
Submitted:
19 December 2024
Posted:
20 December 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Since the initial identification of SARS-CoV-2 infections, numerous clinical challenges have arisen, revealing both acute and long-term effects associated with COVID-19. These effects impact various systems within the body, including the respiratory, cardiovascular, and nervous systems. Background/Objectives: This study aimed to investigate the immunological and inflammatory parameters in patients with severe COVID-19 and evaluate the effects of hyperbaric oxygen therapy (HBOT) on these parameters. Methods: This study enrolled thirty patients from the Military Medical Institute - National Research Institute in Warsaw, who were hospitalized for SARS-CoV-2 infection . Patients were screened for eligibility based on pre-defined inclusion criteria. The subjects were divided into two groups: hyperbaric oxygen therapy (HBOT) and a control group. Immune profiling was performed, measuring cytokine concentrations and leukocyte subpopulations in serum samples. Outcomes were assessed using Bayesian modeling. Results: Bayesian regression analysis confirmed previous findings, indicating that HBOT may reduce inflammatory cytokine levels while improving oxygen saturation (SpO2) in patients with moderate and severe COVID-19. Moreover, the analysis suggested a higher probability of HBOT success in modulating the immune response and reducing inflammatory parameters, particularly in T lymphocyte subpopulations. Conclusions: Hyperbaric oxygen therapy (HBOT) may serve as an effective adjunctive treatment for patients with COVID-19 by enhancing oxygen saturation and modulating the immune response. Further studies are needed to elucidate the underlying mechanisms of HBOT on inflammatory and immunological parameters in COVID-19 patients.
Keywords:
HBOT
; COVID-19
; immune response
1. Introduction
As of early May 2020, there have been more than 770 million confirmed cases of SARS-CoV-2 infection worldwide, resulting in approximately 7 million deaths [1]. Despite the current lack of significant threat posed by the novel coronavirus disease (COVID-19), the emergence of new cases and fatalities due to infection with the recently identified Pango lineages [2] underscores the necessity for continued vigilance.
Since the initial identification of cases of SARS-CoV-2 infection, numerous clinical challenges have been encountered, both in the context of ongoing infection and in the subsequent acute and long-term effects [3, 4]. These effects encompass a range of systems, including the respiratory, cardiovascular, and nervous systems, as well as cognitive processes [5,6,7].
The SARS-CoV-2 virus gains entry into lung alveolar cells via the angiotensin-converting enzyme 2 (ACE2) receptor, thereby exerting a negative regulatory effect on vasoconstriction, cell proliferation, and inflammation [8]. Consequently, the most prominent respiratory symptoms are observed in patients who have developed symptoms. These primarily include cough, shortness of breath, and pneumonia with acute respiratory distress syndrome (ARDS). Therefore, the first-line treatment for patients with respiratory failure due to SARS-CoV-2 is the administration of oxygen via a high-flow nasal cannula for patients with COVID-19 respiratory failure is the use of oxygen via a high-flow nasal cannula [9].
At the immunological level, studies have described excessive activation of immune cells and blood clotting in patients, accompanied by tissue inflammation [10, 11]. A number of studies have demonstrated that patients with moderate to severe cases of coronavirus disease 2019 (Covid-19) exhibited an impaired T-cell response and an imbalance of major T helper lymphocyte (Th) subpopulations [12,13,14,15].
In severe cases, this could result in an imbalance of the immune system. The excessive and uncontrolled production of pro- and anti-inflammatory cytokines has been identified as a key factor contributing to both a worse prognosis of SARS-CoV-2 infection and acute respiratory distress syndrome [17, 18]. This includes a significant role in the excessive production of early pro-inflammatory cytokines, including TNF-α, IL-6, IL-1β, and IFN-γ [18]. The precise relationship between cytokine levels and the course of infection remains unclear.
Nevertheless, in the acute phase of infection, the key roles are played by interferon gamma (IFN-γ), interleukin 1 alpha (IL-1α), interleukin 7 (IL-7), interleukin 9 (IL-9), interleukin 10 (IL-10), granulocyte colony-stimulating factor (G-CSF), fibroblast growth factor (FGF), granulocyte-macrophage colony-stimulating factor (GM-CSF), tumor necrosis factor alpha (TNF-α), and vascular endothelial growth factor (VEGF). Additionally, chemokines CXCL-8 (IL-8), CXCL-10 (IP-10), CCL-2 (MCP-1), CCL-3 (M1α), and CCL-4 (MIP-1β) were identified in a previous study [19]. The elevated levels of IL-1β, IFN-γ, MCP1, and IP10 observed in patients with severe SARS-CoV-2 infection may stimulate the activation of Th1 lymphocytes, thereby triggering a cascade of cytokines and exacerbating the inflammatory response [20]. In a separate study, elevated levels of pro-inflammatory cytokines, including IL-6, IL-8, IL-2R, and TNF-α, and anti-inflammatory IL-10, were observed in the serum of patients with severe disease progression [21].
The precise mechanism by which a cytokine storm is triggered in severe cases of coronavirus disease 2019 (Covid-19) remains unclear. The data indicate that a reduction in the number of lymphocytes, particularly Tc cells, which function by eliminating infected cells [22], in conjunction with neutrophils that mediate the cytokine storm [23], may be a pivotal factor in the pathogenesis of SARS-CoV-2 infection. Recent reports of pathological findings in autopsied patients with confirmed diagnosis of SARS-CoV-2 infection have noted the presence of neutrophil infiltration in affected tissues [24, 25]. Similarly, it has been reported that an increase in neutrophils and reactive oxygen species is observed in patients with severe SARS-CoV-2 infection [26]. The production of excessive reactive oxygen species (ROS) by neutrophils can result in the propagation of local inflammation, ultimately leading to its systemic dissemination [27]. The clinical efficacy of hyperbaric oxygen (HBO) therapy has been demonstrated in the reversal of local hypoxia and subsequent reduction of inflammatory processes [28, 29, 30]. Additionally, an increase in reactive oxygen species (ROS) production has been observed during HBOT-induced hyperoxia [31]. Nevertheless, the findings indicate that participation in multiple HBOT sessions diminishes the capacity of neutrophils to generate ROS, while not elevating plasma cytokine concentrations [32, 33]. Furthermore, the temporary increase in ROS levels resulting from HBOT has led to its successful application in the treatment of acute and chronic wounds, diabetic foot ulcers, and infectious diseases [34,35,36,37,38]. In recent years, there has been a notable increase in the number of clinical studies that have provided evidence supporting the efficacy of hyperbaric oxygen therapy (HBOT) in modifying the immune system, particularly in the context of soft tissue infections (NSTIs) and non-specific intestinal inflammations. Furthermore, there is evidence that hyperbaric oxygen therapy is effective in the treatment of nonspecific intestinal inflammations [39] (pp. 55–65) and in bowel disease [40]. Some studies have proposed hyperbaric oxygen therapy (HBOT) as an effective method of reversing acute complications and treating patients with long-term COVID-19 symptoms [5, 6]. From the outset of the SARS-CoV-2 pandemic, there has been a focus on the efficacy of hyperbaric oxygen therapy (HBOT) in improving oxygen saturation in patients with coronavirus disease 2019 [41]. Nevertheless, the application of HBOT for the sole purpose of transient improvement in patient oxygenation is not advised [42].
In addition, there are an increasing number of scientific reports proving the efficacy of HBOT in improving saturation in COVID-19 patients, with a clinical trial protocol published in 2022 to evaluate the safety and efficacy of HBOT in patients with COVID-19 [43]. The study proved an increase in SpO2 in COVID-19 patients with severe hypoxemia, without significant adverse effects. These results are consistent with a study we published previously [44], despite the objective of our report being a reduction in mortality, the statistical reduction in mortality was not significant. A growing number of studies are demonstrating the benefits of HBOT, both in patients with active infection and long-term COVID-19 [45,46,47,48]. Considering the mounting evidence attesting to the efficacy of hyperbaric oxygen therapy (HBOT) in treating patients with the novel coronavirus disease (2019-nCoV), this study broadens the analysis of immunological and inflammatory parameters. It also implements Bayesian modeling to evaluate different scenarios and compounds on which HBOT exerts a significant influence, with a high probability of success. The objective was to evaluate the probability of a reduction in inflammatory cytokine parameters, particularly the proportion of T lymphocyte subpopulations and the concentrations of pro- and anti-inflammatory cytokines.
2. Materials and Methods
The following sections are the same as presented in our previous publication [44].
2.1. Patients
Thirty patients of the Military Medical Institute - National Research Institute in Warsaw, aged 24 to 78 years (6 women; mean age 55 ± 13.4 years), hospitalized for SARS-CoV-2 infection between March 1, 2021 and February 3, 2022, participated in the study [44].
Two patients were excluded due to not meeting the inclusion criteria 14 patients were assigned to the HBOT group, and 14 patients were placed in the control group. There were 3 deaths in the control (C) group. No adverse events (AEs) leading to discontinuation of any single HBOT session were observed in the HBOT group.
2.2. Study Design
The study design was consistent with that of our previous publication [44]. From the 30 patients randomly assigned to either the control group or the HBOT group, 28 met the inclusion criteria and participated in the clinical trial, thus being included in the subsequent analysis. In contrast to the control group, the HBOT group underwent five hyperbaric sessions. Prior to and following each session, an arterial blood gas test was conducted, and vital signs were documented. Additionally, blood samples were obtained for comprehensive biochemical and hematological analyses. Immunological tests were conducted on the first, fifth, and tenth days.
2.3. Detection of Cytokines and Growth Factors in Serum
IL-12p70, TNF-α, IL-4, IL-10, IL-1β, Arginase, TARC, IL-1RA, IL-12p40, IL-23, IFN-γ and IP-10 in serum were measured by the LEGENDPlex bead method (HU Macrophages/Microglia Panel (13-plex), Biolegend, USA). Serum samples were thawed on ice, centrifuged at 1000 x g for 10 minutes at 4°C, diluted according to the manufacturer's protocol and incubated with capture beads for 2 at RT with shaking. It was then washed twice and incubated with detection antibodies for 1 hour at room temperature with shaking. Detection was performed by incubating SA-PE for 30 minutes at room temperature with shaking, and after washing beads were acquired on CytoFLEX Flow Cytometer (Beckman Coulter, USA) and analysed by CytExpert v.2.3.0.84 software (Beckman Coulter, USA) according to the manufacturer's instructions. The concentration of factors was calculated relative to the standard curve using the recombinant proteins provided in the kit.
2.4. T-Cell Immunophenotyping
Peripheral blood samples were collected in EDTA-anticoagulated tube (Blood Collection tube Vacutainer®, BD, Warsaw, Poland). Whole blood was used for extracellular markers immunofluorescence staining, 100 µl of blood was stained with anti- CD4-APC (# IM2468, Beckman Coulter), anti- CD8-APC-AF700 (# B49181, Beckman Coulter), anti- CD3-APC-AF750 (# A94680, Beckman Coulter) and anti-CD45-KrO (# B36294, Beckman Coulter) for 30 min at RT. As a negative control we used unstained blood, single staining was used for compensation settings and gating strategy. Erythrocytes were lysed for 15 min at RT using BD FACS TM Lysing Solution (BD Bioscience, USA) and washed twice in PBS and then cells were fixed with Cytofix fixation buffer for 5 min (BD Bioscience, USA). Cells were acquired on CytoFLEX Flow Cytometer (Beckman Coulter, USA) and analyzed by CytExpert v.2.3.0.84 software (Beckman Coulter, USA). Debris was gated out on FCS/SSC dot plot and 30 000 events in “Cells” gate were analyzed (Figure 1).
2.5. Model Construction and Validation
The analysis was conducted in RStudio (version 2023.06.1; R version 4.3.1) with the brms package (version 2.20.1) employed for this purpose. Five Bayesian multiple regression models were constructed. The first model considers only the interaction between the day x group factor and the random factor (patient ID). The second model includes the day factor as the grouping factor of the group factor and the random factor (patient ID). The third model examines the interaction of the day x group factor and the random factor of the day as the grouping factor. Factor of the random factor of the patient ID; 4. A model with the day factor as the grouping factor of the "group" factor and the random factor of the patient ID; 5. A logistic model with the calculated change between days 10/5 and 5/1 within the group and a random factor of the patient ID.
Given the considerable variability observed, the raw values in models 1–4 were transformed into Z-values and assigned a Gaussian family. In Model 5, the family parameter was set to Bernoulli. In each model, a normal distribution with mean M = 0 and standard deviation SD = 1 was used as the prior, and the models were run with four Markov chains of 4,000 iterations. As this is the first study using HBOT in COVDI-19 patients, it is a weak prior criterion based on data distribution only.
The model with the optimal fit to the data was selected using the leave-one-out cross-validation (LOO) method with the LOO criterion, as well as the expected log pointwise predictive density (ELPD) difference, which was used to assess the overall predictive distribution of each of the first four models. Model 5, however, could not be included in this comparison due to its distinct design. Additionally, the LOO weights of each model were evaluated. Validation selected model 3 as the best fit to the data (supplementary materials table 1S).
3. Results
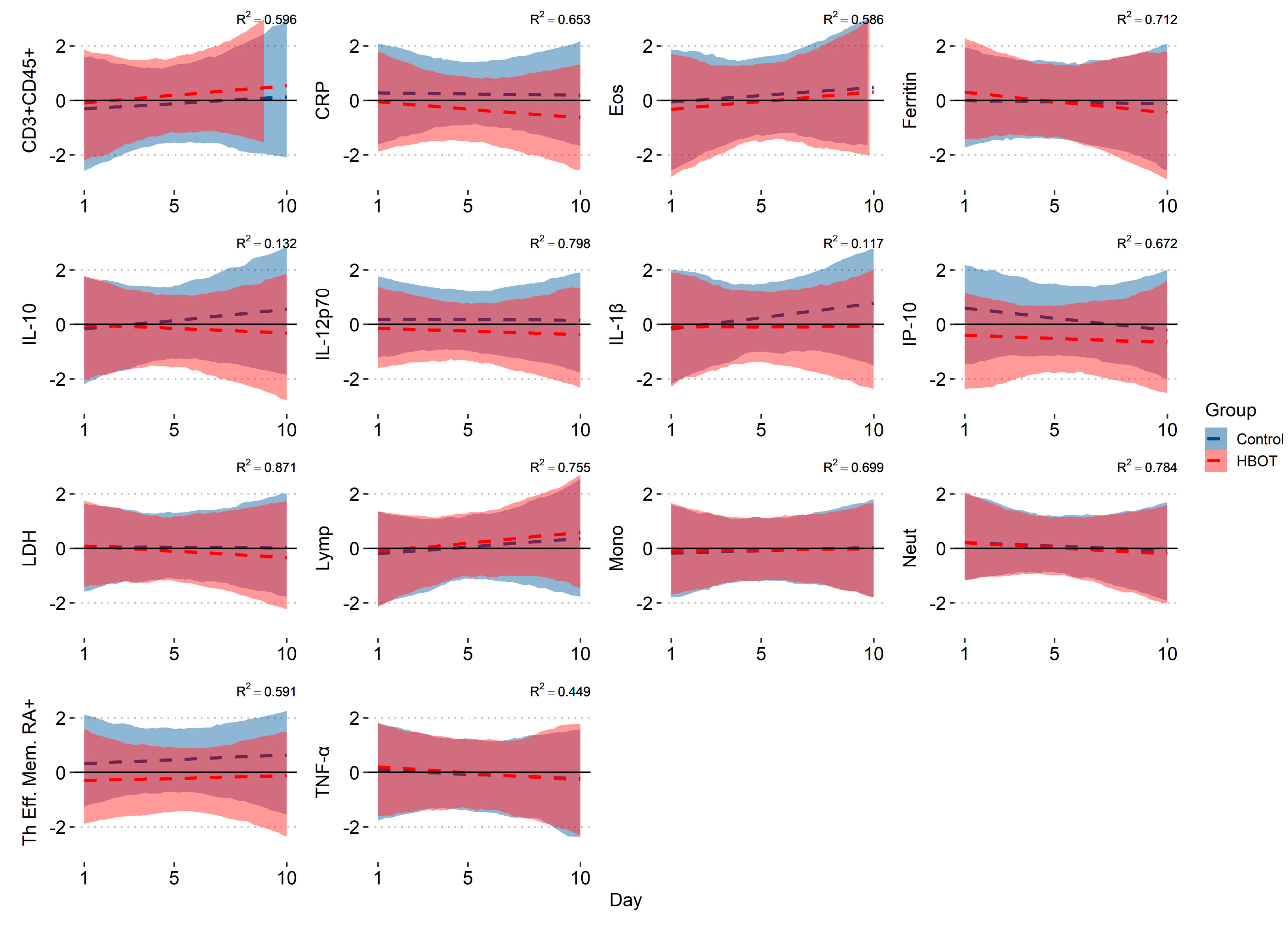
In the input measure, Control and HBOT subjects did not differ significantly in the concentrations of the analyzed cytokines and leukocyte subpopulations (Man-Whitney analysis: p > 0.05), except for IP-10 (p = 0.0018). Bayesian regression analysis showed consistent values with our previous publication, i.e. a decrease in the HBOT group in CRP -0.077 (95% CI: -0.122;-0.027), Ferritin -0.066 (95% CI: -0.107; -0.024), LDH -0.047 (95% CI: -0.083; -0.014), an increase in both groups in Eos (HBOT: 0.073 [95% CI: 0.019; 0.125]; C: 0.068 [95% CI: 0.015; 0.121]) and Lymp (HBOT: 0.074 [95% CI: 0.026; 0.122]; C: 0.059 [95% CI: 0.012; 0.109]) and a decrease in Neutr (HBOT: -0.046 [95% CI: -0.079; -0.015]; C: -0.034 [95% CI: -0.066; -0.003]), and an increase in the CD3+(% CD45+) lymphocyte population in the HBOT group of 0.071 (95% CI: 0.023; 0.122). In addition, the HBOT group showed a probability of a decrease over time in cytokine levels of TNF-α -0.048 (95% CI: -0.098; -0.0002), IL-10 -0.085 (95% CI: -0.154; -0.017), IP-10/CXCL10 -0.080 (95% CI: -0.129; -0.031), a decrease in IL-12p70 -0.026 (95% CI: -0.051;-0.0007); in the control group, an increase in the percentage of RA+ Th effector cells 0.047 (95% CI: 0.0006; 0.095) and IL-1β 0.094 (95% CI: 0.034; 0.158), Mono 0.021 (95% CI: 0.003; 0.039) (Figure 2). In the remaining variables, the probabilities were not significant (95% CI exceeded 0), so there was no basis to conclude any probability of change over time in both groups in: IL-6, IFN-γ, IL-12p40, IL-1R, IL-23, IL-4, TARC, CD8+, Tc subpopulations, Th central memory, Th effector memory, Th naïve, WBC.
4. Discussion
The present study demonstrates that hyperbaric therapy effectively influences immune dysregulation in patients with SARS-CoV-2 infection. The results indicated a reduction in inflammatory mediators, including TNF-α, IL-10, IP-10, and IL12p70, which have been associated with unfavorable patient outcomes when present at elevated levels. Furthermore, the absence of hyperbaric oxygen therapy (HBOT) was associated with an increased likelihood of an increase in interleukin-1 beta (IL-1β) levels within 10 days.
While there is a growing body of literature on the positive effects of hyperbaric oxygen therapy (HBOT) in patients infected with SARS-CoV-2, the majority of studies have focused on the positive effects on the respiratory system [40, 42, 45, 47, 49], including blood saturation, myocardial function [48] and cognitive function [49, 50]. In case of short effects of HBOT, findings corroborate the safety and efficacy of hyperbaric oxygen therapy (HBOT) in the treatment of Coronavirus Disease 2019 (COVID-19). Furthermore, these findings indicate that the time required for the correction of hypoxemia was shorter in patients who underwent HBOT [43]. A publication describing the effect of hyperbaric oxygen therapy (HBOT) on respiratory function and inflammatory parameters in patients requiring oxygen supplementation demonstrated that HBOT reduced the levels of lactate dehydrogenase (LDH), d-dimers, and endothelial adhesion molecules, including sVCAM, sICAM, sPselectin, and inflammation-related proteins such as SAA and MPO. Among the cytokines tested, a significant difference was observed only in IL-15 [46].
Nevertheless, the majority of extant studies concerning the utilization of hyperbaric oxygen therapy (HBOT) in the context of SARS-CoV-2 infection concentrate on its deployment in the management of the long-term consequences of coronavirus disease 2019 (COVID-19). In a study evaluating cognitive function in post-COVID-19 patients treated HBOT [49] authors proved that the administration of hyperbaric oxygen therapy (HBOT) resulted in a statistically significant improvement in higher cognitive functions and attention. In a case series of ten patients following SARS-CoV-2 infection, Robbins et al. [50] proposed that HBOT may confer benefits with respect to fatigue and cognitive function. They observed notable improvements in both cognitive function and physical and mental symptoms. In addition to this clinical study, cardiac function was also assessed. In another study involving post-Covid patients reporting cognitive problems affecting their quality of life, HBOT was demonstrated to reduce impaired systolic function (GLS) [48].A growing body of clinical and scientific evidence suggests that hyperbaric oxygen therapy (HBOT) may be an effective method for improving the course of infection and reducing the risk of distant complications [3, 4, 47, 48, 49, 50].
This study reveals that hyperbaric oxygen therapy (HBOT) has a significant effect on immune dysfunction in individuals afflicted with SARS-CoV-2. The findings showed a notable decrease in various inflammatory markers, including TNF-α, IL-10, IP-10, and IL-12p70, which are typically linked to poor outcomes in patients when present at high levels. Furthermore, patients not receiving HBOT displayed a higher likelihood of increased interleukin-1 beta (IL-1β) levels within 10 days. Additionally, there’s been showed that the probability of increase of Th effector memory RA+ lymphocytes is higher in a control group. On the one hand, this may suggest that patients in this group have a more effective Th cell response, but the results suggest that although HCs that have overall higher levels of RA+ memory effector Th cells, these cells do not predict a better outcome [51]. While there is a growing body of research supporting the beneficial effects of HBOT, particularly concerning respiratory health, our results affirm its safety and effectiveness as a treatment option for COVID-19. Benefits of this study consist of the analysis of molecules involved in immune responses through sophisticated analytical techniques, offering crucial insights into the interaction between HBOT and immune modulation, particularly when treatment commences early during the illness. This suggests that HBOT could be an effective supplementary therapy for enhancing patient recovery and easing complications associated with COVID-19. Future clinical trials are necessary to substantiate these findings and broaden the understanding of HBOT's role in treating SARS-CoV-2 infections and their aftereffects. Limitations of this investigation include the relatively small participant group, which may limit the applicability of the results. Moreover, further studies are essential to confirm the long-term impact of HBOT on inflammatory indicators and immune reactions.
5. Conclusions
The findings of our study are complementary to our previous findings and supplement them with new molecules, i.e. T lymphocyte subpopulations and pro-inflammatory molecules and using more complex probability-based statistical modeling. By analyzing TNF-α, IP-10/CXCL10 and IL-12p70, we showed that the probability of a decrease in these factors, associated with a poor outcome, was observed in HBOT but not in the control group. These results suggest that hyperbaric oxygen therapy (HBOT) may improve the condition of patients with SARS-CoV-2 infection and reduce excessive immune cell activity, particularly when initiated early in the course of illness and probably only in narrow spectrum of highly selected patients for whom other treatments were ineffective or have been refused by patients. While there is optimism regarding the potential role of HBOT in the treatment of patients with SARS-CoV-2 infection — especially those with long-term complications from the virus — further clinical trials are necessary to ascertain whether such an intervention can improve the prognosis of hospitalized patients.
Author Contributions
Conceptualization: J.S., K.B. and J.K.; methodology: J.S., K.B., N.J. and J.K.; formal analysis: N.J., J.S., K.B. and J.K.; investigation: J.S., K.B., A.L., K.K.; writing—original draft preparation: N.J., J.S. and J.K.; writing—review and editing: N.J., J.K, J.S., K.B.,A.L. and K.K.; funding acquisition, J.S. and J.K. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by the Polish Medical Research Agency (grant 2020/ABM/COVID19/0043).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee of Military Institute of Medicine (no. 25/WIM/2020 approved on 18 November 2022) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors are especially indebted to all employees of the designated COVID-19 clinics of the Military Medical Institute involved in the implementation of this clinical trial.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online at: https://covid19.who.int/ (accessed 17 Sep 2023).
- WHO. Currently circulating variants of interest (VOIs) (as of 28 June 2024). Available online at: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed 8 Sep 2024).
- Oliaei, S.; Paranjkhoo, P.; SeyedAlinaghi, S.; Mehraeen, E.; Hackett D. Is There a Role for Hyperbaric Oxygen Therapy in Reducing Long-Term COVID-19 Sequelae? J. Clin. Med. 2023, 12, 2270.
- Kjellberg, A.;Hassler, A.; Boström, E. et al. Hyperbaric oxygen therapy for long COVID (HOT-LoCO), an interim safety report from a randomised controlled trial. BMC Infect. Dis. 2023, 23(1), 33. [CrossRef]
- Zamani Rarani, F.; Zamani Rarani, M.; Hamblin, M.R.; Rashidi, B.; Hashemian, S.M.R.; Mirzaei, H. Comprehensive overview of COVID-19-related respiratory failure: focus on cellular interactions. Cell Mol. Biol. Lett. 2022, 27(1), 63. [CrossRef]
- Ramadan, M.S.; Bertolino, L.; Zampino, R.; Durante-Mangoni, E.; Monaldi Hospital Cardiovascular Infection Study Group. Cardiac sequelae after coronavirus disease 2019 recovery: a systematic review. Clin. Microbiol. Infect. 2021, 27(9), 1250-1261. [CrossRef]
- Cothran, T.P.; Kellman, S.; Singh, S; et al. A brewing storm: The neuropsychological sequelae of hyperinflammation due to COVID-19. Brain Behav. Immun. 2020, 88, 957-958. [CrossRef]
- Gheware, A.; Ray, A.; Rana, D.; et al. ACE2 protein expression in lung tissues of severe COVID-19 infection. Sci. Rep. 2022, 12(1), 4058. [CrossRef]
- Perkins, G.D.; Ji, C.; Connolly, B.A.; et al. Effect of Noninvasive Respiratory Strategies on Intubation or Mortality Among Patients With Acute Hypoxemic Respiratory Failure and COVID-19: The RECOVERY-RS Randomized Clinical Trial. JAMA. 2022, 327(6), 546-558.
- Phetsouphanh, C.; Darley, D.R.; Wilson, D.B.; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat. Immunol. 2022, 23(2), 210-216.
- van de Veerdonk, F.L.; Giamarellos-Bourboulis ,E.; Pickkers, P.; et al. A guide to immunotherapy for COVID-19. Nat. Med. 2022, 28(1), 39-50. [CrossRef]
- Gil-Etayo, F.J.; Suarez-Fernandez, P.; Cabrera-Marante, O.; Arroyo, D.; Garcinuno, S.; Naranjo, L.; et al. T-Helper Cell Subset Response Is a Determining Factor in COVID-19 Progression. Front. Cell. Infect. Microbiol. 2021, 11, 624483. [CrossRef]
- Boechat, J.L.; Chora, I.; Morais, A.; Delgado, L. The immune response to SARS-CoV-2 and COVID-19 immunopathology - Current perspectives. Pulmonology. 2021, 27(5), 423-37.
- Moss, P. The T cell immune response against SARS-CoV-2. Nat. Immunol. 2022, 23(2), 186-93.
- Habel, J.R.; Nguyen, T.H.O.; van de Sandt, C.E.; Juno, J.A.; Chaurasia, P.; Wragg, K.; et al. Suboptimal SARS-CoV-2-specific CD8(+) T cell response associated with the prominent HLA-A*02:01 phenotype. Proc. Natl. Acad. Sci. U.S.A. 2020, 117(39), 24384-91.
- Laing, A.G.; Lorenc, A.; del Molino del Barrio, I.; Das, A.; Fish, M.; Monin, L.; Muñoz-Ruiz, M.; McKenzie, D.R.; Hayday, T.S.; Francos-Quijorna, I.; et al. A dynamic COVID-19 immune signature includes associations with poor prognosis. Nat. Med. 2020, 26, 1623-1635.
- Gorenstein, S.A.; Castellano, M.L.; Slone, E.S.; et al. Hyperbaric oxygen therapy for COVID-19 patients with respiratory distress: treated cases versus propensity-matched controls. Undersea Hyperb. Med. 2020, 47(3), 405-413.
- Wang, J.; Yang, X.; Li, Y.; Huang, J.-A.; Jiang, J.; Su, N. Specific cytokines in the inflammatory cytokine storm of patients with COVID-19-associated acute respiratory distress syndrome and extrapulmonary multiple-organ dysfunction. Virol. J. 2021, 18, 117.
- Rarani, F.Z.; Rashidi, B.; Jafari Najaf Abadi M.H.; Hamblin, M.R.; Reza Hashemian, S.M.; Mirzaei, H. Cytokines and microRNAs in SARS-CoV-2: What do we know? Mol. Ther. Nucleic Acids. 2022, 29, 219-242.
- Mulchandani, R.; Lyngdoh, T.; Kakkar, A.K. Deciphering the COVID-19 cytokine storm: Systematic review and meta-analysis. Eur. J. Clin. Investig. 2021, 51, e13429. [CrossRef]
- Kuppalli, K.; Rasmussen, A.L. A glimpse into the eye of the COVID-19 cytokine storm. EBioMedicine 2020, 55, 102789.
- Mangalmurti, N.; Hunter, C.A. Cytokine Storms: Understanding COVID-19. Immunity 2020, 53(1), 19-25.
- Zhang, Q.; Zhang, H.; Yan, X.; et al. Neutrophil infiltration and myocarditis in patients with severe COVID-19: A post-mortem study. Front. Cardiovasc. Med. 2022, 9, 1026866. [CrossRef]
- Hosseini, A.; Stojkov, D.; Fettrelet, T.; Bilyy, R.; Yousefi, S.; Simon, H.U. Transcriptional Insights of Oxidative Stress and Extracellular Traps in Lung Tissues of Fatal COVID-19 Cases. Int. J. Mol. Sci. 2023, 24(3), 2646.
- Veenith, T.; Martin, H.; Le Breuilly, M.; et al. High generation of reactive oxygen species from neutrophils in patients with severe COVID-19. Sci. Rep. 2022, 12(1), 10484.
- Diao, B.; Wang, C.; Tan, Y.; et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [CrossRef]
- Laforge, M.; Elbim, C.; Frère, C.; et al. Tissue damage from neutrophil-induced oxidative stress in COVID-19 [published correction appears in Nat. Rev. Immunol. 2020, 20(9), 515-516.
- Mathieu, D.; Marroni, A.; Kot, J. Tenth European Consensus Conference on Hyperbaric Medicine: recommendations for accepted and non-accepted clinical indications and practice of hyperbaric oxygen treatment. Diving hyperbar. med.: j. South Pac. Under. Med. Soc.. 2017, 47(1):24-32.
- Shinomiya, N.; Asai, Y. Hyperbaric Oxygenation Therapy: Molecular Mechanisms and Clinical Applications. Singapore: Springer Nature; 2019; pp. 55–65.
- Boet, S.; Martin, L.; Cheng-Boivin, O.; et al. Can preventive hyperbaric oxygen therapy optimise surgical outcome?: A systematic review of randomised controlled trials. Eur. J. Anaesthesiol. 2020, 37(8), 636-648.
- Fosen, K.M,; Thom, S.R. Hyperbaric oxygen, vasculogenic stem cells, and wound healing. Antioxid. Redox. Signal. 2014, 21(11), 1634-1647. [CrossRef]
- de Wolde, S.D.; Hulskes, R.H.; de Jonge, S.W.; et al. The Effect of Hyperbaric Oxygen Therapy on Markers of Oxidative Stress and the Immune Response in Healthy Volunteers. Front. Physiol. 2022, 13, 826163.
- Bosco, G.; Paganini, M.; Giacon, T.A.; et al. Oxidative Stress and Inflammation, MicroRNA, and Hemoglobin Variations after Administration of Oxygen at Different Pressures and Concentrations: A Randomized Trial. Int. J. Environ. Res. Public Health 2021, 18(18), 9755. [CrossRef]
- Lalieu, R.C.; Brouwer, R.J.; Ubbink, D.T.; Hoencamp, R.; Bol Raap, R.; van Hulst, R.A. Hyperbaric oxygen therapy for nonischemic diabetic ulcers: A systematic review. Wound Repair Regen. 2020, 28, 266–275. [CrossRef]
- Brouwer, R.J.; Lalieu, R.C.; Hoencamp, R.; van Hulst, R.A.; Ubbink, D.T. A systematic review and meta-analysis of hyperbaric oxygen therapy for diabetic foot ulcers with arterial insufficiency. J. Vasc. Surg. 2020, 71, 682–692.e681. [CrossRef]
- Löndahl, M.; Boulton, A.J. Hyperbaric oxygen therapy in diabetic foot ulceration: Useless or useful? A battle. Diabetes/Metab. Res. Rev. 2020, 36, e3233. [CrossRef]
- Lerche, C.J.; Schwartz, F.; Pries-Heje, M.M.; Fosbøl, E.L.; Iversen, K.; Jensen, P.Ø.; Høiby, N.; Hyldegaard, O.; Bundgaard, H.; Moser, C. Potential advances of adjunctive hyperbaric oxygen therapy in infective endocarditis. Front. Cell. Infect. Microbiol. 2022, 12, 15. [CrossRef]
- Hajhosseini, B.; Kuehlmann, B.A.; Bonham, C.A.; Kamperman, K.J.; Gurtner, G.C. Hyperbaric oxygen therapy: Descriptive review of the technology and current application in chronic wounds. Plast. Reconstr. Surg. Glob. Open 2020, 8, e3136. [CrossRef]
- Vinkel, J.; Rib, L.; Buil, A.; Hedetoft, M.; Hyldegaard, O. Key pathways and genes that are altered during treatment with hyperbaric oxygen in patients with sepsis due to necrotizing soft tissue infection (HBOmic study). Eur. J. Med. Res. 2023, 28(1), 507. [CrossRef]
- Wu, X.; Liang, T.Y.; Wang, Z.; Chen, G. The role of hyperbaric oxygen therapy in inflammatory bowel disease: a narrative review. Med. Gas. Res. 2021, 11(2), 66-71.
- Zhong, X.T.Y.; Chen, R. Effect of Hyperbaric Oxygen Therapy on HBOT in Patients with Severe New Coronavirus Pneumonia: First Report Chinese. Chin. J. Naut. Med. Hyperb. Med. 2020, 27, 132–135.
- ECHM. European Committee for Hyperbaric Medicine (ECHM) Position on Hyperbaric Oxygen Therapy (HBOT) in Multiplace Chambers During Coronavirus Disease (COVID-19) Outbreak. Available online: http://www.echm.org/documents/ECHM%20position%20on%20HBOT%20and%20COVID-19%20(16th%20March%202020).pdf (accessed on 8 Sep 2024).
- Cannellotto, M.; Duarte, M.; Keller, G.; et al. Hyperbaric oxygen as an adjuvant treatment for patients with COVID-19 severe hypoxaemia: a randomised controlled trial. Emerg. Med. J. 2022, 39(2), 88-93.
- Siewiera, J.; Brodaczewska, K.; Jermakow, N.; Lubas, A.; Kłos, K.; Majewska, A.; Kot, J. Effectiveness of Hyperbaric Oxygen Therapy in SARS-CoV-2 Pneumonia: The Primary Results of a Randomised Clinical Trial. J. Clin. Med. 2023, 12(1), 8.
- Gorenstein, S.A.; Castellano, M.L.; Slone, E.S.; et al. Hyperbaric oxygen therapy for COVID-19 patients with respiratory distress: treated cases versus propensity-matched controls. Undersea Hyperb Med. 2020, 47(3), 405-413.
- Keller, G.A.; Colaianni, I.; Coria, J.; Di Girolamo, G.; Miranda, S. Clinical and biochemical short-term effects of hyperbaric oxygen therapy on SARS-Cov-2+ hospitalized patients with hypoxemic respiratory failure. Respir. Med. 2023, 209, 107155.
- Bhaiyat, A.M.; Sasson, E.; Wang, Z.; et al. Hyperbaric oxygen treatment for long coronavirus disease-19: a case report. J. Med. Case. Rep. 2022, 16(1), 80.
- Leitman, M.; Fuchs, S.; Tyomkin, V.; Hadanny, A.; Zilberman-Itskovich, S.; Efrati, S. The effect of hyperbaric oxygen therapy on myocardial function in post-COVID-19 syndrome patients: a randomized controlled trial. Sci. Rep. 2023, 13(1), 9473.
- Robbins, T.; Gonevski, M.; Clark, C.; Baitule, S.; Sharma, K.; Magar, A.; Patel, K.; Sankar, S.; Kyrou, I.; Ali, A.; et al. Hyperbaric oxygen therapy for the treatment of long COVID: Early evaluation of a highly promising intervention. Clin. Med. 2021, 21, e629–e632.
- Ceban, F.; Leber, A.; Jawad, M.Y.; et al. Registered clinical trials investigating treatment of long COVID: a scoping review and recommendations for research. Infect Dis (Lond). 2022, 54(7), 467-477. [CrossRef]
- Odak, I.; Barros-Martins, J.; Bošnjak, B.; et al. Reappearance of effector T cells is associated with recovery from COVID-19. EBioMedicine, 2020, 57, 102885. [CrossRef]
Figure 1.
Gating strategy for lymphocytes subsets; all cells (A), CD45+ leucocytes (B), T lymphocytes CD45+ CD3+ (C), Th CD45+ and CD3+, CD4+ and Tc CD45+CD3+ CD8+ lymphocytes (D), and then Th cells were identified as Th effector memory re-expressing CD45RA, CD62L–CD45RA+), Th naïve (CD62L+CD45RA+), Th effector memory (CD62L−CD45RA−) and Th central memory, CD62L+CD45RA–) (E).
Figure 1.
Gating strategy for lymphocytes subsets; all cells (A), CD45+ leucocytes (B), T lymphocytes CD45+ CD3+ (C), Th CD45+ and CD3+, CD4+ and Tc CD45+CD3+ CD8+ lymphocytes (D), and then Th cells were identified as Th effector memory re-expressing CD45RA, CD62L–CD45RA+), Th naïve (CD62L+CD45RA+), Th effector memory (CD62L−CD45RA−) and Th central memory, CD62L+CD45RA–) (E).
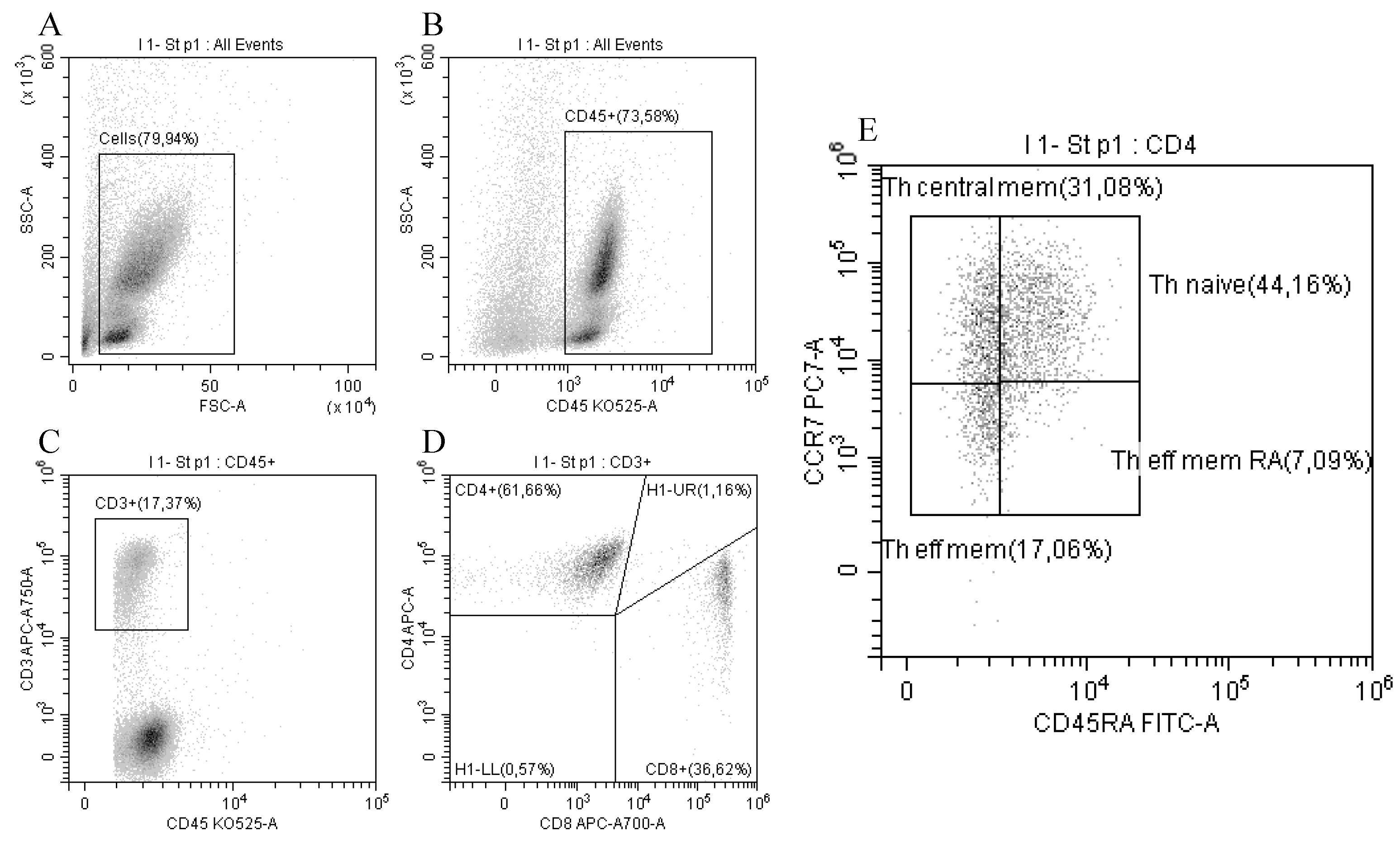
Figure 2.
Bayesian regression model; the figure shows the mean value of the regression coefficient (dashed line) along with 95% confidence intervals and Bayesian R2 measure; respectively: CD3+(% CD45+) lymphocyte population; C-Reactive Protein (CRP); Eosinophiles (Eos); Ferritin, Interleukin 10 (IL-10); Interleukin 12 (IL-12 p70); Interleukin 1 beta (IL-1β); Interferon gamma-induced protein (IP-10/CXCL10); Lactate dehydrogenase (LDH); Lymphocytes (Lymph); Monocytes (Mono); Neutrophils (Neut); RA+ Th effector memory lymphocytes (Th Eff. Mem. RA+); Tumor necrosis factor alpha (TNF-α).
Figure 2.
Bayesian regression model; the figure shows the mean value of the regression coefficient (dashed line) along with 95% confidence intervals and Bayesian R2 measure; respectively: CD3+(% CD45+) lymphocyte population; C-Reactive Protein (CRP); Eosinophiles (Eos); Ferritin, Interleukin 10 (IL-10); Interleukin 12 (IL-12 p70); Interleukin 1 beta (IL-1β); Interferon gamma-induced protein (IP-10/CXCL10); Lactate dehydrogenase (LDH); Lymphocytes (Lymph); Monocytes (Mono); Neutrophils (Neut); RA+ Th effector memory lymphocytes (Th Eff. Mem. RA+); Tumor necrosis factor alpha (TNF-α).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



