-2045(24)00337-1. 2024, 25, e374–e387. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Otero, P.; San Miguel, J.F. Post-CAR-T Cell Therapy (Consolidation and Relapse): Multiple Myeloma. EBMT/EHA CAR-T Cell Handb. 2022, 173–176. [Google Scholar] [CrossRef]
- Davis, J.A.; Dima, D.; Ahmed, N.; DeJarnette, S.; McGuirk, J.; Jia, X.; Raza, S.; Khouri, J.; Valent, J.; Anwer, F.; et al. Impact of Frailty on Outcomes after Chimeric Antigen Receptor T Cell Therapy for Patients with Relapsed/Refractory Multiple Myeloma. Transplant. Cell. Ther. 2024, 30, 298–305. [Google Scholar] [CrossRef]
- Rajeeve, S.; Usmani, S.Z. How Old is Too Old for CAR-T Cell Therapies in Multiple Myeloma? Transplant. Cell. Ther. 2023, 29, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Munshi, N.C.; Anderson, L.D.; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef]
- Berdeja, J.G.; Madduri, D.; Usmani, S.Z.; Jakubowiak, A.; Agha, M.; Cohen, A.D.; Stewart, A.K.; Hari, P.; Htut, M.; Lesokhin, A.; et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b/2 open-label study. Lancet 2021, 398, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, O.S.; Sheeba, B.A.; Azad, F.; Alessi, L.; Hansen, D.; Alsina, M.; Baz, R.; Shain, K.; Grajales Cruz, A.; Castaneda Puglianini, O.; et al. Safety and efficacy of anti-BCMA CAR-T cell therapy in older adults with multiple myeloma: A systematic review and meta-analysis. J. Geriatr. Oncol. 2024, 15. [Google Scholar] [CrossRef] [PubMed]
- Reyes, K.R.; Huang, C.Y.; Lo, M.; Arora, S.; Chung, A.; Wong, S.W.; Wolf, J.; Olin, R.L.; Martin, T.; Shah, N.; et al. Safety and Efficacy of BCMA CAR-T Cell Therapy in Older Patients With Multiple Myeloma. Transplant. Cell. Ther. 2023, 29, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Jacobson, C.A.; Oluwole, O.O.; Munoz, J.; Deol, A.; Miklos, D.B.; Bartlett, N.L.; Braunschweig, I.; Jiang, Y.; Kim, J.J.; et al. Outcomes of older patients in ZUMA-1, a pivotal study of axicabtagene ciloleucel in refractory large B-cell lymphoma. Blood 2020, 135, 2106–2109. [Google Scholar] [CrossRef] [PubMed]
- Yates, S.J.; Cursio, J.F.; Artz, A.; Kordas, K.; Bishop, M.R.; Derman, B.A.; Kosuri, S.; Riedell, P.A.; Kline, J.; Jakubowiak, A.; et al. Optimization of older adults by a geriatric assessment–guided multidisciplinary clinic before CAR T-cell therapy. Blood Adv. 2024, 8, 3785–3797. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Otero P, Usmani S, Cohen AD, International Myeloma Working Group immunotherapy committee consensus guidelines and recommendations for optimal use of T-cell-engaging bispecific antibodies in multiple myeloma. Lancet Oncol. Erratum in Lancet Oncol. 2024, 25, e284. 10.1016/S1470-2045(24)00288-2. 2024, 25, e205–e216. [CrossRef] [PubMed]
- Ellerman, D. Bispecific T-cell engagers: Towards understanding variables influencing the in vitro potency and tumor selectivity and their modulation to enhance their efficacy and safety. Methods 2019, 154, 102–117. [Google Scholar] [CrossRef]
- Tacchetti, P.; Barbato, S.; Mancuso, K.; Zamagni, E.; Cavo, M. Bispecific Antibodies for the Management of Relapsed/Refractory Multiple Myeloma. Cancers 2024, 16, 2337. [Google Scholar] [CrossRef]
- Dieterle, M.P.; Mostufi-Zadeh-Haghighi, G.; Kus, J.W.; Wippel, C.; Brugger, Z.; Miething, C.; Wäsch, R.; Engelhardt, M. Safe and successful teclistamab treatment in very elderly multiple myeloma (MM) patients: a case report and experience from a total of three octogenarians. Ann Hematol 2023, 102, 3639–3641. [Google Scholar] [CrossRef] [PubMed]
- Jourdes, A.; Cellerin, E.; Touzeau, C.; et al. Characteristics and incidence of infections in patients with multiple myeloma treated by bispecific antibodies: a national retrospective study. Clin Microbiol Infect 2024, 30, 764–771. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Mikhael, J.; Hajek, R.; et al. (2021) Management of patients with multiple myeloma beyond the clinical-trial setting: understanding the balance between efficacy, safety and tolerability, and quality of life. Blood Cancer J 2021, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mohty, B.; El-Cheikh, J.; Yakoub-Agha, I.; Moreau, P.; Harousseau, J.L.; Mohty, M. Peripheral neuropathy and new treatments for multiple myeloma: background and practical recommendations. Haematologica 2010, 95, 311–319. [Google Scholar] [CrossRef]
- Du, J.S.; Yen, C.H.; Hsu, C.M.; Hsiao, H.H. (2021) Management of Myeloma Bone Lesions. Int J Mol Sci 2021, 22, 3389. [Google Scholar] [CrossRef] [PubMed]
- Mach, S.; Javed, S.; Chen, G.H.; Huh, B.K. Peripheral Nerve Stimulation for Back Pain in Patients With Multiple Myeloma as Bridge Therapy to Radiation Treatment: A Case Series. Neuromodulation 2023, 26, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Mian, H.S.; Wildes, T.; Vij, R.; Major, A.; Fiala, M.A. Need for Dynamic Frailty Risk Assessment Among Older Adults with Multiple Myeloma: A Population-Based Cohort Study. Blood 2022, 140, 423–424. [Google Scholar] [CrossRef]
- Cook, G.; Pawlyn, C.; Royle, K.-L.; et al. Dynamic Frailty Assessment in Transplant Non-Eligible Newly Diagnosed Myeloma Patients: Initial Data from UK Myeloma Research Alliance (UK-MRA) Myeloma XIV (FiTNEss): A Frailty-Adjusted Therapy Study. Blood 2023, 142, 4748–4748. [Google Scholar] [CrossRef]
- Moreau, P.; Garfall, A.L.; van de Donk, N.W.C.J.; et al. Teclistamab in Relapsed or Refractory Multiple Myeloma. N Engl J Med 2022, 387, 495–505. [Google Scholar] [CrossRef]
- Usmani, S.Z.; Garfall, A.L.; van de Donk, N.W.C.J.; et al. Teclistamab, a B-cell maturation antigen × CD3 bispecific antibody, in patients with relapsed or refractory multiple myeloma (MajesTEC-1): a multicentre, open-label, single-arm, phase 1 study. Lancet 2021, 398, 665–674. [Google Scholar] [CrossRef]
- Raje, N.S.; Leleu, X.P.; Lesokhin, A.M.; Mohty, M.; Nooka, A.K.; Leip, E.; Conte, U.; Viqueira, A.; Manier, S. Efficacy and safety of elranatamab by age and frailty in patients (pts) with relapsed/refractory multiple (RRMM): A subgroup analysis from MagnetisMM-3. J Clin Oncol 2023, 41, 8040–8040. [Google Scholar] [CrossRef]
- Lesokhin, A.M.; Tomasson, M.H.; Arnulf, B.; et al. Elranatamab in relapsed or refractory multiple myeloma: phase 2 MagnetisMM-3 trial results. Nat Med 2023 299 2023, 29, 2259–2267. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Bumma, N.; Richter, J.R.; et al. LINKER-MM1 study: Linvoseltamab (REGN5458) in patients with relapsed/refractory multiple myeloma. J Clin Oncol 2023, 41, 8006–8006. [Google Scholar] [CrossRef]
- Jagannath, S.; Richter, J.; Dhodapkar, M.V.; et al. Patterns of Response to 200 Mg Linvoseltamab in Patients with Relapsed/Refractory Multiple Myeloma: Longer Follow-Up of the Linker-MM1 Study. Blood 2023, 142, 4746–4746. [Google Scholar] [CrossRef]
- Bar, N.; Mateos, M.V.; Ribas, P.; et al. Alnuctamab (ALNUC; BMS-986349; CC-93269), a 2+1 B-Cell Maturation Antigen (BCMA) × CD3 T-Cell Engager (TCE), Administered Subcutaneously (SC) in Patients (Pts) with Relapsed/Refractory Multiple Myeloma (RRMM): Updated Results from a Phase 1 First-in-Human Clinical Study. Blood 2023, 142, 2011–2011. [Google Scholar]
- D’souza, A.; Shah, N.; Rodriguez, C.; et al. A Phase I First-in-Human Study of ABBV-383, a B-Cell Maturation Antigen × CD3 Bispecific T-Cell Redirecting Antibody, in Patients With Relapsed/Refractory Multiple Myeloma. J Clin Oncol 2022, 40, 3576–3586. [Google Scholar] [CrossRef]
- Voorhees, P.M.; D’Souza, A.; Weisel, K.; et al. A Phase 1 First-in-Human Study of Abbv-383, a BCMA × CD3 Bispecific T-Cell-Redirecting Antibody, As Monotherapy in Patients with Relapsed/Refractory Multiple Myeloma. Blood 2022, 140, 4401–4404. [Google Scholar] [CrossRef]
- Suvannasankha, A.; Kapoor, P.; Pianko, M.J.; et al. Abstract CT013: Safety and efficacy from the phase 1/2 first-in-human study of REGN5459, a BCMA×CD3 bispecific antibody with low CD3 affinity, in patients with relapsed/refractory multiple myeloma. Cancer Res 2023, 83, CT013–CT013. [Google Scholar] [CrossRef]
- Rasche, L.; Schinke, C.; Touzeau, C.; et al. Long-Term Efficacy and Safety Results From the Phase 1/2 MonumenTAL-1 Study of Talquetamab, a GPRC5D×CD3 Bispecific Antibody, in Patients With Relapsed/Refractory Multiple Myeloma (RRMM). Clin Lymphoma Myeloma Leuk 2024, 24, S240. [Google Scholar] [CrossRef]
- Carlo-Stella, C.; Mazza, R.; Manier, S.; et al. RG6234, a GPRC5DxCD3 T-Cell Engaging Bispecific Antibody, Is Highly Active in Patients (pts) with Relapsed/Refractory Multiple Myeloma (RRMM): Updated Intravenous (IV) and First Subcutaneous (SC) Results from a Phase I Dose-Escalation Study. Blood 2022, 140, 397–399. [Google Scholar] [CrossRef]
- Trudel, S.; Cohen, A.D.; Krishnan, A.Y.; et al. Cevostamab Monotherapy Continues to Show Clinically Meaningful Activity and Manageable Safety in Patients with Heavily Pre-Treated Relapsed/Refractory Multiple Myeloma (RRMM): Updated Results from an Ongoing Phase I Study. Blood 2021, 138, 157–157. [Google Scholar] [CrossRef]
- Kumar, S.K.; Jacobus, S.J.; Cohen, A.D.; et al. Carfilzomib or bortezomib in combination with lenalidomide and dexamethasone for patients with newly diagnosed multiple myeloma without intention for immediate autologous stem-cell transplantation (ENDURANCE): a multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol 2020, 21, 1317–1330. [Google Scholar]
- Facon, T.; Lee, J.H.; Moreau, P.; et al. Carfilzomib or bortezomib with melphalan-prednisone for transplant-ineligible patients with newly diagnosed multiple myeloma. Blood 2019, 133, 1953–1963. [Google Scholar] [CrossRef] [PubMed]
- Usmani, S.Z.; Nahi, H.; Legiec, W.; et al. Final analysis of the phase III non-inferiority COLUMBA study of subcutaneous versus intravenous daratumumab in patients with relapsed or refractory multiple myeloma. Haematologica 2022, 107, 2408–2417. [Google Scholar] [CrossRef]
- Richardson, P.G.; Kumar, S.K.; Masszi, T.; et al. Final Overall Survival Analysis of the TOURMALINE-MM1 Phase III Trial of Ixazomib, Lenalidomide, and Dexamethasone in Patients With Relapsed or Refractory Multiple Myeloma. J Clin Oncol 2021, 39, 2430–2442. [Google Scholar] [CrossRef]
- Facon, T.; Niesvizky, R.; Mateos, M.V.; et al. Efficacy and safety of carfilzomib-based regimens in frail patients with relapsed and/or refractory multiple myeloma. Blood Adv 2020, 4, 5449–5459. [Google Scholar] [CrossRef] [PubMed]
- Berdeja, J.G.; Raje, N.S.; Siegel, D.S.; et al. Efficacy and Safety of Idecabtagene Vicleucel (ide-cel, bb2121) in Elderly Patients with Relapsed and Refractory Multiple Myeloma: KarMMa Subgroup Analysis. Blood 2020, 136, 16–17. [Google Scholar] [CrossRef]
- Ludwig, H.; Terpos, E.; van de Donk, N.; et al. Prevention and management of adverse events during treatment with bispecific antibodies and CAR T cells in multiple myeloma: a consensus report of the European Myeloma Network. Lancet Oncol. 2023, 24, e255–e269. [Google Scholar] [CrossRef] [PubMed]
- Cook, G.; Pawlyn, C.; Cairns, D.A.; Jackson, G.H. Defining FiTNEss for treatment for multiple myeloma. Lancet Healthy Longev. 2022, 3, e729–e730. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Multiple myeloma pathogenesis:from healthy status to disease. (A) In normal conditions, plasma cells are able to generate and secrete antibodies and are key contributors to humoral immunity. (B) In MM, uncontrolled multiplication of abnormal plasma cells in the BM inhibits the production of protective antibodies. Malignant plasma cells produce an abnormal M protein antibody, considered as a most characteristic feature of MM. [Created in BioRender. Aureli, A. (2024) https://BioRender.com/n09o389].
Figure 1.
Multiple myeloma pathogenesis:from healthy status to disease. (A) In normal conditions, plasma cells are able to generate and secrete antibodies and are key contributors to humoral immunity. (B) In MM, uncontrolled multiplication of abnormal plasma cells in the BM inhibits the production of protective antibodies. Malignant plasma cells produce an abnormal M protein antibody, considered as a most characteristic feature of MM. [Created in BioRender. Aureli, A. (2024) https://BioRender.com/n09o389].
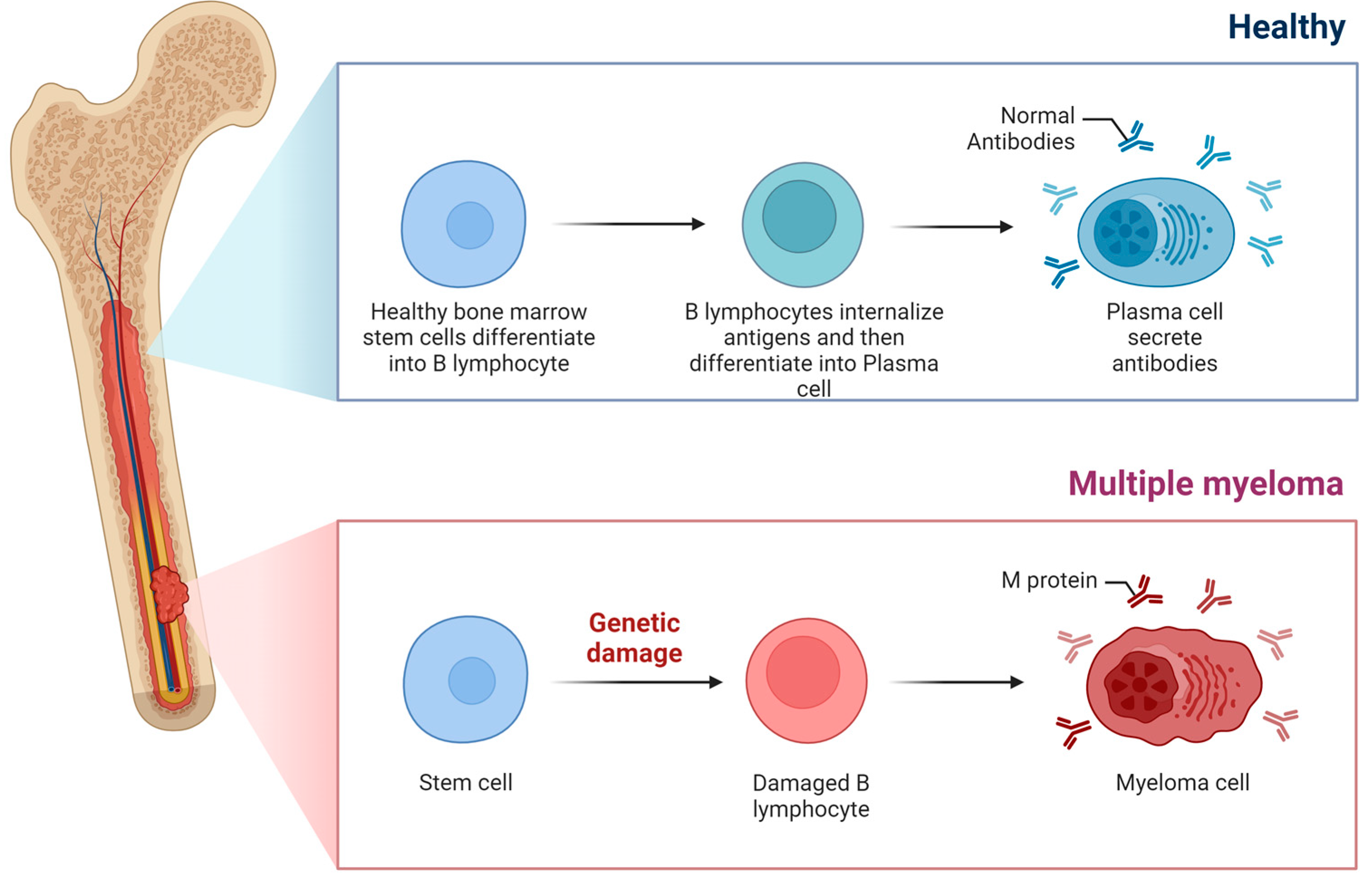
Figure 2.
Mechanism of action of BsAbs. Schematic representation of the mechanisms of action of BsAbs. (1) BsAb simultaneously bind CD3 on T cell surfaces and atumor antigen expressed on MM cell surfaces. The simultaneous interaction of the BsAb on the surface of the T cell and MM cell leads to (2) expansion of activated T cell and (3) secretion of granzymes and perforins (4) promoting MM cell death.[Created in BioRender. Aureli, A. (2024) https://BioRender.com/n08g496].
Figure 2.
Mechanism of action of BsAbs. Schematic representation of the mechanisms of action of BsAbs. (1) BsAb simultaneously bind CD3 on T cell surfaces and atumor antigen expressed on MM cell surfaces. The simultaneous interaction of the BsAb on the surface of the T cell and MM cell leads to (2) expansion of activated T cell and (3) secretion of granzymes and perforins (4) promoting MM cell death.[Created in BioRender. Aureli, A. (2024) https://BioRender.com/n08g496].
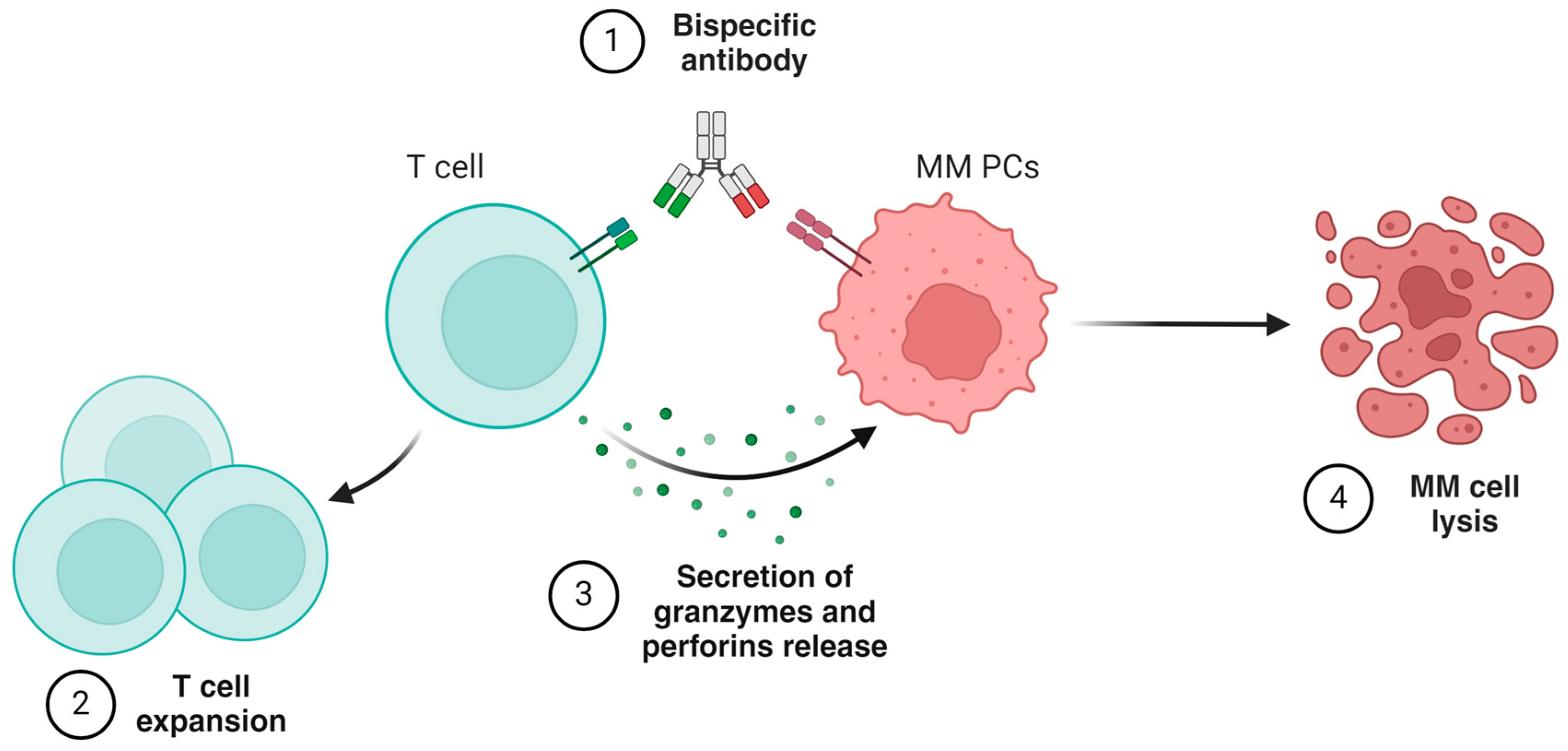

Table 1.
Emerging BsAbs for the management of patients (including older one) with R/R MM.
| Targets | BsAbs | Study | Patients number | Dosing schedule/efficacy (ref.) |
|---|---|---|---|---|
| BCMA | Teclistamab (JNJ-64007957) | Phase 1/2 MajesTEC-1 trial (NCT04557098); (NCT03145181) | 165 Patients≥75 yr: 24 (14.5%). |
subcutaneous injection0.06mg-0.3mg-1.5mg/Kg once weekly.Deep and durable response [77,78]. |
| Elranatab (PF-06863135) | Phase 2 MagnetisMM-3 trial (NCT04649359cohort A) | 123 Patients≥75 yr: 24 (19.5%). |
subcutaneous injection12-32-76 mg once weekly.Good efficacy and safety [79,80] | |
| Linvoseltamab (REGN5458) | Phase 1/2 LINKER-MM1 trial (NCT03761108) | 200 mg.: 117 Patients≥75 yr: 31 (26.4%). |
intravenous injection 5-25-200 mg once weekly.Consistent efficacy across high-risk subgroups and induced responses in pts who progressed on 50 ng[81,82]. | |
| Alnuctamab (CC-93269) | Phase 1 trial (NCT03486067) | 73 Patients≥75 yr: n.a. |
target dose:subcutaneous injection 30 mg one weekly (cycle 1 to 3); every other week (cycle 4 to 6); every 4 weeks from cycle 7. Favorable safety profile[83]. | |
| ABBV-383 (TNB-383B) | Phase 1 trial (NCT03933735) | 124 Patients≥75 yr: n.a. |
intravenous injection 60 mg every three weeks. Good tolerance and durable response [84,85]. | |
| REGN-5459 | Phase 1/2 trial (NCT04083534) | 43 Patients≥75 yr: n.a. |
target dose: intravenous injection 480 mg once weekly. Acceptable safety/tolerability[86]. | |
| GPRC5D | Talquetamab | Phase 1/2 MonumenTAL-1 trial. (NCT03399799); (NCT04634552) | 375 Patients≥75 yr: n.a. |
subcutaneous injection 0.4 mg/kg once weekly or 0.8 mg/kg every other week, with step-up doses. The safety profile was consistent with previous results[87]. |
| Forimtamig (RG6234) | Phase 1 trial (NCT04557150) | 108 Patients≥75 yr: n.a. |
intravenous injection dose range: 6-10000µg (51 pts) subcutaneous injection dose range: 30-7200µg (57 pts).high response rate across all tested doses for both IV and SC dosing[88]. | |
| FcRH5 | Cevostamab | Phase 1 trial (NCT03275103) | 160 Patients≥75 yr: n.a. |
intravenous infusion in 21-day cycles. In the single step-up cohorts, the step dose (0.05-3.6mg) is given on C1 Day (D) 1 and the target dose (0.15-198mg) on C1D8. In the double step-up cohorts, the step doses are given on C1D1 (0.3-1.2mg) and C1D8 (3.6mg), and the target dose (60-160mg) on C1D15. In both regimens, the target dose is given on D1 of subsequent cycles. Cevostamab is continued for a total of 17 cycles, unless progressive disease or unacceptable toxicity occurs. Clinically meaningful activity and no increase in CRS rate[89]. |
Abbreviations: n.a.: not available.
Table 2.
Approved immunotherapy options for older, frail patients ineligible for transplantation, at initial diagnosis and at relapse.
Table 2.
Approved immunotherapy options for older, frail patients ineligible for transplantation, at initial diagnosis and at relapse.
| Newly diagnosed patients | |
|---|---|
| MAIA study [38]. | n= 737 pts (D-Rd, n = 368; Rd, n = 369) 396 non-frail pts (D-Rd, 196 ; Rd, 200 ) 341 frail pts(D-Rd, 172 ; Rd, 169 ) Clinical benefit irrespective of frailty in newly diagnosed, transplant-ineligible patients |
| ALCYONE[47]. | n=706 pts (D-VMP, n = 350; VMP, n = 356) 391 non frail pts (D-VMP, 187; VMP, 204) 315 frail pts (D-VMP, 163; VMP,152) Clinical benefit of D-VMP irrespective of frailty in newly diagnosed transplant-ineligible patients enrolled in ALCYONE, regardless of frailty status. |
| SWOG S0777[33,34] | n=460 pts (VRd, n = 235; Rd, n = 225) 91/235 pts in the VRd arm were aged >65 years Addition of bortezomib to standard lenalidomide/dexamethasone clinically advantageous irrespective of age in previously untreated patients. |
| ENDURANCE[90] | n= 1087 pts (VRd, n = 542; KRd, n = 545) VRd lite in older pts [35,36] Addition of Carfilzomib to VRd in newly diagnosed multiple myeloma patients not more effective and characterized by higher toxicity. A modified VRd treatment effective in >65 years old, newly diagnosed, transplant-ineligible patients |
| CLARION [91] | n=955 pts (KMP, n = 478; VMP, n = 477). KMP not more effective than VMP in newly diagnosed multiple myeloma patients ineligible for transplant, irrespective of age. |
| HOVON 143 [51] | n= 65 frail newly diagnosed multiple myeloma pts, treated with Ixa-Dara-Dex. High response rate but toxicity and early mortality. |
| Treatment options at relapse | |
| COLUMBA [92] | n=522 pts (DARA SC, n=263; DARA IV, n=259) Similar effectiveness of daratumumab upon subcutaneous or intravenous administration in relapsed or refractory multiple myeloma. |
| TOURMALINE[93] | n= 722 (IRd, n = 360; Rd, n = 362) Improved PFS upon treatment with IRd than with Rd in patients with relapsed or refractory multiple myeloma. |
| ASPIRE-ENDEAVOR-ARROW [94] | ASPIRE n=792 pts (KRd27, n= 396 vs Rd n= 396) ENDEAVOR n=929 pts (Kd56, n= 464vs Vd, n= 465) ARROW (once-weekly) n=478 pts (Kd70, n=240 vs Kd27, n=238) Efficacy and safety were consistent across frailty subgroups with KRd27, Kd56, and weekly Kd70 in relapsed and/or refractory MM. |
| KarMMa study[95] | CAR T-Therapy (n=128; n=45 ≥65 years; n=20 ≥70 years) Durable responses and manageable safety profile in patients with relapsed/recurrent multiple myeloma aged ≥65 years and ≥70 years. |
Abbreviations: pts=patients; D-Rd = daratumumab plus lenalidomide and dexamethasone; Rd = lenalidomide and dexamethasone; D-VMP = daratumumab, plus bortezomib, melphalan, and prednisone; VMP=bortezomib, melphalan, and prednisone; VRd= bortezomib + lenalidomide + dexamethasone; Rd=Lenalidomide-dexamethasone; KRd=carfilzomib, lenalidomide and dexamethasone; KMP = carfilzomib-melphalan-prednisone; Ixa-Dara-Dex= ixazomib-daratumumab-low-dose-dexamethasone; DARA=daratumumab; SC=subcutaneous; IV=intravenous; IRd=ixazomib-lenalidomide-dexamethasone; KRd27=(carfilzomib [27 mg/m2]-lenalidomide-dexamethasone; Kd56=carfilzomib [56 mg/m2]-dexamethasone; Vd=bortezomib-dexamethasone; Kd70=carfilzomib [70 mg/m2]-dexamethasone.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



