Submitted:
09 January 2025
Posted:
09 January 2025
You are already at the latest version
Abstract
Familial adenomatous polyposis (FAP) is a genetic disease caused by an APC mutation. It develops into multiple adenomatous polyps when patients are in their early 20s and eventually transforms into colorectal cancer at 100% penetrance unless treated. Therefore, prophylactic surgery is recommended as the only effective treatment option. However, individual approaches, such as total colectomy with ileorectal anastomosis, proctocolectomy with stapled ileal pouch-anal anastomosis (IPAA), proctocolectomy with mucosectomy and handsewn IPAA, and total proctocolectomy with end ileostomy, are required based on the balance between the risk of metachronous rectal cancer, postoperative complications, and a decreased anal function. We herein summarize the current evidence regarding the surgical treatment and postoperative surveillance for FAP.
Keywords:
familial adenomatous polyposis
; surgical treatment
; postoperative surveillance
1. Overview
Familial adenomatous polyposis (FAP) is a hereditary autosomal dominant disease caused by pathogenic germline variants of the adenomatous polyposis coli (APC) gene, a tumor suppressor gene located on the long arm of chromosome 5 (5q22.2), the main symptom of which is colorectal adenomatous polyposis [1]. As patients with FAP have an extremely high risk of developing colorectal cancer, appropriate therapeutic interventions for preventing colorectal cancer are necessary. Unless treated, approximately 50% of patients with FAP develop colorectal cancer in their 40s, and almost all patients with FAP develop colorectal cancer by 60 years old [2]. In addition, surveillance and treatment considering extracolonic lesions associated with FAP are necessary because various associated neoplastic and non-neoplastic lesions can develop in the gastrointestinal tract and other organs [1]. Neoplastic lesions, such as desmoid tumors and duodenal cancer, can also cause death in patients with FAP [3], although most deaths in patients with FAP are due to colorectal cancer [3].
2. Clinical Features
FAP is sometimes classified into three categories based on adenoma density: severe FAP, sparse FAP, and attenuated FAP (AFAP) (Table 1) [1]. Severe FAP is a phenotype with more than 1000 adenomas, in which normal colorectal mucosa cannot be endoscopically observed because of the presence of numerous adenomas. Sparse FAP is a phenotype with 100-1000 adenomas in which normal colorectal mucosa is visualized. AFAP is a phenotype with 10-100 adenomas in which germline variants are often detected. Severe and sparse FAP are collectively referred to as classical FAP. The density of adenomas is associated with the presence of germline variants in APC [1]. Classical FAP is characterized by hundreds to thousands of colorectal adenomatous polyps, with an onset at a mean age of 16 [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36] years old. In classical FAP, 95% of patients will have polyps by 35 years old, and colorectal cancer is inevitable without intervention, such as colectomy/proctocolectomy. AFAP is associated with fewer adenomas, an older age at the diagnosis, and a lower lifetime risk of colorectal cancer than classical FAP [4,5]. According to a Japanese multicenter study, the age at which half of colorectal cancers develop was 41 years old for patients with severe FAP, 48 years old for those with sparse FAP, and 59 years old for those with AFAP [6].
3. Surveillance from the Diagnosis of FAP to Surgery
Recommendations for endoscopic surveillance for FAP are as follows: in patients with classical FAP, it is recommended to begin endoscopy at an interval of 1-2 years after reaching 10 years old [10] because colorectal cancer development is at a very low frequency before 10 years old; however, a European study found a 0.2% incidence of colorectal cancer in the early teenage years [8]. In patients with AFAP, it is recommended to begin endoscopy at an interval of 2-3 years in the late teenage years [1], as the age at which colorectal cancer develop is 10-15 years later than in patients with classical FAP, and colorectal cancer development is rare in patients under 30 years old [4,5].
4. Factors Determining the Timing of Surgery
A staging system based on the endoscopic findings, such as the number and diameter of colorectal adenomas, has been proposed by the International Society for Gastrointestinal Hereditary Tumors (InSiGHT) [9]. This staging system, based on polyp burden, is useful for judging surgical indications. Furthermore, an increase in polyp burden indicates the need for surgical treatment [10]. In addition, the cumulative prevalence of colorectal cancer, APC gene mutation site [11,12], age at death or age at cancer onset, presence of desmoid tumors in members of the pedigree [13], social background such as education and employment [14], and fertility [15] are also important factors that determine the timing of surgical treatment. From the perspective of avoiding the development of colorectal cancer, most patients with FAP are recommended to undergo surgical treatment in their 20s, but some patients with classical FAP may be recommended to undergo surgical treatment even in their teens [16,17]. It has been reported that if surgical treatment is not performed, the risk of developing stage ≥II colorectal cancer increases dramatically after 34 years old in patients with the classical FAP genotype and after 49 years old in patients with the AFAP genotype [12].
5. Surgical Treatment
5.1. Selection of Surgical Procedure
The goal of surgery in patients with FAP is to prevent the development of colorectal cancer and maintain the quality of life. Although intensive endoscopic removal for downstaging of polyp burden in patients with mild-to-moderate FAP who request postponement of surgery or refuse to undergo surgery may prevent colorectal cancer without implementing colectomy/proctocolectomy [18,19], the most effective and reliable treatment to avoid death from colorectal cancer is prophylactic colectomy/proctocolectomy before the development of colorectal cancer.
The surgical options for FAP are (i) total proctocolectomy with end ileostomy (TPC), (ii) total proctocolectomy with ileal pouch anal anastomosis (IPAA), and (iii) total colectomy with ileorectal anastomosis (IRA). IPAA includes hand-sewn IPAA with mucosectomy of the anal transition zone (AZT), and stapled IPAA. TPC, which requires permanent ileostomy, is performed in patients with an impaired sphincter function, lower rectal cancer, or cancer requiring radiation therapy and in those who wish to avoid the functional sequelae of a pouch. IRA is a relatively simple and straightforward procedure compared to IPAA, while IPAA is a more extensive surgery than IRA, with a higher possibility of disadvantages such as pelvic abscess, fistula, reoperation, fecal incontinence, and decreased fertility [15,20]. In contrast, patients who undergo IRA may develop polyps or cancer in the remaining rectum and subsequently require additional rectal resection [21]. Owing to advances in surgical techniques, the proportion of IPAA is increasing, and IPAA is currently the most commonly selected surgical procedure for FAP. However, no randomized trials have compared the impact of IPAA and IRA on the long-term prognosis. Ardoino et al. performed a retrospective analysis of 925 cases of FAP treated surgically using data from the Italian nationwide registry, and found that the 20-year survival rate was higher in the IRA group than in the IPAA group (0.82 vs. 0.75: p=0.003) [22]. The main prognostic factors affecting overall survival were age and the presence of cancer during surgery. Based on the above, it has been stated that IPAA is not necessarily required if there is no cancer or high-grade dysplasia and that the surgical procedure should be selected based on individual background factors. Although IRA carries a risk of rectal cancer, IRA can be offered as an option for surgical treatment of FAP, specifically when rectal adenomas of ≥5 mm can be endoscopically removed [22]. In addition, IRA plus strict follow-up with colonoscopy can also be an option for patients with <20 rectal polyps because the incidence of rectal cancer development is relatively low (1.6%) in such cases [23]. Nieuwenhuis et al. also demonstrated that the cumulative risks of secondary proctectomy 20 years after primary colectomy varied by genotype (attenuated: 10%, intermediate: 39%, severe: 61%) and argued that patients with a severe genotype will benefit from primary proctocolectomy with IPAA because they have a high risk of secondary proctectomy [24]. Furthermore, according to a meta-analysis of colectomy and desmoid tumors in FAP, fewer desmoid tumors were observed after laparoscopic IRA than laparoscopic IPAA [25]. Conversely, IRA should not be selected in the following cases because of the increased risk of cancer development in the remaining rectum: rectal cancer, >20 synchronous rectal adenomas, adenomas with high-grade dysplasia, polyps ≥30 mm, and cases with a severe family history of an aggressive phenotype [22]. The incidence of postoperative adenomas after hand-sewn IPAA with mucosectomy of the AZT was lower than that after stapled IPAA (22.6% vs. 51.1% at 10 years) [26]. In addition, Tatsuta et al. reported that the overall survival was significantly better in the hand-sewn IPAA with mucosectomy of AZT group than in the stapled IPAA group (96.6% vs. 63.7 at 20 years) [27], although this study was a retrospective analysis of a small number of cases. However, handsewn IPAA with mucosectomy of the AZT may result in worse functional outcomes than stapled IPAA, and there was no marked difference in the risk of postoperative cancer development between the two methods [26]. To date, there has been little evidence that mucosectomy of AZT should be performed routinely [22]. However, mucosectomy of AZT is necessary in cases where the polyp burden extends to the dentate line [22].
5.2. Surgical Treatment for FAP with Advanced Colorectal Cancer
Regarding surgical treatment for FAP with advanced colorectal cancer, a comprehensive judgment should be made, taking into account the TNM stage of the colorectal cancer and the location of the tumor. If radical resection of colorectal cancer is expected, total proctocolectomy, including regional lymph node dissection, may be an option [1].
5.3. Surgical Techniques for Mesenteric Lengthening in IPAA
Creating tension-free IPAA following proctocolectomy is an important challenge in reconstruction during the surgical treatment of FAP. In patients with obesity, a narrow pelvis, thick mesentery, and extensive adhesions, sufficient mesentery length may not be available, resulting in tension at the anastomotic site. Tension at the anastomotic site may cause ischemia, necrosis, and anastomotic leakage. Therefore, surgical lengthening techniques are required to create tension-free anastomoses.
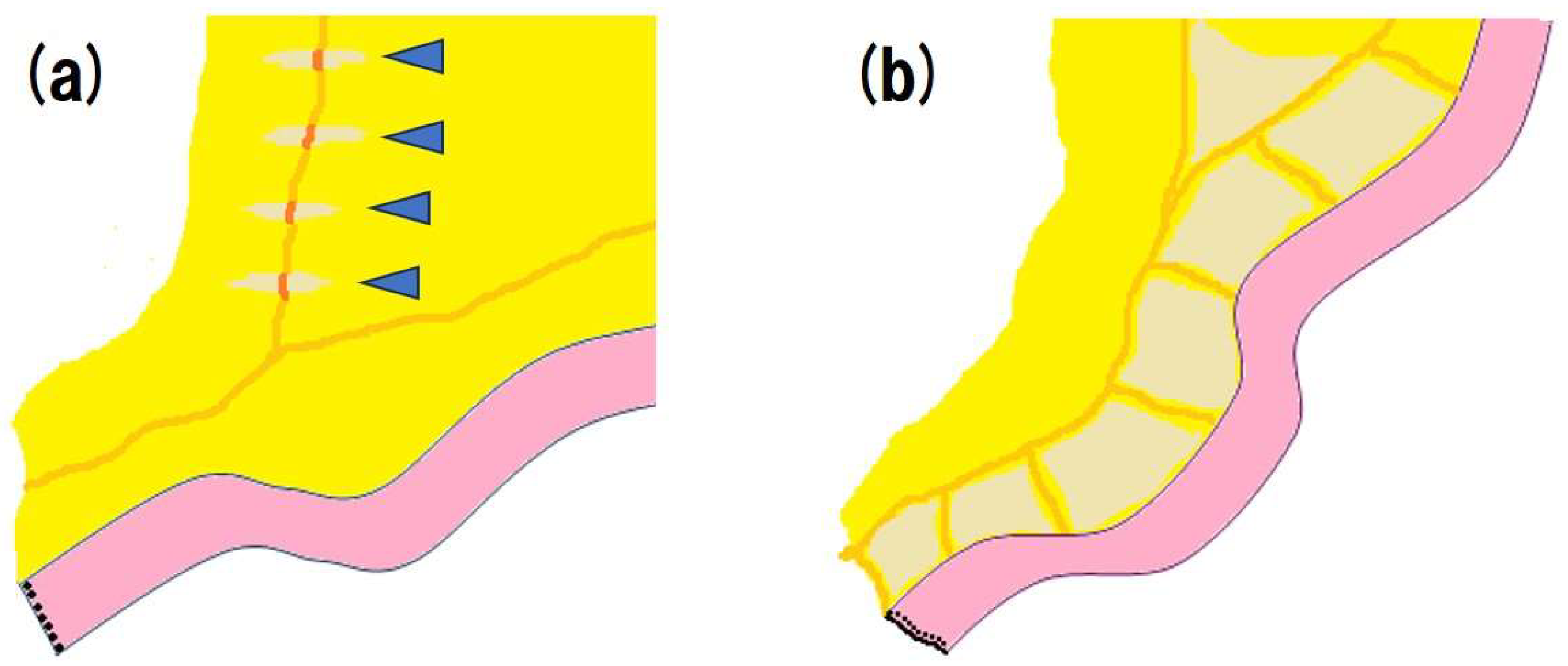
Several surgical techniques are available for lengthening the mesentery. Folding the pouch anteriorly (with the mesentery posterior) has been reported to result in a mesentery approximately 1 cm longer than when the pouch is folded posteriorly [28]. Stepladder incision is a simple and safe technique for lengthening the mesentery (Fig.1a). It has been reported that by making serial transverse incisions of approximately 1-3 cm in width on the anterior and posterior surfaces of the mesentery, the mesentery can be lengthened by 6-8 cm [29]. If sufficient mesentery length cannot be secured even after performing stepladder incision, it may be possible to lengthen the mesentery further by skeletonizing the mesentery around the vessels (Fig.1b). In addition, although the J-type ileal pouch is popular, it has been reported that the mesentery in the S-type ileal pouch is on average 2-4 cm longer than that in the J-type ileal pouch [30]. Division and ligation of the mesenteric vessels are frequently used as lengthening techniques. It is possible to further increase the length by dividing the ileocolonic or superior mesenteric arteries. Depending on the case, an additional length of 5 cm or more can be obtained [31,32,33]. Ligation of the terminal ileal mesenteric artery, right colic artery, and marginal vascular arcade is another option. However, this procedure may result in decreased blood supply to the ileal pouch. If a sufficient blood supply to the terminal ileum is not ensured, there may be an increased risk of anastomotic leakage and malfunction of the ileal pouch. To maintain sufficient blood supply to the terminal ileum even after the division and ligation of the mesenteric vessels, a clamping test, in which blood flow is temporarily interrupted before the mesenteric arteries are divided, is useful. If vascular pulsations remain and the color of the intestinal tract does not change after interruption of the blood flow for 15 minutes, the mesenteric arteries can be divided safely.
Figure 1.
Surgical techniques for lengthening the mesentery; stepladder incisions (b)skeletonization.
Figure 1.
Surgical techniques for lengthening the mesentery; stepladder incisions (b)skeletonization.
For tension-free anastomosis, a balance between an adequate mesenteric length and sufficient blood supply is important.
5.4. Surgical Approach
In recent years, the laparoscopic approach has been adopted increasingly frequently for surgical treatment of FAP [34,35,36,37]. According to a nationwide Japanese multicenter study, the incidence of postoperative complications and the rate of preservation of the anal, urinary, and sexual functions were equivalent between laparoscopic surgery and open surgery, although the laparoscopic approach was associated with a longer operation time (TPC with IPAA: 482 min vs. 275 min, respectively, p<0.001) [35]. A report from the United States that examined the impact of the surgical approach to IPAA for ulcerative colitis and FAP showed that laparoscopic surgery takes longer than open surgery (266.7 min vs. 187.5 min, respectively, P<0.0001), but there was no significant difference between laparoscopic and open IPAA with respect to blood loss, blood transfusions, length of hospital stay, re-admission rate, and incidence of postoperative complications, and that diverting loop ileostomy closure can be performed earlier in patients who received laparoscopic IPAA than in those who received open IPAA (80.4 days vs. 104.5 days, respectively, p=0.045) [38]. It has also been reported that laparoscopic surgery is less likely to cause postoperative adhesions than open surgery, resulting in a lower decline in fertility [36].
5.5. Disadvantages of Undergoing Surgery
Postoperative complications include anastomotic leakage, pelvic abscesses, and fistulas. The incidence of anastomotic leakage after IPAA was reported to be relatively high (6.3%) [39], although this result was obtained from a study that included patients with ulcerative colitis only, ulcerative colitis and a combination with Crohn’s disease, indeterminate colitis, FAP, and colorectal cancer. Such infectious complications may necessitate reoperation and result in a permanent endileostomy. In addition, postoperative infectious complications increase the risk of pouch dysfunction, such as frequent bowel movements, fecal incontinence, and difficulty in defecation due to stenosis. Furthermore, pouchitis is also a complication that affects patients, although it is less frequent in patients with FAP than in those with ulcerative colitis. Most cases improve with antibiotics; however, some patients suffer from refractory pouchitis, which develops repeatedly in a short period and is resistant to antibiotic treatment. Pouch dysfunction and pouchitis have a significant negative impact on patients’ quality of life and mental wellbeing.
Other concerns include ileus due to postoperative adhesions and, although rare, afferent limb syndrome, obstruction of passage due to flexion, and torsion at the proximal portion of the ileal pouch [40].
Other disadvantages of surgical treatment include deterioration of the body image and self-esteem. Women tend to have lower postoperative self-esteem than men [41]; however, choosing laparoscopic surgery may solve these problems.
Because surgical treatment of FAP is often performed in young patients, maintaining fertility and the sexual function is also an important issue. In men, pelvic nerve damage can cause sexual dysfunction such as difficulty in achieving erection or orgasm, and decreased sexual desire, intercourse satisfaction, and overall sexual satisfaction. In women, sexual dysfunction can also occur, such as decreased desire, arousal, lubrication, orgasm, satisfaction, and dyspareunia. Infertility can also occur because of blockage of the fallopian tubes caused by postoperative adhesions [42].
In surgical treatment for FAP, it is important to focus on preserving the organ function so as not to reduce the patient's quality of life, as well as to prevent the development of cancer.

Table 2.
Disadvantage of undergoing surgery.
| Postoperative infectious complications | |
| Anastomotic leakage | |
| Pelvic abscess | |
| Fistula | |
| Pouch-related complications | |
| Pouch dysfunction (frequent bowel movements, fecal incontinence, difficulty in defecation due to stenosis) | |
| Pouchitis | |
| Others | |
| Deterioration of the body image and self-esteem | |
| Decreasing fertility and the sexual function |
6. Surveillance After Surgical Treatments
In patients who undergo IRA, cancer development in the remaining rectum is not uncommon. According to previous reports, 24%-43% of patients who undergo IRA develop cancer in the remaining rectum [43,44]. Therefore, long-term endoscopic surveillance after IRA to monitor cancer development is necessary. Annual endoscopic surveillance is typically recommended [22], but biannual endoscopic surveillance is acceptable, depending on the polyp burden [45]. Even in patients who have undergone IPAA, a small amount of rectal mucosa and AZT mucosa remains, and adenomas and cancers may develop in the ileal pouch, although the incidence is very low (the overall prevalence of pouch neoplasia is estimated to be approximately 0.01%) [45]. Therefore, long-term endoscopic surveillance is necessary for patients who have undergone IPAA. In addition, extracolonic manifestations of FAP, such as desmoid tumors and duodenal cancer, can cause death. Therefore, surveillance of extracolonic manifestations of FAP is also necessary.
Table 3.
Surveillance after surgical treatments.
| Examination | Comment |
| Colonoscopy | |
| After IRA | Typically annual, but biannual is acceptable depending on polyp burden |
| After IPAA | For small amount of rectal mucosa, AZT mucosa, and ileal pouch |
| Upper gastrointestinal endoscopy | Gastric polyps and duodenal polyps/cancer |
| Abdominal CT | Desmoid tumors |
| Thyroid ultrasound | Thyroid cancer |
| Brain CT | Brain tumor |
IRA, ileorectal anastomosis; IPAA, ileal pouch anal anastomosis; AZT, anal transition zone; CT, computed tomography.
7. Conclusions
In surgical treatment for FAP, the timing and the type of procedure, especially the extent of resection and reconstruction methods, are all important factors. It is desirable to provide individualized surgical treatment based on each patients’ specific background, including the genetic type.
Author Contributions
Conceptualization, M.S. and K.M; supervision, H.K. and T.F.; writing—original draft, M.S.; writing—review and editing, M.S., H.K., T.F. and K.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
We thank Dr. Brian Quinn, who provided medical writing services on behalf of JMC Ltd.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tomita N, Ishida H, Tanakaya K, Yamaguchi T, Kumamoto K, Tanaka T, Hinoi T, Miyakura Y, Hasegawa H, Takayama T, Ishikawa H, Nakajima T, Chino A, Shimodaira H, Hirasawa A, Nakayama Y, Sekine S, Tamura K, Akagi K, Kawasaki Y, Kobayashi H, Arai M, Itabashi M, Hashiguchi Y, Sugihara K; Japanese Society for Cancer of the Colon, Rectum. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2020 for the Clinical Practice of Hereditary Colorectal Cancer. Int J Clin Oncol. 2021 Aug;26(8):1353-1419. PMID: 34185173. [CrossRef]
- Bussey HJR, Morson BC: Familial Polyposis Coli. In: Lipkin M, Good RA 8eds): Gastrointestinal Tract Cancer. Sloan-Kettering Institute Cancer Series. Springer, Boston, MA, 1978.
- Iwama T, Tamura K, Morita T, Hirai T, Hasegawa H, Koizumi K, Shirouzu K, Sugihara K, Yamamura T, Muto T, Utsunomiya J; Japanese Society for Cancer of the Colon and Rectum. A clinical overview of familial adenomatous polyposis derived from the database of the Polyposis Registry of Japan. Int J Clin Oncol. 2004 Aug;9(4):308-16. PMID: 15375708. [CrossRef]
- Nielsen M, Hes FJ, Nagengast FM et al (2007) Germline mutations in APC and MUTYH are responsible for the majority of families with attenuated familial adenomatous polyposis. Clin Genet 71:427–433.
- Burt RW, Leppert MF, Slattery ML, Samowitz WS, Spirio LN, Kerber RA, Kuwada SK, Neklason DW, Disario JA, Lyon E, Hughes JP, Chey WY, White RL. Genetic testing and phenotype in a large kindred with attenuated familial adenomatous polyposis. Gastroenterology. 2004 Aug;127(2):444-51. PMID: 15300576. [CrossRef]
- Kobayashi H, Ishida H, Ueno H, Hinoi T, Inoue Y, Ishida F, Kanemitsu Y, Konishi T, Yamaguchi T, Tomita N, Matsubara N, Watanabe T, Sugihara K. Association between the age and the development of colorectal cancer in patients with familial adenomatous polyposis: a multi-institutional study. Surg Today. 2017 Apr;47(4):470-475. Epub 2016 Aug 9.PMID: 27506752. [CrossRef]
- Jasperson KW, Patel SG, Ahnen DJ (1993–2020) APC-associated polyposis conditions. 1998 Dec 18 [updated 2017 Feb 2 In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. University of Washington, Seattle. Available via http:// www.ncbi.nlm.nih.gov/books/NBK1245/.
- Vasen HF, Möslein G, Alonso A, Aretz S, Bernstein I, Bertario L, Blanco I, Bülow S, Burn J, Capella G, Colas C, Engel C, Frayling I, Friedl W, Hes FJ, Hodgson S, Järvinen H, Mecklin JP, Møller P, Myrhøi T, Nagengast FM, Parc Y, Phillips R, Clark SK, de Leon MP, Renkonen-Sinisalo L, Sampson JR, Stormorken A, Tejpar S, Thomas HJ, Wijnen J. Guidelines for the clinical management of familial adenomatous polyposis (FAP). Gut. 2008 May;57(5):704-13. Epub 2008 Jan 14.PMID: 18194984. [CrossRef]
- Lynch PM, Morris JS, Wen S, Advani SM, Ross W, Chang GJ, Rodriguez-Bigas M, Raju GS, Ricciardiello L, Iwama T, Rossi BM, Pellise M, Stoffel E, Wise PE, Bertario L, Saunders B, Burt R, Belluzzi A, Ahnen D, Matsubara N, Bülow S, Jespersen N, Clark SK, Erdman SH, Markowitz AJ, Bernstein I, De Haas N, Syngal S, Moeslein G. A proposed staging system and stage-specific interventions for familial adenomatous polyposis. Gastrointest Endosc. 2016 Jul;84(1):115-125.e4. Epub 2016 Jan 6.PMID: 26769407. [CrossRef]
- Septer S, Lawson CE, Anant S, Attard T. Familial adenomatous polyposis in pediatrics: natural history, emerging surveillance and management protocols, chemopreventive strategies, and areas of ongoing debate. Fam Cancer. 2016 Jul;15(3):477-85. PMID: 27056662. [CrossRef]
- Rozen P, Macrae F. Familial adenomatous polyposis: The practical applications of clinical and molecular screening. Fam Cancer. 2006;5(3):227-35. PMID: 16998668. [CrossRef]
- Mori Y, Ishida H, Chika N, Ito T, Amano K, Chikatani K, Takeuchi Y, Kono M, Shichijo S, Chino A, Nagasaki T, Takao A, Takao M, Nakamori S, Sasaki K, Akagi K, Yamaguchi T, Tanakaya K, Naohiro T, Ajioka Y. Usefulness of genotyping APC gene for individualizing management of patients with familial adenomatous polyposis. Int J Clin Oncol. 2023 Dec;28(12):1641-1650. Epub 2023 Oct 18.PMID: 37853284. [CrossRef]
- Sturt NJ, Gallagher MC, Bassett P, Philp CR, Neale KF, Tomlinson IP, Silver AR, Phillips RK. Evidence for genetic predisposition to desmoid tumours in familial adenomatous polyposis independent of the germline APC mutation. Gut. 2004 Dec;53(12):1832-6. PMID: 15542524. [CrossRef]
- Crabtree MD, Tomlinson IP, Talbot IC, Phillips RK. Variability in the severity of colonic disease in familial adenomatous polyposis results from differences in tumour initiation rather than progression and depends relatively little on patient age. Gut. 2001 Oct;49(4):540-3. PMID: 11559652. [CrossRef]
- Olsen KØ, Juul S, Bülow S, Järvinen HJ, Bakka A, Björk J, Oresland T, Laurberg S. Female fecundity before and after operation for familial adenomatous polyposis. Br J Surg. 2003 Feb;90(2):227-31. PMID: 12555301. [CrossRef]
- Rozen P, Samuel Z, Rabau M, Goldman G, Shomrat R, Legum C, Orr-Urtreger A. Familial adenomatous polyposis at the Tel Aviv Medical Center: demographic and clinical features. Fam Cancer. 2001;1(2):75-82. PMID: 14574001. [CrossRef]
- Eccles DM, Lunt PW, Wallis Y, Griffiths M, Sandhu B, McKay S, Morton D, Shea-Simonds J, Macdonald F. An unusually severe phenotype for familial adenomatous polyposis. Arch Dis Child. 1997 Nov;77(5):431-5. PMID: 9487968. [CrossRef]
- Ishikawa H, Mutoh M, Iwama T, Suzuki S, Abe T, Takeuchi Y, Nakamura T, Ezoe Y, Fujii G, Wakabayashi K, Nakajima T, Sakai T. Endoscopic management of familial adenomatous polyposis in patients refusing colectomy. Endoscopy. 2016 Jan;48(1):51-5. Epub 2015 Sep 9. PMID: 26352809. [CrossRef]
- Ishikawa H, Yamada M, Sato Y, Tanaka S, Akiko C, Tajika M, Doyama H, Takayama T, Ohda Y, Horimatsu T, Sano Y, Tanakaya K, Ikematsu H, Saida Y, Ishida H, Takeuchi Y, Kashida H, Kiriyama S, Hori S, Lee K, Tashiro J, Kobayashi N, Nakajima T, Suzuki S, Mutoh M; J-FAPP Study III Group. Intensive endoscopic resection for downstaging of polyp burden in patients with familial adenomatous polyposis (J-FAPP Study III): A multicenter prospective interventional study. Endoscopy. 2023 Apr;55(4):344-352. PMID: 36216266. [CrossRef]
- Aziz O, Athanasiou T, Fazio VW, Nicholls RJ, Darzi AW, Church J, Phillips RK, Tekkis PP. Meta-analysis of observational studies of ileorectal versus ileal pouch-anal anastomosis for familial adenomatous polyposis. Br J Surg. 2006 Apr;93(4):407-17. PMID: 16511903. [CrossRef]
- Ten YV, Tillyashakhov M, Islamov H, Ziyaev Y. The risk of malignization incidence in patients with polyps and polyposis of the colon and rectum. Ann Oncol. 2019;30:ix37.
- Ardoino I, Signoroni S, Malvicini E, Ricci MT, Biganzoli EM, Bertario L, Occhionorelli S, Vitellaro M. Long-term survival between total colectomy versus proctocolectomy in patients with FAP: a registry-based, observational cohort study. Tumori. 2020 Apr; 106(2): 139-148. [CrossRef]
- Poylin VY, Shaffer VO, Felder SI, Goldstein LE, Goldberg JE, Kalady MF, Lightner AL, Feingold DL, Paquette IM; Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Inherited Adenomatous Polyposis Syndromes. Dis Colon Rectum. 2024 Feb 1;67(2):213-227. PMID: 37682806. [CrossRef]
- Church J, Burke C, McGannon E, Pastean O, Clark B. Predicting polyposis severity by proctoscopy: how reliable is it? Dis Colon Rectum. 2001;44:1249–1254.
- Nieuwenhuis MH, Bülow S, Björk J, Järvinen HJ, Bülow C, Bisgaard ML, Vasen HF. Genotype predicting phenotype in familial adenomatous polyposis: a practical application to the choice of surgery. Dis Colon Rectum. 2009 Jul;52(7):1259-63. PMID: 19571702. [CrossRef]
- Aelvoet AS, Struik D, Bastiaansen BAJ, Bemelman WA, Hompes R, Bossuyt PMM, Dekker E. Colectomy and desmoid tumours in familial adenomatous polyposis: a systematic review and meta-analysis. Fam Cancer. 2022 Oct;21(4):429-439. PMID: 35022961. [CrossRef]
- von Roon AC, Will OC, Man RF, et al. Mucosectomy with handsewn anastomosis reduces the risk of adenoma formation in the anorectal segment after restorative proctocolectomy for familial adenomatous polyposis. Ann Surg. 2011;253:314–317.
- Tatsuta K, Sakata M, Iwaizumi M, Okamoto K, Yoshii S, Mori M, Asaba Y, Harada T, Shimizu M, Kurachi K, Takeuchi H. Long-term prognosis after stapled and hand-sewn ileal pouch-anal anastomoses for familial adenomatous polyposis: a multicenter retrospective study. Int J Colorectal Dis. 2024 Mar 2;39(1):32. PMID: 38431759. [CrossRef]
- Rottoli M, Tanzanu M, Lanci AL, Gentilini L, Boschi L, Poggioli G. Mesenteric lengthening during pouch surgery: technique and outcomes in a tertiary centre. Updates Surg. 2021 Apr;73(2):581-586. PMID: 33492620. [CrossRef]
- Baig MK, Weiss EG, Nogueras JJ, Wexner SD. Lengthening of small bowel mesentery: stepladder incision technique. Am J Surg. 2006 May;191(5):715-7. PMID: 16647367. [CrossRef]
- Smith L, Friend WG, Medwell SJ. The superior mesenteric artery. The critical factor in the pouch pull-through procedure. Dis Colon Rectum. 1984 Nov;27(11):741-4. PMID: 6499610. [CrossRef]
- Martel P, Majery N, Savigny B, Sezeur A, Gallot D, Malafosse M. Mesenteric lengthening in ileoanal pouch anastomosis for ulcerative colitis: Is high division of the superior mesenteric pedicle a safe procedure? Dis Colon Rectum. 1998 Jul;41(7):862-6; discussion 866-7. PMID: 9678371. [CrossRef]
- Cherqui D, Valleur P, Perniceni T, Hautefeuille P. Inferior reach of ileal reservoir in ileoanal anastomosis. Experimental anatomic and angiographic study. Dis Colon Rectum. 1987 May;30(5):365-71. PMID: 3568927. [CrossRef]
- Martel P, Blanc P, Bothereau H, Malafosse M, Gallot D. Comparative anatomical study of division of the ileocolic pedicle or the superior mesenteric pedicle for mesenteric lengthening. Br J Surg. 2002 Jun;89(6):775-8. PMID: 12027990. [CrossRef]
- Ueno H, Kobayashi H, Konishi T, Ishida F, Yamaguchi T, Hinoi T, Kanemitsu Y, Inoue Y, Tomita N, Matsubara N, Komori K, Ozawa H, Nagasaka T, Hasegawa H, Koyama M, Akagi Y, Yatsuoka T, Kumamoto K, Kurachi K, Tanakaya K, Yoshimatsu K, Watanabe T, Sugihara K, Ishida H. Prevalence of laparoscopic surgical treatment and its clinical outcomes in patients with familial adenomatous polyposis in Japan. Int J Clin Oncol. 2016 Aug;21(4):713-722. PMID: 26820718. [CrossRef]
- Konishi T, Ishida H, Ueno H, Kobayashi H, Hinoi T, Inoue Y, Ishida F, Kanemitsu Y, Yamaguchi T, Tomita N, Matsubara N, Watanabe T, Sugihara K. Feasibility of laparoscopic total proctocolectomy with ileal pouch-anal anastomosis and total colectomy with ileorectal anastomosis for familial adenomatous polyposis: results of a nationwide multicenter study. Int J Clin Oncol. 2016 Oct;21(5):953-961. PMID: 27095110. [CrossRef]
- Campos FG. Surgical treatment of familial adenomatous polyposis: dilemmas and current recommendations. World J Gastroenterol. 2014 Nov 28;20(44):16620-9. PMID: 25469031. [CrossRef]
- Kjaer MD, Laursen SB, Qvist N, Kjeldsen J, Poornoroozy PH. Sexual function and body image are similar after laparoscopy-assisted and open ileal pouch-anal anastomosis. World J Surg. 2014 Sep;38(9):2460-5. PMID: 24711157. [CrossRef]
- Fajardo AD, Dharmarajan S, George V, Hunt SR, Birnbaum EH, Fleshman JW, Mutch MG. Laparoscopic versus open 2-stage ileal pouch: laparoscopic approach allows for faster restoration of intestinal continuity. J Am Coll Surg. 2010 Sep;211(3):377-83. PMID: 20800195. [CrossRef]
- Heuthorst L, Wasmann KATGM, Reijntjes MA, Hompes R, Buskens CJ, Bemelman WA. Ileal Pouch-anal Anastomosis Complications and Pouch Failure: A systematic review and meta-analysis. Ann Surg Open. 2021 Jun 21;2(2):e074. eCollection 2021 Jun. PMID: 37636549. [CrossRef]
- Okita Y, Araki T, Kawamura M, Kondo S, Inoue M, Kobayashi M, Toiyama Y, Ohi M, Tanaka K, Inoue Y, Uchida K, Mohri Y, Kusunoki M. Clinical features and management of afferent limb syndrome after ileal pouch-anal anastomosis for ulcerative colitis. Surg Today. 2016 Oct;46(10):1159-65. Epub 2016 Jan 22. PMID: 26801343. [CrossRef]
- Kjaer MD, Laursen SB, Qvist N, Kjeldsen J, Poornoroozy PH. Sexual function and body image are similar after laparoscopy-assisted and open ileal pouch-anal anastomosis. World J Surg. 2014 Sep;38(9):2460-5. PMID: 24711157. [CrossRef]
- Oresland T, Palmblad S, Ellström M, Berndtsson I, Crona N, Hultén L. Gynaecological and sexual function related to anatomical changes in the female pelvis after restorative proctocolectomy. Int J Colorectal Dis. 1994 May;9(2):77-81. PMID: 8064194. [CrossRef]
- Koskenvuo L, Renkonen-Sinisalo L, Järvinen HJ, Lepistö A. Risk of cancer and secondary proctectomy after colectomy and ileorectal anastomosis in familial adenomatous polyposis. Int J Colorectal Dis. 2014 Feb;29(2):225-30. Epub 2013 Nov 30. PMID: 24292488. [CrossRef]
- Campos FG, Perez RO, Imperiale AR, Seid VE, Nahas SC, Cecconello I. Surgical treatment of familial adenomatous polyposis: ileorectal anastomosis or restorative proctolectomy? Arq Gastroenterol. 2009 Oct-Dec;46(4):294-9. PMID: 20232009. [CrossRef]
- Sriranganathan D, Kilic Y, Nabil Quraishi M, Segal JP. Prevalence of pouchitis in both ulcerative colitis and familial adenomatous polyposis: a systematic review and meta-analysis. Colorectal Dis. 2022;24:27–39.
Table 1.
Classification of familial adenomatous polyposis (FAP).
| Classical FAP | |||
| severe FAP | sparse FAP | attenuated FAP | |
| The number of adenomas | more than 1000 | 100-1000 | 10-100 |
| Endoscopic features | A normal mucosa cannot be observed | A normal mucosa is visualized | |
| The median age at which half of the cancers develop (years) | 41 | 48 | 59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



