Submitted:
23 December 2024
Posted:
24 December 2024
You are already at the latest version
Abstract
Background/Objectives: Several studies describe the sex-specific difference in cardiovascular diseases. However, there are still limited research reporting the difference between men and woman with chronic thromboembolic pulmonary hypertension (CTEPH) treated with ballon pulmonary angioplasty (BPA). The aim of the study was to evaluate sex–specific differences in patients with CTEPH treated with BPA. Methods: This retrospective study included CTEPH patients treated with BPA. Patients’ hemodynamic and clinical parameters were assessed at baseline and 3 months after completion of BPA treatment. Results: The study included 94 patients (44 women, 46.8%). At baseline women had higher systolic pulmonary arterial pressure (sPAP) (7618.5 vs. 8517.6 mmHg; p=0.03), and pulmonary vascular resistance (8.21 [5.55-10.17] vs. 9.89 [6.31-14.06] Wood Units; p=0.03), compared to men. There were no differences in clinical characteristics between sexes. At follow-up, women had lower sPAP (49 [41-54] vs. 43 [37-49] mmHg; p=0.04) and pulmonary capillary wedge pressure (10 [9-14] vs. 9 [8-11] mmHg; p=0.03), but higher cardiac index (2.570.53 vs. 2.820.50 L/min/m2; p=0.03), as well as better Dyspnea Borg Scale outcomes, compared to men. Women had greater reduction of mean pulmonary artery pressure (-43% vs. -37%; p=0.049) than men. Conclusions: At baseline, women with CTEPH had worse hemodynamic parameters than men despite similar clinical symptoms. However, women hemodynamic status was better after BPA therapy. Hence, women seem better adapted to the disease at baseline and respond better to the BPA. Further data are needed to investigate whether the management of CTEPH a patients should be sex–differentiated.
Keywords:
pulmonary hypertension
; chronic thromboembolic pulmonary hypertension
; ballon pulmonary angioplasty
; sex-specific differences
1. Introduction
Cardiovascular diseases (CVD) remain the leading cause of death among women and men worldwide [1]. In most clinical trials in cardiology, men dominate, and women are underrepresented. However, in the case of various forms of pulmonary hypertension (PH), the opposite is true: women predominate quantitatively among the participants in clinical trials [2,3,4,5]. This is due to the fact that women are more susceptible than men to several forms of PH [6,7].
Chronic thromboembolic pulmonary hypertension (CTEPH) is a condition defined by elevated pressure in pulmonary vascular bed caused by partial occlusion of the pulmonary arteries due to organized persistent thrombi, often accompanied by remodeling of patent resistive pulmonary arterioles [8]. Based on registry data, the prevalence of CTEPH is approximately 25.8-38.4 per million [9,10,11]. Balloon pulmonary angioplasty (BPA) is a minimally invasive procedure that has become an effective treatment option for CTEPH patients who are ineligible for pulmonary endarterectomy (PEA) or present with persistent PH after surgery [8,12,13,14].
Sex-specific differences in CTEPH have been studied, with some evidence suggesting that women may be at higher risk for developing CTEPH.[15]. Some studies suggest that there may be differences in the clinical presentation, risk factors, and outcomes of CTEPH treated by PEA between males and females [16]. However, there is limited research on the differences between women and men in CTEPH treated with BPA.
Therefore, the aim of this study was to evaluate sex–specific differences in patients with CTEPH who were treated with BPA procedures.
2. Materials and Methods
2.1. Study Design and Settings
This retrospective study included patients consulted by the CTEPH-team in the Department of Pulmonary Circulation, Thromboembolic Diseases, and Cardiology between October 2011 and September 2020. Medical history and clinical data were obtained retrospectively from patients’ medical records. As this was a retrospective study, patients were routinely diagnosed and treated, and no additional interventions were performed. A positive opinion from the Bioethics Committee was obtained (L.dz.OIL/KBL/27/2018).
Within routine patient management, the CTEPH-team provided multi-specialist consultations, established the CTEPH diagnosis based on invasive measurement of hemodynamic parameters during right heart catheterization (RHC) [17] and results of imaging studies and then referred patients to appropriate treatment methods: PEA, BPA, medical therapy, or combined therapy involving more than one of the mentioned methods according to current guidelines [8,18,19,20].
Data regarding patients’ characteristics were evaluated including age, anthropometric data, comorbidities, anticoagulant and supporting treatment and reasons for rejection from PEA. Hemodynamic data was obtained during RHC performed according to the current guidelines [17]. In addition, functional class defined by World Health Organization was noted, and results of 6-minute walking test (6-MWT) and Borg dyspnea scale ratings after 6-MWT were collected. Laboratory tests were performed including the levels of N-terminal pro-B-type natriuretic peptide (NT-proBNP) – reference value <125 pg/ml, high-sensitive troponin T – reference value <0.014 ng/ml and creatinine – reference value <0.9 mg/dl for women; <1.20 mg/dl for men.
Data of patients were analyzed at two points of time: at baseline and at follow-up. “Baseline” was defined as the moment of RHC performed before the first BPA procedure. “Follow-up” tests were performed, three to six months, after the last BPA procedure.
2.2. Statistical Analysis
Statistical analysis was performed with Statistica PL software (version 13, StatSoft, Tulsa, OK, USA). Categorical variables were presented as numbers and percentages. Continuous variables were presented as mean and standard deviation or median with interquartile range, depending on the distribution of the analyzed variable assessed using the Shapiro–Wilk test. The Chi-square test for categorized variables and Mann-Whitney U test for continuous variables were used to determine the differences between groups. For categorical variables with more than two categories, also Chi-square test was used. Statistical significance in the study was established at p < 0.05.
3. Results
3.1. Patients
From 417 consulted patients, 128 were included into the study (Figure 1). In 21 patients subsequent BPA sessions were planned; in 11 cases, due to the patient's mortality, the BPA series were unfinished, and follow-up was not performed. Contact loss occurred in 2 cases before the treatment with BPA was completed. Hence, the final population included 94 patients who terminated BPA treatment and had follow-up tests performed after the last BPA session. Among them, there were 44 (46.8%) females and 50 (53.2%) males.
3.2. Evaluation at Baseline
Women were nominally younger than men (median 54 [47-70] vs. 66 [54-73] years) however the differences were not statistically significant (p=0.07). Men were significantly taller and heavier and had greater body surface area, but not BMI. Regarding comorbidities, men were more likely to suffer from chronic obstructive pulmonary disease (COPD). No differences were observed regarding the anticoagulant treatment used – over half of both women and men used DOAC, and no differences regarding the use of specific medical therapy. There were also no significant differences in the reasons for rejection from PEA – the most common reason was distal pulmonary vascular obstruction in both men and women (Table 1).
Most of women and men presented the symptoms of III and IV WHO Functional Class at baseline. There was no difference between women and men regarding the severity of dyspnea assessed with the Borg scale after 6-MWT. Men presented higher serum levels of creatinine (Table 2).
Hemodynamic measurements at baseline (Table 3) showed that women had higher values of systolic pulmonary arterial pressure (sPAP) and pulmonary vascular resistance (PVR). In turn, men had higher stroke volume (SV).
3.2. Evaluation at Follow-Up
After BPA procedures, there were no differences in the number of sessions (median: 5; IQR: 4-7), the number of treated vessels during one session (mean: 7, SD 2.5) or the required amount of contrast (mean: 253 mL, SD 42.8), and radiation (median: 146 mGy; IQR: 90-248) between men and women. There were no differences in WHO functional classes of CTEPH regarding gender with most females and males presenting WHO class I or II after the BPA treatment was finished (Table 5). Serum levels of troponin and creatinine were significantly higher in men than in women. Evaluation with Dyspnea Borg scale after 6-MWT revealed some differences between sexes – 94.9% of women reported none or mild dyspnea while 20.4% of men reported moderate to rather/very intense dyspnea (Table 4).
Post-treatment RHC data are presented in the Table 5. Men had higher sPAP compared to women, as well as pulmonary arterial wedge pressure. In turn, women had higher mean value of cardiac index.
3.3. Treatment Outcomes
Analyzing the results of the CTEPH treatment with BPA, the classification of patients according to WHO class improved. Proportions of both women and men being class I-II and III-IV reversed at follow-up when compared with baseline outcomes (Figure 2).
Also, outcomes of Borg Dyspnea Scale improved, but benefits were more pronounced for women than for men (Figure 3).
Additionally, detailed analysis of RHC results at baseline and at follow-up was performed. Percentage changes of hemodynamic variables are graphically presented at Figure 4.
The values (both nominal and percentage) of mean pulmonary arterial pressure (mPAP) in women decreased more than in men (-20.9 mmHg vs. -15.8 mmHg, p=0.04; -43% vs -37%, p=0.049). Also, pulmonary vascular resistance (PVR) in women was nominally lower, than in men. but this observation regarded only nominal values (-6.64 j.W. vs. -3.85 j.W. p=0.048; -62% vs. -54%, p=0.12) Detailed hemodynamics variables changes is presented in the Table 5.

Table 5.
Patients’ hemodynamic outcomes at follow-up and changes in some variables from baseline to follow-up.
Table 5.
Patients’ hemodynamic outcomes at follow-up and changes in some variables from baseline to follow-up.
| Variable | Female (n=44) | Male (n=50) | p-value | |
|---|---|---|---|---|
| mRAP, mmHg | 5 [4-7] | 6 [3-7] | 0.77 | |
| sPAP, mmHg | 43 [37-49] | 49 [41-54] | 0.04 | |
| dPAP, mmHg | 15 [12-18] | 17 [13-22] | 0.05 | |
| mPAP, mmHg | 26 [22-30] | 29 [23-33] | 0.11 | |
| Δnominal | -20.9 [±12.2] | -15.8 [±10.8] | 0.04 | |
| Δ% | -43% [-57 – 25] | -37% [-47 – -18] | 0.049 | |
| PCWP, mmHg | 9 [8-11] | 10 [9-14] | 0.03 | |
| CI, L/min/m2 | 2.82 (0.50) | 2.57 (0.53) | 0.03 | |
| Δnominal | +0.40 [±0.77] | +0.30 [±0.50] | 0.42 | |
| Δ% | +16% [-1 – 51] | +11% [-5 – 32] | 0.34 | |
| SV, mL/beat | 70.87 (14.37) | 76.62 (20.02) | 0.12 | |
| SVI, mL/beat/m2 | 40.77 (7.61) | 38.33 (9.21) | 0.17 | |
| PVR, Wood Units | 3.34 [2.63-3.87] | 3.08 [2.58-4.49] | 0.65 | |
| Δnominal | -6.64 [-10.28 – -2.85] | -3.85 [-6.48 – -1.77] | 0.048 | |
| Δ% | -62% [-79 – -42] | -54% [-69 – -36] | 0.12 | |
Data are presented as median [interquartile range] or mean (SD). CI – cardiac index; dPAP – diastolic pulmonary arterial pressure; mPAP – mean pulmonary artery pressure; mRAP – mean right atrial pressure; PCWP – pulmonary capillary wedge pressure; PVR – pulmonary vascular resistance; SD – standard deviation; sPAP – systolic pulmonary arterial pressure; SV – stroke volume; SVI – stroke volume index.
4. Discussion
CTEPH is a rare condition, but it can lead to right heart failure, multiorgan disfunction, and death if left untreated. The BPA therapy which has been used relatively recently in the treatment of patients with CTEPH [21,22], has been upgraded in the recent guidelines for CTEPH treatment, which currently recommended BPA as a part of multimodal approach for patients who have inoperable lesions or have residual PH after PEA and distal obstructions amenable to BPA (class of recommendation IB). This procedure may also be applied to those patients who are operable but have a high proportion of distal disease and a PEA procedure may generate a high risk for them. BPA can also be considered in some symptomatic patients with CTEPD without PH [8].
The recent study which analyzed preoperative computed tomography pulmonary angiography of patients who underwent PEA for CTEPH identified sex-specific differences in the surgical cases [23]. Men had more vessels involved than women (mean 20.3 vs 17.1, p = 0.004) and had fewer disease-free pulmonary segments (mean 4.9, SD 4.3 vs 7.6, SD 5.5, p = 0.001). In addition, men had a greater number of webs, eccentric thickening, and occlusions. The distribution of lesion type did not significantly differ between sexes at the main or lobar level, but men had significantly more lesions in the segmental vasculature while women had a higher proportion of subsegmental lesions (p < 0.001) despite no significant differences in baseline hemodynamics [23]. Although, it was described that after PEA women benefit less in reduction of PVR (437 Dynes∙s∙cm−5 vs 324 Dynes∙s∙cm−5 in males, p < 0.01), the overall 10-years survival after surgical treatment was similar (73% in females vs 84% in males, p = 0.08) [24]. In multivariate analysis female sex remained an independent factor affecting the need for targeted PH medical therapy after PEA (HR 2.03, 95%CI 1.03–3.98, p = 0.04), which suggests other mechanisms may be responsible for worse response to surgical treatment in females with proximal disease [24].
There is a lack of data, whether sex affects BPA results. Therefore, we aimed at evaluation whether differences exist between men and women with CTEPH and to evaluate if outcomes of treatment with BPA differs regarding sex/gender. Women are known to be more susceptible to PH than men, and therefore usually among patients with CTEPH, but on the other hand women have also better survival [16,25,26]. In the case of CTEPH, the latest publication based on European registry indicated an equal ratio of affected women and men [16], similarly as US registry [27]. Registry developed by International CTEPH Association reported general dominance of women (52.4%), however in Europe they made up slightly less than half (48.7%) of patients with CTEPH [28]. (Figure 5 [14,19,27,28,29,30,31,32,33,34]).
European registry indicated that women had lower prevalence of some CV risk factors than men, such as previous acute coronary syndrome, smoking and COPD, but more often were obese, and had cancer or thyroid diseases history [16]. Women and men included in our study did not differ in terms of comorbidities, except for the occurrence of COPD that was much less frequently diagnosed in women.
As the CTEPH is strongly associated with the occurrence of pulmonary embolism and an incomplete thrombus resolution [35], sex/gender differences related to coagulation should be also considered. Typical thrombogenic factors were not proved to increase in patients with CTEPH in contrast to plasma factor VIII [36,37]. This factor physiologically has higher values in women than in men [38], what may predispose women to developing CTEPH. In the Japanese BPA Registry females represented 80% of included patients, and previous episodes of acute pulmonary embolism and deep vein thrombosis were not frequent (15,3% and 43,7% respectively) [19], as compared with reports from other Western countries (74.8% and 58.1%, respectively, in a European registry) [39].
Assessing patients’ status at baseline, we found that woman tended to have worse hemodynamics values than men, as indicated by higher sPAP and PVR and by lower SV. Creatinine levels were slightly higher in men, but this may probably result from physiologically higher muscle mass in men. In turn, clinical presentation in women and men was quite similar – there were no significant differences between sex/gender in results of Dyspnea Borg Scale and also in the distance walked during 6-MWT. Our population also did not differ in terms of WHO FC and most patients were diagnosed with WHO FC class 3. This observation is consistent with results described in other studies [26,28,40] and also with observations from European CTEPH registry [16], indicating that women slightly more often have functional capacity class III/IV diagnosed than men. More severe courses of the disease in women than men with CTEPH was also reported by Wu et al. [41].
More severe baseline hemodynamic parameters in women compared with men together with similar clinical symptomatology suggest that at diagnosis women are better adapted to the disease than men. On the other hand, it may be hypothesized that women will require more BPA sessions to achieve similar improvements in hemodynamics as men.
As there are no detailly defined therapeutic targets of BPA treatment in patients with CTEPH, usually achieving a good functional class (WHO-FC I–II) and/or improvement of hemodynamic parameters, as well as improvement in patients’ quality of life [8]. However, some recent data from ESC Working Group Statement defined BPA treatment goal to achieve final mPAP < 30 mmHg [42]. Comparing the effects of BPA from two multicenter registries (Japanese and Polish) and from single expert-centers (German and French) it was demonstrated that only Japanese were able to reach defined BPA treatment goal of mPAP below 30 mmHg [43]. This may be due to the intrinsic differences between European and Japanese patients, with European CTEPH patients having higher serum concentrations of C-reactive protein, fibrinogen and myeloperoxidase, and more red thrombus than Japanese CTEPH patients [44]. However, high-volume women representation in Japanese registry may be also suggestive for gender-related outcome in BPA treatment.
Control tests performed in the studied population after completion of BPA treatment revealed better hemodynamic status (especially regarding mSAP, sPAP, PCWP and CI) in women than in men, although at baseline the situation was opposite. Detailed analysis demonstrated that after treatment many parameters changed more in women than in men with decreases in mPAP and PVR being the most pronounced. These were reflected particularly in outcomes of Dyspnea Borg Scale – compared with baseline at follow-up in about 30% of women ratings shifted towards point 0-2 and such improvement was observed only by about 5% of men. Results of 6-MWT this difference did not achieve statistical significance.
Our results are even more interesting considering that there were no differences in number of the sessions, number of the treated vessels or the required amount of contrast and radiation between men and women. This may suggest that women respond better to CTEPH treatment with BPA than men.
The above observation seems to stay in line with the previously reported better long-term survival in women compared with men. This phenomenon is suggested to be related to better function of right ventricular in females than in males [45,46]. Unfortunately, echocardiographic data were unavailable in our study, hence we were unable to assess right ventricular functions in our population. However, that hemodynamic differences exist between different types of CTEPH with a worse condition in central than in peripheral form of disease [47]. Besides, in some studies, women tended to deteriorate more than males during follow-up [48].
Strengths and Limitations of the Study
To our knowledge this is the first very detailed study analyzing the impact of patients’ sex/gender on results of BPA therapy in patients with CTEPH. As it was a retrospective (single center, small group) study, we were able to provide valuable data from real clinical practice. However, some assessments are missing which is an inherent limitation to this type of research.
5. Conclusions
Although many studies demonstrated that BPA improves both hemodynamic parameters and clinical status of patients with CTEPH [49,50], sex/gender-specific treatment results are unknown. Also, current guidelines do not promote any sex/gender-specific approach, which implies that the diagnostic-therapeutic process is the same in women and men. Therefore, our data may be used to initiate further studies analyzing different scenarios of clinical management depending on sex/gender. We observed that at diagnosis women had more severe hemodynamic parameters than men that were accompanied by similar clinical symptomatology in both sexes. Despite this, women hemodynamic status was better after BPA therapy. The above outcomes may suggest that at diagnosis women are better adapted to the disease than men, and also women respond better to the BPA treatment. However, we are aware that these data are just preliminary and research evidence from the randomized controlled trials is needed to demonstrate whether the management of a patient with CTEPH should be sex – differentiated.
Author Contributions
Conceptualization, M.K., A.T. and S.D.; methodology, S.D; validation, M.K. and M.F.; formal analysis, Paweł Kurzyna; investigation, Paweł Kurzyna and A.W; data curation, Paweł Kurzyna; writing—original draft preparation, A.W. and Paweł Kurzyna; writing—review and editing, M.K, A.T, S.D., Piotr Kędzierski, P.S., M.P., M.B., A.G-vdP and A.P.; visualization, Paweł Kurzyna, A. W.; supervision, M.K and S.D.; project administration, Paweł Kurzyna; S.D.; funding acquisition, M.K. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by funds from the statutory activity of the Centre of Postgraduate Medical Education in Warsaw, Poland (grant number 501-1-054-25-25).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee (L.dz.OIL/KBL/27/2018).
Informed Consent Statement
Patient consent was waived due to retrospective character of the study.
Acknowledgments
The authors would like to thank Proper Medical Writing Sp. z o. o. for their support in the preparation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BPA | Ballon pulmonary angioplasty |
| CTEPH | Chronic thrombo-embolic pulmonary hypertension |
| CVD | Cardiovascular diseases |
| RHC | Right heart catherization |
| PEA | pulmonary endarterectomy |
| 6-MWT | 6-minute walking test |
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| M | Male |
| F | Female |
| BMI | Body mass index |
| DOAC | Direct oral anticoagulants |
| PH | Pulmonary hypertension |
| SD | Standard deviation |
| VKA | Vitamin K antagonists |
| LMWH | Low molecular weight heparin |
| WHO FC | World Health Organization functional class |
| mRAP | mean right atrial pressure |
| sPAP | systolic pulmonary arterial pressure |
| dPAP | diastolic pulmonary arterial pressure |
| mPAP | mean pulmonary artery pressure |
| PCWP | pulmonary capillary wedge pressure |
| CI | cardiac index |
| SV | stroke volume |
| SVI | stroke volume index |
| PVR | pulmonary vascular resistance |
| IQR | Interquartile range |
| COPD | Chronic obstructive pulmonary disease |
References
- Mensah, G.A.; Fuster, V. Sex and Gender Differences in Cardiovascular Health. J. Am. Coll. Cardiol. 2022, 79, 1385–1387. [Google Scholar] [CrossRef]
- Ghofrani, H.-A.; Galiè, N.; Grimminger, F.; Grünig, E.; Humbert, M.; Jing, Z.-C.; Keogh, A.M.; Langleben, D.; Kilama, M.O.; Fritsch, A.; et al. Riociguat for the Treatment of Pulmonary Arterial Hypertension. N. Engl. J. Med. 2013, 369, 330–340. [Google Scholar] [CrossRef]
- Fritz, J.S.; Blair, C.; Oudiz, R.J.; Dufton, C.; Olschewski, H.; Despain, D.; Gillies, H.; Kawut, S.M. Baseline and Follow-up 6-Min Walk Distance and Brain Natriuretic Peptide Predict 2-Year Mortality in Pulmonary Arterial Hypertension. Chest 2013, 143, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; D’Armini, A.M.; Grimminger, F.; Grünig, E.; Hoeper, M.M.; Jansa, P.; Mayer, E.; Neurohr, C.; Simonneau, G.; Torbicki, A.; et al. Haemodynamic Effects of Riociguat in Inoperable/Recurrent Chronic Thromboembolic Pulmonary Hypertension. Heart 2017, 103, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Nathan, S.D.; Behr, J.; Collard, H.R.; Cottin, V.; Hoeper, M.M.; Martinez, F.J.; Corte, T.J.; Keogh, A.M.; Leuchte, H.; Mogulkoc, N.; et al. Riociguat for Idiopathic Interstitial Pneumonia-Associated Pulmonary Hypertension (RISE-IIP): A Randomised, Placebo-Controlled Phase 2b Study. Lancet Respir. Med. 2019, 7, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Pugh, M.E.; Hemnes, A.R. Pulmonary Hypertension in Women. Expert Rev. Cardiovasc. Ther. 2010, 8, 1549–1558. [Google Scholar] [CrossRef]
- Mair, K.M.; Johansen, A.K.Z.; Wright, A.F.; Wallace, E.; Maclean, M.R. Pulmonary Arterial Hypertension: Basis of Sex Differences in Incidence and Treatment Response. Br. J. Pharmacol. 2014, 171, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Leber, L.; Beaudet, A.; Muller, A. Epidemiology of Pulmonary Arterial Hypertension and Chronic Thromboembolic Pulmonary Hypertension: Identification of the Most Accurate Estimates from a Systematic Literature Review. Pulm. Circ. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Delcroix, M.; Torbicki, A.; Gopalan, D.; Sitbon, O.; Klok, F.A.; Lang, I.; Jenkins, D.; Kim, N.H.; Humbert, M.; Jais, X.; et al. ERS Statement on Chronic Thromboembolic Pulmonary Hypertension. Eur. Respir. J. 2021, 57. [Google Scholar] [CrossRef]
- Kramm, T.; Wilkens, H.; Fuge, J.; Schäfers, H.J.; Guth, S.; Wiedenroth, C.B.; Weingard, B.; Huscher, D.; Pittrow, D.; Cebotari, S.; et al. Incidence and Characteristics of Chronic Thromboembolic Pulmonary Hypertension in Germany. Clin. Res. Cardiol. 2018, 107, 548–553. [Google Scholar] [CrossRef]
- Lang, I.M.; Andreassen, A.K.; Andersen, A.; Bouvaist, H.; Coghlan, G.; Escribano-Subias, P.; Jansa, P.; Kopec, G.; Kurzyna, M.; Matsubara, H.; et al. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: A Clinical Consensus Statement of the ESC Working Group on Pulmonary Circulation and Right Ventricular Function. Eur. Heart J. 2023, 44, 2659–2671. [Google Scholar] [CrossRef]
- Araszkiewicz, A.; Darocha, S.; Pietrasik, A.; Pietura, R.; Jankiewicz, S.; Banaszkiewicz, M.; Sławek-Szmyt, S.; Biederman, A.; Mularek-Kubzdela, T.; Lesiak, M.; et al. Balloon Pulmonary Angioplasty for the Treatment of Residual or Recurrent Pulmonary Hypertension after Pulmonary Endarterectomy. Int. J. Cardiol. 2019, 278, 232–237. [Google Scholar] [CrossRef]
- Darocha, S.; Pietura, R.; Pietrasik, A.; Norwa, J.; Dobosiewicz, A.; Piłka, M.; Florczyk, M.; Biederman, A.; Torbicki, A.; Kurzyna, M. Improvement in Quality of Life and Hemodynamics in Chronic Thromboembolic Pulmonary Hypertension Treated With Balloon Pulmonary Angioplasty. Circ. J. 2017, 81, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Martinez, C.; Wallenhorst, C.; Teal, S.; Cohen, A.T.; Peacock, A.J. Incidence and Risk Factors of Chronic Thromboembolic Pulmonary Hypertension Following Venous Thromboembolism, a Population-Based Cohort Study in England. Pulm. Circ. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Barco, S.; Klok, F.A.; Konstantinides, S.V.; Dartevelle, P.; Fadel, E.; Jenkins, D.; Kim, N.H.; Madani, M.; Matsubara, H.; Mayer, E.; et al. Sex-Specific Differences in Chronic Thromboembolic Pulmonary Hypertension. Results from the European CTEPH Registry. J. Thromb. Haemost. 2020, 18, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Kurzyna, M.; Araszkiewicz, A.; Błaszczak, P.; Grabka, M.; Hawranek, M.; Kopec, G.; Mroczek, E.; Zembala, M.; Torbicki, A.; Ochała, A. Summary of Recommendations for the Haemodynamic and Angiographic Assessment of the Pulmonary Circulation. Joint Statement of the Polish Cardiac Society’s Working Group on Pulmonary Circulation and Association of Cardiovascular Interventions. Pol. Heart J. (Kardiol. Pol.) 2015, 73, 63–68. [Google Scholar] [CrossRef]
- Siennicka, A.; Darocha, S.; Banaszkiewicz, M.; Kędzierski, P.; Dobosiewicz, A.; Błaszczak, P.; Peregud-Pogorzelska, M.; Kasprzak, J.D.; Tomaszewski, M.; Mroczek, E.; et al. Treatment of Chronic Thromboembolic Pulmonary Hypertension in a Multidisciplinary Team. Ther. Adv. Respir. Dis. 2019, 13. [Google Scholar] [CrossRef]
- Ogawa, A.; Satoh, T.; Fukuda, T.; Sugimura, K.; Fukumoto, Y.; Emoto, N.; Yamada, N.; Yao, A.; Ando, M.; Ogino, H.; et al. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: Results of a Multicenter Registry. Circ. Cardiovasc. Qual. Outcomes 2017, 10. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef]
- Mizoguchi, H.; Ogawa, A.; Munemasa, M.; Mikouchi, H.; Ito, H.; Matsubara, H. Refined Balloon Pulmonary Angioplasty for Inoperable Patients with Chronic Thromboembolic Pulmonary Hypertension. Circ. Cardiovasc. Interv. 2012, 5, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Medrek, S.; Safdar, Z. Epidemiology and Pathophysiology of Chronic Thromboembolic Pulmonary Hypertension: Risk Factors and Mechanisms. Methodist. Debakey Cardiovasc. J. 2016, 12, 195–198. [Google Scholar] [CrossRef]
- Bambrick, M.; Grafham, G.; Lajkosz, K.; Donahoe, L.; de Perrot, M.; McInnis, M. Computed Tomography Identifies Sex-Specific Differences in Surgical Chronic Thromboembolic Pulmonary Hypertension. JHLT Open 2024, 6, 100130. [Google Scholar] [CrossRef]
- Chan, J.C.Y.; Man, H.S.J.; Asghar, U.M.; McRae, K.; Zhao, Y.; Donahoe, L.L.; Wu, L.; Granton, J.; de Perrot, M. Impact of Sex on Outcome after Pulmonary Endarterectomy for Chronic Thromboembolic Pulmonary Hypertension. J. Heart Lung Transplant. 2023, 42, 1578–1586. [Google Scholar] [CrossRef]
- Martin, Y.N.; Pabelick, C.M. Sex Differences in the Pulmonary Circulation: Implications for Pulmonary Hypertension. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H1253. [Google Scholar] [CrossRef]
- Bonderman, D.; Wilkens, H.; Wakounig, S.; Schäfers, H.J.; Jansa, P.; Lindner, J.; Simkova, I.; Martischnig, A.M.; Dudczak, J.; Sadushi, R.; et al. Risk Factors for Chronic Thromboembolic Pulmonary Hypertension. Eur. Respir. J. 2009, 33, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Kerr, K.M.; Elliott, C.G.; Chin, K.; Benza, R.L.; Channick, R.N.; Davis, R.D.; He, F.; LaCroix, A.; Madani, M.M.; McLaughlin, V.V.; et al. Results From the United States Chronic Thromboembolic Pulmonary Hypertension Registry: Enrollment Characteristics and 1-Year Follow-Up. Chest 2021, 160, 1822–1831. [Google Scholar] [CrossRef]
- Guth, S.; D’armini, A.M.; Delcroix, M.; Nakayama, K.; Fadel, E.; Hoole, S.P.; Jenkins, D.P.; Kiely, D.G.; Kim, N.H.; Lang, I.M.; et al. Current Strategies for Managing Chronic Thromboembolic Pulmonary Hypertension: Results of the Worldwide Prospective CTEPH Registry. ERJ Open Res. 2021, 7. [Google Scholar] [CrossRef]
- Cannon, J.E.; Su, L.; Kiely, D.G.; Page, K.; Toshner, M.; Swietlik, E.; Treacy, C.; Ponnaberanam, A.; Condliffe, R.; Sheares, K.; et al. Dynamic Risk Stratification of Patient Long-Term Outcome After Pulmonary Endarterectomy: Results From the United Kingdom National Cohort. Circulation 2016, 133, 1761. [Google Scholar] [CrossRef]
- Chan, J.C.Y.; Man, H.S.J.; Asghar, U.M.; McRae, K.; Zhao, Y.; Donahoe, L.L.; Wu, L.; Granton, J.; de Perrot, M. Impact of Sex on Outcome after Pulmonary Endarterectomy for Chronic Thromboembolic Pulmonary Hypertension. J. Heart Lung Transplant. 2023, 42, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Olsson, K.M.; Wiedenroth, C.B.; Kamp, J.C.; Breithecker, A.; Fuge, J.; Krombach, G.A.; Haas, M.; Hamm, C.; Kramm, T.; Guth, S.; et al. Balloon Pulmonary Angioplasty for Inoperable Patients with Chronic Thromboembolic Pulmonary Hypertension: The Initial German Experience. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef]
- Brenot, P.; Jaïs, X.; Taniguchi, Y.; Alonso, C.G.; Gerardin, B.; Mussot, S.; Mercier, O.; Fabre, D.; Parent, F.; Jevnikar, M.; et al. French Experience of Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension. Eur. Respir. J. 2019, 53. [Google Scholar] [CrossRef] [PubMed]
- Masaki, K.; Hosokawa, K.; Funakoshi, K.; Taniguchi, Y.; Adachi, S.; Inami, T.; Yamashita, J.; Ogino, H.; Tsujino, I.; Hatano, M.; et al. Outcomes of Chronic Thromboembolic Pulmonary Hypertension After Balloon Pulmonary Angioplasty and Pulmonary Endarterectomy. JACC Asia 2024, 4, 577–589. [Google Scholar] [CrossRef]
- Kopeć, G.; Dzikowska-Diduch, O.; Mroczek, E.; Mularek-Kubzdela, T.; Chrzanowski, Ł.; Skoczylas, I.; Tomaszewski, M.; Peregud-Pogorzelska, M.; Karasek, D.; Lewicka, E.; et al. Characteristics and Outcomes of Patients with Chronic Thromboembolic Pulmonary Hypertension in the Era of Modern Therapeutic Approaches: Data from the Polish Multicenter Registry (BNP-PL). Ther. Adv. Chronic Dis. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.M.; Pesavento, R.; Bonderman, D.; Yuan, J.X.J. Risk Factors and Basic Mechanisms of Chronic Thromboembolic Pulmonary Hypertension: A Current Understanding. Eur. Respir. J. 2013, 41, 462–468. [Google Scholar] [CrossRef]
- Wolf, M.; Boyer-Neumann, C.; Parent, F.; Eschwege, V.; Jaillet, H.; Meyer, D.; Simonneau, G. Thrombotic Risk Factors in Pulmonary Hypertension. Eur. Respir. J. 2000, 15, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Bonderman, D.; Turecek, P.L.; Jakowitsch, J.; Weltermann, A.; Adlbrecht, C.; Schneider, B.; Kneussl, M.; Rubin, L.J.; Kyrle, P.A.; Klepetko, W.; et al. High Prevalence of Elevated Clotting Factor VIII in Chronic Thromboembolic Pulmonary Hypertension. Thromb. Haemost. 2003, 90, 372–376. [Google Scholar] [CrossRef]
- Kain, K.; Carter, A.M.; Bamford, J.M.; Grant, P.J.; Catto, A.J. Gender Differences in Coagulation and Fibrinolysis in White Subjects with Acute Ischemic Stroke. J. Thromb. Haemost. 2003, 1, 390–392. [Google Scholar] [CrossRef]
- Pepke-Zaba, J.; Delcroix, M.; Lang, I.; Mayer, E.; Jansa, P.; Ambroz, D.; Treacy, C.; D’Armini, A.M.; Morsolini, M.; Snijder, R.; et al. Chronic Thromboembolic Pulmonary Hypertension (CTEPH): Results from an International Prospective Registry. Circulation 2011, 124, 1973–1981. [Google Scholar] [CrossRef]
- Cruz-Utrilla, A.; Cristo-Ropero, M.J.; Calderón-Flores, M.; Velázquez, M.; López-Gude, M.J.; Ostolaza, Y.R.; Vela, J.L.P.; de la Cruz-Bertolo, J.; Bueno, H.; Ynsaurriaga, F.A.; et al. Sex Differences in Chronic Thromboembolic Pulmonary Hypertension. Treatment Options over Time in a National Referral Center. J. Clin. Med. 2021, 10. [Google Scholar] [CrossRef]
- Wu, Y.; Hu, S.; Yan, X.X.; Peng, F.H.; Tan, J.S.; Guo, T.T.; Gao, X.; Hua, L. Chronic Thromboembolic Pulmonary Hypertension in Females: Clinical Features and Survival. J. Cardiovasc. Dev. Dis. 2022, 9, 308. [Google Scholar] [CrossRef]
- Lang, I.M.; Andreassen, A.K.; Andersen, A.; Bouvaist, H.; Coghlan, G.; Escribano-Subias, P.; Jansa, P.; Kopec, G.; Kurzyna, M.; Matsubara, H.; et al. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: A Clinical Consensus Statement of the ESC Working Group on Pulmonary Circulation and Right Ventricular Function. Eur. Heart J. 2023, 44, 2659–2671. [Google Scholar] [CrossRef]
- Lang, I.M. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: Clinical Outcomes. Eur. Cardiol. Rev. 2023, 18. [Google Scholar] [CrossRef]
- Chausheva, S.; Naito, A.; Ogawa, A.; Seidl, V.; Winter, M.P.; Sharma, S.; Sadushi-Kolici, R.; Campean, I.A.; Taghavi, S.; Moser, B.; et al. Chronic Thromboembolic Pulmonary Hypertension in Austria and Japan. J. Thorac. Cardiovasc. Surg. 2019, 158, 604–614. [Google Scholar] [CrossRef] [PubMed]
- Keen, J.; Prisco, S.Z.; Prins, K.W. Sex Differences in Right Ventricular Dysfunction: Insights From the Bench to Bedside. Front. Physiol. 2021, 11. [Google Scholar] [CrossRef]
- Shigeta, A.; Tanabe, N.; Shimizu, H.; Hoshino, S.; Maruoka, M.; Sakao, S.; Tada, Y.; Kasahara, Y.; Takiguchi, Y.; Tatsumi, K.; et al. Gender Differences in Chronic Thromboembolic Pulmonary Hypertension in Japan. Circ. J. 2008, 72, 2069–2074. [Google Scholar] [CrossRef] [PubMed]
- Kaldararova, M.; Simkova, I.; Bohacekova, M.; Reptova, A.; Hlavata, T.; Pacak, J.; Lindner, J.; Jansa, P. Central versus Peripheral CTEPH-Clinical and Hemodynamic Specifications. Medicina 2022, 58. [Google Scholar] [CrossRef]
- Yang, Y.L.; Yu, Y.Z.; Yuan, P.; Gong, S.G.; Wang, C.Y.; Li, Y.; Zhao, Q.H.; Jiang, R.; Wu, W.H.; He, J.; et al. Sex Differences of Hemodynamics during Acute Vasoreactivity Testing to Predict the Outcomes of Chronic Thromboembolic Pulmonary Hypertension. Clin. Respir. J. 2020, 14, 611–621. [Google Scholar] [CrossRef]
- Zoppellaro, G.; Badawy, M.R.; Squizzato, A.; Denas, G.; Tarantini, G.; Pengo, V. Balloon Pulmonary Angioplasty in Patients With Chronic Thromboembolic Pulmonary Hypertension - A Systematic Review and Meta-Analysis. Circ. J. 2019, 83, 1660–1667. [Google Scholar] [CrossRef]
- Kennedy, M.K.; Kennedy, S.A.; Tan, K.T.; de Perrot, M.; Bassett, P.; McInnis, M.C.; Thenganatt, J.; Donahoe, L.; Granton, J.; Mafeld, S. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: A Systematic Review and Meta-Analysis. Cardiovasc. Interv. Radiol. 2023, 46, 5–18. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow chart of patient selection to the study. BPA – ballon pulmonary angioplasty; CTEPH – chronic thromboembolic pulmonary hypertension; F – female, M – male.
Figure 1.
Flow chart of patient selection to the study. BPA – ballon pulmonary angioplasty; CTEPH – chronic thromboembolic pulmonary hypertension; F – female, M – male.
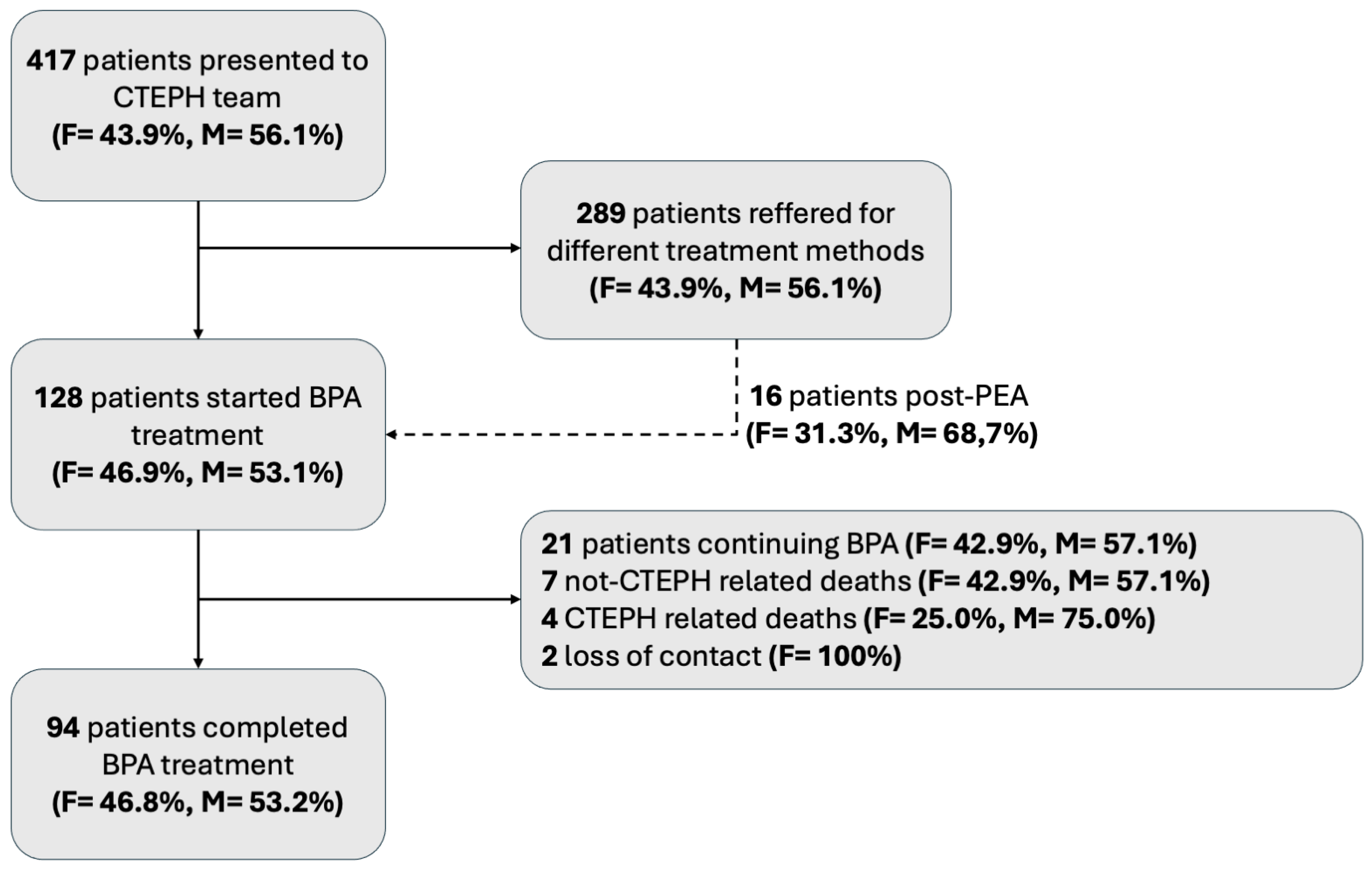
Figure 2.
Comparison of changes in WHO FC in women and men from baseline to follow-up. WHO FC – World Health Organization functional class.
Figure 2.
Comparison of changes in WHO FC in women and men from baseline to follow-up. WHO FC – World Health Organization functional class.
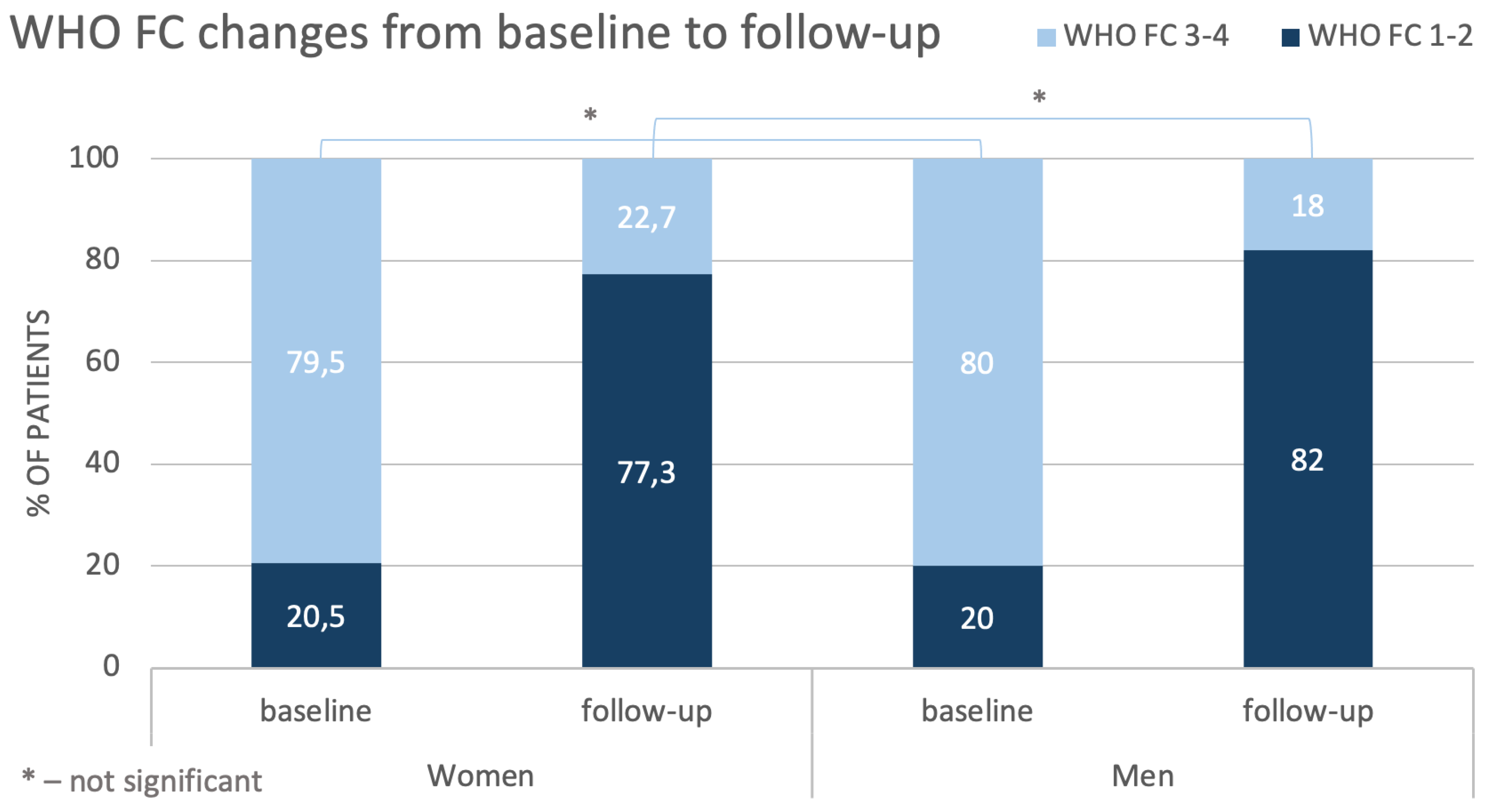
Figure 3.
Comparison of changes in outcomes of Dyspnea Borg Scale in women and men from baseline to follow-up.
Figure 3.
Comparison of changes in outcomes of Dyspnea Borg Scale in women and men from baseline to follow-up.
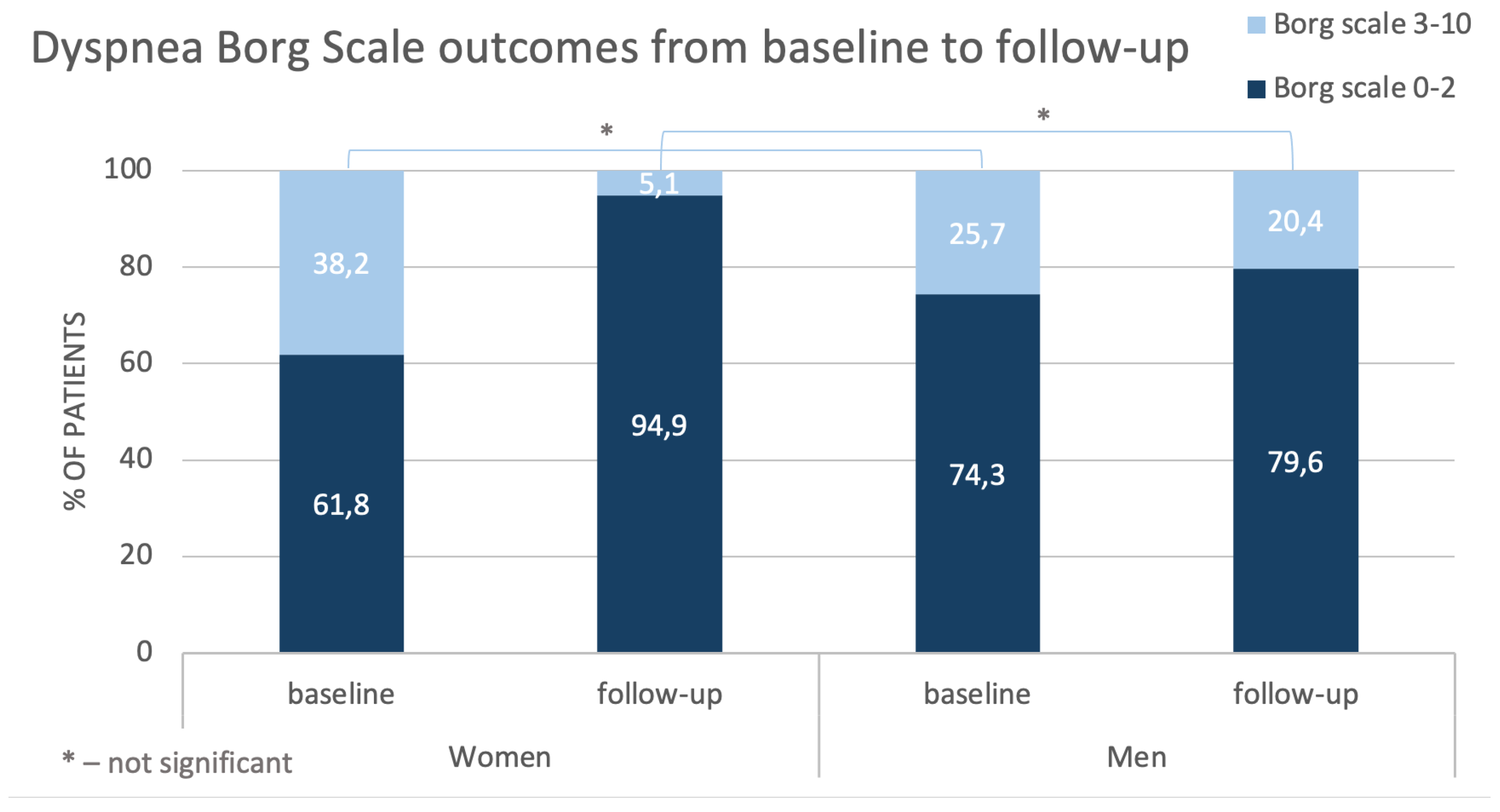
Figure 4.
Changes in values of hemodynamic variable during treatment (from baseline to follow-up). CI – cardiac index; CO – cardiac output; mPAP – mean pulmonary artery pressure; mRAP – mean right atrial pressure; PVR – pulmonary vascular resistance.
Figure 4.
Changes in values of hemodynamic variable during treatment (from baseline to follow-up). CI – cardiac index; CO – cardiac output; mPAP – mean pulmonary artery pressure; mRAP – mean right atrial pressure; PVR – pulmonary vascular resistance.
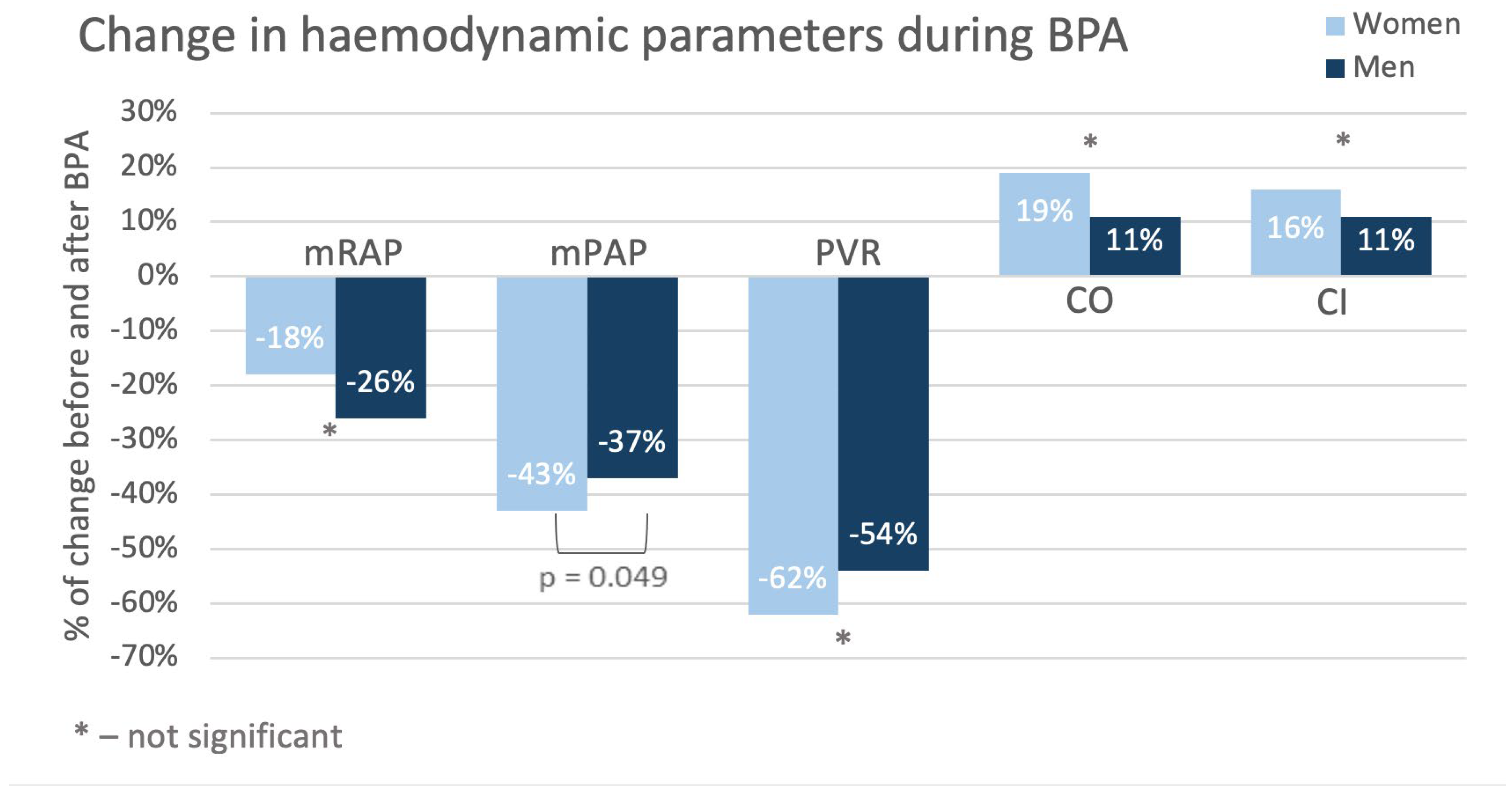
Figure 5.
Percentage of women represented in CTEPH studies [14,19,27,28,29,30,31,32,33,34]. BPA – ballon pulmonary angioplasty; CTEPH – chronic thromboembolic pulmonary hypertension; PEA – pulmonary endarterectomy.
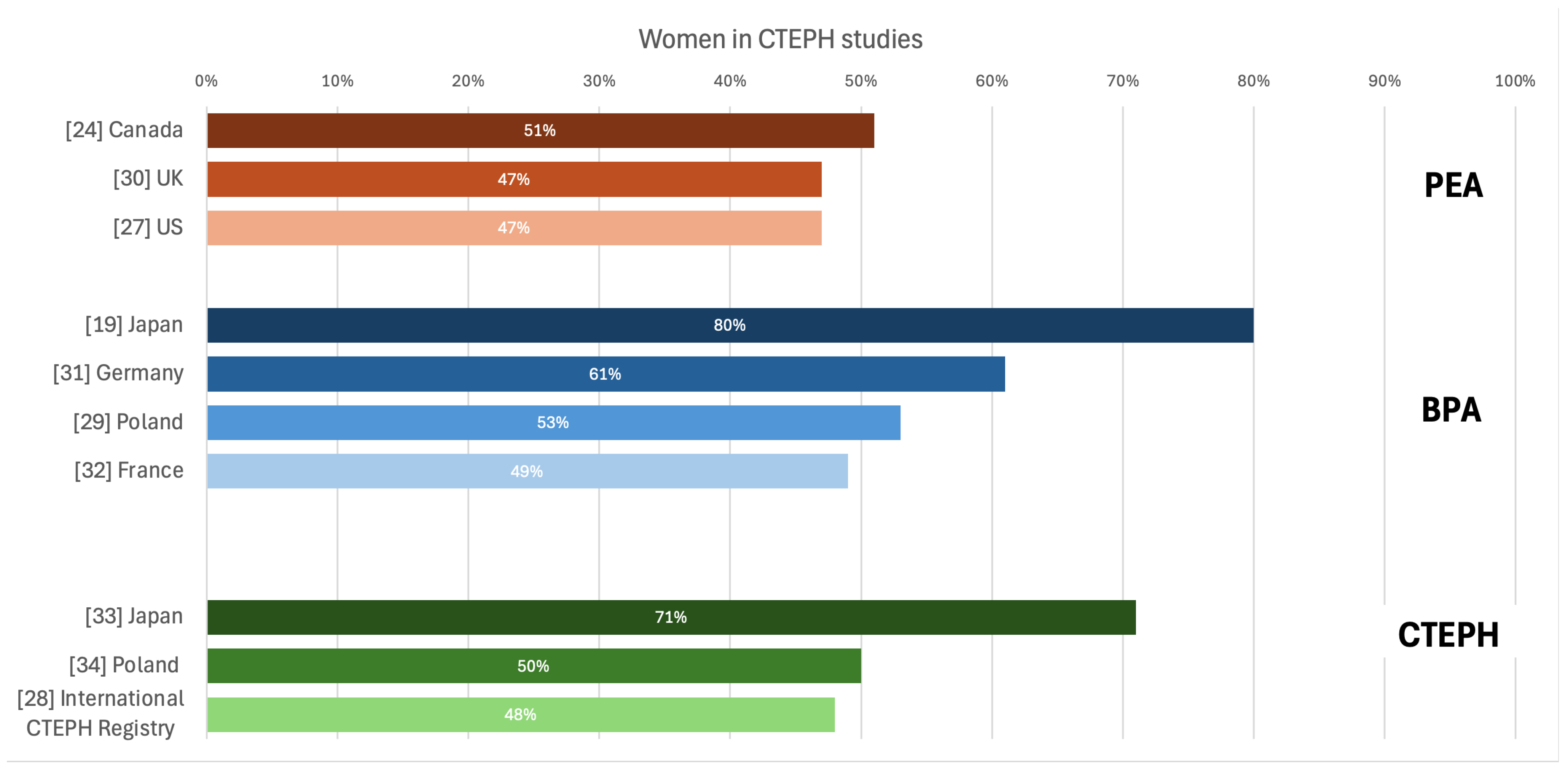
Table 1.
Characteristics of patients at baseline.
| Variable | Female (n=44) | Male (n=50) | p-value | |
|---|---|---|---|---|
| Age, years | 54 [47-70] | 66 [54-73] | 0.07 | |
| Anthropometric measures | Weight, kg | 67 [61-74] | 81 [74-93] | <0.001 |
| Height, cm | 162 (7.8) | 175 (7.4) | <0.001 | |
| BSA, m2 | 1.73 (0.18) | 1.98 (0.17) | <0.001 | |
| BMI, kg/m2 | 25.6 [23.3-28.4] | 26.8 [24.5-29.9] | 0.19 | |
| Comorbidities | Previous venous thrombosis, % | 19 (43.2) | 26 (52.0) | 0.42 |
| Previous acute pulmonary embolism, % | 37 (84.1) | 36 (72.0) | 0.22 | |
| Hypertension, % | 19 (43.2) | 28 (56.0) | 0.30 | |
| Diabetes, % | 2 (4.6) | 7 (14.0) | 0.23 | |
| Coronary artery disease, % | 9 (20.5) | 14 (28.0) | 0.47 | |
| Hyperlipidemia, % | 13 (29.6) | 19 (38.0) | 0.51 | |
| Chronic obstructive pulmonary disease, % | 0 (0.0) | 13 (26.0) | <0.001 | |
| Chronic kidney disease, % | 8 (18.2) | 10 (20.0) | 1.00 | |
| Atrial fibrillation, % | 4 (9.1) | 12 (24.0) | 0.10 | |
| Inferior vena cava filter, % | 6 (13.6) | 5 (10.0) | 0.75 | |
| Anticoagulant treatment | VKA, % | 12 (27.3) | 14 (28.0) | 0.75 |
| LMWH, % | 7 (15.9) | 9 (18.0) | ||
| DOAC, % | 24 (54.6) | 27 (54.0) | ||
| PH specific therapy | Sildenafil or riociguat, % | 36 (81.8) | 39 (78.0) | 0.71 |
| Oxygen therapy, % | 8 (18.2) | 7 (14.0) | 0.58 | |
| Reasons for rejection from PEA | Distal pulmonary vascular obstruction, % | 28 (63.6) | 26 (52.0) | 0.33 |
| Comorbidities, % | 6 (13.6) | 10 (20.0) | ||
| Lack of patient consent, % | 5 (11.4) | 3 (6.0) | ||
| Post-PEA CTEPH, % | 5 (11.4) | 11 (22.0) | ||
Data are presented as n (%), median [interquartile range] or mean (SD). BMI – body mass index; BSA – body surface area; DOAC – direct oral anticoagulants; PEA – pulmonary endarterectomy; PH – pulmonary hypertension; LMWH – low molecular weight heparin; SD – standard deviation; VKA – vitamin K antagonists.
Table 2.
Patients’ clinical status at baseline.
| Variable | Female (n=44) | Male (n=50) | p-value | |
|---|---|---|---|---|
| Heart rate, bpm | 77 [66-92] | 72 [65-78] | 0.09 | |
| WHO FC, n (%) | 1 | 0 | 0 | 0.69 |
| 2 | 9 (20.5) | 10 (20.0) | ||
| 3 | 32 (72.7) | 34 (68.0) | ||
| 4 | 3 (6.8) | 6 (12.0) | ||
| 6-MWT, m | 341 (135.8) | 366 (135.3) | 0.43 | |
| Borg Dyspnea Scale, points (%) | 0 | 17 (50.0) | 22 (62.9) | 0.89 |
| 1 | 0 | 0 | ||
| 2 | 4 (11.8) | 4 (11.4) | ||
| 3 | 5 (14.7) | 3 (8.6) | ||
| 4 | 2 (5.9) | 1 (2.9) | ||
| 5 | 3 (8.8) | 3 (8.6) | ||
| 6 | 0 | 0 | ||
| 7 | 0 | 0 | ||
| 8 | 3 (8.8) | 2 (5.7) | ||
| 9 | 0 | 0 | ||
| 10 | 0 | 0 | ||
| Laboratory tests | NT-proBNP, pg/mL | 1195 [412-1970] | 1367 [652-2533] | 0.71 |
| Troponin T, ng/mL | 0.011 [0.006-0.021] | 0.015 [0.009-0.026] | 0.07 | |
| Creatinine, mg/dL | 0.86 [0.80-0.98] | 1.13 [0.99-1.30] | <0.001 | |
Data are presented as n (%), median [interquartile range] or mean (SD). 6-MWT – 6-minute walking test; NT-proBNP – N-terminal pro-B-type natriuretic peptide; SD – standard deviation; WHO FC – World Health Organization functional class.
Table 3.
Patients’ hemodynamic status at baseline.
| Variable | Female (n=44) | Male (n=50) | p-value |
|---|---|---|---|
| mRAP, mmHg | 7 [5-10] | 9 [5-12] | 0.31 |
| sPAP, mmHg | 85 (17.6) | 76 (18.5) | 0.03 |
| dPAP, mmHg | 29 (7.9) | 28 (8.1) | 0.56 |
| mPAP, mmHg | 49 (10.7) | 45 (10.5) | 0.08 |
| PCWP, mmHg | 9 [6-12] | 10 [9-12] | 0.30 |
| CI, L/min/m2 | 2.24 [1.81-2.80] | 2.24 [1.92-2.50] | 0.70 |
| SV, mL/beat | 54 (17.2) | 64 (17.5) | 0.01 |
| SVI, mL/beat/m2 | 31.59 (9.9) | 31.91 (7.9) | 0.86 |
| PVR, Wood Units | 9.89 [6.31-14.06] | 8.21 [5.55-10.17] | 0.03 |
Data are presented as median [interquartile range] or mean (SD). CI – cardiac index; dPAP – diastolic pulmonary arterial pressure; mPAP – mean pulmonary artery pressure; mRAP – mean right atrial pressure; PCWP – pulmonary capillary wedge pressure; PVR – pulmonary vascular resistance; SD – standard deviation; sPAP – systolic pulmonary arterial pressure; SV – stroke volume; SVI – stroke volume index.
Table 4.
Patients’ clinical outcomes at follow-up.
| Variable | Female (n=44) | Male (n=50) | p-value | |
|---|---|---|---|---|
| Heart rate, bpm | 68 [61-78] | 67 [59-78] | 0.53 | |
| WHO FC, n (%) | 1 | 14 (31.8) | 13 (26.0) | 0.59 |
| 2 | 20 (45.5) | 28 (56.0) | ||
| 3 | 10 (22.7) | 9 (18.0) | ||
| 4 | 0 | 0 | ||
| 6-MWT, m | 428 (134) | 444 (134) | 0.57 | |
| 6-MWT, Δm | +93 (96.6) | +76 (108) | 0.47 | |
| Borg Dyspnea Scale, points (%) | 0 | 34 (87.2) | 35 (79.6) | 0.03 |
| 1 | 0 | 0 | ||
| 2 | 3 (7.7) | 0 | ||
| 3 | 0 | 2 (4.5) | ||
| 4 | 0 | 1 (2.6) | ||
| 5 | 0 | 4 (10.5) | ||
| 6 | 0 | 1 (2.6) | ||
| 7 | 2 (5.1) | 0 | ||
| 8 | 0 | 0 | ||
| 9 | 0 | 0 | ||
| 10 | 0 | 0 | ||
| Laboratory tests | NT-proBNP, pg/mL | 152 [87-376] | 223 [73-743] | 0.60 |
| Troponin T, ng/L | 0.007 [0.004-0.012] | 0.014 [0.009-0.022] | <0.001 | |
| Creatinin, mg/dL | 0.79 [0.72-0.90] | 1.05 [0.96-1.20] | <0.001 | |
Data are presented as n (%), median [interquartile range] and mean (SD). 6-MWT – 6-minute walking test; NT-proBNP – N-terminal pro-B-type natriuretic peptide; WHO FC – World Health Organization functional class.
Table 5.
Patients’ hemodynamic outcomes at follow-up and changes in some variables from baseline to follow-up.
Table 5.
Patients’ hemodynamic outcomes at follow-up and changes in some variables from baseline to follow-up.
| Variable | Female (n=44) | Male (n=50) | p-value | |
|---|---|---|---|---|
| mRAP, mmHg | 5 [4-7] | 6 [3-7] | 0.77 | |
| sPAP, mmHg | 43 [37-49] | 49 [41-54] | 0.04 | |
| dPAP, mmHg | 15 [12-18] | 17 [13-22] | 0.05 | |
| mPAP, mmHg | 26 [22-30] | 29 [23-33] | 0.11 | |
| Δnominal | -20.9 [±12.2] | -15.8 [±10.8] | 0.04 | |
| Δ% | -43% [-57 – 25] | -37% [-47 – -18] | 0.049 | |
| PCWP, mmHg | 9 [8-11] | 10 [9-14] | 0.03 | |
| CI, L/min/m2 | 2.82 (0.50) | 2.57 (0.53) | 0.03 | |
| Δnominal | +0.40 [±0.77] | +0.30 [±0.50] | 0.42 | |
| Δ% | +16% [-1 – 51] | +11% [-5 – 32] | 0.34 | |
| SV, mL/beat | 70.87 (14.37) | 76.62 (20.02) | 0.12 | |
| SVI, mL/beat/m2 | 40.77 (7.61) | 38.33 (9.21) | 0.17 | |
| PVR, Wood Units | 3.34 [2.63-3.87] | 3.08 [2.58-4.49] | 0.65 | |
| Δnominal | -6.64 [-10.28 – -2.85] | -3.85 [-6.48 – -1.77] | 0.048 | |
| Δ% | -62% [-79 – -42] | -54% [-69 – -36] | 0.12 | |
Data are presented as median [interquartile range] or mean (SD). CI – cardiac index; dPAP – diastolic pulmonary arterial pressure; mPAP – mean pulmonary artery pressure; mRAP – mean right atrial pressure; PCWP – pulmonary capillary wedge pressure; PVR – pulmonary vascular resistance; SD – standard deviation; sPAP – systolic pulmonary arterial pressure; SV – stroke volume; SVI – stroke volume index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



