
Submitted:
31 December 2024
Posted:
03 January 2025
You are already at the latest version
Abstract
Background/Objectives: Cryptogenic stroke, a challenging subtype of acute ischemic stroke (AIS), is characterized by the absence of an identifiable etiology despite thorough diagnostic assessment. The role of pre-admission antiplatelet therapy (APT) in this population remains poorly understood, as current guidelines are primarily based on evidence from other stroke subtypes. Therefore, this study investigates the impact of pre-admission APT on functional outcomes in pa-tients with cryptogenic stroke.
Methods: A total of 224 patients with cryptogenic stroke admitted to the University of Pécs between February 2023 and September 2024 was retrospectively analyzed. Propensity score matching (PSM) with sensitivity analysis was employed to balance baseline characteristics, resulting in a matched cohort of 122 patients. Logistic regression and mediation analysis were used to evaluate the association between pre-admission APT and favorable outcome at 90 days, defined as a modified Rankin Scale (mRS) score of 0–2.
Results: A favorable outcome was achieved by 39.3% of patients with pre-admission APT (n = 61), compared to 61.7% of those not receiving pre-admission APT (n = 162) (odds ratio [OR] = 0.40, 95% confidence interval [CI]: 0.22–0.74, p = 0.004). After PSM and adjusting for confounders, including pre-morbidity mRS (pre-mRS) (p < 0.001), National Institutes of Health Stroke Scale (NIHSS) at 72 hours post-stroke (p = 0.004), and smoking status (p = 0.025), pre-admission APT remained associated with poorer functional outcomes (adjusted OR [aOR] = 0.21, 95% CI: 0.06–0.76, p = 0.018).
Conclusions: Pre-admission APT is independently associated with poorer functional outcomes in cryptogenic stroke patients. These findings challenge traditional assumptions regarding APTs protective role and highlight the need for prospective studies to refine its use in cryptogenic stroke management.
Keywords:
pre-admission antiplatelet therapy
; cryptogenic stroke
; 90-day mRS
1. Introduction
Cryptogenic strokes, accounting for approximately 25-40% of acute ischemic strokes (AIS) [1,2,3], present a significant challenge in modern neurology. Unlike other ischemic stroke subtypes with well-defined causes, cryptogenic strokes are diagnosed in the absence of an identifiable etiology despite extensive diagnostic evaluation [4]. This diagnostic uncertainty complicates secondary prevention strategies, which therefore often rely on generalized guidelines rather than targeted, etiology-specific interventions [5].
Pre-admission antiplatelet therapy (APT) introduces additional complexity to this already challenging scenario. While APT remains the standard prevention method to reduce thrombotic risk in individuals with prior non-cardioembolic ischemic events [5,6], its impact on functional outcomes in patients who experience a cryptogenic stroke remains poorly understood. Studies comparing APT to anticoagulation therapy in patients with cryptogenic stroke, including embolic stroke of undetermined source (ESUS), have found both approaches to be similarly ineffective in preventing recurrent strokes, calling into question the overall efficacy of APT in this population [7,8]. Moreover, cryptogenic stroke patients frequently lack the traditional risk profiles observed in other stroke subtypes [9,10], raising concerns that pre-admission APT may inadvertently contribute to poorer functional outcomes.
This study investigates the association between pre-admission APT and 90-day functional outcomes in cryptogenic stroke patients. By examining this relationship, the findings aim to shed light on the complex role of pre-admission APT in this population and address critical gaps in understanding its impact on post-stroke recovery. These insights could contribute to the development of more targeted clinical guidelines for managing cryptogenic stroke patients with prior APT use.
2. Materials and Methods
2.1. Study Design and Patient Population
This retrospective study was conducted using data from the prospective Transzlációs Idegtudományi Nemzeti Laboratórium (TINL) STROKE-registry. The study included 236 patients with cryptogenic stroke who were admitted to the Department of Neurology, University of Pécs, between February 2023 and September 2024. Cryptogenic stroke was defined as “an imaging-confirmed stroke with unknown source despite thorough diagnostic assessment” [4,5]. Patients were included in the absence of evidence for cardioembolism, large artery atherosclerosis (stenosis >50%), small vessel disease or atrial fibrillation detected on a 12-lead echocardiogram (ECG) or 24-hour cardiac monitoring. Additionally, patients who died before completing the diagnostic work-up (n = 12) were excluded to ensure that a full standard evaluation could be conducted, resulting in a final cohort of 224 patients.
2.2. Data Collection and Measurements
Baseline characteristics included demographic data (age and sex) and clinical variables, such as pre-morbidity modified Rankin Scale (pre-mRS) scores and stroke severity, assessed using the National Institutes of Health Stroke Scale (NIHSS) at admission and 72 hours post-stroke. Additionally, recorded factors included the classification of cryptogenic stroke subtypes (e.g. ESUS), onset-to-door times and admission plasma glucose levels. Vascular risk factors (current smoking, alcohol use and prior stroke history) and comorbidities, such as hypertension and diabetes mellitus were also documented. Furthermore, treatment modalities for cryptogenic stroke (thrombolysis [TL], mechanical thrombectomy [MT], or combined therapy [TL + MT]) were recorded.
2.3. Outcome Measures
The primary endpoint of the study was a favorable functional outcome at 90 days, defined as a modified Rankin Scale (mRS) score of 0–2. Outcomes were evaluated through telephone interviews conducted by a physician or a certified neurology nurse 90 days post-admission.
2.4. Statistical Analyses
Data analysis was performed using Python (version 3.13.0). Baseline characteristics between the groups were compared using Fisher’s exact test or test for categorical variables (reported as fractions and percentages) and independent samples t-tests for continuous variables (reported as means ± standard deviations [SD]).
Propensity score matching (PSM) was performed using a nearest-neighbor approach to minimize baseline differences between patients receiving pre-admission APT (n = 61) and those not receiving pre-admission APT (n = 162). A caliper width of 0.1 was applied to ensure rigorous matching of patients with highly similar propensity scores, thereby reducing residual confounding. Following matching, 122 patients were included in the final cohort for outcome analysis.
Logistic regression was used to estimate the adjusted odds of achieving a favorable functional outcome, with results reported as odds ratios (OR) and 95% confidence intervals (CI). Mediation analysis was employed to evaluate the potential indirect effects of prior stroke history as a mediator between pre-admission APT and functional outcomes. The analysis decomposed the total effect into direct and indirect effects. For all statistical analyses, significance was defined as a p-value < 0.05.
3. Results
3.1. Baseline Characteristics
Before matching, patients with pre-admission APT (n = 61) were older (mean age 69.87 ± 11.20 years vs. 64.76 ± 13.26 years, p = 0.005), more likely to have a history of prior stroke (29.5% vs. 2.5%, p < 0.001), hypertension (86.9% vs. 72.8%, p = 0.042), and diabetes mellitus (41.0% vs. 21.0%, p = 0.004) than patients without pre-admission APT (n = 162) (Table 1).
3.2. Propensity Score Matching and Sensitivity Analysis
After PSM, 122 patients (n = 61 with pre-admission APT and n = 61 without pre-admission APT) were included in the final cohort. As shown in Table 1 and Figure 1, baseline characteristics were well balanced between the groups, with standardized mean differences (SMD) for all covariates below 0.1, indicating minimal residual confounding. Sensitivity analyses using stricter propensity score calipers (0.1) confirmed the robustness of the findings, with results consistent with the primary analysis.
3.3. Functional Outcomes
Before matching, the unadjusted analysis revealed that pre-admission APT was significantly associated with lower odds of achieving a favorable functional outcome (OR = 0.40, 95% CI: 0.22–0.74, p = 0.004): Only 39.3% of patients receiving pre-admission APT achieved a favorable outcome, compared to 61.7% of patients without pre-admission APT (Figure 2).
3.4. Logistic Regression and Mediation Analysis
As shown in Table 2, significant predictors of favorable outcome included lower pre-mRS score (OR = 0.17, 95% CI: 0.06–0.49, p < 0.001), lower NIHSS score at 72 hours post-stroke (OR = 0.67, 95% CI: 0.50–0.88, p = 0.004), and non-smoking status (OR = 0.14, 95% CI: 0.02–0.78, p = 0.025).
Notably, even after adjusting for confounders, pre-admission APT remained independently associated with unfavorable functional outcomes at 90 days (adjusted odds ratio [aOR] = 0.21, 95% CI: 0.06–0.76, p = 0.018, indicating that patients receiving pre-admission APT had a 79% lower chance of achieving a favorable functional outcome compared to those without pre-admission APT (Figure 3).
Mediation analysis indicated that a prior history of stroke was not a significant mediator of the relationship between pre-admission APT and unfavorable functional outcome (p = 0.684). Both the average direct effect (ADE) and average causal mediation effect (ACME) estimates are nonsignificant, as shown in Table 3. These results suggest that the association between pre-admission APT and unfavorable outcome is predominantly direct rather than mediated by prior stroke history.
4. Discussion
This study demonstrates that pre-admission APT is independently associated with poorer 90-day functional outcomes in cryptogenic stroke patients, raising important questions about the underlying mechanisms and its implications for clinical management.
4.1. Comparison to Current Literature
Existing literature indicates that approximately 50–60% of cryptogenic stroke patients achieve favorable long-term functional outcomes (mRS ≤2) [11,12,13,14], with lower or similar rates of functional dependency (mRS >2) compared to non-cardioembolic stroke patients at discharge or 6 months, respectively [9,15].
However, the role of pre-admission APT in these outcomes remains uncertain. Research in general stroke populations has yielded mixed results: while some studies report no significant influence on stroke severity, in-hospital mortality, or long-term recovery [16,17,18,19,20], others suggest modest functional benefits at discharge [21,22,23] and improved 3-month mRS scores in selected patient groups [24]. In contrast, our findings align with studies in patients undergoing MT, where pre-admission APT has been associated with poorer functional outcomes (OR = 2.36, 95% CI: 1.03–5.54, p = 0.04) [25].
4.2. Possible Explanations
The mechanisms through which APT influences ischemic stroke outcomes extend beyond platelet aggregation. While platelets are central to clot formation, they also play critical roles in inflammation, immune responses, tissue repair, and vascular integrity [26]. Consequently, platelet inhibitors not only prevent aggregation but also stabilize atherosclerotic plaques, promote vascular dilation, and mitigate oxidative stress and thrombus propagation [27]. However, these effects can act as a double-edged sword, providing protective benefits while also introducing potential complications during stroke recovery.
In certain cases, APT may predispose patients to worse outcomes, particularly in the presence of undiagnosed cerebrovascular abnormalities. Subclinical vascular damage, often undetected during routine evaluations, can increase microvascular fragility, elevating the risk of microbleeds and hemorrhagic transformation [28].
These adverse effects may be further amplified by systemic risk factors such as hypertension and diabetes mellitus, potentially worsening functional outcomes and hindering recovery [29].
4.3. Clinical Implications
These findings underline the need to critically reassess APT use in cryptogenic stroke patients. Current stroke prevention guidelines, primarily developed for broader ischemic stroke populations, may not fully address the unique complexities of cryptogenic stroke. Given the potential for both protective and detrimental effects, clinicians must carefully balance the risks and benefits of APT in this population.
Future research should focus on prospective trials to clarify the role of pre-admission APT in cryptogenic stroke and identify subgroups that might benefit from its use. Mechanistic studies are also needed to explore how APT interacts with vascular pathology and systemic risk factors, influencing post-stroke recovery.
Incorporating advanced diagnostic tools into routine care could further refine treatment strategies. For example, the use of magnetic resonance imaging (MRI) to detect microbleeds or subtle vascular abnormalities, alongside biomarkers of vascular damage, and extended cardiac monitoring to identify subclinical embolic sources could improve risk stratification. These advancements would enable the development of personalized therapeutic strategies that optimize functional outcomes while minimizing unnecessary risks.
4.4. Limitations
This study has several limitations that should be considered when interpreting the results. The retrospective design and modest sample size may limit generalizability, and while PSM was used to minimize observed confounding, the potential influence of unmeasured confounders cannot be entirely excluded.
The reliance on the mRS as the primary outcome measure, while widely accepted, may not fully capture the multidimensional aspects of functional recovery. Dichotomizing outcomes into 'favorable' and 'unfavorable' categories, while practical for analysis, risks oversimplifying the complexity of post-stroke recovery. Future studies should consider continuous measures or multidimensional scales that incorporate cognitive, emotional, and physical recovery to provide a more comprehensive assessment of outcomes.
Additionally, the 90-day follow-up period may not fully reflect the long-term recovery trajectory. Longer follow-up periods could reveal whether patients not receiving pre-admission APT eventually achieve comparable outcomes to those on APT, potentially indicating an accelerated progression of unfavorable outcomes in the latter group.
5. Conclusions
Pre-admission APT is independently associated with poorer 90-day functional outcomes in cryptogenic stroke patients. Future prospective studies are necessary to reevaluate the role of APT in this population and to investigate the underlying mechanisms driving this association.
Author Contributions
Conceptualization, J.S. and B.C.; methodology, J.S. and L.S.; validation, Z.N.K. and E.B.; formal analysis, J.S.; data curation, J.S.; writing—original draft preparation, J.S. and B.C.; writing—review and editing, Z.N.K. and E.B.; visualization, J.S.; supervision, L.S.; project administration, L.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Scientific and Research Ethics Committee of the Medical Research Council of the University of Pécs (RRF-2.3.1-21-2022-00011, 01/09/22) and re-approved by the Scientific and Research Ethics Committee of the Medical Research Council of Hungary (BM/22444-1/2024, 01/09/24).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article and further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
List of Abbreviations
| AIS | acute ischemic stroke |
| APT | antiplatelet therapy |
| PSM | propensity score matching |
| mRS | modified Rankin Scale |
| OR | odds ratio |
| CI | confidence interval |
| Pre-mRS | pre-morbidity modified Rankin Scale |
| NIHSS | National Institutes of Health Stroke Scale |
| aOR | adjusted odds ratio |
| ESUS | embolic stroke of undetermined source |
| TINL | Transzlációs Idegtudományi Nemzeti Laboratórium |
| ECG | electrocardiogram |
| TL | thromboylsis |
| MT | mechanical thrombectomy |
| SD | standard deviation |
| SMD | standardized mean difference |
| ADE | average direct effect |
| ACME | average causal mediation effect |
| MRI | magnetic resonance imaging |
References
- Lee, B.I.; Nam, H.S.; Heo, J.H.; Kim, D.I. Yonsei Stroke Registry. Cerebrovascular Diseases 2001, 12, 145–151. [CrossRef]
- Putaala, J.; Metso, A.J.; Metso, T.M.; Konkola, N.; Kraemer, Y.; Haapaniemi, E.; Kaste, M.; Tatlisumak, T. Analysis of 1008 Consecutive Patients Aged 15 to 49 With First-Ever Ischemic Stroke. Stroke 2009, 40, 1195–1203. [CrossRef]
- Ornello, R.; Degan, D.; Tiseo, C.; Di Carmine, C.; Perciballi, L.; Pistoia, F.; Carolei, A.; Sacco, S. Distribution and Temporal Trends From 1993 to 2015 of Ischemic Stroke Subtypes. Stroke 2018, 49, 814–819. [CrossRef]
- Saver, J.L. Cryptogenic Stroke. New England Journal of Medicine 2016, 374, 2065–2074. [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52. [CrossRef]
- Lansberg, M.G.; O’Donnell, M.J.; Khatri, P.; Lang, E.S.; Nguyen-Huynh, M.N.; Schwartz, N.E.; Sonnenberg, F.A.; Schulman, S.; Vandvik, P.O.; Spencer, F.A.; et al. Antithrombotic and Thrombolytic Therapy for Ischemic Stroke. Chest 2012, 141, e601S-e636S. [CrossRef]
- Hart, R.G.; Sharma, M.; Mundl, H.; Kasner, S.E.; Bangdiwala, S.I.; Berkowitz, S.D.; Swaminathan, B.; Lavados, P.; Wang, Y.; Wang, Y.; et al. Rivaroxaban for Stroke Prevention after Embolic Stroke of Undetermined Source. New England Journal of Medicine 2018, 378, 2191–2201. [CrossRef]
- Diener, H.-C.; Sacco, R.L.; Easton, J.D.; Granger, C.B.; Bernstein, R.A.; Uchiyama, S.; Kreuzer, J.; Cronin, L.; Cotton, D.; Grauer, C.; et al. Dabigatran for Prevention of Stroke after Embolic Stroke of Undetermined Source. New England Journal of Medicine 2019, 380, 1906–1917. [CrossRef]
- Li, L.; Yiin, G.S.; Geraghty, O.C.; Schulz, U.G.; Kuker, W.; Mehta, Z.; Rothwell, P.M. Incidence, Outcome, Risk Factors, and Long-Term Prognosis of Cryptogenic Transient Ischaemic Attack and Ischaemic Stroke: A Population-Based Study. Lancet Neurol 2015, 14, 903–913. [CrossRef]
- Bang, O.Y.; Lee, P.H.; Yeo, S.H.; Kim, J.W.; Joo, I.S.; Huh, K. Non-Cardioembolic Mechanisms in Cryptogenic Stroke: Clinical and Diffusion-Weighted Imaging Features. Journal of Clinical Neurology 2005, 1, 50. [CrossRef]
- Arsava, E.M.; Helenius, J.; Avery, R.; Sorgun, M.H.; Kim, G.-M.; Pontes-Neto, O.M.; Park, K.Y.; Rosand, J.; Vangel, M.; Ay, H. Assessment of the Predictive Validity of Etiologic Stroke Classification. JAMA Neurol 2017, 74, 419. [CrossRef]
- Grau, A.J.; Weimar, C.; Buggle, F.; Heinrich, A.; Goertler, M.; Neumaier, S.; Glahn, J.; Brandt, T.; Hacke, W.; Diener, H.-C. Risk Factors, Outcome, and Treatment in Subtypes of Ischemic Stroke: The German Stroke Data Bank. Stroke 2001, 32, 2559–2566. [CrossRef]
- Bang, O.Y.; Lee, P.H.; Joo, S.Y.; Lee, J.S.; Joo, I.S.; Huh, K. Frequency and Mechanisms of Stroke Recurrence after Cryptogenic Stroke. Ann Neurol 2003, 54, 227–234. [CrossRef]
- Ntaios, G.; Papavasileiou, V.; Milionis, H.; Makaritsis, K.; Vemmou, A.; Koroboki, E.; Manios, E.; Spengos, K.; Michel, P.; Vemmos, K. Embolic Strokes of Undetermined Source in the Athens Stroke Registry. Stroke 2015, 46, 2087–2093. [CrossRef]
- Prabhakaran, S.; Messé, S.R.; Kleindorfer, D.; Smith, E.E.; Fonarow, G.C.; Xu, H.; Zhao, X.; Lytle, B.; Cigarroa, J.; Schwamm, L.H. Cryptogenic Stroke. Neurol Clin Pract 2020, 10, 396–405. [CrossRef]
- Silimon, N.; Drop, B.; Clénin, L.; Nedeltchev, K.; Kahles, T.; Tarnutzer, A.A.; Katan, M.; Bonati, L.; Salmen, S.; Albert, S.; et al. Ischaemic Stroke despite Antiplatelet Therapy: Causes and Outcomes. Eur Stroke J 2023, 8, 692–702. [CrossRef]
- Sylaja, P.; Nair, S.S.; Pandian, J.; Khurana, D.; Srivastava, M.V.P.; Kaul, S.; Arora, D.; Sarma, P.S.; Singhal, A.B. Impact of Pre-Stroke Antiplatelet Use on 3-Month Outcome After Ischemic Stroke. Neurol India 2021, 69, 1645–1649. [CrossRef]
- Couture, M.; Finitsis, S.; Marnat, G.; Richard, S.; Bourcier, R.; Constant-dits-Beaufils, P.; Dargazanli, C.; Arquizan, C.; Mazighi, M.; Blanc, R.; et al. Impact of Prior Antiplatelet Therapy on Outcomes After Endovascular Therapy for Acute Stroke: Endovascular Treatment in Ischemic Stroke Registry Results. Stroke 2021, 52, 3864–3872. [CrossRef]
- Merlino, G.; Sponza, M.; Gigli, G.L.; Lorenzut, S.; Vit, A.; Gavrilovic, V.; Pellegrin, A.; Cargnelutti, D.; Valente, M. Prior Use of Antiplatelet Therapy and Outcomes after Endovascular Therapy in Acute Ischemic Stroke Due to Large Vessel Occlusion: A Single-Center Experience. J Clin Med 2018, 7, 518. [CrossRef]
- van de Graaf, R.A.; Zinkstok, S.M.; Chalos, V.; Goldhoorn, R.-J.B.; Majoie, C.B.; van Oostenbrugge, R.J.; van der Lugt, A.; Dippel, D.W.; Roos, Y.B.; Lingsma, H.F.; et al. Prior Antiplatelet Therapy in Patients Undergoing Endovascular Treatment for Acute Ischemic Stroke: Results from the MR CLEAN Registry. International Journal of Stroke 2021, 16, 476–485. [CrossRef]
- Xian, Y.; Federspiel, J.J.; Grau-Sepulveda, M.; Hernandez, A.F.; Schwamm, L.H.; Bhatt, D.L.; Smith, E.E.; Reeves, M.J.; Thomas, L.; Webb, L.; et al. Risks and Benefits Associated With Prestroke Antiplatelet Therapy Among Patients With Acute Ischemic Stroke Treated With Intravenous Tissue Plasminogen Activator. JAMA Neurol 2016, 73, 50. [CrossRef]
- Sohn, J.-H.; Kim, C.; Sung, J.H.; Han, S.-W.; Minwoo Lee; Oh, M.S.; Yu, K.-H.; Kim, Y.; Park, S.-H.; Lee, S.-H. Effect of Pre-Stroke Antiplatelet Use on Stroke Outcomes in Acute Small Vessel Occlusion Stroke with Moderate to Severe White Matter Burden. J Neurol Sci 2024, 456, 122837. [CrossRef]
- Sanossian, N.; Saver, J.L.; Rajajee, V.; Selco, S.L.; Kim, D.; Razinia, T.; Ovbiagele, B. Premorbid Antiplatelet Use and Ischemic Stroke Outcomes. Neurology 2006, 66, 319–323. [CrossRef]
- Huo, X.; R.; Jing, J.; Wang, A.; Mo, D.; Gao, F.; Ma, N.; Wang, Y.; Wang, Y.; Miao, Z. Safety and Efficacy of Oral Antiplatelet for Patients Who Had Acute Ischaemic Stroke Undergoing Endovascular Therapy. Stroke Vasc Neurol 2021, 6, 230–237. [CrossRef]
- Krieger, P.; Melmed, K.R.; Torres, J.; Zhao, A.; Croll, L.; Irvine, H.; Lord, A.; Ishida, K.; Frontera, J.; Lewis, A. Pre-Admission Antithrombotic Use Is Associated with 3-Month MRS Score after Thrombectomy for Acute Ischemic Stroke. J Thromb Thrombolysis 2022, 54, 350–359. [CrossRef]
- SMYTH, S.S.; MCEVER, R.P.; WEYRICH, A.S.; MORRELL, C.N.; HOFFMAN, M.R.; AREPALLY, G.M.; FRENCH, P.A.; DAUERMAN, H.L.; BECKER, R.C. Platelet Functions beyond Hemostasis. Journal of Thrombosis and Haemostasis 2009, 7, 1759–1766. [CrossRef]
- Dowlatshahi, D.; Hakim, A.; Fang, J.; Sharma, M. Pre Admission Antithrombotics Are Associated with Improved Outcomes Following Ischaemic Stroke: A Cohort from the Registry of the Canadian Stroke Network. International Journal of Stroke 2009, 4, 328–334. [CrossRef]
- Qiu, J.; Ye, H.; Wang, J.; Yan, J.; Wang, J.; Wang, Y. Antiplatelet Therapy, Cerebral Microbleeds, and Intracerebral Hemorrhage. Stroke 2018, 49, 1751–1754. [CrossRef]
- Eikelboom, J.W.; Hirsh, J.; Spencer, F.A.; Baglin, T.P.; Weitz, J.I. Antiplatelet Drugs. Chest 2012, 141, e89S-e119S. [CrossRef]
Figure 1.
Standardized Mean Differences Before and After Propensity Score Matching. Abbreviations: Pre-mRS = pre-morbidity modified Rankin Scale, NIHSS = National Institute of Health Stroke Scale score at admission, 72hNIHSS = National Institute of Health Stroke Scale score 72 hours post-stroke.
Figure 1.
Standardized Mean Differences Before and After Propensity Score Matching. Abbreviations: Pre-mRS = pre-morbidity modified Rankin Scale, NIHSS = National Institute of Health Stroke Scale score at admission, 72hNIHSS = National Institute of Health Stroke Scale score 72 hours post-stroke.
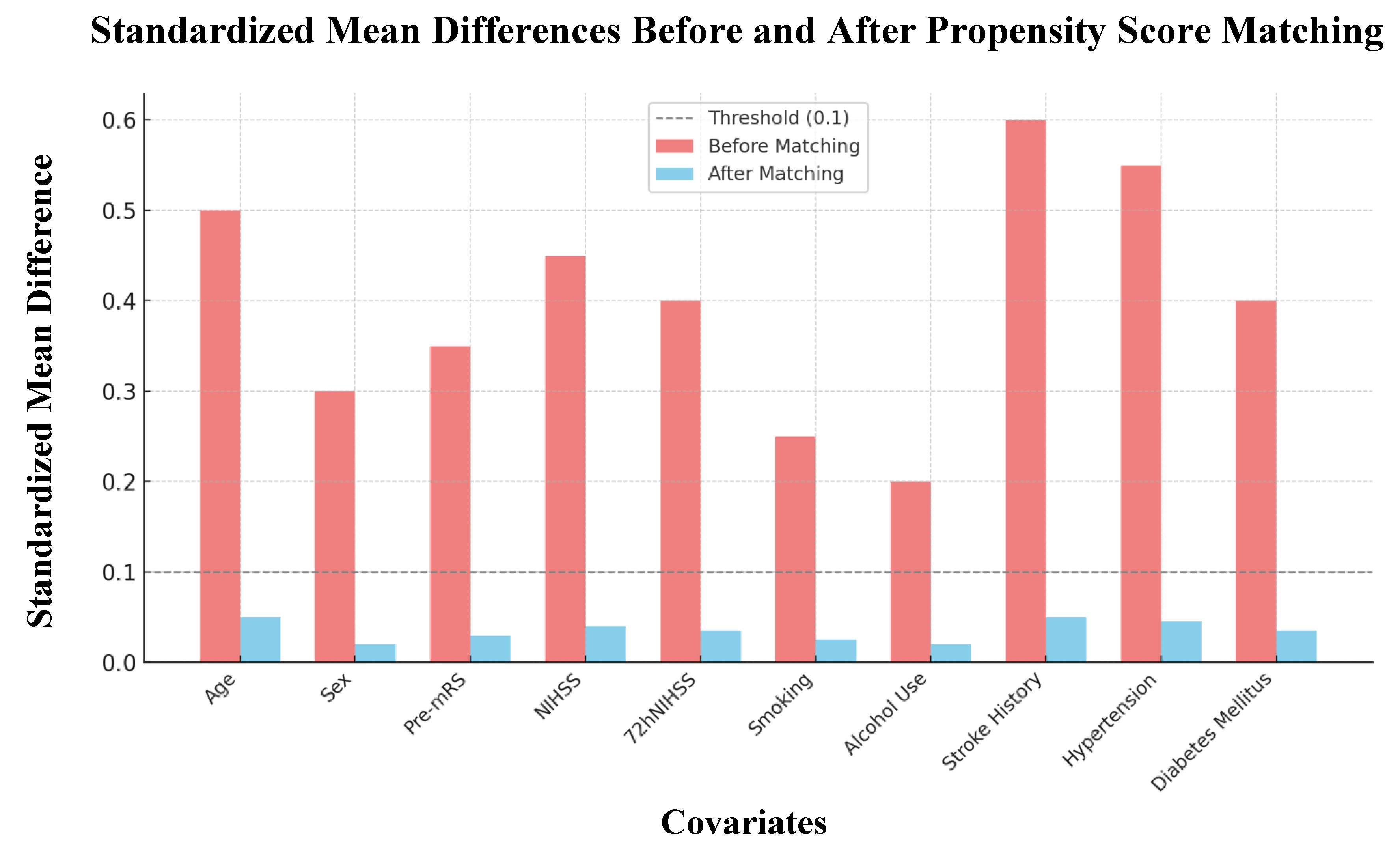
Figure 2.
Distribution of Favorable Outcomes Before Propensity Score Matching. Abbreviations: mRS = modified Rankin Scale, APT = antiplatelet therapy.
Figure 2.
Distribution of Favorable Outcomes Before Propensity Score Matching. Abbreviations: mRS = modified Rankin Scale, APT = antiplatelet therapy.
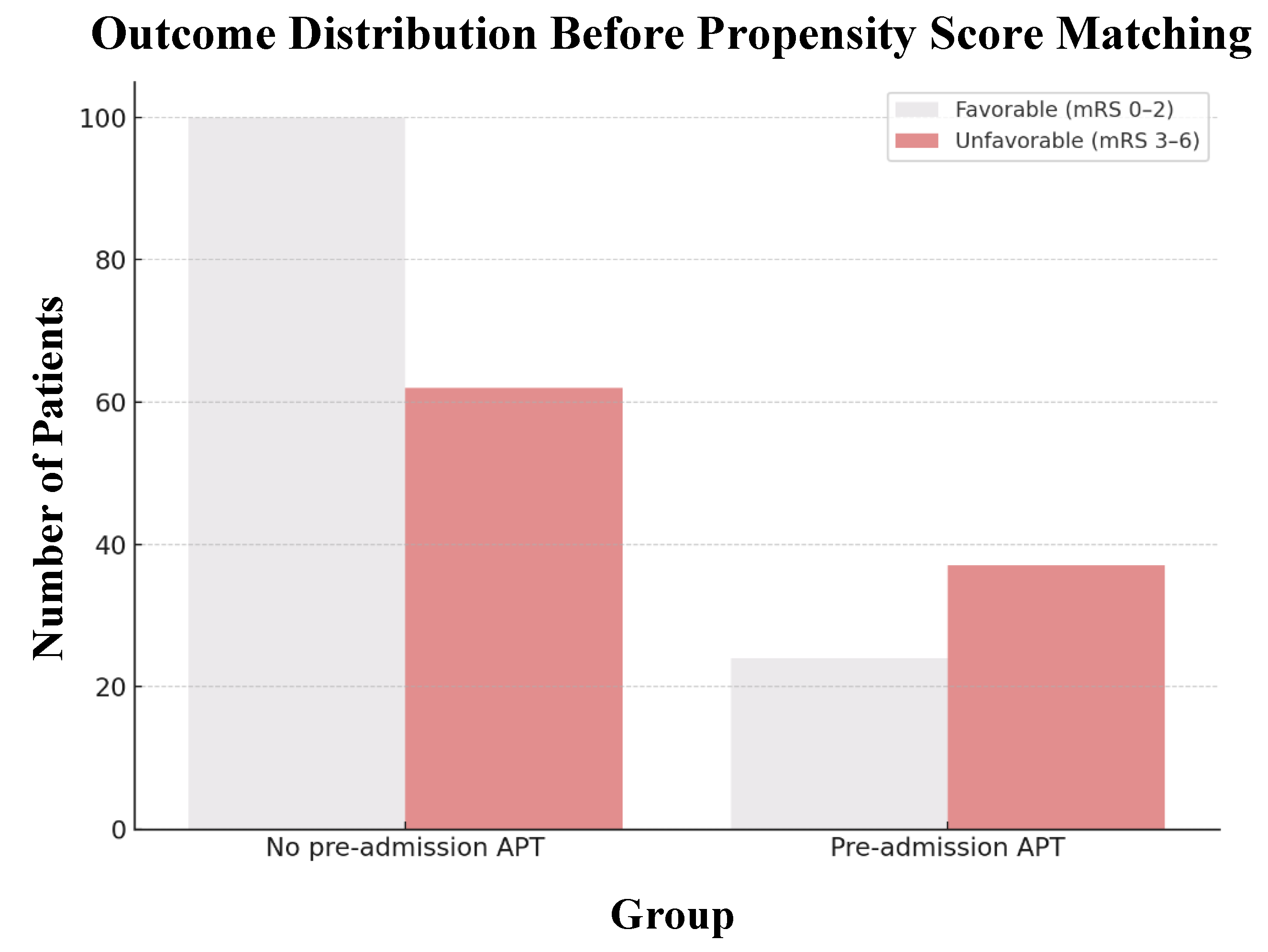
Figure 3.
Combined Forest and Bubble Plot of Predictors of Favorable Outcome. Abbreviations: Pre-mRS = pre-morbidity modified Rankin Scale, NIHSS = National Institute of Health Stroke Scale score at admission, 72hNIHSS = National Institute of Health Stroke Scale score 72 hours post-stroke, APT = antiplatelet therapy.
Figure 3.
Combined Forest and Bubble Plot of Predictors of Favorable Outcome. Abbreviations: Pre-mRS = pre-morbidity modified Rankin Scale, NIHSS = National Institute of Health Stroke Scale score at admission, 72hNIHSS = National Institute of Health Stroke Scale score 72 hours post-stroke, APT = antiplatelet therapy.
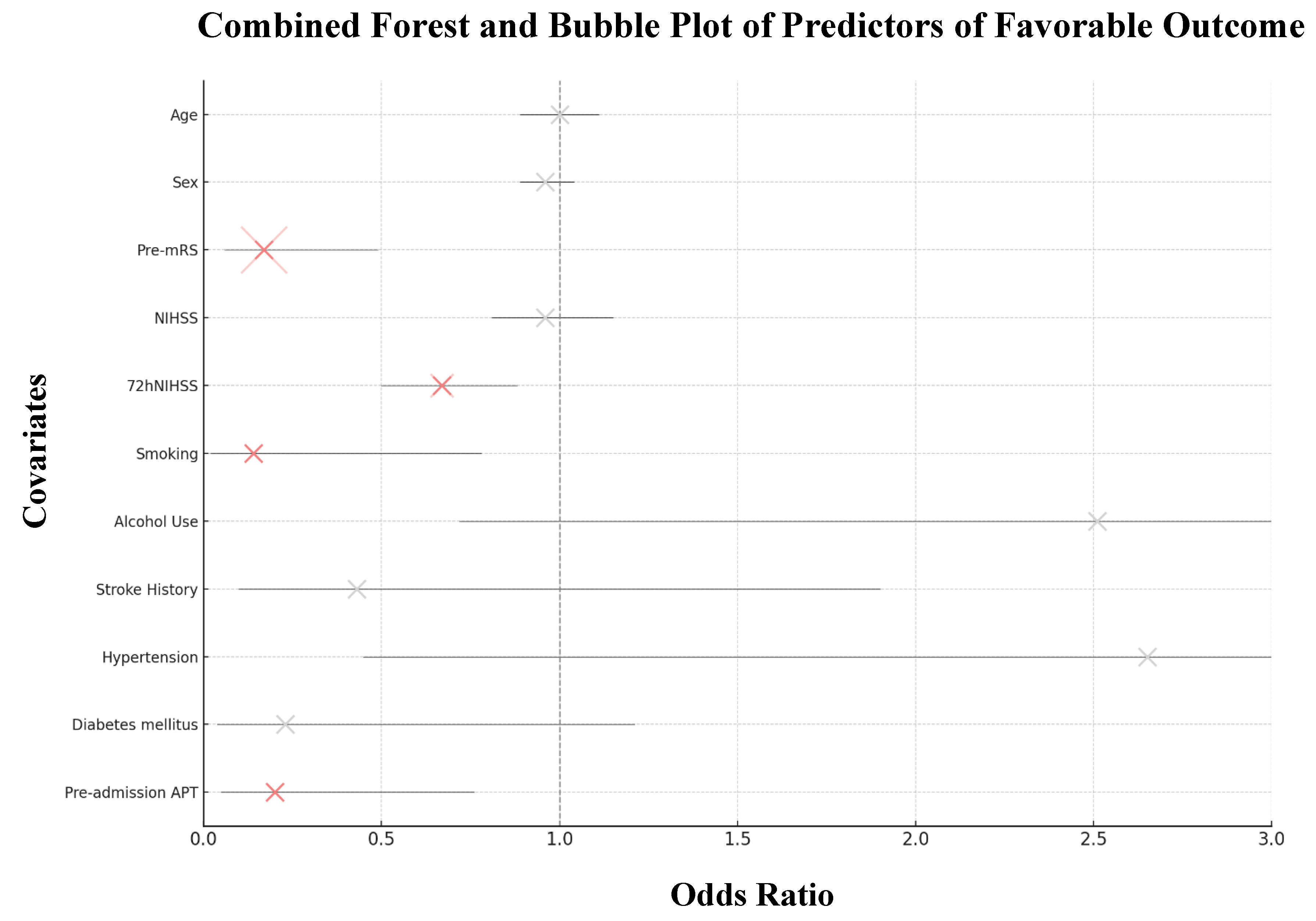

Table 1.
Baseline Characteristics Before and After Propensity Score Matching.
| Before Propensity Score Matching | After Propensity Score Matching | |||||
|
Pre-admission APT n = 61 |
No pre-admission APT n = 162 |
P-value |
Pre-admission APT n = 61 |
No pre-admission APT n = 61 |
P-value | |
| Patient Demographics | ||||||
| Age, years, mean ± SD Sex, male, n (%) |
69.87 ± 11.20 30 (49.2%) |
64.76 ± 13.26 73 (45.1%) |
0.005 0.690 |
69.87 ± 11.20 30 (49.2%) |
72.10 ± 9.35 24 (39.3%) |
0.235 0.362 |
| Clinical Variables | ||||||
| Pre-mRS score, mean ± SD NIHSS score, mean ± SD 72hNIHSS score, mean ± SD Etiology, ESUS, n (%) Onset-to-door time, mean ± SD Plasma glucose, mean ± SD |
0.61 ± 1.24 6.5 ± 6.1 4.2 ± 5.2 11 (18.0%) 484.44 ± 1116 7.62 ± 2.47 |
0.46 ± 1.04 6.6 ± 5.5 4.1 ± 5.2 28 (17.3%) 600.56 ± 1073 7.12 ± 2.27 |
0.404 0.926 0.852 1.00 0.486 0.175 |
0.61 ± 1.24 6.5 ± 6.1 4.2 ± 5.2 11 (18.0%) 484.44 ± 1116 7.62 ± 2.47 |
1.05 ± 1.48 7.6 ± 5.7 4.7 ± 5.5 6 (9.8%) 398.10 ± 456 7.66 ± 1.88 |
0.078 0.290 0.601 0.296 0.577 0.925 |
| Medical History, n (%) | ||||||
| Current Smoking Alcohol Use Stroke history Hypertension Diabetes mellitus |
14 (23.0%) 24 (39.3%) 18 (29.5%) 53 (86.9%) 25 (41.0%) |
57 (35.2%) 73 (45.1%) 4 (2.5%) 118 (72.8%) 34 (21.0%) |
0.113 0.538 <0.001 0.042 0.004 |
14 (23.0%) 24 (39.3%) 18 (29.5%) 53 (86.9%) 25 (41.0%) |
16 (26.2%) 20 (32.8%) 15 (24.6%) 56 (91.8%) 32 (52.5%) |
0.833 0.572 0.684 0.557 0.276 |
| Recanalization therapy, n (%) | ||||||
| TL MT TL + MT |
25 (41.0%) 10 (16.4%) 5 (8.2%) |
48 (29.6%) 36 (22.2%) 11 (6.8%) |
0.147 0.439 0.943 |
25 (41.0%) 10 (16.4%) 5 (8.2%) |
31 (50.8%) 5 (8.2%) 4 (6.6%) |
0.364 0.270 1.00 |
Abbreviations: APT = antiplatelet therapy, Pre-mRS = pre-morbidity modified Rankin Scale, NIHSS = National Institute of Health Stroke Scale score at admission, 72hNIHSS = National Institute of Health Stroke Scale score 72 hours post-stroke, ESUS = embolic stroke of undetermined source, TL = thrombolysis, MT = mechanical thrombectomy.
Table 2.
Predictors of Favorable Outcome After Propensity Score Matching.
| OR | 95% CI | P-value | ||
|---|---|---|---|---|
| Patient Demographics | ||||
| Age, years Sex, male |
0.96 1.03 |
0.89 to 1.04 0.30 to 3.55 |
0.308 0.964 |
|
| Clinical Variables | ||||
| Pre-mRS score NIHSS score 72hNIHSS score Etiology, ESUS Onset-to-door time Plasma glucose |
0.17 0.96 0.67 0.39 1.00 1.12 |
0.06 to 0.49 0.81 to 1.15 0.50 to 0.88 0.06 to 2.38 1.00 to 1.00 0.78 to 1.61 |
<0.001 0.674 0.004 0.306 0.663 0.536 |
|
| Medical History | ||||
| Current Smoking Alcohol Use Stroke history Hypertension Diabetes mellitus |
0.14 2.51 0.43 2.65 0.23 |
0.02 to 0.78 0.72 to 8.70 0.10 to 1.90 0.45 to 15.6 0.04 to 1.21 |
0.025 0.148 0.263 0.282 0.083 |
|
| Recanalization therapy | ||||
| TL MT TL + MT |
2.28 1.08 5.08 |
0.49 to 10.5 0.12 to 9.95 0.53 to 48.8 |
0.290 0.944 0.159 |
|
Abbreviations: OR = odds ratio, CI = confidence interval, Pre-mRS = pre-morbidity modified Rankin Scale, NIHSS = National Institute of Health Stroke Scale score at admission, 72hNIHSS = National Institute of Health Stroke Scale score 72 hours post-stroke, ESUS = embolic stroke of undetermined source, TL = thrombolysis, MT = mechanical thrombectomy.
Table 3.
Mediation Analysis Results of Prior Stroke.
| Estimate | Lower CI | Upper CI | P-value | |
|---|---|---|---|---|
| ADE no pre-admission APT | -0.037 | -0.021 | 0.128 | 0.684 |
| ADE pre-admission APT | -0.037 | -0.020 | 0.127 | 0.684 |
| ACME no pre-admission APT | -0.015 | -0.080 | 0.041 | 0.596 |
| ACME pre-admission APT | -0.014 | -0.080 | 0.039 | 0.596 |
| Total Effect | -0.051 | -0.230 | 0.127 | 0.534 |
Abbreviations: CI = confidence interval, ADE = average direct effect, APT = antiplatelet therapy, ACME = average casual mediation effect.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



