Submitted:
10 January 2025
Posted:
13 January 2025
You are already at the latest version
Abstract
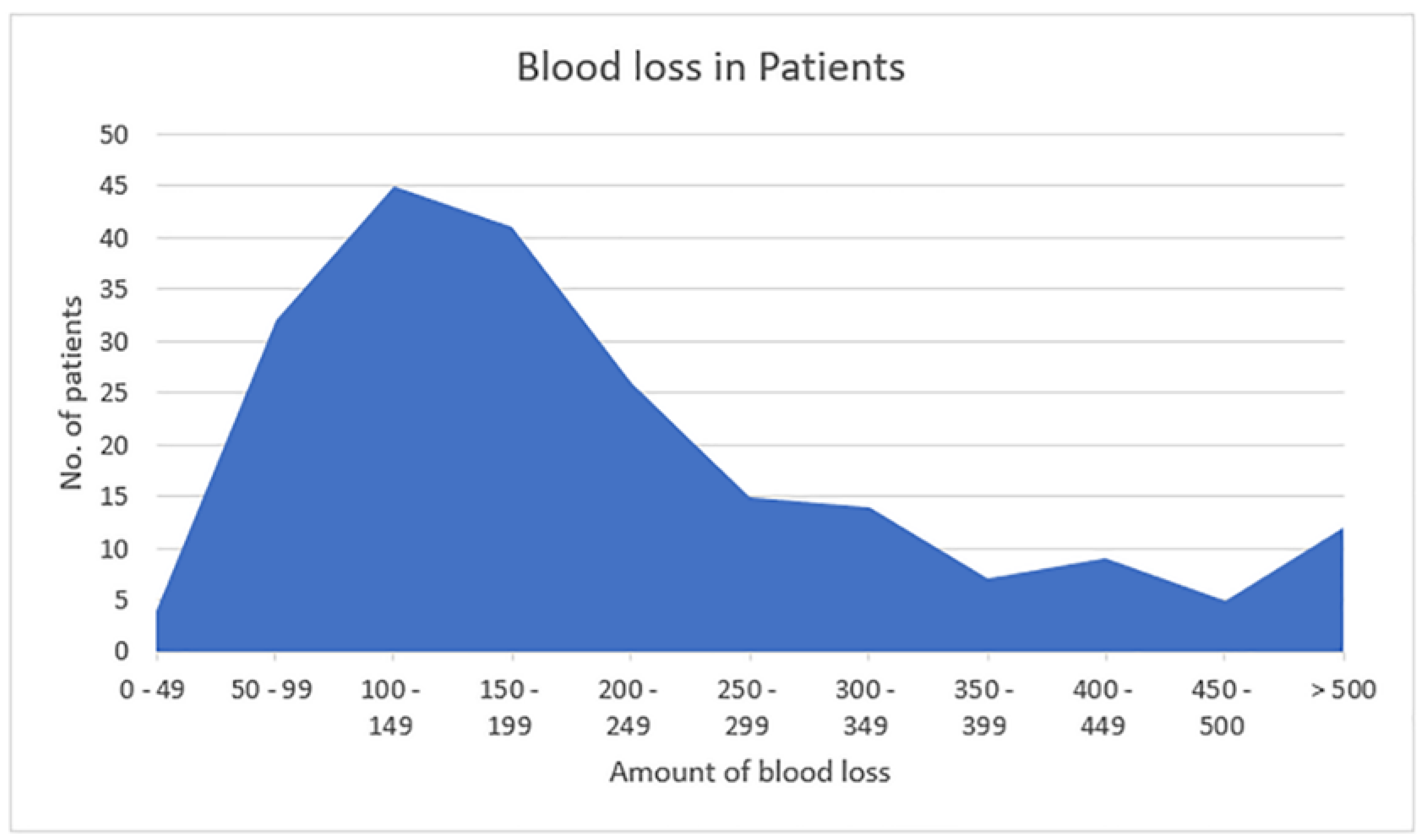
Background: This study aims to find the correlation between risk factors and the incidence of post-partum hemorrhage (PPH) in normal vaginal deliveries. Methods: The present research is an observational cohort study. 239 women undergoing normal labor who delivered vaginally were given 0.2mg of Ergometrine or 600 μg of Misoprostol as a prophylaxis to prevent PPH. The blood loss was estimated by the use of blood collection drapes during delivery. All statistical analysis was conducted via SPSS version 27. The risk factors were compared between the groups with or without PPH.Results: The majority 87 (36.4%) of the participants were in the 25-29 years age group, had zero parity status 113 (47.3%), and 93 (38.9%) were primigravida. The prevalence of PPH was 4.6% (11/239). Almost half of the cases of PPH (5/11, 45.5%) had no risk factors, whereas those with risk factors had twin pregnancy (25%), low-lying placenta (50%), grand multipara (33.3%) and previous history of PPH (33.3%). Furthermore, a moderate positive correlation be-tween the risk factors and the incidence of PPH was observed (R= 0.512). Conclusion: In this study, women with risk factors like twin pregnancy, low-lying placenta, grand multipara, and previous history of PPH developed PPH despite giving prophylaxis and close monitoring. However, almost half of the cases of PPH occurred in people where there was no risk factor.
Keywords:
1. Introduction
2. Materials and Methods
- Obstetrics (Gestational age < 32 wk, Prolonged labor, Preeclampsia, Eclampsia, Vaginal instrumental deliveries)
- Non-obstetrics (H/o Asthma, H/o Epilepsy, H/o Heart disease, H/o Kidney disease, H/o Jaundice, Coagulation disorder)
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.B.; Daniels, J.; et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health 2014, 2, e323–e333. [Google Scholar] [CrossRef]
- Fatima, N. Postpartum Hemorrhage: Causes and Outcome. J Neonatal Surg 2019, 24, 28–33. [Google Scholar]
- Khan, K.S.; Wojdyla, D.; Say, L.; Gülmezoglu, A.M.; Van Look, P.F. WHO analysis of causes of maternal death: a systematic review. Lancet 2006, 367, 1066–1074. [Google Scholar] [CrossRef] [PubMed]
- Khorrami, N.; Stone, J.; Small, M.J.; Stringer, E.M.; Ahmadzia, H.K. An overview of advances in global maternal health: From broad to specific improvements. Int J Gynaecol Obstet 2019, 146, 126–131. [Google Scholar] [CrossRef]
- Lutomski, J.E.; Byrne, B.M.; Devane, D.; Greene, R.A. Increasing trends in atonic postpartum hemorrhage in Ireland: an 11-year population-based cohort study. BJOG: An Int J Gynaecol Obstet 2011, 119, 306–314. [Google Scholar] [CrossRef]
- Ononge, S.; Mirembe, F.; Wandabwa, J.; Campbell, O.M. Incidence and risk factors for postpartum hemorrhage in Uganda. Reprod Health 2016, 13, 1–7. [Google Scholar] [CrossRef]
- Oberg, A.S.; Hernandez-Diaz, S.; Palmsten, K.; Almqvist, C.; Bateman, B.T. Patterns of recurrence of postpartum hemorrhage in a large population-based cohort. Am J Obstet Gynecol 2014, 210, 229–e1. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG practice bulletin: clinical management guidelines for obstetrician-gynecologists number 76, October 2006, postpartum hemorrhage. Obstet Gynecol 2006, 108, 1039–1047. [Google Scholar]
- Gill, P.; Patel, A.; Van Hook, J.W. Uterine Atony. In: StatPearls [Internet]. StatPearls Publishing; 2024. [Google Scholar]
- Sosa, C.G.; Althabe, F.; Belizán, J.M.; Buekens, P. Risk factors for postpartum hemorrhage in vaginal deliveries in a Latin-American population. Obstet Gynaecol 2009, 113, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Newsome, J.; Martin, J.G.; Bercu, Z.; Shah, J.; Shekhani, H.; Peters, G. Postpartum hemorrhage. Tech Vasc Interv Radiol 2017, 20, 266–273. [Google Scholar] [CrossRef]
- Lertbunnaphong, T.; Lapthanapat, N.; Leetheeragul, J.; Hakularb, P.; Ownon, A. Postpartum blood loss: visual estimation versus objective quantification with a novel birthing drape. Singapore Med J 2016, 57, 325. [Google Scholar] [CrossRef]
- Natrella M, Di Naro E, Loverro M, Benshalom-Tirosh N, Trojano G, Tirosh D, et al. The more you lose the more you miss: accuracy of postpartum blood loss visual estimation. A systematic review of the literature. Matern Fetal Neonatal Med 2018, 31, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Borovac-Pinheiro A, Pacagnella RC, Cecatti JG, Miller S, El Ayadi AM, Souza JP, et al. Postpartum hemorrhage: new insights for definition and diagnosis. Am J Obstet Gynecol 2018, 219, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Kramer MS, Berg C, Abenhaim H, Dahhou M, Rouleau J, Mehrabadi A, et al. Incidence, risk factors, and temporal trends in severe postpartum hemorrhage. Am J Obstet Gynecol 2013, 209, 449–e1. [Google Scholar]
- Hytten, F. Blood volume changes in normal pregnancy. Clin Haematol 1985, 14, 601–612. [Google Scholar] [CrossRef]
- Christenson, R.K.; Prior, R.L. Uterine blood flow and nutrient uptake during late gestation in ewes with different numbers of fetuses. J Anim Sci 1978, 46, 189–200. [Google Scholar] [CrossRef]
- Blitz MJ, Yukhayev A, Pachtman SL, Reisner J, Moses D, Sison CP, et al. Twin pregnancy and risk of postpartum hemorrhage. J Matern Fetal Neonatal Med 2020, 33, 3740–3745. [Google Scholar] [CrossRef] [PubMed]
- Fan D, Xia Q, Liu L, Wu S, Tian G, Wang W, et al. The incidence of postpartum hemorrhage in pregnant women with placenta previa: a systematic review and meta-analysis. PloS one 2017, 12, e0170194. [Google Scholar]
- Fan, D.; Wu, S.; Wang, W.; Xin, L.; Tian, G.; Liu, L.; Feng, J.; Guo, X.; Liu, Z. Prevalence of placenta previa among deliveries in Mainland China: A PRISMA-compliant systematic review and meta-analysis. Medicine 2016, 95, e5107. [Google Scholar] [CrossRef] [PubMed]
- Adere, A.; Mulu, A.; Temesgen, F. Neonatal and maternal complications of placenta praevia and its risk factors in Tikur Anbessa specialized and Gandhi memorial hospitals: Unmatched case-control study. J. Pregnancy 2020, 2020, 5630296. [Google Scholar] [CrossRef]
- Ge, J.; Liao, H.; Duan, L.; Wei, Q.; Zeng, W. Uterine packing during cesarean section in the management of intractable hemorrhage in central placenta previa. Arch Gynecol Obstet 2012, 285, 285–289. [Google Scholar] [CrossRef]
- Akhtar, R.; Sanodia Afridi, R.K.; Malik, N.N. Frequency of maternal and fetal outcome in grand multipara women. KJMS 2018, 11, 376–379. [Google Scholar]
- Mgaya, A.H.; Massawe, S.N.; Kidanto, H.L.; Mgaya, H.N. Grand multiparity: is it still a risk in pregnancy? . BMC Pregnancy Childbirth 2013, 13, 1–8. [Google Scholar] [CrossRef]
- A Performance, monitoring & accountability 2020 (PMA) ETHIOPIA: Addis Ababa University’s School of Public Health at the College of Health Sciences (AAU/SPH/CHS) 2014.Available at: https://www.pmadata.org/sites/default/files/data_product_results/PMA2020-Ethiopia-R6-FP-Brief.pdf.

| Variables | N | (%) |
| Age in Yrs. | ||
| 15 - 19 yrs. | 06 | 2.5 |
| 20 - 24 yrs. | 48 | 20.1 |
| 25 - 29 yrs. | 87 | 36.4 |
| 30 - 34 yrs. | 70 | 29.2 |
| 35 - 39 yrs. | 26 | 10.9 |
| > 40 yrs. | 02 | 0.84 |
| Gravidity status | ||
| Primigravida | 93 | 38.9 |
| Second gravida | 48 | 20.1 |
| Third gravida | 44 | 18.4 |
| Fourth gravida | 26 | 10.9 |
| Fifth gravida | 13 | 5.4 |
| Sixth gravida | 09 | 3.7 |
| Seventh gravida | 03 | 1.3 |
| Eighth gravida & above | 03 | 1.3 |
| Parity | ||
| 0 | 113 | 47.3 |
| 1 | 71 | 29.7 |
| 2 | 32 | 13.4 |
| 3 | 14 | 5.9 |
| 4 | 04 | 1.7 |
| 5 | 03 | 1.2 |
| > 5 | 02 | 0.8 |
| Risk Factors | ||
| Twin pregnancy | 04 | 1.7 |
| Polyhydramnios | 06 | 2.5 |
| Grand multipara | 09 | 3.8 |
| H/o previous PPH | 03 | 1.2 |
| Anemia | 32 | 13.4 |
| Low-lying Placenta | 02 | 0.8 |
| Hypotension | 08 | 3.4 |
| Chorioamnionitis | 01 | 0.4 |
| IUFD | 05 | 2.1 |
| GDM | 05 | 2.1 |
| Macrosomia | 02 | 0.8 |
| Variables | N | % |
| Change in HB (%) | ||
| 0-0.5 | 161 | 67.4 |
| 0.6-1.0 | 63 | 26.4 |
| 1.1-2 | 11 | 4.6 |
| 2.1-5 | 03 | 1.2 |
| > 5 | 01 | 0.4 |
| Change in P.C.V. (%) | ||
| < 1 | 08 | 3.4 |
| 1 – 2 | 177 | 74.0 |
| 3 – 4 | 44 | 18.4 |
| > 5 | 10 | 4.2 |
| Risk Factor | Total | PPH | % |
| Twin pregnancy | 04 | 01 | 25.0 |
| Low-lying Placenta | 02 | 01 | 50 |
| Previous h/o PPH | 03 | 01 | 33.33 |
| Grand multipara | 09 | 03 | 33.33 |
| Others | 62 | 00 | 00 |
| +No risk factors | 159 | 05 | 3.1 |
|
PPH (n=11) |
No PPH (n=228) |
Pearson Chi-Square P value (X2, Df) |
Yaes corrected Chi-Square P value (X2, Df) |
|
|
With any risk factors (n=80) |
6 (3.68%) [1.46] |
74 (76.32%) [0.07] |
0.012 (2.299, 1) |
0.234 (1.414, 1) |
| Without any risk factors (n=159) | 5 (7.32%) [0.73] |
154 (151.68%) [0.04] |
| R | R Square | Adjusted R Square | Std. Error of the Estimate |
| .512a | .262 | .226 | .159 |
| Sum of Squares | df | Mean Square | F | Sig. | |
| Regression | 2.026 | 11 | .184 | 7.298 | .000b |
| Residual | 5.705 | 226 | .025 | ||
| Total | 7.731 | 237 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



