Submitted:
19 December 2024
Posted:
19 December 2024
You are already at the latest version
Abstract
Obstructive Sleep Apnea is a highly prevalent disease effecting and estimated 1 billion people worldwide. Untreated, Obstructive Sleep Apnea is associated with elevated levels of mortality, decreased quality of life and increased economic costs. However, the strong efficacy of Continuous Positive Airway Pressure therapy, the most frequently prescribed treatment for Obstructive Sleep Apnea, is compromised by frequent refusal and termination rates. As a result, healthcare providers are evaluating non-CPAP treatment options for patients who terminate or refuse Continuous Positive Airway Pressure therapy. Oral Appliance Therapy devices have emerged as a leading alternative. With dozens of Oral Appliance Therapy devices available to healthcare providers, this review investigates whether different Oral Appliance Therapy device designs matter; are different Oral Appliance device designs associated with different levels of efficacy? This review evaluated 149 different source papers investigating the efficacy of Oral Appliance Therapy, yielding 39 unique papers that met the inclusion criteria, encompassing a pooled sample of 3,799 patients treated with six distinctly different Oral Appliance Therapy device designs. Chi-squared and two-sided Fisher’s exact tests revealed significant differences. As a result, healthcare providers and medical guidelines should consider Oral Appliance Therapy device designs when prescribing Oral Appliance Therapy for the treatment of Obstructive Sleep Apnea.
Keywords:
Obstructive sleep apnea
; OSA
; sleep Apnea
; Sleep Disordered Breathing
; Respiratory Medicine
; Oral Appliance Therapy
; sleep Medicine
; Dental Sleep MEdicine
; Medical Devices
Introduction & Background
Obstructive Sleep Apnea (“OSA”) is a highly prevalent disease afflicting an estimated 1 billion people worldwide [1]. Left untreated, OSA is associated with elevated levels of mortality, economic expenses [2], and reductions in quality of life [3]. Many healthcare providers are revisiting contemporary Oral Appliance Therapy (“OAT” also called “Mandibular Advancement” or “Mandibular Repositioning”) as a treatment modality for OSA, largely motivated by adverse developments over treatment with Continuous Positive Airway Pressure (“CPAP”). Studies have associated CPAP with low compliance rates [4,5] and negative heart health outcomes for certain types of patients [6]. Several brands of CPAP devices have also been recalled by the US Food and Drug Administration [7]. However, some remain skeptical of non-CPAP treatment options, and continue prescribing CPAP more frequently than OAT [8].
This is the first review, to the best of the authors’ knowledge, to evaluate the specific association between different OAT device designs and treatment efficacy, specifically defined as the percentage of patients who achieve a residual AHI of less than 10 events per hour as the standardized definition for therapeutic success.
Prescription of Oral Appliance Therapy (“OAT”) is a standard recommendation for the treatment of Obstructive Sleep Apnea (“OSA”) for adult patients who are intolerant of Continuous Positive Airway Pressure (“CPAP”) or prefer alternative treatment [9]. Research establishes that OAT is non-inferior to CPAP in terms of cardiovascular and neurobehavioral outcomes [10], systolic blood pressure [9], diastolic blood pressure [9], mean arterial blood pressure [11], and overall health outcomes [12]. OAT is covered by most commercial medical insurances in the United States [13] and by government-sponsored programs in several countries around the world, including Medicare in the USA [14]. Successful OAT response is also associated with improved cardiac autonomic adaptability in patients with OSA [15], improved cognition [16], and significant reverse left ventricular hypertrophic remodeling [17]. It is thought that the greater Apnea Hypopnea Index (“AHI”) reduction of CPAP is offset by the superior adherence of OAT, resulting in similar, non-inferior, mean disease alleviation [18]. It is hypothesized that improved adherence is necessary to improve the therapeutic effectiveness of CPAP and that improved efficacy is necessary to improve the therapeutic effectiveness of OAT [19].
More discerning OAT device selection is thought to be one strategy for optimizing the efficacy of OAT. Guidelines establish that efficacious OAT devices are those that successfully: 1. reposition, 2. stabilize and 3. titrate the mandible to reduce the risk of airway collapse [20]. Other hypothesized strategies for optimizing OAT include the expertise of the therapy provider and preselecting patients based upon endotypical and phenotypical characteristics [21].
A comparative study supports our hypothesis that different OAT device design are associated with different levels of efficacy [22]. Other comparative studies find no statistically significant difference in efficacy based on OAT device designs [23], but does acknowledge clinically meaningful differences.
OAT Mechanistic Device Design Categories
For this review OAT devices were organized into six categories of designs, specifically defined by how each device is engineered to achieve the cardinal mechanism of action that is associated with efficacy: mandibular repositioning. The six categories of OAT device designs were: 1. Lateral Push, 2. Lateral Pull, 3. Interlocking Dorsal, 4. Precision Post, 5. Mono/Twin Block, and 6. Anterior Pull.
Lateral Push
Lateral Push device designs have mechanisms, typically metal rods known as Herbst arms, on each side of upper and lower overlays that sit on the upper and lower dentitions, respectively. Lateral Push devices reposition the mandible by pushing the lower overlay component forward, using the upper overlay as an anchor. Titration of the mandibular position is achieved by turning displacement screws embedded into the metal Herbst rods.
Lateral Pull
Lateral Pull device designs have mechanisms, typically elastomeric or nylon components, on each side of the upper and lower overlays that sit on the upper and lower dentitions, respectively. Lateral Pull devices reposition the mandible by pulling the lower overlay component forward, using the upper overlay as an anchor. Titration of the mandibular position is achieved by swapping out/in different size elastomeric or nylon components.
Interlocking Dorsal
Interlocking Dorsal device designs have angled dorsal posts that extend occlusally from each side of the lower overlays. These dorsal posts reposition and stabilize the mandible by interlocking with block features affixed to either side of the upper overlay. Titration of the mandibular position is achieved by turning displacement screws embedded into the block mechanisms (e.g. 10 turns of the screw yield +1mm of mandibular repositioning)
Precision Post
Precision Post device designs feature dual posts that extend occlusally from each side of the upper and lower overlays that sit on the upper and lower dentitions, respectively. The dual posts interlock to precisely reposition and stabilize the mandible at the prescribed location to minimize the risk of airway collapse. Titration of the mandibular position is achieved iteratively by swapping out an upper or lower overlay for a new overlay that contains a different mandibular repositioning setting (eg +1mm of mandibular repositioning).
Mono/Twin Block
Mono/Twin Block device designs reposition and stabilize the mandible with upper and lower overlays that are fused together (mono block) at the occlusal surface of each overlay, or mated (twin block) by interlocking block components affixed to the occlusal surfaces of the upper and lower overlays. Titration of the mandibular position is achieved by swapping out an upper or lower overlay for a new overlay that contains a different setting.
Anterior Pull
Anterior Pull device designs use upper and lower overlay components that sit on the upper and lower dentitions, respectively, and feature an anterior fixation mechanism, typically a screw or a nylon strap, that repositions the mandible using the opposing overlay as an anchor. Titration of the mandibular position is achieved by turning the anterior displacement screw or by swapping out the strap for a new strap with a different length.
OAT devices can be custom-made, or prefabricated. This review is limited to custom-made, titratable devices. Guidelines, based on systemic scientific reviews, recommend the prescription of custom-made titratable devices [8].
Review
Objective
The primary objective of this review is to interrogate the hypothesis that different OAT designs are associated with different rates of efficacy.
Search Strategy
A literature search was conducted, drawing from the bibliographies of four, existing, systemic reviews that evaluate the efficacy of Oral Appliance Therapy for the treatment of Obstructive Sleep Apnea. The four reviews were: Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy [9], Definition of an Effective Oral Appliance [20], Mandibular Advancement Device: A Systemic Review on Outcomes [24], and Precision vs. Traditional Oral Appliance Therapy: A Comparison of Efficacy [25]. This search strategy was selected as a safeguard against selection bias, as each of these reviews had previously identified articles relevant to the efficacy of OAT, and had applied screening criteria including quality assessment tools such as the GRADE system, Cochrane Risk Bias, Network-Ottawa Scale, and Rand-UCLA Appropriateness Method.
Selection Criteria
The following selection criteria were applied to the universe of source articles.
To be selected, the article must:
- Evaluate the efficacy of Oral Appliance Therapy devices;
- Describe the interventional OAT device in enough detail to facilitate definitive OAT device design categorization;
- Define and report therapeutic success as the percentage of patients achieving a residual AHI of less than 10 events per hour; and,
Definition of Therapeutic Efficacy: Residual AHI < 10 Events Per Hour
Defining the success for the treatment of OSA with OAT is not a straightforward endeavor [26]. Several articles define efficacy as a residual AHI value of less than five events per hour, which is typically considered a CPAP definition of success. Others use the Sher’s criteria for surgical success, which calls for a residual AHI of less than 20 events per hour and a 50% improvement relative to baseline [27]. Others report the mean percent reduction in AHI events per hour for the study population as a definition of success. Each of these definitions of efficacy have merits and limitations. A residual AHI of less than 10 events per hour is used in this review. AHI of less than 10 events per hour was the most frequently used definition of success amongst the total universe of eligible articles.
It should be noted that recent scientific investigations have scrutinized the utility of AHI as a definition for success. Specifically, investigations have concluded that AHI is a poor surrogate for predicting health outcomes [28]. Nonetheless, AHI remains the most commonly used metric for diagnosing patients, evaluating treatment success, determining insurance coverage and managing long term treatment.
Collection of Data
Data related to the sample size, the percentage of patients who achieved a residual AHI of less than 10 events per hour, the design of the interventional OAT device, and other notable study features were collected, organized and summarized in a database. Data on treatment planning characteristics such as mandibular starting location, titration schedule, sleep testing approaches, were not collected as data was sparse and protocols were inconsistent across the eligible articles.
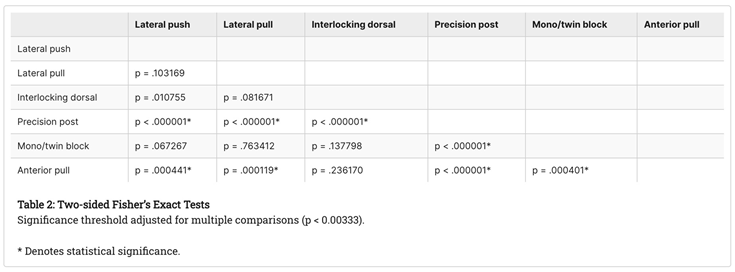
Statistical Methods
Chi-squared and two-sided Fisher’s exact tests were selected to evaluate the significance of differences between the six categories of device designs. The p-value threshold for statistical significance of the two-sided Fisher’s exact tests were adjusted to 0.00333 to account for the multiple comparisons (0.05/15 comparisons).
Search Strategy Results
The bibliographies of the four systemic reviews encompassed 149 articles. After eliminating redundancies, 39 articles met the inclusion criteria. The 39 articles encompassed a pooled sample of 3,799 individual subjects, for an average of 97 subjects per article. The article with the largest sample size had 601 subjects. The article with the smallest sample size had 16 subjects. Four articles for a total of 113 subjects reported the efficacy of Lateral Push OAT devices. Seven articles encompassing 820 subjects reported the efficacy of Lateral Push devices. Six articles encompassing 366 subjects reported the efficacy of Interlocking Flange devices. Nine articles involving 729 subjects reported the efficacy of Precision Post devices. Eight articles involving 833 subjects reported on Twin/Mono Block devices. Five articles involving 1,027 subjects reported efficacy for Anterior Pull devices.

Table 1.
Search Results.
| OAT Device Design Category | Short Description | Sample Size (“n”) | % AHI<10 |
|---|---|---|---|
| Lateral Push | Bloch 2000 | 16 | 67% |
| Lateral Push | Randerath 2022 | 20 | 30% |
| Lateral Push | Gagnadoux 2009 | 30 | 70% |
| Lateral Push | Ghazal 2008 | 47 | 43% |
| Lateral Pull | Henke 1999 | 28 | 32% |
| Lateral Pull | Kuna 2005 | 21 | 43% |
| Lateral Pull | Vecchirini 2016 | 369 | 64% |
| Lateral Pull | Isacsson 2017 | 55 | 56% |
| Lateral Pull | Isacsson 2019 | 146 | 50% |
| Lateral Pull | Tekelberg 2020 | 146 | 68% |
| Lateral Pull | Isacsson 2017 | 55 | 61% |
| Interlocking Flange | Vanderveken 2024 | 91 | 56% |
| Interlocking Flange | de Ruiter 2020 | 36 | 75% |
| Interlocking Flange | Remmers 2013 | 67 | 87% |
| Interlocking Flange | Van Haesendonck 2016 | 112 | 57% |
| Interlocking Flange | Mehta 2001 | 24 | 54% |
| Interlocking Flange | Schneiderman 2021 | 36 | 69% |
| Dual Post | Mosca 2022 | 58 | 81% |
| Dual Post | Murphy 2021 | 50 | 83% |
| Dual Post | Remmers 2017 | 53 | 86% |
| Dual Post | Sall 2021 | 115 | 87% |
| Dual Post | Sall 2023 | 91 | 89% |
| Dual Post | Silva 2023 | 22 | 95% |
| Dual Post | Stern 2021 | 28 | 89% |
| Dual Post | Kang 2024 | 24 | 88% |
| Dual Post | Dekow 2023 | 288 | 86% |
| Block | Bloch 2000 | 17 | 75% |
| Block | de Britto 2013 | 19 | 58% |
| Block | Dutta 2022 | 62 | 59% |
| Block | Lettieri 2011 | 203 | 64% |
| Block | Isacsson 2017 | 110 | 61% |
| Block | Isacsson 2019 | 156 | 53% |
| Block | Tekelberg 2020 | 156 | 65% |
| Block | Isacsson 2017 | 110 | 56% |
| Anterior Pull | Vanderveken 2024 | 118 | 75% |
| Anterior Pull | Lettieri 2011 | 602 | 74% |
| Anterior Pull | Schneiderman 2021 | 36 | 56% |
| Anterior Pull | Ghazal 2008 | 48 | 39% |
| Anterior Pull | Pancer 1999 | 134 | 51% |
Statistical Analysis
The chi-squared test demonstrated significant (p < 0.000001) differences between the device categories.
The two-sided Fisher’s exact tests indicated significance differences in efficacy for the Precision Post category relative to the other five categories: Lateral Push, Lateral Pull, Interlocking Dorsal, Mono-Twin Block and Anterior Pull categories.
The two-sided fisher’s exact tests also indicated significant differences in efficacy for the Anterior Pull category relative to Lateral Push (p = 0.000441), Lateral Pull (p = 0.000119) and the Mono/Twin Block (p = 0.000401).
The two-sided Fisher’s exact test did not indicate significant differences in efficacy amongst any of the other device design categories.
Descriptive Statistical Results
Across all device categories, 63% of the 3,799 subjects included in this review of 39 articles achieved a residual AHI of less than 10 events per hour. The median efficacy value was 64%. The maximum efficacy reported by any individual article was 95%. The minimum efficacy reported any individual article was 30%.
Efficacy by Device Design Category
The Precision Post device design category was associated with the greatest median efficacy, with 87% of the 729 subjects achieving a residual AHI of less than 10 events per hour. Conversely, the Lateral Push device design category was associated with the lowest median efficacy, with 55% of 113 subjects achieving a residual AHI of less than 10 events per hour. Lateral Pull, Anterior Pull, Mono/Twin Block, Interlocking Dorsal device design categories were associated with achieving 56%, 56%, 60% and 63% mean residual AHI of less than 10 events per hour, respectively. See Figure 1 for additional detail.
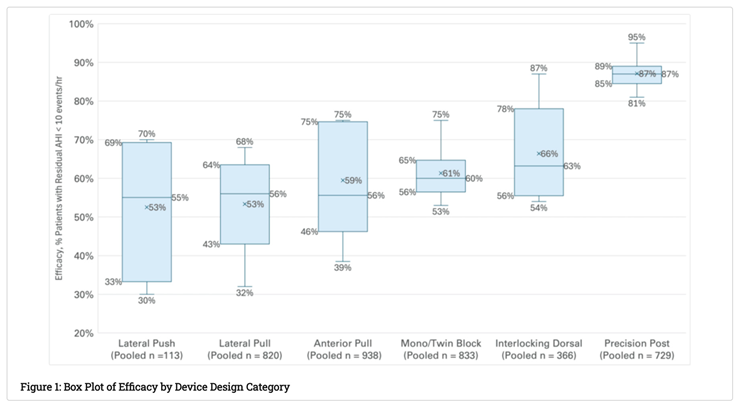
Subjective Device Design Observations
The Precision Post category of devices demonstrated significant, favorable, efficacy over all other categories of devices. To a lesser extent, the Anterior Pull category of devices also demonstrated significant efficacy over Lateral Push, Lateral Pull, and Mono/Twin Block categories of devices. A subjective observation is that both categories share some similar, and potentially relevant, design characteristics relative to the other categories. Both categories of devices achieve precision mandibular repositioning and mandibular stabilization in the prescribed location to prevent airway collapse. And both have designs that promote mouth closure, a characteristic previously associated with improved efficacy [29].
Limitations
There are several limitations for this review article. The main limitations involve the inability to conduct post hoc analyses for variables that could significantly impact efficacy values. For example, it is thought that baseline OSA severity, starting mandibular positions and sleep testing thresholds, can have a significant impact on efficacy values. However, only a handful of the source documents for this systemic review measure and disclose data for these key variables. This limits the ability to conduct post hoc analyses to understand the significant of these variables with respect to this investigation. Another limitation, which is somewhat endemic for review articles, is the general variability in study methods. These articles contain protocol variabilities, or are silent on protocols, with respect to: baseline testing, follow up testing, mandibular positioning protocols, device selection rationale, device titration protocols, patient anthropomorphic and disease severity profiles, and more. These differences could translate into biases. However as previously mentioned, the sporadic disclosure of these variables across the source papers limits the ability to control for these factors in post hoc analyses.
One way to address these limitations is to design a prospective randomized clinical trial that interrogates the findings from this review.
Conclusions
OAT is an effective treatment for Obstructive Sleep Apnea. However, the specific mechanical design of an OAT device can have a meaningful impact on efficacy. This review finds a greater than 30% point difference between the most (Precision Post) and least (Lateral Push) efficacious OAT device design categories.
Healthcare providers should consider OAT device design when selecting, prescribing, delivering and managing patients with OSA. This review also suggests that relevant medical guidelines should go beyond the basic distinction between custom and non-custom OAT device designs.
References
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Anandam, A.; Patil, M.; Akinnusi, M.; Jaoude, P.; El-Solh, A.A. Cardiovascular mortality in obstructive sleep apnoea treated with continuous positive airway pressure or oral appliance: An observational study. Respirology 2013, 18, 1184–1190. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of obstructive sleep apnea: A population health perspective. Am J Respir Crit Care Med. 2 0021, 165, 1217–1239. [Google Scholar] [CrossRef]
- Patel, S.R.; Bakker, J.P.; Stitt, C.J.; Aloia, M.S.; Nouraie, S.M. Age and Sex Disparities in Adherence to CPAP. Chest 2021, 159, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Pépin, J.L.; Woehrle, H.; Liu, D.; et al. Adherence to Positive Airway Therapy After Switching From CPAP to ASV: A Big Data Analysis. J Clin Sleep Med. 2018, 15, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Peker, Y.; Celik, Y.; Behboudi, A.; et al. CPAP may promote an endothelial inflammatory milieu in sleep apnoea after coronary revascularization. EBioMedicine 2024, 101, 105015. [Google Scholar] [CrossRef] [PubMed]
- Recalled Philips Ventilators, BiPAP Machines, and CPAP Machines. Available online: https://www.fda.gov/medical-devices/respiratory-devices/recalled-philips-ventilators-bipap-machines-and-cpap-machines (accessed on 11 November 2024).
- Hidden Health Crisis Costing America Billions. Available online: https://aasm.org/wp-content/uploads/2017/10/sleep-apnea-economic-crisis.pdf (accessed on 11 November 2024).
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J Clin Sleep Med. 2015, 15, 773–827. [Google Scholar] [CrossRef]
- Phillips, C.L.; Grunstein, R.R.; Darendeliler, M.A.; et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: A randomized controlled trial. Am J Respir Crit Care Med. 2013, 15, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Ou, Y.H.; Colpani, J.T.; Cheong, C.S.; et al. Mandibular Advancement vs CPAP for Blood Pressure Reduction in Patients With Obstructive Sleep Apnea. J Am Coll Cardiol. 2024, 7, 1760–1772. [Google Scholar] [CrossRef]
- Trzepizur, W.; Cistulli, P.A.; Glos, M.; et al. Health outcomes of continuous positive airway pressure versus mandibular advancement device for the treatment of severe obstructive sleep apnea: An individual participant data meta-analysis. Sleep 2021, 9, 015. [Google Scholar] [CrossRef]
- Obstructive and Central Sleep Apnea Treatment. Available online: https://www.uhcprovider.com/content/dam/provider/docs/public/policies/comm-medical-drug/obstructive-sleep-apnea-treat (accessed on 11 November 2024).
- Oral Appliances for Obstructive Sleep Apnea - Policy Article. Available online: https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleId=52512 (accessed on 11 November 2024).
- Ucak, S.; Dissanayake, H.U.; Sutherland, K.; Bin, Y.S.; de Chazal, P.; Cistulli, P.A. Effect of mandibular advancement splint therapy on cardiac autonomic function in obstructive sleep apnoea. Sleep Breath. 2024, 28, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.; McEvoy, R.D.; Banks, S.; Tarquinio, N.; Murray, C.G.; Vowles, N.; Pierce, R.J. Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med. 2004, 15, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Dieltjens, M.; Vanderveken, O.M.; Shivalkar, B.; et al. Mandibular advancement device treatment and reverse left ventricular hypertrophic remodeling in patients with obstructive sleep apnea. J Clin Sleep Med. 2 0221, 18, 903–909. [Google Scholar] [CrossRef]
- Vanderveken, O.M. ; Gagnadoux F: Comparative outcomes in obstructive sleep apnea therapy: Mean disease alleviation as a more appropriate measure-it’s about time. Sleep 2023, 11, 210. [Google Scholar] [CrossRef] [PubMed]
- Vanderveken, O.M.; Dieltjens, M.; Wouters, K.; De Backer, W.A.; Van de Heyning, P.H.; Braem, M.J. Objective measurement of compliance during oral appliance therapy for sleep-disordered breathing. Thorax 2013, 68, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Scherr, S.C.; Dort, L.C.; Almeida, F.R.; et al. Definition of an effective oral appliance for the treatment of obstructive sleep apnea and snoring: A report of the American Academy of Dental Sleep Medicine. Journal of Dental Sleep Medicine. 2014, 1, 39–50. [Google Scholar] [CrossRef]
- Verbraecken, J.; Dieltjens, M.; Op de Beeck, S.; Vroegop, A.; Braem, M.; Vanderveken, O. ; Randerath W: Non-CPAP therapy for obstructive sleep apnoea. Breathe 2022, 18, 220164–10. [Google Scholar] [CrossRef] [PubMed]
- Vanderveken, O.M.; Van Daele, M.; Verbraecken, J.; Braem, M.J. ; Dieltjens M: Comparative analysis of two custom-made mandibular advancement devices with varied designs for treating moderate to severe obstructive sleep apnea. Sleep Med. 2024, 117, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, I.H.; Cistulli, P.A.; Jahrami, H.; Alamoud, K.A.; Saeed, M.; Soulimiotis, A.P.; BaHammam, A.S. Comparative efficacy of mandibular advancement devices in obstructive sleep apnea: A network meta-analysis. Sleep Breath. 2023, 27, 1365–1381. [Google Scholar] [CrossRef] [PubMed]
- Uniken Venema, J.A.M.; Rosenmöller, B.R.A.M.; de Vries, N.; de Lange, J.; Aarab, G.; Lobbezoo, F.; Hoekema, A. Mandibular advancement device design: A systematic review on outcomes in obstructive sleep apnea treatment. Sleep Med Rev. 2021, 60, 101557–10. [Google Scholar] [CrossRef]
- Charkhandeh, S.; Mosca, E.; Remmers, J. Precision vs. traditional oral appliance therapy: A comparison of efficacy. ERJ Open Research 2023, 9, 37. [Google Scholar] [CrossRef]
- Cai, Y.; Tripuraneni, P.; Gulati, A.; Stephens, E.M.; Nguyen, D.K.; Durr, M.L.; Chang, J.L. Patient-Defined Goals for Obstructive Sleep Apnea Treatment. Otolaryngol Head Neck Surg. 2022, 167, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Sher, A.E.; Schechtman, K.B.; Piccirillo, J.F. The efficacy of surgical modifications of the upper airway in adults with obstructive sleep apnea syndrome. Sleep 1996, 19, 156–177. [Google Scholar] [CrossRef] [PubMed]
- Azarbarzin, A.; Sands, S.A.; Stone, K.L.; et al. The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: The Osteoporotic Fractures in Men Study and the Sleep Heart Health Study. Eur Heart J. 2019, 7, 1149–1157. [Google Scholar] [CrossRef] [PubMed]
- Labarca, G.; Sands, S.A.; Cohn, V.; et al. Mouth Closing to Improve the Efficacy of Mandibular Advancement Devices in Sleep Apnea. Ann Am Thorac Soc. 2022, 19, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



