1. Introduction
Anxiety is a common negative emotion that many people experience when undergoing a surgical procedure, potentially impacting the course of their recovery adversely. The first existing definition of preoperative anxiety is attributed to Ramsay M.A. [
1], who described it as “an unpleasant state of discomfort or tension in the patient, secondary to their concern about illness, hospitalization, anesthesia, or surgery”. Various studies have shown that the vast majority of patients scheduled for surgery, up to 62%, experience moderate preoperative anxiety [
2]. Among the etiological factors, they found concerns about the anesthetist’s experience, the duration of the surgical process, the possibility of waking up during surgery, limitations, and the presence of postoperative nausea, vomiting, or pain.
Cataract surgery is one of the most common surgical procedures, with this condition ranking as the leading cause of blindness worldwide. There are bibliographic records indicating that more than 22 million cataract surgeries are performed annually worldwide [
3]. As in other surgical interventions, ocular surgery can induce significant anxiety, often linked to fear of the procedure being painful, deterioration or loss of vision, fear of moving the head during the intervention, among other concerns [
4].
Considering the increasing number of surgeries and the associated anxiety, it is of vital importance to measure its levels and design mechanisms for its reduction. There are various scales for assessing anxiety, such as the State-Trait Anxiety Inventory (STAI) questionnaire, but not all of them are applicable to a surgical process. Therefore, it is necessary to use a brief and easy-to-use tool in a perioperative setting that allows for quick and approximate results regarding the patient’s anxiety state. The APAIS scale (Amsterdam Preoperative Anxiety and Information Scale), created and validated by Moerman N. [
5], is considered a practical and useful tool. Several studies have used this measuring instrument to identify preoperative anxiety and the need for information in patients undergoing ocular surgery [
6].
The management of anxiety before a surgical intervention is part of the standardized nursing care, particularly during preanesthetic assessment, as asserted by Medina-Garzón M. [
7]. During that visit, a therapeutic relationship is established through the implementation of specific standardized nursing interventions, such as
Anxiety reduction (5820) and
Pre-surgical teaching (5610), which promote an environment of trust and security by conveying information to the patient according to their needs [
8]. Both interventions involve a series of activities such as describing preoperative routines, informing about what will be heard or seen during the process, assisting in creating a realistic description of the impending event, among others.
The Nursing Interventions Classification (NIC) is a comprehensive, standardized classification based on research on the various interventions performed by nurses. This classification was first published in 1992 by the American Nurses Association (ANA), allowing for the establishment of standardized nursing languages. In addition, the advanced practice nurse conducts nursing care documentation using standardized language according to the North American Nursing Diagnosis Association (NANDA), which establishes globally accepted nursing diagnoses and has contributed to the profession’s development. Through this, a specific care plan can be established, defining expected outcomes (NOC) and the nursing interventions (NIC) necessary to achieve them. Many studies conducted by nurses determine and examine the effectiveness of NIC interventions in patients undergoing a specific surgical process, thus deepening nursing care to achieve quality advanced practice [
9,
10]. One of the most applied nursing interventions in a surgical process would be
Learning Facilitation (5520), which aims to promote the ability to process and understand information, encompassing activities such as incorporating multimedia presentations, informational pamphlets, videos, and online resources, presenting information in a stimulating manner, among others. The different instruments mentioned are used for their positive effects on pre-surgical anxiety control and post-surgical pain. In addition to being a cost-effective intervention, it is recommended that it be carried out by nurses [
11].
Another new multimedia resource that has been gradually implemented in health sciences, offering innovative solutions in healthcare, is the use of Virtual Reality (VR). In previous studies, VR has been considered a safe and effective resource, complementary to analgesia protocols, capable of reducing pain and anxiety in patients undergoing surgery, as demonstrated by Mosso Vázquez J.L. [
12].
The objective of this study is to describe the prevalence of anxiety in patients undergoing cataract surgery and to assess the impact of a nursing intervention using an informational video. The relationship between preoperative anxiety and postoperative pain was also investigated.
2. Materials & Methods
2.1. Setting and Sample
A total of 147 patients awaiting cataract surgery were randomly selected and classified into an intervention group or a control group. The study was conducted in the ophthalmology department of a public hospital, between October 2022 and April 2023. The inclusion criteria were: voluntarily accepting participation in the study, being over 18 years old, undergoing cataract surgery for the first time, having knowledge and understanding of Spanish, and binocular visual acuity greater than 10.0%. Patients under 18 years old, those who did not have proficiency in Spanish, individuals with cognitive impairment, mental health conditions hindering participation, or those who refused to sign the informed consent were excluded from the study.
The sample size calculation is based on the data resulting from the APAIS scale in the sample studied in other similar studies, where a mean of 16.2 points with a standard deviation of 6.1 was obtained. It is established that a difference of 3 points is the minimum clinically relevant to consider the success of the new protocol. Therefore, for a comparison between two groups of a quantitative variable using a Student’s T-test for independent data, two-tailed test, an alpha error of 0.05, and a statistical power of 80.0%, 70 patients are needed per group (140 patients in total) to detect a statistically significant difference of at least 3 points on the APAIS scale, assuming a standard deviation of 6 and considering a maximum follow-up loss of 10%. The inclusion of more patients, reaching a total of 147, helped prevent possible participant losses throughout the study, which strengthened the validity and reliability of the results obtained. Despite this, there were no withdrawals of patients throughout the study.
2.2. Ethical Considerations
The institutional Ethics Committee for Drug Research at the hospital XX approved this study, protocol number 202X/105X0. Participation in these evaluative processes was voluntary and confidential. This study pursues quality standards, including respect for persons, beneficence and non-maleficence, and justice. All participants provided written informed consent regarding their involvement in the study. Information regarding participants’ data is guaranteed to be kept confidential, and each participant gets the same rights and treatment in the study. The research was conducted in accordance with the World Medical Association’s Ethical Principles for Medical Research Involving Human Subjects, Declaration of Helsinki (1964).
2.3. Instruments
The APAIS questionnaire [
5], is a validated measuring instrument with a short completion time. It is effective in detecting preoperative anxiety and easily applicable to the older population. This last piece of information is crucial to consider since the vast majority of the patients attended are of advanced age. The questionnaire has been used in similar studies [
13] to assess the presence of preoperative anxiety and the need for information before surgical interventions. It was translated into Spanish and validated in other studies, such as the one conducted by Vergara-Romero [
14]. It is a self-completion instrument composed of 6 questions. Four of them gather information regarding the fear of surgery and anesthesia, while the remaining two identify the need for more information (
Table 1). The response to each question follows a Likert scale with 5 options, ranging from 1 “not at all” to 5 “extremely.” The sum of all these values results in a score ranging from 6 to 30 points.
According to the original authors, the observed cutoff points were set at 11, increasing to 13 when used for research purposes. Vergara-Romero [
14] achieved a cross-cultural adaptation and validation of the Spanish version, resulting in a version with semantic, idiomatic, and conceptual equivalence to the original. The cutoff points established to determine clinically significant anxiety in a patient are ≥ 14. The VAS-A measurement instrument is considered one of the scales most easily applicable in clinical practice due to its brevity and easy interpretation, especially in older individuals. It is based on a horizontal line of 100 mm in length, ranging from 0 (no anxiety) to 10 (extreme anxiety). The patient selects the point on the line that corresponds to their level of anxiety. The results are interpreted as mild anxiety ranging from 0 to 3 points, moderate from 4 to 6, and severe from 7 to 10 [
15].
The intervention variable has been the informational video. During its 3-minute duration, the sequence of the journey that patients typically undergo from admission to the Day Surgery Unit, for the surgical intervention until discharge to home, is shown.
The video showcased images of all the steps to be followed during the patient’s hospital stay, including all areas they will pass through on the day of surgery, activities throughout the perioperative process, the individuals involved, among others. The video was created by the study’s principal investigator and recorded on a regular day of clinical practice, with prior consent obtained from the center while maintaining the confidentiality and privacy of the patients depicted. Verbal permission was requested regarding the possibility of appearing in the video or refusal thereof. Additionally, the images were pixelated to prevent patient recognition.
2.4. Data Collection
For the execution of the study, initial approval was obtained from the Institutional Ethics Committee. The safety, well-being, and rights of the participating patients were the most important considerations taken into account and consistently prevailed over the interests of science. Each subject was informed that they could refuse to participate or withdraw from the study at any time. The research was conducted in accordance with the codes of good clinical practices. All data related to patients were anonymized throughout, preventing their linkage to individuals, as indicated by the local Organic Law 3/2018, of December 5, on the Protection of Personal Data and Guarantee of Digital Rights (2018).
To structure the interventions to be carried out throughout the entire study and achieve a more appropriate level of replication, a checklist was designed with a description of the interventions, taking into account the guideline list designed by Hoffmann T.C et al. [17]. Following standard clinical practice, patients diagnosed with cataracts and included on a surgical waiting list were visited by the ophthalmology nurse during the pre-anesthetic assessment.
After the nurse’s visit, the researcher individually explained the existence of the study to each patient. Once voluntary participation was accepted, sufficient time was provided to carefully read the informed consent, and any doubts were addressed. All criteria were assessed to ensure that each inclusion criterion was met and none of the exclusion criteria applied.
Patient inclusion was carried out successively, and for classification into each study group, a pre-designed randomization list was followed. This list was generated using random number tables obtained through computer programs, allowing for representative recruitment. Patients in the experimental group received standard usual care based on oral information, in addition to watching an informational video about the cataract surgery process. Access to the video content was shown by the principal investigator trained in the study protocol, who presented the video during the inclusion visit at a specific time, without providing a URL for unlimited access to the tool. Currently, efforts are being made to make the information content permanently available to future patients. The recruitment process, as well as data collection and intervention, took place in a room adjacent to the nursing consultation room, where participants had been previously attended. Privacy was preserved throughout, ensuring a quiet space for the participants.
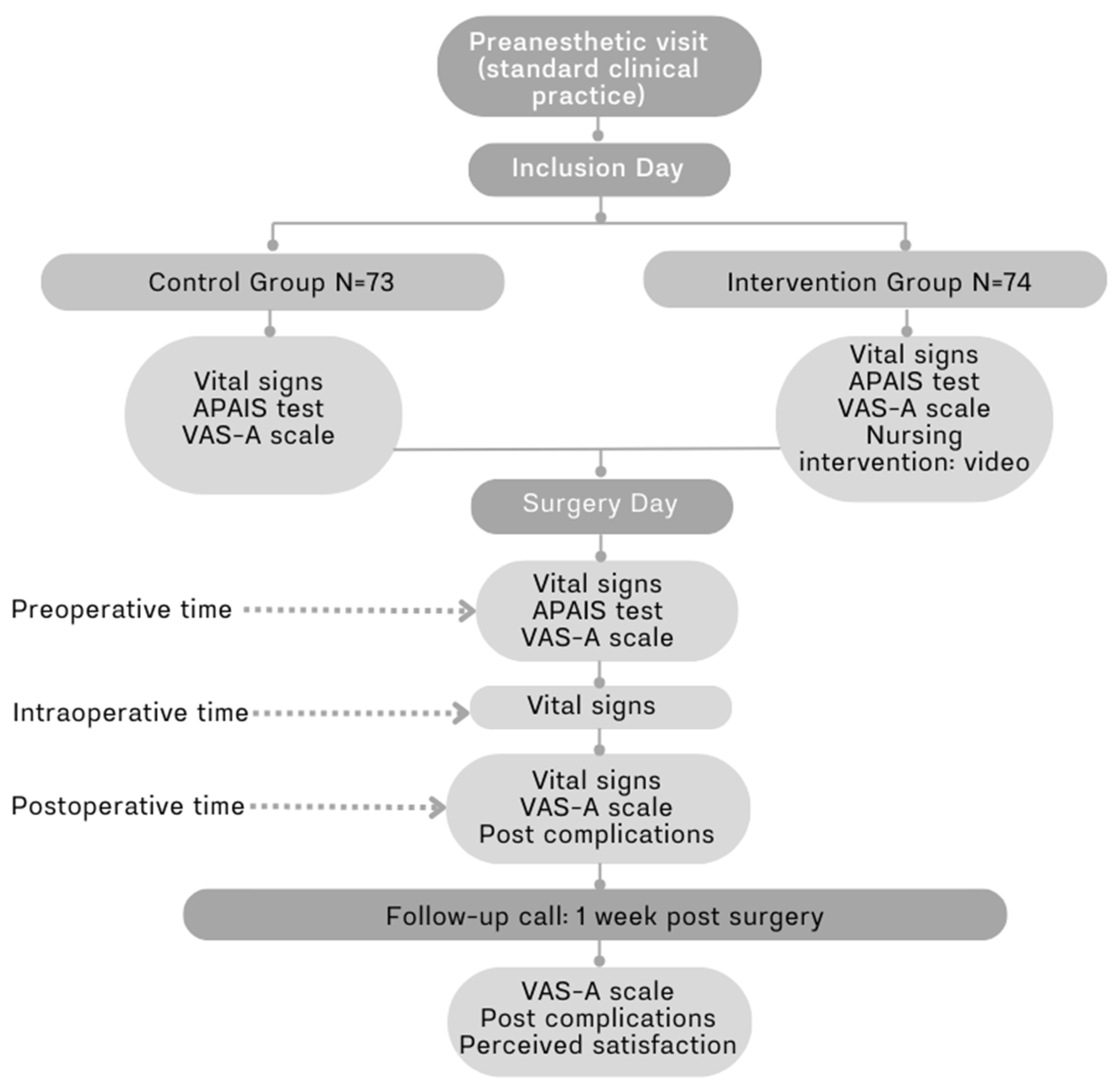
The variables collected during the inclusion visit for the study included sociodemographic data, previous surgeries, treatment with antidepressants and/or anxiolytics, blood pressure, heart rate, and post-surgical pain. Additionally, the APAIS questionnaire along with the VAS-A scale were administered. The APAIS test was initially measured on the day of inclusion in the study and for a second time on the day of surgery before the administration of preanesthetic medication. For the VAS-A scale, values were obtained at different times to assess fluctuations, initially during the study inclusion and on the day of surgery, both before and after the procedure. Finally, values were collected during the follow-up call, which took place 7 days after the intervention (
Figure 1).
2.5. Data Analysis
A descriptive analysis of the sample was performed. Quantitative variables were described using mean, standard deviation, median, and percentiles 25 and 75. Categorical variables were summarized with frequencies and percentages. Subsequently, bivariate analysis was conducted: Possible differences in quantitative variables regarding the group variable were tested using the student’s t-test for independent data or the Mann-Whitney U test depending on the conditions of application. The relationship between the dimensions and the total assessment of the APAIS questionnaire and quantitative variables was assessed using the Pearson and/or Spearman correlation coefficient. Finally, categorical variables were compared using the chi-square test or Fisher’s exact test as appropriate. In all tests, P values less than 0.05 were considered statistically significant. The analysis was carried out with the statistical program R 4.3 (R Core Team (2018). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL
https://www.R-project.org/).
3. Results
A total of 147 subjects were included randomly, with 73 in the control group and 74 in the intervention group, completing the study according to the protocol. The average age of the sample was 74 years, ranging from 27 to 94 years. 59.2% were women, and the remaining 40.8% were men. 77.6% had basic education, and 85.7% had previously undergone another surgical intervention. Additionally, 39.5% of the subjects had a prior diagnosis of anxiety or another psychological condition, and 56 subjects (38.1%) routinely took psychotropic medications. The most common patient profile would be a woman with basic education, without a prior diagnosis of anxiety or another psychological condition. Additionally, she is not undergoing psychotropic medication treatment and has previously undergone surgery, indicating prior experience in the operating room.
Analyzing the sociodemographic characteristics between both study groups reveals significant similarity without finding important differences (
Table 2).
In the intervention group, it is observed that 32.4% of participants had intermediate and/or university education compared to 12.3% in the control group. The percentage of women is slightly higher in the experimental group, with a difference of 6.0%. Additionally, in this same group, almost 5.0% more of the population has a prior diagnosis of anxiety. The history of previous surgeries in both cases is very similar. No significant differences have been found in other variables analyzed throughout the study, such as vital parameters, including blood pressure and heart rate.
The results of the APAIS questionnaire, as well as the VAS-A scale, are consistent and fluctuate depending on the moment of measurement, regardless of the study intervention performed. In both groups, an increase in anxiety levels is detected according to the APAIS questionnaire, with an average score of 12.80 points at the time of inclusion in the study and 13.70 points on average before surgery. There is an observed increase in anxiety as the day of the intervention approaches (
Table 3).
This increase in anxiety has been particularly noted in subjects over 76 years old. Despite the aforementioned figures, almost 30.0% of the subjects in the intervention group show a decrease in anxiety levels after the educational video. In addition, it should be noted that 100% of the subjects who participated in this group recommended the video, and 93.2% found it useful for the reassurance it provided by showing the sequence of steps to be taken on the day of surgery. Despite not finding a statistically significant relationship in the reduction of anxiety analyzed before the operation, this action is recommended by the subjects and considered highly useful.
Among the responses highlighted by participants in the APAIS questionnaire, the highest score was for the need to obtain more information about the operation (average score of 2.80 points at the inclusion visit and on the day of surgery). No differences were found between both study groups. This need has been particularly detected in patients under 64 years old. On the other hand, the lowest score was in the second item “I think about the anesthesia all the time,” in which the vast majority of subjects in both groups gave a score of 1.40 points at the inclusion visit and 1.5 on the day of surgery.
Complications after surgery were minimal in both groups, with constant tearing, itching, stinging, a sensation of a foreign body, and pain being the detected issues, with pain being the most frequent. 8.7% of the subjects in the intervention group experienced postoperative pain of mild intensity, compared to 14.9% in the control group, with 3.0% experiencing moderate to severe intensity in the latter. Despite not establishing a correlation between the variable of preoperative anxiety and postoperative pain, a slight trend of pain reduction has been observed in patients with lower anxiety levels in the comparison of their percentages (
Figure 2).
The resolution of complications was assessed one week after the day of surgery through a follow-up phone call. As part of this study, contact was made with each and every participant to evaluate whether the identified symptoms were resolved. It was observed that mild pain had persisted in the control group at a rate of 14.9%, although moderate to severe pain had decreased to 1.5%. However, mild pain increased in the intervention group, reaching 15.2%, which is 6.5% more than after the surgical intervention. Other reported symptoms included the persistence of a sensation of a foreign body and blurred vision.
The satisfaction of the study participants and their perception of the received assistance were also assessed using a numerical scale ranging from 0 as “Not satisfied at all” to 10 as “Maximum satisfaction.” The average result obtained was 9.44 points. During the same follow-up phone call, anxiety was reevaluated one week after surgery using the VAS-A scale, and it was observed that the average score for the entire sample was 1 point. The cause of this score was the persistence of post-surgical complications.
4. Discussion
Many patients awaiting elective surgery experience preoperative anxiety, which tends to increase as the scheduled date approaches. The results of this study indicate that the majority of the population experiences anxiety on the day of surgery, with 9% classified as severe and 55% as moderate according to the VAS-A scale. A slight upward trend in the final APAIS questionnaire score has also been observed, primarily in individuals over the age of 76.
Furthermore, from this age onwards, a higher percentage of diagnoses of anxiety or other psychological conditions have been identified, reaching 23.0% of the total sample, compared to 12.0% among those aged 65-75 and 4.0% in subjects under 64. In individuals over 76 years old, a slightly higher rate of post-surgical pain has been detected compared to other age groups. It would be interesting to analyze whether there is a significant relationship between these variables: a preoperative anxiety diagnosis and increased postoperative pain. Socea S.D. et al. [18] asserted that preoperative anxiety was the only significant predictor of pain, concluding that 20.0% experience anxiety and severe pain after cataract surgery.
In the present study, according to the APAIS scale, 52.5% of the sample had preoperative anxiety, mostly related to a lack of information about the surgery. This finding aligns with the study by Gómez Rodríguez S.V. et al. [19]. After using the APAIS questionnaire with a total of 241 patients undergoing elective general surgery procedures, they found a greater need for information related to the surgical procedure compared to anesthesia. Other studies that have also used the APAIS questionnaire have recorded higher anxiety levels in patients with a greater need for information [20]. Anxiety levels may vary depending on the timing of the APAIS instrument’s use. According to the literature, higher anxiety levels are recorded as the surgery date approaches, especially if measured just before the surgical intervention [21]. Similar trends can be observed in the present study, where the anxiety level increased by an average of 0.90 points in the total sample, going from 12.80 points on the day of inclusion to 13.70 points just before surgery.
Addressing these anxiety levels to prevent an increase before surgery has become one of the main objectives carried out during the pre-anesthetic assessment visit. Various nursing interventions have been designed to enhance care for surgical patients and reduce associated anxiety, as shown by Ruiz Fernández et al. [22] in a systematic review of different articles. They identified various types of pre-surgical visits conducted by nursing, in which various multimedia resources such as videos, pamphlets, or images were used. In their study, Wisely E. et al. [23] observed that an informational video about cataract surgery improves patients’ perception and anxiety about the procedure. With this type of intervention, considered cost-effective and effective, it is demonstrated that anxiety levels before surgery can be reduced, and overall patient perception can be improved [24]. Zhang et al. [25] also demonstrated in a study with 91 patients that the implementation of an informational video for patients undergoing cataract surgery improves understanding of the procedure and reduces anxiety levels.
The results found in our study contrast with those by Zhang et al. [25], confirming that the visualization of an informational video is useful for patients and facilitates their understanding of the surgical process. All subjects in our study who watched the video recommended its use, and in addition, 93.2% reported finding it useful. The time interval between the study intervention, in this case, the video presentation, and the surgical procedure may influence the final impact of the intervention, as demonstrated in the experimental clinical trial conducted by Felix M.M.S. et al. [26].
After creating two groups, they analyzed the impact of guided imagery therapy in the immediate preoperative period of bariatric surgery, finding significant differences between the control group and the intervention group regarding the reduction of anxiety. Similar results were observed in an experimental study conducted in a tertiary hospital in India [27], which evaluated the effectiveness of an informational video in reducing anxiety in patients undergoing elective infraumbilical surgery. Patients in the experimental group watched the video the day before surgery and experienced lower anxiety levels and higher satisfaction. Rajput S. K. et al. [28] observed, after using an informational video with patients undergoing spinal anesthesia and providing an electronic link for access, that anxiety levels immediately before the surgical intervention were lower. In our study, the intention was to present the video several days before the operation, given the limited timeframes established for surgical scheduling. Therefore, not showing the video on the same day of surgery or providing access for unlimited and close-to-surgery home viewing could be influential factors in the results found compared to the previous literature.
Some studies have demonstrated that the use of an informational video is helpful in managing anxiety generated by a surgical process. Others have evidenced the effectiveness of a nursing intervention based on the use of a useful micro video for physical and psychological recovery after enterostomy [29]. They showed that the improvement in psychological status and quality of life in the experimental group was significantly better than in the control group (p < 0.05). Principio del formulario
The literature evidences the relationship between pre-surgical anxiety and the development of complications such as pain, insomnia, nausea, and vomiting [30]. This is consistent with our study, where 23.6% of the total sample experienced pain after surgery, with higher rates observed in patients who had a higher level of preoperative anxiety.
5. Conclusions
The results of various studies show that the prevalence of preoperative anxiety increases as the surgery approaches and exacerbates pain and complications after the surgery, which aligns with our findings. The use of an informational video as an explanatory tool for patients undergoing cataract surgery is beneficial and helps reduce anxiety levels associated with the surgical process.
Based on our experience, a video showing real images of the care pathway the patient will undergo should be integrated into daily clinical practice as part of nursing interventions to facilitate learning and manage anxiety. This video should be viewed during the preoperative assessment of the patient as close to the day of surgery as possible, serving as an educational support tool to alleviate preoperative anxiety as well as postoperative complications (pain, nausea, vomiting, delayed recovery), and communication with the patient, ultimately enhancing the overall surgical experience. Furthermore, the implementation of digital tools to improve the patient experience represents innovation in traditional care, enhancing the effectiveness of nursing interventions in healthcare nursing care plans and overcoming the limitations of usual education.
Future research on the nursing process in surgical patients could be conducted to explore the impact of the video being used on the same day of the intervention, a few hours prior to surgery. This could potentially reduce the intermediate time that could lead to forgetting the information presented in the video.
Author Contributions
Conceptualization and Methodology -> Ideas; formulation or evolution of overarching research goals and aims. Development or design of methodology: 1,2,3,4 Investigation -> Conducting a research and investigation process, specifically data collection: 1 Formal analysis -> Application of statistical, mathematical, computational, or other formal techniques to analyze or synthesize study data: 1,2,3,4 Writing - Original Draft -> Preparation, creation and/or presentation of the published work, specifically writing the initial draft: 1,2,3,4 Supervision -> Oversight and leadership responsibility for the research activity planning and execution, including mentorship external to the core team: 2,3 Project administration -> Management and coordination responsibility for the research activity planning and execution: 1,2.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. No external funding.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Ramsay, M.A. A survey of pre–operative fear*. Anaesthesia. 1972; 27(4):396-402. [CrossRef]
- Çelïk F, Edipoglu I. Evaluation of preoperative anxiety and fear of anesthesia using APAIS score. European Journal of Medical Research. 2018;23. [CrossRef]
- Weiser T, Haynes A, Molina G, et al. Size and distribution of the global volume of surgery in 2012. Bulletin of the World Health Organization. 2016;94:201 - 209F. [CrossRef]
- Obuchowska I, Konopińska J. Fear and Anxiety Associated with Cataract Surgery Under Local Anesthesia in Adults: A Systematic Review. Psychology Research and Behavior Management. 2021;14:781-793. [CrossRef]
- Moerman N (Nelly), Dam FV, Muller MJ, Oosting H. The Amsterdam Preoperative Anxiety and Information Scale (APAIS). Anesthesia & Analgesia. 1996;82:445-451. [CrossRef]
- Lemaître S, González-Candial M. Evaluation of anxiety and pain in eyelid surgery patients: a pilot study. Canadian journal of ophthalmology. Journal canadien d’ophtalmologie. 2019;54 6:723-726. [CrossRef]
- Medina-Garzón M. Effectiveness of a Nursing Intervention to Diminish Preoperative Anxiety in Patients Programmed for Knee Replacement Surgery: Preventive Controlled and Randomized Clinical Trial. Investigacion y Educacion en Enfermeria. 2019;37. [CrossRef]
- Sepúlveda-Plata MC, García-Corzo G, Gamboa-Delgado E. Effectiveness of nursing intervention to control fear in patients scheduled for surgery. Revista de la Facultad de Medicina. 2018;66:195-200. [CrossRef]
- Kocaçal E, Karadağ E. Nursing diagnoses and NIC interventions in adult males undergoing radical prostatectomy. Revista da Escola de Enfermagem da U S P. 54:e03541. [CrossRef]
- Arslan E, Gezer N. The effect of discharge training developed based on nursing interventions classification (NIC) on surgical recovery in oncology patients: Randomized controlled trial - A pilot study. Nursing Open. 2022;10:1151-1162. [CrossRef]
- Álvarez-García C, Yaban Z. The effects of preoperative guided imagery interventions on preoperative anxiety and postoperative pain: A meta-analysis. Complementary therapies in clinical practice. 2020;38:101077. [CrossRef]
- Mosso Vázquez JL, Wiederhold BK. et al. Virtual Reality Assisted Anesthesia (VRAA) during Upper Gastrointestinal Endoscopy: Report of 115 Cases— Analysis of Physiological Responses. Surgical Research Updates. 2017;5. [CrossRef]
- Maurício S, Rebêlo I, Madeira C, Resende F, Esteves S. Validation of the Portuguese version of Amsterdam Preoperative Anxiety and Information Scale (APAIS). Health and Quality of Life Outcomes. 2020;19. [CrossRef]
- Vergara-Romero M, Morales-Asencio J, Morales-Fernández A, Canca-Sánchez JC, Rivas-Ruíz F, Reinaldo-Lapuerta JA. Validation of the Spanish version of the Amsterdam Preoperative Anxiety and Information Scale (APAIS). Health and Quality of Life Outcomes. 2017;15. [CrossRef]
- González-Estavillo AC, Jiménez-Ramos A, Rojas-Zarco EM, Velasco-Sordo LR, Chávez-Ramírez MA, Coronado-Ávila SA. Correlación entre las escalas unidimensionales utilizadas en la medición de dolor postoperatorio. Revista Mexicana de Anestesiología. 2018;41(1):7–14. Available online: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=77264.
- Boletín Oficial del Estado. Ley Orgánica 3/2018, de 5 de diciembre, de Protección de Datos Personales y garantía de los derechos digitales. (s/f). [Internet]. [citado el 21 de febrero de 2024]. Available online: https://www.boe.es/eli/es/lo/2018/12/05/3/dof/spa/pdf.
- Hoffmann, T. et al. Die TIDieR Checkliste und Anleitung – ein Instrument für eine verbesserte Interventionsbeschreibung und Replikation. Gesundheitswesen, 2016;78(03), 175-188. [CrossRef]
- Socea S, Abualhasan H, Magen O, et al. Preoperative Anxiety Levels and Pain during Cataract Surgery. Current Eye Research. 2020;45:471-476. [CrossRef]
- Victoria, G. R. S., Eugenia, D. L. R. V., & Alberto, D. C. N. “PREVALENCIA DE ANSIEDAD PERI-OPERATORIA EN PACIENTES SOMETIDOS a PROCEDIMIENTOS DE CIRUGÍA GENERAL ELECTIVA EN CENTRO MÉDICO ISSEMYM TOLUCA “LIC. ARTURO MONGTIEL ROJAS“ y HOSPITAL REGIONAL ATLACOMULCO DE JULIO a AGOSTO DEL 2016.”. Available online: http://hdl.handle.net/20.500.11799/65872.
- Jiwanmall M, Jiwanmall S, Williams A, et al. Preoperative Anxiety in Adult Patients Undergoing Day Care Surgery: Prevalence and Associated Factors. Indian Journal of Psychological Medicine. 2020;42:87-92. [CrossRef]
- Navarro-Gastón D, Munuera-Martínez PV. Prevalence of Preoperative Anxiety and Its Relationship with Postoperative Pain in Foot Nail Surgery: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020;17. [CrossRef]
- Hernández CRR, Gómez-Urquiza JL, Pradas-Hernández L, et al. Effectiveness of nursing interventions for preoperative anxiety in adults: A systematic review with meta-analysis. Journal of advanced nursing. 2021; 77(8), 3274-3285. [CrossRef]
- Wisely CE, Robbins CB, Stinnett S, Kim T, Vann R, Gupta PK. Impact of Preoperative Video Education for Cataract Surgery on Patient Learning Outcomes. Clinical Ophthalmology (Auckland, N.Z.). 2020;14:1365-1371. [CrossRef]
- Ahmed K, Pilling JD, Ahmed K, Buchan J. Effect of a patient-information video on the preoperative anxiety levels of cataract surgery patients. Journal of cataract and refractive surgery. 2019;45 4:475-479. [CrossRef]
- Zhang MH, Haq Z, Braithwaite EM, Simon N, Riaz K. A randomized, controlled trial of video supplementation on the cataract surgery informed consent process. Graefe’s Archive for Clinical and Experimental Ophthalmology. 2019; 257(8), 1719-1728. [CrossRef]
- Felix MMS, Ferreira MBG, Oliveira LF de, Barichello E, Pires P, Barbosa MH. Guided imagery relaxation therapy on preoperative anxiety: a randomized clinical trial*. Revista Latino-Americana de Enfermagem. 2018;26. [CrossRef]
- Kumar V, Yadav P, Bangarwa N, Budhwar D, Kumar P, Arora V. A Randomized Controlled Trial to Assess the Efficacy of a Pre-operative Virtual Operation Theatre Tour on Anxiety and Patient Satisfaction in Adults Undergoing Elective Surgery. Cureus. 2022;14. [CrossRef]
- Rajput S, Tiwari T, Chaudhary A. Effect of preoperative multimedia based video information on perioperative anxiety and hemodynamic stability in patients undergoing surgery under spinal anesthesia. Journal of Family Medicine and Primary Care. 2021;10(1):237-242. [CrossRef]
- Yan Q, Li Y. Micro video incentive nursing intervention improves the psychological state and quality of life in patients with rectal cancer after enterostomy. American journal of translational research. 2023;3:2040-2048. Available online: https://www.semanticscholar.org/paper/6250a62835bc72c5243dfbce1a0cec4cd2b0b839.
- Sobol-Kwapińska M, Bąbel P, Płotek W, Stelcer B. Psychological correlates of acute postsurgical pain: A systematic review and meta-analysis. European Journal of Pain. 2016;20 (10). [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).