1. Introduction
As part of the monitoring of the Portuguese mental health program, the indicator
“Proportion of users aged 65 and over, without prolonged prescription of anxiolytics, sedatives or hypnotics” was defined [
1], which reveals the importance given to this topic in Portugal.
The drugs in question are benzodiazepines and analogues (e.g. zolpidem), in the scope of this study referred to as
Benzodiazepine Receptor Agonists (BZRA). According to the description of the indicator referred to, prolonged prescription is understood as the sum of an
Average Daily Maintenance Dose > 53 in the last 12 months. This value is estimated according to the maximum thresholds foreseen for the treatment of pathological anxiety or insomnia, adjusted for the elderly population, according to the Clinical Practice Guideline nº 55/2011 of the Portuguese Directorate-General of Health (DGS) [
2].
BZRA are the most prescribed group of drugs used to treat symptomatic anxiety, primary and secondary sleep disorders. Although well-tolerated, their use has been restricted due to the risk of dependence and habituation in a considerable number of users, leading to marked difficulty in discontinuing them in users who have been taking them for a few weeks [
2].
Alongside with the high prevalence of anxiety syndromes, Portugal has one of the highest prescription rates of BZRA in Europe. Recent reports show that these drugs are responsible for 7% of the drug market share in the country [
3]
Despite the existing evidence on the increased risk of these therapies in this age group, the major consumers of BZRA tend to be older patients and, in general, their consumption increases with ageing. Recent estimates of prevalence in the older population throughout the developed world have shown a rate of approximately 8-12% in community-based studies [
4].
Although their use may be indicated in certain circumstances, most prescriptions of BZRA for the elderly are considered inappropriate. Pharmacological treatment with BZRA in elderly patients is associated with an increased risk of falls, balance problems, drowsiness, cognitive impairment, memory disorders, functional impairment and physical dependence. [
5]
Therefore, understanding patient perspectives, more in depth, may help identify and provide a foundation for the development of interventions with greater reach, sustainability, and effectiveness in primary care [
5,
6]. In this sense, it is crucial to develop tools that help the discontinuation of BZRA in the elderly to prevent its possible negative consequences. However, the predictors of successful discontinuation are not well known due to lack of research on the subject [
4,
5,
6,
7].
Deprescription is defined as ‘‘the withdrawal of an inappropriate medication, supervised by a health care professional with the goal of managing polypharmacy and improving outcomes’’ [
4]
While studies have identified several barriers, including dependence, withdrawal symptoms and lack of supports, there are gaps in comprehensive analysis of both barriers and facilitators, as well as in comparing the experiences of current and previous long-term BZRA users. To ensure that future interventions target behavioral determinants and provide theoretical underpinning, discontinuation of long-term BZRA use needs to be studied with more focus from the patients' point of view. [
8]
In developing new interventions aimed at BZRA deprescribing, it is increasingly recommended that researchers adopt a systematic approach and explicitly describe the process of its development [
8].
A systematic review by Rasmussen et al. in 2021 [
5] aimed to identify and compare barriers and facilitators in stakeholders involved in BZRA deprescribing in the elderly (patients, physicians, nurses and caregivers) to identify potential gaps in this field of research.
Eight themes emerged from this review defined as barriers to BZRA deprescribing in patient-directed studies: understanding BZRA as an effective treatment; understanding BZRA as an inducer of well-being; thinking that BZRA are not harmful; concern about withdrawal symptoms; ageism (understanding unnecessary de-escalation due to age); lack of information (on side effects, dependency, alternative treatments); dependence (feeling unable to reduce or stop therapy); lack of medical support.
Five themes emerged that were defined as facilitators for BZRA deprescribing in patient-directed studies: educational tools (e.g., brochures); motivation of health professionals; perception of side effects; willingness to stop therapy; time to consider the benefits after counselling in the face of deprescribing.
The same review points in its conclusions to the importance of communication and shared decision-making between doctors and patients to improve medication according to patient preferences, as well as the need for further research on this topic.
A systematic review and meta-synthesis of patients’ experiences and perceptions of seeking and using BZRA, published in 2016 [
9], points out seven themes from published qualitative research which relate with factors perpetuating their use: patients’ negative perceptions of insomnia and its impact, failed self-care strategies, triggers to medical help-seeking, attitudes towards treatment options/service provision, varying patterns of use, withdrawal and reasons for initial or ongoing use. The authors point out three main strategies which may support patients with conditions for which these drugs may be prescribed: creation of educational resources (implementation of self-care strategies, help patients to have realistic expectations of what treatments might achieve), providing alternative treatments (such as cognitive behavioral therapy) and expanding the range of help options to explore and encourage the use of non-pharmacological treatments, ensuring that patients know that their problems are taken seriously. Further research is needed to ascertain the efficacy of different approach(es) to deprescribing (e.g., patient education, group therapy, mixed interventions). Moreover, it is important to consider the influence resulting from patient characteristics (e.g., comorbidities).
Intervention studies on deprescribing show that BZRA withdrawal seem to be feasible and safe in the elderly population, despite heterogeneity in the study methodology and outcomes [
4], which has been substantiated by three additional systematic reviews on the evidence for interventions to reduce or discontinue BZRA in this age group [
10,
11,
12].
A review article by Ng et al. [
4], related to the impact of interventions aimed at BZRA deprescribing in elderly patients, reports quite different success rates (ranging from 27 to 80%). This variability is assignable to the heterogeneity of intervention methodologies as well as limited applicability to patients with cognitive impairment. They distinguished two main intervention typologies targeting patients, each of them grouping different interventional strategies:
Raising Awareness Interventions consisted of: written information (patient information book), minimal intervention or geriatrician one-off counselling;
Providing Resources for BZRA Discontinuation consisted of: gradual self-managed dose reduction, supervised gradual dose reduction, supervised gradual dose reduction plus cognitive behavioural therapy and other techniques.
Oliveira et al. [
3] summarize, among other topics concerning BZRA withdrawal in primary health care, available strategies to discontinue these drugs at this setting. It points out that the success of discontinuing therapy in long-term users seems to be associated with the perception of self-efficacy, beliefs about withdrawal symptoms, initial motivation to quit, information about the risks of BZRA and gradual dose decreasing withdrawal.
Related qualitative studies have examined patients' experiences and perceptions of BZRA use. Very few peer review studies have considered benzodiazepines from the user perspective and even fewer have drawn on the language employed by users themselves to explore firsthand experiences of withdrawal or discontinuation syndrome [
13].
A study carried in Ireland by Lynch et al. [
8], consisting of semi-structured interviews based on the
Theoretical Domains Framework with people with current or previous experience of prolonged BZRA use, highlights the complexity of BZRA discontinuation, identifying a wide range of mediators (barriers and facilitators) of discontinuing long-term BZRA use from the perspective of both current and previous users. They propose that future work will involve developing a theory-based intervention that may support BZRA discontinuation in Primary Health Care.
A study carried in Canada by Allary et al. [
14], designed to figure out psychological predictors of benzodiazepine among older adults, points out three psychological factors that were significant predictors for BZRA discontinuation: social support satisfaction, intensity of depressive symptoms and self-perceived competence in the ability to withdraw. According to the authors, the importance of social support satisfaction and self-perceived competence should make future BZRA withdrawal programs to focus more on these factors to be more effective, as it appears to be the best way to achieve long-term discontinuation.
A recent qualitative study in primary health care centres in an interior and mostly rural region of Portugal (similar to the context of our study) explored General Practitioner’s perspectives on solutions to address the excessive prescription of benzodiazepines [
15]. Solutions proposed focused on organizational aspects, alternative approaches to prescribing and wider community-based initiatives (such as fostering public awareness about the perils of BZRA, creating socially adapted consultations and more community-based programs that would enable the pursuit of therapeutic non-pharmacologic alternatives).
In this sense and having not found in the literature review any similar qualitative studies carried out in Portugal to date, we proposed to identify the barriers and facilitators in the discontinuation of BZRA from the perceptions of elderly patients under prolonged prescription of BZRA, belonging to the same rural community.
The potential contributions for further research are the identification of intervention targets directed at patients, to reduce the prevalence of elderly patients under prolonged prescription of BZRA.
2. Materials and Methods
Design: Since the main purpose of the study was to identify individual perceptions on this topic, we considered the qualitative methodology would be the most proper to carry out this investigation. Therefore, the aim was to conduct a set of semi-structured interviews headed from an interview guide drawn up based on literature to then conduct the respective content analysis.
Preparation of the interview guide: An interview topic guide with open-ended questions was developed based on eight domains called
"Barriers to the Deprescribing of BZRA" and five domains called
"Facilitators to the Deprescribing of BZRA", according to the themes identified in the systematic review by Rasmussen et al. [
5].
The interview guide was reformulated after carrying out a pilot test for its experimental application, which consisted of obtaining a written opinion on it, voluntarily requested from two family doctors and two patients who did not comply with the performance indicator of interest to the study (i.e. potentially eligible for inclusion).
Recruitment: A convenience non-probability sampling was obtained (with a minimum quota of 25% by gender), from the population of patients registered in the Family Health Unit Matriz (Arraiolos Health Centre, Alentejo Region). The inclusion criteria were: not accomplish the indicator "Proportion of users aged 65 years or over, without prolonged prescription of anxiolytics, sedatives or hypnotics", according to the respective list obtained, relative to December 2021, from the database made available by the software MIM@UF - Module for Information and Monitoring of Functional Units. As exclusion criteria we defined: a.) registration in the Electronic Health Record's Active Problems List of codes N88 (Epilepsy) and/or P70 (Dementia), according to the ICPC-2 (International Classification of Primary Health Care); b.) severe psychiatric illness (defined as any clinical condition requiring the inclusion of antipsychotic drugs and/or lithium in the patient's chronic medication list); c.) record of any previous medical consultation carried out by the main researcher (due to the circumstance of being himself a Family Doctor at the Unit where the study was develop), which was intended to cancel a possible effect of "moderator bias" that the existence of a previous doctor-patient relationship may induce; d.) any circumstances or conditions which would make the interview infeasible to be performed without the presence of a third person.
A prior telephone contact with patients selected, for invitation and scheduling of the interview, was carried by a participants’ Family Health Unit nurse, who was therefore assigned the role of referrer/interlocutor between the main researcher and each study participant.
Data Collection: Semi-structured interviews were conducted by the main researcher with a group of fifteen patients from the sampling obtained, dimension needed to reach data saturation.
The interviews were taken at Arraiolos Health Centre, in an office usually used for institutional meetings, where medical or nursing consultations are not carried out.
Prior to the completion of each interview, the respective informed consent was obtained in duplicate, signed by the participant, interviewer, the scientific supervisors and the doctor responsible for the unit where the study was carried out, with both interviewer and participant keeping the respective copies. The document pointed out the commitment from the main researcher to the use of the data collected exclusively for the purposes of the study.
In the preliminary phase of each interview, the following general data were recorded for description of participants: a.) gender; b.) age; c.) active principle and dosage of the current BZRA; d.) year of current BZRA’s first prescription; e.) previous intake of other BZRAs; f.) cause for taking BZRA (according to the interviewee); g.) frequency of intake; h.) previous attempts to discontinue the BZRA carried by the interviewee.
The data collection of the interview was conducted through audio recording by two electronic devices with voice recording software in .mp3 and .wav format.
The transcripts from the recordings made were obtained in full by the main researcher, following the interviews. None returned to the participants for comments and/or corrections.
A numeric code was assigned to each participant to ensure their anonymity in the study from the stage of obtaining the transcript of the audio recording.
Data Analysis: The main and the collaborating researchers independently went ahead to review the transcripts, using thematic analysis method to identify original emerging themes for the two underlying domains (Barriers to discontinuation / Facilitators to discontinuation). Thematic analysis data were organized using Microsoft Excel ® software.
A second version of the thematic analysis was obtained, reconciling the data obtained by the two researchers by consensus.
A third (definitive) version of the thematic analysis was obtained, adapting the original themes obtained to those previously found in the systematic review by Rasmussen et al. [
5].
At every stage of the data analysis process, we intended to understand key themes in the data and how they relate to one another, allowing the ongoing inclusion of emergent themes, which were supported by participants’ quotations.
The
Consolidated Criteria for Reporting Qualitative studies (COREQ) [
16] was used to ensure the study met the recommended standards of qualitative data reporting.
Ethical Considerations: The study was conducted in accordance with the Declaration of Helsinki and approved by the Alentejo’s Regional Health Administration Ethics Committee (Process number 09/CE/2022. Feedback number 05/CE/2022, 2022/05/12). In this regard, and at the request of the Ethics Committee, the researcher added a safeguard to the Study Protocol, in the event that, during the interview, the perception of some clinical condition or other in the interviewee that could imply, due to professional responsibility, the need for some type of medical intervention, the appropriate referral would be made to the respective family health team, provided that the express consent of the interviewee was obtained, with the exception of legally foreseen circumstances. This eventuality did not occur in any of the 15 interviews carried out. Also, aiming to minimize any possible negative impact on the participant's health that could result from carrying out the interview, the Protocol also expressed the possibility that it could be interrupted in the event of any circumstance that could constitute an overload (physical or psychological) to its continuation. This situation also did not occur in any of the interviews carried out.
3. Results
3.1. Participant Characteristics
Fifteen individual interviews were conducted with selectable patients, the longest lasting 27 minutes and the shortest 10 minutes. Each interview was carried out in a single moment and none of the interviewees withdrew from participating in the study during or after the interview. Eleven in fifteen of those interviewed were women. The median age was 70 years (mean 71.3), ranging from 65 to 82 years of age. All respondents were medicated with only one BZRA, the most frequent being brotizolam 0.25 mg and ethyl loflazepate 2 mg. The time elapsed since the current BZRA prescription ranged from 1 to 22 years, with a median of 8 years (mean 7.6 years). Nine of the interviewees had previously been medicated with other BZRAs other than the current one. The reasons for taking BZRA, according to the interviewee, varied between insomnia and anxiety with equal frequency. Ten of the interviewees were taking BZRA continuously and six had made previous attempts to discontinue it (
Table 1).
3.2. Barriers and Facilitators do Discontinuation of BZRA
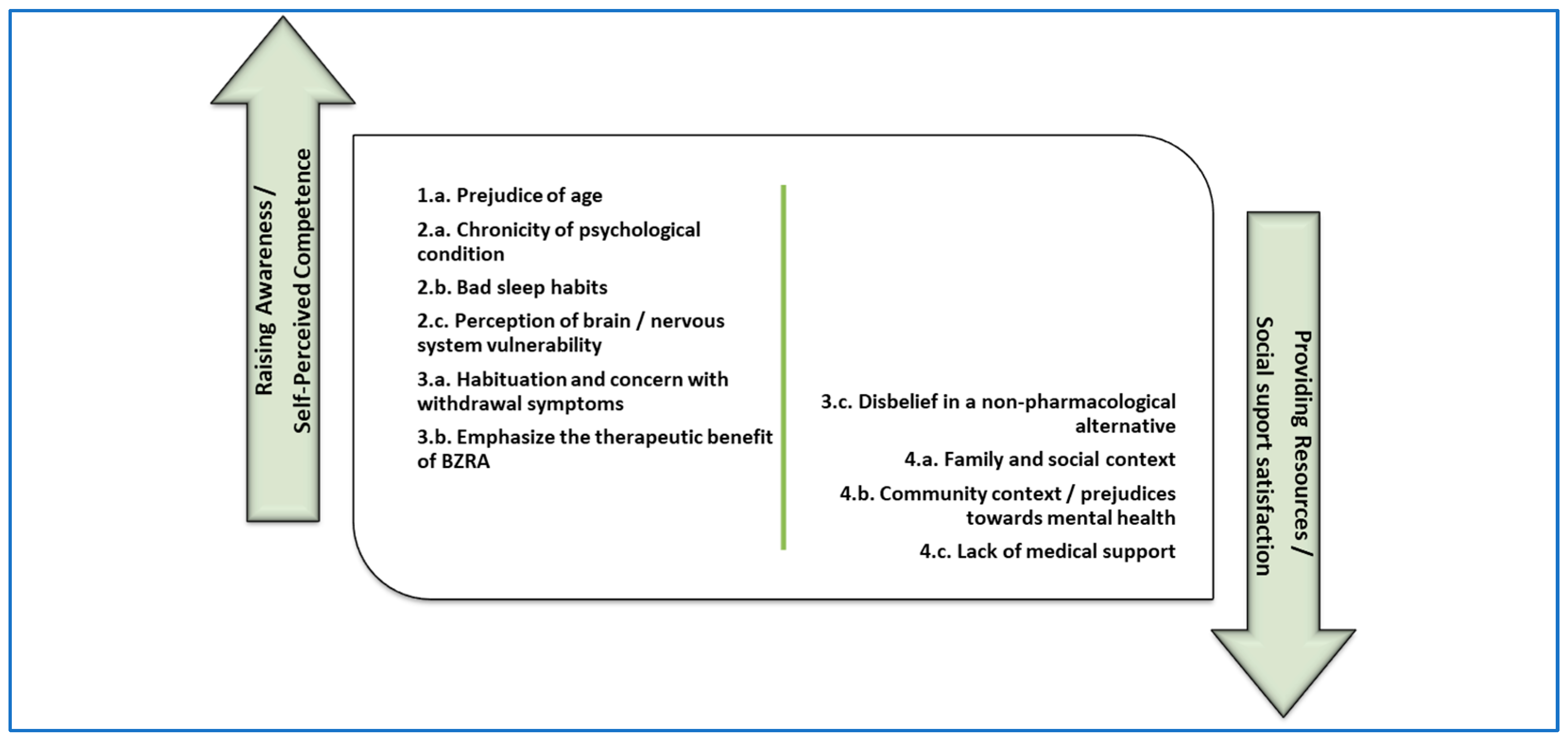
After adjusting the data obtained individually by each of the two investigators in the content analysis performed, about the barriers to discontinuation of BZRA, four themes emerged, subdivided into eleven specific sub-themes. Themes identified were:
1. Patient characteristics, subdivided into subtheme 1.a.) Prejudice of age.
2. Clinical factors, subdivided into subthemes 2.a.) Chronicity of the psychological condition related to the use of BZRA; 2.b.) Bad sleep habits; 2.c.) Perception of brain / nervous system vulnerability.
3. Medication-related factors, subdivided into subthemes 3.a.) Habituation and concern with withdrawal symptoms; 3.b.) Valuing the therapeutic benefit of BZRA; 3.c.) Disbelief in a non-pharmacological alternative.
4.Context and external factors, subdivided into subthemes 4.a.) Family and social context; 4.b.) Community context / Prejudices towards mental health; 4.c.) Lack of medical support; 4.d.) Other anxiety inducers.
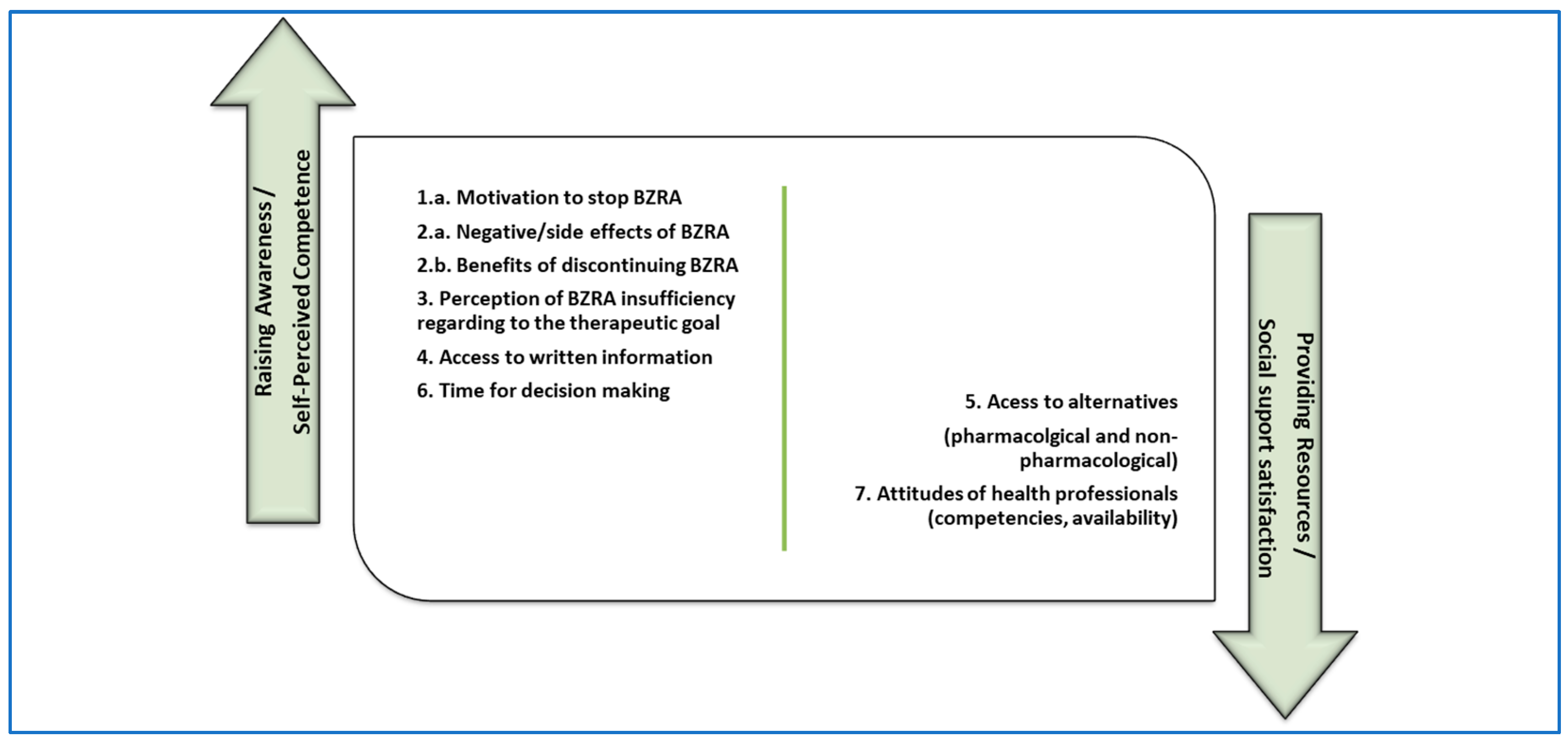
Regarding the facilitators to discontinuation of BZRA, seven themes and six sub-themes emerged. Themes identified were:
1. Motivation to stop BZRA.
2. Patient’s knowledge about BZRA, subdivided into subthemes 2.a.) Negative/side effects of BZRA; 2.b.) Benefits of discontinuing medication.
3. Perception of BZRA insufficiency regarding to the therapeutic goal.
4. Access to written information.
5. Access to alternatives, subdivided into subthemes 5.a.) Pharmacological alternatives; 5.b.) Non-pharmacological alternatives.
6. Time for decision making.
7. Attitudes of health professionals, subdivided into subthemes 7.a.) Competencies; 7.b.) Availability.
Text Boxes A1 and A2 (
Appendix A) compile the identified factors, documented with illustrative quotes selected as the best descriptive for each theme/sub-theme. Each quote is followed by the code assigned to each interviewee.
4. Discussion
Summary of key findings: This study enabled the identification of barriers and facilitators towards the discontinuation of BZRA from the perspective of elderly patients in a rural community in Portugal, chronically medicated with this pharmacological group.
Four themes emerged as barriers to BZRA deprescribing (patient characteristics; clinical factors; medication-related factors; context and external factors), subdivided into eleven specific sub-themes.
Seven themes emerged as facilitators to BZRA deprescribing (motivation to stop BZRA; patients' knowledge about BZRA; perception of BZRA insufficiency regarding to the therapeutic goal; access to written information; access to alternatives; time for decision making; attitudes of health professionals), subdivided into six specific sub-themes.
Comparison with previous literature: Regarding the
Barriers to discontinuation of BZRA, four of the identified sub-themes corresponded to themes identified in the systematic review by Rasmussen et al. [
5]: 1.a:
prejudice of age; 3.a:
habituation and concern with withdrawal symptoms; 3.b:
valuing the therapeutic benefit of BZRA; 4.c:
lack of medical support. Seven new sub-themes emerged that did not correspond to those identified in the aforementioned review: 2.a:
chronicity of the psychological condition related to the use of BZRA; 2.b:
bad sleep habits; 2.c:
perception of brain / nervous system vulnerability; 3.c:
disbelief in a non-pharmacological alternative; 4.a:
family and social context; 4.b:
community context / prejudices towards mental health; 4.d:
other anxiety inducers.
Concerning 1.
patient characteristics, other studies point out several topics that didn’t emerge in this study such as ‘the existence of an underlying condition forming part of individuals’ identity and necessitating BZRA use’ [
8], ‘patients’ negative perceptions of insomnia and its impact and failed self-care strategies’ [
9].
Regarding 2.
clinical factors,
chronicity of the psychological condition related to the use of BZRA (2.a.) is also pointed out by Lynch et al. [
8] as ‘a perceived continued need for BZRA use’. Allary et al. [
14] also found ‘intensity of depressive symptoms’ as a barrier to discontinuation.
Respecting 3.
medication-related factors,
habituation / concern with withdrawal symptoms (3.a.) is also pointed out by themes such as ‘identifying as being addicted to or dependent on BZRAs’, ‘negative impact of withdrawal symptoms and lack of continued availability of BZRAs if needed’ [
8]. Sirdifield et al. [
9] underline ‘the perception from patients of being unable to reduce medication use’ and ‘fear of what would happen if they did discontinue (either based on imagined negative consequences or past experiences)’ as additional barriers.
Valuing the therapeutic benefit of BZRA (3.b.) is illustrated by Cook et al. [
6] as ‘the attribution to these medications of soothing properties that extend beyond their ordinary use, i.e., affording control over daily stress, bringing tranquility and even prolonging life’. It is also described that ‘self-reported benzodiazepine dependence was associated with perceptions of (…) feeling reliant on benzodiazepines to be comfortable and able to handle life’ [
8].
Disbelief in a non-pharmacological alternative (3.c.) is also pointed out by themes such as ‘availability and commitment required with non-BZRA alternatives’ and ‘effectiveness of alternatives to BZRAs’ [
8].
About 4.
context and external factors,
family and social context (4.a.) is also pointed out by themes such as ‘encouragement from family members to continue BZRA use’ [
8] and ‘importance of social support satisfaction’ [
14].
Community context / prejudices towards mental health (4.b.) is also illustrated as the ‘negative information regarding BZRA discontinuation-process posted on online
fora’ [
8].
Lack of medical support (4.c.) is also pointed out by themes such as ‘access to resources and supports for discontinuing BZRA use’, ‘variation in experience regarding BZRA use/discontinuation with different healthcare professionals’ and ‘perceived lack of insight into BZRA use and discontinuation methods among GPs’ [
8]. It is also described the ‘lack of support from GPs’, ‘a need for specialist withdrawal services’, and ‘absence of an appropriate support network’ as barriers to discontinuation of BZRA [
9].
Relating to the
Facilitators to discontinuation of BZRA, five of the identified themes corresponded to those identified in the systematic review by Rasmussen et al.[
5]: 1.:
motivation to stop BZRA; 2:
patients' knowledge about BZRA (subdivided into sub-themes 2.a:
negative/side effects of BZRA and 2.b:
benefits of discontinuing medication); 4:
access to written information; 6:
time for decision making; 7:
attitudes of health professionals (subdivided into sub-themes 7.a:
competencies and 7.b:
availability). Two new themes emerged that did not correspond to those found in the aforementioned review: 3:
perception of BZRA insufficiency regarding to the therapeutic goal; 5:
access to alternatives (subdivided into sub-themes 5.a:
pharmacological alternatives and 5.b:
non-pharmacological alternatives).
Regarding 1.
motivation to stop BZRA, it’s also pointed out by themes such as ‘confidence in ability to discontinue BZRA use’, ‘optimistic outlook towards BZRA discontinuation’, ‘support from family and friends regarding discontinuation of BZRA use’ [
8] and ‘self-perceived competence in the ability to withdraw’ [
14].
With reference to 2.
patients' knowledge about BZRA, it is also highlighted the ‘knowledge of potential risks associated with long-term BZRA use’ [
8]. Relatively to subtheme
negative/side effects of BZRA (2.a.), it is also pointed out that ‘patients’ knowledge of, and attitudes towards, potential side effects from medication could influence their patterns of use’ [
8]. Relatively to subtheme
benefits of discontinuing medication (2.b.), it’s also pointed out as ‘positive consequences of discontinuing BZRA use’ and ‘the goal of no longer being dependent on BZRA’ [
8]. It is also highlighted that among reasons for withdrawal is ‘a realization that the use of these drugs was interfering with their life and the people around them’ [
9].
No related themes were found in literature concerning 3. perception of BZRA insufficiency regarding to the therapeutic goal and 4. access to written information.
About 5.
access to alternatives, it is also pointed out ‘comparable symptomatic relief from any alternative intervention or non-BZRA treatment’ and ‘use of resources and supports to augment dosage reduction process’ [
8].
Relating to 6.
time for decision making it’s also marked the ‘use of gradual dosage reduction or limiting BZRA intake’ [
8].
Finally, respecting 7.
attitudes of health professionals, it is also highlighted ‘the patients’ perception of the attitude of physicians towards continuous benzodiazepine use’ as a key factor affecting discontinuation [
6]. It’s also pointed out ‘advice and support from healthcare professionals regarding discontinuation of BZRA use’ [
8]. Sirdifield et al. [
9] mark ‘attitudes towards treatment options/service provision’, adding in this regard that ‘patients discussed a desire for continuity of care, more discussion with a health professional prior to receiving a prescription and longer consultation times. Patients wanted more detailed information, and for their problem to be taken seriously.’
Strengths and limitations of the study: The relevance of this study stems from previous investigations related to this topic, which underline the need for further investigations with more focus on the patient's point of view [
4,
5,
6].
The emerging themes were framed in the information obtained found in literature, upon which the interview guide was built up.
All interviews were coded independently by two researchers, which enhanced the robustness of the analysis.
Other possible stakeholders that could have been enrolled in this context (health professionals, caregivers) were not involved in the study.
The results of this study should only be interpreted within the context in which it was developed, a group of patients aged 65 years and over, chronically medicated with BZRA, belonging to the same community in Alentejo Region (Portugal).
By restricting the sample to patients on current use of BZRA, we lack the perspective of patients who have successfully previously discontinued this medication.
The fact that only one researcher did the interviews, as well as the lack of previous experience in conducting semi-structured interviews, are potential bias of the study that may, therefore, have limited the possibility of exploring additional aspects which could be brought up with more experienced interviewers.
Implications for research: Figure 1 and
Figure 2 are a proposal for distribution of the elements identified as barriers and facilitators from the study, subdivided in two potential areas of intervention. We associated the aforementioned two main intervention typologies indicated by Ng et. al. [
4] with the two main psychological predictors for BZRA discontinuation pointed out by Allary et al. [
14] as main gains for withdrawal programs. Therefore, in the first (left) group we allocated factors related to
raising awareness interventions [
4] which we associated with
self-perceived competence in the ability to withdraw [
14]. In the second (right) group we allocated factors related with
providing resources for BZRA discontinuation [
4] which we associated with
social support satisfaction [
14].
This model may supply an opportunity for the design of a future implementation study in which in which different intervention components could be involved, such as dissemination among healthcare professionals of validated tools for BZRA discontinuation and health promotion strategies towards integration of this problem in the community. Examples of these strategies could be intersectional intervention, community participation and promoting literary, training and autonomy of people.
We intend that this study may provide a starting point either for other studies in this area of interest, as for the identification of potential targets for withdrawal programs or interventions, aiming at a more comprehensive approach that can meet the different variables involved in the maintenance of these drugs.
Learnings and insights: Considering the findings of this study we may ponder about how suitable may be to monitor the proportion of elderly patients without long-term prescription of BZRA as a measure of quality of life provision, taking into account the implications inherent to the socio-family and community context, difficulties in accessing non-pharmacological alternatives and risks inherent to discontinuation in patients with many years of prolonged BZRA intake.
In this sense, it may be important to ponder alternative ways of checking the proportion of elderly patients prescribed long-term BZRA. Some alternative possibilities could be to measure new long-term prescription users over a period, rather than in full, and also to value the implementation of local intervention programs towards the discontinuation of BZRA.
5. Conclusions
In this study, we intended to explore the experiences and perceptions of elderly patients from a rural community in Alentejo region (Portugal) under prolonged prescription of BZRA regarding their discontinuation, to identify barriers and facilitators that may lead to their chronic usage.
The findings highlight the challenging nature of BZRA discontinuation and the range of barriers and facilitators that may impact patients’ behaviour towards this purpose.
We subdivided the elements identified in two areas of intervention, according to the initial motivation indicated in the Introduction, therefore aiming at producing significant knowledge to outline potential intervention targets to support patients in discontinuing BZRA use, to reduce the prevalence of elderly patients under prolonged prescription of BZRA.
Author Contributions
Conceptualization, T.B.M.; Methodology, T.B.M.; Validation, A.L.N. and P.B.-G.; Formal analysis, T.B.M. and MN; Investigation, T.B.M. and M.N.; Writing – original draft, T.B.M.; Writing – review & editing, T.B.M. and M.N.; Supervision, A.L.N. and P.B.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Alentejo’s Regional Health Administration Ethics Committee (Process number 09/CE/2022. Feedback number 05/CE/2022, 2022/05/12).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy and ethical reasons.
Acknowledgments
The authors are grateful to all the participants who contributed to. this study and to everyone who facilitated the recruitment and dissemination of study-related information.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
BZRA
COREQ |
Benzodiazepine agonist receptors
Consolidated Criteria for Reporting Qualitative Studies |
DGS
ICPC-2 |
Directorate-General of Health (Portugal)
International Classification of Primary Health Care |
| MIM@UF |
Module for Information and Monitoring of Functional Units |
Appendix A
Text Box A1.1.
Themes and subthemes identified as Barriers to discontinuation of BZRA (part 1/3)
Text Box A1.1.
Themes and subthemes identified as Barriers to discontinuation of BZRA (part 1/3)
| 1. Patient characteristics |
| a. Prejudice of age |
"I think so (...) at this age, what should you do? On the couch... One no longer gets tired, doesn't do anything anymore, at night one can't sleep (...) " [M2]
|
"Yes, I think so [age interferes with the possibility of stopping BZRA] (...) For me it will no longer help, but it might help my children, who are in their 50s... " [W2]
|
|
"When we're young, we want to sleep. Now at old age we don’t, we think a lot, we no longer sleep (...) " [M4]
|
| 2. Clinical factors |
| a. Chronicity of the psychological condition related to the use of BZRA |
|
|
|
|
| b. Bad sleep habits |
|
"And then if I come down here at 10 or 11 o'clock, I sit there a little bit on the couch, that's when I get to sleep. (…) If I go to bed, I don't sleep... But here on the couch, I'm watching TV, I want to watch the news, and then I let myself asleep!" [M4]
|
| c. Perception of brain / nervous system vulnerability |
|
"(...) we have already a certain age, therefore we have a weakest brain, I am aware of that. And then the brain will get those things, always... Even if we want to forget, we can't." [W3]
|
|
|
Text Box A1.2.
Themes and subthemes identified as Barriers to discontinuation of BZRA (part 2/3)
Text Box A1.2.
Themes and subthemes identified as Barriers to discontinuation of BZRA (part 2/3)
| 3. Medication-related factors |
| a. Habituation and concern with withdrawal symptoms |
"Possibly, if one keeps not resting as he should, not sleeping as he should, headaches may arise, many problems may arise. " [M2]
|
|
|
"If I don't take it, I'll spend a whole night... Because once there weren’t these pills, (...) they prescribed me some others (...), I spent a whole week without sleeping!... I even thought I went mad, I couldn’t sleep either night or day" [W5]
|
|
"I think this drug should also give habituation, certainly, like any other alike it, doesn't it?... The thing is I feel good having it and I don't think it will do to me anything opposite of what I intend from taking it (...) I'm so used taking that pill and feeling good with it, I really don't know what would happen if I had to stop it." [W7]
|
|
| b. Valuing the therapeutic benefit of BZRA |
|
|
"It's to rest my brain so that next morning I’m able to carry my life forward. (...) Because when I take this precious pill, after half an hour I'm asleep... If I don't take it, I spend a whole night awake..." [W5]
|
"Because I'm doing really fine with it (...) I couldn't sleep anymore, I couldn't eat, I couldn't do anything... I’ve been so bad, so bad..." [W6]
|
"(...) in a way, it calms me down to face situations that come across me (...) With this medicine, I can face things more lightly, in a better way, doing my normal life." [W7]
|
"... I take it, that day... for that moment (...) And that's it, after a while it does the effect I intended, and I carry on…" [W11]
|
| c. Disbelief in a non-pharmacological alternative |
|
"(...) that's why I say it wouldn't be worth another health professional in any other subject, either psychologist or whatever, because it really [would always need a pharmacological alternative]" [W7]
|
Question: "... Do you consider the possibility of an alternative which doesn’t involve medication? " Answer: "There are so many, aren’t there?... I could also train my mind, so I won’t have to deal with this, but no... Other than medicines, I don’t see any other way." [W11]
|
Text Box A1.3.
Themes and subthemes identified as Barriers to discontinuation of BZRA (part 3/3)
Text Box A1.3.
Themes and subthemes identified as Barriers to discontinuation of BZRA (part 3/3)
| 4. Context and external factors |
| a. Family and social context |
Question: "Therefore, having to deal with such a difficult situation for such a long time [family members with alcohol problems], you think that hardly anyone would be able to help you, is that right? " Answer: "I think so" [W1]
|
"Then I get anxious, and everything comes to my mind... The past, being alone, living with a retirement pension of less than five hundred euros... " [W5]
|
"... I’ve had a lot of problems in my family with people who have died, including my husband... and so it wasn't easy ... within four years I lost three people... Since then, there's always this feeling remaining that you cannot carry on alone ... having to deal with so many events, you see? " [W7]
|
|
"...the health of those close to me concerns me a lot. (...) Because it's a lot of accumulated stuff, and it turns out to be that the escape [BZRA intake] that makes me calm down a little bit. (...) This one of those situations which, even if we want to, we can’t make it otherwise ... That's a fact." [W11]
|
| b. Community context / Prejudices towards mental health |
"Nobody took me to the psychiatrist, it was me who felt like I was going crazy. Since then, I start going there on my own, even now it is still so, no one goes with me, and no one forces me to go there. Because my ancestors, from my mother's side, everyone died crazy. (...) And I'm very afraid of that. " [W5]
|
"... I think we all live very closed up... very closed up. And on mental health, or mental well-being, in my point of view, those things we all keep very much to ourselves. (...) If you don’t feel at ease, you keep it to yourself... Otherwise others may think you are crazy! So, it’s better not to say anything..." [W11]
|
| c. Lack of medical support |
|
|
| d. Other anxiety inducers |
"Pain also interferes with these things... If you don't have pain, you sleep better...But with pain... it's a problem... Then it's a headache, then it’s also those things in my head, vertigo... (...) It's already the nervous system that I have." [M4]
|
|
"Because my heart beats very fast, I get tired afterwards... I feel so tired, I get very anxious... my hands freeze a lot, I get very anxious (...) Then I take that pill, that day, for that moment." [W11]
|
Text Box A2.1.
Themes and subthemes identified as Facilitators for the discontinuation of BZRA (part 1/2)
Text Box A2.1.
Themes and subthemes identified as Facilitators for the discontinuation of BZRA (part 1/2)
| 1. Motivation to stop BZRA |
|
|
| 2. Patient’s knowledge about BZRA |
| a. Negative/side effects of BZRA |
Question: "Who do you think could help you stop this medication, first of all? " Answer: "First of all... for me, I should go to a doctor ... to realize if this medication could bring me trouble or not..." [M1]
|
| b. Benefits of discontinuing medication |
"One time I said to myself: "I don't take them anymore! » It was even worse! I didn't dream so many stuffs, but I couldn't get myself asleep... But I didn't dream so much, with this medicine you imagine things while you sleep..." [M4]
|
"I'm really sick with taking it... It's not because it harms me, but still, I don't know… This addiction, if I just could do without it, it would be good..." [W9]
|
"As it has its effect on me, it whets my appetite and that's when I get to eat… And as I tend to put on weight, I think it even does me so, I can't lose weight because of this medication." [W10]
|
| 3. Perception of BZRA insufficiency regarding to the therapeutic goal |
"Look, it has this effect: if I go to bed and don't think about the pill, sometimes I even sleep well... It’s all psychological!... And if I go to bed and realize, "Hey! I didn't take the pill! ", I can't sleep!... I just have to take it! " [M4]
|
" This kind of medication also has a lot to do with our ability to fit things in our head... Because sometimes I think that when we take the pill, of course it does what it has to do in ourselves, but the fact that we know we are taking it also comforts us somehow... " [W11]
|
| 4. Access to written information |
|
|
|
Text Box A2.2.
Themes and subthemes identified as Facilitators for the discontinuation of BZRA (part 2/2)
Text Box A2.2.
Themes and subthemes identified as Facilitators for the discontinuation of BZRA (part 2/2)
| 5. Access to alternatives |
| a. Pharmacological alternatives |
|
"There's already so much you can take, natural products, from what I'm told... But I've never got into that yet... But maybe there are some other things at the pharmacy ... A kind of supplement, something that could replace that pill but that was a natural product..." [W9]
|
| b. Non-pharmacological alternatives |
"If I stand a while without taking it, or if there was something else that the doctor should advise me: "For your health or for your age, I think the proper medicine is this...", then I might even try other things instead." Question: "What kind of "other things" could help other than medication?" Answer: "A psychologist. It could be a psychologist." [W3]
|
|
| 6. Time for decision making |
|
"Yes, only if I was given the time to think even a little bit... Other than that, I couldn't, no, I couldn't..." [W6]
|
|
| 7. Attitudes of health professionals |
| a. Competencies |
|
|
|
Question: (…) so, considering this possibility, you think only a specialized doctor could help?" Answer: "With all due respect, I think a general practitioner wouldn’t be able to help on this." [W6]
|
|
| b. Availability |
"If in one of my regular medical appointments, (…) my doctor says to me "you should stop taking this medication, because this may be harming you for this and for that reasons", then automatically I shall stop taking it..." [M1]
|
References
- Ministry of Health: Central Administration of the Health System (Portugal). Bilhete de Identidade dos Indicadores dos Cuidados de Saúde Primários para o ano de 2017 [Identity card of Primary Health Care Indicators for the year 2017]. 2017.
- Directorate-General of Health (Portugal). Norma 055/2011 (atualização 21/01/2015): Tratamento Sintomático da Ansiedade e Insónia com Benzodiazepinas e Fármacos Análogos [Clinical Guideline 055/2011 (updated 21/01/2015): Symptomatic Treatment of Anxiety and Insomnia with Benzodiazepines and Analogue Drugs]. 2015.
- Oliveira J, Neves I, Fernandes M, et al. Prescribing and facilitating withdrawal from benzodiazepines in primary health care. Revista Portuguesa de Clínica Geral. 2019 07/01;35:305-312.
- Ng BJ, Le Couteur DG, Hilmer SN. Deprescribing Benzodiazepines in Older Patients: Impact of Interventions Targeting Physicians, Pharmacists, and Patients. Drugs Aging. 2018 Jun;35(6):493-521. [CrossRef]
- Rasmussen AF, Poulsen SS, Oldenburg LIK, et al. The Barriers and Facilitators of Different Stakeholders When Deprescribing Benzodiazepine Receptor Agonists in Older Patients-A Systematic Review. Metabolites. 2021 Apr 20;11(4). [CrossRef]
- Cook JM, Biyanova T, Masci C, et al. Older patient perspectives on long-term anxiolytic benzodiazepine use and discontinuation: a qualitative study. J Gen Intern Med. 2007 Aug;22(8):1094-100. [CrossRef]
- Voshaar RC, Gorgels WJ, Mol AJ, et al. Predictors of long-term benzodiazepine abstinence in participants of a randomized controlled benzodiazepine withdrawal program. Can J Psychiatry. 2006 Jun;51(7):445-52. [CrossRef]
- Lynch T, Ryan C, Cadogan CA. 'I just thought that it was such an impossible thing': A qualitative study of barriers and facilitators to discontinuing long-term use of benzodiazepine receptor agonists using the Theoretical Domains Framework. Health Expect. 2022 Feb;25(1):355-365. [CrossRef]
- Sirdifield C, Chipchase SY, Owen S, et al. A Systematic Review and Meta-Synthesis of Patients' Experiences and Perceptions of Seeking and Using Benzodiazepines and Z-Drugs: Towards Safer Prescribing. Patient. 2017 Feb;10(1):1-15. [CrossRef]
- Reeve E, Ong M, Wu A, et al. A systematic review of interventions to deprescribe benzodiazepines and other hypnotics among older people. Eur J Clin Pharmacol. 2017 Aug;73(8):927-935. [CrossRef]
- Gould RL, Coulson MC, Patel N, et al. Interventions for reducing benzodiazepine use in older people: meta-analysis of randomised controlled trials. Br J Psychiatry. 2014 Feb;204(2):98-107. [CrossRef]
- Paquin AM, Zimmerman K, Rudolph JL. Risk versus risk: a review of benzodiazepine reduction in older adults. Expert Opin Drug Saf. 2014 Jul;13(7):919-34.
- Fixsen AM, Ridge D. Stories of Hell and Healing: Internet Users' Construction of Benzodiazepine Distress and Withdrawal. Qual Health Res. 2017 Nov;27(13):2030-2041.
- Allary A, Proulx-Tremblay V, Belanger C, et al. Psychological predictors of benzodiazepine discontinuation among older adults: Results from the PASSE 60. Addict Behav. 2020 Mar;102:106195.
- Alves-dos-Reis T, Serra H, Faria I, et al. General Practitioners’ Perspectives Over Solutions To Change BZD Prescription Trends – A Qualitative Study. 2021.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007 Dec;19(6):349-57.
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).