Submitted:
13 December 2024
Posted:
13 December 2024
You are already at the latest version
Abstract
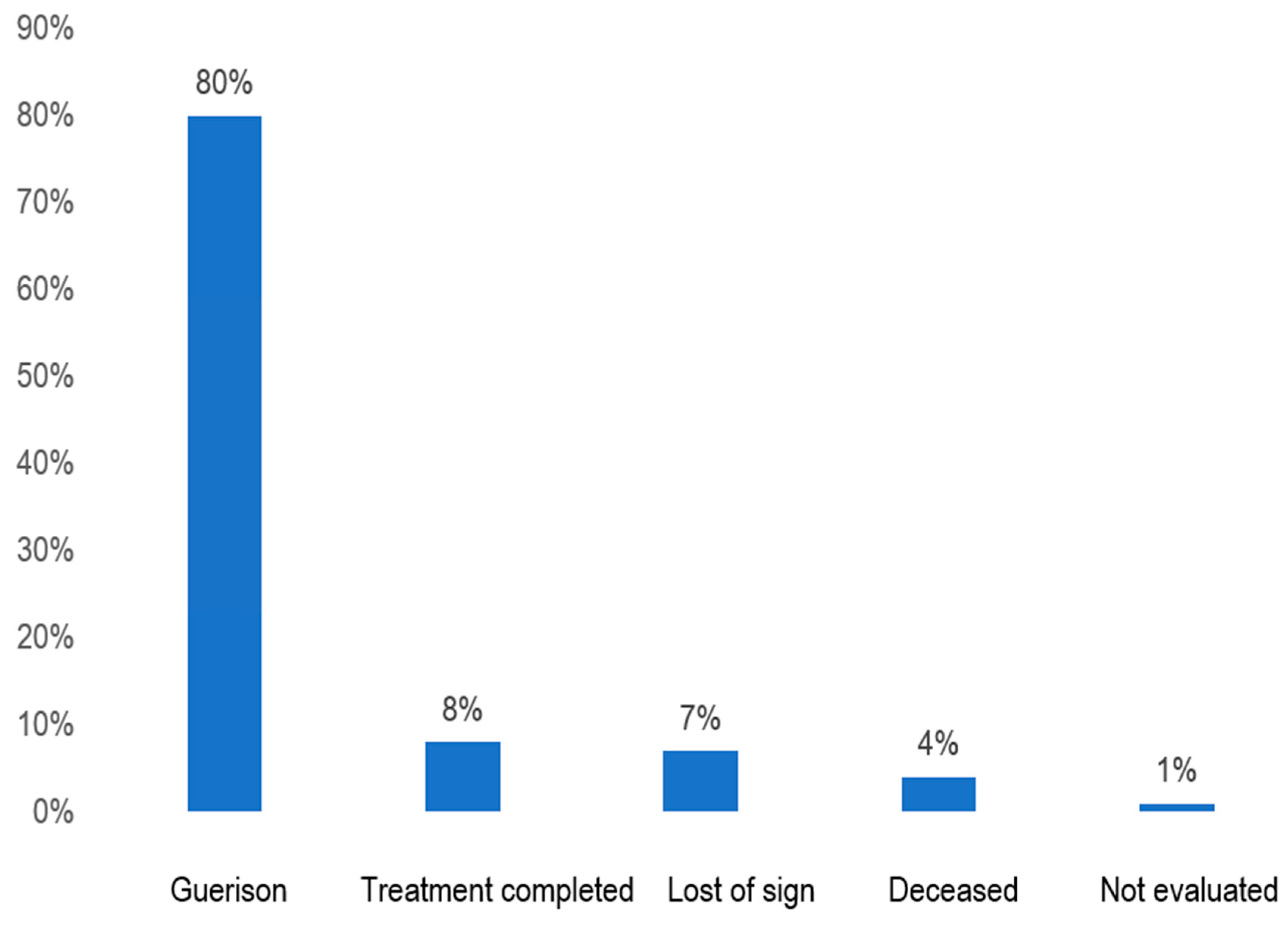
Introduction: Evaluating the quality of patient care is a key indicator of the effectiveness of a health system. In the context of tuberculosis, such an evaluation appears necessary and timely in one of the specialized centers for tuberculosis patient care to assess its impact on achieving the targets of a health program, such as the tuberculosis control program. Objective: To assess the quality of care provided to tuberculosis patients at the Anti-Tuberculosis Center in Brazzaville. Method: A de-scriptive study conducted over six months using a questionnaire administered to tuberculosis pa-tients receiving follow-up during the study period. Results: A total of 139 tuberculosis patients were interviewed, including 75 women (54%) and 64 men (46%). The mean age was 36.7 ± 16.82 years (range: 17–76 years). Most patients were married (56.1%), lived in Brazzaville (95%), and had a secondary education level (49%). The reception was poorly rated in 72% of cases at the administrative level and 65% at the care level, including the lack of respect for privacy (99%). Patients were informed about their disease (87%), and the information provided was clear (73%). However, the reception quality was rated as poor (83%), although administrative procedures were easy. The waiting time for consultations and care was relatively long in 73% and moderately long in 84% of cases, respectively. The waiting conditions were deemed very poor in 90% of cases, and cleanliness was insufficient in 85%. The consultation duration was considered adequate in 90% of cases. The level of patient sat-isfaction was rated as insufficient in 48.2% of cases. Therapeutic success was achieved in 88% of cases, while 7% of patients were lost to follow-up, and 4% died. Conclusion: The quality of care for tu-berculosis patients at the Anti-Tuberculosis Center in Brazzaville should be improved by prioritizing patient-centered care.
Keywords:
1. Introduction
2. Methods
2.1. Study Setting, Nature, Population, and Period
2.2. Inclusion and Exclusion Criteria
2.3. Sampling Methods and Techniques
2.4. Study Variables
2.5. Scoring Procedure
2.6. Organization of Data Collection
2.7. Data Processing and Analysis
2.8. Ethical Considerations
3. Results

| Male | Female | Total | ||||
|---|---|---|---|---|---|---|
| N=64 | N=75 | |||||
| n | % | n | % | n | % | |
| Marital status | ||||||
| Bachelor | 23 | 35.9 | 28 | 37.3 | 51 | 36.7 |
| Married | 40 | 62.5 | 38 | 50.7 | 78 | 56.1 |
| Divorce | 0 | 0.0 | 2 | 2.7 | 2 | 1.4 |
| Widower | 0 | 0 | 7 | 9.3 | 7 | 5.1 |
| Free union | 1 | 1.6 | 0 | 0.0 | 1 | 0.7 |
| Origin | ||||||
| Brazzaville | 62 | 96.9 | 70 | 93.3 | 132 | 95.0 |
| Other city | 2 | 3.1 | 5 | 6.7 | 7 | 5.0 |
| Level of study | ||||||
| Not in school | 1 | 1.6 | 0 | 0.0 | 1 | 0.7 |
| Primary | 3 | 4.7 | 7 | 9.3 | 10 | 7.2 |
| Secondary | 28 | 43.7 | 40 | 53.3 | 68 | 49.0 |
| Superior | 32 | 50.0 | 28 | 37.4 | 60 | 43.1 |
| Male N=64 |
Female N=75 |
Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Level of satisfaction | ||||||
| Very satisfactory | 6 | 9.4 | 12 | 16.0 | 18 | 12.9 |
| Satisfying | 10 | 15.6 | 9 | 12.0 | 19 | 13.7 |
| Insufficient | 27 | 42.2 | 40 | 53.3 | 67 | 48.2 |
| Very bad | 15 | 23.4 | 8 | 10.7 | 23 | 16.5 |
| Rather not | 1 | 1.6 | 6 | 8.0 | 7 | 5.1 |
| No way | 5 | 7.8 | 0 | 0.0 | 5 | 3.6 |
4. Discussion
Sociodemographic Characteristics
Age and Gender
Marital Status
Residence
Assessment of Reception, Privacy, and Quality of Information Received
Quality of the relationship between healthcare staff and patients
Quality of services at the anti-tuberculosis center in Brazzaville
Patient satisfaction level
Infrastructure of the anti-tuberculosis center in Brazzaville
5. Conclusions
References
- Gregory, D.; Kennedy Sarah, E.; Tevis Kent, C. Is there a relationship between patient satisfaction and favorable outcomes? Ann Surg 2014, 260, 592–600. [Google Scholar]
- Rachid, A.; Amina, A.B. Patient satisfaction as a tool towards quality improvement. Oman Medical journal 2014, 29, 3–7. [Google Scholar]
- Beattie, M.; Douglas, J.M.; Artherton, L.; Lauder, W. Instrument to measure patient satisfaction experience of health care quality in hospital: a systemic review Biomed Central. 2015, 4, 97. [Google Scholar]
- Varkevisser, C.M. Designing and conducting health systems research projets: Proposal. KIT Publishers,2003,195 pages.
- Bitchong, C.; Massongo, M.; Palai, Y. Devenir des patients traités pour tuberculose diagnostiquée cliniquement à l’hôpital Jamot-de-Yaoundé. Rev Mal Respir 2018, 35, A182. [Google Scholar] [CrossRef]
- Anniche H, Zaghba N, Benjelloun H, et al. La tuberculose multifocale chez l’immunocompétent. Rev Mal Respir 2022, 14, 268–269. [Google Scholar]
- Okemba-Okombi, F.H.; Ossibi Ibara, B.R.; Bopaka, R.G. État des lieux des patients tuberculeux perdus de vue à Brazzaville. Rev Mal Respir 2019, 36, A129. [Google Scholar] [CrossRef]
- Congo-taux d’alphabétisation des adultes (+ 15ans). Congo Taux d'alphabétisation des adultes, 1960-2022 - knoema.
- Yamba Yamba, M.K.; Mashinda, D.K.; Kayembe NJ, C.; Onyambokol, M.A.; Nyandwe, J.K. Evaluation de la qualité des soins aux cliniques universitaire de Kinshasa : Etude de satisfaction des patients hospitalisés. Ann.Afr. Med 2018, 11, 2926–2935. [Google Scholar]
- Haute Autorité de Santé, Satisfaction des patients hospitalisés & résultats 2016 qualité et sécurité des soins dans les hôpitaux et cliniques en France, Dossier de Presse 15 Décembre 2016. www.hassante.fr/portail/upload/docs/application/pdf/2016-12 Consulté le 28 Décembre 2016.
- Soufi, G.; Belayachi, J.; Salma, H.; Samir, H.; Zekraoui, A.; Abouqal, A. Patient satisfaction in an acute medicine department in Morocco. BMC Health Services Research 2010, 10, 149. [Google Scholar] [CrossRef]
- Mendoza Aldana Jorge, Piechulek Helga, Al-Sabir Ahmed. Satisfaction des patients et qualité des soins dans la zone rurale du Bangladesh. Bulletin of the World Heath Organisation, 2001, 79, 512–517. [Google Scholar]
- Margot, P. Qualité et continuité des soins. In : la personne au cœur du processus de soins : qualité et continuité. Coimbra, Portugal. 2005, 23.
- Al-Sabir, A. Evaluation of FWVs skills as MCH-FP services providers in Bangladesh. Dhaka (Bangladesh), National Institute of Population Research and Training, 1995.
- Kamal, GM; et al. The quality of NORPLANT services in Bangladesh. Dhaka (Bangladesh), Associates for Community and Population Research (ACPR), 1991.
- Brian, w. Patient satisfaction: a valid concept? Social Science and Medicine. 1994, 38, 509–516. [Google Scholar]
- Sitzia, J.; Wood, N. Patient satisfaction: a review of issues and concepts. Soc Sci Med. 1997, 45, 1829–43. [Google Scholar] [CrossRef]
- Daix A T J, Bakayoko A S, Coulibaly G, Samake K, Kone Z, Coulibaly T N, Diakité A, Pitta M, Kouasi F, Kouame A, Kouakou A O, Kouakou J, Domoua K. Effet de la guerre sur le contrôle de la tuberculose en Côte d’Ivoire de 2002 à 2007.Rev Pneumol Clin 2013, 69, 237–243.
- Mjid, M.; Cherif, J.; Ben Salah, N.; Toujani, S.; Ouahchi, Y.; Zakhama, H.; Louzir, B.; Mehiri-Ben Rhouma, N.; Beji, M. Epidémiologie de la tuberculose. Rev Pneumol Clin 2015, 71, 67–72. [Google Scholar] [CrossRef] [PubMed]
| Male N=64 |
Female N=75 |
Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Welcome at the entrance of the CAT | ||||||
| Excellent | 1 | 1.6 | 3 | 4.0 | 4 | 2.9 |
| Very good | 6 | 9.4 | 4 | 5.3 | 10 | 7.2 |
| Good | 10 | 15.6 | 15 | 20.0 | 25 | 18.0 |
| Bad | 28 | 43.7 | 40 | 53.3 | 68 | 48.9 |
| Very bad | 19 | 29.7 | 13 | 17.4 | 32 | 23.0 |
| Reception by care services | ||||||
| Excellent | 6 | 9.4 | 10 | 13.3 | 16 | 11.5 |
| Very good | 8 | 12.5 | 6 | 8.0 | 14 | 10.1 |
| Good | 8 | 12.5 | 11 | 14.7 | 19 | 13.7 |
| Bad | 30 | 46.9 | 25 | 33.3 | 55 | 39.5 |
| Very bad | 12 | 18.7 | 23 | 30.7 | 35 | 25.2 |
| Respect for privacy | ||||||
| Excellent | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Very good | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Good | 2 | 3.1 | 0 | 0.0 | 2 | 1.4 |
| Bad | 35 | 54.7 | 50 | 66.7 | 85 | 61.2 |
| Very bad | 27 | 42.2 | 25 | 33.3 | 52 | 37.4 |
| Information about the disease | ||||||
| Always | 30 | 46.9 | 36 | 48.0 | 66 | 47.5 |
| Almost always | 25 | 39.0 | 30 | 40.0 | 55 | 39.6 |
| Often | 1 | 1.6 | 0 | 0.0 | 1 | 0.7 |
| Sometimes | 2 | 3.1 | 0 | 0.0 | 2 | 1.4 |
| Very rarely or never | 6 | 9.4 | 9 | 12.0 | 15 | 10.8 |
| Clarity of information received | ||||||
| Always | 27 | 42.2 | 10 | 13.3 | 37 | 26.6 |
| Almost always | 32 | 50.0 | 32 | 42.7 | 64 | 46.0 |
| Often | 5 | 7.8 | 3 | 4.0 | 8 | 5.8 |
| Sometimes | 0 | 0.0 | 22 | 29.3 | 22 | 15.8 |
| Very rarely or never | 0 | 0.0 | 8 | 10.7 | 8 | 5.8 |
| Male N=64 |
Female N=75 |
Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Annoying remarks from the doctor | ||||||
| Very often | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Quite often | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Sometimes | 4 | 6.2 | 2 | 2.7 | 6 | 4.3 |
| Very rarely | 20 | 31.3 | 23 | 30.7 | 43 | 31.0 |
| Never | 40 | 62.5 | 50 | 66.6 | 90 | 64.7 |
| Annoying remarks from the lab technician | ||||||
| Very often | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Quite often | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Sometimes | 1 | 1.6 | 0 | 0.0 | 1 | 0.7 |
| Very rarely | 30 | 46.9 | 45 | 60.0 | 75 | 54.0 |
| Never | 33 | 51.5 | 30 | 40.0 | 63 | 45.3 |
| Politeness of staff | ||||||
| Very often | 57 | 89.1 | 71 | 94.7 | 128 | 92.1 |
| Quite often | 5 | 7.8 | 0 | 0.0 | 5 | 3.6 |
| Sometimes | 2 | 3.1 | 0 | 0.0 | 2 | 1.4 |
| Very rarely | 0 | 0.0 | 4 | 5.3 | 4 | 2.9 |
| Never | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Help with daily living activities | ||||||
| Always | 30 | 46.9 | 41 | 54.7 | 71 | 51.1 |
| Almost always | 20 | 31.2 | 15 | 20.0 | 35 | 25.1 |
| Often got the help needed | 8 | 12.5 | 6 | 8.0 | 14 | 10.1 |
| Sometimes | 5 | 7.8 | 9 | 12.0 | 14 | 10.1 |
| Very rarely or never | 1 | 1.6 | 4 | 5.3 | 5 | 3.6 |
| Explanation of the disease | ||||||
| Yes | 64 | 100.0 | 75 | 100.0 | 139 | 100.0 |
| No | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Explanation of anti-tuberculosis treatment | ||||||
| Yes | 64 | 100.0 | 75 | 100.0 | 139 | 100.0 |
| No | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Explanation of the tests to be carried out for monitoring | ||||||
| Yes | 56 | 87.5 | 70 | 93.3 | 126 | 90.6 |
| No | 8 | 12.5 | 5 | 6.7 | 13 | 9.4 |
| Male N=64 |
Female N=75 |
Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Annoying remarks from the doctor | ||||||
| Very often | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Quite often | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Sometimes | 4 | 6.2 | 2 | 2.7 | 6 | 4.3 |
| Very rarely | 20 | 31.3 | 23 | 30.7 | 43 | 31.0 |
| Never | 40 | 62.5 | 50 | 66.6 | 90 | 64.7 |
| Annoying remarks from the lab technician | ||||||
| Very often | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Quite often | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Sometimes | 1 | 1.6 | 0 | 0.0 | 1 | 0.7 |
| Very rarely | 30 | 46.9 | 45 | 60.0 | 75 | 54.0 |
| Never | 33 | 51.5 | 30 | 40.0 | 63 | 45.3 |
| Politeness of staff | ||||||
| Very often | 57 | 89.1 | 71 | 94.7 | 128 | 92.1 |
| Quite often | 5 | 7.8 | 0 | 0.0 | 5 | 3.6 |
| Sometimes | 2 | 3.1 | 0 | 0.0 | 2 | 1.4 |
| Very rarely | 0 | 0.0 | 4 | 5.3 | 4 | 2.9 |
| Never | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Help with daily living activities | ||||||
| Always | 30 | 46.9 | 41 | 54.7 | 71 | 51.1 |
| Almost always | 20 | 31.2 | 15 | 20.0 | 35 | 25.1 |
| Often got the help needed | 8 | 12.5 | 6 | 8.0 | 14 | 10.1 |
| Sometimes | 5 | 7.8 | 9 | 12.0 | 14 | 10.1 |
| Very rarely or never | 1 | 1.6 | 4 | 5.3 | 5 | 3.6 |
| Explanation of the disease | ||||||
| Yes | 64 | 100.0 | 75 | 100.0 | 139 | 100.0 |
| No | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Explanation of anti-tuberculosis treatment | ||||||
| Yes | 64 | 100.0 | 75 | 100.0 | 139 | 100.0 |
| No | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Explanation of the tests to be carried out for monitoring | ||||||
| Yes | 56 | 87.5 | 70 | 93.3 | 126 | 90.6 |
| No | 8 | 12.5 | 5 | 6.7 | 13 | 9.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



