
Submitted:
09 December 2024
Posted:
12 December 2024
You are already at the latest version
Abstract
African trypanosomiasis, or sleeping sickness, is a neglected tropical disease caused by Trypanosoma brucei parasites and transmitted by tsetse flies. Traditionally recognized for its neurological manifestations, including meningoencephalitis and cognitive impairment, sleeping sickness also profoundly affects sleep patterns and quality of life among affected individuals. This comprehensive review explores the intricate interplay between African trypanosomiasis and sleep disorders, examining the disease's epidemiology, pathogenesis, clinical manifestations, and diagnosis. We delve into the mechanisms underlying sleep disturbances in sleeping sickness, including disruptions of circadian rhythms, neurotransmitter imbalances, immune system dysregulation, and neurological complications. Furthermore, we discuss the challenges and opportunities in diagnosing, treating, and managing sleep disorders in the context of African trypanosomiasis, emphasizing the importance of integrated approaches to healthcare delivery, community engagement, and interdisciplinary research collaboration. By synthesizing current evidence from clinical studies and experimental research, this review provides insights into the bidirectional relationship between African trypanosomiasis and sleep disorders, identifies gaps in knowledge, and proposes future research directions to improve clinical outcomes for individuals affected by sleeping sickness.
Keywords:
trypanosomiasis
; sleeping sickness
; sleep disorders
; Trypanosoma brucei
; circadian rhythms
; parasitic infections
; neuroimmunology
; neurozoonotic
; neuroparasitology
; neglected tropical disease
1. Introduction
1.1. Background and Epidemiology
African trypanosomiasis, commonly known as sleeping sickness, is a neglected tropical disease caused by the parasitic protozoa Trypanosoma brucei. The disease primarily affects rural communities in sub-Saharan Africa, where conditions are conducive to spreading the tsetse fly vector responsible for transmitting the parasite between humans and animals [1]. The two main subspecies of Trypanosoma brucei that cause sleeping sickness in humans are T. b. gambiense and T. b. rhodesiense, each with distinct epidemiological characteristics (Table 1) [2].
T. b. gambiense is responsible for the chronic form of sleeping sickness, which is endemic in West and Central Africa. This subspecies accounts for approximately 98% of reported cases and is associated with a slower progression of symptoms, often leading to misdiagnosis and delayed treatment [3]. Transmission occurs in regions where humans live close to infected animals, particularly in rural areas with limited access to healthcare and adequate vector control measures.
In contrast, T. b. rhodesiense causes acute sleeping sickness, predominantly found in East and Southern Africa. This subspecies is responsible for a smaller proportion of cases but tends to progress rapidly, leading to more severe symptoms and a higher risk of mortality if left untreated [4]. Transmission occurs in savannah areas where humans frequently come into contact with wild and domestic animals, emphasizing the importance of targeted vector control interventions [5].
Various factors, including environmental conditions, population movements, and socioeconomic determinants, influence the epidemiology of African trypanosomiasis [6]. The presence of suitable habitats for tsetse flies, such as dense vegetation and proximity to water sources, contributes to the spatial distribution of the disease. Human activities, such as agriculture, livestock farming, and deforestation, can exacerbate the risk of transmission by altering tsetse fly habitats and increasing human-vector contact [7].
Furthermore, population movements within and between endemic regions play a significant role in the spread of the disease. Migration patterns, seasonal movements, and displacement due to conflicts or environmental disasters can introduce Trypanosoma brucei to new areas, leading to outbreaks and localized epidemics [8]. Additionally, socioeconomic factors, such as poverty, inadequate healthcare infrastructure, and limited access to diagnostic and treatment services, contribute to the persistence of African trypanosomiasis in affected communities [9].
Despite significant progress in disease control efforts over the past decades, African trypanosomiasis remains a significant public health challenge in many parts of sub-Saharan Africa. The complexity of the disease transmission cycle, coupled with socioeconomic and environmental factors, underscores the need for integrated approaches to prevention, diagnosis, and treatment [10]. In this study, we narratively reviewed the literature regarding African trypanosomiasis.
1.2. Trypanosoma Brucei Parasitology
Trypanosoma brucei is a unicellular parasitic protozoan belonging to the Trypanosoma genus and the family Trypanosomatidae. It is a flagellated organism with a complex life cycle involving multiple developmental stages and hosts. Also, Trypanosoma brucei exhibits a characteristic morphology that is typical of trypanosomes. The parasite is elongated and spindle-shaped, with a single flagellum protruding from the anterior end. The flagellum is essential for motility and contributes to the parasite’s ability to move within the bloodstream and tissues of its host [11].
The life cycle of Trypanosoma brucei involves the tsetse fly (Glossina species) and a mammalian host, typically humans or other animals (Figure 1). The parasite undergoes several developmental stages in each host, adapting to the specific environments encountered. The life cycle begins when a bloodstream form of Trypanosoma brucei, known as the trypomastigote, is ingested by a tsetse fly during a blood meal. Once ingested, the trypomastigotes transform into procyclic trypomastigotes within the fly’s midgut. These procyclic forms develop further, eventually differentiating into epimastigotes and infective metacyclic trypomastigotes. The metacyclic trypomastigotes migrate to the salivary glands of the tsetse fly, where they await transmission to a mammalian host during subsequent blood feeding [12].
Transmission occurs when an infected tsetse fly takes a blood meal, releasing metacyclic trypomastigotes into the bloodstream of the mammalian host. Once in the bloodstream, the metacyclic trypomastigotes transform into bloodstream trypomastigotes, the form responsible for causing clinical disease. These bloodstream trypomastigotes multiply by binary fission within the bloodstream, evading the host’s immune system through antigenic variation. The parasites can also cross the blood-brain barrier, leading to neurological manifestations in the late stage of the disease [13]. In addition to the bloodstream form, Trypanosoma brucei can also exist in a non-dividing, quiescent form known as the stumpy form, which plays a role in transmission back to the tsetse fly [14].
One of the critical survival strategies employed by Trypanosoma brucei is antigenic variation, whereby the parasite periodically changes the expression of its surface coat proteins [15]. This allows the parasite to evade host immune responses and persist in the bloodstream for extended periods. Antigenic variation contributes to the chronicity of infection and presents a significant challenge for vaccine development and immune-based interventions.
1.3. Sleep Disorders
Emerging evidence suggests that Trypanosoma brucei infection disrupts regular sleep-wake cycles, leading to a spectrum of sleep disorders ranging from insomnia to excessive daytime sleepiness [16]. In this context, African trypanosomiasis disrupts the body’s internal clock, leading to disturbances in circadian rhythms. Studies have shown alterations in the timing and duration of sleep phases, with individuals experiencing fragmented sleep patterns and difficulty maintaining a regular sleep-wake cycle. The disruption of circadian rhythms may result from direct effects of the parasite on the central nervous system or indirect consequences of systemic inflammation and immune activation [17].
Trypanosoma brucei infection can affect the neurotransmitters involved in sleep regulation, such as serotonin, dopamine, and gamma-aminobutyric acid [18]. Imbalances in these neurotransmitters may contribute to sleep disturbances observed in infected individuals, including changes in sleep latency, sleep efficiency, and rapid eye movement sleep. Additionally, alterations in neurotransmitter function may underlie the neuropsychiatric symptoms commonly associated with African trypanosomiasis, further exacerbating sleep problems [19].
The immune response to Trypanosoma brucei infection plays a crucial role in the pathogenesis of sleeping sickness and may also influence sleep patterns. Dysregulation of pro-inflammatory cytokines, such as tumor necrosis factor-alpha and interleukin-6, has been implicated in developing sleep disturbances in infectious diseases [20]. Chronic inflammation associated with African trypanosomiasis may contribute to sleep disorders by directly affecting brain regions involved in sleep regulation or inducing sickness behavior characterized by lethargy and increased sleepiness [21].
2. Pathophysiology of Sleep Disorders in African Trypanosomiasis
2.1. Disruption of Circadian Rhythms
African trypanosomiasis profoundly affects circadian rhythms, including sleep-wake cycles (Figure 2). The disruption of circadian rhythms in individuals infected with Trypanosoma brucei can lead to fragmented sleep patterns, altered sleep architecture, and disturbances in overall sleep quality [22]. Understanding the mechanisms underlying this disruption is essential for elucidating the pathophysiology of sleeping sickness and developing targeted interventions to improve sleep outcomes in affected individuals.
Trypanosoma brucei parasites have been shown to invade the central nervous system (CNS), including the brain regions involved in circadian rhythm regulation, such as the hypothalamus and suprachiasmatic nucleus [17]. This disruption can lead to desynchronization of the internal clock, resulting in irregular sleep-wake patterns and difficulty keeping a stable sleep schedule. In addition to direct effects on the CNS, African trypanosomiasis triggers a robust immune response characterized by neuroinflammation and activation of microglial cells within the brain [23]. Chronic inflammation in the CNS can interfere with the function of neurotransmitter systems implicated in sleep regulation, such as serotonin and dopamine. Imbalances in these neurotransmitters can disrupt the normal sleep-wake cycle, leading to insomnia, hypersomnia, or other sleep disturbances commonly observed in individuals with sleeping sickness. Also, studies have suggested that Trypanosoma brucei infection may alter melatonin production or secretion, potentially contributing to disturbances in sleep patterns [24]. Disruptions in melatonin signaling can affect the timing and quality of sleep, exacerbating sleep-related symptoms in infected individuals.
Circadian rhythms are not limited to the CNS but are also present in peripheral tissues and organs throughout the body [25]. Trypanosoma brucei infection may perturb the synchronization between central and peripheral clocks, leading to dysregulation of metabolic processes, hormone secretion, and immune function. These systemic effects can further contribute to sleep disturbances and exacerbate the overall impact of sleeping sickness on health and well-being.
2.2. Neurotransmitter Imbalance
Serotonin can be affected by Trypanosoma brucei infection [26]. Studies have shown alterations in serotonin levels and receptor expression in infected individuals’ CNS, leading to sleep architecture and quality disruptions. Imbalances in serotonin signaling may contribute to insomnia, hypersomnia, and changes in REM sleep observed in patients with sleeping sickness.
Dopamine is also dysregulated in African trypanosomiasis [27]. The parasite-induced inflammatory response and neuroinflammation can alter dopamine synthesis, release, and receptor activity. Dysfunctional dopaminergic signaling may contribute to sleep disturbances, cognitive deficits, and neuropsychiatric symptoms commonly observed in infected individuals.
Dysregulation of GABAergic neurotransmission in sleeping sickness may result from the direct effects of Trypanosoma brucei on GABA-producing neurons or secondary to neuroinflammatory processes [28]. Imbalances in GABA signaling can disrupt sleep onset, maintenance, and overall sleep quality, contributing to the burden of sleep-related symptoms in affected individuals.
Glutamate is implicated in the pathogenesis of neurological complications associated with African trypanosomiasis [29]. The parasite-induced neuroinflammatory response can lead to excessive glutamate release and excitotoxicity, contributing to neuronal damage and dysfunction.
Targeting neurotransmitter imbalances represents a promising approach for managing sleep disturbances and other neurological symptoms associated with sleeping sickness [30]. Pharmacological interventions to restore neurotransmitter homeostasis, such as selective serotonin reuptake inhibitors, dopaminergic agonists, or GABAergic modulators, may help alleviate sleep-related symptoms and improve overall patient well-being. However, further research is needed to elucidate neurotransmitter dysregulation mechanisms in African trypanosomiasis and identify optimal therapeutic strategies for addressing these abnormalities.
2.3. Immune System Modulation
African trypanosomiasis involves a complex interplay between the parasite and the host immune system. The immune response mounted against the parasite plays a critical role in the pathogenesis of the disease, influencing the control of parasite growth and contributing to the development of various clinical manifestations, including sleep disturbances. Understanding the modulation of the immune system in sleeping sickness is essential for unraveling the mechanisms underlying sleep disorders and developing targeted therapeutic interventions to alleviate these symptoms [31].
Trypanosoma brucei infection induces a robust pro-inflammatory immune response characterized by the production of cytokines such as tumor necrosis factor-alpha, interleukin-1 beta, and interleukin-6 [32]. These cytokines are crucial in activating immune effector cells and coordinating the host defense against the parasite. However, excessive production of pro-inflammatory cytokines can lead to neuroinflammation and disrupt normal CNS function, contributing to sleep disturbances [33].
In response to Trypanosoma brucei infection, microglial cells within the central nervous system activate and release pro-inflammatory mediators, amplifying the neuroinflammatory response [34]. Chronic neuroinflammation is associated with neuronal damage, disruption of synaptic function, and alterations in neurotransmitter signaling, all of which can contribute to sleep disorders. Microglial activation may directly impact sleep regulatory centers within the brain, leading to disturbances in circadian rhythms and sleep-wake patterns [35].
The immune response to Trypanosoma brucei infection can induce sickness behavior and nonspecific symptoms, including lethargy, anorexia, and increased sleepiness [36]. Sickness behavior is thought to be mediated by pro-inflammatory cytokines acting on the CNS, signaling the presence of infection and promoting behaviors that conserve energy and facilitate recovery. While adaptive in acute disease, persistent sickness behavior can lead to prolonged sleep disturbances and impaired quality of life in individuals with chronic sleeping sickness [37].
Trypanosoma brucei has evolved several strategies to evade the host immune response and establish chronic infection. These include antigenic variation, allowing the parasite to escape immune recognition and suppress host immune effector mechanisms [38]. By modulating host immune responses, the parasite can create an immunosuppressive microenvironment that facilitates its survival and dissemination within the host, further exacerbating immune-mediated pathology, including sleep disturbances.
Targeting the immune dysregulation associated with African trypanosomiasis represents a promising approach to managing sleep disturbances and other neurological symptoms. Immunomodulatory therapies, such as anti-inflammatory agents or immunosuppressive drugs, may help alleviate neuroinflammation and restore immune homeostasis, improving sleep outcomes in affected individuals. However, further research is needed to evaluate the safety and efficacy of such interventions in the context of sleeping sickness.
3. Clinical Manifestations of Sleep Disorders in African Trypanosomiasis
3.1. Subtypes of African Trypanosomiasis
African trypanosomiasis, commonly known as sleeping sickness, encompasses two main subtypes based on the Trypanosoma brucei species involved and the disease's geographical distribution. These subtypes exhibit distinct epidemiological characteristics, clinical manifestations, and diagnostic and treatment considerations.
Trypanosoma brucei gambiense is responsible for the chronic form of African trypanosomiasis and is primarily found in West and Central Africa [39]. Transmission of T. b. gambiense occurs primarily through the bite of infected tsetse flies of the genus Glossina, particularly in rural and forested areas where the human population comes into contact with the vector. The chronic form of sleeping sickness caused by T. b. gambiense is characterized by a prolonged incubation period lasting months to years. Patients often present with non-specific symptoms in the early stages, including fever, headaches, and joint pain. As the disease progresses, neurological symptoms such as sleep disturbances, behavioral changes, and cognitive impairment become prominent. Diagnosing T. b. gambiense infection relies on parasitological techniques such as microscopic examination of blood, lymph node aspirates, or cerebrospinal fluid. Treatment typically involves administering drugs such as pentamidine or suramin in the early stages of the disease. At the same time, late-stage infections require more potent medications such as eflornithine or a combination of eflornithine and nifurtimox [40].
Trypanosoma brucei rhodesiense is responsible for the acute form of African trypanosomiasis and is predominantly found in East and Southern Africa [41]. Transmission of T. b. rhodesiense occurs in savannah areas through the bite of infected tsetse flies, with humans frequently coming into contact with wild and domestic animals serving as reservoir hosts for the parasite. The acute form of sleeping sickness caused by T. b. rhodesiense is characterized by a relatively short incubation period lasting weeks to months. Patients typically present with a rapid onset of symptoms, including fever, malaise, and swelling at the site of the tsetse fly bite. Neurological involvement occurs early in the disease, with symptoms such as severe headaches, confusion, and motor disturbances. Diagnosis of T. b. rhodesiense infection is similar to that of T. b. gambiense infection, relying on parasitological techniques such as blood smear examination. Treatment usually involves administering drugs such as suramin or melarsoprol, effective against early-stage infections. Late-stage infections may require treatment with melarsoprol or a combination of eflornithine and nifurtimox [42].
3.2. Sleep Disturbances
Sleep disturbances represent a significant clinical feature of African trypanosomiasis, contributing to the overall burden of the disease and impacting patients' quality of life. These disturbances manifest in various forms and severity levels, ranging from mild insomnia to severe disruptions in sleep architecture [43]. Understanding the spectrum of sleep-related symptoms and their severity is crucial for effectively diagnosing, managing, and monitoring individuals affected by sleeping sickness.
Insomnia, characterized by difficulty falling or staying asleep, is a common manifestation of African trypanosomiasis [44]. Patients may report prolonged sleep latency, frequent awakenings during the night, and non-restorative sleep. Insomnia severity can vary, ranging from transient and mild sleep difficulties to chronic and severe insomnia that significantly impairs daytime functioning and quality of life. The severity of insomnia may fluctuate throughout the disease, influenced by factors such as disease progression, treatment response, and comorbidities.
Hypersomnia is excessive daytime sleepiness and prolonged sleep duration despite adequate nighttime sleep. Patients may experience persistent drowsiness, difficulty staying awake during daytime hours, and episodes of unintentional sleep. The severity of hypersomnia can range from mild sleepiness to severe impairment of wakefulness, leading to functional impairment, decreased productivity, and increased risk of accidents or injuries. Severe hypersomnia may interfere with daily activities and social functioning, contributing to the overall disease burden in affected individuals [45].
Fragmented sleep patterns are characterized by frequent awakenings at night, disrupting sleep continuity, and poor sleep quality [46]. Patients may experience multiple brief awakenings, difficulty maintaining deep or REM sleep stages, and a sense of non-restorative sleep. The severity of fragmented sleep patterns can vary depending on the frequency and duration of awakenings and their impact on sleep architecture and overall sleep quality. Severe fragmentation of sleep may lead to sleep deprivation, fatigue, and cognitive impairment, exacerbating the burden of disease in affected individuals [47].
Circadian rhythm disturbances involve disruptions in the timing and regularity of sleep-wake cycles, leading to irregular sleep patterns and difficulty maintaining a consistent sleep schedule. Patients may experience variations in sleep onset and wake times, as well as fluctuations in daytime alertness and sleep quality. The severity of circadian rhythm disturbances can range from mild deviations in sleep timing to severe misalignment of the internal clock, resulting in significant sleep fragmentation and daytime dysfunction. Severe circadian disruptions may exacerbate other sleep-related symptoms and contribute to the overall severity of sleeping sickness [48].
In addition to primary sleep disturbances, African trypanosomiasis can cause various neurological symptoms that indirectly impact sleep, such as headaches, confusion, hallucinations, and motor disturbances [49]. These symptoms may exacerbate sleep-related difficulties and contribute to the severity of sleep disturbances in affected individuals. The severity of neurological symptoms can vary depending on the stage and progression of the disease, as well as individual differences in susceptibility and host response. Severe neurological manifestations may further compromise sleep quality and exacerbate the functional impairment associated with sleeping sickness.
3.3. Differential Diagnosis Challenges
The diagnosis of African trypanosomiasis, particularly in its early stages, presents several challenges due to the nonspecific nature of its symptoms and overlapping clinical features with other infectious and non-infectious conditions. Differential diagnosis requires careful consideration of epidemiological factors, clinical presentation, and laboratory findings to distinguish sleeping sickness from other diseases with similar manifestations.
The early symptoms of African trypanosomiasis, such as fever, headache, malaise, and joint pain, are nonspecific and can mimic many infectious diseases prevalent in endemic regions, including malaria, typhoid fever, and viral illnesses [50]. Healthcare providers must maintain a high index of suspicion for African trypanosomiasis in individuals presenting with fever and other constitutional symptoms, particularly in endemic areas. Comprehensive clinical evaluation, including travel history and exposure to tsetse flies, can help narrow the list of differential diagnoses.
Neurological symptoms, such as confusion, behavioral changes, and motor disturbances, are common in African trypanosomiasis but can also occur in other neurological conditions, including meningitis, encephalitis, and cerebral malaria [51]. Detailed neurological assessment, including evaluation of mental status, cranial nerve function, and motor coordination, is essential for distinguishing sleeping sickness from other causes of neurological impairment. Cerebrospinal fluid analysis, neuroimaging studies, and electroencephalography may provide valuable diagnostic information in cases of suspected CNS involvement.
African trypanosomiasis can present with variable disease progression, ranging from an acute, rapidly progressing form (T. b. rhodesiense) to a chronic, slowly evolving form (T. b. gambiense). The clinical course may be influenced by host immune response, parasite strain, and co-infections. Recognizing the different clinical patterns associated with T. b. rhodesiense and T. b. gambiense infections is essential for guiding diagnostic and treatment decisions. Epidemiological information, such as the geographical distribution of the parasite and the patient's travel history, can help differentiate between the two subtypes of African trypanosomiasis [52].
Laboratory confirmation of African trypanosomiasis relies on parasitological techniques, such as microscopic examination of blood, lymph node aspirates, or cerebrospinal fluid for the presence of trypanosomes [53]. However, the sensitivity and specificity of these tests can be variable, particularly in cases of low parasitemia or atypical clinical presentation. Clinicians should consider complementary diagnostic tests, such as serological assays (e.g., enzyme-linked immunosorbent assay, immunofluorescence), polymerase chain reaction (PCR) assays, or rapid diagnostic tests, to enhance the sensitivity and specificity of laboratory diagnosis. Repeat testing may be necessary to confirm the diagnosis, especially in cases with clinical suspicion but negative initial results.
Coinfections with other infectious pathogens, such as HIV, tuberculosis, or parasitic diseases (e.g., malaria, schistosomiasis), are common in endemic regions and can complicate the clinical presentation of African trypanosomiasis [54]. Additionally, non-infectious conditions, such as autoimmune diseases or metabolic disorders, may present with symptoms overlapping with sleeping sickness. A comprehensive evaluation of the patient's medical history, physical examination findings, and laboratory results is necessary to identify potential coinfections or underlying comorbidities that may contribute to the clinical picture. Multidisciplinary collaboration between infectious disease specialists, neurologists, and other relevant healthcare providers is essential for accurate diagnosis and management.
4. Diagnostic Approaches
4.1. Polysomnography and Actigraphy
The application of polysomnography and actigraphy in the context of African trypanosomiasis presents several challenges and considerations due to the unique features of the disease and its impact on sleep architecture and patterns [55]. While these sleep monitoring techniques are valuable tools in assessing sleep disorders, their utility in the context of African trypanosomiasis may be limited by factors such as the availability of resources, patient mobility, and the feasibility of conducting sleep studies in affected regions.
Polysomnography (PSG) is the gold standard for diagnosing sleep disorders. It offers comprehensive monitoring of physiological parameters during sleep, including brain activity (EEG), eye movements (EOG), muscle tone (EMG), and respiratory variables [56]. Conducting PSG in the context of African trypanosomiasis presents logistical challenges, particularly in endemic regions with limited access to healthcare infrastructure and specialized sleep laboratories. The availability of trained personnel, equipment, and facilities for conducting PSG may be scarce in these areas. PSG may be feasible in research settings or specialized facilities that handle sleep studies in endemic regions. However, its implementation may be limited by cost, infrastructure, and the need for overnight stays, which can be impractical for patients in remote areas. Despite these challenges, PSG may be valuable for studying the impact of African trypanosomiasis on sleep architecture, respiratory function, and neurological manifestations [57]. Research using PSG could provide insights into the pathophysiology of sleep disturbances in sleeping sickness and inform the development of targeted interventions.
Actigraphy is a non-invasive method for monitoring sleep-wake patterns and physical activity using a portable device worn on the wrist [58]. It provides objective data on sleep duration, sleep onset latency, wake after sleep onset, and overall sleep efficiency over extended periods. Actigraphy offers several advantages for studying sleep disturbances in African trypanosomiasis, particularly in resource-limited settings [59]. It is portable, easy to use, and well-suited for monitoring sleep patterns in naturalistic environments, such as patients' homes or community settings. Actigraphy may be a valuable tool for assessing sleep disturbances and circadian rhythm disruptions in individuals with sleeping sickness. Longitudinal monitoring using actigraphy could help characterize sleep-wake patterns, identify trends over time, and evaluate the effectiveness of interventions in managing sleep-related symptoms. While actigraphy is less resource-intensive than PSG, its accuracy in detecting sleep-wake patterns may be affected by factors such as movement artifacts, environmental conditions, and comorbidities. Interpretation of actigraphy data requires careful consideration of these factors and validation against other measures of sleep.
4.2. Biomarkers and Laboratory Testing
Biomarkers and laboratory testing play crucial roles in diagnosing, monitoring, and managing African trypanosomiasis. These tools aid in detecting the parasite, assessing disease severity, evaluating treatment response, and identifying potential complications.
Microscopic examination of blood smears remains the primary method for diagnosing African trypanosomiasis. Giemsa-stained blood smears are examined for the presence of trypanosomes, which appear as slender, motile organisms within the blood. In cases of suspected central nervous system involvement, cerebrospinal fluid (CSF) analysis is performed to detect trypanosomes and assess inflammatory markers. CSF examination may reveal elevated white blood cell counts, protein levels, and the presence of trypanosomes, indicating meningoencephalitis.
Human African Trypanosomiasis is classified into three subclasses according to the number of white blood cells (WBCs) on the CSF [60]. The first (hemo-lymphatic) stage is characterized by less than five WBCs and no trypanosomes in CSF. The second stage can be divided into meningoencephalitis (early second stage) and severe meningoencephalitis (severe second stage). In this context, the early second stage has more than five WBCs, and the severe second stage has more than 100 WBCs. Interestingly, the second stage is independent of the presence of trypanosomes in CSF.
Serological assays, such as ELISA, detect specific antibodies against Trypanosoma brucei antigens in serum or plasma samples. ELISA can confirm the diagnosis of African trypanosomiasis and complement parasitological tests, particularly in cases of low parasitemia or extraneous tissue localization of the parasite [61]. The Card Agglutination Test for Trypanosomiasis (CATT) is a rapid serological test used for screening large populations in endemic areas [62]. It detects anti-trypanosome antibodies in serum or plasma samples and provides rapid results suitable for mass screening campaigns.
PCR-based assays amplify and detect Trypanosoma brucei DNA from various biological samples, including blood, CSF, and tissue specimens [63]. PCR offers high sensitivity and specificity and can detect low levels of parasitemia, making it valuable for diagnosing early or latent infections and monitoring treatment response. Loop-Mediated Isothermal Amplification (LAMP) is an isothermal nucleic acid amplification technique that detects T. brucei DNA with high sensitivity and specificity [64]. LAMP assays are particularly useful in resource-limited settings due to their simplicity, rapidity, and minimal equipment requirements.
Measuring pro-inflammatory cytokines and inflammatory markers in serum or CSF samples provides insights into the host immune response to Trypanosoma brucei infection [65]. Elevated levels of cytokines may indicate active infection, disease progression, or treatment response. CRP is an acute-phase reactant that increases in response to inflammation. Elevated CRP levels may reflect systemic inflammation associated with African trypanosomiasis and can be a marker of disease severity or treatment response.
Hematological abnormalities, such as anemia, leukopenia, and thrombocytopenia, are commonly observed in African trypanosomiasis and can provide valuable diagnostic information. CBC analysis helps assess disease severity, monitor hematological changes during treatment, and identify potential complications. Measurement of liver enzymes and renal function markers helps in assessing organ dysfunction and monitoring for drug-related toxicity during treatment.
4.3. Neuroimaging Techniques
Neuroimaging techniques are vital in assessing neurological complications associated with African trypanosomiasis, particularly in CNS involvement.
CT imaging provides detailed cross-sectional images of the brain, allowing visualization of structural abnormalities, such as brain atrophy, hydrocephalus, and focal lesions. CT scans help detect gross structural changes in the brain, particularly in cases of advanced neurological involvement or complications such as meningoencephalitis or intracranial hemorrhage [66].
MRI is the imaging modality for evaluating CNS involvement in African trypanosomiasis [67]. It can detect characteristic findings such as hyperintense signal changes in the basal ganglia, thalamus, and brainstem on T2-weighted and FLAIR sequences, indicative of encephalitic involvement. MRI also helps identify complications such as cerebral edema, demyelination, and ischemic lesions [68].
DTI can provide insights into microstructural changes in white matter integrity, such as axonal degeneration, demyelination, and gliosis, which may occur in neurological diseases such as African trypanosomiasis [69]. DTI can detect subtle alterations in white matter connectivity and assess the extent of damage to neuronal pathways.
fMRI is valuable for studying functional alterations in the brain associated with African trypanosomiasis, such as changes in cerebral perfusion, connectivity disruptions, and alterations in neural networks involved in motor, cognitive, and emotional processing [70]. fMRI can provide insights into the pathophysiology of neurological symptoms and guide rehabilitation strategies.
PET imaging can assess metabolic changes and neuroinflammatory responses in the brain associated with African trypanosomiasis. It may help identify regions of increased glucose uptake, microglial activation, or neuroreceptor alterations, providing valuable insights into disease pathogenesis and potential targets for therapeutic intervention.
5. Management Strategies
5.1. Pharmacological Interventions
Pharmacological interventions for African trypanosomiasis, caused by Trypanosoma brucei parasites, aim to eliminate the parasites from the body, control disease progression, and manage symptoms. Treatment choice depends on the disease stage, the parasite species involved (T. b. gambiense or T. b. rhodesiense), and individual patient factors (Table 2) [71].
For early-stage T. b. gambiense infection, the drugs of choice include pentamidine and suramin [72]. Pentamidine is administered intramuscularly or intravenously, while suramin is given intravenously. These drugs effectively treat early-stage infection and prevent progression to the CNS. Late-stage T. b. gambiense infection and T. b. rhodesiense infection typically involve CNS penetration, requiring drugs that can cross the blood-brain barrier. Drugs such as melarsoprol, eflornithine, and nifurtimox are used for late-stage infections [73]. Melarsoprol is administered intravenously and is effective against both T. b. gambiense and T. b. rhodesiense. Eflornithine, often used with nifurtimox, is preferred for T. b. gambiense infections due to its better safety profile.
Suramin, followed by melarsoprol, is the recommended treatment regimen for T. b. rhodesiense infection [74]. Suramin is initially administered intravenously, followed by melarsoprol, also given intravenously. This combination therapy effectively treats both early and late stages of T. b. rhodesiense infection.
Eflornithine-nifurtimox combination therapy is recommended as the first-line treatment for late-stage T. b. gambiense infection, particularly in areas with prevalent melarsoprol resistance [75]. Eflornithine is administered intravenously, often in combination with oral nifurtimox, and is associated with lower toxicity compared to melarsoprol.
In addition to specific trypanocidal medications, supportive therapy may be necessary to manage symptoms and complications associated with African trypanosomiasis. This may include treatment for fever, pain, inflammation, and neurological symptoms. Patients with severe disease may require hospitalization and supportive care to address fluid and electrolyte imbalances, nutritional deficiencies, and organ dysfunction.
Pharmacological interventions for African trypanosomiasis carry risks of adverse effects and toxicity, necessitating careful monitoring of patients during treatment. Close monitoring for drug-related adverse events, such as nephrotoxicity, hepatotoxicity, neurotoxicity, and cardiac toxicity, is essential. Laboratory tests, including renal and hepatic function tests, complete blood count, and electrocardiography, may be performed to assess treatment safety and efficacy.
Continuous surveillance for drug resistance is critical for monitoring the effectiveness of pharmacological interventions and informing treatment guidelines. Surveillance involves monitoring parasite susceptibility to antitrypanosomal drugs and identifying emerging resistance patterns. Strategies for mitigating drug resistance include combination therapy, drug rotation, and the development of novel therapeutics.
5.2. Non-Pharmacological Therapies
Non-pharmacological therapies support the management of African trypanosomiasis, particularly in addressing symptoms, promoting patient comfort, and improving overall well-being. While pharmacological interventions target eradicating the parasite and controlling the disease, non-pharmacological therapies focus on supportive care and adjunctive measures to enhance treatment outcomes.
Non-pharmacological approaches such as heat therapy, massage, and physical therapy techniques can help alleviate pain and discomfort associated with African trypanosomiasis [76]. These modalities may be particularly beneficial for managing musculoskeletal pain, joint stiffness, and neuropathic pain. Cooling measures, such as tepid sponging, cool baths, and air conditioning, can help reduce fever and promote patient comfort. Hydration and fluid intake are essential to prevent dehydration and fever-related electrolyte imbalances. Nutritional counseling and supplementation may be necessary to address malnutrition and dietary deficiencies commonly observed in patients with African trypanosomiasis. A balanced diet rich in protein, vitamins, and minerals supports immune function, tissue repair, and overall health.
Physical therapy interventions, including range of motion exercises, gait training, and balance exercises, help improve mobility and functional independence in patients with neurological deficits. Rehabilitation programs tailored to individual needs can address motor impairments, muscle weakness, and coordination difficulties. Occupational therapy focuses on restoring activities of daily living, cognitive function, and vocational skills in individuals with neurological sequelae of African trypanosomiasis [77]. Adaptive equipment, assistive devices, and environmental modifications may be recommended to promote independence and quality of life. Speech therapy interventions target communication and swallowing difficulties in patients with dysarthria, dysphagia, or cognitive communication impairments. Speech-language pathologists assess speech and language function and develop personalized treatment plans to optimize communication and swallowing function.
Psychosocial support services, including individual counseling, group therapy, and family counseling, address psychological distress, anxiety, depression, and adjustment difficulties in patients with African trypanosomiasis [78]. Counseling interventions focus on coping strategies, stress management, and psychosocial adjustment to the disease and its consequences. Building strong social support networks, including family, friends, community members, and support groups, provides emotional support, practical assistance, and encouragement to patients and their caregivers. Peer support networks and community-based organizations are valuable in reducing isolation, stigma, and social barriers to care.
Patient education programs provide information about African trypanosomiasis, its transmission, symptoms, treatment, and preventive measures. Empowering patients with knowledge about the disease promotes treatment adherence, self-management skills, and early recognition of complications. Community-based health education initiatives raise awareness about sleeping sickness, vector control strategies, and the importance of early diagnosis and treatment. Health promotion activities, including community meetings, radio broadcasts, and educational campaigns, mobilize community members to participate in disease prevention and control efforts.
Environmental interventions targeting tsetse fly habitat reduction, insecticide spraying, and insecticide-treated bed nets help reduce tsetse fly populations and prevent transmission of Trypanosoma brucei parasites [79]. Community-based vector control programs and integrated pest management strategies contribute to sustainable control of sleeping sickness. Improving access to clean water, sanitation facilities, and hygiene practices reduces the risk of disease transmission and secondary infections in endemic regions. Health education programs promote proper sanitation, hand hygiene, and waste management practices to prevent the spreading of infectious diseases.
6. Impact on Public Health and Socioeconomic Burden
6.1. Global Health Implications
The global health implications of African trypanosomiasis extend beyond the affected regions, impacting public health, socio-economic development, and healthcare systems worldwide.
African trypanosomiasis is classified as one of the neglected tropical diseases (NTDs), a group of infectious diseases affecting marginalized populations in low-resource settings. The burden of NTDs, including sleeping sickness, extends beyond endemic regions and contributes to the global health disparity, particularly affecting the most vulnerable and marginalized communities [80].
The socio-economic burden of African trypanosomiasis is substantial, affecting individuals, families, and communities in endemic regions [81]. The disease primarily affects rural populations engaged in agriculture, livestock farming, and other primary economic activities. Loss of productivity due to illness, disability, and premature death hampers economic growth, exacerbates poverty, and perpetuates cycles of deprivation.
Diagnosing, treating, and controlling African trypanosomiasis pose significant challenges to healthcare systems in endemic regions [82]. Limited healthcare infrastructure, inadequate resources, and a staff shortage impede efforts to effectively prevent, diagnose, and treat sleeping sickness. The burden on health systems further undermines their capacity to address other health priorities and deliver essential health services.
African trypanosomiasis threatens global health security because it can spread beyond endemic regions through human migration, travel, and trade. The movement of infected individuals, asymptomatic carriers, and animal reservoirs increases the risk of disease transmission to non-endemic areas, raising concerns about the emergence of new foci of infection and potential outbreaks [83].
Despite advances in diagnosis, treatment, and control efforts, African trypanosomiasis remains a challenging and neglected disease. A sustained investment in research and development is needed to develop new diagnostic tools, safer and more effective treatments, and innovative control strategies. Collaborative efforts between researchers, policymakers, pharmaceutical companies, and funding agencies are essential to accelerate progress in combating sleeping sickness.
The interconnectedness of global health systems underscores the importance of addressing African trypanosomiasis as part of broader efforts to strengthen health systems, promote universal health coverage, and achieve sustainable development goals. Addressing neglected tropical diseases, including sleeping sickness, requires a multisectoral approach, integrating health, agriculture, environmental, and socio-economic interventions.
6.2. Socioeconomic Factors Influencing Disease Burden
Socioeconomic factors significantly influence the disease burden of African trypanosomiasis. In this context, poverty is a significant driver of African trypanosomiasis, with endemic regions characterized by high levels of poverty, food insecurity, and limited access to healthcare services [84]. Poverty exacerbates the risk of disease transmission through inadequate housing, poor sanitation, and lack of resources for vector control and healthcare infrastructure.
African trypanosomiasis predominantly affects rural communities engaged in agriculture, livestock farming, and other primary economic activities [85]. Agricultural practices, such as slash-and-burn cultivation, deforestation, and encroachment into wildlife habitats, increase human-tsetse fly contact and contribute to disease transmission in endemic regions. Livestock, particularly cattle, serve as reservoir hosts for Trypanosoma brucei parasites, sustaining transmission cycles in endemic areas. Livestock ownership and animal husbandry practices, such as extensive grazing and mixed farming systems, influence the risk of human exposure to tsetse flies and contribute to disease transmission among humans and animals.
Gender dynamics shape the distribution of disease burden and access to healthcare services in endemic regions. Women and girls may bear a disproportionate burden of caregiving responsibilities, increasing their risk of exposure to tsetse flies during domestic activities such as fetching water, collecting firewood, and tending to livestock [86].
Population mobility, including rural-urban migration, seasonal movements, and displacement due to conflict or environmental factors, influences the spread of African trypanosomiasis beyond endemic regions [87]. Migration patterns contribute to disseminating infected individuals, asymptomatic carriers, and animal reservoirs, potentially seeding new foci of infection.
Social determinants of health, such as education, literacy, and access to information, influence health-seeking behaviors, preventive practices, and treatment adherence among affected populations. Limited health literacy, cultural beliefs, and stigma associated with sleeping sickness may hinder early diagnosis, treatment uptake, and disease control efforts [88].
African trypanosomiasis significantly burdens affected communities, reducing productivity, agricultural output, and household income. Illness, disability, and premature death due to sleeping sickness undermine human capital development, perpetuate cycles of poverty, and impede socio-economic development in endemic regions.
7. Psychological Impact of Sleep Disorders
The psychological impact of sleep disorders can be profound, affecting various aspects of mental health, cognitive function, emotional well-being, and quality of life. Sleep disorders disrupt normal sleep patterns, leading to sleep fragmentation, reduced sleep duration, poor sleep quality, and daytime sleepiness, which can exacerbate psychological distress and impair overall functioning [89].
Sleep disorders are strongly associated with mood disturbances, including depression and anxiety disorders. Chronic sleep deprivation and disrupted sleep patterns can exacerbate symptoms of mood disorders and increase the risk of developing depressive or anxiety symptoms [90]. Conversely, mood disorders can also contribute to sleep disturbances, creating a bidirectional relationship between sleep and mental health.
Sleep is critical in cognitive function, including attention, memory, executive function, and decision-making [91]. Sleep disorders impair cognitive performance, leading to difficulties in concentration, memory consolidation, problem-solving, and information processing. Cognitive dysfunction due to sleep disorders can negatively impact academic, occupational, and daily functioning.
Adequate sleep is essential for emotional regulation and resilience to stress. Sleep disorders disrupt the balance of neurotransmitters involved in mood regulation, such as serotonin, dopamine, and norepinephrine, leading to heightened emotional reactivity, irritability, and emotional instability [92]. Individuals with sleep disorders may experience mood swings, emotional outbursts, and difficulty coping with stressors. Sleep disorders impair daytime functioning and performance across various domains, including work, school, social interactions, and leisure activities. Excessive daytime sleepiness, fatigue, and reduced alertness due to sleep disorders can lead to decreased productivity, impaired concentration, accidents, and errors in judgment. Chronic sleep deprivation further exacerbates these effects, compromising overall functioning and safety. Sleep disorders significantly impact the overall quality of life, affecting physical health, mental well-being, social relationships, and overall life satisfaction. Sleep disturbances can lead to decreased energy levels, reduced motivation, social withdrawal, and diminished enjoyment of activities. Poor sleep quality and daytime dysfunction contribute to impaired quality of life and subjective well-being. Sleep disorders are associated with an increased risk of developing psychiatric disorders, including mood disorders, anxiety disorders, psychotic disorders, and substance use disorders. Insomnia, in particular, is a common precursor to depression and anxiety disorders, while sleep disturbances are prevalent in individuals with schizophrenia, bipolar disorder, and substance use disorders. Sleep disorders can strain interpersonal relationships and family dynamics, affecting communication, emotional intimacy, and mutual support. Partners of individuals with sleep disorders may experience disrupted sleep themselves, leading to conflicts, resentment, and relationship dissatisfaction. Sleep disturbances in children can also impact family functioning and parental well-being.
8. Prevention and Control Measures
8.1. Vector Control Strategies
Vector control strategies are essential to comprehensive efforts to prevent and control African trypanosomiasis, a vector-borne disease transmitted by tsetse flies. These strategies aim to reduce the population of tsetse flies, interrupt disease transmission, and minimize human-vector contact. Effective vector control measures not only prevent new infections but also contribute to eliminating and eradicating the disease.
Altering or eliminating tsetse fly habitat can reduce the density of tsetse fly populations and minimize human-vector contact [93]. Habitat modification may involve clearing vegetation, draining swampy areas, removing dense undergrowth, and improving land use practices to create less favorable breeding and resting sites for tsetse flies.
Insecticide-treated targets, such as cloth or canvas traps impregnated with insecticides, attract and kill tsetse flies when they come into contact with the treated surfaces [94]. Targets are strategically placed in areas with high tsetse fly density, such as riverbanks, forest edges, and animal resting sites, to lure and eliminate the flies. Insecticide-treated targets are cost-effective and environmentally friendly alternatives to aerial spraying.
Treating cattle with insecticides, such as pour-on formulations or insecticide-impregnated ear tags, can reduce tsetse fly infestations and interrupt disease transmission to livestock. Insecticide-treated cattle act as "bait" for tsetse flies, attracting them to the treated animals and decreasing the likelihood of transmission to humans [95]. Insecticide-treated cattle are particularly effective in areas where animal husbandry is a primary transmission mode.
The sterile insect technique involves mass-rearing tsetse flies in insectaries, sterilizing them using ionizing radiation, and releasing them into target areas to mate with wild tsetse flies [96]. Sterile matings result in infertile eggs, gradually reducing the tsetse fly population. SIT has been successfully used to control tsetse flies in small-scale pilot projects and is being explored for larger-scale implementation.
Trapping and monitoring tsetse fly populations provide valuable data for assessing the effectiveness of vector control interventions and guiding surveillance activities [97]. Various trap designs, such as biconical traps, pyramidal traps, and sticky traps, are used to capture tsetse flies for monitoring purposes. Trapping surveys help identify high-risk areas, monitor changes in tsetse fly abundance, and evaluate the impact of control measures.
Engaging local communities in vector control efforts through education, awareness campaigns, and community-based interventions promotes sustainable disease control and fosters ownership of control activities. Community participation in habitat modification, trap deployment, and insecticide application enhances the effectiveness and acceptability of vector control strategies.
Integrated vector management combines multiple vector control interventions, including environmental management, insecticide application, biological control, and community engagement, to achieve sustainable and cost-effective control of tsetse flies and other vectors [98]. IVM emphasizes using evidence-based approaches tailored to local epidemiological, ecological, and socio-economic contexts.
8.2. Public Health Education and Awareness
Public health education and awareness campaigns are crucial to preventing and controlling African trypanosomiasis [99]. These initiatives aim to increase knowledge, raise awareness, promote behavior change, and empower communities to take action against the disease. Public health education and awareness activities target stakeholders, including affected populations, healthcare providers, policymakers, and the general public.
Providing accurate, culturally appropriate information about African trypanosomiasis, its transmission, symptoms, prevention, diagnosis, and treatment is essential for raising awareness and dispelling myths and misconceptions [100]. Information materials, such as brochures, posters, leaflets, and fact sheets, are distributed through community outreach activities, health facilities, schools, and media channels.
Engaging local communities in the planning, implementing, and evaluating public health interventions fosters ownership, participation, and sustainability [101]. Community meetings, focus group discussions, participatory workshops, and door-to-door outreach sessions facilitate dialogue, knowledge sharing, and collaborative problem-solving. Community leaders, traditional healers, and religious authorities are essential in mobilizing community support and promoting health-seeking behaviors.
Integrating health education into school curricula and extracurricular activities gives children, adolescents, and their families critical messages about preventing and controlling sleeping sickness. Educational materials, interactive workshops, drama skits, and peer-led initiatives raise awareness among students about the importance of personal hygiene, vector control, and seeking prompt medical care for suspected symptoms.
Training healthcare providers, including doctors, nurses, community health workers, and traditional birth attendants, enhances their capacity to recognize, diagnose, and manage cases of African trypanosomiasis [102]. Continuing education programs, workshops, and practical training sessions equip frontline health workers with the knowledge and skills to deliver quality care, conduct active case detection, and promote preventive measures.
Leveraging mass media channels, such as radio, television, newspapers, and social media, amplifies public health messages and reaches diverse audiences across urban and rural areas. Public service announcements, radio dramas, televised documentaries, and social media campaigns raise awareness about sleeping sickness, encourage behavior change, and promote community participation in control efforts.
Collaborating with diverse stakeholders, including government agencies, non-governmental organizations, international partners, and academic institutions, strengthen the impact of public health education and awareness initiatives. Intersectoral partnerships facilitate resource mobilization, coordination of activities, and integration of sleeping sickness control into broader health and development agendas.
Monitoring and evaluating public health education and awareness campaigns assess their reach, effectiveness, and impact on knowledge, attitudes, and practices related to African trypanosomiasis. Surveys, focus group discussions, knowledge tests, and behavioral assessments provide feedback on campaign outcomes, identify areas for improvement, and inform future programming.
9. Future Perspectives
9.1. Future Research Directions
Future research directions in the field of African trypanosomiasis encompass a broad spectrum of scientific inquiries aimed at advancing our understanding of the disease, improving diagnostic tools, developing novel treatments, and enhancing control strategies.
Further elucidation of tsetse fly biology, behavior, and ecology to identify vulnerabilities and develop innovative vector control strategies. Exploration of genetic, molecular, and environmental factors influencing tsetse fly populations and disease transmission dynamics. Evaluation of novel vector control interventions, such as genetic modification, biological control agents, and environmental management techniques.
Investigate host-parasite interactions, immune responses, and disease pathogenesis to identify novel therapeutic targets and vaccine candidates. Characterization of parasite virulence factors, drug resistance mechanisms, and immune evasion strategies. Development of immune-based interventions, including vaccines, immunotherapies, and immune modulators, to enhance host immunity and control parasite replication.
Development of sensitive, specific, and field-deployable diagnostic tests for early detection of Trypanosoma brucei parasites and disease staging. Validation of novel diagnostic platforms, including point-of-care tests, molecular assays, serological markers, and imaging modalities. Integration of diagnostic tools into surveillance systems to enhance active case detection, monitor disease trends, and guide control interventions.
Discovery and optimization of new antitrypanosomal drugs with improved efficacy, safety, and pharmacokinetic profiles. Screening of compound libraries, natural products, and repurposed drugs for activity against Trypanosoma brucei parasites. Development of combination therapies, drug delivery systems, and drug formulations to overcome drug resistance, enhance treatment efficacy, and improve patient compliance.
Epidemiological studies to elucidate disease transmission cycles, identify reservoir hosts, and assess risk factors for human infection. Modeling approaches to predict disease spread, evaluate intervention strategies, and optimize resource allocation for disease control. Integrating molecular epidemiology, spatial mapping, and surveillance data to track parasite genotypes, monitor transmission hotspots, and guide targeted interventions.
Implementation research to evaluate the effectiveness, acceptability, and scalability of community-based interventions, health education programs, and behavior change strategies. Assessment of knowledge, attitudes, and practices related to sleeping sickness, vector control, and healthcare-seeking behavior among affected populations. Development of culturally sensitive communication strategies, social mobilization campaigns, and community empowerment approaches to promote disease awareness and participation in control efforts.
9.2. Clinical Implications and Challenges
The clinical implications of African trypanosomiasis encompass a range of challenges related to diagnosis, treatment, management, and prevention of the disease.
Sleeping sickness presents diagnostic challenges due to its nonspecific symptoms and overlap with other febrile illnesses endemic to sub-Saharan Africa. Limited access to diagnostic facilities, lack of trained personnel, and variability in parasite detection methods hinder timely and accurate diagnosis. Differentiating between the two forms of sleeping sickness (T.b. gambiense and T.b. rhodesiense) is essential for guiding treatment decisions. Still, it may require specialized laboratory tests that are not widely available in endemic regions.
The toxicity, route of administration, and limited availability of existing drugs complicate the treatment of sleeping sickness. First-line therapies, such as pentamidine and suramin for early-stage disease and melarsoprol and eflornithine for late-stage disease, have drawbacks, including adverse effects, parenteral administration, and challenges in procurement and distribution. Drug resistance, particularly to melarsoprol, poses a significant threat to treatment efficacy and patient outcomes. The development of resistance further complicates treatment regimens and necessitates alternative therapeutic options.
Late-stage sleeping sickness is characterized by neurological involvement, including meningoencephalitis, cognitive impairment, and motor dysfunction. Managing neurological complications requires specialized care, supportive therapy, and rehabilitation services to address functional limitations, cognitive deficits, and psychiatric symptoms. Neurological sequelae of sleeping sickness may persist even after successful treatment of the underlying infection, highlighting the need for long-term follow-up and multidisciplinary care to optimize outcomes.
Access to healthcare services is limited in many endemic regions, with scarce infrastructure, resources, and skilled personnel. Remote and marginalized communities face barriers to healthcare access, including geographical distance, transportation challenges, financial constraints, and cultural beliefs. Strengthening healthcare systems, expanding coverage of diagnostic and treatment facilities, and training local healthcare providers are critical for improving access to care and reducing morbidity and mortality associated with sleeping sickness.
Preventing sleeping sickness relies on vector control measures, such as insecticide-treated targets, trapping, and habitat modification, to reduce tsetse fly populations and interrupt disease transmission. Sustainable vector control strategies require community participation, intersectoral collaboration, and long-term infrastructure and capacity-building investment. Health education, awareness campaigns, and behavior change interventions promote preventive practices, such as using insecticide-treated bed nets, wearing protective clothing, and seeking early medical care for suspected symptoms. Targeting at-risk populations, such as travelers, migrant workers, and indigenous communities, enhances the effectiveness of preventive strategies.
10. Conclusion
In conclusion, African trypanosomiasis, or sleeping sickness, remains a significant public health concern in sub-Saharan Africa, posing clinical, social, and economic challenges to affected populations. The disease is characterized by complex epidemiology, diagnostic difficulties, limited treatment options, and neurological sequelae, highlighting the need for comprehensive prevention, diagnosis, and management approaches. Despite progress in research and control efforts, several key issues persist, including diagnostic limitations, treatment toxicity, healthcare access disparities, and vector control challenges. Addressing these challenges requires sustained investment in research, innovation, capacity building, and intersectoral collaboration to develop practical tools and strategies for combating sleeping sickness. Public health education, community engagement, and advocacy are critical for raising awareness, mobilizing resources, and promoting behavior change to prevent and control sleeping sickness. By empowering communities, strengthening healthcare systems, and advancing scientific knowledge, we can work towards eliminating sleeping sickness as a public health threat and improving the health and well-being of affected populations.
Author Contributions
Conceptualization, J.P.R., V.V.B., and A.L.F.C.; methodology, A.L.F.C.; software, A.L.F.C.; validation, A.L.F.C., J.P.R. and V.V.B.; formal analysis, A.L.F.C.; investigation, A.L.F.C.; resources, A.L.F.C.; data curation, J.P.R.; writing—original draft preparation, J.P.R.; writing—review and editing, J.P.R.; visualization, V.V.B.; supervision, V.V.B.; project administration, V.V.B.; funding acquisition, J.P.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data created.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Büscher, P.; Cecchi, G.; Jamonneau, V.; Priotto, G. Human African Trypanosomiasis. The Lancet 2017, 390, 2397–2409. [Google Scholar] [CrossRef] [PubMed]
- Brun, R.; Blum, J.; Chappuis, F.; Burri, C. Human African Trypanosomiasis. The Lancet 2010, 375, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Martínez, Y.; Kouamé, M.G.; Bongomin, F.; Lakoh, S.; Henao-Martínez, A.F. Human African Trypanosomiasis (Sleeping Sickness)—Epidemiology, Clinical Manifestations, Diagnosis, Treatment, and Prevention. Current Tropical Medicine Reports 2023, 10, 222–234. [Google Scholar] [CrossRef] [PubMed]
- Baker, J. Epidemiology of African Sleeping Sickness.; Wiley Online Library, 1974; Vol. 20, pp. 29–50.
- Okwelum, N.; Onagbesan, O.; Shittu, O.; Famakinde, S.; Bemji, M.; Osinowo, O. PREVALENCE OF SAVANNAH-TYPE TRYPANOSOMA CONGOLENSE IN CATTLE IN SOUTH-WESTERN NIGERIA. Nigerian Journal of Animal Production 2024, 347–350. [Google Scholar] [CrossRef]
- Rutto, J.J.; Osano, O.; Thuranira, E.G.; Kurgat, R.K.; Odenyo, V.A.O. Socio-Economic and Cultural Determinants of Human African Trypanosomiasis at the Kenya - Uganda Transboundary. PLoS Negl Trop Dis 2013, 7, e2186. [Google Scholar] [CrossRef]
- Jones, B.A.; Grace, D.; Kock, R.; Alonso, S.; Rushton, J.; Said, M.Y.; McKeever, D.; Mutua, F.; Young, J.; McDermott, J.; et al. Zoonosis Emergence Linked to Agricultural Intensification and Environmental Change. Proc Natl Acad Sci U S A 2013, 110, 8399–8404. [Google Scholar] [CrossRef]
- Yadav, N.; Upadhyay, R.K. Global Effect of Climate Change on Seasonal Cycles, Vector Population and Rising Challenges of Communicable Diseases: A Review. Journal of Atmospheric Science Research 2023, 6, 21–59. [Google Scholar] [CrossRef]
- Kikwai, C.; Ngeiywa, M. Review on the Socio-Economic Impacts of Trypanosomiasis. 2022.
- John, M.A.; Bankole, I.; Ajayi-Moses, O.; Ijila, T.; Jeje, O.; Lalit, P. Relevance of Advanced Plant Disease Detection Techniques in Disease and Pest Management for Ensuring Food Security and Their Implication: A Review. American Journal of Plant Sciences 2023, 14, 1260–1295. [Google Scholar] [CrossRef]
- Garcia, L.S. Parasites. Diagnostic Microbiology of the Immunocompromised Host 2008, 283–330. [Google Scholar]
- Schaub, G.A.; Vogel, P.; Balczun, C. Parasite-Vector Interactions. Molecular Parasitology: Protozoan Parasites and their Molecules 2016, 431–489.
- Rodgers, J. Trypanosomiasis and the Brain. Parasitology 2010, 137, 1995–2006. [Google Scholar] [CrossRef]
- Matthews, K.R.; McCulloch, R.; Morrison, L.J. The Within-Host Dynamics of African Trypanosome Infections. Philos Trans R Soc Lond B Biol Sci 2015, 370, 20140288. [Google Scholar] [CrossRef] [PubMed]
- Vickerman, K. Antigenic Variation in African Trypanosomes.; Wiley Online Library, 1974; pp. 53–80.
- Tesoriero, C.; Del Gallo, F.; Bentivoglio, M. Sleep and Brain Infections. Brain Res Bull 2019, 145, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Kristensson, K.; Nygård, M.; Bertini, G.; Bentivoglio, M. African Trypanosome Infections of the Nervous System: Parasite Entry and Effects on Sleep and Synaptic Functions. Prog Neurobiol 2010, 91, 152–171. [Google Scholar] [CrossRef] [PubMed]
- Imeri, L.; Opp, M.R. How (and Why) the Immune System Makes Us Sleep. Nat Rev Neurosci 2009, 10, 199–210. [Google Scholar] [CrossRef]
- Chakroborty, N.K.; Baksi, S.; Bhattacharya, A. Cognitive Impairment in Parasitic Protozoan Infection. In Pathobiology of Parasitic Protozoa: Dynamics and Dimensions; Springer, 2023; pp. 61–94.
- MOTIVALA, S.J.; IRWIN, M. Immunologic Changes.
- Bouteille, B.; Dumas, M. Human African Trypanosomiasis, Sleeping Sickness. In Tropical Neurology; CRC Press, 2003; pp. 325–343.
- Feuth, T. Interactions between Sleep, Inflammation, Immunity and Infections: A Narrative Review. Immun Inflamm Dis 2024, 12, e70046. [Google Scholar] [CrossRef]
- Combes, V.; Grau, G.E. 11 Cytokines and Defense and Pathology of the CNS. Cytokines and the CNS 2005, 243. [Google Scholar]
- Maestroni, G.J.M. Role of Melatonin in Viral, Bacterial and Parasitic Infections. Biomolecules 2024, 14. [Google Scholar] [CrossRef]
- Buijs, R.M.; van Eden, C.G.; Goncharuk, V.D.; Kalsbeek, A. The Biological Clock Tunes the Organs of the Body: Timing by Hormones and the Autonomic Nervous System. J Endocrinol 2003, 177, 17–26. [Google Scholar] [CrossRef]
- Stibbs, H.H. Neurochemical and Activity Changes in Rats Infected with Trypanosoma Brucei Gambiense. J Parasitol 1984, 70, 428–432. [Google Scholar] [CrossRef]
- Montague, P.; Bradley, B.; Rodgers, J.; Kennedy, P.G.E. Microarray Profiling Predicts Early Neurological and Immune Phenotypic Traits in Advance of CNS Disease during Disease Progression in Trypanosoma. b. Brucei Infected CD1 Mouse Brains. PLoS Negl Trop Dis 2021, 15, e0009892. [Google Scholar] [CrossRef]
- Chaves-Filho, A.J.M.; Macedo, D.S.; de Lucena, D.F.; Maes, M. Shared Microglial Mechanisms Underpinning Depression and Chronic Fatigue Syndrome and Their Comorbidities. Behav Brain Res 2019, 372, 111975. [Google Scholar] [CrossRef] [PubMed]
- Lamour, S.D.; Alibu, V.P.; Holmes, E.; Sternberg, J.M. Metabolic Profiling of Central Nervous System Disease in Trypanosoma Brucei Rhodesiense Infection. J Infect Dis 2017, 216, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- Nimgampalle, M.; Chakravarthy, H.; Sharma, S.; Shree, S.; Bhat, A.R.; Pradeepkiran, J.A.; Devanathan, V. Neurotransmitter Systems in the Etiology of Major Neurological Disorders: Emerging Insights and Therapeutic Implications. Ageing Res Rev 2023, 89, 101994. [Google Scholar] [CrossRef] [PubMed]
- Besedovsky, L.; Lange, T.; Haack, M. The Sleep-Immune Crosstalk in Health and Disease. Physiol Rev 2019, 99, 1325–1380. [Google Scholar] [CrossRef]
- Krueger, J.M.; Fang, J.; Floyd, R.A. Relationships between Sleep and Immune Function. Lung biology in health and disease 1999, 133, 427–427. [Google Scholar]
- Palagini, L.; Geoffroy, P.A.; Miniati, M.; Perugi, G.; Biggio, G.; Marazziti, D.; Riemann, D. Insomnia, Sleep Loss, and Circadian Sleep Disturbances in Mood Disorders: A Pathway toward Neurodegeneration and Neuroprogression? A Theoretical Review. CNS Spectr 2022, 27, 298–308. [Google Scholar] [CrossRef]
- Quintana, J.F.; Chandrasegaran, P.; Sinton, M.C.; Briggs, E.M.; Otto, T.D.; Heslop, R.; Bentley-Abbot, C.; Loney, C.; de Lecea, L.; Mabbott, N.A.; et al. Single Cell and Spatial Transcriptomic Analyses Reveal Microglia-Plasma Cell Crosstalk in the Brain during Trypanosoma Brucei Infection. Nat Commun 2022, 13, 5752. [Google Scholar] [CrossRef]
- Zielinski, M.R.; Gibbons, A.J. Neuroinflammation, Sleep, and Circadian Rhythms. Front Cell Infect Microbiol 2022, 12, 853096. [Google Scholar] [CrossRef]
- Steverding, D. Sleeping Sickness and Nagana Disease Caused by Trypanosoma Brucei. Arthropod borne diseases 2017, 277–297. [Google Scholar]
- Garbarino, S.; Lanteri, P.; Durando, P.; Magnavita, N.; Sannita, W.G. Co-Morbidity, Mortality, Quality of Life and the Healthcare/Welfare/Social Costs of Disordered Sleep: A Rapid Review. Int J Environ Res Public Health 2016, 13. [Google Scholar] [CrossRef]
- Ponte-Sucre, A. An Overview of Trypanosoma Brucei Infections: An Intense Host-Parasite Interaction. Front Microbiol 2016, 7, 2126. [Google Scholar] [CrossRef] [PubMed]
- Franco, J.R.; Simarro, P.P.; Diarra, A.; Jannin, J.G. Epidemiology of Human African Trypanosomiasis. Clin Epidemiol 2014, 6, 257–275. [Google Scholar] [CrossRef] [PubMed]
- Checchi, F.; Piola, P.; Ayikoru, H.; Thomas, F.; Legros, D.; Priotto, G. Nifurtimox plus Eflornithine for Late-Stage Sleeping Sickness in Uganda: A Case Series. PLoS Negl Trop Dis 2007, 1, e64. [Google Scholar] [CrossRef] [PubMed]
- Pépin, J.; Méda, H.A. The Epidemiology and Control of Human African Trypanosomiasis. Adv Parasitol 2001, 49, 71–132. [Google Scholar] [CrossRef]
- Hidalgo, J.; Ortiz, J.F.; Fabara, S.P.; Eissa-Garcés, A.; Reddy, D.; Collins, K.D.; Tirupathi, R. Efficacy and Toxicity of Fexinidazole and Nifurtimox Plus Eflornithine in the Treatment of African Trypanosomiasis: A Systematic Review. Cureus 2021, 13, e16881. [Google Scholar] [CrossRef]
- Zisapel, N. Sleep and Sleep Disturbances: Biological Basis and Clinical Implications. Cell Mol Life Sci 2007, 64, 1174–1186. [Google Scholar] [CrossRef]
- Papagni, R.; Novara, R.; Minardi, M.L.; Frallonardo, L.; Panico, G.G.; Pallara, E.; Cotugno, S.; Ascoli Bartoli, T.; Guido, G.; De Vita, E. Human African Trypanosomiasis (Sleeping Sickness): Current Knowledge and Future Challenges. Frontiers in Tropical Diseases 2023, 4, 1087003. [Google Scholar] [CrossRef]
- Kennedy, P.G.E. The Continuing Problem of Human African Trypanosomiasis (Sleeping Sickness). Ann Neurol 2008, 64, 116–126. [Google Scholar] [CrossRef]
- Medic, G.; Wille, M.; Hemels, M.E. Short- and Long-Term Health Consequences of Sleep Disruption. Nat Sci Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef]
- Bishir, M.; Bhat, A.; Essa, M.M.; Ekpo, O.; Ihunwo, A.O.; Veeraraghavan, V.P.; Mohan, S.K.; Mahalakshmi, A.M.; Ray, B.; Tuladhar, S.; et al. Sleep Deprivation and Neurological Disorders. Biomed Res Int 2020, 2020, 5764017. [Google Scholar] [CrossRef]
- Parish, J.M. Sleep-Related Problems in Common Medical Conditions. Chest 2009, 135, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Gamo, F.Z.; Djiogue, S.; Awounfack, C.F.; Nange, A.C.; Njamen, D. Neurological Disorders: The Use of Traditional Medicine in Cameroon. thought 2024, 1, 9. [Google Scholar] [CrossRef]
- Kozko, V.; Bondarenko, A.; Katsapov, D.; Krasnov, M.; Nikitina, N.; Gradil, G. Tropical Diseases. 2007.
- Walker, M.; Kublin, J.G.; Zunt, J.R. Parasitic Central Nervous System Infections in Immunocompromised Hosts: Malaria, Microsporidiosis, Leishmaniasis, and African Trypanosomiasis. Clin Infect Dis 2006, 42, 115–125. [Google Scholar] [CrossRef]
- Neuberger, A.; Meltzer, E.; Leshem, E.; Dickstein, Y.; Stienlauf, S.; Schwartz, E. The Changing Epidemiology of Human African Trypanosomiasis among Patients from Nonendemic Countries--1902-2012. PLoS One 2014, 9, e88647. [Google Scholar] [CrossRef]
- Chappuis, F.; Loutan, L.; Simarro, P.; Lejon, V.; Büscher, P. Options for Field Diagnosis of Human African Trypanosomiasis. Clin Microbiol Rev 2005, 18, 133–146. [Google Scholar] [CrossRef]
- Boraschi, D.; Abebe Alemayehu, M.; Aseffa, A.; Chiodi, F.; Chisi, J.; Del Prete, G.; Doherty, T.M.; Elhassan, I.; Engers, H.; Gyan, B.; et al. Immunity against HIV/AIDS, Malaria, and Tuberculosis during Co-Infections with Neglected Infectious Diseases: Recommendations for the European Union Research Priorities. PLoS Negl Trop Dis 2008, 2, e255. [Google Scholar] [CrossRef]
- BENTIVOGLIO, M.; BERTINI, G.; GRASSI-ZUCCONI, G.; ETET, P.S. Sleep Research in Africa: From Basic Neuroscience and Clinical Investigations to Health Management in Developing Countries.; Wiley Online Library, 2010; p. 6.
- Kayabekir, M. Sleep Physiology and Polysomnogram, Physiopathology and Symptomatology in Sleep Medicine. Updates in Sleep Neurology and Obstructive Sleep Apnea 2019. [Google Scholar]
- Buguet, A.; Bourdon, L.; Bouteille, B.; Cespuglio, R.; Vincendeau, P.; Radomski, M.W.; Dumas, M. The Duality of Sleeping Sickness: Focusing on Sleep. Sleep Med Rev 2001, 5, 139–153. [Google Scholar] [CrossRef]
- Hussain, Z.; Sheng, Q.Z.; Zhang, W.E.; Ortiz, J.; Pouriyeh, S. Non-Invasive Techniques for Monitoring Different Aspects of Sleep: A Comprehensive Review. ACM Transactions on Computing for Healthcare (HEALTH) 2022, 3, 1–26. [Google Scholar] [CrossRef]
- Kennedy, P.G.E. The Evolving Spectrum of Human African Trypanosomiasis. QJM 2024, 117, 391–395. [Google Scholar] [CrossRef]
- Vincendeau, P.; Bouteille, B. Immunology and Immunopathology of African Trypanosomiasis. An Acad Bras Cienc 2006, 78, 645–665. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, L.; De Witte, J.; Victor, B.; Vermeiren, L.; Zimic, M.; Brandt, J.; Geysen, D. Specific Detection and Identification of African Trypanosomes in Bovine Peripheral Blood by Means of a PCR-ELISA Assay. Vet Parasitol 2009, 164, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, F.; Stivanello, E.; Adams, K.; Kidane, S.; Pittet, A.; Bovier, P.A. Card Agglutination Test for Trypanosomiasis (CATT) End-Dilution Titer and Cerebrospinal Fluid Cell Count as Predictors of Human African Trypanosomiasis (Trypanosoma Brucei Gambiense) among Serologically Suspected Individuals in Southern Sudan. Am J Trop Med Hyg 2004, 71, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Desquesnes, M.; Dávila, A.M.R. Applications of PCR-Based Tools for Detection and Identification of Animal Trypanosomes: A Review and Perspectives. Vet Parasitol 2002, 109, 213–231. [Google Scholar] [CrossRef]
- Dea-Ayuela, M.A.; Galiana-Roselló, C.; Lalatsa, A.; Serrano, D.R. Applying Loop-Mediated Isothermal Amplification (LAMP) in the Diagnosis of Malaria, Leishmaniasis and Trypanosomiasis as Point-of-Care Tests (POCTs). Curr Top Med Chem 2018, 18, 1358–1374. [Google Scholar] [CrossRef]
- Adung’a, V.; Jebet, C.; John, T.; Masiga, D.; John, O.; Field, M.; Matovu, E.; Orindi, B. Roles of Cytokines in Modulating Trypanosoma Brucei Rhodesiense Infection Outcomes in Vervet Monkeys. 2024.
- Villanueva, M.S. Trypanosomiasis of the Central Nervous System. Semin Neurol 1993, 13, 209–218. [Google Scholar] [CrossRef]
- Atadzhanov, M. Tropical Neurology. In Manson’s tropical diseases; Elsevier Science Ltd. Edinburgh, 2003; pp. 275–291.
- Sabbah, P.; Brosset, C.; Imbert, P.; Bonardel, G.; Jeandel, P.; Briant, J.F. Human African Trypanosomiasis: MRI. Neuroradiology 1997, 39, 708–710. [Google Scholar] [CrossRef]
- Patel, N.K.; Clegg, A.; Brown, M.; Hyare, H. MRI Findings of the Brain in Human African Trypanosomiasis: A Case Series and Review of the Literature. BJR Case Rep 2018, 4, 20180039. [Google Scholar] [CrossRef]
- Bentivoglio, M. Trypanosomiasis. Journal of the Neurological Sciences 2015, 357, e465–e466. [Google Scholar] [CrossRef]
- Venturelli, A.; Tagliazucchi, L.; Lima, C.; Venuti, F.; Malpezzi, G.; Magoulas, G.E.; Santarem, N.; Calogeropoulou, T.; Cordeiro-da-Silva, A.; Costi, M.P. Current Treatments to Control African Trypanosomiasis and One Health Perspective. Microorganisms 2022, 10. [Google Scholar] [CrossRef]
- Pepin, J. Trypanosoma Brucei Gambiense and Trypanosoma Brucei Rhodesiense (African Trypanosomiasis). 2010.
- Kansiime, F.; Adibaku, S.; Wamboga, C.; Idi, F.; Kato, C.D.; Yamuah, L.; Vaillant, M.; Kioy, D.; Olliaro, P.; Matovu, E. A Multicentre, Randomised, Non-Inferiority Clinical Trial Comparing a Nifurtimox-Eflornithine Combination to Standard Eflornithine Monotherapy for Late Stage Trypanosoma Brucei Gambiense Human African Trypanosomiasis in Uganda. Parasit Vectors 2018, 11, 105. [Google Scholar] [CrossRef] [PubMed]
- Kuepfer, I.; Schmid, C.; Allan, M.; Edielu, A.; Haary, E.P.; Kakembo, A.; Kibona, S.; Blum, J.; Burri, C. Safety and Efficacy of the 10-Day Melarsoprol Schedule for the Treatment of Second Stage Rhodesiense Sleeping Sickness. PLoS Negl Trop Dis 2012, 6, e1695. [Google Scholar] [CrossRef] [PubMed]
- Babokhov, P.; Sanyaolu, A.O.; Oyibo, W.A.; Fagbenro-Beyioku, A.F.; Iriemenam, N.C. A Current Analysis of Chemotherapy Strategies for the Treatment of Human African Trypanosomiasis. Pathog Glob Health 2013, 107, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Galalain, S.; Bandiya, H.; Galalain, A.; Mohammed, Y. A Review on the Epidemiology and Burden of Neglected Tropical Diseases. SOKOTO JOURNAL OF MEDICAL LABORATORY SCIENCE (SJMLS) 2017, 49. [Google Scholar]
- FORSTER, E.B. The Theory and Practice of Psychiatry in Ghana. Am J Psychother 1962, 16, 7–51. [Google Scholar] [CrossRef]
- Tareen, R.S.; Tareen, K.N. Psychiatry and Tropical Diseases. Journal of Alternative Medicine Research 2016, 8, 23. [Google Scholar]
- Gimonneau, G.; Rayaisse, J.-B.; Bouyer, J. 6. Integrated Control of Trypanosomosis. In Pests and vector-borne diseases in the livestock industry; Wageningen Academic, 2018; pp. 147–174 ISBN 90-8686-863-0.
- Mitra, A.K.; Mawson, A.R. Neglected Tropical Diseases: Epidemiology and Global Burden. Trop Med Infect Dis 2017, 2. [Google Scholar] [CrossRef]
- Bukachi, S.A.; Wandibba, S.; Nyamongo, I.K. The Socio-Economic Burden of Human African Trypanosomiasis and the Coping Strategies of Households in the South Western Kenya Foci. PLoS Negl Trop Dis 2017, 11, e0006002. [Google Scholar] [CrossRef]
- Fèvre, E.M.; Picozzi, K.; Jannin, J.; Welburn, S.C.; Maudlin, I. Human African Trypanosomiasis: Epidemiology and Control. Adv Parasitol 2006, 61, 167–221. [Google Scholar] [CrossRef]
- Bhatia, B.; Sonar, S.; Khan, S.; Bhattacharya, J. Pandemic-Proofing: Intercepting Zoonotic Spillover Events. Pathogens 2024, 13, 1067. [Google Scholar] [CrossRef]
- Gao, J.-M.; Qian, Z.-Y.; Hide, G.; Lai, D.-H.; Lun, Z.-R.; Wu, Z.-D. Human African Trypanosomiasis: The Current Situation in Endemic Regions and the Risks for Non-Endemic Regions from Imported Cases. Parasitology 2020, 147, 922–931. [Google Scholar] [CrossRef] [PubMed]
- McIntire, J.M.; Bourzat, D.; Pingali, P.L. Crop-Livestock Interaction in Sub-Saharan Africa. 1992.
- Trypanosomiasis, H. On the Socio-Economic Impact of Pandemics in Africa.
- Aagaard-Hansen, J.; Nombela, N.; Alvar, J. Population Movement: A Key Factor in the Epidemiology of Neglected Tropical Diseases. Trop Med Int Health 2010, 15, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Barasa, K.W. Access Barriers to Formal Health Services: Focus on Sleeping Sickness in Teso District, Western Kenya. 2012.
- Savard, J.; Ouellet, M.-C. Handbook of Sleep Disorders in Medical Conditions; Academic Press, 2019; ISBN 0-12-813015-6.
- Freeman, D.; Sheaves, B.; Waite, F.; Harvey, A.G.; Harrison, P.J. Sleep Disturbance and Psychiatric Disorders. Lancet Psychiatry 2020, 7, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Molińska, M.; ZŁOTOGÓRSKA, A. Sleep Deficits and Executive Functions at Different Developmental Stages-Meta-Analysis. The Polish Journal of Aviation Medicine, Bioengineering and Psychology 2016, 22, 27–38. [Google Scholar] [CrossRef]
- Mehta, R.; Giri, S.; Mallick, B.N. REM Sleep Loss-Induced Elevated Noradrenaline Could Predispose an Individual to Psychosomatic Disorders: A Review Focused on Proposal for Prediction, Prevention, and Personalized Treatment. EPMA J 2020, 11, 529–549. [Google Scholar] [CrossRef]
- Campbell-Lendrum, D.; Molyneux, D.; Amerasinghe, F.; Davies, C.; Fletcher, E.; Schofield, C.; Hougard, J.; Polson, K.; Sinkins, S.; Epstein, P. Ecosystems and Vector-Borne Disease Control. Ecosystems and human well-being: policy responses 2005, 3, 353–372. [Google Scholar]
- Vale, G.; Mutika, G.; Lovemore, D. Insecticide-Treated Cattle for Controlling Tsetse Flies (Diptera: Glossinidae): Some Questions Answered, Many Posed. Bulletin of Entomological Research 1999, 89, 569–578. [Google Scholar] [CrossRef]
- Torr, S.J.; Vale, G.A. Is the Even Distribution of Insecticide-Treated Cattle Essential for Tsetse Control? Modelling the Impact of Baits in Heterogeneous Environments. PLoS Negl Trop Dis 2011, 5, e1360. [Google Scholar] [CrossRef]
- Kaboré, B.A. Advancing the Sterile Insect Technique for Tsetse (Diptera: Glossinidae): Exploring Alternative Radiation Sources and Protocols. 2024.
- Vreysen, M.J.B.; Seck, M.T.; Sall, B.; Bouyer, J. Tsetse Flies: Their Biology and Control Using Area-Wide Integrated Pest Management Approaches. J Invertebr Pathol 2013, 112 Suppl, S15–25. [Google Scholar] [CrossRef]
- Feldmann, U.; Dyck, V.; Mattioli, R.; Jannin, J. Potential Impact of Tsetse Fly Control Involving the Sterile Insect Technique. Sterile insect technique: Principles and practice in area-wide integrated pest management 2005, 701–723.
- Meyer, A.; Holt, H.R.; Selby, R.; Guitian, J. Past and Ongoing Tsetse and Animal Trypanosomiasis Control Operations in Five African Countries: A Systematic Review. PLoS Negl Trop Dis 2016, 10, e0005247. [Google Scholar] [CrossRef]
- Maudlin, I. African Trypanosomiasis. Ann Trop Med Parasitol 2006, 100, 679–701. [Google Scholar] [CrossRef] [PubMed]
- Jabir, M.; Choolayil, A.C. Social Work with Populations Vulnerable to Neglected Tropical Diseases: Evidence and Insights from India. 2024.
- Palmer, J.J.; Surur, E.I.; Checchi, F.; Ahmad, F.; Ackom, F.K.; Whitty, C.J.M. A Mixed Methods Study of a Health Worker Training Intervention to Increase Syndromic Referral for Gambiense Human African Trypanosomiasis in South Sudan. PLoS Negl Trop Dis 2014, 8, e2742. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Trypanosoma brucei Life Cycle. Tsetse fly acts as the parasite's vector; trypomastigotes are ingested when they bite an infected human. These undergo various developmental stages inside the fly, and when the fly bites another human, metacyclic trypomastigotes are released into the bloodstream. Cattle act as reservoirs.
Figure 1.
Trypanosoma brucei Life Cycle. Tsetse fly acts as the parasite's vector; trypomastigotes are ingested when they bite an infected human. These undergo various developmental stages inside the fly, and when the fly bites another human, metacyclic trypomastigotes are released into the bloodstream. Cattle act as reservoirs.
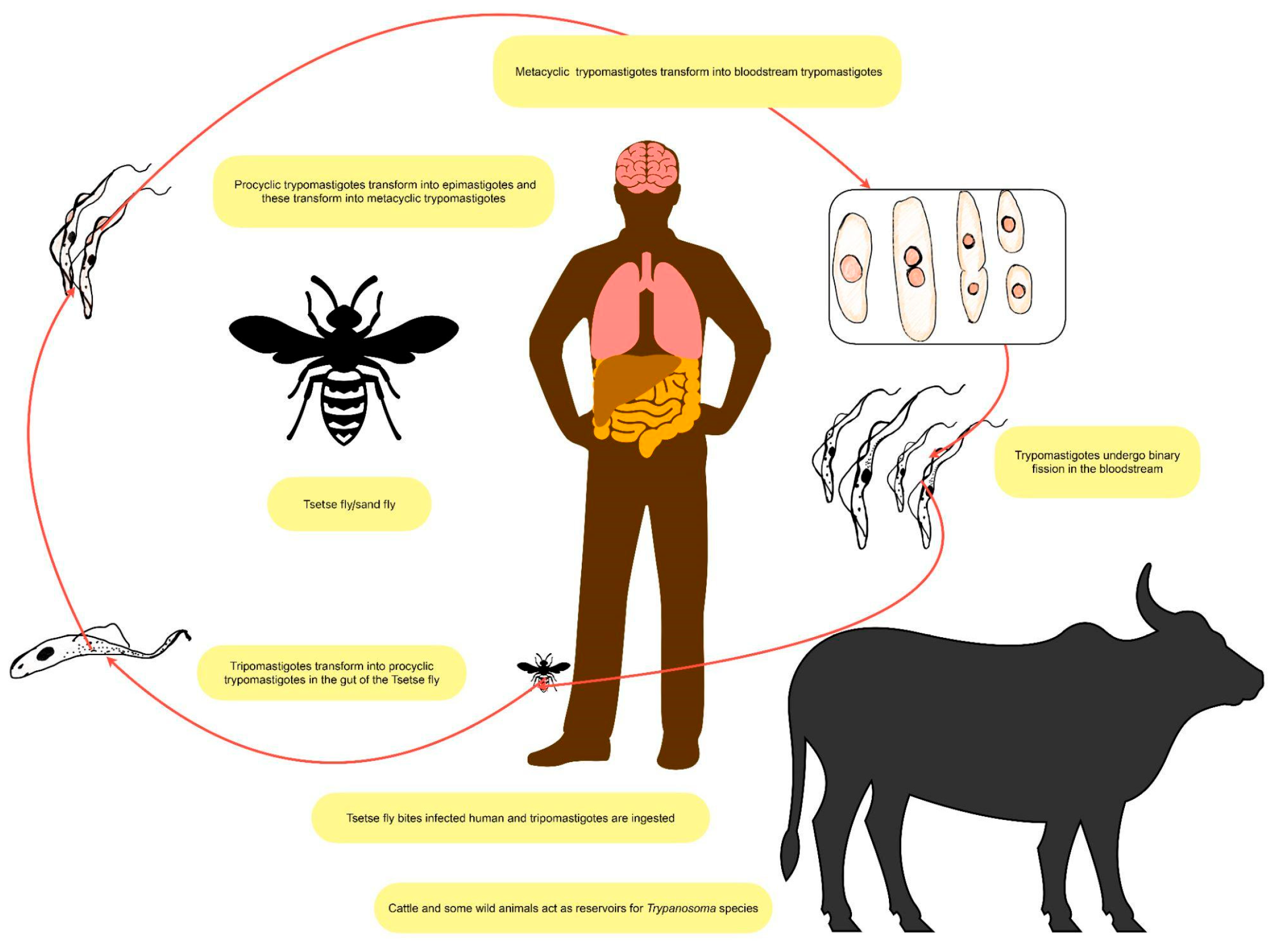
Figure 2.
Pathophysiology of “sleeping sickness.” Trypanosoma parasites breach the blood-brain barrier and affect the hypothalamus and suprachiasmatic nucleus. Circadian rhythm is disrupted, thereby resulting in insomnia, hypersomnia, and lethargy. Complex inter-actions with macrophages, microglial cells, and the immune system underlie the African sleeping sickness.
Figure 2.
Pathophysiology of “sleeping sickness.” Trypanosoma parasites breach the blood-brain barrier and affect the hypothalamus and suprachiasmatic nucleus. Circadian rhythm is disrupted, thereby resulting in insomnia, hypersomnia, and lethargy. Complex inter-actions with macrophages, microglial cells, and the immune system underlie the African sleeping sickness.


Table 1.
The main characteristics of T. b. gambiense and T. b. rhodesiense.
| Subspecies | T. b. gambiense | T. b. rhodesiense |
|---|---|---|
| Distribution | Western and Central Africa | Eastern and Southern Africa |
| Epidemiology (2020) | < 100 cases. It corresponds to 95-97% of all the cases reported. | < 100 cases. It corresponds to 3-5% of all the cases reported. |
| Incidence | Young adults involved in productive activities (hunting, fishing, and cultivating) | Young adults of working age, tourists visiting areas where wildlife is preserved |
| Vector | G. palpalis and G. fuscipes | G. morsitans and G. pallidipes |
| Fly habitat | Humid; river habitat | Dry; savannah and woodland habitat |
| Reservoir | Anthropologic (humans) | Zoonotic (animals) |
| Transmission | Human/ mammalian host - tsetse fly - human | Animal - tsetse fly - animal Animal - tsetse fly - human Human - tsetse fly - human The seasonal variations in transmission linked to the density of the Glossina (higher after the rainy season) |
| Symptoms and signs | Chronic disease, lasting months to years | Acute disease lasting a few weeks |
| Mild fever, headache, personality disorder, and sleeping disorder | Severe fever, persistent headache, and multi-organ damage | |
| Rarely skin manifestations | More frequent skin manifestations. | |
| Laboratory | Screening: available. | Screening: not available. |
| Microscopy: concentration methods | Microscopy: concentration methods | |
| Staging: lumbar puncture | Staging: lumbar puncture | |
| Vaccine | No | No |
| Prognosis | If left untreated, three years of survival. | If left untreated, six to twelve months survival. |
Table 2.
Overview on drugs used for the treatment of African Trypanosomiasis.
| Drug | Mechanism of action | Indication | Adverse effects | Resistance |
|---|---|---|---|---|
| Acoziborole | Block protein biosynthesis by inhibiting leucyl-tRNA synthetase | First and second stage | Not available | Not available |
| Eflornithine (monotherapy) | Suicide inhibitor of ornithine decarboxylase (ODC), inhibition of polyamine biosynthesis | Alone only in the second stage | Itching, fever, headache, abdominal pain, nausea/ vomiting, diarrhea, myelosuppression | Membrane transporter for aminoacids |
| Fexinidazole | Production of reactive amines and other metabolites with toxic effects on trypanosome | First and early second stage | Vomit/ nausea, asthenia, prolongation of QT interval | Nitroreductase mutations, possibly cross-resistance with nifurtimox |
| Melarsoprol | Formation of toxic adducts with trypanothione and alterations of the parasite’s mitotic processes through action on multiple kinases | First choice in the second stage and treatment of recurrent relapse after first-line and rescue treatments | Encephalopathic syndrome, heart failure | Membrane transporters, pentamidine cross-resistance |
| Nifurtimox/ eflornithine combination therapy | Nifurtimox promotes the generation of free radicals. Unknown combination mechanism | First choice in the severe second stage and early second stage | Gastrointestinal symptoms, headache | Nitroreductase mutations, possibly cross-resistance with fexinidazole |
| Pentamidine | Preventing replication and transcription in the kinetoplast and the nucleus-inhibition of the plasma membrane Ca2+-ATPase collapse of the mitochondrial membrane potential | First stage | Hypotension, nausea/vomiting, hyperazotemia, diabetes mellitus | Membrane transporters, melarsoprol cross-resistance |
| Suramin | Inhibition of dihydrofolate reductase, thymidine kinase, and glycolytic enzymes | First stage | Nephrotoxicity | Variant surface glycoprotein |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



