
Submitted:
06 January 2025
Posted:
07 January 2025
You are already at the latest version
Abstract
Background/Objectives: Thyroid cancer is the most common cancer of the en-docrine system worldwide. Despite many available therapeutic options, the mortality rate of some subtypes, including anaplastic thyroid cancer, is still sig-nificant. Photodynamic therapy brings hope, which, through local activation of cell death pathways, as well as its effect on the immune system and vessels feeding the tumor, brings effects incomparable to classical methods. Photosensi-tizers particularly used in the case of thyroid cancer are hypericin, porphyrin, photophrin, radachlorin or 5-aminolevulinic acid. Even better effects are achieved by administering sulforaphane, carboplatin or genistein before therapy
Methods: For this research we review articles in regards to provide a critical summary of the existing literature on thyroid cancer to explain the current state of scientific evidence on this topic.
Conclusions: Photodynamic therapy is undoubtedly a technique of the future, the main advantages of which are low invasiveness, the possibility of combining with other treatment methods, or the possibility of outpatient use.
Keywords:
photophrine
; photosensitizer
; genistein hypericin
; carboplatin
; 5-aminolevulinic acid
; porphyrin
; radachlorin
; thyroid cancer
; ROS
; sulforaphene
; thyroid
; photodynamic therapy
1. Introduction
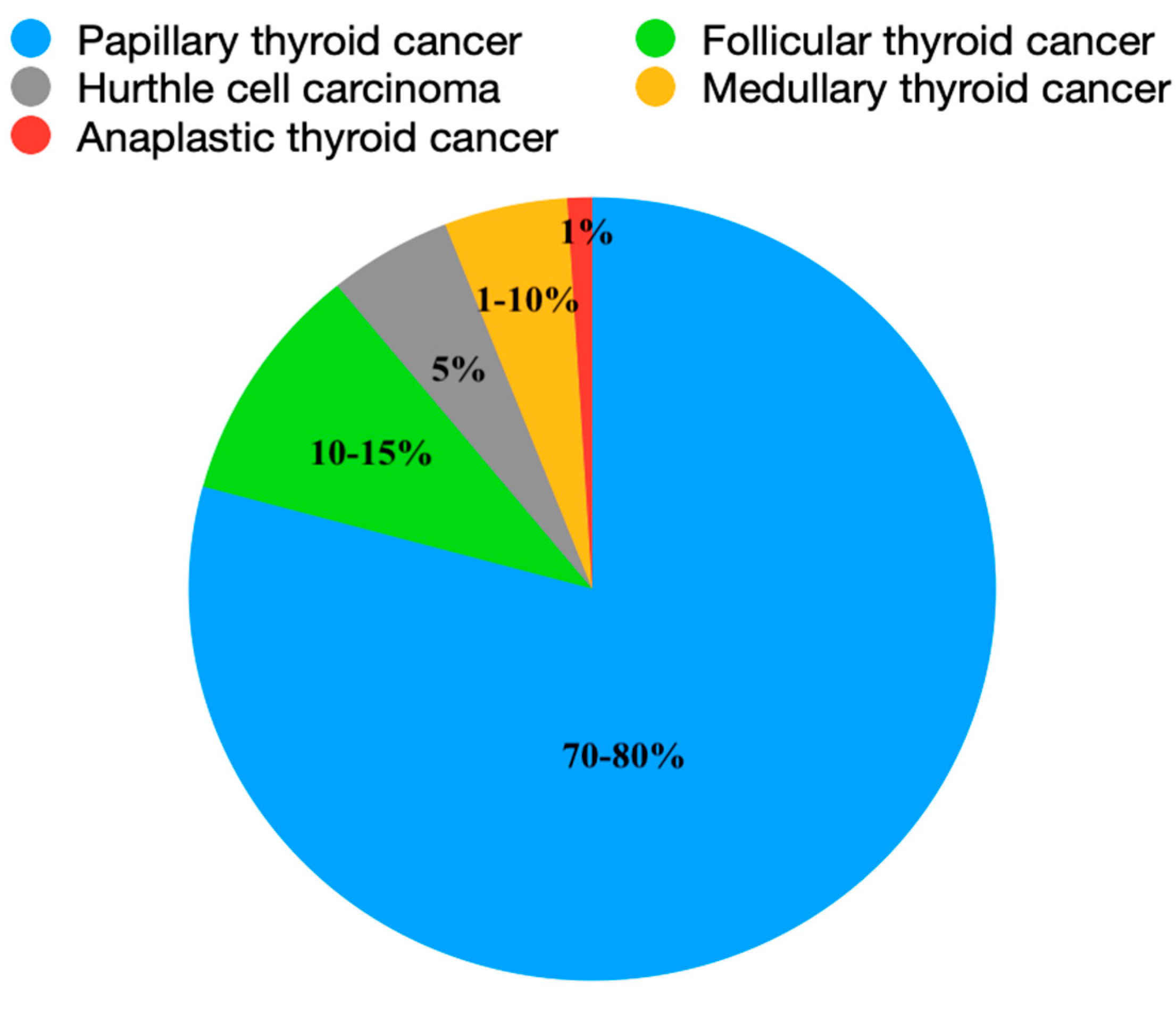
Thyroid cancer is the most common cancer of the endocrine system worldwide. Its incidence is estimated at about 6.7-9 cases per year, and the number of patients has been constantly growing for 30 years, with a constant number of deaths. [1,2,3,4] The peak incidence occurs between the ages of 51 and 60. [5] The prognosis of well-differentiated tumors detected at an early stage in the surgical stage is optimistic, in contrast to the prognosis of anaplastic cancer, which is most often diagnosed in the metastatic stage, and the median survival is about half a year. None of the previously used treatment methods, regardless of the way they are combined or intensified, is able to lead to long-term remission in most patients. Also, some clinical cases of other types of thyroid cancer are resistant to the proposed treatment and end in the patient's death. Photodynamic therapy is a hope, which, used alone or in combination with previously used chemotherapy, gave promising results in preclinical studies. [6,7,8,9,10]. The type of lesion determines the course of the disease, from slow-growing to aggressive, rapidly progressive forms. [1] Malignant changes derived from follicular cells are called differentiated thyroid cancer (DTC), and include papillary thyroid cancer (PTC, 70-80%), which has a 5-year survival rate of about 98% and recurrence of up to 7%, follicular thyroid cancer (FTC, 10-15%), and Hurthle cell carcinoma (HCC, 5%). [1,2,4,11,12,13,14] Together, they constitute 90-95% of thyroid cancers, and the 10-year survival rate is estimated at 98%. [1,2,5,15] The second type is medullary thyroid cancer (MTC), which arises from parafollicular C cells of the neural crest and accounts for approximately 1-10% of thyroid cancers. [1,2,15] The remaining 1% is anaplastic thyroid cancer (ATC), an undifferentiated lesion of follicular cells. It is said to arise from follicular and papillary carcinomas as a result of genomic changes. [16] It is characterized by a median survival of several months, an aggressive course, rapid metastasis, in up to 50% of patients at the time of hospital admission, and invasion of surrounding tissues. [1,2,17] The average age of onset is 65-70 years, and the average survival of patients with ATC using currently used therapies is estimated at 4-6 months, with approximately 35% of patients achieving 6-month survival. [6,16,18].
Figure 1.
Symbolic representation of the relationship between the different types of thyroid cancer.
Figure 1.
Symbolic representation of the relationship between the different types of thyroid cancer.
2. Materials and Methods
This literature review summarizes the current information available in the Pubmed and Google Scholar databases regarding thyroid cancer, its incidence, clinical presentation, genetic background, histopathological features, diagnosis and treatment, and photodynamic therapy, particularly in the context of its potential use in the treatment of thyroid cancer. Due to the type of cells from which thyroid cancer develops, it can be divided into several types.
2.1. Genetic Background
Thyroid cancers may have a genetic background. The association is mainly observed with abnormal activation of the phosphoinositide 3-kinase (PI3K) and mitogen-activated protein kinase (MAP, MAPK) pathways and with genes responsible for iodine metabolism in the thyroid encoding the sodium iodide symporter (NIS). [1,2,4] The PI3K pathway plays an important role in cellular mechanisms, including proliferation, survival, differentiation and apoptosis - its stimulation is the basis for uncontrolled multiplication of cancer cells leading to the development of cancer, especially in the head and neck region. This pathway is stimulated by the epidermal growth factor receptor (EGFR), and inhibited by the phosphatase and tensin homolog (PTEN). Overexpression of EGFR correlates with the clinical stage of ATC. [8] However, the loss of NIS expression in the basement membrane of thyroid cells, including cancer cells, is associated with impaired iodide transport to thyroid follicular cells, which results in the failure of RAI therapy (radioactive iodine therapy). Therefore, RAI is most effective in DTC. [4,21] It is estimated that in the case of PTC and FTC, the familial occurrence is about 5%. [1,2] PTC is associated with a point mutation in the BRAF V600E gene in 29-69%, and in 0-12% in the case of anaplastic carcinoma associated with PTC. The follicular variant of PTC shows a mutation in the RAS pro-to-oncogene in 10-20%. RET/PTC translocation occurs in about 7% of PTC. PTC may also be associated with rarer mutations, such as TERT mutations, in highly aggressive cases, NTRK1/3 fusion, E1F1AX, NF1/2, TP53, ERCC5, ATM or CHEK2 mutations. [1,2,12] In the case of FTC, a correlation was noted with mutations in the RAS proto-oncogene in 40-50%, NRAS more often than HRAS and KRAS, with translocation in the peroxisome proliferator-activated receptor γ PAX8 in 30-35%, with PTEN mutation and with TERT mutation in 17%. BRAF mutation is almost never observed. [1,2,12] Approximately 60% of Hurthle cell thyroid cancer cases are characterized by mutations in mitochondrial DNA. In addition, mTor activation and extensive LOH can often be detected in multiple chromosomes. TP53 and TERT mutations can be found especially in more aggressive forms. BRAF and RAS mutations are more common in other types of differentiated thyroid cancer. [2] Mutations detected in MTC include germline mutations of the RET proto-oncogene in about 25-50% of sporadic forms, in about 95-98% of hereditary forms of MTC, and RAS mutations in 25% of all forms. In about 20%, no RAS and RAT mutations are found. In 20-25% of MTC, it is a component of hereditary cancer syndromes such as multiple endocrine neoplasia 2A (MEN2A) and 2B (MEN2B) and hereditary MTC (FMTC), in the remaining cases it occurs sporadically. [1,2,15,22] 50-80% of anaplastic thyroid cancers are characterized by early inactivating mutations and inactivating mutations of the tumor suppressor gene p53, 66% by mutations in the CTNNB1 gene, 20-40% by RAS mutations, 28-45% by BRAF mutation/fusion, 10-18% by PI3CA mutations, 9-15% by PTEN mutations, 6-73% by TERT promoter mutations, 4-9% by RB1 mutations, 10-21% by NF1/2 mutations, 0-12% by mismatch mutations, 4-8% by CDKN1/2 mutations, 0-6% by STKI1 mutations. [1,2,13,17]
2.2. Histopathological Picture
Each type of thyroid cancer has its own specific appearance under the microscope. PTC forms papillae, the fibrous core of which is surrounded by a layer of neoplastic cells, without the presence of hair follicles. It is characterized by the presence of Psammoma bodies and "Annie's orphan eyes" nuclei. FTC has a variable histological appearance. In addition to typical follicular changes, poorly differentiated changes can also be found, with nuclear atypia, aggressive growth, infiltration of the capsule or vessels, and lack of follicles. The presence of eosinophilic eosinophilic cells with prominent nucleoli and rich cytoplasm indicates Hurthle cell carcinoma. [1] MTC, as it originates from parafollicular C cells of the neural crest, is characterized by the production of a specific neoplastic marker, calcitonin, and several peptides, i.e. CEA, the level of which correlates with the mass of neoplastic cells (C cells) in well-differentiated MTC. [22] Multiple mitotic figures and atypical mitosis are common in anaplastic carcinoma.[1,2]
2.3. Diagnostics
It is estimated that 68% of thyroid nodules are detected during an ultrasound examination (USG), most often by accident. The initial assessment of a thyroid nodule for malignancy is performed by testing a thyroid function panel in the blood - changes associated with hyperthyroidism are usually at a lower risk of malignancy. In case of doubt, an additional radionuclide uptake test can be performed. Fine-needle biopsy is the test with the highest diagnostic accuracy in confirming malignant changes, at around 70-97%. [1,19,23]

Table 1.
Summary of features suggestive of a malignant process in thyroid ultrasound.
| Features indicating a malignant process in an ultrasound examination of the thyroid gland |
|---|
| Hypoechogenicity |
| Irregular margins |
| Shape taller than wide |
| Central vascularization |
| Extension of the lesion beyond the thyroid gland |
| Solid structure |
3. Treatment
The most commonly used methods, in various combinations, include surgical treatment, radioiodine ablation (RAI), thyroid hormone suppression, radiotherapy, and chemotherapy. [1,2,6] Alcohol, laser, and radiofrequency ablation (RFA) techniques are also an alternative, although they are not commonly used. [14,24] Factors influencing decisions regarding the actions taken include, among others, tumor size, tumor growth rate, tumor location, invasion of neighboring tissues, presence of metastases, involvement of lymph nodes, symptoms, patient preferences, comorbidities, and team experience. The TNM (tumor, nodules, metastates), ATA (American Thyroid Association), and AJCC (American Joint Committee on Cancer) scales are also helpful in stratifying treatment. [25] In the case of well-differentiated cancers, surgical treatment is considered first, in the form of hemithyroidectomy or thyroidectomy, with possible lymph node dissection. [1,26] Postoperative radioiodine ablation therapy (RAI) is used at least 4 weeks after the procedure to remove micrometastases from the remaining thyroid tissue or identified metastases, which in the case of DTC may affect up to 60% of patients. In most cases, it is also necessary to use thyroid hormone suppression therapy. [1,26] Its aim is to reduce the risk of cancer recurrence by suppressing TSH, which stimulates the growth of thyroid cells, including neoplastic cells, with supraphysiological doses of L-thyroxine. [26] In cases refractory to conventional treatment, radiotherapy or chemotherapy, including lenvatinib and sorafenib, multikinase inhibitors (MKI), may be considered. [1,2,7] Low-grade cancers, especially papillary microcancers, may also be candidates for RFA treatment.[24] The leading treatment method for MTC is total thyroidectomy with removal of regional and local metastases and prophylactic resection of central lymph nodes. [1] Chemotherapy also plays a role in the treatment of MTC. In cases with RET mutations, kinase inhibitors, vandetanib, cabozantinib, selpercatinib or pralsetinib are used. Due to the different origin of this type of cancer compared to other thyroid cancers, radioiodine ablation and thyroid hormone suppression are not used. [1,2] Radiotherapy, RFA, cryoablation or embolization are also used less frequently. [27] Resectable anaplastic cancers (up to stage IVa) are treated surgically with lymph node excision. In the remaining tumors (IVb and IVc) and as an adjunct to surgical treatment, cytotoxic chemotherapy with carboplatin and cisplatin and targeted radiotherapy are used. In patients with the BRAF V600E mutation, specific BRAF and MEK kinase inhibitors, such as dabrafenib and trametinib, can be additionally used as preparation for surgical treatment or radiotherapy. [1,13,16,17] The treatment of metastatic anaplastic thyroid cancer still poses therapeutic challenges. [13,16] Frequent complications of surgical treatment, especially in thyroidectomy combined with lymph node resection, include neurovascular damage, damage or paralysis of the recurrent laryngeal nerve, including hoarseness and respiratory failure, hypocalcaemia, hypoparathyroidism, visceral fistula, damage to the cervical motor nerve, hemorrhage, hematoma, postoperative fever, wound infection, thromboembolic complications, or Horner's syndrome. [1,3,6,14] Untreated, advanced thyroid cancer may invade the surrounding tissues, including the mediastinum, esophagus, trachea, larynx, carotid artery, and in about 10% of DTC cases, produce distant metastases, most often to the lungs, bones, brain, and liver. [1,3,17,18,19,20,21,22,23,24,25,26,27]
Table 2.
Podsumowanie metod leczenia w zależności od typu raka tarczycy.
| Type of treatment | Type of cancer |
|---|---|
| Active supervision | DTC |
| Lobectomy | DTC |
| Thyroidectomy with/without nodulectomy | DTC, MTC, ATC |
| Chemotherapy | DTC, MTC, ATC |
| Radioterpia | DTC, MTC, ATC |
| Radioiodine ablation | DTC |
| Thyroid hormone suppression therapy | DTC |
| Radiofrequency ablation (RFA) | PTC, small recurrence, symptomatic in non-resectable cancers, MTC |
None of the above-mentioned treatment methods are ideal. Each one differs in medical indications, side effect profile, availability, risk of complications. Moreover, despite maximizing their use and using different combinations, they are not always sufficient to achieve remission or at least stop the progression of the cancer, especially in the case of anaplastic thyroid cancer. [6]
3.1. Photodynamic Therapy (PDT)
Phototherapy, or the healing effects of light, has been known for hundreds of years. It has been used since ancient times to treat diseases such as skin cancer, vitiligo, psoriasis, swelling, paralysis, muscle weakness, rheumatism, scurvy, rickets, tuberculosis, and lupus vulgaris. [28,29] The term "photodynamic effect" was first used in 1907, when oxygen was recognized as an integral component of the process. Currently, it is used in many medical indications, the most important of which are oncological diseases of the urinary bladder, lungs, neck, head, esophagus, skin, as well as non-cancerous diseases including dermatological, ophthalmological, cardiovascular, neurological, gastroenterological, rheumatological, infectious, and dental.[28,29] The cytotoxic effect is caused by 3 components: light of a specific wavelength, photosensitizer (PS) and molecular oxygen.[28,30,31]
3.2. Translation
The main component involved in PDT is a photosensitizer (PS). Research is still underway to develop the ideal PS, which is characterized by, among others, low activity without exposure to light, light absorption in the range of 600 nm to 800 nm, good tissue penetration without energy losses, affinity and accumulation in the tumor, rapid elimination from the body, high quantum yield of singlet oxygen. PS is divided into three generations. The first generation includes derivatives of hematoporphyrin and sodium porphymer. Their main disadvantages are hydrophobicity, causing skin hypersensitivity, toxicity without a light source, low absorption in red light. The second generation PS, which differs in the range of activating light, lower skin phototoxicity, solubility in water, quantum yield of a single oxygen molecule and faster elimination from tissues, includes, among others, derivatives of phthalocyanines, bacteriochlorins and chlorides. Third-generation PSs are characterized by a lack of solubility, selectivity and effectiveness limited to cancer tissue, thanks to the use of antibodies and carriers made of polymers, dendrimers, quantum dots, micelles, liposomes, gold or carbon and magnetic nanoparticles. [28,29] The second element needed to perform photodynamic therapy is light. Depending on the indication and the site undergoing therapy, the type and parameters of the light used may vary. [28,29] Laser light sources include: argon/dye lasers, metal vapor and solid-state lasers. Non-laser light sources include lamp light sources, light-emitting diodes, daylight or X-rays. [31] The wavelength used ranges from 600 nm to 1200 nm, which is the optical window of the tissue, while the optimal range, called the therapeutic window, is 600 nm to 850 nm. Shorter wavelengths - below 600 nm - penetrate the tissue less, focusing on the more superficial layers of the skin, which contributes to its hypersensitivity to light. On the other hand, wavelengths longer than 850 nm do not provide the amount of energy required to produce the appropriate amount of reactive oxygen species, and consequently - to induce the desired therapeutic effect. [28] The last but equally important element is molecular oxygen. Hypoxia of the tissue undergoing therapy causes reduced production of ROS and a decrease in the effectiveness of the treatment, which is particularly noticeable in solid tumors located deeper. It is important to select such light intensity that the rate of oxygen consumption is equal to the rate of oxygen penetration into the tissue undergoing therapy, and also that it does not cause occlusion of the blood vessels of the tumor tissue, which would deepen the hypoxia. [6,28]
3.3. Mechanism of Photodynamic Therapy
Administered locally, intravenously, orally, or intraperitoneally, PS accumulates in the target tissue. Absorbing light, it triggers numerous chemical reactions that result in the generation of reactive oxygen species and the transition of PS from the ground state to an unstable electronically excited singlet state. The singlet state can also be transformed into the triplet state by spin conversion of an electron located in a higher energy orbit. Due to its greater stability, the triplet state can transfer energy to molecular oxygen and enable the creation of singlet oxygen and the ground state of PS, which constitutes a type II reaction, which is the main mechanism of action of photodynamic therapy. Highly reactive singlet oxygen, through its ability to affect the nucleus, lysosomes, mitochondria, endoplasmic reticulum, and cell membrane, leads to cell death. Type I reaction involves direct interaction of excited PS with surrounding tissues, i.e. cell membrane or electron-rich molecule. The radical ions and free radicals generated in this mechanism react with molecular oxygen. By producing reactive superoxide anion, hydrogen peroxide or hydroxyl radical, they cause oxidative damage leading to biological modifications. [28,29,30] The ratio of type I and II reactions, and consequently the entire process of cell death, consists of many components, including PS affinity for the substrate, concentration, location relative to the cell, PS dose and type, light dose, oxygen concentration and availability, time elapsed between PS administration and exposure to light, location and degree of tumor oxygenation. Both reactions can be carried out at the same time. [28,29] Type I reactions in the case of hypoxia proceed better than type II reactions, but are associated with greater damage. [28,29,30] PDT can affect cancer tissue by three mechanisms, the combination of which gives the most durable, long-term effect. Cancer cell necrosis is a mechanism of unprogrammed cell death, occurring under the influence of large amounts of light. It leads to vacuolation of the cytoplasm, destruction of the cell membrane, the release of cytoplasmic content and proinflammatory mediators outside the cell and, as a consequence, local inflammation. Apoptosis is a process of programmed cell death, which occurs under the influence of small amounts of light. Its essence is a reduction in cell dimensions, wrinkling of membranes and production of apoptotic bodies, while maintaining the continuity of the cell membrane. In contrast to necrosis, toxic substances do not escape from the cell. The second mechanism is the destruction of blood vessels supplying cancer tissue, through the accumulation of PS in the vessel walls. This indirect mechanism of cancer tissue death is primarily important in the long-term effects of photodynamic therapy. A relatively recently discovered effect of PDT on cancer tissue is the generation of an immune response through the earlier induction of inflammation. Induction of necrosis and the effect on blood vessels causes a sudden release of inflammatory mediators, which then affect the host's immune system. Macrophages phagocytizing destroyed cancer cells indirectly stimulate Tc lymphocytes, which provide immune defense against cancer cells for a long time. Local PDT probably has an immunosuppressive effect, while systemic PDT is immunostimulant. [28]
3.4. Advantages
The main advantages of PDT include low therapy costs compared to other methods in oncological treatment, short therapy time, no long-term side effects, low invasiveness, possibility of use in outpatient settings, high effectiveness in killing cancer cells, also affecting the vascularization of the tumor, possibility of repeated use, no interaction with other treatment methods, leaving small scars or no scars at all. [6,28,30] Cytotoxic specificity, which distinguishes PDT from other methods, e.g. ablation, is a combination of PS molecules predilection for the tumor, focusing the low-power laser only on the tumor and local action, while generating ROS, not dehydration or temperature change. [14]
3.5. Defects
The main disadvantage of PDT is related to ROS, which causes pain by affecting nociceptors. One of the probable mechanisms is the stimulation of N-methyl-D phosphorylation, which is involved in pain mechanisms. Additionally, ROS stimulates the release of proinflammatory cytokines, including tumor necrosis factor alpha or interleukin 1 and 6 by affecting the transient receptor potential of ankyrin 1, transient receptor potential of vanilloid type 1 and aspartate receptors. [30] Other disadvantages of PDT reported in the literature include possible skin hypersensitivity to light after the procedure, lack of application in the case of disseminated metastases due to the selectivity of action and in poorly oxygenated tumors, dependence on the precision of irradiation of pathological tissue. [28] Another problem may be the difficulty in preparing advanced targeting probes used during PDT, as well as control of their quality. The costs associated with the maintenance of the required, modern equipment, as well as its preparation and transport, must also be taken into account. [6]
PDT is also associated with the occurrence of adverse effects. The literature reports skin phototoxicity, liver damage, nausea, edema, and skin reactions. [10]
Table 3.
Summary of the most important advantages and disadvantages of PDT.
| Advantages of PDT | Disadvantages of PDT |
|---|---|
| Low invasiveness | It causes pain |
| Low costs compared to other oncological treatment methods | Dependence on the accuracy of pathological tissue irradiation |
| Possibility of outpatient use | High costs of preparation, transportation, and maintenance of equipment needed for PDT |
| Protection of surrounding tissues | Lack of specific standards and quality control |
| No long-term side effects | No use in case of disseminated cancers |
| Leaves minor scars or no scars at all. | Not applicable in the case of deeper, less oxygenated tumors |
| High effectiveness | |
| Also affecting the vascularization of the tumor - long-term effects | |
| Short therapy time | |
| Can be used multiple times and combined with other methods |
4. Application of Photodynamic Therapy in Thyroid Cancer
There are limited studies available on the use of PDT in the treatment of thyroid lesions. The main therapeutic problem is anaplastic carcinoma, which, as mentioned above, is characterized by high mortality and resistance to the proposed treatment. PDT, due to its concentration on pathological cells and the possibility of combining with other therapeutic methods, offers a chance to improve the prognosis of patients with this disease. [6] Moreover, it has been shown that the combination of PDT with chemotherapy inhibits tumor growth and induces cell apoptosis to a greater extent than chemotherapy alone, probably by increasing the internalization of anticancer drugs and combating resistance to chemotherapy. [6,10] The most commonly used PS in PDT for the treatment of thyroid cancers include hypericin, porphyrin, photophrin, radachlorin, and 5-aminolevulinic acid (ALA). [8,9,10,14,32]
Table 4.
Summary of the molecular and structural formulas of the most commonly used PSs in PDT for thyroid cancer.
Table 4.
Summary of the molecular and structural formulas of the most commonly used PSs in PDT for thyroid cancer.
| Name | Formula | Ref. | |
| Hipericin | C30H16O8 | 33 | 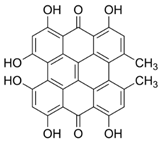 |
| Porphyrin | C44H34N8 | 34, 35, 36 |  |
| Photofrin | C68H74N8O11 | 37, 38 | 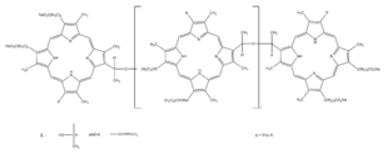 |
| Radachlorin | C38H41N5O9 | 39, 40 | 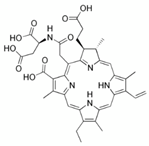 |
| 5-Aminolevulinic acid (ALA) | C5H9NO3 | 38, 41 |  |
Hypericin (HYP) is a potent PS isolated from St. John's wort. Previous studies have shown its efficacy in the treatment of anaplastic thyroid cancer, mainly by stimulating cancer cell apoptosis and mitochondrial damage. [6,9] In vitro studies conducted by Hyejin Kim and colleagues using HYP as PS showed that the absorption peak of HYP was 593 nm, and the degree of absorption was directly proportional to the HYP concentration, making it a suitable potential PS. The viability of anaplastic cancer cell lines under the influence of PDT using HYP decreased significantly, in an amount dependent on the HYP concentration, and this correlation was more pronounced up to a HYP concentration of 10 μg/ml. The study group, i.e. subjected to PDT using HYP, compared to the control groups, i.e. exposed to HYP only, laser only or no treatment at all, was characterized by a large number of induced cell death, significantly increased intracellular ROS and significantly decreased mitochondrial membrane potential. In the mouse study group, tumor weight and volume were almost completely reduced. The tumors in the control groups gradually increased. On day 4 of the study, necrosis was observed in the skin that was exposed to HYP-PDT, while the skin in the control group using only laser remained intact. Studies are ongoing on the combination of HYP with nanocarriers such as iron oxide, polyacrylamide, polyethylene glycol, polylactic acid, in order to increase their efficacy as PS in PDT. [9] In DTC, the PS used is mainly porphyrin-HDL nanoparticle (PLP). Its advantages include safety, low invasiveness, enabling complete ablation of pathological tissue while leaving normal thyroid tissue and the recurrent laryngeal nerve intact. [6] Studies conducted by Nidal Muhanna et al. on mouse and rabbit models have shown high efficacy in the treatment of PTC using PLP as a PS in PDT, assessing cellular toxicity, the function of the recurrent laryngeal nerve by endoscopic assessment of vocal cord mobility, and trachea and thyroid histology. After 24 h, in vitro PDT using light at a wavelength of 671 nm at 10 J/cm2 was associated with significant destruction of cancer cells, with preserved viability of cells from PLP not exposed to light. It was confirmed by fluorescence imaging that PLP administered to mice systemically at a dose of 4 mg/kg accumulated in pathological tissue to a high degree, compared to healthy tissue, which showed minimal fluorescence. PLP labeled with 64Cu after 24 hours of injection showed a significant predilection for tumor, compared to trachea, thyroid and muscles. Additionally, the TUNEL staining test revealed a significant level of apoptosis of tumor cells after PLP-PDT compared to the control group (75.7% vs. 10.6%). Studies conducted on rabbits confirmed a significantly higher accumulation of PLP in pathological tissue, compared to surrounding muscles or nervous tissue. The fluorescence signal after PLP administration also proved helpful for tumor resection together with the surrounding tissues. Also in this case, significant efficacy of PLP-PDT in inducing apoptosis of cancer cells was confirmed, compared to the preservation of normal structure of healthy cells, as confirmed by hematoxylin and eosin (H&E) staining and TUNEL test. Moreover, 24 hours after systemic administration of PLP, the rabbit recurrent laryngeal nerve was subjected to PDT and its structure was assessed histologically in relation to the non-PDT-treated recurrent laryngeal nerve. Both preparations showed minimal apoptosis and normal morphology, which indicates the safety of PDT in relation to the nervous tissue. Long-term effects of PLP-PDT also showed satisfactory results. In comparison to the control groups of rabbits with thyroid tumors left untreated and exposed only to laser, in which significant tumor progression occurred, the study group was characterized by the absence of tumor cells in the histological examination of the thyroid after the 53rd day of the study, as well as a normal image of the neck region in the computed tomography scan. The absence of soft tissue pathology was also confirmed by comparing the functional state of the recurrent laryngeal nerve with the state before the study, 24 hours after and 7 days after the treatment. [14]
Looking at the promising results of studies confirming the high efficacy of 5-aminolevulinic acid in the treatment of actinic keratosis of the skin, Al-Watban et al. examined the effect of PDT using 5-ALA as PS and a 633 nm diode laser in the treatment of undifferentiated thyroid cancer. Compared to the control group, the study group was characterized by a significant reduction in tumor size already on the 7th day after treatment, and the percentages of tumor growth delay were approximately 48% after 7 days, approximately 55% after 14 days, and approximately 51% after 21 days, respectively. In 20% of the mice examined, tumor necrosis occurred. [42] The influence of PDT therapy with photophrin on anaplastic thyroid cancer cells was studied by, among others, Seung Hoon Woo and his colleagues. They proved that the degree of cytotoxicity correlated with the concentration of the photosensitizer, in this case photophrin. Cellular cytotoxicity was most pronounced in the group of cells exposed to photophrin-PDT at a photophrin concentration of 3.2 μg/ml, compared to photophrin-PDT at a photophrin concentration of 1.6 μg/ml and using only photophrin without a laser. In addition, after 24 hours, this group also showed the most marked indicators of cell death, including necrosis, apoptosis, and increased expression of caspase 3, caspase 9, and PARP. Caspase 8 expression was similar to the control group. By examining the fluorescence signal, they found that photophrin accumulated mainly in the mitochondria of anaplastic cancer cells, indicating that cell death was most likely mediated by mitochondria. [43]
The use of sulforaphene (SFE) - 4-methylsufinyl-3-butenyl isothiocyanate is also being studied in PDT. Its main advantages are its low production cost, purity and natural origin. It works by arresting the cell cycle of cancer cells in the G0/G1 phase. Saswata Chatterjee and colleagues have shown that treatment of anaplastic cancer cell lines with SFE, before photophrin PS, and then exposing them to an LED diode is associated with a reduction in cell viability, greater than when using photophrin alone. Cells subjected to combined therapy, especially with a higher dose of photophrin (6.25 μg/ml vs. 1.5 μg/ml) were characterized by a significantly higher number of apoptotic bodies and the intensity of cell death, increased ROS production in cancer cells due to impaired mitochondrial potential, reduced expression of RAS, MEK (1/2) and ERK (1/2) proteins in cells with RAS mutations and inhibited activation of phosphorylated p38. [16] PDT may also have an impact on the inhibition of cancer tissue development by reducing the expression of EGFR and PI3K pathways. It is assumed that the therapeutic effect of carboplatin is enhanced by treatment methods acting as PI3K inhibitors, therefore the effect of combining carboplatin with PDT on the effect of anaplastic thyroid cancer treatment was examined. [8] In one of the first studies by Biswas et al. on this subject, it was shown that the percentage of cell viability of anaplastic cancer lines was inversely proportional to the increase in the concentration of radachlorin as PS in PDT, the increase in the concentration of carboplatin and the incubation time after laser irradiation. A synergistic effect in combined treatment could be observed at a concentration of radachlorin of at least 0.8 μg/ml and it was then gradually increased. Treating cells only with radachlorin did not result in significant changes in the percentage of cell viability. The use of combined therapy was associated with a much better effect than that obtained after the use of individual therapies. A significant decrease in cell viability, an increased percentage of cells showing signs of early and late apoptosis, a significant increase in the percentage of sub-G1 cells, a significant decrease in the percentage of cells in G0/G1, a significant increase in the depolarization of the mitochondrial membrane potential, a significantly increased expression of Bax, cytochrome c, caspase 3, caspase 9, caspase 12, poly ADP-ribose polymerase (PARP) and apoptosis-inducing factor (AIF) proteins, and a significant decrease in Bcl-2 expression were observed, and the values correlated with the concentration of radachlorin and carboplatin. The changes were much more marked in the case of combined treatment. [10] Further, extended studies conducted by the same group of researchers on anaplastic cancer cell lines similarly showed that the number of live cells decreased in direct proportion to the concentration of carboplatin. In the combination of PDT with radachlorin as PS and carboplatin, the percentage of live cells decreased very significantly, to about 30%, compared to the control groups using only carboplatin (about 89%) or only PDT with radachlorin (about 80%). The combination of carboplatin and PDT with radachlorin completely inhibited the cancer cell line at concentrations of 0.05 mg/ml carboplatin and 3.12 ng/ml radachlorin. The combined therapy was characterized by apoptotic cells with irregular outlines, disruption of nuclear membranes, chromatin condensation in histopathological examination. Cell motility also decreased most in the case of combination therapy, and in the case of single therapies, this decrease was greater in the case of PDT than carboplatin. As for EGFR expression, it was unchanged in the case of carboplatin therapy and slightly decreased in the case of PDT and combination therapy. It was shown that in the case of PDT, the number of cells with increased ROS was 81.6%, compared to the combination therapy, where it was 87.1%. Mitochondrial membrane potential was moderately decreased after the treatment of cell lines with carboplatin (14.5%), a noticeable decrease in PDT (49.3%), and in the combination therapy this decrease was significant (80.6%). Cytochrome c expression, which is a marker of mitochondrial membrane depolarization and cell apoptosis associated with mitochondrial dysfunction, increased with PDT and then increased slightly in combination therapy. A relationship between PDT and combination therapy and the expression of proteins involved in the mitochondrial pathway, caspase-3 and caspase-9, was also demonstrated. Their activity increased in both cases, with a greater increase in combination therapy. Combination therapy has a significant effect on the decrease in PI3K expression, with no significant decrease in single therapies. In the case of PTEN expression, PDT showed no change, carboplatin a slight one, and combination therapy a significant one. Combination therapy was the only one to have a significant effect on the change in PI3K and PTEN expression. The size of the tumor was also compared depending on the therapy used after 3, 7, and 14 days. After 7 days, tumor volume was comparable in each of the 3 treatment groups, but inhibited compared to the control group. After 14 days, the decrease in tumor volume was most pronounced in the group of tumors treated with combination therapy, less pronounced with PDT, and least in the group using carboplatin, but the decrease was still significant compared to the control group. Additionally, in the case of tumors treated with combination therapy, significantly increased expression of caspase-3, caspase-9, and PTEN proteins, decreased expression of EGFR and PI3K, and proteolytic cleavage to the active form of poly(ADP-rubose) polymerase (PARP) were observed compared to tumors treated with single therapies. The above reports confirm that the therapeutic effect of combined carboplatin and PDT with radachlorin is due to the effect on the mitochondrial pathway and the EGFR-PI3K pathway. In addition, PDT can increase the internalization of chemotherapy drugs, which may be helpful in chemotherapy resistance, which results from reduced endocytosis of the tumor cell. [8] Jin-Chul Ahn and his colleagues conducted a study on anaplastic cancer cell lines using photophrin as PS in combination with genistein, a chemotherapeutic drug. It was shown that treatment of cells with genistein, regardless of the time interval (3, 6 and 24 h) and concentration (25, 50, 100 mM) did not result in changes in cell viability. Treatment of the cell line with PDT using photophrin at concentrations of 0.8 and 1.6 mg/ml reduced cell viability, to a greater extent at higher photophrin concentrations. However, cell viability was significantly inhibited in the combination therapy. Additionally, in the case of combined therapy compared to individual therapies, after 6 h the following changes were observed: a greater number of apoptotic cells, covering almost all cells, a greater degree of mitochondrial membrane depolarization, increased fluorescence intensity, increased expression of caspase 3, 8, 9, 12, PARP, CHOP, Bax, cytochrome c, AIF and a higher level of ROS, and the above changes were more pronounced when using higher concentrations of photophrin. [32]
Table 5.
Summary of information on sulforaphene, carboplatin and genistein - substances used to enhance PDT.
Table 5.
Summary of information on sulforaphene, carboplatin and genistein - substances used to enhance PDT.
| Name | Formula | ,Name | Structure | Ref |
|---|---|---|---|---|
| Sulforaphane | C6H9NOS2 | 4-methylsulfinyl-3-butenyl isothiocyanate |  |
16, 44, 45 |
| Carboplatin | C6H12N2O2Pt | (SP-4-2)-diamino[cyclobutane-1,1-dicarboxylate(2-)-O,O']-platinum |  |
46 |
| Genisteina | C15H10O5 | 5,7-dihydroxy-3-(4-hydroxyphenyl)chromen-4-one |  |
47 |
5. Future Directions
Currently conducted research aimed at increasing the efficiency and effectiveness of PDT focuses on improving the stimulation, biocompatibility, localization, inactivation, singlet oxygen capture and reducing toxicity to the surrounding tissues. [29,35,48] The solution may be the use of nanotechnology achievements, such as combining PS with antibodies, magnetic nanoparticles or molecules with another, specific structure. [35,49,50] So far, the effectiveness has been demonstrated by using the folic acid receptor or the epidermal growth factor receptor for this purpose. [49] Current research also focuses on modifying PS so that it absorbs in the NIR spectrum, and thus - improves tissue penetration. [35] Self-luminescent systems are beginning to be used, including chemiluminescence or bioluminescence. [36] The solution may also be the use of X-ray induced photodynamic therapy. [51] Another challenge is the measurement of oxygen in pathological tissue before and during PDT, and increasing the oxygenation of the tissue undergoing therapy. Research is ongoing to increase oxygen production at the site of the lesion and to deliver oxygen to the site of the lesion using a carrier. [6,28] Another problem is the generation of anti-tumor immunity, which can be solved by using anti-tumor preparations, such as cancer cells subjected to PDT or vaccines in the form of cancer cell lysates. [49] Research is also ongoing to improve the effect of PDT on gene expression and immune reactions. [48,51]
Summary
Thyroid cancer is one of the most common endocrine cancers worldwide. It is divided into differentiated thyroid cancers, including papillary, follicular and Hurthe cell; medullary and anaplastic cancer. In addition to histological differences, they also show differences in terms of occurrence, prognosis, genetic background, diagnostics and therapeutic options. Currently, the most commonly used treatment methods - surgical treatment, chemotherapy, radiotherapy, radioactive iodine ablation, thyroid hormone suppression - are effective in lower advanced cancers, while in the case of lower differentiated, disseminated, recurrent cancers, they are not sufficient. Photodynamic therapy brings hope, which due to its minimally invasiveness, the possibility of outpatient use and combination with other techniques, the possibility of repeated use, leaving a small scar or no scar at all, is superior to classical methods. Studies on the effect of PDT with hypericin, porphyrin, photophrin, radachlorin or 5-aminolevulinic acid as PS on thyroid cancer have shown promising effects, including a decrease in cell viability, a high percentage of apoptotic cells, an increased percentage of cells showing features of early and late apoptosis, a significant increase in the percentage of sub-G1 cells, a significant decrease in the percentage of cells in G0/G1, a high degree of mitochondrial membrane depolarization, an increase in fluorescence intensity, increased expression of caspase 3, 9, 12, PARP, CHOP, Bax, cytochrome c, AIF, a significant decrease in Bcl-2 expression, a decrease in tumor mass, a decreased expression of EGFR and PI3K, proteolytic cleavage to the active form of poly(ADP-rubose) polymerase and a high level of ROS. The changes were particularly marked in higher concentrations of the photosensitizer or in combination with sulforaphene, carboplatin, or genistein.
Photodynamic therapy is undoubtedly a method of the future, but requires further studies to validate and standardize its use.
List of Abbreviations
| 5-ALA | 5-aminolevulinic acid |
| AIF | apoptosis-inducing factor |
| AJCC | American Joint Committee on Cancer |
| ATA | American Thyroid Association |
| ATC | anaplastic thyroid cancer |
| BACC | fine-needle aspiration biopsy |
| DTC | differentiated thyroid cancer |
| EGFR | epidermal growth factor receptor |
| FTC | follicular thyroid cancer |
| H&E | hematoxylin and eosin |
| HCC | Hurthle cell carcinoma |
| HYP | hypericin |
| MAP, MAPK | mitogen-activated protein kinase |
| MEN | multiple endocrine neoplasia |
| MKI | multikinase inhibitors |
| MTC | medullary thyroid cancer |
| NIS | sodium-iodine symporter |
| PARP | poly(ADP-ribose) polymerase |
| PDT | photodynamic therapy |
| PI3K | 3-kinase phosphoinositide |
| PLP | porphyrin-HDL |
| PLP-PDT | PDT using PLP as PS |
| PS | photosensitizer |
| PTC | papillary thyroid cancer |
| PTEN | phosphatase and tensin homologue |
| RAI | radioactive iodine therapy |
| RFI | radiofrequency ablation |
| ROS | reactive oxygen species |
| SFE | sulforaphene |
| TNM | tumor, nodules, metastates |
| TSH | thyroid-stimulating hormone |
| USG | ultrasound examination |
References
- Lee K, Anastasopoulou C, Chandran C, Cassaro S. Thyroid Cancer. 2023 May 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 29083690.
- Shonka DC Jr, Ho A, Chintakuntlawar AV, Geiger JL, Park JC, Seetharamu N, Jasim S, Abdelhamid Ahmed AH, Bible KC, Brose MS, Cabanillas ME, Dabekaussen K, Davies L, Dias-Santagata D, Fagin JA, Faquin WC, Ghossein RA, Gopal RK, Miyauchi A, Nikiforov YE, Ringel MD, Robinson B, Ryder MM, Sherman EJ, Sadow PM, Shin JJ, Stack BC Jr, Tuttle RM, Wirth LJ, Zafereo ME Jr, Randolph GW. American Head and Neck Society Endocrine Surgery Section and International Thyroid Oncology Group consensus statement on mutational testing in thyroid cancer: Defining advanced thyroid cancer and its targeted treatment. Head Neck. 2022 Jun;44(6):1277-1300. Epub 2022 Mar 11. PMID: 35274388; PMCID: PMC9332138. [CrossRef]
- Avram AM, Zukotynski K, Nadel HR, Giovanella L. Management of Differentiated Thyroid Cancer: The Standard of Care. J Nucl Med. 2022 Feb;63(2):189-195. Epub 2021 Aug 19. PMID: 34413146. [CrossRef]
- Liu J, Liu Y, Lin Y, Liang J. Radioactive Iodine-Refractory Differentiated Thyroid Cancer and Redifferentiation Therapy. Endocrinol Metab (Seoul). 2019 Sep;34(3):215-225. PMID: 31565873; PMCID: PMC6769341. [CrossRef]
- Lechner MG, Praw SS, Angell TE. Treatment of Differentiated Thyroid Carcinomas. Surg Pathol Clin. 2019 Dec;12(4):931-942. Epub 2019 Sep 27. PMID: 31672299. [CrossRef]
- C. Shao C, Li Z, Zhang C, Zhang W, He R, Xu J, Cai Y. Optical diagnostic imaging and therapy for thyroid cancer. Mater Today Bio. 2022 Sep 26;17:100441. PMID: 36388462; PMCID: PMC9640994. [CrossRef]
- Agosto Salgado S, Kaye ER, Sargi Z, Chung CH, Papaleontiou M. Management of Advanced Thyroid Cancer: Overview, Advances, and Opportunities. Am Soc Clin Oncol Educ Book. 2023 May;43:e389708. PMID: 37186883. [CrossRef]
- Biswas R, Mondal A, Ahn JC. Deregulation of EGFR/PI3K and activation of PTEN by photodynamic therapy combined with carboplatin in human anaplastic thyroid cancer cells and xenograft tumors in nude mice. J Photochem Photobiol B. 2015 Jul;148:118-127. Epub 2015 Apr 2. PMID: 25910816. [CrossRef]
- Kim H, Kim SW, Seok KH, Hwang CW, Ahn JC, Jin JO, Kang HW. Hypericin-assisted photodynamic therapy against anaplastic thyroid cancer. Photodiagnosis Photodyn Ther. 2018 Dec;24:15-21. Epub 2018 Aug 15. PMID: 30118906. [CrossRef]
- Biswas R, Chung PS, Moon JH, Lee SH, Ahn JC. Carboplatin synergistically triggers the efficacy of photodynamic therapy via caspase 3-, 8-, and 12-dependent pathways in human anaplastic thyroid cancer cells. Lasers Med Sci. 2014 May;29(3):995-1007. Epub 2013 Oct 10. PMID: 24114422. [CrossRef]
- Miranda-Filho A, Lortet-Tieulent J, Bray F, Cao B, Franceschi S, Vaccarella S, Dal Maso L. Thyroid cancer incidence trends by histology in 25 countries: a population-based study. Lancet Diabetes Endocrinol. 2021 Apr;9(4):225-234. Epub 2021 Mar 1. PMID: 33662333. [CrossRef]
- Genutis LK, Tomsic J, Bundschuh RA, Brock PL, Williams MD, Roychowdhury S, Reeser JW, Frankel WL, Alsomali M, Routbort MJ, Broaddus RR, Wakely PE Jr, Phay JE, Walker CJ, de la Chapelle A. Microsatellite Instability Occurs in a Subset of Follicular Thyroid Cancers. Thyroid. 2019 Apr;29(4):523-529. Epub 2019 Mar 27. PMID: 30747051; PMCID: PMC6457885. [CrossRef]
- Tiedje V, Fagin JA. Therapeutic breakthroughs for metastatic thyroid cancer. Nat Rev Endocrinol. 2020 Feb;16(2):77-78. PMID: 31819229; PMCID: PMC7470005. [CrossRef]
- Muhanna N, Chan HHL, Townson JL, Jin CS, Ding L, Valic MS, Douglas CM, MacLaughlin CM, Chen J, Zheng G, Irish JC. Photodynamic therapy enables tumor-specific ablation in preclinical models of thyroid cancer. Endocr Relat Cancer. 2020 Feb;27(2):41-53. PMID: 31751308. [CrossRef]
- Ciampi R, Romei C, Ramone T, Prete A, Tacito A, Cappagli V, Bottici V, Viola D, Torregrossa L, Ugolini C, Basolo F, Elisei R. Genetic Landscape of Somatic Mutations in a Large Cohort of Sporadic Medullary Thyroid Carcinomas Studied by Next-Generation Targeted Sequencing. iScience. 2019 Oct 25;20:324-336. Epub 2019 Sep 26. PMID: 31605946; PMCID: PMC6817656. [CrossRef]
- Chatterjee S, Rhee Y, Chung PS, Ge RF, Ahn JC. Sulforaphene Enhances The Efficacy of Photodynamic Therapy In Anaplastic Thyroid Cancer Through Ras/RAF/MEK/ERK Pathway Suppression. J Photochem Photobiol B. 2018 Feb;179:46-53. Epub 2017 Dec 11. PMID: 29331658. [CrossRef]
- Wang JR, Zafereo ME, Dadu R, Ferrarotto R, Busaidy NL, Lu C, Ahmed S, Gule-Monroe MK, Williams MD, Sturgis EM, Goepfert RP, Gross ND, Lai SY, Gunn GB, Phan J, Rosenthal DI, Fuller CD, Morrison WH, Iyer P, Cabanillas ME. Complete Surgical Resection Following Neoadjuvant Dabrafenib Plus Trametinib in BRAFV600E-Mutated Anaplastic Thyroid Carcinoma. Thyroid. 2019 Aug;29(8):1036-1043. PMID: 31319771; PMCID: PMC6707029. [CrossRef]
- Maniakas A, Zafereo M, Cabanillas ME. Anaplastic Thyroid Cancer: New Horizons and Challenges. Endocrinol Metab Clin North Am. 2022 Jun;51(2):391-401. Epub 2022 May 4. PMID: 35662448. [CrossRef]
- Kant R, Davis A, Verma V. Thyroid Nodules: Advances in Evaluation and Management. Am Fam Physician. 2020 Sep 1;102(5):298-304. PMID: 32866364.
- LeClair K, Bell KJL, Furuya-Kanamori L, Doi SA, Francis DO, Davies L. Evaluation of Gender Inequity in Thyroid Cancer Diagnosis: Differences by Sex in US Thyroid Cancer Incidence Compared With a Meta-analysis of Subclinical Thyroid Cancer Rates at Autopsy. JAMA Intern Med. 2021 Oct 1;181(10):1351-1358. PMID: 34459841; PMCID: PMC8406211. [CrossRef]
- Palot Manzil FF, Kaur H. Radioactive Iodine for Thyroid Malignancies. 2023 Nov 21. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 35593874.
- Araque KA, Gubbi S, Klubo-Gwiezdzinska J. Updates on the Management of Thyroid Cancer. Horm Metab Res. 2020 Aug;52(8):562-577. Epub 2020 Feb 10. PMID: 32040962; PMCID: PMC7415555. [CrossRef]
- Alexander LF, Patel NJ, Caserta MP, Robbin ML. Thyroid Ultrasound: Diffuse and Nodular Disease. Radiol Clin North Am. 2020 Nov;58(6):1041-1057. Epub 2020 Sep 17. PMID: 33040847. [CrossRef]
- Pace-Asciak P, Russell JO, Tufano RP. The Treatment of Thyroid Cancer With Radiofrequency Ablation. Tech Vasc Interv Radiol. 2022 Jun;25(2):100825. Epub 2022 Mar 10. PMID: 35551804. [CrossRef]
- Tuttle RM, Alzahrani AS. Risk Stratification in Differentiated Thyroid Cancer: From Detection to Final Follow-Up. J Clin Endocrinol Metab. 2019 Sep 1;104(9):4087-4100. PMID: 30874735; PMCID: PMC6684308. [CrossRef]
- Yoon BH, Lee Y, Oh HJ, Kim SH, Lee YK. Influence of Thyroid-stimulating Hormone Suppression Therapy on Bone Mineral Density in Patients with Differentiated Thyroid Cancer: A Meta-analysis. J Bone Metab. 2019 Feb;26(1):51-60. Epub 2019 Feb 28. PMID: 30899725; PMCID: PMC6416150. [CrossRef]
- Kim M, Kim BH. Current Guidelines for Management of Medullary Thyroid Carcinoma. Endocrinol Metab (Seoul). 2021 Jun;36(3):514-524. Epub 2021 Jun 22. PMID: 34154310; PMCID: PMC8258323. [CrossRef]
- Correia JH, Rodrigues JA, Pimenta S, Dong T, Yang Z. Photodynamic Therapy Review: Principles, Photosensitizers, Applications, and Future Directions. Pharmaceutics. 2021 Aug 25;13(9):1332. PMID: 34575408; PMCID: PMC8470722. [CrossRef]
- Maharjan PS, Bhattarai HK. Singlet Oxygen, Photodynamic Therapy, and Mechanisms of Cancer Cell Death. J Oncol. 2022 Jun 25;2022:7211485. PMID: 35794980; PMCID: PMC9252714. [CrossRef]
- Lee CN, Hsu R, Chen H, Wong TW. Daylight Photodynamic Therapy: An Update. Molecules. 2020 Nov 8;25(21):5195. PMID: 33171665; PMCID: PMC7664668. [CrossRef]
- Yang M, Yang T, Mao C. Enhancement of Photodynamic Cancer Therapy by Physical and Chemical Factors. Angew Chem Int Ed Engl. 2019 Oct 1;58(40):14066-14080. Epub 2019 Jul 10. PMID: 30663185; PMCID: PMC6800243. [CrossRef]
- Ahn JC, Biswas R, Chung PS. Combination with genistein enhances the efficacy of photodynamic therapy against human anaplastic thyroid cancer cells. Lasers Surg Med. 2012 Dec;44(10):840-9. Epub 2012 Nov 9. PMID: 23143780. [CrossRef]
- Wang H, Yang X, Lai H, Sun Y, Yan X, Ai Q, Lin M, Yang S, Yang Y, Chu S, Wang Z, Chen N. Novel antidepressant mechanism of hypericin: Role of connexin 43-based gap junctions. Biomed Pharmacother. 2023 Nov;167:115545. Epub 2023 Sep 20. PMID: 37734259. [CrossRef]
- Abrahamse H, Hamblin MR. New photosensitizers for photodynamic therapy. Biochem J. 2016 Feb 15;473(4):347-64. PMID: 26862179; PMCID: PMC4811612. [CrossRef]
- Benov L. Photodynamic therapy: current status and future directions. Med Princ Pract. 2015;24 Suppl 1(Suppl 1):14-28. Epub 2014 May 10. PMID: 24820409; PMCID: PMC6489067. [CrossRef]
- Zhu F, Wang BR, Zhu ZF, Wang SQ, Chai CX, Shang D, Li M. Photodynamic therapy: A next alternative treatment strategy for hepatocellular carcinoma? World J Gastrointest Surg. 2021 Dec 27;13(12):1523-1535. PMID: 35070061; PMCID: PMC8727193. [CrossRef]
- Kano A, Taniwaki Y, Nakamura I, Shimada N, Moriyama K, Maruyama A. Tumor delivery of Photofrin® by PLL-g-PEG for photodynamic therapy. J Control Release. 2013 May 10;167(3):315-21. Epub 2013 Feb 26. PMID: 23454112. [CrossRef]
- Silva ZS Jr, Bussadori SK, Fernandes KP, Huang YY, Hamblin MR. Animal models for photodynamic therapy (PDT). Biosci Rep. 2015 Sep 28;35(6):e00265. PMID: 26415497; PMCID: PMC4643327. [CrossRef]
- Bae SM, Kim YW, Lee JM, Namkoong SE, Han SJ, Kim JK, Lee CH, Chun HJ, Jin HS, Ahn WS. Photodynamic effects of Radachlorin on cervical cancer cells. Cancer Res Treat. 2004 Dec;36(6):389-94. Epub 2004 Dec 31. PMID: 20368834; PMCID: PMC2843882. [CrossRef]
- Kochneva EV, Filonenko EV, Vakulovskaya EG, Scherbakova EG, Seliverstov OV, Markichev NA, Reshetnickov AV. Photosensitizer Radachlorin®: Skin cancer PDT phase II clinical trials. Photodiagnosis Photodyn Ther. 2010 Dec;7(4):258-67. Epub 2010 Aug 14. PMID: 21112549. [CrossRef]
- Sharmin MM, Islam MA, Yamamoto I, Taniguchi S, Yonekura S. 5-ALA Attenuates the Palmitic Acid-Induced ER Stress and Apoptosis in Bovine Mammary Epithelial Cells. Molecules. 2021 Feb 23;26(4):1183. PMID: 33672109; PMCID: PMC7926617. [CrossRef]
- Al-Watban FA, Zhang XY. Photodynamic therapy of human undifferentiated thyroid carcinoma-bearing nude mice using topical 5-aminolevulinic acid. Photomed Laser Surg. 2005 Apr;23(2):206-11. PMID: 15910188. [CrossRef]
- WOO, Seung Hoon, et al. Photodynamic therapy for SNU-80 anaplastic thyroid cancer cells. Medical Lasers; Engineering, Basic Research, and Clinical Application, 2022, 11.2: 84-91.
- Sangthong S, Weerapreeyakul N. Simultaneous quantification of sulforaphene and sulforaphane by reverse phase HPLC and their content in Raphanus sativus L. var. caudatus Alef extracts. Food Chem. 2016 Jun 15;201:139-44. Epub 2016 Jan 20. PMID: 26868558. [CrossRef]
- Kuang P, Song D, Yuan Q, Lv X, Zhao D, Liang H. Preparative separation and purification of sulforaphene from radish seeds by high-speed countercurrent chromatography. Food Chem. 2013 Jan 15;136(2):309-15. Epub 2012 Aug 30. PMID: 23122063. [CrossRef]
- Tanley SW, Diederichs K, Kroon-Batenburg LM, Levy C, Schreurs AM, Helliwell JR. Carboplatin binding to histidine. Acta Crystallogr F Struct Biol Commun. 2014 Sep;70(Pt 9):1135-42. Epub 2014 Aug 29. Erratum in: Acta Crystallogr F Struct Biol Commun. 2016 Mar 1;72(Pt 3):251-2. PMID: 25195881; PMCID: PMC4157408. [CrossRef]
- Sharifi-Rad J, Quispe C, Imran M, Rauf A, Nadeem M, Gondal TA, Ahmad B, Atif M, Mubarak MS, Sytar O, Zhilina OM, Garsiya ER, Smeriglio A, Trombetta D, Pons DG, Martorell M, Cardoso SM, Razis AFA, Sunusi U, Kamal RM, Rotariu LS, Butnariu M, Docea AO, Calina D. Genistein: An Integrative Overview of Its Mode of Action, Pharmacological Properties, and Health Benefits. Oxid Med Cell Longev. 2021 Jul 19;2021:3268136. PMID: 34336089; PMCID: PMC8315847. [CrossRef]
- Li G, Wang Q, Liu J, Wu M, Ji H, Qin Y, Zhou X, Wu L. Innovative strategies for enhanced tumor photodynamic therapy. J Mater Chem B. 2021 Sep 22;9(36):7347-7370. PMID: 34382629. [CrossRef]
- van Straten D, Mashayekhi V, de Bruijn HS, Oliveira S, Robinson DJ. Oncologic Photodynamic Therapy: Basic Principles, Current Clinical Status and Future Directions. Cancers (Basel). 2017 Feb 18;9(2):19. PMID: 28218708; PMCID: PMC5332942. [CrossRef]
- Zhou Z, Zhang L, Zhang Z, Liu Z. Advances in photosensitizer-related design for photodynamic therapy. Asian J Pharm Sci. 2021 Nov;16(6):668-686. Epub 2021 May 2. PMID: 35027948; PMCID: PMC8737425. [CrossRef]
- Alvarez N, Sevilla A. Current Advances in Photodynamic Therapy (PDT) and the Future Potential of PDT-Combinatorial Cancer Therapies. Int J Mol Sci. 2024 Jan 13;25(2):1023. PMID: 38256096; PMCID: PMC10815790. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



