Submitted:
17 December 2024
Posted:
18 December 2024
Read the latest preprint version here
Abstract
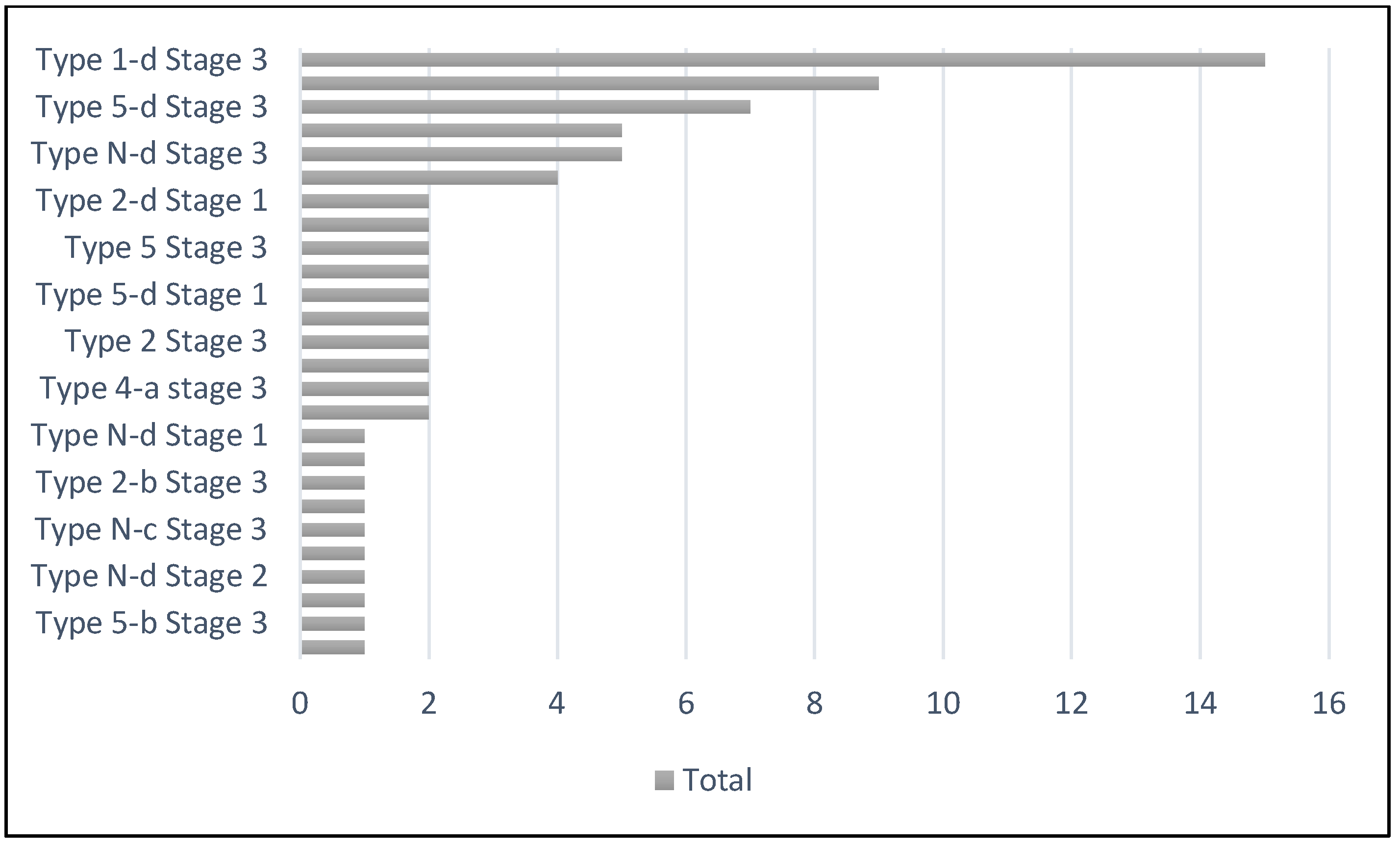
Background/Objectives: Charcot Neuroarthropathy (CN) is the sequelae of longstanding poorly controlled diabetes. This has been detrimental with subsequent cause to the increased amputations and mortality. The lack of early identification and referral for specialized management of these condition had tremendously uplifted the financial burden to the healthcare system worldwide. There are a few recognized classifications; Eichenholtz, Brodsky, Sanders and Frykberg classification systems, that has been useful in the use of Charcot foot management. There is no currently available classification system for ankle CN. The aim of this article is to institute a new classification system for ankle CN – M-CAN. This classification includes the pattern of deformity, amount of bone loss, status of infection and ulceration, glycaemic controls and pe-dal perfusion status. Methods: A 10-years pool, retrospective review of diabetic CN patients with ankle de-formity, under the care of Manchester University NHS Foundation Trust (MFT). Clinical and radiographical assessment was analyzed and an ankle CN classification was constructed, incorporating the Eichenholtz stage at which the patient obtained the treatment. Results: A total of 75 CN ankle were identified and the coronal and sagittal planes of deformity was reviewed. The osseous loss was well documented along with the planes of deformity. The presence of cutaneous break and status of infection were also identified. As a result, large number of the patients were classified as Type 1-d Stage 3. This elaborates into varus ankle with com-bined 2 different articulating joint bone loss. Conclusions: This new classification system for ankle CN, would be of substantial benefit in providing an understanding of the deformity patterns and for descriptive purposes. It enables the condition to be easily grouped in accordance with the acquired deformities and os-seous loss. This would help the treating surgeon or practitioners to perceive a better understanding of the disease progress and plan ahead for the further management.
Keywords:
1. Introduction
2. Materials and Methods
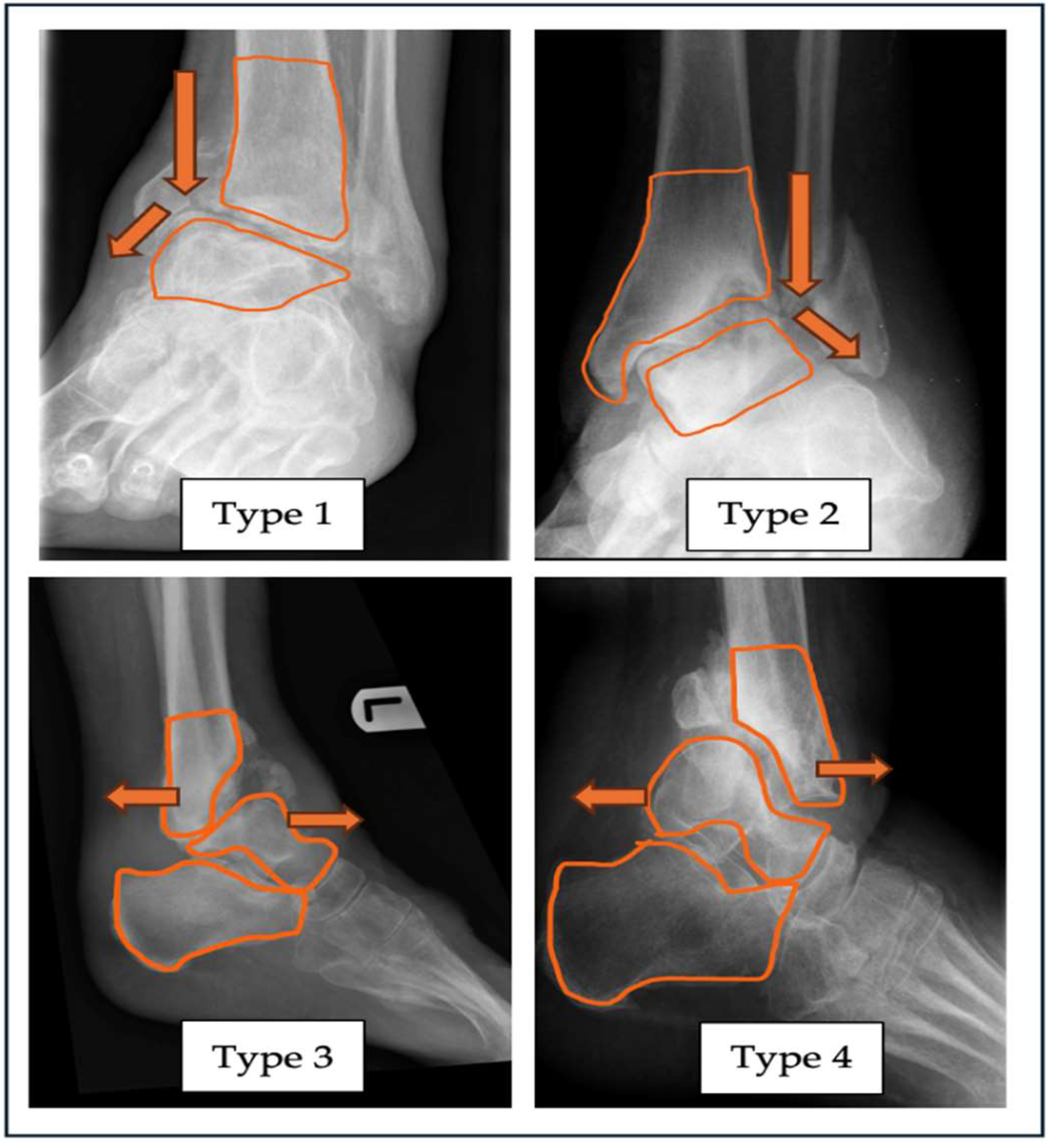

| “A” - Alignment | Varus (Type 1) |
Valgus (Type 2) |
Anterior (Type 3) |
Posterior (Type 4) |
| Neutral – label as Type N Combined Label as Type 5 |
||||
| Dislocation Yes / No | ||||
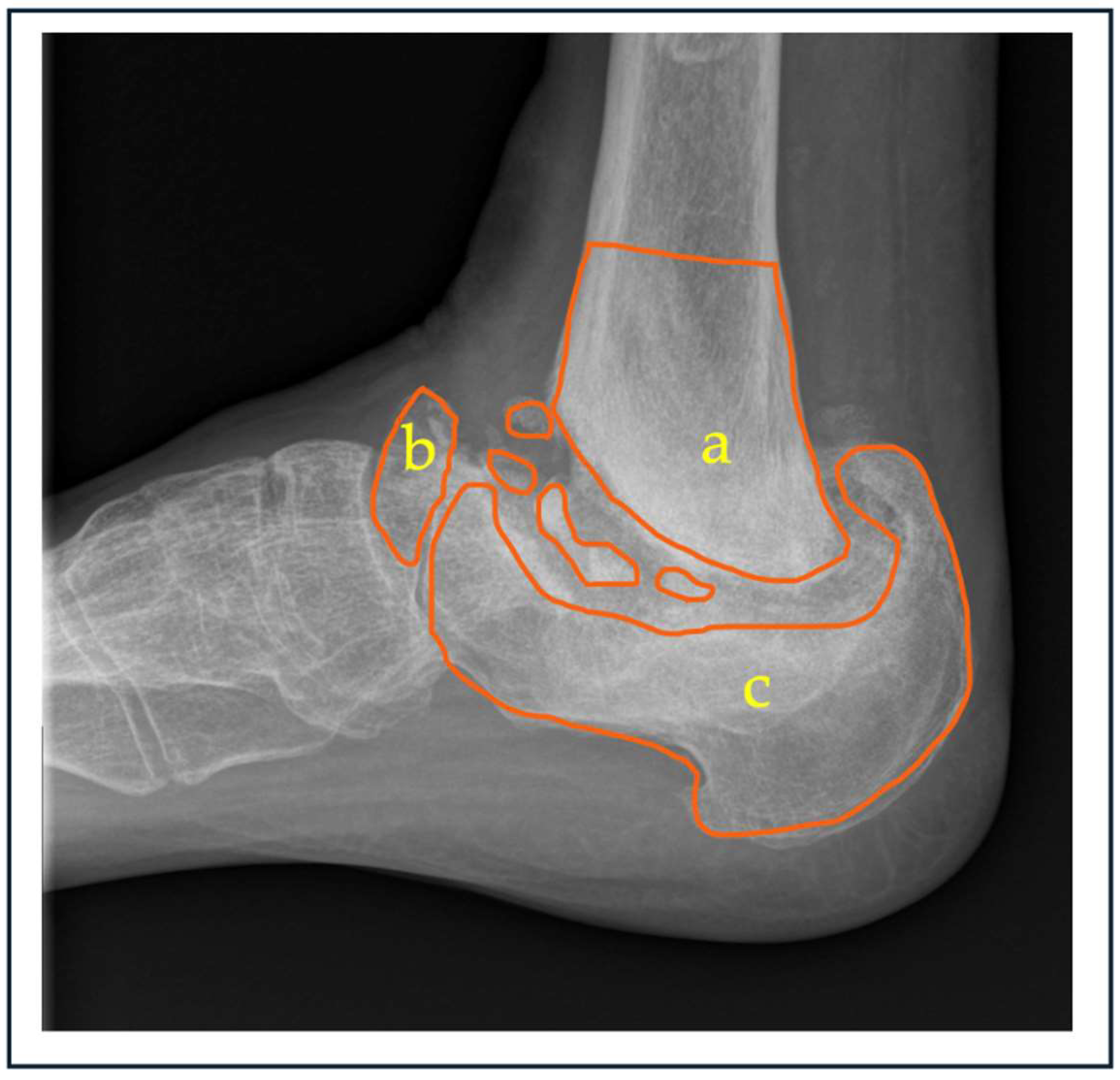
| “B” - Bone loss | Tibia (Subtype a) |
Talus (Subtype b) |
Calcaneum (Subtype c) | Combined (Subtype d) |
| Can further grade the bone loss based on severity – Mild / Moderate / Severe | ||||
| *Leave it unlabelled if there are no bone loss present | ||||
| “C” - Cutaneous condition |
Ulcerated | Non-ulcerated | ||
| Infected | ||||
| Non-Infected | ||||
| “D” – Diabetic Control |
HbA1c < 53 mmmol/L (7.0%) | HbA1c > 53mmmol/L (7.0%) |
||
| NICE guidelines UK 2015 | ||||
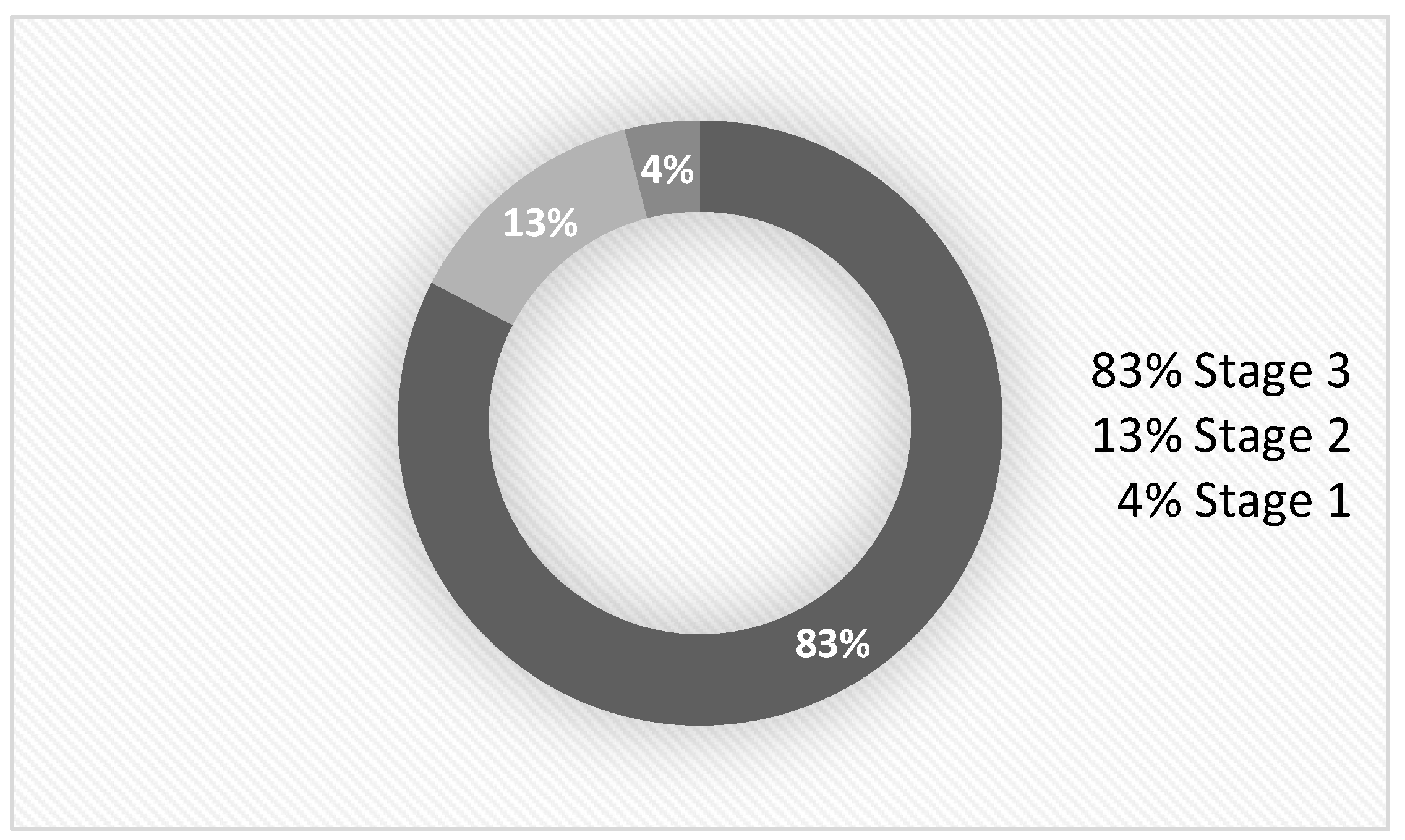
| “E”- Eichenholtz Stage |
Stage 0 Prodromal |
Stage 1 Destruction |
Stage 2 Coalescence |
Stage 3 Consolidation |
| “F”–Foot Perfusion (Pulse/Doppler) *Toe pressure can be used as alternative |
Monophasic (PM) |
Diaphasic (PD) |
Triphasic (PT) |
|
3. Results
| Count of Tibia bone loss | Count of Talus bone loss | ||
| Yes | 49 | 51 | |
| Nil | 26 | 24 | |
| Grand Total | 75 | 75 | |
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- K. A. Cole and D. C. Jupiter, “Charcot neuroarthropathy in diabetic patients in Texas,” Prim Care Diabetes, Oct. 2024. [CrossRef]
- A. Marshall, C. Meyer, M. Hurst, H. Hughes, and P. Burns, “Prevalence of Ankle Charcot Neuroarthropathy Presenting in a Tertiary Care Center,” Journal of Foot and Ankle Surgery, vol. 63, no. 1, pp. 114–118, Jan. 2024. [CrossRef]
- L. Metcalf et al., “Prevalence of active Charcot disease in the East Midlands of England,” Diabetic Medicine, vol. 35, no. 10, pp. 1371–1374, Oct. 2018. [CrossRef]
- A. A. Najefi, R. Brown, and C. Loizou, “Classification and management of the midfoot Charcot diabetic foot,” Orthop Trauma, vol. 37, no. 1, pp. 49–55, Feb. 2023. [CrossRef]
- F. B. Ergen, S. E. Sanverdi, and A. Oznur, “Charcot foot in diabetes and an update on imaging,” Nov. 20, 2013. [CrossRef]
- V. B. Bregovskiy, S. A. Osnach, V. N. Obolenskiy, A. G. Demina, A. L. Rybinskaya, and V. G. Protsko, “CLASSIFICATION OF THE CHARCOT NEUROOSTEOARTHROPATHY: EVOLUTION OF VIEWS AND UNSOLVED PROBLEMS,” Jul. 01, 2024, Russian Association of Endocrinologists. [CrossRef]
- A. B. Rosskopf, C. Loupatatzis, C. W. A. Pfirrmann, T. Böni, and M. C. Berli, “The Charcot foot: a pictorial review,” Dec. 01, 2019, Springer Verlag. [CrossRef]
- L. C. Schon, S. B. Weinfeld, G. A. Horton, and S. Resch, “Radiographic and Clinical Classification of Acquired Midtarsus Deformities,” 1998.
- L. C. Schon et al., “The Acquired Midtarsus Deformity Classification System-Interobserver Reliability and Intraobserver Reproducibility,” 2002.
- E. Gouveri, “Charcot osteoarthropathy in diabetes: A brief review with an emphasis on clinical practice,” World J Diabetes, vol. 2, no. 5, p. 59, 2011. [CrossRef]
- E. Galhoum et al., “Management of ankle charcot neuroarthropathy: A systematic review,” Dec. 01, 2021, MDPI. [CrossRef]
- K. Kupai, H. L. Kang, A. Pósa, Á. Csonka, T. Várkonyi, and Z. Valkusz, “Bone Loss in Diabetes Mellitus: Diaporosis,” Jul. 01, 2024, Multidisciplinary Digital Publishing Institute (MDPI). [CrossRef]
- D. E. Attarian, H. J. McCrackin, D. P. DeVito, J. H. McElhaney, and W. E. Garrett, “Biomechanical Characteristics of Human Ankle Ligaments,” 1985.
- Z. J. Tsegai et al., “Trabecular and cortical bone structure of the talus and distal tibia in Pan and Homo,” Am J Phys Anthropol, vol. 163, no. 4, pp. 784–805, Aug. 2017. [CrossRef]
- E. Pires, C. Lôbo, C. De Cesar Netto, and A. Godoy-Santos, “Hindfoot alignment using weight-bearing computed tomography,” Journal of the Foot & Ankle, vol. 14, no. 3, pp. 239–242, Dec. 2020. [CrossRef]
- C. J. Verdin, G. G. Botek, J. D. Miller, J. D. Kingsley, and D. Plyler, “Association of Anatomical Location of Neuroarthropathic (Charcot’s) Destruction with Age-and Sex-Matched Bone Mineral Density Reduction,” J Am Podiatr Med Assoc, vol. 114, no. 1, Jan. 2024. [CrossRef]
- Andrea B.Rosskopf, Christos Loupatatzis, Christian W. A. Pfirrmann, Thomas Boni, and martin C. Berli, “The Charcot foot: a pictorial review | Enhanced Reader,” Insights Imaging, no. 77, Aug. 2019. [CrossRef]
- J. P. O’Hare et al., “The new NICE guidelines for type 2 diabetes - a critical analysis,” 2015, ABCD (Diabetes Care) Ltd. [CrossRef]
- J. X. Shumin, W. Yang, H. Lei, X. Shanshan, and Z. Z. Tang, “Reasonable Glycemic Control Would Help Wound Healing During the Treatment of Diabetic Foot Ulcers,” Diabetes Therapy, vol. 10. [CrossRef]
- A. M. Müller et al., “Significant prevalence of peripheral artery disease in patients with disturbed wound healing following elective foot and ankle surgery: Results from the ABI-PRIORY (ABI as a PRedictor of Impaired wound healing after ORthopedic surgerY) trial,” Vascular Medicine (United Kingdom), vol. 25, no. 2, pp. 118–123, Apr. 2020. [CrossRef]
- D. K. Wukich, K. M. Raspovic, and N. C. Suder, “Prevalence of Peripheral Arterial Disease in Patients With Diabetic Charcot Neuroarthropathy,” Journal of Foot and Ankle Surgery, vol. 55, no. 4, pp. 727–731, Jul. 2016. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



