Submitted:
14 February 2025
Posted:
17 February 2025
You are already at the latest version
Abstract
Background: The 2011 Very Early Diagnosis of Systemic Sclerosis (VEDOSS) criteria include patients at risk of progression and those with mild non-progressive forms of SSc. Early diastolic and systolic dysfunction can indicate myocardial fibrosis in SSc patients, yet data on myocardial impairment in the VEDOSS population are limited. Objectives: This study aimed to identify subclinical echocardiographic changes and predictive markers of cardiac dysfunction in both very early and mild-longstanding forms of VEDOSS. Methods: We conducted a cross-sectional observational study involving 61 patients meeting VEDOSS criteria followed up regularly within our Scleroderma referral center. Patients were categorized as early VEDOSS (e-VEDOSS) or mild-longstanding VEDOSS (ml-VEDOSS) based on disease duration (≥10 years). We analyzed clinical and demographic data, focusing on echocardiographic parameters such as the E/A ratio and left ventricular (LV) thickness. Statistical analyses included Chi-square, Fischer exact, and Student's T tests, with a significance threshold of p<0.05. Results: ml-VEDOSS patients were older and reported a higher burden of comorbidities. Autoantibody-positive patients exhibited lower E/A ratios and increased left atrial size. Late nailfold videocapillaroscopic pattern patients exhibited increased PWED thickening and aortic valve insufficiency. Notably, patients undergoing vasodilators experienced larger right atrial volume, while patient receiving Renin-Angiotensin-Aldosterone System (RAAS) inhibitors reported reduced E/A ratio. Multivariable analysis confirmed DLCO% as the sole predictor of both diastolic and systolic impairment in VEDOSS population. Conclusion: Careful monitoring of cardiac function in VEDOSS patients is crucial as subclinical alterations may occur even in the absence of symptoms. DLCO% emerged as an important predictor of LV diastolic dysfunction.
Keywords:
VEDOSS
; Systemic Sclerosis
; early diagnosis
; cardiac involvement
; diastolic dysfunction
; echocardiography
1. Introduction
Systemic sclerosis (SSc) is a rare autoimmune disease characterized by the classical triad of microvascular damage, autoimmune dysregulation and fibrosis of the skin and internal organs [1]. The extensive fibrotic process of vital organs, including the lungs and heart, is significantly associated with a high burden of morbidity and mortality [2]. In this context, it is essential to perform a prompt diagnosis to shape the trajectories of potentially progressive disease [3]. Currently, SSc diagnosis can be oriented by consolidated classification criteria such as those proposed by LeRoy and Medsger in 2001 [4], together with the 2013 ACR/EULAR guidelines [5]. However, it is well recognized that these classifications do not encompass all patients within the broader scleroderma spectrum, particularly in the earlier stages of the disease [6]. The 2011 criteria for a Very Early Diagnosis of Systemic Sclerosis (the VEDOSS criteria) and their validation in 2021, have enhanced clinicians’ ability to identify the disease in its initial phase [7,8].
Thus, while VEDOSS may represent the early stage of SSc, it could also reflect a milder form that remains stable over time and does not progress to clinically established disease. Currently, despite the lack of validated criteria that allow clinicians to differentiate between these two forms, VEDOSS represents a critical stage in the scleroderma continuum, in which it results crucial to identify early organ involvement. [9,10]
Moreover, while some organs, such as the gastrointestinal tract have been investigated in VEDOSS [11], cardiac involvement remains a neglected area. All layers of the heart—endocardium, myocardium, and pericardium—can be affected by the pathogenic processes of SSc, with myocardial fibrosis being the predominant pathological finding in postmortem studies [12]. Subclinical left ventricular (LV) diastolic and systolic impairments represent the initial expression of myocardial fibrosis, which may often be asymptomatic [13]. However, several echocardiographic parameters, such as mitral early diastolic inflow velocity (E wave), mitral late filling peak velocity (A wave), early diastolic annular velocity (E’), as well as the E/A and E/E’ ratios may enable the detection of early myocardial involvement in asymptomatic SSc patients. For instance, an E/A ratio less than 1.0 and E/E’ ratio ≥15 indicate elevated filling pressure and predict the development of diastolic heart failure [14]. Moreover, given that cardiac involvement in SSc is highly predictive of poor prognosis and mortality [15], detecting subclinical echocardiographic signs of systolic and diastolic dysfunction seems to be fundamental even in the VEDOSS population.
The aim of the present study is to identify subclinical echocardiographic alterations in VEDOSS patients by analyzing certain clinical, serological and functional predictive markers of systolic and diastolic dysfunction in both mild-longstanding cases and the very early form of SSc, offering insights into the progression and early detection of cardiac involvement in this patient group.
2. Materials and Methods
2.1. Sample Definition
We conducted a cross-sectional observational study involving a cohort of VEDOSS patients attending the Scleroderma Unit of ASST Ovest Milanese (Italy). Participants were selected based on their fulfillment of the 2011 preliminary VEDOSS criteria [7] while not meeting the 2013 ACR/EULAR and/or 2001 LeRoy and Medsger criteria for a definitive diagnosis of SSc [4,5]. Patients with severe heart failure, a positive history of congenital heart disease, severe chronic obstructive pulmonary disease, pulmonary thromboembolism and individuals who underwent cardiac surgery, percutaneous coronary intervention (PCI) and pacemaker implant were excluded from the study. The presence of other autoimmune disease-related antibodies and/or the fulfillment of additional classification criteria for any systemic autoimmune disease served as further exclusion criteria.
Written informed consent was obtained from each participant, and the study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki, with the ethic protocol number S00125/2023 obtained from the Ethic Committee of Milan Area 3.
2.2. Data Collection
Data collection was conducted by experienced rheumatologists and spanned between June and December 2024. Demographic data including sex, age at enrollment, alcohol consumption or smoking habit, age at the first appearance of Raynaud’s Phenomenon (RP) and age at VEDOSS diagnosis were extracted from medical records. Diagnostic delay was calculated as the time interval between the onset of the first VEDOSS symptom and the confirmation of a definitive VEDOSS diagnosis.
Key clinical and anthropometric parameters were recorded at last follow up visit, including height, weight, body mass index (BMI) and body surface area (BSA). The presence of RP and puffy hands was noted, along with the presence of any gastrointestinal complaints that could be attributed to VEDOSS. Additionally, for the main purpose of the study, the absence of skin fibrosis, sclerodactyly, digital ulcers, pitting scars, calcinosis and telangiectasias was documented. Therefore, clinical evaluation involved a comprehensive physical, functional and radiological assessment for dyspnea and other heart-related symptoms. Data from pulmonary function tests (PFTs), including predicted forced vital capacity (FVC%), predicted diffusing capacity for carbon monoxide (DLCO%), and the FVC/DLCO% ratio, were obtained from the most recent available assessments, along-with chest X-ray which allowed to exclude suspected or established interstitial lung disease (ILD) and pulmonary arterial hypertension (PAH) as compelling causes of unexplained dyspnea. Analogously, all patients underwent nailfold Videocapillaroscopy (NVC) at the last follow-up visit, with the NVC results been reported according to Cutolo classification [17].
Laboratory detection of antinuclear antibodies (ANA), anticentromere antibodies (ACA), and anti-topoisomerase I antibodies (ATA) was performed using standardized methods during the initial clinical evaluation.
Data on current comorbidities were collected, including cardiovascular conditions such as chronic systemic arterial hypertension and atrial fibrillation, as well as thyroid disorders, pulmonary diseases, gastrointestinal disorders, renal diseases, malignancies, hematological conditions and psychiatric and neurological issues.
Data concerning treatment modalities were registered, encompassing the administration of Iloprost infusions, the use of calcium channel blockers (CCBs) and low-dose aspirin (LDA). Additionally, treatments employed for managing cardiovascular comorbidities with a known influence on microvascular system were documented, such as angiotensin-converting enzyme inhibitors (ACE-Is), angiotensin receptor blockers (ARBs), beta-blockers and diuretics. Immunosuppressive therapies and the use of hydroxychloroquine were also recorded.
2.3. Echocardiography Procedure
Echocardiographic parameters were collected at the last follow-up visit. All selected patients were imaged by transthoracic echocardiography (TTE) in the left lateral decubitus position by experienced cardiologists at the same hospital in accordance with the guidelines of the American Society of Echocardiography (ASE) [18]. All images and measurements were obtained from the standard views with stable Electrocardiograph (EKG). The following parameters were measured: interventricular septum (IVS) thickness (mm), posterior wall at end diastole (PWED) thickness (mm), left ventricular (LV) volumes and diameters in both end systole and end diastole, aorta diameter at sinuses, along with right and left atrial (RA and LA) volumes at end systole in monoplane apical 4 chamber (4CH) view through both Simpson and indexed methods, RA and LA end systolic diameters were measured via monoplane 4CH view in the longitudinal side (superior-inferior) direction as well as RA and LA end systolic area was assessed in cm2. Left ventricular (LV) ejection fraction (EF) was measured with the modified biplane Simpson’s method from the apical 4CH view [19].
Left ventricular (LV) mass was calculated according to the Devereux formula [20]. Pathological thickening of both IVS and PWED was defined as more than 10 mm and more than 9 mm, respectively. Additionally, the systolic pulmonary artery pressure (sPAP) was estimated using modified Bernoulli’s formula [21]. The tricuspid annular plane systolic excursion (TAPSE) was measured by placing the M-mode line at the junction of the tricuspid valve annulus and the RV free wall [22]. Tricuspid regurgitation and the Tricuspid maximum regurgitation pressure gradient were also assessed. Doppler echocardiographic measurements included: Trans-mitral early diastolic inflow velocity (E), trans-mitral late filling peak velocity (A), and E/A ratio measured in the apical 4-CH view [23]. Tissue Doppler imaging was used to measure the early diastolic annular velocity (E’). Left ventricular dysfunction was defined as mitral E/A ratio <1.0 and E/E’ ratio ≥15 [24]. Additionally, the presence of mitral, aortic, and tricuspid valve insufficiencies was evaluated by the color Doppler method, along with any noted sclerosis of the aortic and mitral valve leaflets and then reported according to the 2020 ACC/AHA guideline for the management of patients with valvular heart disease [25]. Lastly, the presence of pericardial effusion was identified by the appearance of an echo-free space between the two layers of the pericardium.
2.4. Statistical Analysis
Patients’ data were summarized as mean and standard deviation for normally distributed variables or as median and interquartile range (IQR) for skewed ones. Discrete or qualitative variables were summarized as counts and percentages. Mean differences of continuous variables were assessed using Student’s t-test or Mann-Whitney U-test, depending on whether the data followed a parametric or non-parametric distribution. Chi-squared and Fisher’s exact tests were used to compare categorical variables based on sample size. ANOVA test served for multiple comparison analysis.
Based on their established relevance on SSc progression and heart involvement, several clinical determinants—such as BMI, age at VEDOSS diagnosis, DLCO% predicted, ACA/ATA positivity, late NVC patterns and puffy hands were included in the multiple general regression model to assess their independent contribution on left ventricular diastolic and systolic dysfunction. E/A ratio, IVS thickness, and PWED thickness served as dependent variables in the multiple general regression model.
A p-value of ≤0.05 or a 95% confidence interval not crossing zero were considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics version 27 (IBM SPSS Software, Armonk, NY, USA).
3. Results
3.1. Overall Patients’ Characteristics.
The study cohort consisted of 61 participants, with a female predominance (58 out of 61–95.1%). Based on VEDOSS disease duration, patients were distributed into two subgroups: mild longstanding VEDOSS with a disease duration ≥ 10 years (ml-VEDOSS, 24/61– 39.3%) and early VEDOSS group with a disease duration < 10 years (e-VEDOSS, 37/61–60.7%) [Table 1].
The mean age at enrollment was significantly higher in the ml-VEDOSS group compared to the e-VEDOSS group (64.0±12.8 vs 55.2±14.6 years; p=0.01). As expected, the disease durations for VEDOSS and RP were substantially longer in the ml-VEDOSS group (16.8±7.7 vs 4.9±2.7 years; p<0.001 and, 21.6±10.4 vs 12.3±10.9; p=0.002, respectively). Regarding autoimmunity profile, ACA+ patients were more frequently present in the ml-VEDOSS group (50% vs 24.3%, p=0.05).
A greater mean comorbidity count was observed in the ml-VEDOSS group compared to the e-VEDOSS group (3.6±2.0 vs 2.1±1.9; p=0.005), with higher prevalence of patients exhibiting more than 3 comorbidities (66.7% vs 40.5%, p=0.01). Within the same group there was a higher prevalence of cardiovascular and gastrointestinal diseases (66.7% vs 35.1%; p=0.02 and 75% vs 45.9%; p=0.03, respectively), along with hematological disorders (25% vs 5.3%, p=0.04). Furthermore, the late NVC pattern was significantly more common within the ml-VEDOSS group (6 out of 24, 25%; p=0.002).
Similarly, treatment modalities displayed notable variations between the two groups. The administration of vasodilators, such as Iloprost infusion and CCBs, resulted significantly more prescribed in the ml-VEDOSS group (87.5% vs 62.2%, p=0.04 and 50% vs 21.6%, p=0.03, respectively). The use of ACE-Is or ARBs was more common in the ml-VEDOSS group compared to the e-VEDOSS group (41.7% vs 16.2%, p=0.04). Immunosuppressants were prescribed only in 3 out of 61 patients, two of which were receiving methotrexate due to musculoskeletal symptoms, while 1 patient received azathioprine for a concurrent diagnosis of autoimmune hepatitis.
3.2. Subclinical Echocardiographic Findings
Main echocardiographic findings of the entire population are reported in Table 2. Specifically, mean E/A ratio was 0.99±0.39 and 37/61 (60.7%) patients exhibited an E/A ratio less than 1, mean PWED thickness was 8.4±1.6 mm and 19 out of 61 (31.1%) presented with a PWED thickening more than 9 mm, while a pathological IVS thickening(> 10 mm) was documented in 17/61 participants (27.9%). A reduced EF% (less than 55%) was reported only in 3/61 patients (4.9%) while the mean value of EF% was 64.5±4.8%. A reduced TAPSE (< 22 mmHg) was reported in 36/61 patients (59%) while only 1 patient exhibited a TAPSE less than 16 mmHg. Mean sPAP of the entire population was 27.2±5.3 mmHg.
Since the comparison between e-VEDOSS and ml-VEDOSS group did not reveal any statistical difference on echocardiographic parameters [Supplementary Table S5], we further focused on assessing these findings within three intergroups, by selecting the late NVC pattern, SSc specific autoantibodies positivity and puffy hands as compelling variables [Table 3].
Notably, the prevalence of patients exhibiting PWED thickness >9 mm was significantly greater in the late NVC pattern group (66.7% vs 23.6 %, p=0.04). Furthermore, the presence of aortic valve insufficiency (66.7% vs 18.2%, p=0.02) and sclerosis (66.7% vs 16.4%, p=0.01) were significantly more prevalent in the same group. Moreover, the E/A ratio was significantly lower in the ACA/ATA+ group (0.84±0.27 vs 1.08±0.42, p=0.02) by exhibiting a longer A wave measurement (0.84±0.20 vs 0.70±0.15 m/s, p=0.006). Additionally, IVS thickness was greater in the same group (9.9 ± 1.3 vs 8.9 ± 1.9 mm, p=0.03). Further significant differences were noted in the LA end systolic (LAES) volume, even indexed for BSA, which were significantly higher in the ACA/ATA+ group (p=0.01 for both). Likewise, the LAES diameter (49.7±5.9 vs 45.0±8.4 mm/m², p=0.04) and the relative wall thickness (0.48±0.09 vs 0.42±0.10, p=0.04) were significantly larger in the ACA/ATA+ group. Additionally, ACA/ATA+ group revealed a greater proportion of both aortic and mitral valve insufficiency and sclerosis of valve leaflets. Lastly, in the puffy hands group, E deceleration time was significantly longer compared to the non-puffy hands group (194.4±47.9 vs 230.5±52.8 m/s, p=0.02). Any differences in RV and RA function parameters emerged from the intergroup comparisons of TAPSE, sPAP, and the tricuspid maximum regurgitation gradient, along with RAES volumes and diameters.
Acronyms: ACE-Is/ARBs= Angiotensin Converting Enzyme Inhibitors; ARBs= Angiotensin Receptor Blockers; E/A ratio= ; E’= early diastolic tissue velocity of the mitral annulus/late diastolic filling velocity ratio; LAES= Left atrial end systolic; m2= square meters.
Additionally, patients receiving ACE-Is/ARBs showed a statistically significant reduction in the E/A ratio compared to those who did not receive these treatments (0.81±0.28 vs 1.06±0.4, p=0.01). This treatment group also exhibited a statistically larger LA diameter measured in the superior-inferior direction at end-systole (49.5±5.8 vs 45.3±8.4 mm/m2, p=0.04) and a greater prevalence of aortic valve leaflets sclerosis (35.3% vs 11.6%, p=0.03). [Figure 1]
3.3. Subclinical Echocardiographic Findings by Comparing Patients Receiving Current Therapy with Vasodilators
Subclinical echocardiographic alterations in patients receiving vasodilators were further assessed. We exclusively selected Iloprost iv administration and/or calcium channel blockers, as no other vasodilator was administered to our patients. Accordingly, patients were divided into four groups: Group 1 encompassing patients receiving Iloprost intravenously only (n=25), Group 2 with patients receiving CCBs orally only (n=8), while Group 3 included patients undergoing both monthly Iloprost infusion and daily oral CCB (n=18), lastly, Group 4 encompassed patients receiving no vasodilators (n=13). Our analysis revealed that patients receiving CCBs only exhibited a greater LVES volume measured by Simpson method (p=0.001), while reporting a reduced RAES volume compared to each group (p=0.005). Moreover, patients undergoing the combination therapy with Iloprost and CCBs exhibited a greater RAES volume measured via Indexed method compared to the other groups (p=0.01). [Table 4]
3.4. General Multivariable Regression Model
Furthermore, E/A ratio, IVS thickness, and PWED thickness were identified as key descriptors of diastolic and systolic LV dysfunction. A general multivariable regression model incorporating BMI, age at VEDOSS diagnosis, DLCO% predicted, ACA/ATA positivity, late NVC patterns and puffy hands as relevant clinical determinants, revealed that only DLCO% emerged as a significant predictor of both IVS thickening (p=0.034) and PWED thickening (p=0.002). Additionally, ACA positivity was significantly associated with PWED thickening (p=0.004). These findings persisted even when the model was applied exclusively to the e-VEDOSS group.
4. Discussion
The present study provides relevant insights into subclinical echocardiographic abnormalities of patients meeting the VEDOSS criteria. The occurrence of cardiac involvement at the early stage of SSc was previously reported by researchers Gotschy A et al. and De Luca G et al. The former conducted a Cardiac Magnetic Resonance driven study which has proved the presence of myocardial fibrosis in a cohort of 24 VEDOSS patients [26], while the latter described three cases of myocardial involvement, emphasizing the role of vasculopathy, inflammation and fibrosis as major SSc-related pathogenic mechanisms [27].
Our cohort was initially divided into mild longstanding VEDOSS (ml-VEDOSS) and early VEDOSS (e-VEDOSS) groups based on disease duration as suggested by Blaja et al. [9]. The authors stated that subjects fulfilling the criteria for VEDOSS encompass a heterogeneous mixture of patients with both early potentially at risk of progression and long standing, very mild diseases. This observation has important implications, as these two subgroups cannot be easily differentiated based on clinical phenotype at first presentation and since patients with mild long-standing disease need different frequencies of follow up and therapeutic considerations [9].
The ml-VEDOSS group exhibited a greater comorbidity count compared to the e-VEDOSS group, reflecting the cumulative burden of disease. This observation is consistent with previous research indicating that prolonged disease duration is correlated with prolonged chronic inflammation and prolonged exposure to altered vasoreactivity, ultimately increasing cardiovascular comorbidity [28, 29]. These findings are particularly relevant given that SSc patients account a five–fold increased mortality rate due to cardiac causes and sudden cardiac death occurring in 21%–54% of cases [15, 30]
The intergroup comparisons showed several differences on LV diastolic function parameters. In fact, as demonstrated by Giunta A et al., LV function can reflect heart involvement of SSc more sensitively than RV function [31]. Firstly, VEDOSS patients with late NVC patterns had significantly greater PWED thickness and a higher prevalence of aortic valve insufficiency. This aligns with findings of Markusse IM et al., who confirmed the independent association between advanced NVC pattern and heart/lung involvement [32]. Insightfully, the relationship between macrovascular and microvascular damage in SSc has been largely investigated. Pagkopoulou et al. demonstrated that reduced capillary density was inversely correlated with arterial stiffness. The authors reported also that the Framingham Risk Score, QRISK3, and ASCVD (Atherosclerotic Cardiovascular Disease) were inversely correlated with capillary density [33]. Conversely, Szucs et al. showed that the flow-mediated endothelium-dependent dilation was substantially reduced in SSc patients compared to healthy controls, indicating that impaired endothelium-dependent vasodilation is also present in pre-atherosclerotic stages [34]. Nevertheless, accurately quantifying the roles of intrinsic microangiopathy versus more common atherosclerotic processes in shaping the cardiovascular risk of SSc patients remains challenging.
Our results support these findings, providing additional evidence for the VEDOSS population, revealing that more advanced microarchitectural changes in NVC are related to greater echocardiographic alterations.
Additionally, it is worth mentioning that the ongoing process of endothelial dysfunction also affects coronary microvasculature [35]. Due to abnormal vasoreactivity, patients with SSc may experience repeated cycles of myocardial ischemia-reperfusion, potentially contributing to the development of myocardial fibrosis, even in the absence of significant heart-related symptoms.
Furthermore, we observed that VEDOSS patients with specific SSc autoantibody positivity exhibited a reduced E/A ratio, greater modifications in LAES area, valve dysfunction and, an increased PWED thickness, positioning with previous research that has shown a relationship between specific autoantibodies and cardiac involvement [36]. Despite the causal relationship between autoantibodies and myocardial fibrosis is not yet fully understood, Henault et al. demonstrated that ATA can directly bind to fibroblast surfaces, inducing their activation and proliferation in endothelial tissue [37]. Moreover, Shen et al. found that ACA and ATA antibodies could induce vascular endothelial cell senescence via mechanisms distinct from the classic p53-p21 pathway in vitro, as observed in the sera of patients with Raynaud’s phenomenon [38].
Moreover, Bellando-Randone et al. stated that autoimmunity plays a crucial role in shaping the progressive trajectories of VEDOSS patients, highlighting that SSc-specific antibodies are the most significant isolated predictor of progression from VEDOSS to definitive SSc, whereas negativity for antinuclear antibodies (ANA) at baseline has a strong negative predictive value [39].
Interestingly, by comparing patients undergoing vasodilators to patients not receiving such treatment, the former reported a greater percentage of enlarged RA, potentially reflecting an increased pressure or volume load on the RV. However, our echocardiographic findings did not show any discrepancies in RV functionality, as reported by the similar values of TAPSE, sPAP and Tricuspid maximum regurgitation gradient.
Our intriguing data did not allow easy interpretation. On one hand, our observation suggests that vasodilators may exert detrimental effects on right atrial enlargement, without causing detectable changes in RV measurements. On the other hand, patients in the VEDOSS cohort could be characterized by an overall greater disease severity due to more severe microvascular involvement, which encompasses RA abnormalities, and vasodilators may simply be insufficient to detain the damage progression.
As demonstrated by Guedón et al., in a prospective three-years survival analysis, Iloprost administration did not show any effect on reducing nor increasing the occurrence of diastolic dysfunction and PAH, while Sildenafil demonstrated a potential protective role in preventing the progression toward diastolic dysfunction and heart failure with altered EF [40]. The authors also emphasized the need for a comprehensive analysis of the potential benefits of sodium-glucose cotransporter 2 (SGLT2) inhibitors, such as empagliflozin and dapagliflozin, on diastolic dysfunction in patients with SSc. These medications have demonstrated beneficial effects in patients with heart failure and preserved EF [41]. However, we have no evidence regarding their efficacy in the VEDOSS population, as the present study focused on detecting subclinical echocardiographic changes in patients without heart-related symptoms.
Nevertheless, the increased use of both ACE-Is and ARBs in ml-VEDOSS points to a proactive approach in mitigating cardiovascular risk in patients experiencing a longer disease duration. This strategy is supported by evidence implying that these medications can improve cardiovascular and renal outcomes in the general population. In fact, ACE-Is and ARBs encompass the same Renin-Angiotensin-Aldosterone System (RAAS) inhibitors group although exerting different mechanisms of action, including increased bradykinin levels, potentiated bradykinin response and stimulated nitric oxide production with ACE- Is [42]. Moreover, the reduced E/A ratio in RAAS inhibitors group could reinforce the theory of their usage in more at-risk individuals, potentially mitigating the occurrence of major cardiac events and mortality. However, the preventive role of RAAS inhibitors in the early stages of SSc is still debated and their usage should be practiced with caution. In fact, as reported by Bütikofer L. et al. in an EUSTAR cohort analysis, ACE-Is in SSc patients with concomitant arterial hypertension display an independent risk factor for the development of Scleroderma Renal Crisis (SRC) but they still represent the first choice in SRC treatment. This study advocate that ARBs might be a safer alternative than ACE-Is, yet the overall safety of alternative antihypertensive drugs needs to be further investigated [43].
Furthermore, the multivariable analysis, indicating that DLCO% was the only significant predictor of IVS and PWED thickening, supported the role of pulmonary function in uncovering subclinical cardiac changes within our population. As recently described by He H. et al in a magnetic resonance guided study, the DLCO% values are inversely correlated with myocardial native T1 values in SSc patients, suggesting that DLCO might be a potential indicator for subclinical myocardial fibrosis [44].
Although the present study adds new evidence on the underexplored occurrence of subclinical cardiac involvement in VEDOSS, it is limited by several factors. The relatively limited sample size of 61 participants may impact on the robustness of our conclusions. However, this small sample size primarily stems from the low prevalence of systemic sclerosis, as well as the even lower prevalence of VEDOSS. Therefore, multicenter studies involving larger cohorts are necessary to enhance the validity of these findings. Furthermore, inter-operator variability in the echocardiographic technique should be considered, although standardized protocols in accordance with the 2020 ACC/AHA guidelines were implemented to minimize its impact, as detailed in the methods section. Additionally, since the study was conducted at a single center in Italy, the generalizability of these findings may be limited. Due to the cross-sectional nature of the study, causal inferences cannot be made. To address this limitation, we strongly recommend conducting further multicenter prospective studies.
In conclusion, we demonstrated that various subclinical echocardiographic alterations occur in both early and mild-longstanding form of VEDOSS, however, we excluded patients initially classified as VEDOSS who further developed an established SSc. Future research is warranted to detect early differences in echocardiographic parameters between progressive and stable forms.
5. Conclusions
This study highlighted critical echocardiographic changes among patients fulfilling VEDOSS criteria. The associations between pulmonary function, cardiac structure, specific autoantibodies profile and microvascular damage underscored the complexity of VEDOSS and the need for comprehensive management strategies. Timely detection of heart involvement, especially in patients with advanced microangiopathy and features of SSc-related autoimmunity, is crucial for predicting disease progression and mortality.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Echocardiographic findings comparison between e-VEDOSS and ml-VEDOSS.
Author Contributions
E.C.: Conceptualization, Software, Methodology, Validation, Formal analysis, Investigation, Resources, Data curation, Writing—original draft, Writing—review & editing E.Z.: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation, Writing—review & editing. I.S.: Resources, Data curation. A.L.: Resources, Data curation, L.C.: Resources. Data curation. E.M. Resources. Data curation. D.B.: Resources. Data curation. AT.: Resources. Data curation. M.I.: Methodology. Supervision. M.S.C.: Methodology. Supervision A.M.: Conceptualization, Validation, Resources, Supervision. Project administration. P.F.: Conceptualization, Validation, Resources, Writing—review & editing, Supervision. Project administration.
Funding
This research received no external funding.
Institutional Review Board Statement
“The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of ASST OVEST MILANESE.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request. The data is not publicly available due to ethical restrictions.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ko J, Noviani M, Chellamuthu VR, Albani S, Low AHL. The Pathogenesis of Systemic Sclerosis: The Origin of Fibrosis and Interlink with Vasculopathy and Autoimmunity. Int J Mol Sci. 2023 Sep 19;24(18):14287. [CrossRef]
- Rosa I, Romano E, Fioretto BS, Manetti M. The contribution of mesenchymal transitions to the pathogenesis of systemic sclerosis. Eur J Rheumatol. 2020 Oct;7(Suppl 3):S157-S164. [CrossRef]
- Herrick AL, Assassi S, Denton CP. Skin involvement in early diffuse cutaneous systemic sclerosis: an unmet clinical need. Nat Rev Rheumatol. 2022 May;18(5):276-285. [CrossRef]
- LeRoy EC, Medsger TA Jr. Criteria for the classification of early systemic sclerosis. J Rheumatol. 2001 Jul;28(7):1573-6.
- van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013 Nov;65(11):2737-47.
- Yang M, Goh V, Lee J, Espinoza M, Yuan Y, Carns M et al. Clinical Phenotypes of Patients with Systemic Sclerosis With Distinct Molecular Signatures in Skin. Arthritis Care Res (Hoboken). 2023 Jul;75(7):1469-1480. [CrossRef]
- Bellando-Randone S, Galdo FD, Lepri G, et al. Progression of patients with Raynaud’s phenomenon to systemic sclerosis: a five-year analysis of the European Scleroderma Trial and Research group multicentre, longitudinal registry study for Very Early Diagnosis of Systemic Sclerosis (VEDOSS). The Lancet Rheumatology 2021; 3: e834–43. [CrossRef]
- Avouac J, Fransen J, Walker UA, et al. Preliminary criteria for the very early diagnosis of systemic sclerosis: results of a Delphi Consensus Study from EULAR Scleroderma Trials and Research Group. Ann Rheum Dis 2011; 70: 476–81. [CrossRef]
- Blaja E, Jordan S, Mihai CM, Dobrota R, Becker MO et al. The Challenge of Very Early Systemic Sclerosis: A Combination of Mild and Early Disease? J Rheumatol. 2021 Jan 1;48(1):82-86. [CrossRef]
- Ross RL, Caballero-Ruiz B, Clarke EL, Kakkar V, Wasson CW, Mulipa P et al. Biological hallmarks of systemic sclerosis are present in the skin and serum of patients with Very Early Diagnosis of SSc (VEDOSS). Rheumatology (Oxford). 2024 Dec 19:keae698. Epub ahead of print. [CrossRef]
- El Aoufy K, Melis MR, Bandini G, et al POS1593-HPR GASTROINTESTINAL INVOLVEMENT IS ALREADY REPORTED IN AN ITALIAN VEDOSS COHORT: RESULTS FROM A RHEUMATOLOGICAL NURSE ASSESSMENT Annals of the Rheumatic Diseases 2023;82:1172-1173. [CrossRef]
- Zhu L, Wang Y, Zhao S, Lu M. Detection of myocardial fibrosis: Where we stand. Front Cardiovasc Med. 2022 Sep 29;9:926378. [CrossRef]
- Cusmà Piccione M, Zito C, Bagnato G, Oreto G, Di Bella G, Bagnato G, Carerj S. Role of 2D strain in the early identification of left ventricular dysfunction and in the risk stratification of systemic sclerosis patients. Cardiovasc Ultrasound. 2013 Feb 3;11:6. [CrossRef]
- Lee SW, Choi EY, Jung SY, Choi ST, Lee SK, Park YB. E/E’ ratio is more sensitive than E/A ratio for detection of left ventricular diastolic dysfunction in patients with systemic sclerosis. Clin Exp Rheumatol. 2010 Mar-Apr;28(2 Suppl 58):S12-7.
- Pokeerbux, M.R.; Giovannelli, J.; Dauchet, L.; Mouthon, L.; Agard, C.; Lega, J.C.; Allanore, Y.; Jego, P.; Bienvenu, B.; Berthier, S.; et al. Survival and prognosis factors in systemic sclerosis: Data of a French multicenter cohort, systematic review, and meta-analysis of the literature. Arthritis Res. Ther. 2019, 21, 86. [Google Scholar] [CrossRef] [PubMed]
- Avouac J, Fransen J, Walker UA, Riccieri V, Smith V, Muller C, Miniati I, Tarner IH, Randone SB, Cutolo M, Allanore Y, Distler O, Valentini G, Czirjak L, Müller-Ladner U, Furst DE, Tyndall A, Matucci-Cerinic M; EUSTAR Group. Preliminary criteria for the very early diagnosis of systemic sclerosis: results of a Delphi Consensus Study from EULAR Scleroderma Trials and Research Group. Ann Rheum Dis. 2011 Mar;70(3):476-81. [CrossRef]
- Ruaro B, Smith V, Sulli A, Decuman S, Pizzorni C, Cutolo M. Methods for the morphological and functional evaluation of microvascular damage in systemic sclerosis. Korean J Intern Med. 2015 Jan;30(1):1-5. [CrossRef]
- Mitchell C, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, Foster MC, Horton K, Ogunyankin KO, Palma RA, Velazquez EJ. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2019 Jan;32(1):1-64. [CrossRef]
- Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology Journal of the American Society of Echocardiography, Volume 18, Issue 12, 1440 – 1463.
- Devereux RB, Alonso DR, Lutas EM,Gottlieb GJ, Campo E, Sachs I, Reichek N (1986) Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 57:450–458.
- Pyxaras SA, Pinamonti B, Barbati G, Santangelo S, Valentincic M, Cettolo F, Secoli G, Magnani S, Merlo M, Lo Giudice F, Perkan A, Sinagra G. Echocardiographic evaluation of systolic and mean pulmonary artery pressure in the follow-up of patients with pulmonary hypertension. Eur J Echocardiogr. 2011 Sep;12(9):696-701. [CrossRef]
- Skinner H, Kamaruddin H, Mathew T. Tricuspid Annular Plane Systolic Excursion: Comparing Transthoracic to Transesophageal Echocardiography. J Cardiothorac Vasc Anesth. 2017 Apr;31(2):590-594. [CrossRef]
- Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA et al. (2009) Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr 10(2):165–193. [CrossRef]
- Schwarz ER, Dashti R. The clinical quandary of left and right ventricular diastolic dysfunction and diastolic heart failure. Cardiovasc J Afr. 2010 Jul-Aug;21(4):212-20. [CrossRef]
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Feb 2;143(5):e35-e71. Erratum in: Circulation. 2021 Feb 2;143(5):e228. Erratum in: Circulation. 2021 Mar 9;143(10):e784.
- Gotschy A, Jordan S, Stoeck CT, von Deuster C, Peer T, Gastl M, Vishnevskiy V, Wissmann L, Dobrota R, Mihai C, Becker MO, Maurer B, Kozerke S, Ruschitzka F, Distler O, Manka R. Diffuse myocardial fibrosis precedes subclinical functional myocardial impairment and provides prognostic information in systemic sclerosis. Eur Heart J Cardiovasc Imaging. 2023 Feb 17;24(3):373-382. [CrossRef]
- De Luca G, Campochiaro C, Peretto G, Busnardo E, Matucci-Cerinic M, Dagna L. Cardiac involvement, a threatening very early manifestation of systemic sclerosis: evidence from VEDOSS patients. Clin Exp Rheumatol. 2023 Aug;41(8):1723-1724. [CrossRef]
- Volkmann ER, Fischer A. Update on Morbidity and Mortality in Systemic Sclerosis-Related Interstitial Lung Disease. J Scleroderma Relat Disord. 2021 Feb;6(1):11-20. [CrossRef]
- Alfaddagh A, Martin SS, Leucker TM, Michos ED, Blaha MJ, Lowenstein CJ, Jones SR, Toth PP. Inflammation and cardiovascular disease: From mechanisms to therapeutics. Am J Prev Cardiol. 2020 Nov 21;4:100130. [CrossRef]
- Rangarajan, V.; Matiasz, R.; Freed, B.H. Cardiac complications of systemic sclerosis and management: Recent progress. Curr. Opin. Rheumatol. 2017, 29, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Giunta A, Tirri E, Maione S et al.: Right ventricular diastolic abnormalities in systemic sclerosis. Relation to left ventricular involvement and pulmonary hypertension. Ann Rheum Dis 2000; 59: 94-8. [CrossRef]
- Markusse IM, Meijs J, de Boer B, Bakker JA, Schippers HPC, Schouffoer AA, Ajmone Marsan N, Kroft LJM, Ninaber MK, Huizinga TWJ, de Vries-Bouwstra JK. Predicting cardiopulmonary involvement in patients with systemic sclerosis: complementary value of nailfold videocapillaroscopy patterns and disease-specific autoantibodies. Rheumatology (Oxford). 2017 Jul 1;56(7):1081-1088. [CrossRef]
- Pagkopoulou E, Soulaidopoulos S, Triantafyllidou E, Arvanitaki A, Katsiki N, Loutradis C, Karagiannis A, Doumas M, Garyfallos A, Kitas GD, Dimitroulas T. Peripheral microcirculatory abnormalities are associated with cardiovascular risk in systemic sclerosis: a nailfold video capillaroscopy study. Clin Rheumatol. 2021 Dec;40(12):4957-4968. [CrossRef]
- Szucs, G.; Tímár, O.; Szekanecz, Z.; Dér, H.; Kerekes, G.; Szamosi, S.; Shoenfeld, Y.; Szegedi, G.; Soltész, P. Endothelial Dysfunction Precedes Atherosclerosis in Systemic Sclerosis–Relevance for Prevention of Vascular Complications. Rheumatology 2007, 46, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Zanatta E, Famoso G, Boscain F, Montisci R, Pigatto E, Polito P, Schiavon F, Iliceto S, Cozzi F, Doria A, Tona F. Nailfold avascular score and coronary microvascular dysfunction in systemic sclerosis: A newsworthy association. Autoimmun Rev. 2019 Feb;18(2):177-183. [CrossRef]
- Tsai CY, Hsieh SC, Wu TH, Li KJ, Shen CY, Liao HT, Wu CH, Kuo YM, Lu CS, Yu CL. Pathogenic Roles of Autoantibodies and Aberrant Epigenetic Regulation of Immune and Connective Tissue Cells in the Tissue Fibrosis of Patients with Systemic Sclerosis. Int J Mol Sci. 2020 Apr 27;21(9):3069. [CrossRef]
- Hénault J, Robitaille G, Senécal JL, Raymond Y. DNA topoisomerase I binding to fibroblasts induces monocyte adhesion and activation in the presence of anti-topoisomerase I autoantibodies from systemic sclerosis patients. Arthritis Rheum. 2006 Mar;54(3):963-73. [CrossRef]
- Shen CY, Lu CH, Wu CH, Li KJ, Kuo YM, Hsieh SC, Yu CL. Molecular Basis of Accelerated Aging with Immune Dysfunction-Mediated Inflammation (Inflamm-Aging) in Patients with Systemic Sclerosis. Cells. 2021 Dec 2;10(12):3402. [CrossRef]
- Bellando-Randone S, Galdo FD, Lepri G, et al. Progression of patients with Raynaud’s phenomenon to systemic sclerosis: a five-year analysis of the European Scleroderma Trial and Research group multicentre, longitudinal registry study for Very Early Diagnosis of Systemic Sclerosis (VEDOSS). Lancet Rheumatol 2021; 3: e834–843.
- Guédon AF, Carrat F, Mouthon L, Launay D, Chaigne B, Pugnet G, Lega JC, Hot A, Cottin V, Agard C, Allanore Y, Fauchais AL, Lescoat A, Dhote R, Papo T, Chatelus E, Bonnotte B, Kahn JE, Diot E, Aouba A, Magy-Bertrand N, Queyrel V, Le Quellec A, Kieffer P, Amoura Z, Granel B, Gaultier JB, Balquet MH, Wahl D, Lidove O, Espitia O, Cohen A, Fain O, Hachulla E, Mekinian A, Rivière S. Vasodilator drugs and heart-related outcomes in systemic sclerosis: an exploratory analysis. RMD Open. 2024 Dec 9;10(4):e004918. [CrossRef]
- Lee HC, Shiou YL, Jhuo SJ, Chang CY, Liu PL, Jhuang WJ, Dai ZK, Chen WY, Chen YF, Lee AS. The sodium-glucose co-transporter 2 inhibitor empagliflozin attenuates cardiac fibrosis and improves ventricular hemodynamics in hypertensive heart failure rats. Cardiovasc Diabetol. 2019 Apr 1;18(1):45. [CrossRef] [PubMed] [PubMed Central]
- Alcocer LA, Bryce A, De Padua Brasil D, Lara J, Cortes JM, Quesada D, Rodriguez P. The Pivotal Role of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers in Hypertension Management and Cardiovascular and Renal Protection: A Critical Appraisal and Comparison of International Guidelines. Am J Cardiovasc Drugs. 2023 Nov;23(6):663-682. [CrossRef]
- Bütikofer L, Varisco PA, Distler O, Kowal-Bielecka O, Allanore Y, Riemekasten G, Villiger PM, Adler S; EUSTAR collaborators. ACE inhibitors in SSc patients display a risk factor for scleroderma renal crisis-a EUSTAR analysis. Arthritis Res Ther. 2020 Mar 24;22(1):59. [CrossRef]
- He H, Tong X, Ning Z, Zhou J, Du C, Wang Y, Wang Q, Xu D, Zeng X, He ZX, Zhao X. Diffusing capacity of lungs for carbon monoxide associated with subclinical myocardial impairment in systemic sclerosis: A cardiac MR study. RMD Open. 2023 Dec 7;9(4):e003391. [CrossRef]
Figure 1.
Bar chart showing main echocardiographic findings differences between patients undergoing ACE-Is/ARBs treatment versus patients not receiving ACE-Is/ARBs therapy.
Figure 1.
Bar chart showing main echocardiographic findings differences between patients undergoing ACE-Is/ARBs treatment versus patients not receiving ACE-Is/ARBs therapy.
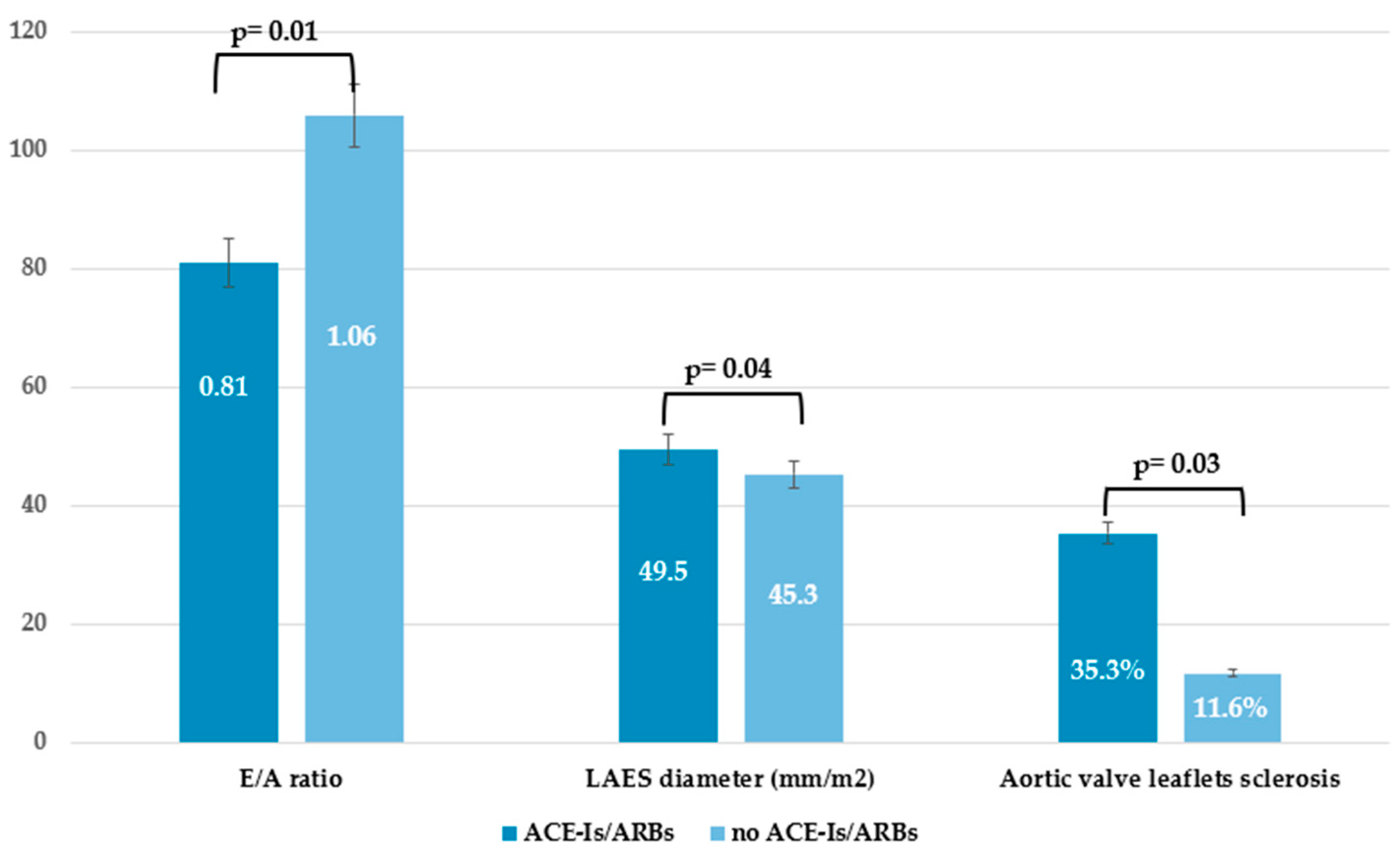

Table 1.
Patient’s main characteristics according to VEDOSS disease duration.
| TOTAL n=61 |
e-VEDOSS n=37 |
ml-VEDOSS n=24 |
p-Value | |
|---|---|---|---|---|
| Female, n(%) | 58 (95.1) | 36 (97.3) | 22 (91.7) | 0.56 |
| Male, n(%) | 3 (4.9) | 1 (2.7) | 2 (8.3) | 0.56 |
| Age at enrollment, mean±SD | 58.7 ± 14.5 | 55.2 ± 14.6 | 64.0 ± 12.8 | 0.01 |
| Age at VEDOSS diagnosis, mean±SD | 49.8 ± 14.7 | 51.7 ± 15.1 | 47.3 ±14.1 | 0.27 |
| Age at RP onset, mean±SD | 43.2 ±17.1 | 44.2 ± 17.4 | 41.8 ± 16.9 | 0.62 |
| Disease Duration of VEDOSS, mean±SD | 9.9 ± 7.9 | 4.9 ± 2.7 | 16.8 ± 7.7 | <0.001 |
| Disease duration of RP, mean±SD | 16.1 ± 11.6 | 12.3 ± 10.9 | 21.6 ± 10.4 | 0.002 |
| Diagnostic delay, mean±SD | 6.4 ± 9.5 | 7.5 ± 10.6 | 4.7 ± 7.4 | 0.28 |
| Body Mass Index (Kg/m2), mean±SD | 23.5 ± 5.9 | 22.4 ± 5.7 | 25.2 ± 5.9 | 0.07 |
| Smoking habits, n(%) | 10 (16.4) | 8 (21.6) | 2 (8.3) | 0.29 |
| Alcohol Consumption, n(%) | 13 (21.3) | 2 (5.3) | 1 (4.2) | 1.0 |
| Puffy hands, n(%) | 18 (29.5) | 10 (27.0) | 8 (33.3) | 1.0 |
| ANA (positive) only, n(%) | 21 (34.4) | 16 (43.2) | 5 (20.8) | 0.09 |
| Anticentromere (positive), n(%) | 21 (34.4) | 9 (24.3) | 12 (50) | 0.05 |
| Anti-topoisomerase I (positive), n(%) | 3 (4.9) | 2 (5.3) | 1 (4.2) | 1.0 |
| Gastrointestinal tract symptoms, n(%) | 30 (49.2) | 15 (40.5) | 15 (62.5) | 0.12 |
| COMORBIDITIES, n(%) | ||||
| Cardiovascular diseases, | 29 (47.5) | 13 (35.1) | 16 (66.7) | 0.02 |
| Dyslipidemia | 17 (27.9) | 9 (24.3) | 8 (33.3) | 0.56 |
| Hyperuricemia | 2 (3.3) | 0 (0) | 2 (8.3) | 0.15 |
| Type 2 Diabetes Mellitus | 4 (6.6) | 2 (5.3) | 2 (8.3) | 0.64 |
| Thyroid disorders | 13 (21.3) | 7 (18.9) | 6 (25.0) | 0.75 |
| Lung Diseases | 12 (19.6) | 6 (16.2) | 6 (25.0) | 0.51 |
| Kidney Diseases | 8 (13.1) | 4 (10.8) | 4 (16.7) | 0.7 |
| Gastrointestinal diseases | 35 (57.4) | 17 (45.9) | 18 (75.0) | 0.03 |
| Hematological disorders | 8 (13.1) | 2 (5.3) | 6 (25.0) | 0.04 |
| Malignancies | 10 (16.4) | 5 (13.5) | 5 (20.8) | 0.49 |
| Psychiatric disorders | 3 (4.9) | 2 (5.3) | 1 (4.2) | 1.0 |
| Neurological disorders | 11 (18.0) | 5 (13.5) | 6 (25.0) | 0.32 |
| Comorbidities count, mean±SD | 2.7 ± 2.1 | 2.1 ±1.9 | 3.6 ± 2.0 | 0.005 |
| Comorbidities count ≥ 3, n(%) | 31 (50.8) | 15 (40.5) | 16 (66.7) | 0.01 |
|
NVC PATTERN, n(%) Aspecific alterations Early pattern Active pattern Late pattern |
7 (11.5) 34 (55.7) 14 (23.0) 6 (9.8) |
5 (13.5) 23 (62.2) 9 (24.3) 0 (0) |
2 (8.3) 11 (45.8) 5 (20.8) 6 (25.0) |
0.69 0.29 1.0 0.002 |
| TREATMENT, n(%) | ||||
| Iloprost | 44 (72.1) | 23 (62.2) | 21 (87.5) | 0.04 |
| Calcium Channel Blockers | 20 (32.7) | 8 (21.6) | 12 (50.0) | 0.03 |
| Low-dose Aspirin | 39 (63.9) | 23 (62.2) | 16 (66.7) | 0.78 |
| ACE-I/ARBs | 16 (26.2) | 6 (16.2) | 10 (41.7) | 0.04 |
| Beta-Blockers | 4 (6.6) | 2 (5.3) | 2 (8.3) | 0.64 |
| Diuretics | 1 (1.6) | 1 (2.7) | 0 | 1.0 |
| Hydroxychloroquine | 20 (32.7) | 9 (24.3) | 11 (45.8) | 0.09 |
| Immunosuppressants | 3 (4.9) | 1 (2.7) | 2 (8.3) | 0.56 |
Acronyms: n=number; %=percentage; SD= Standard Deviation; e-VEDOSS= early very early diagnosis of Systemic Sclerosis; ml-VEDOSS=mild longstanding very early diagnosis of Systemic Sclerosis; RP= Raynaud’s Phenomenon; ANA=antinuclear antibodies; ACE-I=Angiotensin Converting Enzyme Inhibitors; Angiotensin Receptor Blockers; ns=not significant; Kg=Kilograms; m2=square meters, NVC= Nailfold Videocapillaroscopy.
Table 2.
Echocardiographic findings across the entire population.
| ECHOCARDIOGRAPHIC PARAMETERS | TOTAL n=61 |
|---|---|
| E deceleration time (m/s), mean±SD | 244.3±281.7 |
| E/E’ ratio, mean±SD | 6.9±1.9 |
| E wave, (m/s), mean±SD | 0.69±0.17 |
| A wave, (m/s), mean±SD | 0.75±0.19 |
| E/A ratio, mean±SD | 0.99±0.39 |
| E/A ratio < 1.0, n (%) | 37 (60.7) |
| LVED diameter, (mm), mean±SD | 40.3±4.8 |
| PWED thickness, (mm), mean±SD | 8.4±1.6 |
| PWED > 9 mm, n(%) | 19 (31.1) |
| IVS thckness, (mm), mean±SD | 9.3±1.8 |
| IVS > 10 mm, n (%) | 17 (27.9) |
| LVED volume 4CH Simpson, (ml), mean±SD | 67.7±16.6 |
| LVES volume 4CH Simpson, (ml), mean±SD | 25.5±11.8 |
| LVED volume 4CH AL, (ml/m2), mean±SD | 43.4±8.8 |
| LVES volume 4CH AL, (ml/m2), mean±SD | 14.7±4.3 |
| EF%, mean±SD | 64.5±4.8 |
| EF%<55% | 3 (4.9) |
| Mass ASE, (g), mean±SD | 123.2±123.9 |
| Mass/BSA, (g/m2), mean±SD | 66.3±17.3 |
| Relative wall thickness, mean±SD | 0.44±0.10 |
| Mass/height, (g/m), mean±SD | 65.8±18.2 |
| Aortic diameter, (mm2), mean±SD | 29.7±3.9 |
| LAES area, (cm2), mean±SD | 15.6±3.6 |
| LAES 4CH Simpson, (ml), mean±SD | 40.4±13.7 |
| LAES 4CH ind, (ml/m2), mean±SD | 24.4±7.5 |
| LAES diameter sup-inf 4CH, (mm/m2), mean±SD | 46.5±7.6 |
| RAES diameter AL, (mm), mean±SD | 46.1±5.8 |
| RAES 4CH Simpson, (ml), mean±SD | 30.3±8.9 |
| RAES 4CH ind, (ml/m2), mean±SD | 18.5±5.0 |
| RAES area, (cm2), mean±SD | 13.5±3.1 |
| TAPSE, (mmHg), mean±SD | 21.5±3.0 |
| TAPSE < 22 mmHg, n (%) | 36 (59.0) |
| TAPSE < 16 mmHg, n (%) | 1 (1.6) |
| TAPSE/sPAP, mean±SD | 0.72±0.32 |
| TAPSE/sPAP < 0.55, n (%) | 1 (1.6) |
| sPAP, (mmHg), mean±SD | 27.2±5.3 |
| Tricuspid maximum regurgitation gradient, (mmHg), mean±SD | 22.2±6.5 |
| Mitral Valve Insufficiency, n (%) | 42 (68.9) |
| Mitral Valve Sclerosis, n (%) | 25 (40.9) |
| Tricuspid Valve Insufficiency, n (%) | 33 (54.1) |
| Aortic Valve Insufficiency, n (%) | 13 (21.3) |
| Aortic Valve Sclerosis, n (%) | 11 (18.0) |
| Pericardial Effusion, n (%) | 4 (6.6) |
Acronyms: SD= Standard deviation. ACA= Anti-centromere autoantibodies; ATA= Anti Topoisomerase I autoantibodies; E wave= early diastolic filling velocity of the left ventricle; E’= early diastolic tissue velocity of the mitral annulus; A=late diastolic filling velocity; LVED= Left ventricular end diastolic; LVES= Left ventricular end systolic; PWED=Posterior wall end diastolic; IVS=Interventricular septum; LAES= Left atrial end systolic; RAES= Right Atrial End Systolic; TAPSE= Tricuspid Annular Plane Systolic Excursion; sPAP= systolic Pulmonary Artery Pressure; 4CH=4 chamber; AL=anterolateral; EF= ejection fraction; %= percentage; BSA=Body Surface Area; ASE= American Society of echocardiography; ind= indexed; sup-inf= superior—inferior; m/s= meter/seconds; mm= millimeters; g= grams; g/m2= grams/square meters; cm2= square centimeters; mmHg= millimeters of mercury.
Table 3.
Echocardiographic findings among intergroups analysis.
| Late pattern N=6 |
No late pattern N=55 |
p-value |
ACA/ATA+ N=24 |
ACA/ATA- N=37 |
p-value |
Puffy Hands N=18 |
No Puffy hands N=43 |
p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| E deceleration time (m/s), mean±SD | 225-2±46-1 | 246.7±298.9 | 0.86 | 213.4±56.2 | 261.6±349.9 | 0.55 | 230.5±52.8 | 194.4±47.9 | 0.02 |
| E/E’ ratio, mean±SD | 7.55±1.37 | 6.92±1.90 | 0.52 | 7.6±1.8 | 6.7±1.8 | 0.12 | 7.0±1.3 | 6.8±1.9 | 0.77 |
| E wave, (m/s), mean±SD | 0.70±0.22 | 0.68±0.16 | 0.86 | 0.71±0.17 | 0.65±0.17 | 0.27 | 0.68±0.19 | 0.69±0.16 | 0.78 |
| A wave, (m/s), mean±SD | 0.81±0.17 | 0.75±0.19 | 0.46 | 0.84±0.20 | 0.70±0.15 | 0.006 | 0.79±0.20 | 0.74±0.18 | 0.38 |
| E/A ratio, mean±SD | 0.92±0.40 | 1.0±0.39 | 0.61 | 0.84±0.27 | 1.08±042 | 0.02 | 0.92±0.4 | 1.02±0.39 | 0.39 |
| E/A ratio < 1.0, n (%) | 3 (50) | 34 (61.8) | 0.12 | 18 (75) | 19 (51.4) | 0.11 | 10 (55.6) | 27 (62.8) | 0.77 |
| LVED diameter, (mm), mean±SD | 38.5±3.6 | 40.5±4.9 | 0.34 | 39.4±5.6 | 40.8±4.4 | 0.45 | 40.2±6.2 | 40.4±4.07 | 0.86 |
| PWED thickness, (mm), mean±SD | 8.4±1.5 | 8.3±1.6 | 0.89 | 8.6±1.2 | 8.2±1.8 | 0.31 | 8.5±1.5 | 8.3±1.7 | 0.63 |
| PWED > 9 mm, n(%) | 4 (66.7) | 13 (23.6) | 0.04 | 9 (37.5) | 8 (21.6) | 0.24 | 8 (44.4) | 9 (20.9) | 0.11 |
| IVS thckness, (mm), mean±SD | 9.9±1.6 | 9.3±1.8 | 0.37 | 9.9±1.3 | 8.9±1.9 | 0.03 | 9.4±1.6 | 9.4±2.0 | 0.90 |
| IVS > 10 mm, n (%) | 2 (33.3) | 20 (36.4) | 0.39 | 10 (41.7) | 12 (32.4) | 0.58 | 6 (33.3) | 16 (37.2) | 1.0 |
| LVED volume 4CH Simpson, (ml), mean±SD | 69.7±22.2 | 67.5±16.1 | 0.76 | 66.9±17.3 | 68.3±16.4 | 0.75 | 24.8±3.5 | 85.3±363.2 | 0.49 |
| LVES volume 4CH Simpson, (ml), mean±SD | 24.8±9.7 | 25.6±12.1 | 0.88 | 24.0±9.9 | 26.4±12.8 | 0.46 | 68.3±17.8 | 68.7±16.3 | 0.93 |
| LVED volume 4CH AL, (ml/m2), mean±SD | 41.3±12.4 | 43.6±8.4 | 0.88 | 41.7±10.3 | 44.3±7.8 | 0.29 | 25.7±10.9 | 26.0±12.7 | 0.92 |
| LVES volume 4CH AL, (ml/m2), mean±SD | 14.8±5.6 | 14.7±4.2 | 0.54 | 14.7±6.2 | 14.7±2.9 | 0.92 | 43.1±10.5 | 44.3±8.2 | 0.64 |
| EF%, mean±SD | 64.5±6.8 | 64.6±4.6 | 0.92 | 64.9±5.7 | 64.4±4.3 | 0.64 | 15.6±6.2 | 14.6±3.2 | 0.42 |
| EF%<55% | 1 (16.7) | 2 (3.6) | 0.27 | 2 (8.3) | 1 (2.7) | 0.55 | 2 (11.1) | 1 (2.3) | 0.21 |
| Mass ASE, (g), mean±SD | 108.3±30.9 | 124.9±130.8 | 0.96 | 129.1±153.4 | 112±30.3 | 0.63 | 63.5±5.7 | 65.1±4.5 | 0.26 |
| Mass/BSA, (g/m2), mean±SD | 65.5±17.0 | 66.4±17.0 | 0.90 | 68.8±17.4 | 64.9±17.4 | 0.42 | 163.3±217.5 | 107.3±36.9 | 0.14 |
| Relative wall thickness, mean±SD | 0.48±0.08 | 0.44±0.1 | 0.35 | 0.48±0.09 | 0.42±0.10 | 0.04 | 68.3±19.5 | 66.5±17.0 | 0.73 |
| Mass/height, (g/m), mean±SD | 69.2±21.8 | 65.5±17.9 | 0.64 | 68.1±20.3 | 64.7±17.2 | 0.51 | 0.45±0.12 | 0.44±0.09 | 0.65 |
| Aortic diameter, (mm2), mean±SD | 29.7±2.4 | 29.6±4.1 | 0.96 | 29.7±3.7 | 29.6±4.1 | 0.94 | 65.3+20.6 | 67.5±17.8 | 0.68 |
| LAES area, (cm2), mean±SD | 16.1±2.7 | 15.6±3.7 | 0.75 | 16.7±4.1 | 15.1±3.2 | 0.11 | 28.5±2.5 | 30.0±4.3 | 0.19 |
| LAES 4CH Simpson, (ml), mean±SD | 41.6±10.5 | 40.3±14.3 | 0.83 | 46.7±18.7 | 37.2±8.9 | 0.01 | 15.4±3.3 | 16.1±3.8 | 0.52 |
| LAES 4CH ind, (ml/m2), mean±SD | 24.6±5.7 | 24.4±7.8 | 0.95 | 27.7±10.2 | 22.6±5.1 | 0.01 | 42.3±13.2 | 40.8±14.2 | 0.73 |
| LAES diameter 4CH, (mm/m2), mean±SD | 50.3±5.8 | 46.1±8.1 | 0.27 | 49.7±5.9 | 45.0±8.4 | 0.04 | 25.6±8.3 | 24.6±7.3 | 0.68 |
| RAES diameter AL, (mm), mean±SD | 47.2±1.7 | 46.0±6.1 | 0.74 | 47.8±45.4 | 45.4±5.8 | 0.22 | 46.9±6.0 | 46.7±9.1 | 0.91 |
| RAES 4CH Simpson, (ml), mean±SD | 32.9±9.6 | 30.0±8.9 | 0.55 | 30.1±8.1 | 30.5±9.5 | 0.91 | 44.8±4.5 | 47.0±6.2 | 0.27 |
| RAES 4CH ind, (ml/m2), mean±SD | 19.1±5.4 | 18.4±5.1 | 0.78 | 18.5±3.6 | 18.5±5.6 | 0.98 | 28.4±7.9 | 31.7±9.5 | 0.33 |
| RAES area, (cm2), mean±SD | 13.8±2.5 | 13.5±3.2 | 0.83 | 14.4±2.9 | 13.0±3.2 | 0.12 | 17.9±4.8 | 18.9±5.4 | 0.59 |
| TAPSE, (mmHg), mean±SD | 22.0±4.9 | 21.5±2.9 | 0.70 | 21.9±3.7 | 21.4±2.7 | 0.61 | 13.1±2.2 | 13.8±3.6 | 0.43 |
| TAPSE < 22 mmHg, n (%) | 4 (66.7) | 32 (58.2) | 1.0 | 14 (58.3) | 22 (59.4) | 1.0 | 12 (66.7) | 23 (53.5) | 0.40 |
| TAPSE < 16 mmHg, n (%) | 0 (0) | 1 (1.8) | 1.0 | 1 (4.2) | 0 (0) | 0.39 | 0 (0) | 1 (2.3) | 1.0 |
| TAPSE/sPAP, mean±SD | 0.98±0.31 | 0.69±0.32 | 0.24 | 0.71±0.38 | 0.72±0.29 | 0.92 | 21.8±3.3 | 21.3±2.8 | 0.59 |
| TAPSE/sPAP < 0.55, n (%) | 1 (16.7) | 3 (5.5) | 0.35 | 1 (4.2) | 3 (8.1) | 1.0 | 1 (5.6) | 3 (7.0) | 1.0 |
| sPAP, (mmHg), mean±SD | 28.0±4.2 | 27.1±5.5 | 0.83 | 26.7±4.4 | 27.7±6.2 | 0.63 | 0.7+±.36 | 0.69±0.33 | 0.29 |
| Tricuspid maximum regurgitation gradient, (mmHg), mean±SD | 21.9±3.4 | 22.2±6.7 | 0.93 | 22.4±4.8 | 22.1±7.4 | 0.88 | 27.7±3.9 | 26.8±6.3 | 0.75 |
| Mitral Valve Insufficiency, n (%) | 5 (83.3) | 37 (67.3) | 0.66 | 21 (87.5) | 21 (56.8) | 0.01 | 12 (66.7) | 30 (69.8) | 1.0 |
| Mitral Valve Sclerosis, n (%) | 3 (50) | 22 (40) | 0.68 | 17 (70.8) | 8 (21.6) | <0.001 | 9 (50) | 16 (37.2) | 0.40 |
| Tricuspid Valve Insufficiency, n (%) | 3 (50) | 30 (54.5) | 1.0 | 15 (62.5) | 18 (48.6) | 0.31 | 10 (55.6) | 23 (53.5) | 1.0 |
| Aortic Valve Insufficiency, n (%) | 4 (66.7) | 10 (18.2) | 0.02 | 10 (41.7) | 4 (10.8) | 0.01 | 5 (27.8) | 9 (20.9) | 0.74 |
| Aortic Valve Sclerosis, n (%) | 4 (66.7) | 9 (16.4) | 0.01 | 9 (37.5) | 4 (10.8) | 0.02 | 5 (27.8) | 8 (18.6) | 0.49 |
| Pericardial Effusion, n (%) | 0 (0) | 4 (7.3) | 1.0 | 1 (4.2) | 3 (8.1) | 1.0 | 2 (11.1) | 2 (4.7) | 0.57 |
Acronyms: SD= Standard deviation. ACA= Anti-centromere autoantibodies; ATA= Anti Topoisomerase I autoantibodies; E wave= early diastolic filling velocity of the left ventricle; E’= early diastolic tissue velocity of the mitral annulus; A=late diastolic filling velocity; LVED= Left ventricular end diastolic; LVES= Left ventricular end systolic; PWED=Posterior wall end diastolic; IVS=Interventricular septum; LAES= Left atrial end systolic; RAES= Right Atrial End Systolic; TAPSE= Tricuspid Annular Plane Systolic Excursion; sPAP= systolic Pulmonary Artery Pressure; 4CH=4 chamber; AL=anterolateral; EF= ejection fraction; %= percentage; BSA=Body Surface Area; ASE= American Society of echocardiography; ind= indexed; sup-inf= superior—inferior; m/s= meter/seconds; mm= millimeters; g= grams; g/m2= grams/square meters; cm2= square centimeters; mmHg= millimeters of mercury.
Table 4.
Echocardiographic findings across patients undergoing vasodilators compared to those not receiving vasodilators.
Table 4.
Echocardiographic findings across patients undergoing vasodilators compared to those not receiving vasodilators.
| Echocardiographic parameters | Iloprost iv N=25 |
CCBs N=8 |
Iloprost+CCBs N=18 |
No Vasodilators N=13 |
|
|---|---|---|---|---|---|
| E deceleration time (m/s), mean±SD | 295.0±422.8 | 176.7±40.7 | 203.6±62.8 | 220.9±49.7 | 0.74 |
| E/E’ ratio, mean±SD | 7.3±2.1 | 7.8±2.8 | 6.8±1.8 | 6.6±1.1 | 0.71 |
| E wave, (m/s), mean±SD | 0.67±0.18 | 0.68±0.22 | 0.68±0.15 | 0.77±0.23 | 0.59 |
| E/A ratio, mean±SD | 1.08±0.44 | 0.92±0.35 | 0.85±0.21 | 1.0±0.46 | 0.32 |
| LVED diameter, (mm), mean±SD | 40.6±5.1 | 42.5±7.4 | 39.6±4.4 | 40.4±5.0 | 0.72 |
| PWED thickness, (mm), mean±SD | 8.2±1.9 | 8.7±0.8 | 8.2±0.9 | 8.7±2.1 | 0.75 |
| IVS thckness, (mm), mean±SD | 9.3±1.8 | 8.9±1.4 | 9.5±1.4 | 9.3±2.6 | 0.93 |
| LVED volume 4CH Simpson, (ml), mean±SD | 67.5±13.8 | 54.1±31.5 | 67.8±15.3 | 73.8±14.6 | 0.17 |
| LVES volume 4CH Simpson, (ml), mean±SD | 23.7±6.5 | 47.2±35.1 | 23.8±6.0 | 24.6±7.4 | 0.001 |
| LVED volume 4CH AL, (ml/m2), mean±SD | 42.8±9.8 | 41.4±8.4 | 42.1±8.7 | 46.9±7.1 | 0.46 |
| LVES volume 4CH AL, (ml/m2), mean±SD | 14.5±3.6 | 16.5±12.9 | 14.4±3.5 | 15.3±4.0 | 0.84 |
| EF%, mean±SD | 64.9±4.4 | 59.6±6.7 | 65.1±5.0 | 65.2±4.2 | 0.12 |
| Mass ASE, (g), mean±SD | 109.3±33.5 | 95.9±60.3 | 160.1±217.4 | 109.1±42.2 | 0.56 |
| Mass/BSA, (g/m2), mean±SD | 66.1±16.8 | 71.9±21.4 | 65.0±13.5 | 68.1±23.4 | 0.89 |
| Relative wall thickness, mean±SD | 0.44±0.11 | 0.45±0.10 | 0.46±0.08 | 0.44±0.13 | 0.93 |
| Mass/height, (g/m), mean±SD | 67.4±20.8 | 57.0±21.1 | 66.9±14.4 | 66.7±18.9 | 0.78 |
| Aortic diameter, (mm2), mean±SD | 30.8±2.9 | 26.9±4.8 | 28.9±4.7 | 29.3±4.1 | 0.27 |
| LAES area, (cm2), mean±SD | 14.4±2.4 | 15.5±4.1 | 16.3±3.8 | 17.0±4.7 | 0.16 |
| LAES 4CH Simpson, (ml), mean±SD | 36.1±8.1 | 41.0±19.8 | 44.7±16.3 | 42.1±16.3 | 0.26 |
| LAES 4CH ind, (ml/m2), mean±SD | 21.6±4.3 | 25.5±11.4 | 26.9±8.3 | 26.0±9.8 | 0.14 |
| LAES diameter 4CH, (mm/m2), mean±SD | 45.8±5.9 | 46.9±5.8 | 48.5±6.2 | 44.0±13.7 | 0.54 |
| RAES diameter AL, (mm), mean±SD | 45.1±5.9 | 40.5±6.1 | 48.7±5.3 | 46.2±5.4 | 0.12 |
| RAES 4CH Simpson, (ml), mean±SD | 31.2±8.4 | 14.1±6.5 | 26.5±5.4 | 30.2±9.1 | 0.005 |
| RAES 4CH ind, (ml/m2), mean±SD | 18.1±5.1 | 12.4±6.7 | 21.7±4.5 | 16.6±2.1 | 0.01 |
| RAES area, (cm2), mean±SD | 13.4±3.6 | 12.1±3.0 | 14.8±3.1 | 12.6±1.9 | 0.24 |
| TAPSE, (mmHg), mean±SD | 20.8±2.9 | 20.9±3.1 | 21.3±2.7 | 22.9±3.3 | 0.29 |
| TAPSE/sPAP, mean±SD | 0.79±0.33 | 0.31±0.44 | 0.76±0.10 | 0.65±0.39 | 0.28 |
| sPAP, (mmHg), mean±SD | 25.1±4.8 | 24.5±6.4 | 29.5±6.1 | 29.4±3.6 | 0.21 |
| Tricuspid maximum regurgitation gradient, (mmHg), mean±SD | 21.0±4.6 | 20.4±6.2 | 24.5±4.9 | 21.6±11.3 | 0.23 |
Acronyms: iv= intravenous; CCB= Calcium Channel Blockers; SD= Standard deviation. E wave= early diastolic filling velocity of the left ventricle; E’= early diastolic tissue velocity of the mitral annulus; A=late diastolic filling velocity; LVED= Left ventricular end diastolic; LVES= Left ventricular end systolic; PWED=Posterior wall end diastolic; IVS=Interventricular septum; LAES= Left atrial end systolic; RAES= Right Atrial End Systolic; TAPSE= Tricuspid Annular Plane Systolic Excursion; sPAP= systolic Pulmonary Artery Pressure; 4CH=4 chamber; AL=anterolateral; EF= ejection fraction; %= percentage; BSA=Body Surface Area; ASE= American Society of echocardiography; ind= indexed; sup-inf= superior—inferior; m/s= meter/seconds; mm= millimeters; g= grams; g/m2= grams/square meters; cm2= square centimeters; mmHg= millimeters of mercury.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



