
Submitted:
05 January 2025
Posted:
06 January 2025
You are already at the latest version
Abstract
Atrial fibrillation (AF) is a supraventricular arrhythmia and the most common heart rhythm disorder in the adult population worldwide with an estimated prevalence of 2% to 4% of the population. Cases of AF have shown an increasing trend in recent decades, while its frequency is expected to rise even more. Given the significant impact on patients’ quality of life, as well as its major complications -including thromboembolic events- effective rhythm control strategies other than antiarrhythmic medication have emerged, with catheter ablation (CA) being the cornerstone of these. During recent years, CA has been upgraded into first-line treatment for selected patients. However, complications do exist and arrhythmia-free survival is not always warranted. The need to better identify patients more suitable for this specific therapeutic measure is crucial in improving outcomes and preventing arrhythmia recurrences. This review aims to present currently identified predictors of AF recurrence after catheter ablation based on clinical characteristics, electrocardiographic and echocardiographic parameters, in an era of increasing interventional rhythm control approaches for the management of AF.
Keywords:
atrial fibrillation
; catheter ablation
; recurrence
; predictors
; clinical
; electrocardiogram
; transthoracic echocardiogram
1. Introduction
Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia globally, with a rising incidence due to its progressive nature and increased morbidity and mortality [1]. Atrial remodeling, including dilation and fibrosis, are characteristics in AF and can contribute to structural and electrical changes in the heart. As a result, not only the burden of AF is increased but also the risk of recurrence is elevated, approaching 90% after the initial episode. To improve patient outcomes, the need for effective rhythm control strategies has arisen and among the available interventions, catheter ablation has emerged [2].
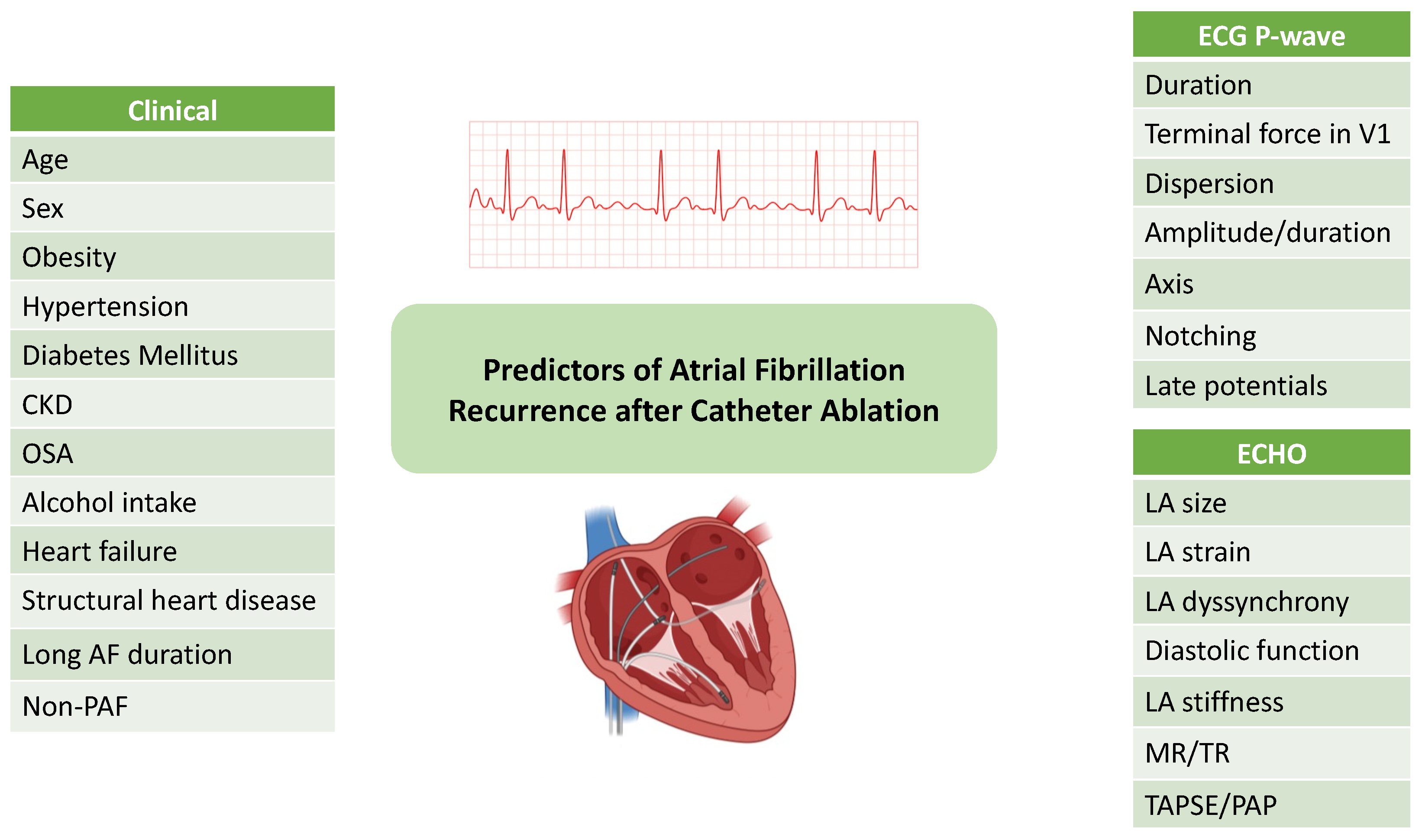
Figure 1.
Graphical abstract. Common predictors of atrial fibrillation recurrence after catheter ablation. CKD=Chronic kidney disease, OSA=obstructive sleep apnea, AF=atrial fibrillation, non-PAF=non-paroxysmal AF, LA=left atrium, MR=mitral regurgitation, TR=tricuspid regurgitation, TAPSE=tricuspid annular plane systolic excursion, PAP=pulmonary artery pressure.
Figure 1.
Graphical abstract. Common predictors of atrial fibrillation recurrence after catheter ablation. CKD=Chronic kidney disease, OSA=obstructive sleep apnea, AF=atrial fibrillation, non-PAF=non-paroxysmal AF, LA=left atrium, MR=mitral regurgitation, TR=tricuspid regurgitation, TAPSE=tricuspid annular plane systolic excursion, PAP=pulmonary artery pressure.
Initially considered a last-resort treatment, catheter ablation (CA) has evolved into a first line option for selected patients, since it is demonstrating significant benefits in reducing the progression from paroxysmal AF (PAF) to persistent AF and improving quality of life compared to antiarrhythmic drugs [3]. The role of pulmonary vein isolation (PVI) and the reduction of procedural risks led to this transition, and thus today early intervention holds promising results in achieving durable rhythm control and potentially curing AF in individuals [1,4]. Techniques for PVI include traditional thermal methods, such as radiofrequency ablation (RFA) and cryoballoon ablation (CBA), as well as novel non-thermal approaches, such as pulsed-field ablation (PFA) [5].
Despite this progress, the long-term success of catheter ablation remains suboptimal, with recurrence rates ranging from 20%-50%. Patient variability plays a core role in the outcomes, with underlying atrial myopathy arising as the key contributor to AF recurrence. Atrial fibrosis stabilizes reentrant circuits that sustain AF and therefore relates to persistent arrhythmia and resistance to therapy. [6]. In addition, cardiac structural changes such as atrial dilation, inflammation and myocyte injury limit the likelihood of a maintained sinus rhythm. These indicate the importance of timely intervention and the optimization of the procedures [7].
Identifying the predictors of recurrence is crucial for patient selection and treatment strategies. Advances in biomarker research may further the ability to predict recurrence and guide personalized treatment plans, yet it is known that older age, structural heart disease, longer AF duration, and larger left atrial size, along with procedural factors such as incomplete PVI, influence patient outcomes [8]. This review article will focus on clinical characteristics, as well as electrocardiographically and echocardiographically-derived parameters, that have been associated with AF relapse after CA.
2. AF Recurrence After Catheter Ablation
It is important to distinguish AF recurrence from other atrial tachyarrhythmias. A 30-second threshold for AF duration after ablation has been proposed, but this binary classification does not always clearly reflect the clinical outcomes of ablation and the improvement in patients’ quality of life [4]. AF is considered as clinical when it is symptomatic or asymptomatic and recorded on a surface ECG or other recorder and subclinical, when it is detected by cardiac implantable electronic devices or smart watches. Recently, AF burden post-catheter ablation has been used as an endpoint by several investigators and may carry a stronger clinical relevance. Up to 50% of patients may experience a recurrence, depending on the method of AF detection, while among these events, 30% may occur very late, after the first year [9]. A large proportion of these patients are led to a repeat procedure, according to a recently published EHRA survey [10].
Based on the timing of AF reappearance post-catheter ablation, recurrences are categorized into early, late and very late. Traditionally, early recurrences of AF (ERAF) were timed within the blanking period, which up until recently was considered as the first three months after ablation, during which time a repeat procedure is advised against [11]. With the recently published 2024 EHRA expert consensus statement on catheter and surgical ablation for atrial fibrillation, the blanking period was reduced to 8 weeks [4]. The mechanisms behind ERAF are not clearly understood, although myocardial inflammation and injury, as well as a transient imbalance in the autonomic nervous system seem to play a major part in this phenomenon, when it occurs early within the blanking period, while PV reconnection might be of significance when ERAF occurs later on [12,13,14]. Recurrences outside the first trimester timeframe and up until the first year post-ablation are late recurrences (LRAF). Many investigators have proven a strongly positive relationship of ERAF with ablation failure, as patients have increased rates of AF after experiencing atrial arrhythmias within the blanking period both with RFA and CBA [15,16]. The number and exact timing of episodes during the first three months also seem to play an important role in the outcome of the procedure [17]. More specifically, ERAF seems to carry a worse prognosis when occurring further away from the procedure date, owing perhaps to the arrhythmogenic effect of local inflammation and scarring, happening during the first 3-4 weeks [18]. Based on this principle, the shortened duration of the blanking period is expected to reclassify up to 3.4% of procedures as failed [19]. On the other hand, very late recurrences (VLRAF) after the first twelve months from the procedure are most commonly attributed to PV reconnection and extrapulmonary triggers of AF [20].
3. Predictors of AF Recurrence After Catheter Ablation
3.1. Clinical Predictors
One of the most important predictors in the long-term success of CA and sinus rhythm maintenance is AF type and duration. Studies have shown that patients with non-paroxysmal AF (persistent and long-standing persistent) have increased incidence of post-ablation atrial arrhythmias[21]. Particularly long-standing persistent AF seems to attain the highest rates of recurrence after ablation [22]. An increasing number of researchers are currently advocating for early ablation in hopes of halting AF progression and atrial myopathy. This approach may be associated with the advantage of lower recurrence rates, as well as stroke and congestive heart failure [23]. The benefit is more pronounced if the diagnosis-to-ablation time remains shorter than three years [24]. This observation has prompted cardiovascular societies across both sides of the Atlantic in publishing guidelines within the last two years, with an upgraded class I indication of CA as first-line therapy in selected patients with paroxysmal AF (PAF) [1,4,25].
The recent ESC/EACTS guidelines for the management of atrial fibrillation also emphasize the pivotal role of comorbidities in AF initiation and perpetuation, with the AF-CARE algorithm. More specifically, conditions such as hypertension, heart failure, diabetes mellitus, increased BMI, obstructive sleep apnoea and excessive alcohol intake, are considered triggers of arrhythmia presentation and should be appropriately managed, in order to prevent recurrences [1]. Furthermore, demographic characteristics, including older age particularly more than 75 years old, hold an positive association with AF relapses after CA [26,27]. The role of gender in AF recurrence rates remain controversial, with some studies suggesting females have decreased arrhythmia-free survival rates, and others show neutral results [28,29]. Chronic kidney disease has also been long linked with worse outcomes regarding rhythm control after CA [30]. A large meta-analysis of 23.468 patients who underwent RFA or CBA showed that the recurrence risk was greater in those patients with impaired renal function [31]. In the case of structural heart disease coexistence, a background of coronary artery disease and cardiomyopathy -such as amyloidosis-, increases AF recurrence after CA, with the exception of tachycardia-induced cardiomyopathy [32,33,34,35]. Finally, even though heart failure patients seem to have worse rhythm outcomes after CA, reducing time-to-ablation time may prevent a reasonable number of recurrences in this group and therefore, improve quality of life [36,37].
The presence of low voltage areas (LVAs) within the atrial myocardium is a critical indicator of the progression of AF and the stage of the disease in terms of atrial myopathy and remodeling. LVAs have been shown in several studies to be strongly associated with worse clinical outcomes after ablation [38]. Factors such as persistent AF, female sex, increased left atrial volume (LAV) have been independently associated with LVAs [39]. Therefore, predictive scores regarding the presence of LVAs may have clinical value in individualizing the approach, selecting different treatment strategies, and improving ablation outcomes in appropriate patients.
Several scores have been developed to predict atrial myopathy and, as a result, recurrence rates after ablation. Most of these scores use the aforementioned clinical predictors for AF recurrence, sometime in conjunction with imaging parameters. The CHADS2, CHA2DS2-VASc and R2CHADS2 scores, initially developed for thromboembolic risk prediction, were able to be correlated with both clinical AF recurrences and the presence of LVAs [40,41]. Later, scoring systems were created based on the results of ablation in rhythm control. Among the most promising are the APPLE score and the MB-LATER score, which can also predict late recurrences (>12 months). The APPLE score includes several factors such as age over 65 years, persistent AF, GFR <60 ml/min/1.73 m2, left atrial dilation >43 mm and ejection fraction <50%. The MB-LATER score has also been shown to be useful for accurately predicting VLRAF after RFA or CBA [42,43]. The C2HEST and HATCH scores were also significantly associated with risk of late recurrence after RFA [44]. Other scoring systems target exclusively the electroanatomical substrate, such as the DR-FLASH score, which -in multiple cohorts- was able to successfully predict those patients who required extensive substrate modification [45,46]. Finally, the LAGO score combined advanced imaging of the LA with CTA or MRA with clinical parameters, such as AF phenotype and presence of structural heart disease. Values ≥ 3 were correlated with more adverse rhythm outcomes after RFA [47].
To this date, no ideal prognostic score has been developed to predict adverse rhythm outcomes after AF ablation. In order to increase the risk stratification accuracy, a combination of more than one of the available scoring systems is suggested [48]. Table 1 and Table 2 provide a representation of some of the most frequently used clinical scores and the associated variables, as well as a categorization based on the type of recurrence they can predict.
3.2. Electrocardiographic Predictors
Various electrocardiographic (ECG) measurements of P-wave parameters have been investigated in AF recurrences after AFCA. A few of the most commonly researched indices are P-wave duration (PWD), P-wave terminal force in V1 (PTFV1), P-wave dispersion, P-wave amplitude (PWA), P-wave axis, P-wave notching and atrial late potentials. These parameters reflect atrial cardiomyopathy and remodeling, which is a recognized substrate of AF recurrences [58]. Table 3 demonstrates the upper limits of these indices that have been related with increase in AF recurrence after CA.
P-wave duration is an independent predictor of AF recurrence after ablation according to a recent systematic review and meta-analysis published in Europace [59]. Traditionally, PWD has been measured in lead II where the P-wave was considered to better visualized. However, the location of the longest P-wave duration varies from individual to individual. Automated or manual measurement is possible [58]. PWD is considered normal when measured below 120 ms, while PWD >120 ms indicates partial interatrial block (IAB) in which there is delayed activation of the LA via the Bachmann bundle. In advanced IAB, there is retrograde activation of the LA via muscle bundles near the atrioventricular junction, and as a result, the P-wave morphology in the inferior leads (II,III,avF) tends to be biphasic with a late negative branch reflecting retrograde conduction in the LA [60]. The risk of AF recurrence increases exponentially with progressively greater PWD. Partial IAB leads to a doubling of recurrences, while advanced IAB leads to a quadrupling. A strong association between PWD and AF recurrences after ablation was also demonstrated in a 2019 meta-analysis, showing that PWD >120ms to >150ms in sinus rhythm before PVI leads to recurrence regardless of age, sex, LA dimension, and the presence of structural disease [61]. Therefore, PWD could be a quite useful and easily accessible indicator of underlying atrial remodeling and have clinical significance in better stratifying patients with atrial fibrillation to different treatments [62].
PTFV1 was first described by Morris et al in 1964 and was initially considered to be an indirect electrocardiographic predictor of left atrial enlargement (LAE) [63]. Since then, several studies have been able to demonstrate a strong association of this marker with interatrial conduction delays, low voltage areas and diffuse atrial fibrosis [64,65]. PTFV1 is defined as the negative deflection at the end of the P-wave in lead V1 due to posterior displacement of the LA. It is measured by multiplying the duration of the terminal negative force of the p wave in lead V1 in seconds by its width in mm. A PTFV1>0.04 mm*s is considered pathological. According to a recent meta-analysis, the presence of an abnormal PTFV1 derived from a resting ECG analysis is strongly associated with an increased risk of AF recurrence of at least 23% [66]. A cohort study of 453 patients with persistent atrial fibrillation who underwent ablation for the first time was able to demonstrate a strong relationship between PTFV1 measured 3 months later and AF recurrence [67]. Another prospective study also showed that abnormal PTFV1 was more frequent in the recurrence group post AFCA, despite normal LA diameter and volume [68]. Finally, increasing values of PTFV1 by more than 0.69 might be able to predict PV reconnection in patients undergoing a second ablation procedure [69].
P-wave dispersion is defined as the absolute difference between the longest and shortest P-wave durations on a 12-lead surface ECG [70]. Although no threshold has been established at which it is considered pathological, a value greater than 40 ms is considered increased, although it can also occur in healthy individuals [71]. The hypothesis that an increased P-wave dispersion could predict paroxysmal AF or recurrence after ablation is based on the assumption that any difference in P-wave duration in different leads reflects local delays in atrial conduction that could be the manifestation of fibrosis acting as a substrate for AF [72]. A retrospective ECG cohort of 42,751 patients showed that a P wave dispersion >80 ms had a hazard ratio of 2 for atrial fibrillation when adjusted for age and sex [73]. Results from a meta-analysis of 1674 AF patients showed a significantly increased P-wave dispersion in patients with recurrence after CBA or RFA, suggesting the possible predictive value of this parameter[74].
Changes in P-wave amplitude (PWA) have been studied post-AF catheter ablation, with most researchers agreeing that PWA decreases, although its correlation with recurrences is still not clear [75]. However, another parameter, the PWD/PWA ratio, has been associated with AF recurrence and low voltage areas (LVAs) in the atrial myocardium, with some researchers suggesting that a ratio of >830ms/mV has a 61.8% sensitivity and 88.4% specificity for the prediction of the AF recurrence [76]. In another study, researchers used a mapping system to identify LVAs and simultaneously measured the maximum PWD to the maximum P-wave height in lead I. This model was statistically significantly associated with recurrences of atrial tachyarrhythmia after ablation [77].
Other P-wave parameters being considered as markers of AF recurrences post-catheter ablation are P-wave axis and notching. While P-wave axis is one of the most studied parameters for predicting AF risk in general population -as a reflection of adverse anatomical and electrical atrial remodeling-, its predictive value in AF recurrence has not been clearly specified, with studies showing mixed results. Values between 0-75 ̊ being considered normal [73,78,79,80]. Based on a Japanese study of 249 patients undergoing AF ablation, an abnormal P-wave axis value was identified in 14% of patients and was considered to be independently associated with AF recurrence [81]. One the other hand, the morphological change in the P-wave observed in lead II on a 12-lead ECG as M-shaped with a peak-to-peak distance of more than 20ms is recorded as a notch and reflects the conduction delay caused by LA remodeling and has been shown to predict recurrences in patients who have undergone ablation [82,83].
Finally, a special mention should be made regarding atrial late potentials. These represent low-amplitude, high-frequency electrical signals recorded at the end of the P wave using high-resolution techniques and signal averaging ECG. They are attributed to delayed and disorganized activity in small areas of the atrial myocardium. The average P wave signal has been used to predict the risk of developing atrial tachyarrhythmias in patients with structural heart disease [84]. Even though no clear normal limits have been established for the atrium and it is a rarely studied parameter -owing to the necessity of special equipment- dynamic changes in late atrial potentials have been described after AF ablation [85]. The most commonly used measurements are the duration of the filtered P-wave and the root mean square of the potentials in the last 20 ms of the P wave (RMS20). The role of this marker in AF recurrences after rhythm control strategies is highlighted by a study of patients undergoing electrical cardioversion [86]. Also, another small study of 15 patients demonstrated that the duration of the P-wave as measured by signal-averaging techniques was longer in patients who relapsed after ablation [87].
Considering other ECG features, the presence of bundle branch block seems to influence patient outcomes. More specifically, both left (LBBB) and right (RBBB) bundle branch block have been associated with AF recurrences after ablation [88,89]. Also, larger amplitude of fibrillatory waves in persistent AF has been related with better prognosis in a study of 704 patients, given that “fine AF” almost always implies more advances atrial myopathy [90]. Early repolarization changes, especially in inferior or lateral leads, may also predispose patients in AF recurrence, although the mechanism can only be hypothesized, with possible autonomic dysregulation, ion-channel imbalances and genetic background being held accountable [91]. Particularly in the context of hypertrophic cardiomyopathy, QRS fragmentation and QTc prolongation have been independently associated with arrhythmia recurrences [92]. However, all of these abnormalities need validation in larger cohorts.
3.3. Echocardiographic Predictors
The echocardiographic parameters associated with adverse LA remodeling include LA anatomical and functional features, LA synchrony, measures of diastolic function and the presence of atrioventricular valvular heart disease, as well as novel markers, such as the left atrioventricular coupling index, LA stiffness index and right ventricular-to-pulmonary artery coupling (RV-to-PA coupling). Table 4 indicates the respective cut-off values that have been associated with increase in AF recurrence after CA.
The hallmark of LA anatomical remodeling is LA dilatation, with progressive alteration in mechanical and electrical function and fibrosis [93]. Measures include the anteroposterior LA diameter (LAD) in the parasternal long axis view or the LA volume (LAV) and LA volume index (LAVi) on the apical four- and two-chamber view on transthoracic echocardiogram. Increased LAD is closely associated with atrial myopathy and atrial remodeling, therefore it is considered an independent predictor of AF recurrence after ablation [94,95]. Additionally, its integration in many of the clinical scores previously mentioned has led to their improved sensitivity in predicting recurrences [96]. According to the results of a meta-analysis that examined data from 22 studies and a total of 3750 patients, an increase in LAD was associated with AF recurrence after ablation [97]. Another recent meta-analysis of 20 studies showed that patients with larger left atrial volume (LAV) and left atrial volume index (LAVi) show an increased rate of AF recurrence after RFA ablation [98]. Increased LAV is associated with progressive diastolic dysfunction and consequently reflects a deterioration of LA function leading to a higher risk of AF recurrence after RFA [99]. Finally, the left atrial sphericity index is an important parameter of left atrial geometric remodeling, calculated as the ratio of the maximum transverse to the maximum longitudinal diameter in the apical four-chamber view, and has been associated with AF recurrences after ablation [100,101].
Left atrial function is responsible for adequate left ventricular filling. Its assessment by LA strain may be more sensitive than conventional measurement of LV filling pressures [102,103]. According to a 2018 consensus document of the European Association for Cardiovascular Imaging (EACVI), LA strain—as calculated by 2D speckle-tracking echocardiography (2D-STE)—is a cyclical process that can be subdivided into three phases, the reservoir (LASr), conduit (LAScd) and contraction (LASct), with the latter two phases being valid only for patients in sinus rhythm [104]. Recent studies and meta-analyses have highlighted LA deformation as a potential marker for detecting that population at risk of AF recurrence after ablation [105,106]. Specifically, the CASA-AF study evaluated the three phases of LA deformation in 83 patients with long-term persistent AF before and after ablation. The results showed an improvement in LA function after ablation, with an increase in LASr and restoration of LASct, while impaired LASct after the blanking period appeared to be the only independent predictor of AF recurrence in this population [107]. The recently published ASTRA-AF study examined 9 parameters in 132 patients with paroxysmal and persistent AF who underwent PVI with thermal techniques (RFA/cryoablation), including left atrial deformation (LASr, LAScd, LASct). The only parameter with a statistically significant association with AF recurrence was LASr [108]. Finally, echocardiographically-derived LASr has also been corelated with LA-LVAs, thus being a useful risk stratification tool for post-ablation success outcomes [109]. Figure 2 represents a pathological LA strain analysis from a patient with PAF 24 hours before CA.
One of the most studied indices of left atrial dyssynchrony is the total atrial conduction time (PA-TDI duration). PA-TDI duration is a modern echocardiographic parameter for the assessment of the total atrial conduction time and directly reflects both electrical and structural changes in the atria, therefore the extent of atrial remodeling. The measurement is made in sinus rhythm and is the time interval from the onset of the P wave in lead II of the ECG (onset of electrical depolarization) to the maximum A' wave in tissue Doppler of the lateral wall of the LA (active atrial contraction) [110]. Several studies have shown the correlation of this marker with AF recurrences after ablation [111,112,113,114]. Another indicator of left atrial dyssynchrony is left atrial mechanical dispersion (LA-MD), defined as the standard deviation of the time to maximum positive strain corrected by the R-R interval (SD-TPS, %) [115]. In a study by Sarvari et al., the authors observed that in patients with AF recurrence and normal LA size, the left atrium exhibits significantly greater mechanical dispersion compared with patients after successful CA ablation. Therefore, LA mechanical dispersion may be a useful tool for predicting recurrence in patients with structurally normal hearts [116].
Parameters of diastolic function can be assessed by mitral annular inflow with the use of pulse wave (PW) and tissue Doppler imaging (TDI) and constitute an indirect measurement of LA pressure. Traditional indicators for assessing left ventricular (LV) diastolic dysfunction include are LV septal (e’septal) and lateral(e’lateral) wall velocity, the E/e’ ratio, the LA volume index (LAVi) and the maximum tricuspid velocity. Indicators for assessing filling pressures and the degree of diastolic dysfunction are the E/A ratio, the S/D ratio in the pulmonary veins, the DT, the presence of an L wave and the duration of the Ar/A. Based on the above measurements, left atrial pressure (LAP) can be estimated [117]. Several of the abovementioned markers have been associated with AF recurrence after ablation [118,119,120,121]. In addition, emerging parameters of diastolic dysfunction are currently being considered as predictors of AF recurrence after PVI. One such marker, the left atrioventricular coupling index (LACI), which is the ratio of LA end-diastolic volume to the LV end-diastolic volume has been associated with AF recurrences post-RFA for paroxysmal AF [122]. Finally, the left atrial stiffness index (LASi) as another measure of LA myopathy is a promising parameter in the prediction of AF recurrence after ablation [123]. Measurement by TTE is possible by dividing the E/e’ ratio to peak LA strain. Studies have shown that patients with LVAs on voltage-mapping had increased LASi, especially when these areas were located in the anterior wall of the left atrium [124].
Other echocardiographic indices being explored in the field include mitral and tricuspid valve regurgitation. Many investigators have investigated the possibility that the presence of functional mitral regurgitation (MR) may lead to increased AF recurrences after PVI. A retrospective study of 132 patients reported that functional MR significantly contributes to remodeling of the LA substrate, is associated with LVAs and is also statistically significantly associated with AF recurrence after PVI compared with the absence of regurgitation [125]. The results of the EARNEST-PVI study support this hypothesis, as they concluded that in patients with persistent AF and any degree of mitral valve regurgitation, extended PVI methods were superior to simple PVI in preventing recurrences [126]. Tricuspid regurgitation (TR) has also been highlighted as a possible predictor of AF recurrence after RFA, especially when combined with MR [127,128].
Apart from tricuspid regurgitation, other right heart chamber parameter are currently being investigated in AF recurrence post-catheter ablation. According to the results of a prospective cohort published in 2023, the AF recurrence rate after ablation in patients with paroxysmal atrial fibrillation is closely related to pulmonary artery pressure (PAP) measured by TTE, although this was not reproduced in the case of persistent AF [129]. This association highlights the importance of pulmonary vascular dysfunction in atrial remodeling and its role in the pathogenesis of AF, as the pulmonary veins are the main source of AF initiation. A novel marker of right ventricular-to-pulmonary artery coupling, as measured by the TAPSE/PAP ratio, was shown to be an independent predictor of late recurrence of atrial fibrillation after ablation in a group of 203 patients with persistent AF [130]. The size of the right atrium may also influence ablation outcomes, with reports focusing on right atrial volume (RAV) as a predictor of recurrence [131,132]. A meta-analysis of 12 studies concluded that higher RAV and RAVi increases the risk of AF after RFA [133]. Finally, right ventricular function is nowadays considered a significant parameter in various heart conditions, including AF outcomes. In a total of 164 patients with PAF, persistent of long-standing persistent AF, improvement of RV strain values was noted after RFA, however the absolute change in RV-free wall strain and 4-chamber strain was smaller in patients with AF recurrence, highlighting the importance of RV function in maintaining sinus rhythm [134].
4. Discussion
Despite numerous studies in the recent years regarding AF ablation strategies, prognostic markers and outcomes, major questions around AF recurrence remain unanswered. For example, the recent shortening of the blanking period from 3 months to 8 weeks may be more reflective of the pathophysiological processes occurring after CA and recognize patients in need for adjunctive therapy earlier, therefore offering improved outcomes. However, there are reports suggesting that when ablating with certain technologies, such as pulsed-field (PFA), an even shorter blanking period of one month may be adequate, as patients presenting with ERAF in the second or third month after CA have a high chance of undergoing a redo procedure [136]. Furthermore, as electroporation was not widely used for cardiac arrhythmia ablation up until recently, there is lack of sufficient data regarding AF recurrence predictors after ablation with the specific type of energy.
The future seems promising in the field of predicting recurrences, particularly concerning the incorporation of artificial intelligence (AI) into pre-ablation planning. Recent research suggest that AI-enabled pre-ablation computed tomography (PVCT) combined with clinical variables, can accurately predict AF and demonstrated a notable improvement over traditional predictive method[137]. In addition, AI-ECG algorithms that can effectively analyze ECG data prior to ablation and predict the risk of recurrence have also been described, therefore providing physicians with the ability to develop patient-specific interventions [138]. Machine learning models have proved to be effective or even superior compared to conventional statistical methods in predicting AF recurrence post-ablation, owing to their ability to deploy extensive data to reveal complex patterns and associations, offering deeper understanding of factors related to AF recurrence [139,140]. However, challenges remain, as the inclusivity of all different patient-populations when training machine learning models is sometimes questioned, along with ethical and data safety considerations regarding AI use in clinical practice [141].
Given the novelties in electrocardiographic and echocardiographic parameters, along with the accessibility and widespread use of these diagnostic tools in all kinds of socioeconomic backgrounds, currently existing clinical scores for predicting AF recurrence after CA almost seem outdated. The incorporation of these parameters with basic clinical characteristics in a single predictive model sounds exceptionally promising and could aid into achieving a more personalized therapeutic strategy for all AF patients, depending on their risk for recurrence after CA, thereby improving long-term success of the procedure.
5. Conclusions
Atrial fibrillation recurrence following catheter ablation remains a significant challenge, with clinical, ECG and echocardiographic parameters playing pivotal roles in its prediction. Early recurrences often result from transient procedural effects, whereas late and very late recurrences are more indicative of structural remodeling and pulmonary vein reconnection. While no single predictor is sufficient, the integration of clinical scores, electrocardiographic markers, such as P-wave parameters and left atrial echocardiographic indices, provides promising tools for enhancing prediction accuracy and guiding treatment strategies. Looking ahead, there is a lot of progress to be made on the field. The incorporation of AI is being introduced and a new area of exploration emerges. By advancing predictive tools and embracing innovative technologies, the field is well-positioned to meet these challenges and improve patient treatment strategies and therefore, outcomes.
Author Contributions
A.-E.K., M.T., I.D., A.L., P.T., N.A., A.S. and K. P.: conceptualization, collection of data and writing of the manuscript; A.K., C-K.A.: editing of the manuscript; K.T. and D.T.: supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Van Gelder IC, Rienstra M, Bunting K V, et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): Developed by the task force for the management of atrial fibrillation of the European Society of Ca. Eur Heart J. 2024, 45, 3314–3414. [Google Scholar] [CrossRef] [PubMed]
- Tønnesen J, Ruwald MH, Pallisgaard J, et al. Lower Recurrence Rates of Atrial Fibrillation and MACE Events After Early Compared to Late Ablation: A Danish Nationwide Register Study. J Am Heart Assoc. 2024, 13, e032722. [Google Scholar] [CrossRef] [PubMed]
- Poole JE, Bahnson TD, Monahan KH, et al. Recurrence of Atrial Fibrillation After Catheter Ablation or Antiarrhythmic Drug Therapy in the CABANA Trial. J Am Coll Cardiol. 2020, 75, 3105–3118. [Google Scholar] [CrossRef] [PubMed]
- Tzeis S, Gerstenfeld EP, Kalman J, et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. EP Eur. 2024, 26, euae043. [Google Scholar] [CrossRef]
- Lévy S, Steinbeck G, Santini L, et al. Management of atrial fibrillation: two decades of progress — a scientific statement from the European Cardiac Arrhythmia Society. J Interv Card Electrophysiol. 2022, 65, 287–326. [Google Scholar] [CrossRef]
- Pallisgaard JL, Gislason GH, Hansen J, et al. Temporal trends in atrial fibrillation recurrence rates after ablation between 2005 and 2014: a nationwide Danish cohort study. Eur Heart J. 2018, 39, 442–449. [Google Scholar] [CrossRef]
- Chew DS, Black-Maier E, Loring Z, et al. Diagnosis-to-Ablation Time and Recurrence of Atrial Fibrillation Following Catheter Ablation: A Systematic Review and Meta-Analysis of Observational Studies. Circ Arrhythm Electrophysiol. 2020, 13, e008128. [Google Scholar] [CrossRef]
- El-Harasis MA, Quintana JA, Martinez-Parachini JR, et al. Recurrence After Atrial Fibrillation Ablation and Investigational Biomarkers of Cardiac Remodeling. J Am Heart Assoc. 2024, 13, e031029. [Google Scholar] [CrossRef]
- Musat DL, Milstein NS, Bhatt A, et al. Incidence and Predictors of Very Late Recurrence of Atrial Fibrillation Following Cryoballoon Pulmonary Vein Isolation. Circ Arrhythmia Electrophysiol. 2020, 13, e008646. [Google Scholar] [CrossRef]
- Schwab AC, Anic A, Farkowski MM, et al. Rhythm monitoring, success definition, recurrence, and anticoagulation after atrial fibrillation ablation: results from an EHRA survey. Eur Eur pacing, arrhythmias, Card Electrophysiol J Work groups Card pacing, arrhythmias, Card Cell Electrophysiol Eur Soc Cardiol. 2023, 25, 676–681. [CrossRef]
- Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Hear Rhythm. 2017, 14, e275–e444. [Google Scholar] [CrossRef] [PubMed]
- Erhard N, Metzner A, Fink T. Late arrhythmia recurrence after atrial fibrillation ablation: incidence, mechanisms and clinical implications. Herzschrittmachertherapie + Elektrophysiologie. 2022, 33, 71–76. [Google Scholar] [CrossRef]
- Wei Y, Bao Y, Lin C, et al. Early recurrence after cryoballoon versus radiofrequency ablation for paroxysmal atrial fibrillation: mechanism and implication in long-term outcome. BMC Cardiovasc Disord. 2022, 22, 400. [Google Scholar] [CrossRef]
- Noujaim C, Lim C, Mekhael M, et al. Identifying the prognostic significance of early arrhythmia recurrence during the blanking period and the optimal blanking period duration: insights from the DECAAF II study. Eur Eur pacing, arrhythmias, Card Electrophysiol J Work groups Card pacing, arrhythmias, Card Cell Electrophysiol Eur Soc Cardiol. 2023, 25(6). [CrossRef]
- Davtyan K V, Topchyan AH, Brutyan HA, et al. The predictive role of early recurrences of atrial arrhythmias after pulmonary vein cryoballoon ablation. Is blanking period an outdated concept? Insights from 12-month continuous cardiac monitoring. BMC Cardiovasc Disord. 2021, 21, 483. [Google Scholar] [CrossRef]
- Popa MA, Kottmaier M, Risse E, et al. Early arrhythmia recurrence after catheter ablation for persistent atrial fibrillation: is it predictive for late recurrence? Clin Res Cardiol. 2022, 111, 85–95. [CrossRef]
- Liang JJ, Elafros MA, Chik WW, et al. Early recurrence of atrial arrhythmias following pulmonary vein antral isolation: Timing and frequency of early recurrences predicts long-term ablation success. Hear Rhythm. 2015, 12, 2461–2468. [Google Scholar] [CrossRef]
- Steinberg C, Champagne J, Deyell MW, et al. Prevalence and outcome of early recurrence of atrial tachyarrhythmias in the Cryoballoon vs Irrigated Radiofrequency Catheter Ablation (CIRCA-DOSE) study. Hear Rhythm. 2021, 18, 1463–1470. [Google Scholar] [CrossRef]
- Iqbal SUR, Kueffer T, Knecht S, et al. Impact of shortening the blanking period to 8 weeks after PVI: Insights from COMPARE-CRYO using continuous rhythm monitoring. Hear Rhythm. December, 20 December. [CrossRef]
- Mainigi SK, Sauer WH, Cooper JM, et al. Incidence and predictors of very late recurrence of atrial fibrillation after ablation. J Cardiovasc Electrophysiol. 2007, 18, 69–74. [Google Scholar] [CrossRef]
- Themistoclakis S, Schweikert RA, Saliba WI, et al. Clinical predictors and relationship between early and late atrial tachyarrhythmias after pulmonary vein antrum isolation. Hear Rhythm. 2008, 5, 679–685. [Google Scholar] [CrossRef]
- Mo P, Fan C, Chen J, et al. Atrial Fibrillation Types and Chronic Kidney Disease are Independent Predictors of Atrial Fibrillation Recurrence After Radiofrequency Ablation. Ther Clin Risk Manag. 2024, 20, 817–828. [Google Scholar] [CrossRef]
- Farghaly AAA, Ali H, Lupo P, et al. Early versus Late Radiofrequency Catheter Ablation in Atrial Fibrillation: Timing Matters. J Clin Med. [CrossRef]
- De Greef Y, Bogaerts K, Sofianos D, Buysschaert I. Impact of Diagnosis-to-Ablation Time on AF Recurrence: Pronounced the First 3 Years, Irrelevant Thereafter. JACC Clin Electrophysiol. 2023, 9, 2263–2272. [Google Scholar] [CrossRef] [PubMed]
- Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024, 149, e1–e156. [Google Scholar] [CrossRef]
- Tabaja C, Younis A, Santangeli P, et al. Catheter ablation of atrial fibrillation in elderly and very elderly patients: safety, outcomes, and quality of life. J Interv Card Electrophysiol. 2024, 67, 1083–1092. [Google Scholar] [CrossRef]
- Kozhuharov N, Karim N, Creta A, et al. Long-term outcomes of catheter ablation for atrial fibrillation in octogenarians. J Interv Card Electrophysiol an Int J Arrhythm pacing. August, 20 August. [CrossRef]
- Li H, Wang Z, Cheng Z, et al. Sex differences involved in persistent atrial fibrillation recurrence after radiofrequency ablation. BMC Cardiovasc Disord. 2022, 22, 549. [Google Scholar] [CrossRef]
- Bukari A, Nayak H, Aziz Z, Deshmukh A, Tung R, Ozcan C. Impact of race and gender on clinical outcomes of catheter ablation in patients with atrial fibrillation. Pacing Clin Electrophysiol. 2017, 40, 1073–1079. [Google Scholar] [CrossRef]
- Li M, Liu T, Luo D, Li G. Systematic review and meta-analysis of chronic kidney disease as predictor of atrial fibrillation recurrence following catheter ablation. Cardiol J. 2014, 21, 89–95. [Google Scholar] [CrossRef]
- Lee W-C, Wu P-J, Fang C-Y, Chen H-C, Chen M-C. Impact of chronic kidney disease on atrial fibrillation recurrence following radiofrequency and cryoballoon ablation: A meta-analysis. Int J Clin Pract. 2021, 75, e14173. [Google Scholar] [CrossRef]
- Yamashita S, Tokuda M, Matsuo S, et al. Comparison of atrial arrhythmia recurrence after persistent atrial fibrillation ablation between patients with or without tachycardia-induced cardiomyopathy. J Cardiovasc Electrophysiol. 2019, 30, 2310–2318. [Google Scholar] [CrossRef]
- Tan NY, Mohsin Y, Hodge DO, et al. Catheter Ablation for Atrial Arrhythmias in Patients With Cardiac Amyloidosis. J Cardiovasc Electrophysiol. 2016, 27, 1167–1173. [Google Scholar] [CrossRef]
- Barbhaiya CR, Kumar S, Baldinger SH, et al. Electrophysiologic assessment of conduction abnormalities and atrial arrhythmias associated with amyloid cardiomyopathy. Hear Rhythm. 2016, 13, 383–390. [Google Scholar] [CrossRef]
- Hiraya D, Sato A, Hoshi T, et al. Impact of coronary artery disease and revascularization on recurrence of atrial fibrillation after catheter ablation: Importance of ischemia in managing atrial fibrillation. J Cardiovasc Electrophysiol. 2019, 30, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Lador A, Maccioni S, Khanna R, Zhang D. Influence of time to ablation on outcomes among patients with atrial fibrillation with pre-existing heart failure. Hear Rhythm O2 2024, 5, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Ando M, Yanagisawa S, Suzuki H, et al. Early Cryoablation After First Diagnosis of Atrial Fibrillation Reduces Arrhythmia Recurrence in Heart Failure Patients. JACC Asia. 2024, 4, 857–871. [Google Scholar] [CrossRef] [PubMed]
- Seewöster T, Kosich F, Sommer P, Bertagnolli L, Hindricks G, Kornej J. Prediction of low-voltage areas using modified APPLE score. EP Eur. 2021, 23, 575–580. [Google Scholar] [CrossRef]
- Xin Y, Hang F, Wu Y. Predictors of Low Voltage Zone and Sex Differences in Low Voltage Zone Distribution in Patients with Atrial Fibrillation. Rev Cardiovasc Med. 2023, 24, 324. [Google Scholar] [CrossRef]
- Ribo T, Jianzeng D, Xiaohui L, et al. [Impact of CHA2DS2 VASc score on substrate for persistent atrial fibrillation and outcome post catheter ablation of atrial fibrillation]. Zhonghua Xin Xue Guan Bing Za Zhi 2015, 43, 695–699. [Google Scholar]
- Kornej J, Hindricks G, Kosiuk J, et al. Comparison of CHADS2, R2CHADS2, and CHA2DS2-VASc scores for the prediction of rhythm outcomes after catheter ablation of atrial fibrillation: the Leipzig Heart Center AF Ablation Registry. Circ Arrhythm Electrophysiol. 2014, 7, 281–287. [Google Scholar] [CrossRef]
- Kornej J, Schumacher K, Dinov B, et al. Prediction of electro-anatomical substrate and arrhythmia recurrences using APPLE, DR-FLASH and MB-LATER scores in patients with atrial fibrillation undergoing catheter ablation. Sci Rep. 2018, 8, 12686. [Google Scholar] [CrossRef]
- Sano M, Heeger C-H, Sciacca V, et al. Evaluation of predictive scores for late and very late recurrence after cryoballoon-based ablation of atrial fibrillation. J Interv Card Electrophysiol an Int J Arrhythm pacing. 2021, 61, 321–332. [Google Scholar] [CrossRef]
- Han J, Li G, Zhang D, Wang X, Guo X. Predicting Late Recurrence of Atrial Fibrillation After Radiofrequency Ablation in Patients With Atrial Fibrillation: Comparison of C2HEST and HATCH Scores. Front Cardiovasc Med. 2022, 9, 907817. [Google Scholar] [CrossRef]
- Kosiuk J, Dinov B, Kornej J, et al. Prospective, multicenter validation of a clinical risk score for left atrial arrhythmogenic substrate based on voltage analysis: DR-FLASH score. Hear Rhythm. 2015, 12, 2207–2212. [Google Scholar] [CrossRef] [PubMed]
- Sato T, Sotomi Y, Hikoso S, et al. DR-FLASH Score Is Useful for Identifying Patients With Persistent Atrial Fibrillation Who Require Extensive Catheter Ablation Procedures. J Am Heart Assoc. 2022, 11, e024916. [Google Scholar] [CrossRef] [PubMed]
- Bisbal F, Alarcón F, Ferrero-de-Loma-Osorio A, et al. Left atrial geometry and outcome of atrial fibrillation ablation: results from the multicentre LAGO-AF study. Eur Hear J - Cardiovasc Imaging. 2018, 19, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Kosich F, Schumacher K, Potpara T, Lip GY, Hindricks G, Kornej J. Clinical scores used for the prediction of negative events in patients undergoing catheter ablation for atrial fibrillation. Clin Cardiol. 2019, 42, 320–329. [Google Scholar] [CrossRef]
- Kornej J, Hindricks G, Shoemaker MB, et al. The APPLE score: a novel and simple score for the prediction of rhythm outcomes after catheter ablation of atrial fibrillation. Clin Res Cardiol. 2015, 104, 871–876. [Google Scholar] [CrossRef]
- Mujović N, Marinković M, Marković N, Shantsila A, Lip GYH, Potpara TS. Prediction of very late arrhythmia recurrence after radiofrequency catheter ablation of atrial fibrillation: The MB-LATER clinical score. Sci Rep. 2017, 7, 40828. [Google Scholar] [CrossRef]
- Akkaya E, Berkowitsch A, Greiss H, et al. PLAAF score as a novel predictor of long-term outcome after second-generation cryoballoon pulmonary vein isolation. EP Eur. 2018, 20, f436–f443. [Google Scholar] [CrossRef]
- Canpolat U, Aytemir K, Yorgun H, Şahiner L, Kaya EB, Oto A. A proposal for a new scoring system in the prediction of catheter ablation outcomes: Promising results from the Turkish Cryoablation Registry. Int J Cardiol. 2013, 169, 201–206. [Google Scholar] [CrossRef]
- Mesquita J, Ferreira AM, Cavaco D, et al. Development and validation of a risk score for predicting atrial fibrillation recurrence after a first catheter ablation procedure – ATLAS score. EP Eur. 2018, 20, f428–f435. [Google Scholar] [CrossRef]
- Winkle RA, Jarman JWE, Mead RH, et al. Predicting atrial fibrillation ablation outcome: The CAAP-AF score. Hear Rhythm. 2016, 13, 2119–2125. [Google Scholar] [CrossRef]
- Sanhoury M, Moltrasio M, Tundo F, et al. Predictors of arrhythmia recurrence after balloon cryoablation of atrial fibrillation: the value of CAAP-AF risk scoring system. J Interv Card Electrophysiol. 2017, 49, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Peigh G, Kaplan RM, Bavishi A, et al. A novel risk model for very late return of atrial fibrillation beyond 1 year after cryoballoon ablation: the SCALE-CryoAF score. J Interv Card Electrophysiol an Int J Arrhythm pacing. 2020, 58, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Luo Y, Tang Y, Huang W, Xiong S, Long Y, Liu H. Age, creatinine, and ejection fraction (ACEF) score as predictive values for late non-valvular atrial fibrillation recurrence after radiofrequency ablation. Clin Exp Hypertens. 2023, 45, 2207784. [Google Scholar] [CrossRef]
- Chen LY, Ribeiro ALP, Platonov PG, et al. P Wave Parameters and Indices: A Critical Appraisal of Clinical Utility, Challenges, and Future Research—A Consensus Document Endorsed by the International Society of Electrocardiology and the International Society for Holter and Noninvasive Electrocardio. Circ Arrhythmia Electrophysiol. 2022, 15, e010435. [Google Scholar] [CrossRef]
- Intzes S, Zagoridis K, Symeonidou M, et al. P-wave duration and atrial fibrillation recurrence after catheter ablation: a systematic review and meta-analysis. Eur Eur pacing, arrhythmias, Card Electrophysiol J Work groups Card pacing, arrhythmias, Card Cell Electrophysiol Eur Soc Cardiol. 2023, 25, 450–459. [Google Scholar] [CrossRef]
- Bayés de Luna A, Escobar-Robledo LA, Aristizabal D, et al. Atypical advanced interatrial blocks: Definition and electrocardiographic recognition. J Electrocardiol. 2018, 51, 1091–1093. [Google Scholar] [CrossRef]
- Pranata R, Yonas E, Vania R. Prolonged P-wave duration in sinus rhythm pre-ablation is associated with atrial fibrillation recurrence after pulmonary vein isolation-A systematic review and meta-analysis. Ann noninvasive Electrocardiol Off J Int Soc Holter Noninvasive Electrocardiology, Inc. 2019, 24, e12653. [Google Scholar] [CrossRef]
- Koutalas E, Kallergis E, Nedios S, Kochiadakis G, Kanoupakis E. P-wave duration as a marker of atrial remodeling in patients referred to ablation for atrial fibrillation: A new stratification tool emerging? Hell J Cardiol. 2023, 73, 53–60. [Google Scholar] [CrossRef]
- MORRIS JJJ, ESTES EHJ, WHALEN RE, THOMPSON HKJ, MCINTOSH HD. P-WAVE ANALYSIS IN VALVULAR HEART DISEASE. Circulation 1964, 29, 242–252. [Google Scholar] [CrossRef]
- Tiffany Win T, Ambale Venkatesh B, Volpe GJ, et al. Associations of electrocardiographic P-wave characteristics with left atrial function, and diffuse left ventricular fibrosis defined by cardiac magnetic resonance: The PRIMERI Study. Hear Rhythm. 2015, 12, 155–162. [Google Scholar] [CrossRef]
- Qiu Y, Sun J, Wang Y, et al. Association between P-wave terminal force in lead V(1) and extent of left atrial low-voltage substrate in older patients with paroxysmal atrial fibrillation. J Interv Card Electrophysiol an Int J Arrhythm pacing. 2024, 67, 1153–1160. [Google Scholar] [CrossRef]
- Huang Z, Zheng Z, Wu B, et al. Predictive value of P wave terminal force in lead V1 for atrial fibrillation: A meta-analysis. Ann noninvasive Electrocardiol Off J Int Soc Holter Noninvasive Electrocardiology, Inc. 2020, 25, e12739. [Google Scholar] [CrossRef] [PubMed]
- Sudo Y, Morimoto T, Tsushima R, et al. P-wave terminal force in lead V1 and outcomes in patients with persistent atrial fibrillation undergoing catheter ablation. Am Heart J. 2023, 260, 141–150. [Google Scholar] [CrossRef]
- Wang Z, Wang B, Yang Y, Yang X, Che Y, Xia Y. P-wave terminal force in lead V1 is associated with recurrence after catheter ablation in patients with paroxysmal atrial fibrillation and normal left atrial size. Front Cardiovasc Med. 2024, 11, 1467585. [Google Scholar] [CrossRef]
- Wakabayashi Y, Uesako H, Kobayashi M, Ichikawa T, Koyama T, Abe H. P-wave terminal force is related to left pulmonary vein reconnection in patients with atrial fibrillation recurrence after pulmonary vein isolation. Heart Vessels. September, 20 September. [CrossRef]
- Dilaveris P, Batchvarov V, Gialafos J, Malik M. Comparison of different methods for manual P wave duration measurement in 12-lead electrocardiograms. Pacing Clin Electrophysiol. 1999, 22, 1532–1538. [Google Scholar] [CrossRef]
- Chávez-González E, Donoiu I. Utility of P-Wave Dispersion in the Prediction of Atrial Fibrillation. Curr Heal Sci J. 2017, 43, 5–11. [Google Scholar] [CrossRef]
- Pérez-Riera AR, de Abreu LC, Barbosa-Barros R, Grindler J, Fernandes-Cardoso A, Baranchuk A. P-wave dispersion: an update. Indian Pacing Electrophysiol J. 2016, 16, 126–133. [Google Scholar] [CrossRef]
- Perez M V, Dewey FE, Marcus R, et al. Electrocardiographic predictors of atrial fibrillation. Am Heart J. 2009, 158, 622–628. [Google Scholar] [CrossRef]
- Liu P, Lv T, Yang Y, Gao Q, Zhang P. Use of P wave indices to evaluate efficacy of catheter ablation and atrial fibrillation recurrence: a systematic review and meta-analysis. J Interv Card Electrophysiol. 2022, 65, 827–840. [Google Scholar] [CrossRef]
- Kizilirmak F, Demir GG, Gokdeniz T, et al. Changes in Electrocardiographic P Wave Parameters after Cryoballoon Ablation and Their Association with Atrial Fibrillation Recurrence. Ann noninvasive Electrocardiol Off J Int Soc Holter Noninvasive Electrocardiology, Inc. 2016, 21, 580–587. [Google Scholar] [CrossRef]
- Doğduş M, Turan OE, Başkurt AA, et al. An Effective Novel Index for Predicting the Recurrence of Atrial Fibrillation Ablation: P Wave Duration-to-Amplitude Ratio. Turk Kardiyol Dern Ars. 2022, 50, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Zhang ZR, Ragot D, Massin SZ, et al. P-Wave Duration/Amplitude Ratio Quantifies Atrial Low-Voltage Area and Predicts Atrial Arrhythmia Recurrence After Pulmonary Vein Isolation. Can J Cardiol. 2023, 39, 1421–1431. [Google Scholar] [CrossRef]
- Maheshwari A, Norby FL, Soliman EZ, et al. Refining Prediction of Atrial Fibrillation Risk in the General Population With Analysis of P-Wave Axis (from the Atherosclerosis Risk in Communities Study). Am J Cardiol. 2017, 120, 1980–1984. [Google Scholar] [CrossRef]
- Dhaliwal KK, Upadhya B, Soliman EZ, et al. Association of P-Wave Axis With Incident Atrial Fibrillation in Diabetes Mellitus (from the ACCORD Trial). Am J Cardiol. 2020, 128, 191–195. [Google Scholar] [CrossRef]
- Salah A, Zhou S, Liu Q, Yan H. P wave indices to predict atrial fibrillation recurrences post pulmonary vein isolation. Arq Bras Cardiol. 2013, 101, 519–527. [Google Scholar] [CrossRef]
- Wakatsuki D, Asano T, Mase H, Kurata M, Onuki T, Suzuki H. The characteristic of an abnormal p-wave axis in patients with atrial fibrillation. J Electrocardiol. 2022, 73, 1–7. [Google Scholar] [CrossRef]
- Okuyama T, Kabutoya T, Kario K. Notched P-wave on digital electrocardiogram predicts the recurrence of atrial fibrillation in patients who have undergone catheter ablation. J Arrhythmia. 2024, 40, 472–478. [Google Scholar] [CrossRef]
- Yanagisawa S, Inden Y, Okamoto H, et al. Electrocardiogram characteristics of P wave associated with successful pulmonary vein isolation in patients with paroxysmal atrial fibrillation: Significance of changes in P-wave duration and notched P wave. Ann noninvasive Electrocardiol Off J Int Soc Holter Noninvasive Electrocardiology, Inc. 2020, 25, e12712. [Google Scholar] [CrossRef]
- Ehrlich JR, Zhang GQ, Israel CW, Hohnloser SH. [P-wave signal averaging-ECG: normal values and reproducibility]. Z Kardiol. 2001, 90, 170–176. [Google Scholar] [CrossRef]
- Yugo D, Kuo M-J, Hu Y-F, et al. Dynamic changes in signal-averaged P wave after catheter ablation of atrial fibrillation. J Chinese Med Assoc. /: https, 2022.
- Aytemir K, Aksoyek S, Yildirir A, Ozer N, Oto A. Prediction of atrial fibrillation recurrence after cardioversion by P wave signal-averaged electrocardiography11This study was presented as an oral presentation at NASPE’s 19th Annual Scientific Sessions, San Diego, May 6–9, 1998. Int J Cardiol. 1999, 70, 15–21. [Google Scholar] [CrossRef]
- Okumura Y, Watanabe I, Ohkubo K, et al. Prediction of the efficacy of pulmonary vein isolation for the treatment of atrial fibrillation by the signal-averaged P-wave duration. Pacing Clin Electrophysiol. 2007, 30, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Tang R-B, Lv W-H, Long D-Y, et al. Catheter ablation of atrial fibrillation in patients with left bundle branch block. Pacing Clin Electrophysiol. 2024, 47, 518–524. [Google Scholar] [CrossRef]
- Yano M, Egami Y, Ukita K, et al. Impact of Baseline Right Bundle Branch Block on Outcomes After Pulmonary Vein Isolation in Patients With Atrial Fibrillation. Am J Cardiol. 2021, 144, 60–66. [Google Scholar] [CrossRef]
- Wang L, Yang G, Cui C, et al. The feasibility of atrial Fibrillatory wave amplitude in predicting ablation outcomes in persistent atrial fibrillation. J Electrocardiol. 2024, 86, 153766. [Google Scholar] [CrossRef]
- Hunuk B, de Asmundis C, Mugnai G, et al. Early repolarization pattern as a predictor of atrial fibrillation recurrence following radiofrequency pulmonary vein isolation. Ann noninvasive Electrocardiol Off J Int Soc Holter Noninvasive Electrocardiology, Inc. 2019, 24, e12627. [Google Scholar] [CrossRef]
- Wen S-N, Zhu H-J, Sun P-Y, et al. Depolarization and repolarization parameters on ECG predict recurrence after atrial fibrillation ablation in patients with hypertrophic cardiomyopathy. J Cardiovasc Electrophysiol. 2019, 30, 2405–2413. [Google Scholar] [CrossRef]
- Wazni OM, Tsao H-M, Chen S-A, et al. Cardiovascular imaging in the management of atrial fibrillation. J Am Coll Cardiol. 2006, 48, 2077–2084. [Google Scholar] [CrossRef]
- Zhao Z, Zhang F, Ma R, et al. Development and Validation of a Risk Nomogram Model for Predicting Recurrence in Patients with Atrial Fibrillation After Radiofrequency Catheter Ablation. Clin Interv Aging. 2022, 17, 1405–1421. [Google Scholar] [CrossRef]
- Lee H-L, Hwang Y-T, Chang P-C, Wen M-S, Chou C-C. A three-year longitudinal study of the relation between left atrial diameter remodeling and atrial fibrillation ablation outcome. J Geriatr Cardiol. 2018, 15, 486–491. [Google Scholar] [CrossRef]
- Taylan G, Gök M, Kurtul A, et al. Integrating the Left Atrium Diameter to Improve the Predictive Ability of the Age, Creatinine, and Ejection Fraction Score for Atrial Fibrillation Recurrence After Cryoballoon Ablation. Anatol J Cardiol. 2023, 27, 567–572. [Google Scholar] [CrossRef]
- Zhuang J, Wang Y, Tang K, et al. Association between left atrial size and atrial fibrillation recurrence after single circumferential pulmonary vein isolation: a systematic review and meta-analysis of observational studies. EP Eur. 2012, 14, 638–645. [Google Scholar] [CrossRef]
- Njoku A, Kannabhiran M, Arora R, et al. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: a meta-analysis. Eur Eur pacing, arrhythmias, Card Electrophysiol J Work groups Card pacing, arrhythmias, Card Cell Electrophysiol Eur Soc Cardiol. 2018, 20, 33–42. [Google Scholar] [CrossRef]
- Kranert M, Shchetynska-Marinova T, Liebe V, et al. Recurrence of Atrial Fibrillation in Dependence of Left Atrial Volume Index. In Vivo 2020, 34, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Sanna G, Moccia E, Canonico ME, et al. Left atrial remodeling in heart failure: the role of sphericity index (the SPHERICAT-HF study). Int J Cardiovasc Imaging. [CrossRef]
- Shi J, Xu S, Chen L, et al. Impact of Left Atrial Sphericity Index on the Outcome of Catheter Ablation for Atrial Fibrillation. J Cardiovasc Transl Res. 2021, 14, 912–920. [Google Scholar] [CrossRef]
- Olsen FJ, Christensen LM, Krieger DW, et al. Relationship between left atrial strain, diastolic dysfunction and subclinical atrial fibrillation in patients with cryptogenic stroke: the SURPRISE echo substudy. Int J Cardiovasc Imaging. 2020, 36, 79–89. [Google Scholar] [CrossRef]
- Morris DA, Parwani A, Huemer M, et al. Clinical Significance of the Assessment of the Systolic and Diastolic Myocardial Function of the Left Atrium in Patients With Paroxysmal Atrial Fibrillation and Low CHADS2 Index Treated With Catheter Ablation Therapy. Am J Cardiol. 2013, 111, 1002–1011. [Google Scholar] [CrossRef]
- Badano LP, Kolias TJ, Muraru D, et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: a consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur Hear J - Cardiovasc Imaging. 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Li Y, Li Y, Sun L, et al. Left atrial strain for predicting recurrence in patients with non-valvular atrial fibrillation after catheter ablation: a single-center two-dimensional speckle tracking retrospective study. BMC Cardiovasc Disord. 2022, 22, 468. [Google Scholar] [CrossRef]
- Ma X-X, Boldt L-H, Zhang Y-L, et al. Clinical Relevance of Left Atrial Strain to Predict Recurrence of Atrial Fibrillation after Catheter Ablation: A Meta-Analysis. Echocardiography. 2016, 33, 724–733. [Google Scholar] [CrossRef]
- Khan HR, Yakupoglu HY, Kralj-Hans I, et al. Left Atrial Function Predicts Atrial Arrhythmia Recurrence Following Ablation of Long-Standing Persistent Atrial Fibrillation. Circ Cardiovasc Imaging. 2023, 16, e015352. [Google Scholar] [CrossRef]
- Knappe D, Vogler J, Weimann J, et al. Left Atrial Reservoir Strain and Recurrence of Atrial Fibrillation Following De-Novo Pulmonary Vein Isolation - Results of the ASTRA-AF Pilot Study. Circ J. June, 20 June. [CrossRef]
- Chang S, Zhang X, Ge C, et al. Automatic Echocardiographic Assessment of Left Atrial Function for Prediction of Low-Voltage Areas in Non-Valvular Atrial Fibrillation. Int J Gen Med. 2024, 17, 4493–4506. [Google Scholar] [CrossRef] [PubMed]
- Müller P, Weijs B, Bemelmans NMAA, et al. Echocardiography-derived total atrial conduction time (PA-TDI duration): risk stratification and guidance in atrial fibrillation management. Clin Res Cardiol. 2021, 110, 1734–1742. [Google Scholar] [CrossRef] [PubMed]
- den Uijl DW, Gawrysiak M, Tops LF, et al. Prognostic value of total atrial conduction time estimated with tissue Doppler imaging to predict the recurrence of atrial fibrillation after radiofrequency catheter ablation. EP Eur. 2011, 13, 1533–1540. [Google Scholar] [CrossRef]
- Evranos B, Aytemir K, Oto A, et al. Predictors of atrial fibrillation recurrence after atrial fibrillation ablation with cryoballoon. Cardiol J. 2013, 20, 294–303. [Google Scholar] [CrossRef]
- Ejima K, Kato K, Arai K, et al. Impact of Atrial Remodeling on the Outcome of Radiofrequency Catheter Ablation of Paroxysmal Atrial Fibrillation. Circ J. 2014, 78, 872–877. [Google Scholar] [CrossRef]
- Fukushima K, Fukushima N, Ejima K, et al. Left Atrial Appendage Flow Velocity and Time from P-Wave Onset to Tissue Doppler–Derived A’ Predict Atrial Fibrillation Recurrence after Radiofrequency Catheter Ablation. Echocardiography 2015, 32, 1101–1108. [Google Scholar] [CrossRef]
- Shang Z, Su D, Cong T, et al. Assessment of left atrial mechanical function and synchrony in paroxysmal atrial fibrillation with two-dimensional speckle tracking echocardiography. Echocardiography. 2017, 34, 176–183. [Google Scholar] [CrossRef]
- Sarvari SI, Haugaa KH, Stokke TM, et al. Strain echocardiographic assessment of left atrial function predicts recurrence of atrial fibrillation. Eur Hear J - Cardiovasc Imaging. 2016, 17, 660–667. [Google Scholar] [CrossRef]
- Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Masuda M, Fujita M, Iida O, et al. An E/e′ ratio on echocardiography predicts the existence of left atrial low-voltage areas and poor outcomes after catheter ablation for atrial fibrillation. EP Eur. 2018, 20, e60–e68. [Google Scholar] [CrossRef]
- Gong K-Z, Yan Q-D, Huang R-D, et al. The impact of echocardiographic parameter ratio of E/E’ on the late recurrence paroxysmal atrial fibrillation in patients accepted radiofrequency catheter ablation: A retrospective clinical study. Medicine 2020, 99, e19897. [Google Scholar] [CrossRef]
- Wada R, Shinohara M, Fujino T, et al. Significance of mitral L-waves in predicting late recurrences of atrial fibrillation after radiofrequency catheter ablation. Pacing Clin Electrophysiol. 2023, 46, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Kosiuk J, Breithardt O-A, Bode K, et al. The predictive value of echocardiographic parameters associated with left ventricular diastolic dysfunction on short- and long-term outcomes of catheter ablation of atrial fibrillation. EP Eur. 2014, 16, 1168–1174. [Google Scholar] [CrossRef]
- Li A, Zhang M, Ning B. Predictive value of the left atrioventricular coupling index for recurrence after radiofrequency ablation of paroxysmal atrial fibrillation. J Cardiothorac Surg. 2024, 19, 552. [Google Scholar] [CrossRef]
- Khurram IM, Maqbool F, Berger RD, et al. Association Between Left Atrial Stiffness Index and Atrial Fibrillation Recurrence in Patients Undergoing Left Atrial Ablation. Circ Arrhythm Electrophysiol. [CrossRef]
- Kishima H, Mine T, Fukuhara E, Ashida K, Ishihara M. The association between left atrial stiffness and low-voltage areas of left atrium in patients with atrial fibrillation. Heart Vessels. 2019, 34, 1830–1838. [Google Scholar] [CrossRef]
- Qiao Y, Wu L, Hou B, et al. Functional mitral regurgitation: predictor for atrial substrate remodeling and poor ablation outcome in paroxysmal atrial fibrillation. Medicine (Baltimore). /: https, 2016.
- Sunaga A, Matsuoka Y, Nakatani D, et al. Extensive ablation for persistent atrial fibrillation patients with mitral regurgitation: Insights from the EARNEST-PVI prospective randomized trial. Int J Cardiol. 2024, 410, 132231. [Google Scholar] [CrossRef]
- Zhao Y, Zhao L, Huang Q, et al. Nomogram to predict recurrence risk factors in patients with non-valvular paroxysmal atrial fibrillation after catheter radiofrequency ablation. Echocardiography. 2024, 41, e15779. [Google Scholar] [CrossRef]
- Nakamura K, Takagi T, Kogame N, et al. Impact of atrial mitral and tricuspid regurgitation on atrial fibrillation recurrence after ablation. J Electrocardiol. 2021, 66, 114–121. [Google Scholar] [CrossRef]
- Choi YY, Choi J-I, Jeong JH, et al. Impact of pulmonary artery pressure on recurrence after catheter ablation in patients with atrial fibrillation. Front Cardiovasc Med. 2023, 10, 1187774. [Google Scholar] [CrossRef]
- Yano M, Egami Y, Ukita K, et al. Clinical impact of right ventricular-pulmonary artery uncoupling on predicting the clinical outcomes after catheter ablation in persistent atrial fibrillation patients. Int J Cardiol Hear Vasc. 2022, 39, 100991. [Google Scholar] [CrossRef]
- Moon J, Jin Hong Y, Shim J, et al. Right Atrial Anatomical Remodeling Affects Early Outcomes of Nonvalvular Atrial Fibrillation After Radiofrequency Ablation. Circ J. 2012, 76, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Akutsu Y, Kaneko K, Kodama Y, et al. Association between left and right atrial remodeling with atrial fibrillation recurrence after pulmonary vein catheter ablation in patients with paroxysmal atrial fibrillation: a pilot study. Circ Cardiovasc Imaging. 2011, 4, 524–531. [Google Scholar] [CrossRef]
- Han J-M, Xie Q, Song X-Y, Ma Y-L. Right atrial volume index and right atrial volume predict atrial fibrillation recurrence: A meta-analysis. PLoS One 2024, 19, e0315590. [Google Scholar] [CrossRef]
- Kim M, Uhm J-S, Park J-W, et al. The Effects of Radiofrequency Catheter Ablation for Atrial Fibrillation on Right Ventricular Function. Korean Circ J. 2024, 54, 203–217. [Google Scholar] [CrossRef]
- Pathan F, D’Elia N, Nolan MT, Marwick TH, Negishi K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J Am Soc Echocardiogr. 2017, 30, 59–70.e8. [Google Scholar] [CrossRef]
- Mohanty S, Torlapati PG, Casella M, et al. Redefining the blanking period after pulsed-field ablation in patients with atrial fibrillation. Hear Rhythm. August, 20 August. [CrossRef]
- Liu C-M, Chen W-S, Chang S-L, et al. Use of artificial intelligence and I-Score for prediction of recurrence before catheter ablation of atrial fibrillation. Int J Cardiol. 2024, 402, 131851. [Google Scholar] [CrossRef]
- Jiang J, Deng H, Liao H, et al. An Artificial Intelligence-Enabled ECG Algorithm for Predicting the Risk of Recurrence in Patients with Paroxysmal Atrial Fibrillation after Catheter Ablation. J Clin Med. [CrossRef]
- Sun S, Wang L, Lin J, Sun Y, Ma C. An effective prediction model based on XGBoost for the 12-month recurrence of AF patients after RFA. BMC Cardiovasc Disord. 2023, 23, 561. [Google Scholar] [CrossRef]
- Fan X, Li Y, He Q, et al. Predictive Value of Machine Learning for Recurrence of Atrial Fibrillation after Catheter Ablation: A Systematic Review and Meta-Analysis. Rev Cardiovasc Med. 2023, 24, 315. [Google Scholar] [CrossRef]
- Truong ET, Lyu Y, Ihdayhid AR, Lan NSR, Dwivedi G. Beyond Clinical Factors: Harnessing Artificial Intelligence and Multimodal Cardiac Imaging to Predict Atrial Fibrillation Recurrence Post-Catheter Ablation. J Cardiovasc Dev Dis. [CrossRef]
Figure 2.
Abnormal left atrial strain parameters by 2D-STE in a 44-year old male patient with paroxysmal atrial fibrillation. TTE was performed 24 hours before pulmonary vein isolation with Pulsed-Field Ablation.
Figure 2.
Abnormal left atrial strain parameters by 2D-STE in a 44-year old male patient with paroxysmal atrial fibrillation. TTE was performed 24 hours before pulmonary vein isolation with Pulsed-Field Ablation.
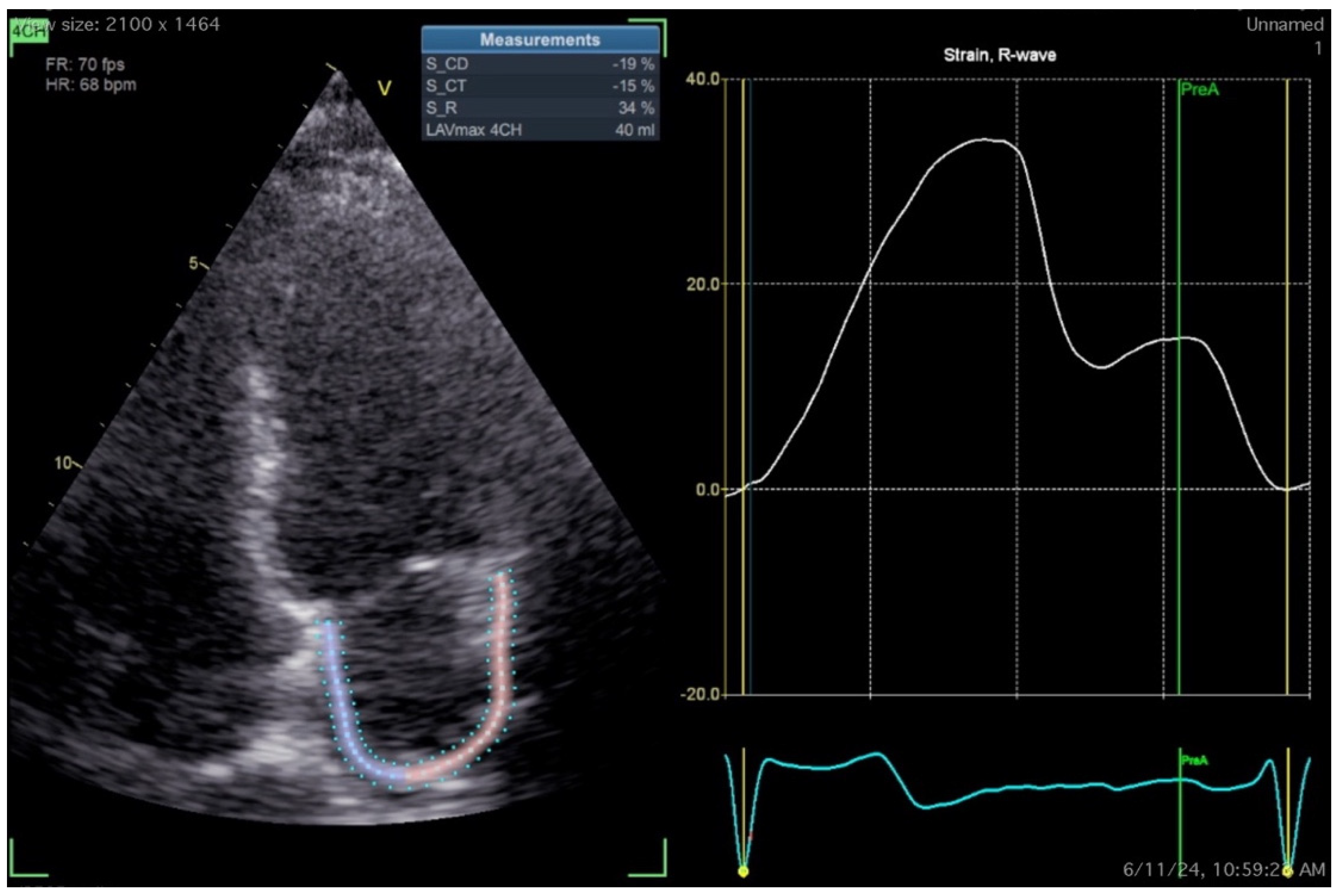

Table 1.
Commonly used clinical scores to predict atrial fibrillation recurrence after catheter ablation.
Table 1.
Commonly used clinical scores to predict atrial fibrillation recurrence after catheter ablation.
| Score | Parameters included | ||||||
|---|---|---|---|---|---|---|---|
| CHADS2 | CHF | Age≥75 | DM | TIA/Stroke | |||
| CHA2DS2-VASc [41] | CHF | Age≥75 | DM | TIA/Stroke | Vascular disease | Age≥65 | Female |
| R2CHADS2 [41] | CHF | Age≥75 | DM | TIA/Stroke | Renal dysfunction | ||
| APPLE [49] | Age > 65 | Persistent AF | eGFR< 60 | LAD≥43mm | LVEF < 50% | ||
| MB-LATER [50] | Male | BBB on ECG | LAD>47mm | ERAF | Persistent AF | ||
| C2HEST [44] | CAD/COPD | HTN | Age >75 | HF | Thyroid disease | ||
| HATCH [44] | HTN | Age≥75 | TIA/Stroke | COPD | HF | ||
| DR-FLASH [45] | DM | CKD | Persistent AF | LAD>45mm | Age>65 | Female | HTN |
| PLAAF [51] | Persistent AF | LA area | Abnormal PV anatomy | AF history | Female | ||
| BASE-AF2 [52] | BMI>28 | LAD>40mm | Smoking | ERAF | AF duration>6 years | Non-PAF | |
| ATLAS [53] | Age > 60 | Female | Non-PAF | Smoking | LAVi | ||
| CAAP-AF [54,55] | CAD | LAD>40 | Age>50 | Persistent AF | AADs failure | Female | |
| SCALE-CryoAF [56] | SHD | CAD | LAD>43mm | LBBB | ERAF | Non-PAF | |
| LAGO [47] | SHD | AF type | CHA2DS2-VASc ≤ 1 | LAD>40mm | LA sphericity | ||
| ACEF [57] | Age | Creatinine | LVEF | ||||
*CHF=Congestive heart failure, DM=Diabetes mellitus, TIA=Transient ischemic attack, LAD=Left atrial diameter, LVEF=Left ventricular ejection fraction, BBB=bundle branch block, ERAF=early recurrence of AF, CAD=Coronary artery disease, COPD=Chronic obstructive pulmonary disease, HTN=Hypertension, CKD=Chronic kidney disease, PV=Pulmonary veins, PAF=Paroxysmal AF, AAD=Antiarrhythmic drugs, SHD=Structural heart disease, LBBB=Left bundle branch block.
Table 2.
Commonly used clinical scores and type of recurrence after catheter ablation.
| Score | Ablation strategy | Type of recurrence |
|---|---|---|
| CHADS2 | RFA | ERAF, LRAF |
| CHA2DS2-VASc | RFA | ERAF, LRAF |
| R2CHADS2 | RFA | ERAF, LRAF |
| APPLE | RFA | LRAF, VLRAF |
| MB-LATER | RFA, CBA | LRAF, VLRAF |
| C2HEST | RFA | LRAF |
| HATCH | RFA | LRAF |
| DR-FLASH | RFA | Substrate |
| PLAAF | CBA | LRAF, VLRAF |
| BASE-AF2 | CBA | LRAF, VLRAF |
| ATLAS | RFA | Any |
| CAAP-AF | RFA, CBA | LRAF |
| SCALE-CryoAF | CBA | VLRAF |
| LAGO | RFA | Any |
| ACEF | RFA | LRAF |
*RFA=radiofrequency ablation, CBA=cryoballoon ablation, ERAF=early recurrence of AF, LRAF=late recurrence of AF, VLARF=very late recurrence of AF.
Table 3.
ECG P-waves parameters and values associated with atrial fibrillation recurrence after catheter ablation.
Table 3.
ECG P-waves parameters and values associated with atrial fibrillation recurrence after catheter ablation.
| P-wave parameter | Abnormal values |
|---|---|
| P-wave duration (PWD) [60] | >120 ms |
| PTFV1 [66] | >0.04 mm*s |
| P-wave dispersion [71,73] | >40 ms or >80ms |
| PWD/PWA [76] | >830ms/mV |
| P-wave axis [73] | <0 or > 75 ̊ |
| P-wave notch [82,83] | peak-to-peak distance in lead II of more than 20ms |
Table 4.
Echocardiographic parameters and values associated with atrial fibrillation recurrence after catheter ablation.
Table 4.
Echocardiographic parameters and values associated with atrial fibrillation recurrence after catheter ablation.
| Echocardiographic parameter | Recurrence | No Recurrence |
|---|---|---|
| LA diameter (LAD) [97] | Variable, >40mm is enlarged | |
| LA volume (LAV)/LA volume index (LAVi) [98] | Variable, most agree >153ml/>34ml/m2 favours recurrence | |
| LA sphericity index [101] | >0.678 | ≤0.678 |
| LA reservoir strain (LASr) [135] | 39% (95% CI, 38%–41%) | |
| LA conduit strain (LAScd)* [135] | 23% (95% CI, 21%–25%) | |
| LA contraction strain (LASct)* [135] | 17% (95% CI, 16%–19%) | |
| Total atrial conduction time (PA-TDI)* [110] | 146.7±20.4 ms | 130.1 ±23.0 ms |
| LA mechanical dispersion (LA-MD) [116] | 38 ± 14 ms | 30 ± 12 ms |
| E/A [121] | 1.8 ± 0.9 | 1.5 ± 0.9 |
| DT [121] | 214 ± 67 ms | 243 ± 68 ms |
| E/E’ [118] | >14 | ≤14 |
| L-wave [120] | Presence | - |
| Left atrioventricular coupling index (LACI) [122] | 44.0 (43.0–45.0)% | 49.5 (47.0–53.0) % |
| LA stiffness index (LASi) [123,124] | 0.83±0.46 or 1.64 ± 1.70 | 0.40±0.22 or 0.61 ± 0.46 |
| Mitral/tricuspid regurgitation (MR/ TR) [128] | More than mild | - |
| Pulmonary artery pressure (PAP) [129] | ≥35 mmHg | < 35mmHg |
| TAPSE/PAP [130] | ≤ 0.57 | >0.57 |
| Right atrial volume (RAV) [132] | ≥87 ml | |
* Indicates parameters measured only during sinus rhythm.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



