Submitted:
11 December 2024
Posted:
13 December 2024
Read the latest preprint version here
Abstract
Introduction: Surgical mesh is the standard for hernia repair, however, suture fixation can cause chronic pain and tissue irritation. Alternative atraumatic fixations using fibrin or cyanoacrylate glue, have some limitations. This study presents the feasibility of using new, UV-curable biodegradable PhotoBioCure biomaterial for anastomosis of surgical mesh incisions in treating inguinal hernia, concentrating on short- and long-term outcomes.Materials and Methods: Five men (aged 20-40 years) with unilateral inguinal hernias participated in the study. The mesh was fixed with PhotoBioCure biomaterial, which was UV-cured in 3 minutes. Follow-up lasted 24 months, with regular clinical supervision including ultrasonography, thermal imaging, and assessment of VAS, CCS, EuraHS QoL, and SF-36.Results: Using PhotoBioCure reduced surgical time compared to suture fixation. VAS pain scores decreased from 2.6 (± 0.55) on the first day after surgery to 0.8 (± 0.84) after 8 days, with complete pain resolution after 6 weeks. The Carolinas Comfort Scale showed a gradual decline in foreign body sensation, from 54.08% on the first day post-surgery to 30.38% after 6 weeks. No recurrence or complications, like hematomas or infections, occurred over 24 months. Patients reported improved quality of life, with SF-36 questionnaire scores increasing from 77.8 pre-surgery to 92.4 after 24 months.Conclusions: PhotoBioCure is an innovative biomaterial for effective and efficient anastomosis of surgical mesh incisions in inguinal hernia repair, reducing procedure duration and surgical complexity without increasing the risk of post-operative complications.
Keywords:
herniorrhaphy
; surgical meshes
; UV-activated biomaterial
; mesh fixation
1. Introduction
Synthetic meshes (polyester, polypropylene) are considered the gold standard in hernia repair. Prosthetic meshes are fixed with different methods to prevent their dislocation, and thus hernia recurrence, as well as ensure effective mesh integration with surrounding tissues [1]. Mesh and the sutures used do not cause chronic pain and sensation, and for this reason they are the gold standard in the treatment of hernias, but like any foreign body they can cause occasional tissue reactions. For this reason, it is reasonable to look for surgical methods or polymers that can reduce these complications and facilitate their implantation and stabilization (fixation) in the tissues. Among classical fixation methods, surgical sutures and staples are the most popular. Such penetrating fixation is known to cause acute chronic pain [2,3] and irritation, likely due to tension or nerve compression by the sutures [4,5]. These complications have prompted surgeons to use atraumatic methods of fixation, including natural sealants such as fibrin glue [6,7], genetically engineered protein glues [8] or synthetic adhesives from the cyanoacrylates family [9,10]. However, despite being on the market for a long time, they are not ideal solutions, since fibrin glue shows relatively low mechanical strength [11] and very short shelf-life after defrizzing, while cyanoacrylates can cause an inflammatory reaction [12]. Additionally, cyanoacrylates are fast-acting adhesives [13] with limited control by the surgeon – they react too quickly, thus hindering the easiness of the surgical procedure and increasing the risk of making a mistake that is difficult to undo (once the glue is applied, it can no longer be moved or detached).
Therefore, there is a need to explore novel biomaterials that combine strong fixation properties with better handling and reduced post-surgery complications. Light-sensitive materials have emerged as promising candidates, turning from liquid to solid upon UV light activation and offering potentially improved control over the fixation process [14,15]. Their sensitivity to UV light comes from terminal methacrylic groups while physical/mechanical properties (elasticity, mechanical strength) are controlled by the core of a precursor [16,17]. Moreover, their chemistries can be easily adjusted making them biodegradable after a certain time. Recently, UV-curable biomaterials featuring tailored chemistries and biodegradability were developed and successfully screened for medical applications in soft tissue repair [14,16,17].
The newly developed PhotoBioCure technology, delivers UV-curable and biodegradable polymers for hernia mesh anastomosis and fixation. Unlike traditional adhesives, PhotoBioCure provides controlled curing, allowing for precise placement and minimizing unwanted adhesion. Moreover, these materials demonstrate biodegradation in vivo (over 65% mass loss after one year of implantation in rabbits) and a shelf-life of over two years (unpublished data), making them a promising alternative to current fixation materials.
Fixation techniques cannot be evaluated solely based on technical performance, without considering the patient’s experience, such as pain or possible hernia recurrence. Chronic pain or persistent neuralgia has been recognized as a complication after inguinal hernia repair, with symptoms appearing more than a year post-surgery [18]. Pain severity can range from mild to disabling and can significantly impact the patient’s quality of life [19].
The aim of this work was to evaluate the short-term outcomes (pain, local numbness, hematoma, wound infection, urinary retention), long-term outcomes (chronic pain, sensation of extraneous body, recurrence), and operation time for patients who underwent a mesh procedure for open inguinal hernia repair with new biodegradable and UV-curable material for mesh fixation.
2. Materials and Methods
2.1. PhotoBioCure Material
Viscous biomaterial (PhotoBioCure, PolTiss sp. z o.o., Poland) has been delivered in sterile, non-transparent syringes (1 ml).
2.2. Patients
The study involved ten patients who underwent inguinal herniorrhaphy according to the Lichtenstein technique. The spermatic cord, and hernia sac, were dissected typically from an incision over the inguinal ligament. After separating the spermatic cord from the hernia sac, the hernia sac was managed according to the principles of hernia surgery: in the case of an oblique hernia, after draining the contents into the peritoneal cavity, the excess sac was cut off and closed with a capsular suture. In the case of a straight hernia, draining the contents of the bag without opening it, and suturing the transverse fascia. The next step was to reinforce the posterior wall of the inguinal canal by sewing in a polymer mesh. The mesh was sutured to the inguinal ligament with continuous non-absorbable Prolen 3.0 sutures. Then, to prevent rolling or displacement of the mesh, it was spot-sewn with absorbable sutures to the external oblique muscle. In the control group (five patients), the mesh was sewn with Prolen 4.0 sutures, and in the study group (five patients), the mesh was fixed with drops of PhotoBioCure material spread over the areas of the applied sutures. The PhotoBioCure material was cured with UV light and delivered to the surgical field with a sterile fiber optic cable. The curing time was 3 min. Number of anchor sutures - 8, number of points anchored with the PhotoBioCure material (number of drops – 1 drop = 0.04 ml) - 8. The procedures were performed under standard epidural or subarachnoid anesthesia. Each patient received a standard (as in the case of using a tissue implant) dose of antibiotic (biofazolin, 1g) approximately 30 min before the procedure.
2.3. Inclusion Criteria
The study included active males aged 20 to 40 years with a Body Mass Index (BMI) of 25 to 27 and an uncomplicated unilateral primary inguinal hernia. All participants were eligible for elective hernia repair using the Lichtenstein technique and provided written, signed informed consent.
2.4. Exclusion Criteria
The exclusion criteria included: hernia recurrence, post-laparotomy status, history of leg vein thrombosis, history of pulmonary embolism, and other associated diseases such as autoimmune, cardiovascular, or respiratory disorders. Additionally, patients with allergies, addictions, or mental illnesses were excluded.
2.5. Postoperative Care
Postoperative care included an assessment of the general condition along with measurements of body temperature, heart rate, and blood pressure. Clinical evaluation of the wound was performed, including the assessment of tissue swelling, mesh distribution, and the presence of fluid in the implant area. Additionally, an ultrasound examination of the operated tissues was conducted, accompanied by an objective, non-invasive assessment of wound temperature using a FLIR T335 thermal imaging camera.
2.6. Ethical Approval
The study was conducted in accordance of the Ethics Committee of the Pomeranian Medical University (Resolution no. 04/2022 dated 24.03.2022) and conformed to the ethical guidelines of the 1975 Declaration of Helsinki.
3. Results
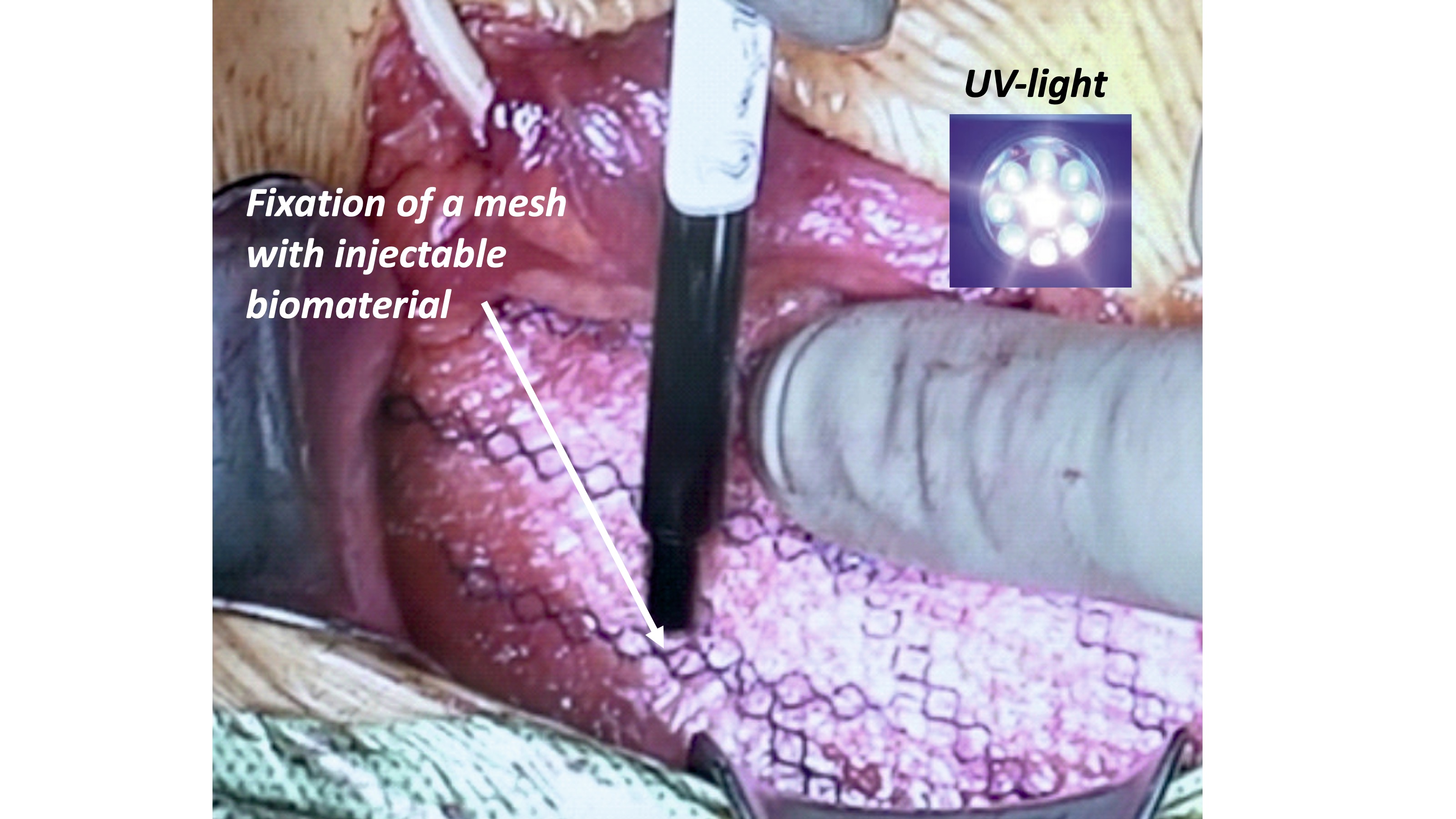
Here we present a medical experiment introducing an innovative concept and material: utilizing PhotoBioCure, a UV-curable and biodegradable material instead of sutures to fix the incised mesh to form a window for the spermatic cord in inguinal hernia repair (Figure 1). In the case of this most common male hernia, and in order to pass the spermatic cord through the mesh, it is necessary to cut the mesh at a distance of 2-3 cm and then the outer part of the incision is sutured. In this way, a window is created and the spermatic cord passes through the created window. In the study group, a UV-cured polymer was used instead of a suture, and it was successful - the polymer showed strong adhesion and well stabilized the incised mesh and the window created for the spermatic cord fulfilled its function. All patients were discharged on the next day after open surgery. Our findings demonstrate that this less invasive approach lasted significantly shorter compared to the routine approach with sutures (p < 0.005), indicating a statistically significant difference (Table 1). The application of the polymer is simpler and less time-consuming than suture placement, allowing for shorter procedure times and reducing the need for complex surgical manipulations.
We have a good evaluation of our observational study in the patients operated, 24 months after surgery. No complications like hematoma or seroma were observed in follow-up at 1 day, 8 day, 6 week, 12 month, and 24 month. At 24 months, none of the patients had developed a recurrence. In our observational study, postoperative pain was evaluated by a phone call from 1 week to 24 months after surgery, using a Visual Analogue Scale (VAS) going from 1 to 10, where 0 corresponded to no-pain status and 10 to the worst conceivable pain (Table 2). The collected data represents the outcomes observed in the study group (PhotoBioCure fixation). The mean VAS pain score on the first postoperative day was 2.6 (± 0.55), indicating moderate pain. By the 8th day, the pain score had significantly decreased to 0.8 (± 0.84), reflecting a rapid reduction in postoperative discomfort. Importantly, no pain was reported at the 6-week, 12-month, and 24-month follow-ups, with a mean VAS score of 0 at each interval.
The results of the evaluation of the sensation of a foreign body in the groin area based on the Carolinas Comfort Scale (Table 3) indicated that the severity of the sensation declined over time, comparably for both fixation methods. All patients in both, the study and control groups, reported similar complaints. On the first postoperative day, the mean foreign body sensation was 54.08% (± 9.74) and 65.32 (± 4.26), respectively after PhotoBioCure and suture fixation, indicating significant discomfort. In the case of fixation with new biomaterial, these values decreased to 40.98% (± 9.54) by day 8, with a further reduction to 30.38% (± 8.94) observed at the 6-week follow-up, until it reached almost minimum values (1.38% (±1.50)) after 24 months.
The evaluation of chronic pain based on the EuraHS QoL scale included examination of pain and restriction of activity. The analysis demonstrated a significant improvement across all evaluated parameters following inguinal hernia repair. Preoperative pain intensity averaged a value of 8.60 for both fixation methods. Then, decrease to 13.40 (± 1.14) and 12.40 (± 1.34) on the 8th postoperative day for PhotoBioCure and suture fixation, respectively, reflected an initial pain relief. The pain level progressively decreased, eventually reaching a point of complete pain absence after 12 months. Activity limitations also showed a marked reduction, from 35.00 (± 3.16) on 1sh day postoperatively to 6.60 (± 1.34) at the 6-week follow-up. Postoperative values for pain experienced while lying down and activity restrictions caused by hernia pain decreased regardless of whether the new biomaterial or sutures were used, which was attributed to the natural wound healing process without any complications. The Friedman test indicated no statistically significant differences in both variables between fixation methods or across follow-up time points (p > 0.05). This suggests that these variables were comparable between the two methods and remained stable over time.

Table 4.
The evaluation of chronic pain based on the EuraHS QoL.
| PhotoBioCure Fixationa | Suture Fixationa | ||
|---|---|---|---|
| Domain | Mean Value (±SD) | Mean Value (±SD) | |
| Pain | |||
| before surgery | 8.60 (2.19) | 8.60 (2.30) | |
| 1st day | 22.60 (1.95) | 21.80 (2.17) | |
| 8th days | 13.40 (1.14) | 12.40 (1.34) | |
| 6th weeks | 3.40 (1.82) | 3.60 (1.14) | |
| 12th months | 0.00 | 0.00 | |
| 24th months | 0.00 | 0.00 | |
| Restriction of activity | |||
| before surgery | 12.80 (4.66) | 11.80 (3.42) | |
| 1st day | 35.00 (3.16) | 34.30 (3.35) | |
| 8th days | 18.40 (3.65) | 17.40 (3.36) | |
| 6th weeks | 6.60 (1.34) | 6.60 (2.41) | |
| 12th months | 1.40 (1.14) | 1.00 (0.00) | |
| 24th months | 1.20 (0.84) | 1.00 (0.00) | |
| ap > 0.05, Friedman test | |||
The patient’s quality of life after surgical treatment of inguinal hernia has been evaluated based on a dedicated SF 36 questionnaire. Table 5 shows that all patients indicated a very high quality of life after 24 months postoperatively.
Ultrasonographic assessment of hernia mesh placement was conducted in five patients. The mesh was appropriately positioned in all cases, with no evidence of hernia recurrence. Two patients exhibited no signs of inflammatory infiltration around the mesh, while one case presented with inflammatory infiltration. A hematoma was identified in one patient. One patient refused further follow-up imaging but reported no symptoms during a 24-month telephone consultation.
A thermal imaging camera was used to assess temperature differences between healthy body regions and those with disease processes. Figure 2 shows maps of tissue temperature distribution before and after surgery. Before surgery (Figure 2a), the tissues in the hernia area showed an elevated temperature, which was visible as intense red and yellow areas. Six hours after surgery (Figure 2 b), the temperature of the tissues around the operated site remained high, with distinct red areas. The elevated temperature was still visible one day after surgery (Figure 2 c), but there was a noticeable gradual decrease in heat intensity compared to earlier images.
4. Statistical Method
Statistical analyses were conducted using Statistica version 13.3 software (Statistica Software Inc., Palo Alto, CA, USA). Means and standard deviations (SD) were calculated for descriptive statistics. The normality of quantitative data was assessed using the Shapiro–Wilk test and the homogeneity of variances was evaluated with Levene’s test. When data met the assumptions of normal distribution and homogeneity of variances, ANOVA with the NIR post hoc test was applied. In cases where one or both assumptions were violated, nonparametric tests, specifically the Mann-Whitney U test for comparisons between groups and the Friedman test for comparisons among groups, were used. Statistical significance was set at p < 0.05.
5. Discussion
Inguinal hernia repair is one of the most commonly performed surgical procedures worldwide, with optimizing patient outcomes is paramount. The primary goal is to settle the patient’s return to normal function through a quick return to work and no (or low <1%) recurrence rate, and no patient discomfort, numbness, or neuralgia. While traditional mesh fixation methods using sutures are well-established, our study explores the novel use of the PhotoBioCure biomaterial, which offers the potential for reduced postoperative pain and quicker recovery, contributing to advancements in atraumatic fixation techniques. The effectiveness of mesh fixation, defined as the absence of hernia recurrence, using the new biomaterial is comparable to the traditional use of sutures but may have the added benefit of less pain and a faster return to full activity. Our results are consistent with previous studies showing that alternative fixation methods such as the use of glues can reduce postoperative pain sensation [20,21,22]. Compared to the study by E. Wassenaar et al., in which traditional mesh fixation with sutures showed VAS values of 4.5 ± 10.5 (absorbable sutures) and 11.2 ± 21.2 (non-absorbable sutures) after 3 months, the PhotoBioCure group reported significantly lower pain levels on the first day after surgery (VAS 2.6 ± 0.55). The pain sensation decreased over time, the greatest reduction occurred in the initial weeks post-surgery, reaching a minimum value (VAS 0.8 ± 0.84) after 8 days until it disappeared completely after 6 weeks, underscoring the long-term effectiveness of PhotoBioCure in pain management (p < 0.05). A study by S.K. Jain and A. Vindal [21] on the use of the atraumatic fixation method with tissue glue (GRF glue) led to the complete disappearance of pain after 7 days, where our result was similar (VAS 0.8), although still slightly above zero. In contrast, in the study by Amera Odobasic et al. [24], postoperative pain sensations ranged from 2.23 to 3.16 after 7 days using fibrin glue. Similarly, the use of cyanoacrylate-based adhesive resulted in a postoperative pain sensation of 2.28 (SD = 1.79) after the same time) [23]. These results support the hypothesis that non-penetrating fixation methods, such as with the use of PhotoBioCure, effectively reduce early postoperative pain thus discomfort and speeding recovery. It may be attributed to the atraumatic nature of fixation, which avoids nerve entrapment and reduces tissue irritation commonly observed with suture-based methods [4,24]. This effect is further supported by thermal imaging observations, which demonstrated reduced tissue inflammation and a gradual decrease in temperature within the first 24 hours post-surgery, indicating a normal healing process without excessive inflammatory response. Similarly, the evaluation of chronic pain based on the EuraHS QoL also confirmed that it diminishes over time. The application of PhotoBioCure material in inguinal hernia repair significantly reduces foreign body sensation in the groin, as assessed by the Carolinas Comfort Scale, within 6 weeks post-surgery, and does not cause discomfort in the long term, up to 24 months. Statistically significant differences in discomfort levels were observed at 12 and 24 months (p < 0.05), consistent with findings in the control group. On the other hand, no significant differences in sensation were observed between the groups (p > 0.05), indicating similarly effective treatment outcomes. Patients’ quality of life associated with hernias significantly improved 24 months, consistent with other atraumatic mesh fixation methods [25]. Moreover, using the new material for mesh fixation with UV- light activated material appears to be suitable for open tension-free repairs. After 24 months, we have not observed any complications associated with this technique, no mesh migration, infections, or chronic pain were observed. While these results are promising, longer follow-ups and larger sample sizes are necessary to fully assess the long-term safety profile of PhotoBioCure, particularly in comparison to established fixation methods. In addition to clinical benefits, the use of new biomaterial offers potential economic advantages. The application of PhotoBioCure fixation resulted in an average time reduction of 13.63% compared to traditional suture fixation methods, highlighting its effectiveness in significantly decreasing operational duration, therefore minimizes hospital resource utilization, leading to lower procedural costs [26]. Additionally, the reduced risk of postoperative complications could further reduce long-term healthcare expenses. In addition, shorter wound exposure may reduce the risk of infection, but to prove this thesis, studies on a larger group of patients are necessary. The results indicate that pain after polymer application was not greater, which supports the lack of tissue reaction and proves the biocompatibility of the polymer in the human tissue environment.
6. Conclusions
This study presents the pioneering application of PhotoBioCure technology in hernia reconstruction. The use of this novel and adhesive biomaterial introduces a significant advancement in surgical techniques without increasing perioperative or postoperative risks. Importantly, this biodegradable material does not provoke adverse tissue reactions or impair in wound healing, making it a promising alternative to conventional absorbable sutures for hernia mesh fixation. Furthermore, the elimination of the need for stitching and knot-tying during the application reduces the risk of injury to fine sensory and motor nerves in the vicinity of spermatic cord, which may lower the incidence of chronic neuralgia-type pain often observed following inguinal hernia repair. The adhesive properties of the material provide enhanced fixation of a mesh. Biodegradable and adhesive PhotoBioCure technology offers a dual benefit: material is gradually resorbed, thus minimizing foreign body presence, while simultaneously supporting the natural healing process. However, further studies are necessary to evaluate the long-term degradation profile and broader clinical efficacy of this material in various patient populations and hernia types.
Acknowledgments
Financial support from the Regional Operational Program Project RPZP.01.01.00-32-0002/20 is acknowledged.
Conflicts of Interest
M. El Fray is a co-inventor of patents that are licensed to PolTiss Sp. z o.o. A. Goszczyńska and G. Demirci has performed paid consulting for PolTiss Sp. z o.o. which is commercializing photocurable biomaterials.
References
- Hollinsky, C.; Kolbe, T.; Walter, I.; Joachim, A.; Sandberg, S.; Koch, T.; Rülicke, T. Comparison of a New Self-Gripping Mesh with Other Fixation Methods for Laparoscopic Hernia Repair in a Rat Model. J. Am. Coll. Surg. 2009, 208, 1107–1114. [CrossRef]
- Nikkolo, C.; Lepner, U. Chronic pain after open inguinal hernia repair. Postgrad. Med. 2015, 128, 69–75. [CrossRef]
- Nguyen, D.K.; Amid, P.K.; Chen, D.C. Groin Pain After Inguinal Hernia Repair. Adv. Surg. 2016, 50, 203–220. [CrossRef]
- Kim-Fuchs C, Angst E, Vorburger S, et al. Prospective randomized trial comparing sutured with sutureless mesh Wxation for Lichtenstein hernia repair: Long-term results. Hernia 2012; 16(1): 21–27. [CrossRef]
- Helbling, C.; Schlumpf, R. Sutureless Lichtenstein: First results of a prospective randomised clinical trial. Hernia 2003, 7, 80–84. [CrossRef]
- Campanelli, G.; Pettinari, D.; Cavalli, M.; Avesani, E.; Ec, A. A modified Lichtenstein hernia repair using fibrin glue. J. Minimal Access Surg. 2006, 2, 129–33. [CrossRef]
- Lovisetto F, Zonta S, Rota E, et al. Use of human fibrin glue (Tissucol) versus staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty: A prospective, randomized study. Ann Surg 2007; 245(2): 222–231. [CrossRef]
- Liu, H.; Zheng, X.; Gu, Y.; Guo, S. A Meta-Analysis Examining the Use of Fibrin Glue Mesh Fixation versus Suture Mesh Fixation in Open Inguinal Hernia Repair. Dig. Surg. 2014, 31, 444–451. [CrossRef]
- Trisca, R.; Oprea, V.; Toma, M.; Bucuri, C.E.; Stancu, B.; Grad, O.; Gherman, C. The Effectiveness of Cyanoacrylates versus Sutures for Mesh Fixation after Lichtenstein Repair (SCyMeLi STUDY) A Systematic Review and Meta-Analyze of Randomized Controlled Trials. Chirurgia 2024, 119, 87–101. [CrossRef]
- Dąbrowiecki, S.; Pierściński, S.; Szczęsny, W. The Glubran 2 glue for mesh fixation in Lichtenstein’s hernia repair: a double-blind randomized study.. Videosurgery Other Miniinvasive Tech. 2012, 7, 96–104. [CrossRef]
- Odobasic, A.; Krdzalic, G.; Hodzic, M.; Hasukic, S.; Sehanovic, A.; Odobasic, A. The Role of Fibrin Glue Polypropylene Mesh Fixation in Open Inguinal Hernia Repair. Med Arch. 2014, 68, 90–93. [CrossRef]
- Ladurner, R.; Drosse, I.; Bürklein, D.; Plitz, W.; Barbaryka, G.; Kirchhoff, C.; Kirchhoff, S.; Mutschler, W.; Schieker, M.; Mussack, T. Cyanoacrylate Glue for Intra-abdominal Mesh Fixation of Polypropylene-Polyvinylidene Fluoride Meshes in a Rabbit Model. J. Surg. Res. 2011, 167, e157–e162. [CrossRef]
- Haroon, M.; Morarasu, S.; Morarasu, B.C.; Al-Sahaf, O.; Eguare, E. Assessment of feasibility and safety of cyanoacrylate glue versus absorbable tacks for inguinal hernia mesh fixation. A prospective comparative study.. Videosurgery Other Miniinvasive Tech. 2022, 17, 90–98. [CrossRef]
- Skrobot, J.; Zair, L.; Ostrowski, M.; El Fray, M. New injectable elastomeric biomaterials for hernia repair and their biocompatibility. Biomaterials 2016, 75, 182–192. [CrossRef]
- Taboada, G.M.; Yang, K.; Pereira, M.J.N.; Liu, S.S.; Hu, Y.; Karp, J.M.; Artzi, N.; Lee, Y. Overcoming the translational barriers of tissue adhesives. Nat. Rev. Mater. 2020, 5, 310–329. [CrossRef]
- Pradas MM, Vicent MJ. Polymers in Regenerative Medicine: Biomedical Applications from Nano- to Macro-Structures. Polymers in Regenerative Medicine: Biomedical Applications from Nano- to Macro-Structures. 2014. p. 1–393.
- El Fray, M.; Skrobot, J.; Bolikal, D.; Kohn, J. Synthesis and characterization of telechelic macromers containing fatty acid derivatives. React. Funct. Polym. 2012, 72, 781–790. [CrossRef]
- Fortelny, R.H.; Petter-Puchner, A.H.; Redl, H.; May, C.; Pospischil, W.; Glaser, K. Assessment of Pain and Quality of Life in Lichtenstein Hernia Repair Using a New Monofilament PTFE Mesh: Comparison of Suture vs. Fibrin-Sealant Mesh Fixation. Front. Surg. 2014, 1, 45. [CrossRef]
- Jeroukhimov, I.; Dykman, D.; Hershkovitz, Y.; Poluksht, N.; Nesterenko, V.; Ben Yehuda, A.; Stephansky, A.; Zmora, O. Chronic pain following totally extra-peritoneal inguinal hernia repair: a randomized clinical trial comparing glue and absorbable tackers. Langenbeck’s Arch. Surg. 2023, 408, 1–5. [CrossRef]
- Mathes T, Prediger B, Walgenbach M, et al. Mesh fixation techniques in primary ventral or incisional hernia repair. Vol. 2021, Cochrane Database of Systematic Reviews. John Wiley and Sons Ltd; 2021. [CrossRef]
- Jain, S.K.; Vindal, A. Gelatin–resorcin–formalin (GRF) tissue glue as a novel technique for fixing prosthetic mesh in open hernia repair. Hernia 2009, 13, 299–304. [CrossRef]
- Hoyuela, C.; Juvany, M.; Carvajal, F.; Veres, A.; Troyano, D.; Trias, M.; Martrat, A.; Ardid, J.; Obiols, J.; López-Cano, M. Randomized clinical trial of mesh fixation with glue or sutures for Lichtenstein hernia repair. Br. J. Surg. 2017, 104, 688–694. [CrossRef]
- Mitura, K.; Garnysz, K.; Wyrzykowska, D.; Michałek, I. The change in groin pain perception after transabdominal preperitoneal inguinal hernia repair with glue fixation: a prospective trial of a single surgeon’s experience. Surg. Endosc. 2018, 32, 4284–4289. [CrossRef]
- Fortelny, R.H.; Petter-Puchner, A.H.; May, C.; Jaksch, W.; Benesch, T.; Khakpour, Z.; Redl, H.; Glaser, K.S. The impact of atraumatic fibrin sealant vs. staple mesh fixation in TAPP hernia repair on chronic pain and quality of life: results of a randomized controlled study. Surg. Endosc. 2011, 26, 249–254. [CrossRef]
- Tish, S.; Krpata, D.; AlMarzooqi, R.; Huang, L.-C.; Phillips, S.; Fafaj, A.; Tastaldi, L.; Alkhatib, H.; Zolin, S.; Petro, C.; et al. Comparing 30-day outcomes between different mesh fixation techniques in minimally invasive inguinal hernia repair. Hernia 2020, 24, 961–968. [CrossRef]
- Bellad, A.P.; Pratap, K.A. Effectiveness of tissue adhesive versus conventional sutures in the closure of inguinal hernia skin incisions: a prospective randomized controlled trial. Int. Surg. J. 2018, 5, 1797–1801. [CrossRef]
Figure 1.
Application of PhotoBioCure biomaterial (a); curing with UV light (b); fixed mesh with flexible and transparent biomaterial (c).
Figure 1.
Application of PhotoBioCure biomaterial (a); curing with UV light (b); fixed mesh with flexible and transparent biomaterial (c).
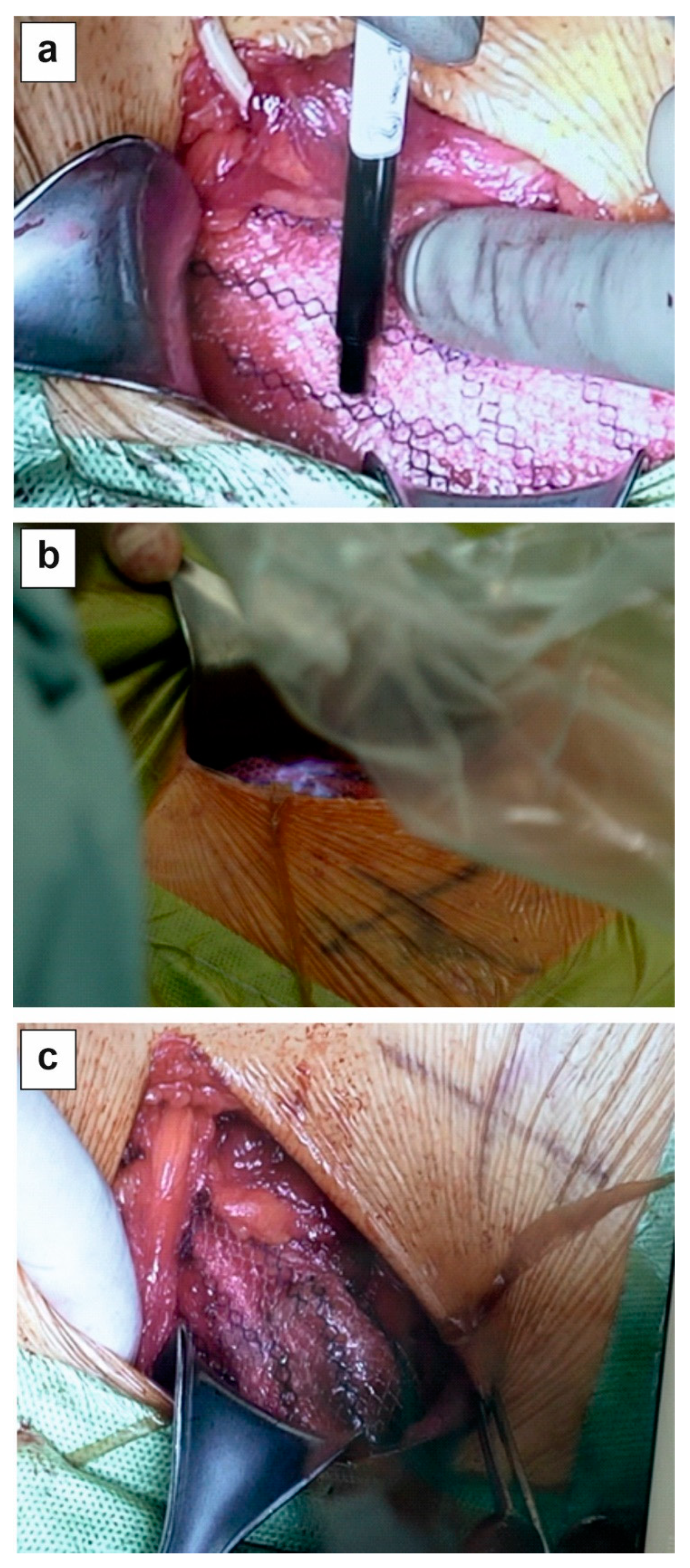
Figure 2.
Images from the thermal camera showing herniated tissue before surgery (a), 6 hours after surgery (b), 1st day after surgery (c).
Figure 2.
Images from the thermal camera showing herniated tissue before surgery (a), 6 hours after surgery (b), 1st day after surgery (c).
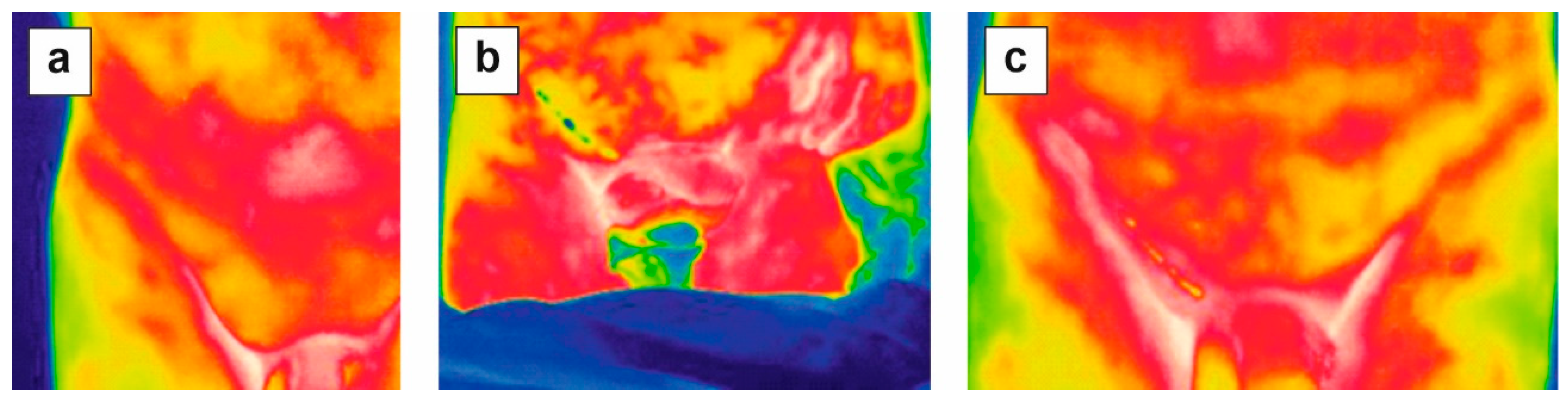
Table 1.
Surgery-related variables.
| PhotoBioCure Fixationa [min] (±SD) |
Suture fixationa [min] (±SD) |
|
|---|---|---|
| Average operating timeb | 52.00 (3.08) | 60.20 (3.70) |
| Postoperative hospital stay | 1 day | 1 day |
| Average time to resumption of normal activity | 6 weeks | 6 weeks |
| Duration of follow-up | 24 | 24 |
| Intraoperative complications (n) | 0 | 0 |
| a n = 5, b p < 0.05, Mann-Whitney U test |
Table 2.
Comparisons of VAS score follow-up among the study group a.
| Follow-Up Period | Fixation | Mean Pain Scorea (±SD) |
|---|---|---|
| 1st day | PhotoBioCure | 2.6 (0.55) |
| 8th day | PhotoBioCure | 0.8 (0.84) |
| 6th week | PhotoBioCure | 0 |
| 12th month | PhotoBioCure | 0 |
| 24th month | PhotoBioCure | 0 |
| a p < 0.05, Mann-Whitney U test | ||
Table 3.
Assessment of groin foreign body sensation using the Carolinas Comfort scale.
| PhotoBioCure Fixationa,b | Suture Fixationa,b | |
|---|---|---|
| Follow-Up Period | Mean Value of Severity [%](±SD) | Mean Value of Severity [%](±SD) |
| 1st day | 54.08 (9.74) | 65.32 (4.26) |
| 8th days | 40.98 (9.54) | 49.45 (5.92) |
| 6th weeks | 30.38 (8.94) | 36.57 (2.21) |
| 12th months | 8.28 (1.71) | 8.97 (1.71) |
| 24th months | 1.38 (1.50) | 1.38 (0,96) |
| ap < 0.05, ANOVA test (among methods); b p > 0.05 Mann-Whitney U test (between methods) | ||
Table 5.
Evaluation of patient’s quality of life after surgical treatment of inguinal hernia based on the SF 36 questionnaire.
Table 5.
Evaluation of patient’s quality of life after surgical treatment of inguinal hernia based on the SF 36 questionnaire.
| SF-36 | Mean Valuea(±SD) |
|---|---|
| preoperatively | 77.8 (6.72)b |
| 6th weeks postoperatively | 71.6 (6.34)b |
| 12th months postoperatively | 88.2 (4.82)b |
| 24th months postoperatively | 92.4 (3.26)b |
| ascore of 100 indicates the highest quality of life, with lower scores reflecting deterioration; b p < 0.05, ANOVA test | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



