Submitted:
06 January 2025
Posted:
08 January 2025
You are already at the latest version
Abstract
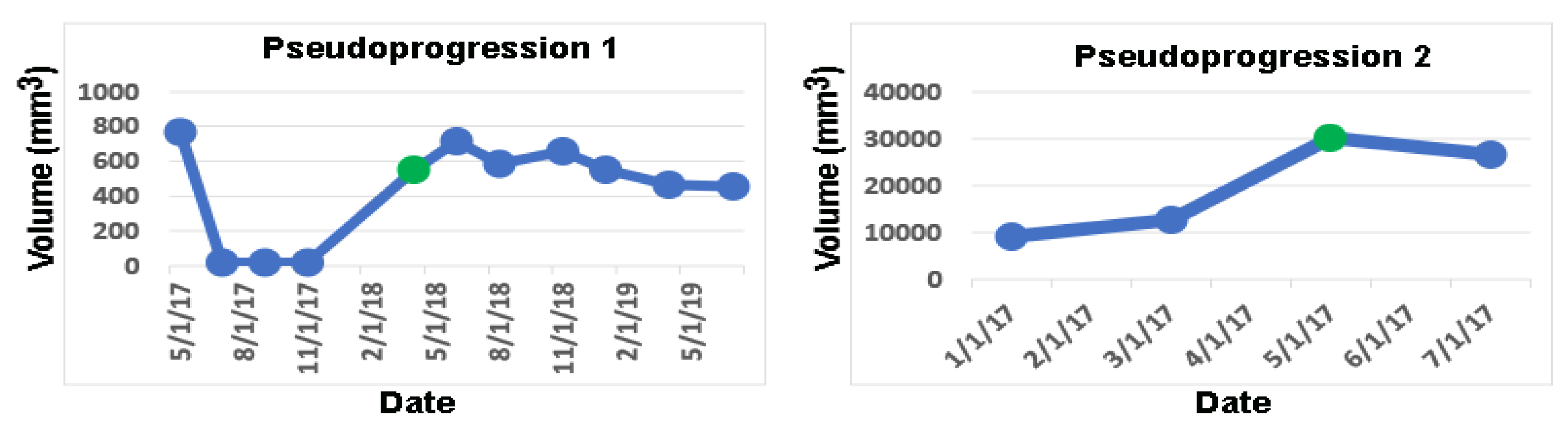
Glioblastomas (GBM) grow rapidly and infiltrate the cerebral parenchyma, leading to significant neurological morbidity and mortality. Early detection of tumor growth promotes early therapeutic interventions that delay neurological progression and possibly prolong survival times. This retrospective observational study evaluates the ability of AI-assisted volumetric analysis to correctly detect tumor progression in longitudinal studies of newly diagnosed GBM, compared to the standard clinical method of visual inspection by radiologists and neuro-oncologists. Fifteen of 56 patients met the inclusion and exclusion criteria. The dates of tumor progression were gathered from clinical reports. Longitudinal tumor volumes were calculated from automated segmentations by the MRIMath T1c AI followed by physician review using the MRIMath Smart manual contouring system. Growth by significant shifts in tumor volumes was detected by using the statistical method of the online change-of-point method. Our results demonstrate that automatic AI segmentation followed by human review detects tumor progression earlier than clinical notes in 4/15 patients at a median of 105 days. Furthermore, the longitudinal AI-measured volumes validated two cases of pseudoprogression as evidenced by subsequent volume stability. This study emphasizes the enhanced diagnostic accuracy achieved by incorporating volumetric data analysis into clinical decision-making. This can be accomplished by integrating efficient AI-powered segmentation and a streamlined human review system into the clinical workflow.
Keywords:
1. Introduction
2. Materials and Methods
Ethical Approval
Study Design and Patient Selection
Time to Growth Detected by Standard Clinical Care
Tumor Segmentation, Volume Calculation, and Physician Review
Online Change-of-Point Detection
Statistical Methods
3. Results
Patient Characteristics
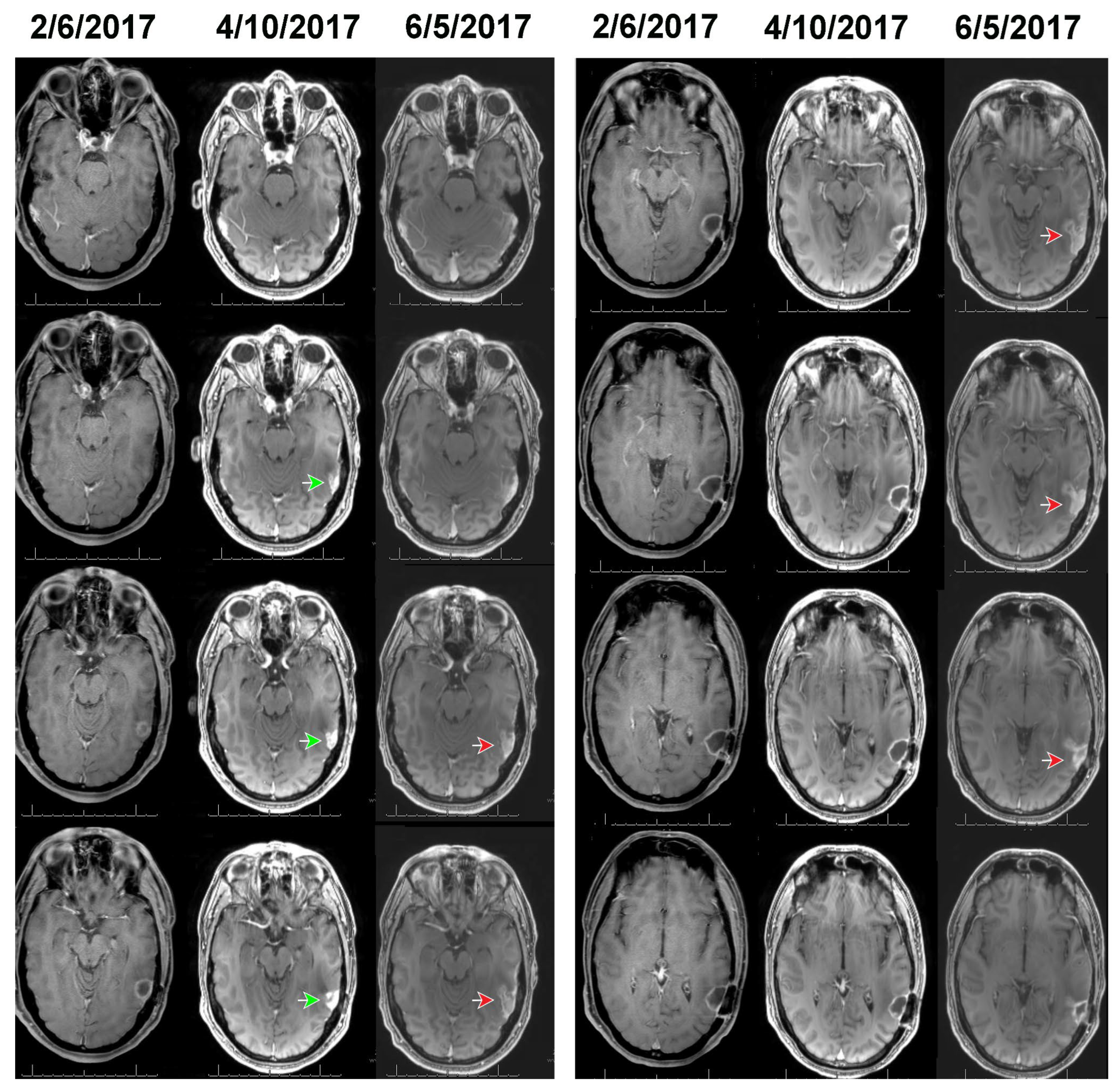
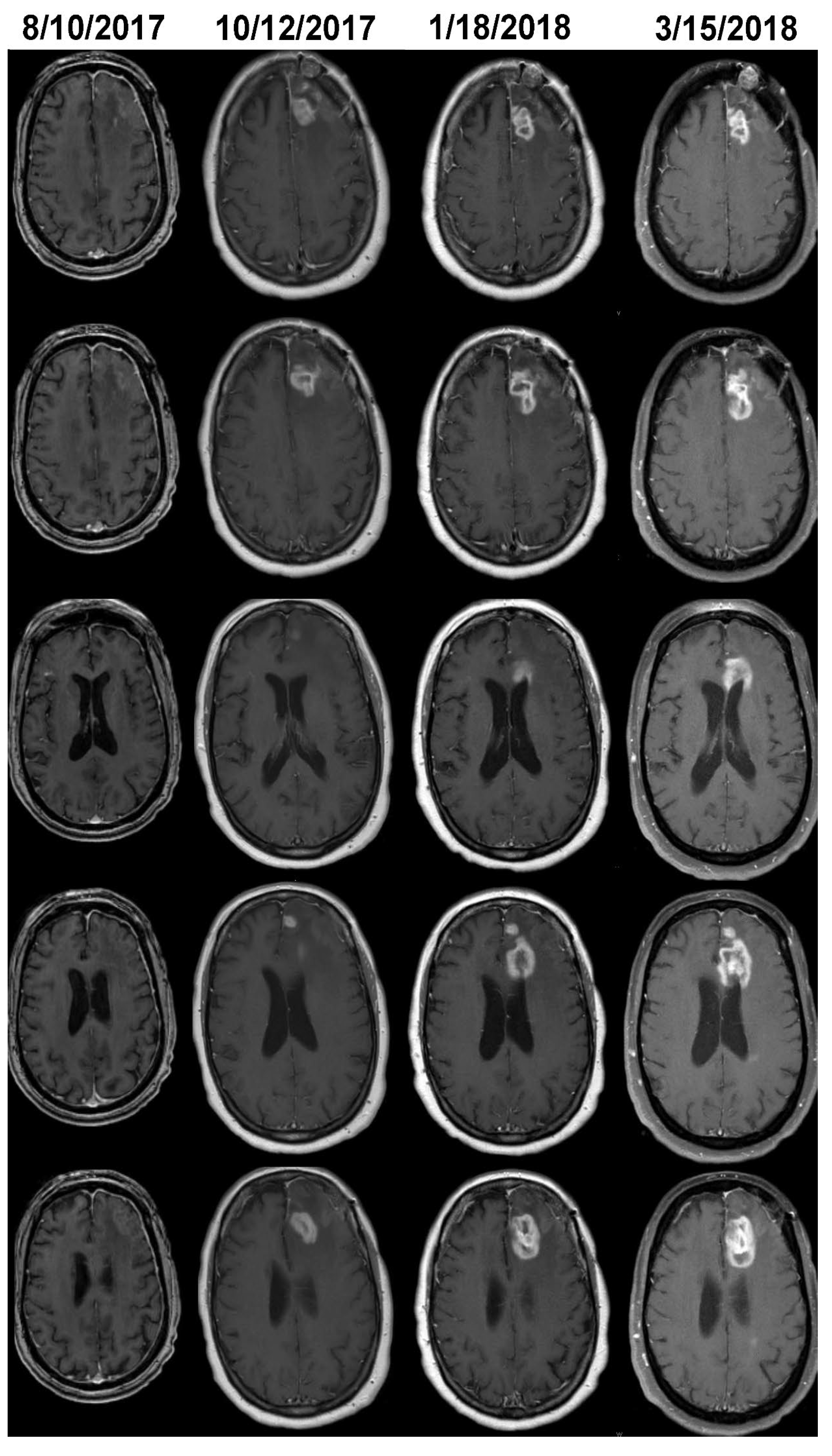
Growth Detection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GBM | Glioblastomas |
| AI | Artificial Intelligence |
| PsPD | Pseudoprogression |
| LGG | Low-grade-glioma |
| MRI | Magnetic Resonance Imaging |
References
- Omuro, A.; DeAngelis, L.M. Glioblastoma and other malignant gliomas: a clinical review. JAMA 2013, 310, 1842-1850, doi:10.1001/jama.2013.280319. [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Stetson, L.; Virk, S.; Barnholtz-Sloan, J.S. Epidemiology of Intracranial Gliomas. Prog Neurol Surg 2018, 30, 1-11, doi:10.1159/000464374. [CrossRef]
- Grochans, S.; Cybulska, A.M.; Siminska, D.; Korbecki, J.; Kojder, K.; Chlubek, D.; Baranowska-Bosiacka, I. Epidemiology of Glioblastoma Multiforme-Literature Review. Cancers (Basel) 2022, 14, doi:10.3390/cancers14102412. [CrossRef]
- Baldi, I.; Huchet, A.; Bauchet, L.; Loiseau, H. [Epidemiology of glioblastoma]. Neurochirurgie 2010, 56, 433-440, doi:10.1016/j.neuchi.2010.07.011. [CrossRef]
- Ostrom, Q.T.; Bauchet, L.; Davis, F.G.; Deltour, I.; Fisher, J.L.; Langer, C.E.; Pekmezci, M.; Schwartzbaum, J.A.; Turner, M.C.; Walsh, K.M.; et al. The epidemiology of glioma in adults: a “state of the science” review. Neuro Oncol 2014, 16, 896-913, doi:10.1093/neuonc/nou087. [CrossRef]
- Tamimi, A.F.; Juweid, M. Epidemiology and Outcome of Glioblastoma. In Glioblastoma, De Vleeschouwer, S., Ed.; Brisbane (AU), 2017.
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005, 352, 987-996, doi:10.1056/NEJMoa043330. [CrossRef]
- Scribner, E.; Saut, O.; Province, P.; Bag, A.; Colin, T.; Fathallah-Shaykh, H.M. Effects of anti-angiogenesis on glioblastoma growth and migration: model to clinical predictions. PLoS One 2014, 9, e115018, doi:10.1371/journal.pone.0115018. [CrossRef]
- Scribner, E.; Hackney, J.R.; Machemehl, H.C.; Afiouni, R.; Patel, K.R.; Fathallah-Shaykh, H.M. Key rates for the grades and transformation ability of glioma: model simulations and clinical cases. J Neurooncol 2017, 133, 377-388, doi:10.1007/s11060-017-2444-6. [CrossRef]
- Raman, F.; Scribner, E.; Saut, O.; Wenger, C.; Colin, T.; Fathallah-Shaykh, H.M. Computational Trials: Unraveling Motility Phenotypes, Progression Patterns, and Treatment Options for Glioblastoma Multiforme. PLoS One 2016, 11, e0146617, doi:10.1371/journal.pone.0146617. [CrossRef]
- Tang, Z.; Araysi, L.M.; Fathallah-Shaykh, H.M. c-Src and neural Wiskott-Aldrich syndrome protein (N-WASP) promote low oxygen-induced accelerated brain invasion by gliomas. PLoS One 2013, 8, e75436, doi:10.1371/journal.pone.0075436. [CrossRef]
- Han, X.; Zhang, W.; Yang, X.; Wheeler, C.G.; Langford, C.P.; Wu, L.; Filippova, N.; Friedman, G.K.; Ding, Q.; Fathallah-Shaykh, H.M.; et al. The role of Src family kinases in growth and migration of glioma stem cells. Int J Oncol 2014, 45, 302-310, doi:10.3892/ijo.2014.2432. [CrossRef]
- Torrisi, F.; Vicario, N.; Spitale, F.M.; Cammarata, F.P.; Minafra, L.; Salvatorelli, L.; Russo, G.; Cuttone, G.; Valable, S.; Gulino, R.; et al. The Role of Hypoxia and SRC Tyrosine Kinase in Glioblastoma Invasiveness and Radioresistance. Cancers (Basel) 2020, 12, doi:10.3390/cancers12102860. [CrossRef]
- Scribner, E.; Fathallah-Shaykh, H.M. Single Cell Mathematical Model Successfully Replicates Key Features of GBM: Go-Or-Grow Is Not Necessary. PLoS One 2017, 12, e0169434, doi:10.1371/journal.pone.0169434. [CrossRef]
- Booth, T.C.; Luis, A.; Brazil, L.; Thompson, G.; Daniel, R.A.; Shuaib, H.; Ashkan, K.; Pandey, A. Glioblastoma post-operative imaging in neuro-oncology: current UK practice (GIN CUP study). Eur Radiol 2021, 31, 2933-2943, doi:10.1007/s00330-020-07387-3. [CrossRef]
- Collaborative, I.-G.; Neurology; Neurosurgery Interest, G.; British Neurosurgical Trainee Research, C. Imaging timing after surgery for glioblastoma: an evaluation of practice in Great Britain and Ireland (INTERVAL-GB)- a multi-centre, cohort study. J Neurooncol 2024, 169, 517-529, doi:10.1007/s11060-024-04705-3. [CrossRef]
- Leao, D.J.; Craig, P.G.; Godoy, L.F.; Leite, C.C.; Policeni, B. Response Assessment in Neuro-Oncology Criteria for Gliomas: Practical Approach Using Conventional and Advanced Techniques. AJNR Am J Neuroradiol 2020, 41, 10-20, doi:10.3174/ajnr.A6358. [CrossRef]
- Gillespie, C.S.; Bligh, E.R.; Poon, M.T.C.; Solomou, G.; Islim, A.I.; Mustafa, M.A.; Rominiyi, O.; Williams, S.T.; Kalra, N.; Mathew, R.K.; et al. Imaging timing after glioblastoma surgery (INTERVAL-GB): protocol for a UK and Ireland, multicentre retrospective cohort study. BMJ Open 2022, 12, e063043, doi:10.1136/bmjopen-2022-063043. [CrossRef]
- Fathallah-Shaykh, H.M.; DeAtkine, A.; Coffee, E.; Khayat, E.; Bag, A.K.; Han, X.; Warren, P.P.; Bredel, M.; Fiveash, J.; Markert, J.; et al. Diagnosing growth in low-grade gliomas with and without longitudinal volume measurements: A retrospective observational study. PLoS Med 2019, 16, e1002810, doi:10.1371/journal.pmed.1002810. [CrossRef]
- Chamberlain, M.C. Pseudoprogression in glioblastoma. J Clin Oncol 2008, 26, 4359; author reply 4359-4360, doi:10.1200/JCO.2008.18.4440. [CrossRef]
- Brandes, A.A.; Franceschi, E.; Tosoni, A.; Blatt, V.; Pession, A.; Tallini, G.; Bertorelle, R.; Bartolini, S.; Calbucci, F.; Andreoli, A.; et al. MGMT promoter methylation status can predict the incidence and outcome of pseudoprogression after concomitant radiochemotherapy in newly diagnosed glioblastoma patients. J Clin Oncol 2008, 26, 2192-2197, doi:10.1200/JCO.2007.14.8163. [CrossRef]
- Le Fevre, C.; Lhermitte, B.; Ahle, G.; Chambrelant, I.; Cebula, H.; Antoni, D.; Keller, A.; Schott, R.; Thiery, A.; Constans, J.M.; et al. Pseudoprogression versus true progression in glioblastoma patients: A multiapproach literature review: Part 1 - Molecular, morphological and clinical features. Crit Rev Oncol Hematol 2021, 157, 103188, doi:10.1016/j.critrevonc.2020.103188. [CrossRef]
- Brandsma, D.; Stalpers, L.; Taal, W.; Sminia, P.; van den Bent, M.J. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol 2008, 9, 453-461, doi:10.1016/S1470-2045(08)70125-6. [CrossRef]
- Kerkhof, M.; Tans, P.L.; Hagenbeek, R.E.; Lycklama, A.N.G.J.; Holla, F.K.; Postma, T.J.; Straathof, C.S.; Dirven, L.; Taphoorn, M.J.; Vos, M.J. Visual inspection of MR relative cerebral blood volume maps has limited value for distinguishing progression from pseudoprogression in glioblastoma multiforme patients. CNS Oncol 2017, 6, 297-306, doi:10.2217/cns-2017-0013. [CrossRef]
- Sidibe, I.; Tensaouti, F.; Roques, M.; Cohen-Jonathan-Moyal, E.; Laprie, A. Pseudoprogression in Glioblastoma: Role of Metabolic and Functional MRI-Systematic Review. Biomedicines 2022, 10, doi:10.3390/biomedicines10020285. [CrossRef]
- Strauss, S.B.; Meng, A.; Ebani, E.J.; Chiang, G.C. Imaging Glioblastoma Posttreatment: Progression, Pseudoprogression, Pseudoresponse, Radiation Necrosis. Neuroimaging Clin N Am 2021, 31, 103-120, doi:10.1016/j.nic.2020.09.010. [CrossRef]
- Barhoumi, Y.; Fattah, A.H.; Bouaynaya, N.; Moron, F.; Kim, J.; Fathallah-Shaykh, H.M.; Chahine, R.A.; Sotoudeh, H. Robust AI-Driven Segmentation of Glioblastoma T1c and FLAIR MRI Series and the Low Variability of the MRIMath(c) Smart Manual Contouring Platform. Diagnostics (Basel) 2024, 14, doi:10.3390/diagnostics14111066. [CrossRef]
- Ce, M.; Irmici, G.; Foschini, C.; Danesini, G.M.; Falsitta, L.V.; Serio, M.L.; Fontana, A.; Martinenghi, C.; Oliva, G.; Cellina, M. Artificial Intelligence in Brain Tumor Imaging: A Step toward Personalized Medicine. Curr Oncol 2023, 30, 2673-2701, doi:10.3390/curroncol30030203. [CrossRef]
- Raman, F.; Mullen, A.; Byrd, M.; Bae, S.; Kim, J.; Sotoudeh, H.; Moron, F.E.; Fathallah-Shaykh, H.M. Evaluation of RANO Criteria for the Assessment of Tumor Progression for Lower-Grade Gliomas. Cancers (Basel) 2023, 15, doi:10.3390/cancers15133274. [CrossRef]
- Dera, D.a.R., Fabio and Bouaynaya, Nidhal and Fathallah-Shaykh, Hassan M. Interactive Semi-automated Method Using Non-negative Matrix Factorization and Level Set Segmentation for the BRATS Challenge. In Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries, Crimi, A.a.M., Bjoern and Maier, Oskar and Reyes, Mauricio and Winzeck, Stefan and Handels, Heinz, Ed.; Springer International Publishing: 2016; pp. 195-205.
- Ramakrishnan, D.; von Reppert, M.; Krycia, M.; Sala, M.; Mueller, S.; Aneja, S.; Nabavizadeh, A.; Galldiks, N.; Lohmann, P.; Raji, C.; et al. Evolution and implementation of radiographic response criteria in neuro-oncology. Neurooncol Adv 2023, 5, vdad118, doi:10.1093/noajnl/vdad118. [CrossRef]
- Hajkova, M.; Andrasina, T.; Ovesna, P.; Rohan, T.; Dostal, M.; Valek, V.; Ostrizkova, L.; Tucek, S.; Sedo, J.; Kiss, I. Volumetric Analysis of Hepatocellular Carcinoma After Transarterial Chemoembolization and its Impact on Overall Survival. In Vivo 2022, 36, 2332-2341, doi:10.21873/invivo.12964. [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009, 45, 228-247, doi:10.1016/j.ejca.2008.10.026. [CrossRef]
- Khalili, N.K., A.F.; Bagheri, S.; Familiar, A.; Viswanathan, K.; Anderson, H.; Haldar, D.; Ware, J.B.; Vossough, A.; Ali Nabavizadeh, A. Volumetric measurment of tumor size outperforms standard two-dimensional method in early prediction of tumor progression in pediatric glioma. Neuro-Oncology 2023, 25, i48.
- von Reppert, M.; Ramakrishnan, D.; Bruningk, S.C.; Memon, F.; Abi Fadel, S.; Maleki, N.; Bahar, R.; Avesta, A.E.; Jekel, L.; Sala, M.; et al. Comparison of volumetric and 2D-based response methods in the PNOC-001 pediatric low-grade glioma clinical trial. Neurooncol Adv 2024, 6, vdad172, doi:10.1093/noajnl/vdad172. [CrossRef]
- Ellingson, B.M.; Kim, G.H.J.; Brown, M.; Lee, J.; Salamon, N.; Steelman, L.; Hassan, I.; Pandya, S.S.; Chun, S.; Linetsky, M.; et al. Volumetric measurements are preferred in the evaluation of mutant IDH inhibition in non-enhancing diffuse gliomas: Evidence from a phase I trial of ivosidenib. Neuro Oncol 2022, 24, 770-778, doi:10.1093/neuonc/noab256. [CrossRef]
- Dempsey, M.F.; Condon, B.R.; Hadley, D.M. Measurement of tumor “size” in recurrent malignant glioma: 1D, 2D, or 3D? AJNR Am J Neuroradiol 2005, 26, 770-776.
- Vos, M.J.; Uitdehaag, B.M.; Barkhof, F.; Heimans, J.J.; Baayen, H.C.; Boogerd, W.; Castelijns, J.A.; Elkhuizen, P.H.; Postma, T.J. Interobserver variability in the radiological assessment of response to chemotherapy in glioma. Neurology 2003, 60, 826-830, doi:10.1212/01.wnl.0000049467.54667.92. [CrossRef]
- Abayazeed, A.H.; Abbassy, A.; Mueller, M.; Hill, M.; Qayati, M.; Mohamed, S.; Mekhaimar, M.; Raymond, C.; Dubey, P.; Nael, K.; et al. NS-HGlio: A generalizable and repeatable HGG segmentation and volumetric measurement AI algorithm for the longitudinal MRI assessment to inform RANO in trials and clinics. Neurooncol Adv 2023, 5, vdac184, doi:10.1093/noajnl/vdac184. [CrossRef]
- Menze, B.H.; Jakab, A.; Bauer, S.; Kalpathy-Cramer, J.; Farahani, K.; Kirby, J.; Burren, Y.; Porz, N.; Slotboom, J.; Wiest, R.; et al. The Multimodal Brain Tumor Image Segmentation Benchmark (BRATS). IEEE Trans Med Imaging 2015, 34, 1993-2024, doi:10.1109/TMI.2014.2377694. [CrossRef]
- Hatamizadeh, A.; Nath, V.; Tang, Y.; Yang, D.; Roth, H.R.; Xu, D. Swin UNETR: Swin Transformers for Semantic Segmentation of Brain Tumors in MRI Images. ArXiv 2022, abs/2201.01266.
- Jia, Z.; Zhu, H.; Zhu, J.; Ma, P. Two-Branch network for brain tumor segmentation using attention mechanism and super-resolution reconstruction. Comput Biol Med 2023, 157, 106751, doi:10.1016/j.compbiomed.2023.106751. [CrossRef]
- Wee, C.W.; Sung, W.; Kang, H.C.; Cho, K.H.; Han, T.J.; Jeong, B.K.; Jeong, J.U.; Kim, H.; Kim, I.A.; Kim, J.H.; et al. Evaluation of variability in target volume delineation for newly diagnosed glioblastoma: a multi-institutional study from the Korean Radiation Oncology Group. Radiat Oncol 2015, 10, 137, doi:10.1186/s13014-015-0439-z. [CrossRef]
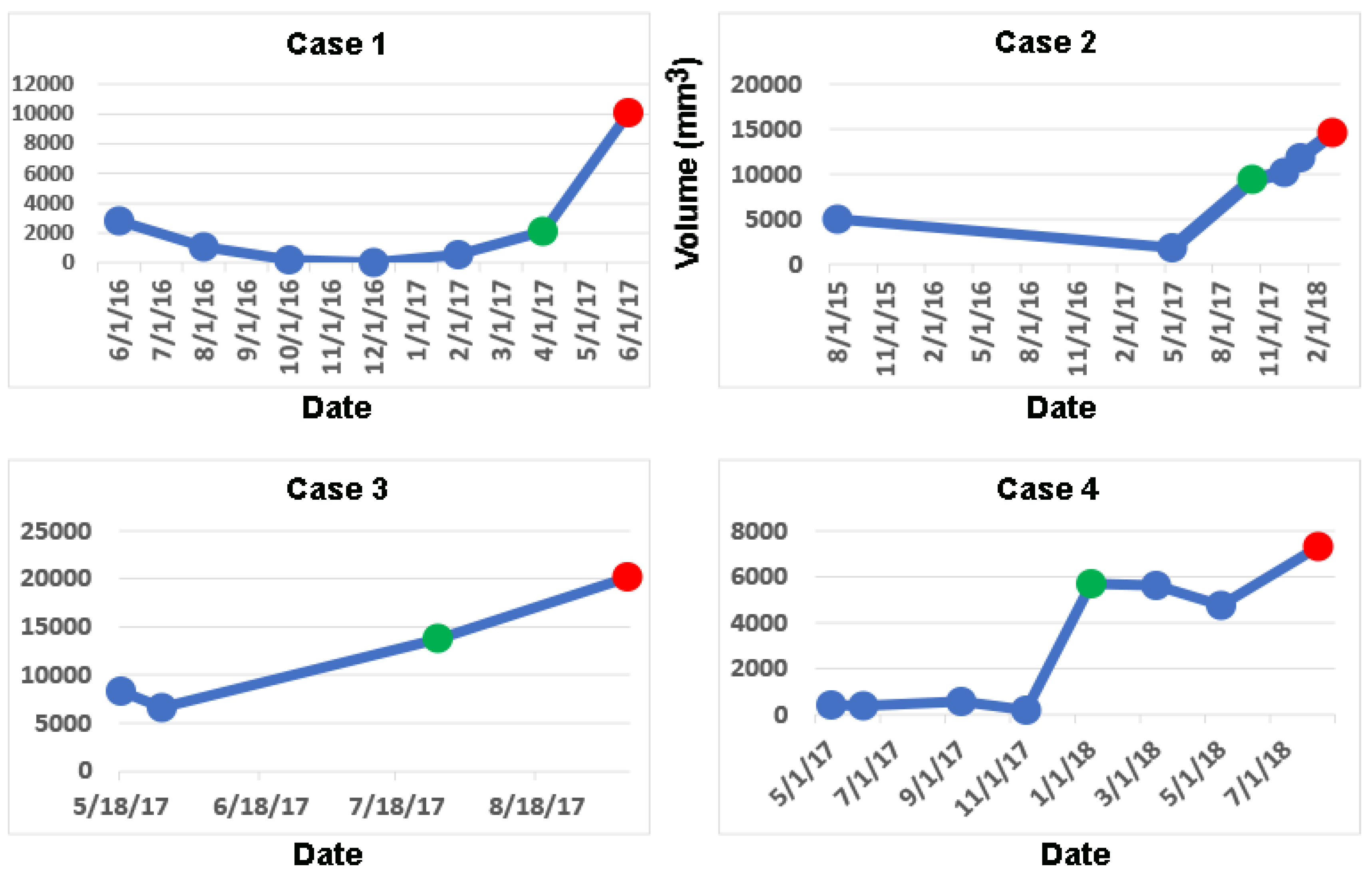

| Cases with earlier detection of progression | Median (IQR) | Mean (STD) |
| 4/15 | 105 (116) days | 56 (80) days |
| Case | Radiological Impression | Neuro-oncologist Impression | Percent Change in Volume |
|---|---|---|---|
| 1 | Stable | Stable | +86% |
| 2 | Treatment Effect | Slight Change | +295% |
| 3 | Mild progression | Mild Progression | +107% |
| 4 | Not available | Stable | +2843% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



