Submitted:
02 January 2025
Posted:
04 January 2025
You are already at the latest version
Abstract
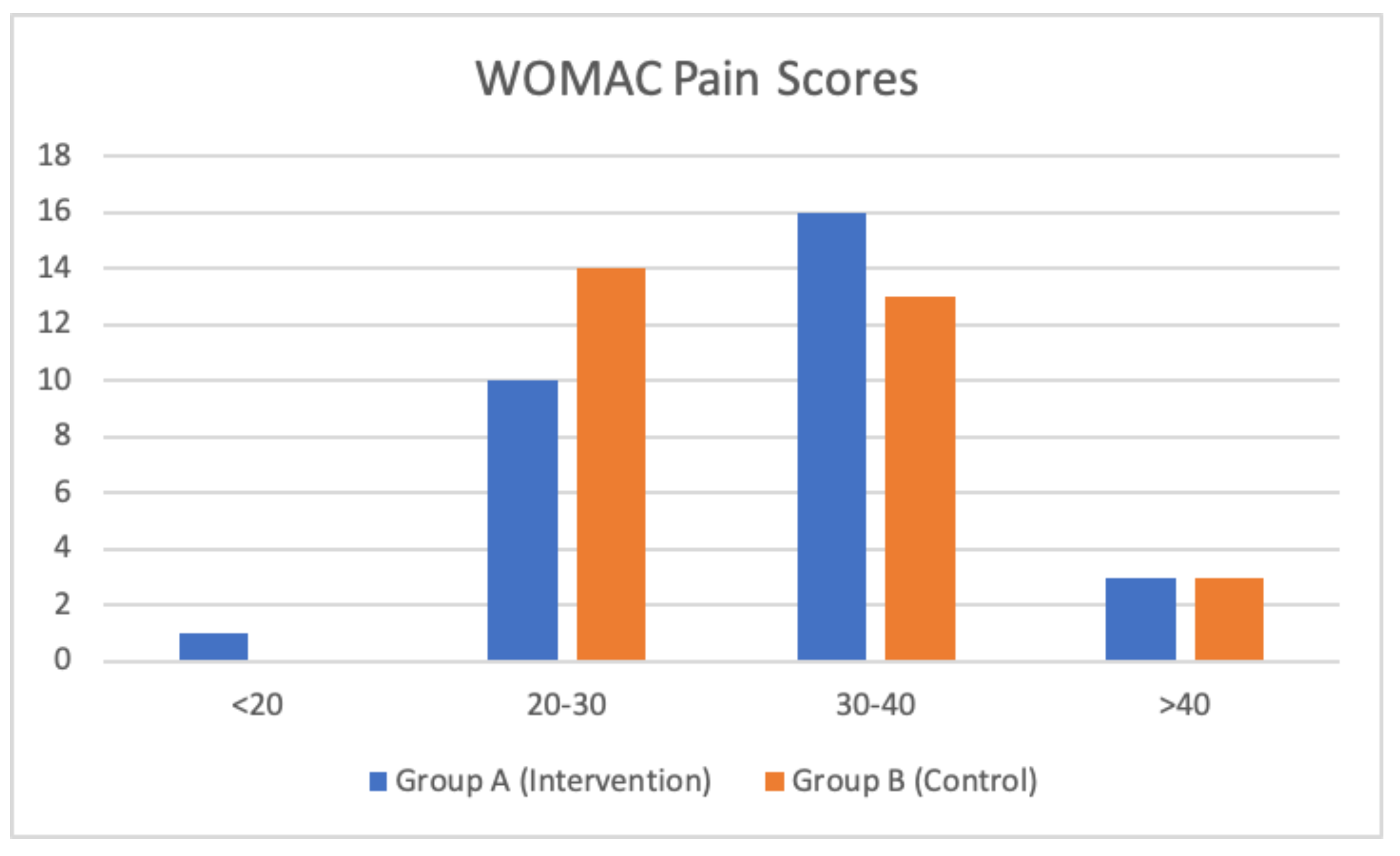
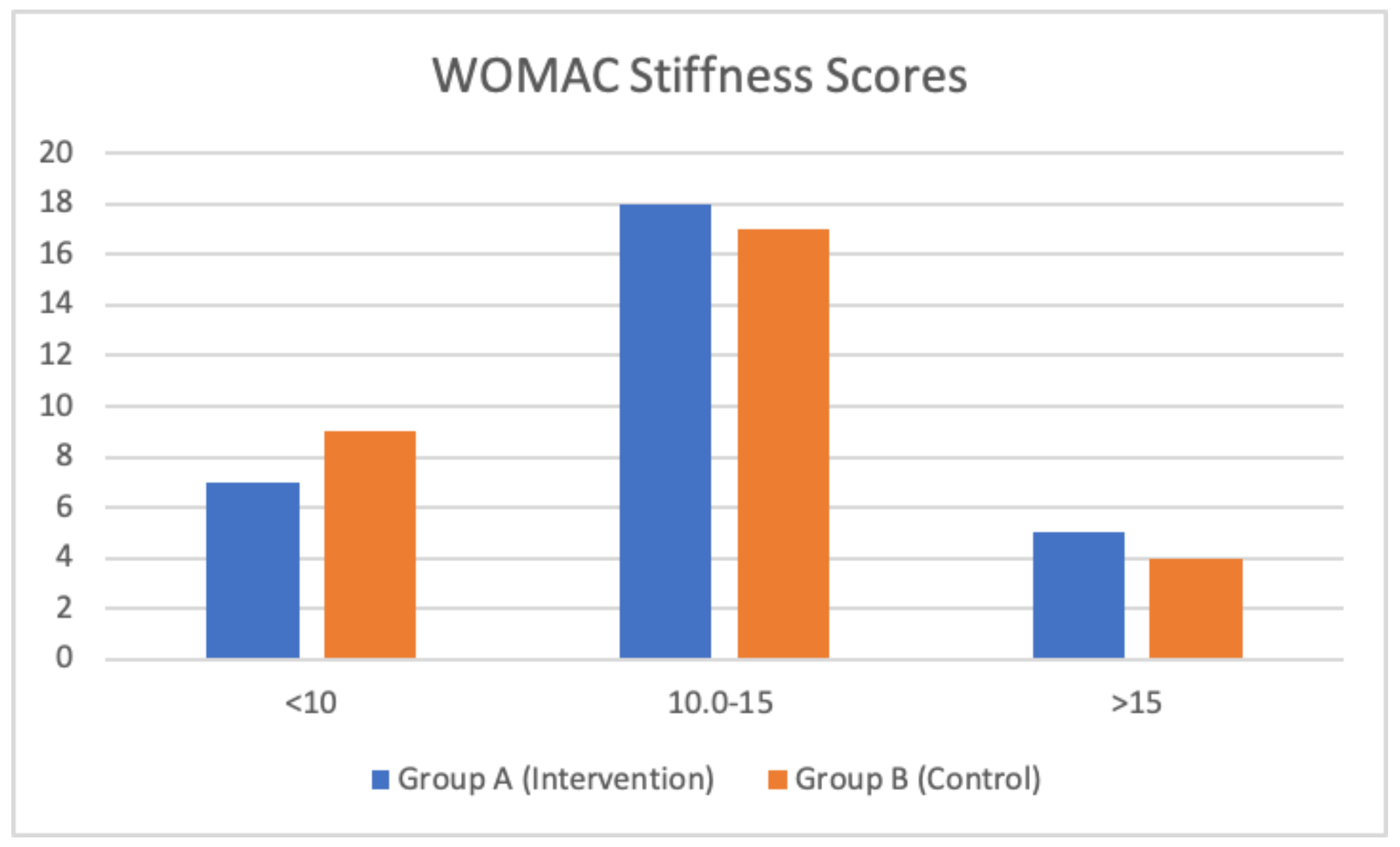
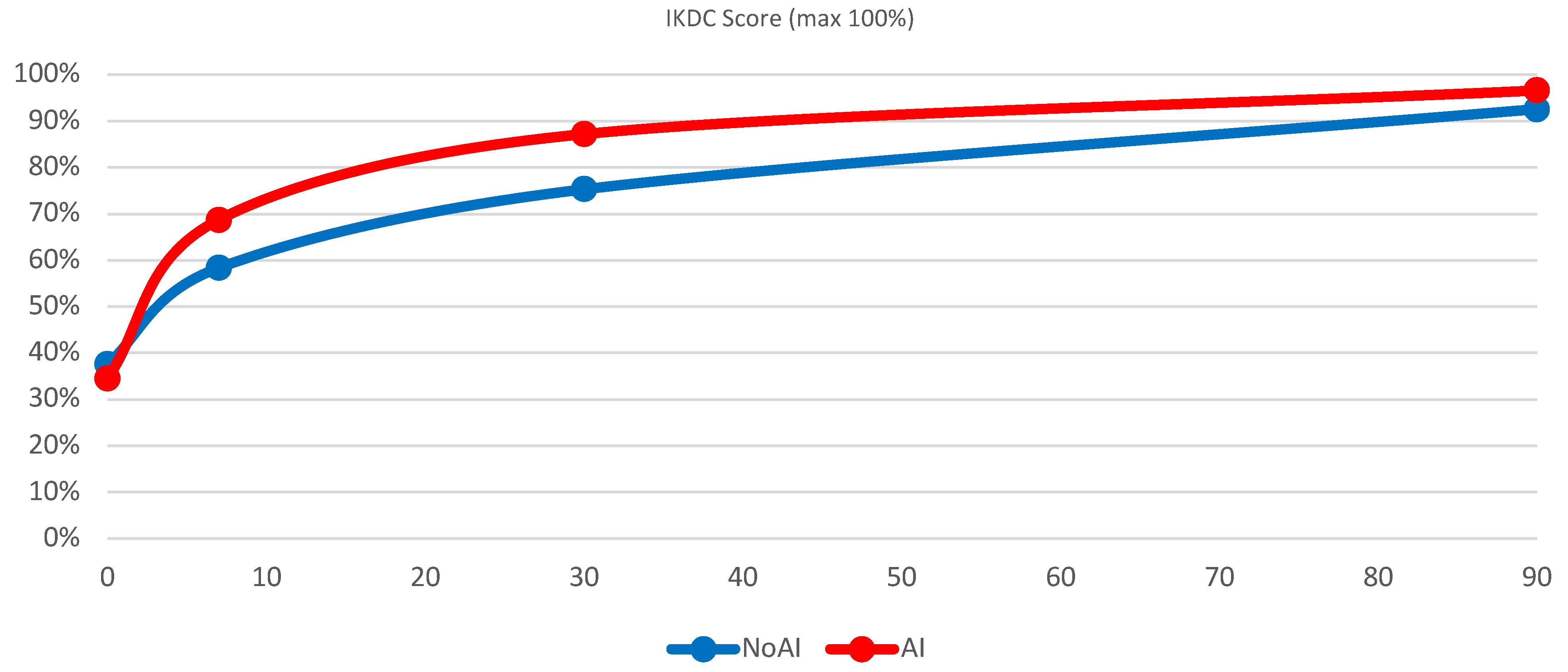
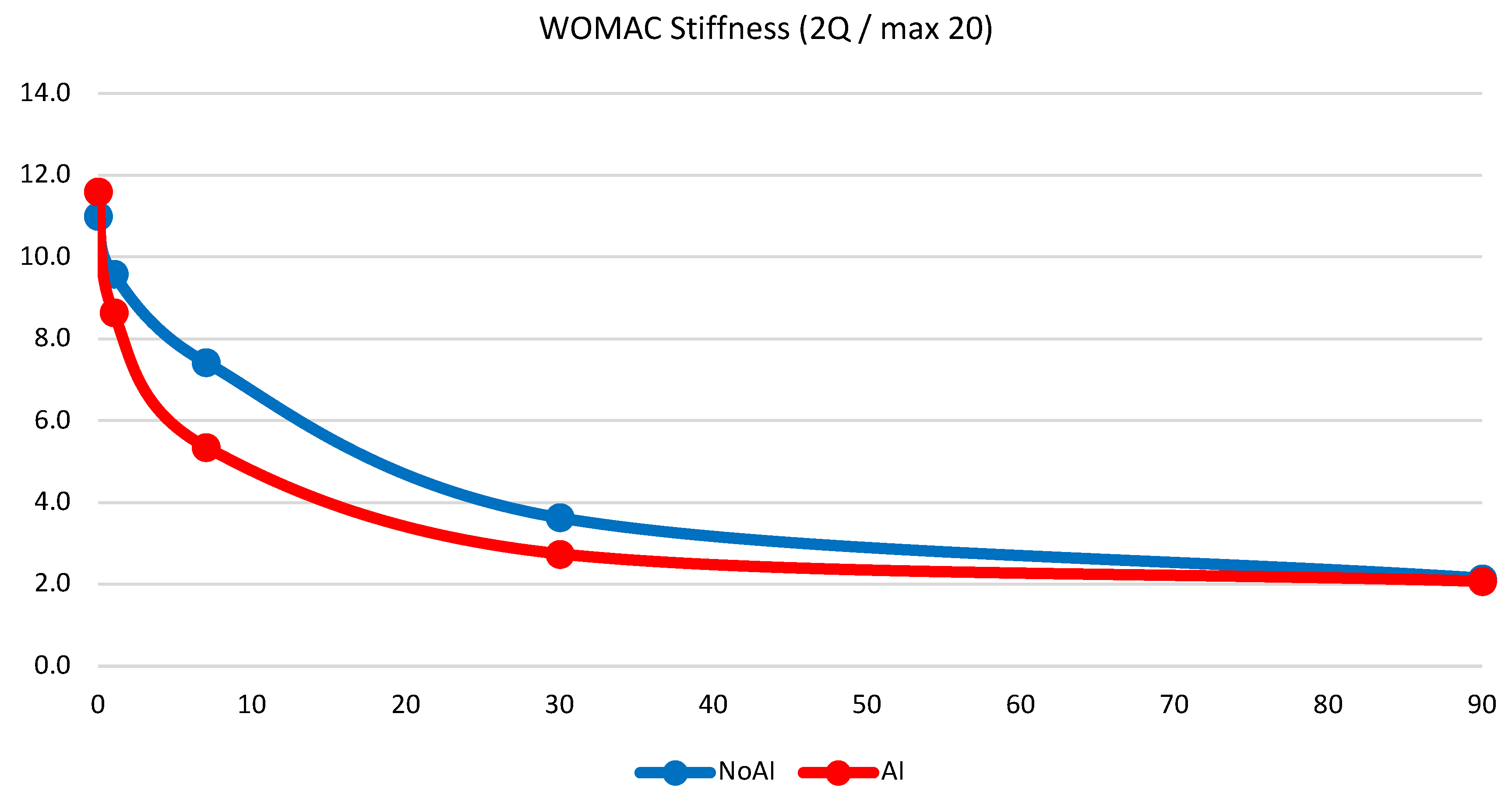
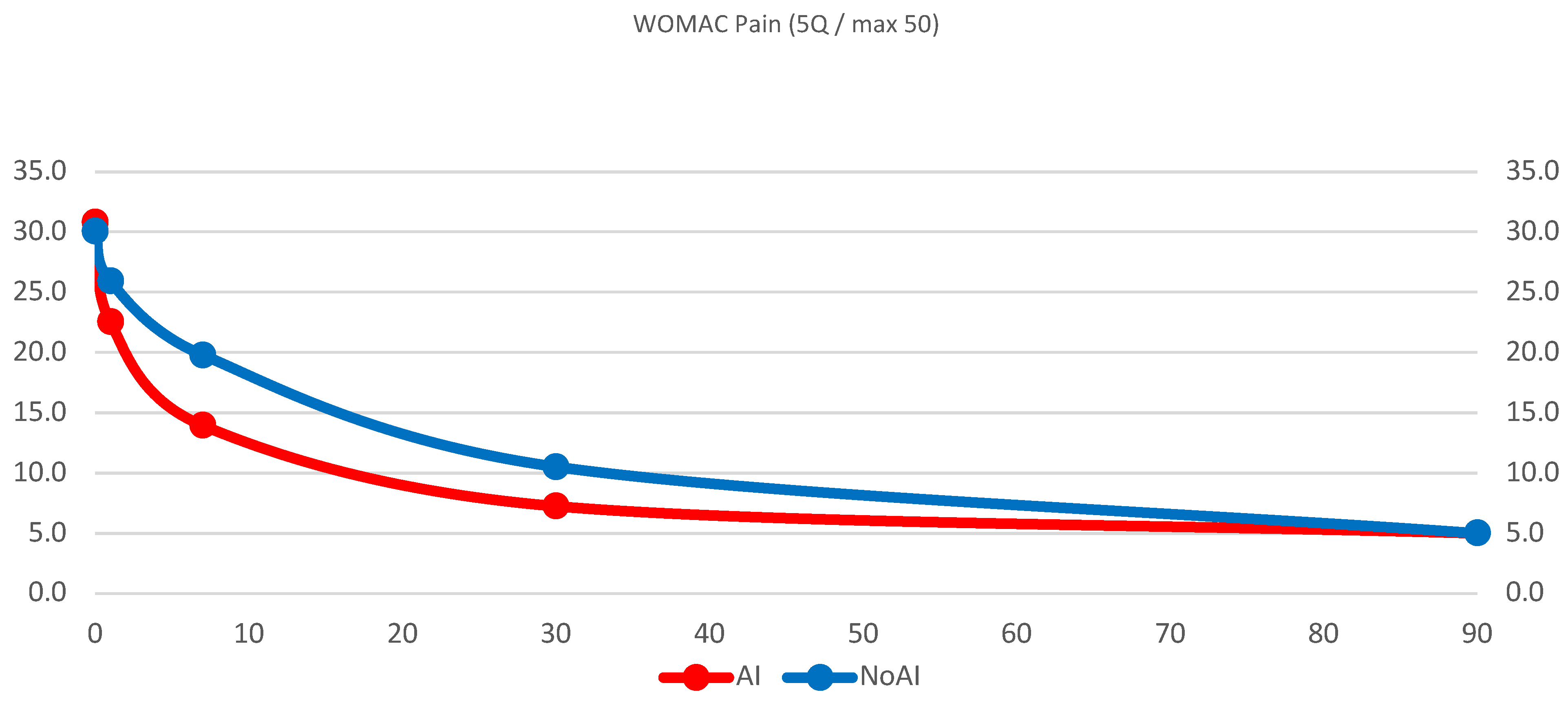
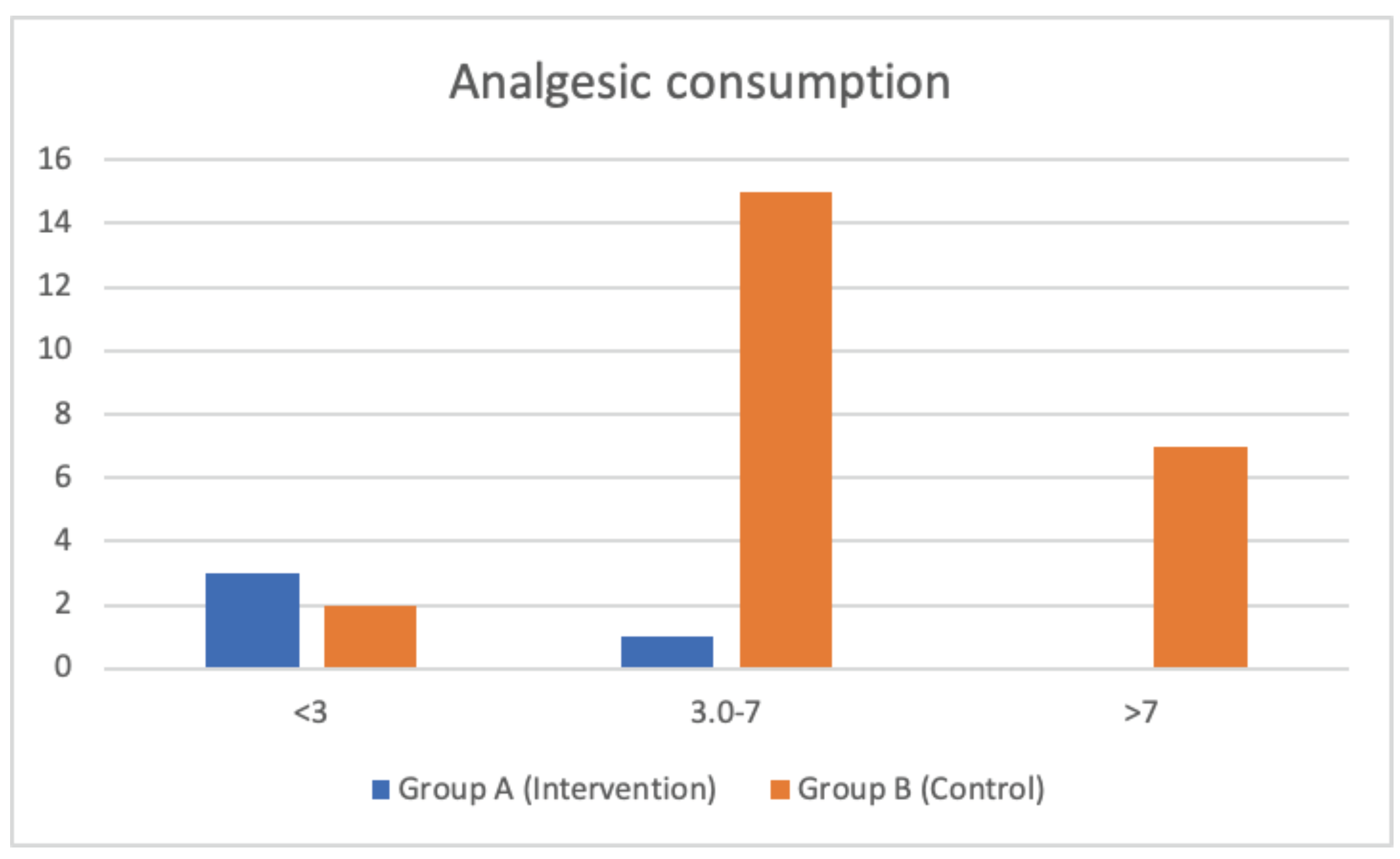
Background: Following non-bleeding arthroscopy, patients that are injected with 6 ml of hyaluronic acid (2%) and sorbitol (4%) formulation (Synolis VA) show better results in terms of pain reduction and improved mobility recovery compared to patients that did not receive the treatment. Introduction: Although there is no best irrigation solution for the knee arthroscopy, many studies showed that the common irrigation fluids, especially cold ones, are toxic for the articular chondrocytes, suppressing their metabolism and function. The purpose of this study is to evaluate the clinical outcome of patients injected with Synolis V-A after knee arthroscopy. Materials and Methods: 60 patients were randomly divided into 2 groups. At the end of the procedure 30 patients received an intra-articular injection of hyaluronic acid (2%) and Sorbitol (4%) solution for a total of 6 ml (2 ml per syringe), the remaining 30 patients did not receive any treatment. Inclusion criteria: age (ranging from 18 to 60 years), meniscectomy or cartilage treatment (non-bleeding knee arthroscopy), body mass index (<30). Patients with joint-line misalignment, ligamentous lesions, bone pathology, synovial membrane pathology, rheumatoid arthritis or inflammatory disease, or pregnancy were excluded from the study. Patients were reviewed at several follow-up points and monitored using outcomes such as the IKDC subjective knee evaluation score, pain variaton (using VAS and WOMAC pain sub-score) and variation of stiffness (using WOMAC Stiffnes sub-score). Patients were also asked to fill in a self-assessment questionnaire on a weekly basis as well as at each visit in order to follow the clinical evolution of the symptoms. The statistical analysis was performed with IBM SPSS Statistics for Windows, Version 28.0. Results: Patients injected with Synolis V-A at the short and intermediate check-points showing better clinical results than the patients that were not injected with the product; these patients had higher IKDC Subjective Knee Evaluation scores, as well as lower point of pain and reduced stiffness. Conclusions: Based on our results, the injection with hyaluronic acid (2%)/sorbitol (4%) formulation (Synolis V-A) in patients undergoing non-bleeding arthroscopy for degenerative and traumatic changes to the knee joint effectively reduces pain and improves mobility in the short-term post-operative phase.
Keywords:
Introduction
Materials and Methods
Results
- -
- Group A (30 patients): mean age 42 years (range 23-58); mean BMI 25.5 (range 20.1-29.6), 27% women and 73% men
- -
- Group B (30 patients): mean age 41 years (range 19-59); mean BMI 23.4 (range 19.8-27.3), 30% women and 70% men.

Discussion
Conclusion
References
- Nam CW, Kim K, Lee HY: The influence of exercise on an unstable surface on the physical function and muscle strength of patients with osteoarthritis of the knee. J Phys Ther Sci, 2014, 26: 1609–1612. [CrossRef]
- Koca I, Boyacı A, Tutoglu A, et al.: The relation between quadriceps thickness, radiological staging and clinical parameters in knee osteoarthritis. J Phys Ther Sci, 2014, 26: 931–936. [CrossRef]
- Mangone G, Orioli A, Pinna A, et al.: Infiltrative treatment with Platelet Rich Plasma (PRP) in knee osteoarthritis. Clin Cases Min Bone Metab, 2014, 11: 67–72.
- Kim G, Kim E: Anti-inflammation effects of low intensity laser therapy on monosodium iodoacetate-induced osteoarthritis in rats. J Phys Ther Sci, 2013, 25: 173–175. [CrossRef]
- Bjordal JM, Johnson MI, Lopes-Martins RA, Bogen B, Chow R, Ljunggren AE. Short-term efficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials. BMC Musculoskelet Disord 2007;8:51. [CrossRef]
- DeLee JC; Committee on Complications of Arthroscopy Association of North America. Complications of arthroscopy and arthroscopic surgery: results of a national survey. Arthroscopy 1985;1(4): 214–220. [CrossRef]
- Small NC; Committee on Complications of the Arthroscopy Association of North America. Complications in arthroscopy: the kneeand other joints. Arthroscopy 1986;2(4):253–258. [CrossRef]
- Small NC. Complications in arthroscopic surgery performed by experienced arthroscopists. Arthroscopy 1988;4(3):215–221. [CrossRef]
- Reagan BF, McInerny VK, Treadwell BV, Zarins B, Mankin HJ. Irrigating solutions for arthroscopy. A metabolic study. J Bone Joint Surg Am 1983;65(5):629–631. [CrossRef]
- Bulstra SK, Kuijer R, Eerdmans P, van der Linden AJ. The effect in vitro of irrigating solutions on intact rat articular cartilage. J Bone Joint Surg Br 1994;76(3):468–470. [CrossRef]
- Straehley D, Hellar A, Solomons C, et al. The effect of arthroscopic irrigating solutions on cartilage and synovium. Trans Orthop ResSoc 1985;10:260.
- Kobayashi K, Matsuzaka S, Yoshida Y, Miyauchi S,Wada Y, Moriya H. The effects of intraarticularly injected sodium hyaluronate on levels of intact aggrecan and nitric oxide in the joint fluid of patients with knee osteoarthritis. Osteoarthritis Cartilage 2004; 12(7):536–542. [CrossRef]
- Dervin G, Stiell I, Rody K, Grabowski J. The effect of arthroscopic debridement for osteoarthritis of the knee on healthrelatedquality of life. J Bone Joint Surg Am 2003;85:10-19.
- Bhattacharyya T, Gale D, Dewire P, et al. The clinical importance of meniscal tears demonstrated by magnetic resonance imaging in osteoarthritis of the knee. J Bone Joint Surg Am 2003;85:4-9. [CrossRef]
- BJ, Cushner FD, Scott WN. Debridement arthroscopy. 10-year follow-up. Clin Orthop Relat Res 1999; (367):190-4.
- Day B. The indications for arthroscopic debridement for osteoarthritis of the knee. Orthop Clin North Am 2005;36: 413-7. [CrossRef]
- Bulstra SK, Douw C, Kuijer R. NaCL irrigation of the rat knee inhibits cartilage metabolism; hyaluranon restores this disturbed metabolism to normal. Presentation at the 45th Annual Meeting of the Orthopaedic Research Society, Anaheim, USA, 1–4 February 1999.
- Webber RJ, Zitaglio T, Hough Jr AJ. Serum-free culture of rabbit meniscal fibrochondrocytes: proliferative response. J Orthop Res 1988;6:13-23. [CrossRef]
- Shinjo H, Nakata K, Shino K, Hamada M, Nakamura N, Mae T, Miyama T, Horibe S, Yoshikawa H, Ochi T. Effect of irrigation solutions for arthroscopic surgery on intraarticular tissue: comparison in human meniscus-derived primary cell culture between lactate Ringer’s solution and saline solution. Journal of Orthopaedic Research 20 (2002) 1305-1310. [CrossRef]
- Matsusue Y, Thomson NL. Arthroscopic partial medial meniscectomy in patients over 40 years old: A 5- to 11-year follow-up study. Arthroscopy 1996;12:39-44. [CrossRef]
- Bin SI, Lee SH, Kim CW, Kim TH, Lee DH. Results of arthroscopic medial meniscectomy in patients with grade IV osteoarthritis of the medial compartment. Arthroscopy 2008; 24:264-268. [CrossRef]
- Outerbridge R. The etiology of chondromalacia of the patella. J Bone Joint Surg Br 1961;42:752-760. [CrossRef]
- Smith MD, Wetherall M, Darby T, Esterman A, Slavotinek J, Roberts-Thomson P, et al. A randomized placebo-controlled trial of arthroscopic lavage versus lavage plus intra- articular corticosteroids in the management of symptomatic osteoarthritis of the knee. Rheumatology 2003; 42:1477-85. [CrossRef]
- Conrozier T, Mathieu P, Schott AM, Laurent I, Hajri T, Crozes P, et al. Factors predicting long-term efficacy of Hylan GF-20 viscosupplementation in knee osteoarthritis. Joint Bone Spine 2003;70:128-33. [CrossRef]
- Marshall D, Johnell O, Wedel H. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 1996;312:1254-1259. [CrossRef]
- Chen Y, Peng D, Sun CJ, Wang WC, Li JY, Zhang W. Clinical study on sodium hyaluronate intra-articular injection in treatmentof degenerative osteoarthritis of knee. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2002;16:19-20.
- Hempfling H. Intra-articular hyaluronic acid after knee arthroscopy: A two-year study. Knee Surg Sports Traumatol Arthrosc 2007;15:537-546. [CrossRef]
- Tetik O, Doral MN, Atay AO, Leblebicioglu G. Influence of irrigation solutions combined with colchicine and diclofenac sodium on articular cartilage in a rat model. Knee Surg Sports Traumatol Arthrosc 2004;12:503-9. [CrossRef]
- Vad VB, Bhat AL, Sculco TP, Wickiewicz TL. Management of knee osteoarthritis: knee lavage combined with hylan versus hylan alone. Arch Phys Med Rehabil 2003; 84:634-7.
- Jansen EJ, Emans PJ, Douw CM, Guldemond NA, Van Rhijn LW, Bulstra SK, et al. One intra-articular injection of hyaluronan prevents cell death and improves cell metabolism in a model of injured articular cartilage in the rabbit. J Orthop Res 2008;26:624-30. [CrossRef]
- Scott JE. In: Evered D, Whelan J, eds. The biology of hyaluronan. Ciba Foundation Symposium 143. Chichester: John Wiley, 1989: pp 6–20.
- Balazs EA, Denlinger JL. In: Evered D, Whelan J, eds. The biology of hyaluronan. Ciba Foundation Symposium 143. Chichester: John Wiley, 1989: pp 265–75.
- Colwell CW Jr, D’Lima DD, Hoenecke HR, et al.. In vivo changes after mechanical injury. Clin Orthop Relat Res 2001. 116 – 123. [CrossRef]
- D’Lima DD, Hashimoto S, Chen PC, et al.. Human chondrocyte apoptosis in response to mechanical injury. Osteoarth Cart 2001 9:712 – 719. [CrossRef]
- Diaz-Gallego L, Prieto JG, Coronel P, et al.. Apoptosis and nitric oxide in an experimental model of osteoarthritis in rabbit after hyaluronic acid treatment. J Orthop Res 2005. 23:1370 – 1376. [CrossRef]
- Kobayashi K, Matsuzaka S, Yoshida Y, Miyauchi S, Wada Y, Moriya H. The effects of intraarticularly injected sodium hyaluronate on levels of intact aggrecan and nitric oxide in the joint fluid of patients with knee osteoarthritis. Osteoarthritis Cartilage. 2004 Jul;12(7):536-42. [CrossRef]
- Mongkhon JM1, Thach M, Shi Q, Fernandes JC, Fahmi H, Benderdour M. Sorbitol-modified hyaluronic acid reduces oxidative stress, apoptosis and mediators of inflammation and catabolism in human osteoarthritic chondrocytes. Inflamm Res. 2014 Aug;63(8):691-701. [CrossRef]
- Campo GM, Avenoso A, Capo S. Hyaluronan reduces inflammation in experimental arthritis by modulating TLR-2 and TLR-4 cartilage expression., Biochimica et Biophysica Acta 2009 Oct;1790(10):1353-67. [CrossRef]
- Amin AK1, Huntley JS, Patton JT, Brenkel IJ, Simpson AH, Hall AC. Hyperosmolarity protects chondrocytes from mechanical injury in human articular cartilage: an experimental report. J Bone Joint Surg Br. 2011 Feb;93(2):277-84. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



