
Submitted:
09 December 2024
Posted:
10 December 2024
You are already at the latest version
Abstract
(1) Background: Silver and silver-based alloys are not mutagenic, carcinogenic or toxic to reproduction. However, the European Chemicals Agency (ECHA) has decided to include ionic silver and silver nanoparticles in the list of biocidal substances. In this context, we aimed to evaluate the quantities of silver released and the cytotoxicity of silver-based dental alloys sourced from two distinct suppliers present in the EU (European Union) markets. (2) Methods: Five dental alloys, with silver contents ranging from 9.2% to 58%, were tested by extraction tests in a solution of racemic lactic acid and sodium chloride (7-day extraction at 37°C). The cytotoxic behavior of five other dental alloys with silver contents ranging from 22.4% to 59% was evaluated, as well. (3) Results: Extraction test results indicate small quantities of silver, ranging from 55μg/L to 243μg/L. The assessment of alloys’ cytotoxicity reveals variability of the obtained results; however, none of the tested alloys can be considered cytotoxic. (4) Conclusions: The obtained results indicate that the silver-based alloys included in this study do not pose a risk when used in the oral cavity.
Keywords:
Silver
; Alloys
; Dental Alloys
; Dental Materials
; Toxicity
; Cytotoxicity
; Biocidal
; European Union
1. Introduction
Silver is often found as a by-product during the recovery of the copper, lead, zinc and gold ores. It is used to manufacture jewelry, silverware, electronic equipment, electrical connectors and dental metallic alloys, and for surgical prostheses and several other medical devices, as well [1]. Silver was used in the photography, in the manufacture of soldering and welding electrodes for metal alloys and coinage, or to disinfect drinking water and swimming pool water as an antibacterial agent. Moreover, ancient civilizations were aware of the bactericidal properties of silver [1], as fungicides. Since 1500 BC, the Egyptians have used silver salts as astringent [2, 3]. Indians, Egyptians, Persian kings, Phoenicians, Greeks and Romans used equally silver and copper to preserve food and to disinfect the water [4,5]. Recently, silver has been used as element for suture and infections prevention [6]. The antimicrobial properties of this metal have been used in a variety of applications throughout history, but their uses in the medical applications rapidly declined when antibiotics were discovered by Fleming in 1920. Soluble silver compounds, such as silver salts, have been used in the treatment of mental illness, epilepsy, gastro-enteritis and infectious diseases, including syphilis and gonorrhea [7-9]. It has also been used in lozenges and chewing gum to help people quit smoking and eliminate nicotine addiction.
Several factors influence the capacity of a metal to produce toxic effects on human organism, especially the metal solubility, its capacity to link with the biological sites and the extent to which the metal complexes formed are sequestered or metabolized and excreted [10,11]. Existing studies suggest that some forms of silver are more toxic than others [1, 12-16]. Due to the seemingly different toxicities that soluble and insoluble forms of silver have in humans, the scientific literature has been critically reviewed to investigate the occurrence of adverse health outcomes, with a focus on cases of occupational exposure. As for the protection of the population, there is also information but little legislation regarding exposure limits in humans.
1.1. Sources of Silver Exposure in Humans
Silver is a naturally occurring substance in the environment, people are exposed to this substance and its compounds from environmental sources (air, dust and drinking water, etc.) and food (silver being a permitted food additive), as well as from products available to consumers (jewelry, watches, cosmetics, natural health products, food packaging materials, silverware, medicines, dental alloys/amalgam, electronic items, toys etc.) [17-19]. Silver is naturally released into the environment by the weathering of soils and rocks. It also be released into the environment from industrial activities. This includes its production such as mining, manufacturing of Ag alloys, smelting and refining, manufacturing of silver-containing substances, disposal of landfill leachate-type products after waste disposal, other activities such as cloud seeding and wastewater (including silver in final effluent discharged from wastewater treatment systems).
1.2. Silver in Direct Contact with Food Substances
Metals and alloys that contain silver are used in food contact materials and objects such as food processing equipment, household containers and utensils, as well as food packaging sheets. These materials are frequently used as a safety barrier between food and the environment [20]. Silver is used in the manufacture of cutlery and tableware products; in this regard, particular attention should be paid to the European standard EN ISO 8442-2 (1997) [21] applicable to silver-coated nickel silver or stainless steel cutlery and to EN ISO 8442-3 [22] applicable to silver-coated silverware and silver-coated silverware. Metal ions may be released into food from such materials and, if the release exceeds the toxicological reference values, may endanger the life of the consumer, lead to an unacceptable change in the composition of the food or to an alteration in its organoleptic characteristics. Thus, a technical guide in this field has been drawn up [20]. The release is defined in this guide [20] as the unintentional transfer of metal ions to food from materials or articles made of metals or alloys. A "specific release limit" (LLS) is, for a given metal or metalloid ion, the maximum amount (in milligrams) that is permitted for release into a food or simulant (in kilograms) from a material or object of defined surface. For Silver, the LLS value is set at 0.08 mg/Kg [20]. This value is applied to the unintentional release of metallic silver ions from materials and objects during their end use. They are manufactured or imported into Europe, made up wholly or partly of metals or alloys, with or without a surface coating – if they are finished products. For example, household utensils and food processing equipment such as food processors, food packaging sheet, containers, pans, blenders, knives, forks, spoons, etc. In some countries, silver salts are used to disinfect drinking water because of their germicidal properties [23,24]. Silver is also used as a coloring agent in confectionery and alcoholic beverages.
1.3. Health Effects of Silver in Humans
The wide variety of uses of silver allows for exposure through various routes of entry into the body. Ingestion is the primary route of entry for silver compounds and colloidal silver proteins (Silver, 2003) [17]. Inhalation of silver-containing dust or vapors occurs primarily in the workplace [17]. Dermal contact occurs in the workplace [17], but also in the consumer from the application of burn creams [18] and contact with jewelry [19]. Silver can also enter the body through the use of acupuncture needles [25], catheters [26], dental amalgam and dental alloys [19], or accidental puncture wounds [27]. Soluble silver compounds are more readily absorbed than metallic or insoluble silver [13, 28, 29] and can therefore have adverse effects on the human body [10].
Acute symptoms of overexposure to silver nitrate are decreased blood pressure, diarrhea, stomach irritation, and breathing difficulties. Chronic symptoms of prolonged ingestion of low doses of soluble silver salts include fatty degeneration of the liver and kidneys and changes in blood cells [30]. The use of silver nitrate in oral ulcerations can be generated by Argyria [31,32]. The uses of silver nitrate as a topical for gum bleeding can also generate Argyria, silver deposits in organs and abdominal pain [7]. Long-term inhalation or ingestion of soluble silver or colloidal silver compounds (nanoparticles) can cause Argyria and/or Argyrosis [9,33,34]. They can also accumulate in small amounts in the brain and muscles [29]. Silver in any form is not considered toxic to the immune, cardiovascular, nervous, or reproductive systems [17] and is not considered carcinogenic [35].
Argyria and Argyrosis are the result of exposure to soluble silver compounds that generate toxic effects, including liver and kidney damage, irritation of the eyes (Argyrose), skin (Argyria), respiratory system and intestinal tract, and changes in humans blood cells The affected area becomes bluish-grey or ashy grey and is most visible on body sun-exposed areas [8,9,17] and Argyrosis have been reported during placement of silver-containing solids in the skin or body [36]. Argyria and Argyrosis can be generated by the use of certain drugs or devices, for example: Silver nitrate (AgNO3) solution used for varicose veins [8]; Silver acetate (CH3COOAg), anti-smoking lozenges and tablets [37-39]; Silver in colloidal form used to fight allergies and colds [9]; Colloidal Ag proteins for nasal drops [40] and for eye drops [41]; Silver-coated acupuncture needles [25]; Silver-coated tablets – air freshener [25]; Silver in water – Hemodialysis treatment [42]; Additive antigen - food processing [43]. Metallic silver appears to pose minimal health risk [15,16,44,45].
1.4. Toxicity Generated by Exposure to Silver and Silver Salts
Concerns regarding professionals who are in prolonged contact with Ag/Ag salts are not specifically addressed in this paper. However, it should be remembered that there are several occupational exposure limits and guidelines for silver, but the values for each depend on the form of the silver as well as the organization that makes the recommendations [46,47]. From a toxicological perspective, the issue can be addressed by considering both soluble silver components and insoluble silver components [47]. The general population is exposed to silver primarily through the ingestion of drinking water and food, as previously mentioned. On the other hand, inhalation is probably the most important route of occupational exposure [47]. Populations exposed to higher levels of silver than natural levels include workers in industries that process or use the antigen compound and members of the general public who consume drinking water and foods containing high levels of silver. This includes seafood from areas near sewage outfalls or industrial sources, as well as crops grown in areas with high ambient concentrations of silver in air or soil. For the consumer, potential exposures are frequently used products such as cosmetics and health products, jewelry, silverware, medicines, toys. It is the cutaneous route that reveals a potential risk of poisoning. These types of exposures have already been assessed by different organizations, which published a variety of assessment documents, subject to rigorous reviews and approval processes [47]. At the public health level, it was considered that these assessments constitute reliable characterizations of the hazards. Early in 2008, more than 16 international and national organizations were involved in population risk assessments of exposure to silver [47]. Literature review results reveal extensive data on toxic effects of exposure to silver or silver salts. Hays et al. [47] show that the majority of existing toxicological studies in experimental animals, along with epidemiological studies in humans have external doses by different routes of exposure (e.g., oral, dermal or inhalation). Therefore, there is no direct method to interpret the concentrations of chemicals measured in blood or urine in biomonitoring studies to assess potential health risks to the general population. It is not possible to directly compare an external dose expressed as intake in mg/kg bw/day to concentrations in the blood (e.g., in mg/L) or to concentrations of chemicals in the urine (e.g., in mg/L or mg/g creatinine) [47].
1.5. Information Concerning the Canadian Health Measures Survey (CHMS)
A survey worth mentioning is the Canadian Health Measures Survey (CHMS), a national survey conducted by “Statistics Canada” to collect information from Canadians about their general health [48]. The survey was designed to be nationally representative and includes a biomonitoring component; metal concentrations were measured in the blood and urine of approximately 5,500 to 7,000 Canadians during each survey cycle [48]. The metals concerned were Barium (Ba), Molybdenum (Mo), Silver (Ag), Thallium (Th) and Tin (Sn). The evaluation was based on 2016 relevant data; this assessment considered only human health effects and exposure associated with barium, molybdenum, silver, thallium and tin (inorganic) entities, and does not consider other elements that may be present in some substances that may release these elements (such as gold) [48]. Subjects ranged in age from 3 to 79 years, and pregnant women and people with serious chronic illnesses were excluded [48]. Total concentrations of a metal moiety in whole blood or urine are a relevant biological indicator and an integrated measure of exposures that can occur through multiple routes (i.e., oral, dermal, and inhalation) and sources (i.e., environment, diet, or frequent or daily use of certain public consumer products) [17-27,47,48]. So, the estimates are based on the total amounts of silver found in the blood. The chemical compounds considered as sources in the amount of total silver in blood are metallic Ag (CAS 7440-22-4), Silver Nitrate (AgNO3, CAS 7761-88-8), Silver Chloride (AgCl, CAS 7783-90-6), Silver Bromide (AgBr, CAS 7785-23-1), Silver Sulphate (Ag2SO4, CAS 10294-26-5), Silver Oxide (Ag2O, CAS 20667-12-3) and Silver Sulfide (Ag2S, CAS 21548-73-2) [47,48]. In this Canadian study, human biomonitoring data (levels measured in whole human blood used to estimate exposure) were compared to biomonitoring guidance values (associated with health effects) that are protective of human health [48]. There are groups of individuals (vulnerable populations) within the Canadian population who, due to greater susceptibility or exposure, presented a greater risk of adverse health effects from exposure to substances [48]. Certain subpopulations are systematically considered throughout the screening assessment process, such as infants, children and persons of childbearing age. For example, age-specific estimates of exposure are routinely made and the risk of adverse health effects is assessed based on developmental and reproductive toxicity studies [48]. Results from the risk assessment revealed that Silver and its compounds pose a low risk to human health, at the exposure levels analyzed in the screening assessment. Moreover, exposure assessments of the Canadian population, using whole blood concentrations, demonstrate a minimal environmental risk from silver and its compounds.
1.6. Legislation Concerning Values of Metallic Silver, Soluble Silver, and Daily Silver Intake Amounts
In 1966, the American Conference of Governmental Industrial Hygienists (ACGIH) established a limit value (Threshold Limit Value–Time-Weighted Average/ TLV-TWA) of 0.01mg/m3 for soluble compounds as silver [46], primarily based on Hill and Pillsbury publication [46]. However, in response to the results of studies undertaken since the work of Hill and Pillsbury [46], in 1980 a new TLV of 0.1mg/m3 was establish for metallic silver [46]. The ACGIH recognized the different results of exposure to soluble and/or insoluble silver, rationalizing that "the available data on soluble compounds of silver salts show a greater propensity to argyria than metallic silver dust or fumes and that the respective exposure levels of 0.01mg/m3, for soluble silver, and 0.1mg/m3 for metallic silver are adequate for the prevention of Argyria in workers exposed to silver in air [46]. The ACGIH is not the only organization to note different health outcomes from exposure to different forms of silver. For example, The Health and Safety Executive of the United Kingdom also reached a similar conclusion after examining metallic silver, stating "from the available data, it is concluded that exposure to 0.1 mg/m3 8h TWA of silver metal would not result in significant pigmentation development [29]. In searching for data on Silver/Silver Salts, we found no specific legislation or test standards that evaluate the migration or release of ionic silver and its compounds from consumer products. On the other hand, there is information on the subject that can help to develop new orientations in the approaches for the protection of consumers [49].
Moreover, based on actual concentrations of silver in drinking water, which are generally less than 0.005mg/L [50], World Health Organization (WHO) estimated intake amounts to be approximately 0.007 mg/day (0.12μg/kg body weight/day). It is estimated that the average daily intake is 1.29-2.65μg/kg body weight/day (depending on low or high binding assumptions) in adults and 1.60-3.47μg/kg body weight/day in children [50,51]. United States Environmental Protection Agency (EPA) [52,53] analyzed and described a series of experiments that concluded that silver ion concentrations greater than 0.2mg/L in drinking water had no adverse effects in experimental animals that had consumed silver ions continuously for 11 months. In the fourth edition of the "Guidelines for Drinking-Water Quality", WHO today did not set a value for silver, as in previous editions [54-57]. Using argyria (a condition due to silver overload) as a benchmark, Gaul et al. [58] estimated that 10 g of silver (or 0.39 mg/person/day) is the total oral dose that is not expected to cause any effects over a person's lifetime. The European Food Safety Authority (EFSA) has defined a group restriction for substances containing 0.05mg Ag/kg of food [59]. In its decision, EFSA took into account the limit of 0.39mg/person/day set out in the WHO Guidelines for Drinking Water Quality and concluded that a restriction of 0.05mg Ag/kg of food would contribute to approximately 12.5% of the human NOAEL (no-observed-adverse-effect level) [60].
1.7. Silver in Dental Applications
Regarding the field of dentistry, modern materials embedded with silver and those coated with silver, are nowadays recognized for their antibacterial properties, in addition to silver-based alloys [61]. Fixed or removable dental prostheses, implant-supported prostheses, oral appliances, occlusal splints, and orthodontic appliances can be treated with or incorporate silver. Moreover, it is acknowledged the antimicrobial efficacy of dental implant surfaces following the application of diverse metal element coatings in order to prevent bacterial growth associated with peri-implantitis[61]. In this regard, studies reported the antibacterial efficacy of metallic coatings, such as silver or silver-zinc coating on endosseous oral implants [61]. However, there is a very delicate line between the antimicrobial or biocidal properties of a material and the potential negative effects it may induce, both at local and systemic levels.
In the light of the multifaceted, general scenario presented above, this study is designated to investigate specific silver-based alloys within the domain of dentistry. Despite the prevalent use of zirconia ceramics and CoCr-type alloys in contemporary dental prosthetics, facilitated by CAD-CAM (Computer-Aided De-sign/Computer-Aided Manufacturing), implying, for example advanced computerized milling and 3D-printing techniques, silver-based dental alloys remain in use. It should be remembered that in the oral environment, prosthetic alloys are in permanent contact with the oral environment, i.e., saliva and living tissue. Dental alloys are considered medical devices and therefore must meet the requirements of the ISO 10993 standard [62]. To our knowledge, the specialized literature does not specify requirements for the quantities of ions released; however, other evaluations are presented, including cytotoxicity, sensitization, irritation, intracutaneous reactivity, acute systemic toxicity, sub-chronic toxicity, genotoxicity and carcinogenicity tests, which are essential for acceptance of medical devices.
Given this complex context, the objective of our research was to assess the quantities of silver ions released by five silver-based dental alloys, which contain silver ranging from 9.2% to 58%. Furthermore, our study aimed to investigate the cytotoxic behavior of an additional five dental alloys (with silver content ranging from 22.4% to 59%) in accordance with ISO 10993-Part 5 [62].
2. Materials and Methods
Our research employed two series of silver-based dental alloys obtained from two distinct suppliers in the EU (European Union) markets. The coding for the alloys tested for extraction and cytotoxicity, and their chemical compositions are presented in Table 1. The dental alloys tested for extraction were coded from #1-#5 and the ones tested for cytotoxicity were coded from #6 to #10. The amount of silver varies between 9.2% and 59% in the samples compositions. The samples were prepared according to ISO 10271:2020 [63].
2.1. Cations Release Assessment
For extraction tests, three samples were tested for each type of the five dental alloys (coded #1-#5) (n=15). Each sample, with a surface area of 11.3 cm was immersed in 10 ml of a 10 g/l (± 0.1) solution of 90% racemic lactic acid and 5.85 g (± 0.005) of ultrapure sodium chloride in a Falcon medical device test tube. The solution was also prepared with ultrapure quality water. After 7 days (± 1 hour) at 37°C the samples were removed from the solution and were analyzed by ICP OES (Inductively Coupled Plasma Optical Emission Spectroscopy) and ICP-MS (Inductively Coupled Plasma Mass Spectrometry). The values given are the average of the three analyses.
2.2. Cytotoxicity Tests
Samples #6-#10 were evaluated in cytotoxicity assays according to ISO 10993 part 5 [62]. The tested metal specimens were in the form of a disc (11mm in diameter) with a surface metallographically polished with a 1 µm diamond paste. The samples were cleaned in a 1% detergent solution (RBS 35) with ultrasounds. Both samples and controls were autoclaved at 121°C for 30 min. For direct contact tests, the samples were fixed on Thermanox discs with a biocompatible fixative.
Reagents: Anti-BrdU antibody was supplied by ICN (Meckenheim, Germany). BCA protein assay reagent was ob-tained from Pierce, Rockford, USA. Bovine serum albumin (BSA) was bought from Serva Feinbiochemica, Heidelberg, Germany. Uridine, Ethylenediamine-tetra-acetic acid (EDTA), MTT S-diphenyl tetrazolium bromide), trypsin type Ill, Triton X-100 were supplied by Sigma Chemie, Deisenhofcn, Germany. RPMI medium, L-glutamine, penicil-in/streptomycin solution, Fungizone, Fetal calf serum (FCS), phosphate buffered saline solution (PBS) were supplied by Gibco BRL, Life Technologies, Eggenstein, FRG. Ethanol, methanol, 2-propanol, hydrochloric acid, Tris (hy-droxymethyl) aminomethane (Tris) were bought from Merck, Darmstadt, Germany. Filters (0.22 urn-pore size; mixed cellulose-esters) were supplied by Millipore, Eschborn, FRG. Tissue culture ware was supplied by Becton & Dickinson, Heidelberg, Germany. Trypan blue solution was obtained from Boehringer Mannheim, Mannheim, Germany. Microplate reader, Titertek Il, and software (EIA3) were supplied by fCN-Flow, Meckenheim, Germany.
Cells, reference materials and samples negative controls: silicone rubber tubing (polydimethylsiloxane; medical grade; supplied by Rehau, Rehau, Germany) and Thermanox tissue (pure discs, Nunc, Wiesbaden, Germany). Positive controls, Zn-and Ni-chloride, were obtained from Sigma, Germany. Mouse fibroblast cells L-929 (CCLI; strain L, NCTC clone 929) were obtained from American Type Culture Collection, Rockville, USA; HeLa cells (ATCC code: CCLZ) were obtained from ICN-F10w, Meckenheim, Germany and human fibroblasts were isolated from the human umbilical cord. All cells were cultured in RPMI medium with additional L-glutamine, penicillin/streptomycin and 10% fetal calf serum in a humidified atmosphere containing 5% CO2.
Preparation of cell cultures: In order to prepare test wells, cells were detached from the culture flasks using a trypsin/EDTA solution (0.25%/0.25% w/v) and resuspended as a single cell suspension in culture medium at a density of 2 x 105 viable cells/ml (trypan blue exclusion test). HeLa, L929 and human fibroblasts were seeded into the wells of microtiter plates and 24-well clusters, at a density of 1 x 105 cells/cm2. After overnight incubation, the wells were emptied and refilled with the extracts, as well as their dilutions or fresh culture medium.
Techniques used: All three cell lines USED (L-929 mouse fibroblasts, HeLa-like cells from human cervical carcinoma, and human fibroblasts from umbilical cord) were used by extract and direct and indirect contact techniques [62].
Extract dilution tests: The samples were extracted in culture medium for 24 h at 37 °C (1 cm 2/mL). The pH was adjusted to be between 7.2 and 7.4, the extracts were sterile filtered (pore size: 0.22-um) and diluted 2, 4,8 and 16 times with fresh culture medium. Positive and negative must be viewed as an assessment control. Materials were diluted to defined molar concentrations, whereas the extract of the negative control was not diluted.
MTT-test: 20 µI of a 1 % MTT solution was added to each well of a 96-well microtiter plate. The plates were shaken briefly and incubated for a further 1 h (4 h in case of human fibroblast experiments) at 37° C. After careful aspiration of the supernatants, 100 µL of 2-propanol were added to each well. After complete solubilization of the MTT formazan, the absorbance at λ = 590 nm of each well was measured after transferring the supernatants into fresh microtiter plates [64].
BrdU labelling index: To each well, except for the negative control, 10 µI of a BrdU solution (final concentration 10 mM) were added. After incubation for a 120 min period of time (24 h in case of human fibroblast experiments) the cells fixed in methanol/ethanol (1 : 2 v/v) and washed using PBS. The labelling index was determined by EIA methods after incubation of the cells with an antiBrdU antibody [65].
Direct contact tests: Zn and Ni-alloys as well as copper were used as positive controls in the direct contact tests. Silicone was the negative control. Cells, human primary isolated fibroblasts, were seeded on the materials and incubated under standard culture conditions for a 24 h period. Samples were fixed with methanol/ethanol and were stained with hematoxylin/eosin following standard protocols. The evaluation of cytotoxic effects was performed with the help of transmission light microscopy (in the case of silicone) or dark field microscopy in the case of metal alloys.
Evaluation and statistics: Data were evaluated using Student's t-test/f-test. P-values of less than 0.01 were considered to indicate statistically significant differences and calculated with the assistance of Microsoft Excel.
3. Results and Discussions
3.1. Cations Release
The tests were carried out on three extracts of each dental alloy (coded #1-#5). The results presented are an average of the three values obtained (Table 2). As previously mentioned, in their compositions, the amount of silver varies between 9.2% and 58% (Table 1). The analyses were made by ICP MS for Au, Cr, Ga, In, Pd, Pt, Sn, and by ICP AES Be, Cu, Fe, Mo, Mn, Ni and Zn. In our measurements we did not find traces of Be, Ni, Mn, Ga, so these elements do not appear in Table 2. Table 3 shows the quantities of silver in the alloys' compositions in relation to the quantities of silver released in the performed extraction tests.
The findings of our investigation indicate that the quantities of silver released in the extraction tests performed are minimal, on the order of micrograms; therefore, it can be asserted that the tested alloys do not pose toxicity problems. Conversely, given the minimal quantities of silver released, a question can arise: can silver alloys be generally regarded to have biocidal behavior? In this context, some relevant aspects concerning the obtained results and their correlation with the findings of other studies in the specialized literature will be presented.
3.1.1. Migration of Metallic Silver in Ionic Solutions
Silver in the metallic state is very poorly soluble in water; its solubility is 30 ng/L. The measurements were made within the framework of the Consortium Precious Metals and Rehnium REACH Euro Métaux [66]. A first approach to the migration of silver in ionic solutions was made by Steppan et al. [67] proposing the following mechanism:
Ag →Ag+
H2O→ H+ + OH-
Ag+ + OH- → AgOH
2 AgOH → Ag2O + H2O
Ag2O + H2O → 2 AgOH → 2 Ag+ + 2OH-
The proposed model is for Ag-Pd alloys in an H2O medium. According to Vu et al. [68] in an Ag-Pd binary alloy, the anodic formation of palladium oxide blocks the migration of Ag+ ions in the electrolyte solution. The proposed mechanism is based on the dependence of potential energies and the pH values according to the Pourbaix diagrams, as follows:
Ag + ½ H2O → ½ Ag2O + H+ + e-
E0 = 1.173 – 0.0591 pH
Ag2O + H2O → Ag2O + 2 H+ + 2 e-
E0 = 1.398 – 0.0591 pH
Pd + H2O → PdO + 2 H+ + 2 e-
E0 = 0.896 – 0.0591 pH
Their study was conducted on two binary alloys with 15% Palladium and another that contains 30% Palladium. In other words, the formation of palladium oxide blocks the migration of silver ions and consequently the concentration of ions in solution is greatly decreased. In reality, biological media are more complex than H2O and can therefore contain chlorides (NaCl, KCl, CaCl2), phosphates (Na2HPO4), lactic acid, urea, many proteins, including enzymes, amino acids (peptides) etc.
Taking into account the aspects mentioned above, it is worth noting certain results that were obtained in a study presenting the corrosion behaviour of silver-based alloys in Fusayama artificial saliva solution [69]. This medium contains chlorides, NaCl 0.4 g/l: KCI 0.4g/l and CaCl2.H20 0.79 g/l. The two alloys that were tested had in their composition the same amount of Pd but two different silver amounts of 4.17% and respectively 62.7%. The study indicated that, on the one hand, silver reduced corrosion resistance and, on the other hand, that these alloys were two-phase and therefore there could be phenomena of micro-galvanism between phases. In the case of alloy 11.8Au 47.7Ag 22.8Pd 6.7In 6.8Zn an examination of the microstructure showed that it was a two-phase alloy, one gold-silver phase and (one) palladium-indium phase. After the corrosion test, it was observed that the gold-silver phase corroded with the formation of silver chloride. Elimination of silver chloride by dissolving in a 20% ammonia solution and the repetition of the corrosion test showed that the gold-silver phase was the corroding one - it was therefore less noble [69]. In the case of alloy 1.6Au62.7Ag22.Pd1.8InCu10.6Zn0.8, which is also two-phase, the silver was distributed across both phases. After the corrosion test, the formation of silver chloride was also visible. By applying the same technique to dissolve the silver chloride formed at the specimen’s surface, it was observed that the degradation by corrosion occurred in both phases. An analysis of the solution composition from the first corrosion tests is presented for both alloys in Table 4, Figure 1 and Figure 2.
Thus, the model of silver ions migration in ionic solutions based on the diagrams of Pourbaix according to [67,68] seems a bit simplistic to us. The solubility of silver chloride in water at 25°C is approximately 1.3 x 10-5 moles per litre (or approximately 1.77 mg/L). Also, the Product Solubility (Ksp) of silver chloride at 25°C is about 1.8 x 10-10. This low Ksp indicates a very low solubility. However, the solubility of silver chloride can be affected by the presence of other ions in the solution. For example, solubility may increase in the presence of ammonia (NH3) or sodium thiosulfate (Na2S2O3), urea, lactic acid because these substances can form soluble complexes with Ag+. These aspects explain the results obtained in the extraction tests.
The electrical conductivity of silver chloride (AgCl) is extremely low due to its low solubility in water. In aqueous solution, conductivity depends on the concentration of dissolved ions. The molar conductivity of Ag+ and Cl- ions in solution is 61.9 S·cm²/mol and 76.3 S·cm²/mol, respectively. However, solubility and conductivity can be modified in the presence of certain chemical substances capable of forming complexes with silver ions.
3.1.2. Aspects Regarding Migration of Metallic Silver
Considering the complexity of the topic addressed, it is worth noting that various factors could influence the migration of metallic silver, outlined as follows:
- − Alloy Composition:
Silver Ratio: The higher silver content in the alloy composition, the greater the potential for silver ion release will be.
Alloying Elements: Other elements present in the alloy can influence the dissolution of silver. For example, elements such as gold, copper, palladium, indium or zinc can change the release of silver ions.
- − Microstructural structure of the alloy:
Phase distribution: The presence of different phases in the alloy can affect cations release. For example, silver-rich phases - where silver is distributed in all phases - will be more likely to release silver ions.
Grains and grain boundaries: The size of the grains and the nature of the grain boundaries can also influence corrosion and, consequently, the release of silver ions, through the formation of micro-galvanic phenomena.
- − Chemical environment of the solution:
Solution pH: Acidic solutions (low pH) can accelerate the release of silver ions through corrosion.
Presence of ion complexes: Some ions in solution, such as chloride (Cl-) or thiosulfate (S2O3-2 ) ions, or substances such as urea, lactic acid, can form soluble complexes with silver ions, increasing their release.
Redox potential of the solution: An oxidizing environment can promote the dissolution of silver.
- − Temperature: Higher temperature can accelerate dissolution and corrosion processes, increasing the release of silver ions.
- − Alloy Surface:
Surface roughness: A rough surface may have a larger area exposed to solutions, increasing leaching.
Surface treatments: Surface treatments, such as polishing, plating, or passivation, can reduce the release of silver ions.
- − Alloy tension state: Mechanical stresses or deformations can create local anodic sites, increasing corrosion and leaching of silver ions.
- − Presence of biofilms or biological organisms: The formation of biofilms on the surface of the alloy can influence microbiological corrosion, thereby altering the release of silver ions.
- − Exposure time: The longer the alloy is exposed to an ionic solution, the greater the release of silver ions can be.
These factors can interact in complex ways, influencing the rate and amount of silver ion release in ionic solutions. A detailed understanding of these factors is essential for controlling and predicting the behaviour of silver-based alloys in various applications, including in the field of prosthetic dentistry.
3.2. Impact of Silver on Cytotoxicity
Cytotoxicity is a mandatory evaluation of medical devices according to standardization which is described by ISO 10993-5 [62]. Cytotoxicity tests are of great interest in terms of their predictive capacity, reliability and reproducibility. Cytotoxicity tests consist of the in vitro evaluation of reactions induced by materials or extracts on mammalian cells. Cell lines are used typically in these kinds of studies. Cell lysis (cell death), inhibition of cell growth, colony formation, and other effects on cells caused by the presence of materials or extracts in cell culture media are evaluated. To enhance the evaluation of cytotoxic effects and ensure the reliability of cytotoxicity test results, it is important to adhere to several guidelines. These include employing a variety of measurement techniques and utilizing multiple cell lines to provide a comprehensive assessment; additionally, incorporating both negative and positive controls in the testing protocol is essential. The tests should also facilitate quantitative or semi-quantitative analysis, allowing for the classification of results into multiple levels of toxicity. By following these rules, the correlation between different cytotoxicity tests can be improved, leading to more valuable outcomes.
In our study, we tested the silver alloys with a high concentration of silver (Code #6 with 59%Ag, Code #7 with 58.5% Ag and Code#8 with 59% Ag) and also two alloys with reduced silver content (Code#9 with 26% Ag and Code #10 with 22.4% Ag).
3.2.1. Extract Dilution Method
As it is illustrated in Figure 3 silicone gave no significant effects in the MTT assays, while the positive control (copper extract) elicited cytotoxic effect in every dilution of the series (1x- 8x). Higher dilution gave no significant effects on the MTT reduction. The silver alloy #8 with 59 % Ag in composition gave no effects on MTT reduction compared to the negative control, while the MTT reduction was significantly decreased in the copper dilution series (Figure 3). The BrdU incorporation of Hela-cells was significantly decreased by molar concentrations of zinc and nickel between 5 x 10-4 M and 1.25 x 10 -4 M. Lower zinc/nickel concentrations elicited no significant effect on the BrdU-incorporation of this ceil type, while silicone was also ineffective.
Figure 4 illustrates the effects of Zn/Ni-ions in defined molar concentrations on the BrdU incorporation of HeLa cells in comparison to those of an extract dilution series of a selected non-amalgam. It could be shown that the alloy coded #8 elicited no significant effects on the BrdU incorporation of HeLa, while zinc/nickel had deleterious effects. The results of the experiment conducted on sample coded #8 on HeLa were representative of further experiments performed on sample alloys coded #6, #7, #9 and #10, showing no significant reduction of the BrdU-incorporation. The data were also representative of extract dilution experiments on samples coded #6 - #10 using the cell line L-929, as well as primary isolated human fibroblasts, independent of the alloy which had to be tested.
3.2.2. Direct Contact Tests
Human fibroblasts elicited a monolayer-like growth when being cultured on Thermanox tissue culture plates (Figure 3), which represented the internal negative control of the direct contact experiments. Darkfield illumination of copper-wire which had been incubated with human fibroblasts under the same standard culture conditions elicited massive cytotoxic effects (Figure 4).
Thus, only some cells remained adherent on the metal surface and gave a rounded-up shape. The silicone negative control gave a different shape of cellular growth compared to the Thermanox control, with a colony-like growth being found on this polymeric material (Figure 5). Figure 6 illustrates the results of the direct contact tests on the silver-based alloy coded #10. Human fibroblasts presented a monolayer structure after standard culture on this material, which was comparable to the monolayer found on Thermanox plates. Clear cytotoxic effects were not found. Overall, after the three tests (morphological evaluation, MTT-test (evaluation of cell viability) and BrdU labelling index (evaluation of cell proliferation)) conducted on the three types of cell cultures, it was possible to characterize the dental alloys according to the grade of positivity acquired (Table 5).
According to the indications of the ISO 10993-5 standard, the levels of cytotoxicity can be categorized in different levels: "0" means non-cytotoxic, "1" - slightly cytotoxic, “2” – mildly cytotoxic, "3" - moderately cytotoxic, "4" - severely cytotoxic [62] Our result regarding the cytotoxicity of the tested alloys are presented in Figure 7, in accordance with ISO 10993-5 standard [62].
Based on the results of the in vitro cytotoxicity assessment results, the alloys tested in this study do not pose a risk when used in the oral cavity.
The study of the cellular cytotoxicity of dental alloys has been the subject of numerous studies. Graig et al. [70, 71] studied more than 70 valuable and non-precious alloys for the conventional technique and for the ceramic-metal technique on Balb/c 3T3 cell lines. The surface analyses of the samples using ESCA, the quantification of released cations measured by atomic absorption spectroscopy and the observed cellular damage resulting from cellular metabolic activity allow the authors to draw several conclusions, as follows: cytotoxicity varies with the composition of the alloy; the surface condition (polished or unpolished) also plays an important role, the polished surfaces show better tolerance; the presence of Cu, Ni, Cd in precious alloys can lead to deterioration of biological tolerance; the non-precious alloys Co-Cr also show good tolerance, probably due to the formation of a chromium oxide layer [70, 71]. Bumgarner et al. [72] studied copper-based alloys (with 58 to 87% Cu) on gingival fibroblast cell lines in two media (Waymouth's MB752/1 medium and RPMI 1640 medium) and arrived at similar conclusions: the concentration of copper cations released into the biological medium (16.0 ppm in Waymouth's and 10 ppm in RPMI) reduce cell proliferation, i.e., DNA replication, and thus, these alloys exhibit high cytotoxicity. On the other hand, Knun and Rae [73] suggested that concerns regarding the biocompatibility of nickel alloys should be considered, as the safety of these alloys for use in the human body remains uncertain [73]. Watha et al. [74,75] have also tested more than 100 pure alloys and metals using the direct contact technique with MTT [74,75]. This encompasses virtually all alloy systems available on the market. Based on these results, they classified the alloys according to cytotoxic response (cell viability) into four groups:
- −
- "A", alloys that reveal cytotoxicity close to Teflon (90% to 100% cell viability). In this group are silver-palladium-based alloys, gold-rich alloys, and medium-grade gold alloys.
- −
- "B", alloys that reveal a cellular viability of between 70-89% and that do not represent any risk of toxicity in the oral environment. In this group are classified the titanium-based alloys and silver-based alloys.
- −
- "C", alloys that reveal a cellular viability between 45 -69%, therefore represent significant cytotoxicity, and which may represent a risk of toxicity from their use in the mouth.
- −
- "D", alloys that reveal a cell viability < 44%, therefore have a strong cytotoxic response. In this group are classified metals such as nickel, copper and gold-nickel and gold-cadmium alloys.
Moreover, Wataha et al. [76] also studied the toxicity of silver in cell culture, presenting the cell activity response of Balb/c mouse fibroblasts as a function of the concentration of Ag+1 ions. After the contact test, the cell layer was separated from the material and cell viability was checked; over the entire cell layer, only living cells could be stained by the MTT formazan dye in a blue color [76]. The findings of this study indicated that gold (Au), indium (In), and palladium (Pd) typically did not dissolve in the medium, whereas silver (Ag), cadmium (Cd), copper (Cu), gallium (Ga), nickel (Ni), and zinc (Zn) dis-solved frequently [76]. The commercial dental alloys investigated in this research [76] showed complex and unpredictable release behavior [76].
As a resolution, it can be stated that scientific literature presents fragmented data on silver. Silver appears to be an inhibitor of the repair of DNA, but only at concentrations greater than 1mg/L on bacteria [77]. Some studies suggested that silver does not appear to induce gene mutations or primary lesions in bacteria [78,79] and on mammalian cells [80,81]. Although certain studies are limited in their protocol, it is difficult to select available and reliable data that suggest a mutagenic and carcinogenic risk. However, in this context, relatively recent studies revealed that silver nanoparticles can produce genotoxic effects, observed especially for in vitro, but also for in vivo studies [82-85]. A thorough geno-toxicological assessment of silver nanoparticles is essential for informed decision-making [82].
Limits of the study
The limited number of the investigated silver-based dental alloys and test performed may be considered limitations of this study. Furthermore, this in vitro study has limitations regarding the applicability of the results to the actual oral conditions. The tests were conducted under conditions that do not specifically replicate the oral environment; they do not aim to precisely simulate what occurs in the oral cavity. During the tests, the neutrality of the cellular environment must remain perfectly constant, which is not characteristic of the oral environment; additionally, the cell lines used can differ significantly from oral/gingival tissue cells. This raises questions about whether the effects observed in cell culture assays accurately reflect the behavior of dental alloys in the oral environment. Scientific research demonstrated that the in vitro cell culture technique is well-suited for an initial approach to analyzing processes related to the material/tissue interface. It also enables the evaluation of the biological properties of materials for their future use in the oral cavity. In other words, unfavorable results in the evaluation of a material at this stage could imply the rejection of the material under examination. Once a decision is has been made based on the cytotoxicity studies, a follow-up review should be conducted in order to evaluate the biocompatibility and bio-functionality of the material.
Future perspectives
It is acknowledged that the toxicity assessment tests carried out on the population of Canada [48] have demonstrated rigor, competence, scientific and legislative professionalism. The survey provided reliable data indicating that the risk to human health posed by silver and its compounds is low at the exposure levels examined [48]. This outcome was based on the comparison of total silver concentrations measured in human whole blood with levels associated with health effects. On the other hand, there is about 30 years of knowledge and experience in migration tests for nickel [86]. Currently, extremely low concentrations of nickel cations, on the order of 0.2 μg/L, are measured in extracts using ICP-MS Inductively Coupled Plasma Mass Spectrometry).
On dental alloys, ions extractions are carried out in specific biological media, plasma, artificial saliva, lactic acid, urea, etc., and concentrations of released cations are measured in the order of micrograms per liter. The MDD93/42/EEC directive [87] stipulates these requirements for a medical device.
Consequently, it is possible that future scientific advancements will enable the development an extraction method that could be applied to metallic objects (comprising silver and silver-based metal alloys), quantifying silver concentrations in μg/cm²/week. This constitutes the straightforward, easy aspect of the research. However, the challenging component involves correlating these values with the total silver concentrations found in human whole blood. Such correlations could potentially align with data derived from the Canadian survey [48]. Addressing this complex issue will likely necessitate the collaboration of multidisciplinary team. In this context, it may be possible to develop a new legal framework to enhance consumer protection in the future.
Historically recognized for its antiseptic properties, silver continues to serve as an inorganic antimicrobial agent [61]. Recent scientific research highlights the use of silver-embedded materials or and of those coated with silver to combat bacterial infections associated with dental implants [61,88-90] and to demonstrate its broad antibacterial properties in various conditions, without damaging mammalian cells at the given concentrations [61,91,92].
Today, the European Chemicals Agency has opted to include silver in the list of biocidal substances, specifically in the forms of ionic silver (Ag+) and silver nanoparticles. While nano-silver offers numerous advantages across microbiological, health, and consumer applications, it remains unclassified under the European Regulation on Chemical Substances (REACH) [65]. Considering the presented elements, this topic seems to be important and warrants further research. [93,94].
The basic principle of the Biocidal Products Regulation (Regulation (EU) No 528/2012 (BPR)) [95] is that a biocidal product must be authorized before it can be made available on the market or used in the European Economic Area (EEA). First, the active substance (Anti) of the product is evaluated and, if the criteria are met, it is then approved in the specified product type. The second step is the authorization of each product consisting of, containing or generating the approved active substance(s). Under these conditions, dental alloys that are classified as medical devices are not affected, but other materials that contain silver and used by the consumer can be included in the restrictions of the new EU regulation.
5. Conclusions
Within the limitations of this study, we have reached the following conclusions:
- The quantities of silver detected during the extraction tests were minimal, suggesting no significant concerns related to toxicity;
- Based on the results of cytotoxicity assessment, it has been determined that the silver-based dental alloys included in our study do not pose a risk to the oral cavity when utilized.
- In the future, it may be necessary for dental alloys to be accompanied by a certificate detailing the cations released into an appropriate biological medium. This documentation could pave the way for innovative strategies and guidelines in the development of new methods to protect patients and consumers based on the latest knowledge. It's plausible that as medical standards evolve and our understanding of material science and its biological impacts deepens, such requirements could become more common to better protect patients from potential toxicity or allergic reactions. Such measures would also help in maintaining quality control and traceability of materials used in dental practices.
Supplementary Material
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, L.R. and M.P.; methodology, L.R. and N.C.F; software, L.R. and D.A.F.; validation, L.R., N.C.F. and M.P.; formal analysis, L.R. and M.P.; investigation, L.R.; resources, L.R., D.A.F.; data curation, N.C.F. and D.A.F.; writing—original draft preparation, L.R., M.P., and N.C.F; writing—review and editing, L.R., M.P, and N.C.F.; visualization, N.C.F., D.A.F. and M.P.; supervision, L.R.; project administration, L.R.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hill, WR; Pillsbury, D.M. Argyria: the pharmacology of silver. Baltimore, MD, U.SA. Williams & Wilkins Company, 1939.
- Gold, K.; Slay, B.; Knackstedt, M.; Gaharwar, A.K. Antimicrobial activity of metal and metal-oxide based nanoparticles. Advanced Therapeutics 2018, 1, 1700033. [Google Scholar] [CrossRef]
- Lemire, J.A; Harrison, J.J.; Turner, R.J. Antimicrobial activity of metals: mechanisms, molecular targets and applicationsNature Reviews. Microbiology 2013, 11, 371–384. [Google Scholar] [CrossRef]
- Alexander, J.W. History of the medical use of silver. Surgical infections 2009, 10, 289–292. [Google Scholar] [CrossRef]
- Borkow, G.; Gabbay, J. Copper, An ancient remedy returning to fight microbial, fungal and viral infections. Current Chemical Biology 2009, 3, 272–278. [Google Scholar]
- Silver, S.; Phung, L. T.; Silver, G. Silver as biocides in burn and wound dressings and bacterial resistance to silver compounds. Journal of industrial microbiology and biotechnology 2006, 33, 627–634. [Google Scholar] [CrossRef]
- Marshall, J. P.; Schneider, R. P. Systemic argyria secondary to topical silver nitrate. Archives of Dermatology 1977, 113, 1077–1079. [Google Scholar] [CrossRef]
- Shelley, W. B.; Shelley, E. D.; Burmeister, V. Argyria: the intrademal “photograph,” a manifestation of passive photosensitivity. Journal of the American Academy of Dermatology 1987, 16, 211–217. [Google Scholar] [CrossRef]
- Gulbranson, S. H.; Hud, J. A.; Hansen, R. C. Argyria following the use of dietary supplements containing colloidal silver protein. Cutis-New York 2000, 66, 373–378. [Google Scholar]
- Weir, F.W. Health hazard from occupational exposure to metallic copper and silver dust. Am Ind Hyg Assoc J 1979, 40, 245–247. [Google Scholar] [CrossRef]
- James, R.C.; Roberts, S.M.; Williams, P.L. General principles of toxicology. In Principles of toxicology: environmental and industrial applications, Second edition, John Wiley and Sons, Inc., New York, U.S.A., 2000; pp. 3–4.
- Brooks, S.M. Lung disorders resulting from the inhalation of metals. Clin Chest Med 1981, 2, 235–254. [Google Scholar] [CrossRef]
- Rosenman, K.D.; Moss, A.; Kon, S. Argyria: clinical implications of exposure to silver nitrate and silver oxide. J Occup Med 1979, 21, 430–435. [Google Scholar]
- Pifer, J.W.; Friedlander, B.R.; Kintz, R.T.; Stockdale, D. K. Absence of toxic effects in silver reclamation workers. Scand J Work Environ Health 1989, 15, 210–221. [Google Scholar] [CrossRef]
- Breitstadt, R. Occupational exposure limits for metallic silver. In Proceedings of the 2nd European Precious Metals Conference, Lisbon, Portugal, May 1995, pp. 1–13.
- Williams, N.; Gardner, I. Absence of symptoms in silver refiners with raised blood silver levels. Occup Med 1995, 45, 205–208. [Google Scholar] [CrossRef]
- Silver, S. Bacterial silver resistance: molecular biology and uses and misuses of silver compounds. FEMS microbiology reviews 2003, 27, 341–353. [Google Scholar] [CrossRef]
- Wan, A.T.; Conyers, R.A.; Coombs, C.J.; Masterton, J.P. Determination of silver in blood, urine, and tissues of volunteers and burn patients. Clin Chem 1991, 37, 1683–1687. [Google Scholar] [CrossRef]
- Catsakis, L.H. , Sulica, V.I. Allergy to silver amalgams. Oral Surg 1978, 46, 371–375. [Google Scholar]
- Committee of Ministers, European Committee for Food Contact Materials and Articles (CD-P-MCA) 2021. Available online: https://www.edqm.eu/documents/52006/82182/Terms+of+reference+CD-P-MCA.pdf/54ac2c0e-21e6-676c-ee74-98fc5a43364b?t=1640002298681 (accessed 02.10.2024).
- ISO 8442-2 :1997, Matériaux et objets en contact avec les denrées alimentaires - Coutellerie et orfèvrerie de table - Partie 2 : exigences relatives à la coutellerie et aux couverts en acier inoxydable et en métal argenté. Available online: https://www.iso.org/obp/ui/#iso:std:iso:8442:-2:ed-1:v1:fR (accessed on 20.11.2024).
- ISO 8442-3 :1997, Matériaux et objets en contact avec les denrées alimentaires - Coutellerie et orfèvrerie de table - Partie 2 : exigences relatives à l’orfèvrerie de table et décorative en métal argenté. Available online: https://www.iso.org/fr/standard/2464.html (accessed on 20.11.2024 ).
- Beliles, R.P. The metals. In: Patty’s Industrial Hygiene and Toxicology. Fourth Edition. Edited by Clayton, G.D. and Clayton, F.E., John Wiley & Sons, Inc., New York, U.S.A., 1994; Volume 2, part C.
- Fowler, B.A.; Nordberg, G.F. Silver. In: Handbook on the toxicology of metals. Second Edition. Elsevier, Amsterdam, New York, Oxford; 1986; Volume 2, pp. 55.
- Gill, P.; Richards, K.; Cho, W. C.; Nagarajan, P.; Aung, P. P.; Ivan, D.; Curry, J.L.; Prieto, V.G.; Torres-Cabala, C. A. Localized cutaneous argyria: Review of a rare clinical mimicker of melanocytic lesions. Annals of Diagnostic Pathology 2021, 54, 151776. [Google Scholar] [CrossRef]
- Saint, S.; Veenstra, D.L.; Sullivan, S.D.; Chenoweth, C.; Fendrick, A.M. The potential clinical and economic benefits of silver alloy urinary catheters in preventing urinary tract infection. Archives of Internal Medicine 2000, 160, 2670–2675. [Google Scholar] [CrossRef]
- Rongioletti, F.; Robert, E.; Buffa, P.; Bertagno, R.; Rebora, A. Blue nevi-like dotted occupational argyria. Journal-American Academy of Dermatology 1992, 27, 1015. [Google Scholar] [CrossRef]
- Rosenman, K.D; Seixas, N.; Jacobs, I. Potential nephrotoxic effects of exposure to silver. Br J Ind Med 1987, 44, 267–272. [Google Scholar] [CrossRef]
- Żyro, D.; Sikora, J.; Szynkowska-Jóźwik, M.I.; Ochocki, J. Silver, its salts and application in medicine and pharmacy. International journal of molecular sciences 2023, 24, 15723. [Google Scholar] [CrossRef]
- Venugopal, B. , Luckey, T.D. Metal toxicity in mammals. In Chemical toxicology of metals and metalloids. Plenum Press, New York, U.S.A., 1978; 32–36.
- Aaseth, J.; Olsen, A.; Halse, J.; Hovig, T. Argyria-tissue deposition of silver as selenide. Scan J Clin Lab Invest 1981, 41, 247–251. [Google Scholar] [CrossRef]
- Lee, S.M.; Lee, S.H. Generalized argyria after habitual use of AgNO3. J Dermatol 1994, 21, 50–3. [Google Scholar] [CrossRef]
- Seiler, H.G.A.; Sigel, H. Silver. In Handbook on Toxicity of Inorganic Compounds, Editor Marcel Dekker, New York, U.S.A., 1998; pp. 619–24.
- Fung, M.C.; Bowen, D.L. Silver products for medical indications: risk-benefit assessment. Clin Toxicol 1996, 34, 119–26. [Google Scholar] [CrossRef] [PubMed]
- Furst, A.; Schlauder, M.C. Inactivity of two noble metals as carcinogens. J Environ Pathol Toxicol 1978, 1, 51–7. [Google Scholar]
- Espinal, M.L.; Ferrando, L.; Jimenex, D.F. Asymptomatic blue nevus-like macule. Diagnosis: localized argyria. Arch Dermatol 1996, 132, 461–464. [Google Scholar]
- Jensen, E.J.; Rungby, J.; Hansen, J.C.; Schmidt, E.; Pedersen, B.; Dahl, R. Serum concentrations and accumulation of silver in skin during three months treatment with an anti-smoking chewing gum containing silver acetate. Hum Toxicol 1998, 7, 535–540. [Google Scholar] [CrossRef]
- MacIntyre, D. Silver poisoning associated with anti-smoking lozenge. Br Med J 1978, 2, 1749–1759. [Google Scholar] [CrossRef]
- Van Garsse, L.; Versieck, J. General argyria caused by administration of tobacco-withdrawal tablets containing silver acetate. Nederlands Tijdschrift Voor Geneeskunde 1995, 139, 2658–2661. [Google Scholar]
- Gaslin, M. T.; Rubin, C.; Pribitkin, E. A. Silver nasal sprays: misleading Internet marketing. Ear, Nose & Throat Journal 2008, 87, 217–220. [Google Scholar]
- Mora, N. F.; De Los Bueis, A. B. Ocular argyrosis. Oman Journal of Ophthalmology 2023, 16, 373–376. [Google Scholar] [CrossRef]
- Cirigliano, F.; Meschia, A.; Taietti, D.; Aliverti, M.; Wu, M.A. Painted in black: deciphering the cornerstones of a challenging case. Internal and Emergency Medicine 2024, 1–3. [Google Scholar] [CrossRef]
- Kowalczyk, P.; Szymczak, M.; Maciejewska, M.; Laskowski, Ł. ; Laskowska, M; Ostaszewski, R.; Skiba, G.; Franiak-Pietryga, I. All that glitters is not silver—a new look at microbiological and medical applications of silver nanoparticles. International Journal of Molecular Sciences, 2021; 22, 854. [Google Scholar]
- Farhadian, N.; Mashoof, R.U.; Khanizadeh, S.; Ghaderi, E.; Farhadian, M.; Miresmaeili, A. Streptococcus mutans counts in patients wearing removable retainers with silver nanoparticles vs those wearing conventional retainers: A randomized clinical trial. American Journal of Orthodontics and Dentofacial Orthopedics 2016, 149, 155–160. [Google Scholar] [CrossRef]
- Drake, P.L.; Hazelwood, K.J. Exposure-related health effects of silver and silver compounds: a review. Annals of Occupational Hygiene 2005, 49, 575–585. [Google Scholar]
- Silver and Compounds, American Conference of Governmental Industrial Hygienists (ACGIH). Available online : https://www.acgih.org/silver-and-compounds/ (accessed on 02.10.2024).
- Hays, S.M.; Aylward, L.L.; LaKind, J.S.; Bartels, M.J.; Barton, H.A.; Boogaard, P.J.; Brunk, C.; DiZio, S.; Dourson, M.; Goldstein, D.A.; Lipscomb, J.; Kilpatrick, M.E.; Krewski, D.; Krishnan, K.; Nordberg, M.; Okino, M. ; Yu-Mei Tan, Y-M.; Viau, C.; Yager, J.W. Guidelines for the derivation of Biomonitoring Equivalents: report from the Biomonitoring Equivalents Expert Workshop. Regul Toxicol Pharmacol 2008, 51, S4-15. [Google Scholar] [CrossRef]
- Argent et ses composés, Santé Canada, 2022. Available online : Argent et ses composés — Fiche d’information - Canada.ca (accessed on 02.10.2024). (accessed on 02.10.2024).
- Steck, M.B.; Murray, B.P. SilverToxicity. In StatPearlsPublishing, 2024. Available on line: https://www.ncbi.nlm.nih.gov/books/NBK604211/ (accessed on 02.11.2024).
- World Health Organization (WHO), Guidelines for drinking-water quality. Second edition, 1993. Available online: https://iris.who.int/bitstream/handle/10665/259956/9241544600-eng.pdf?sequence=1 (accessed on 20.11.2024 ).
- The French Agency for Food, Environmental and Occupational Health & Safety (ANSES) Etude de l’alimentation totale française 2 (EAT 2), Tome 1 : contaminants inorganiques, minéraux, polluants organiques persistants, mycotoxines et phytoestrogènes, 2011. Available online: https://www.anses.fr/fr/system/files/PASER2006sa0361.pdf (accessed on 20.11.2024).
- United States Environmental Protection Agency (EPA), Ambient water quality criteria for silver, 1980. Available online:.
- https://www.epa.gov/sites/default/files/2019-03/documents/ambient-wqc-silver-1980.pdf (accessed on 20.11.2024).
- United States Environmental Protection Agency (EPA), Integrated Risk Information System, Silver (CASRN 7440-22-4), 1987. Available online: https://iris.epa.gov/static/pdfs/0099_summary.pdf (accessed on 20.11.2024).
- World Health Organization (WHO), Directives de qualité pour l’eau de boisson, Deuxième édition, Volume 1, Recommandations, 1995. Available online: https://iris.who.int/bitstream/handle/10665/259937/9242541680-fre.pdf?sequence=1&isAllowed=y (accessed on 20.11.2024).
- World Health Organization (WHO), Silver in drinking-water. Background document for preparation of WHO Guidelines for drinking-water quality, 2003. Available online: https://cdn.who.int/media/docs/default-source/wash-documents/wash-chemicals/silver.pdf?sfvrsn=195cf8b3_4 (accessed on 20.11.2024).
- World Health Organization (WHO), Directives sur la qualité de l’eau de boisson, Troisieme édition incorporant les 1er et 2e addendum, Volume 1, Recommandations, 2004. Available online: https://www.pseau.org/outils/ouvrages/oms_directives_de_qualite_pour_l_eau_de_boisson_vol1_recommendations_2004.pdf (accessed on 20.11.2024).
- World Health Organization (WHO), Directives sur la qualité de l’eau de boisson, Quatrième édition, 2017. Available online https://iris.who.int/bitstream/handle/10665/258887/9789242549959-fre.pdf (accessed on 20.11.2024).
- Gaul, L.E.; Staud, A.H. Clinical spectroscopy. Seventy cases of generalized argyrosis following organic and colloidal silver medication. J. Am. Med. Assoc. 1935, 104, 1387–1390. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA), Opinion of the Scientific Panel on food additives, flavourings, processing aids and materials in contact with food (AFC) related to a 7th list of substances for food contact materials. Available on line : https://efsa.onlinelibrary.wiley.com/doi/epdf/10.2903/j.efsa.2005.201a (accessed on 20.11.2024). (accessed on 20.11.2024).
- European Food Safety Authority (EFSA), Opinion of the Scientific Panel on food additives, flavourings, processing aids and materials in contact with food (AFC) on a 4th list of substances for food contact materials. The EFSA Journal 2004, 1-17. Available online: https://efsa.onlinelibrary.wiley.com/doi/epdf/10.2903/j.efsa.2004.65a (accessed on 20.11.2024).
- Gkioka, M.; Rausch-Fan, X. Antimicrobial Effects of Metal Coatings or Physical, Chemical Modifications of Titanium Dental Implant Surfaces for Prevention of Peri-Implantitis: A Systematic Review of In Vivo Studies. Antibiotics 2024, 13, 908. [Google Scholar] [CrossRef] [PubMed]
- ISO 10993-5:2009. Biological evaluation of medical devices — Part 5: Tests for in vitro cytotoxicity. Available online: https://www.iso.org/obp/ui/#iso:std:iso:10993:-5:ed-3:v1:en; accessed on 20.11.2024).
- ISO 10271:2020. Dentistry — Corrosion test methods for metallic materials. Available online: https://www.iso.org/obp/ui/#iso:std:iso:10271:ed-3:v1:en (accessed on 20.11.2024).
- Mosmann, T. Rapid colorimetric assay for cellular growth and survival: application to proliferation and cytotoxicity assays. Journal of immunological methods, 1983, 65, 55–63. [Google Scholar] [CrossRef]
- Gratzner, H. G. Monoclonal antibody to 5-bromo-and 5-iododeoxyuridine: a new reagent for detection of DNA replication. Science, 1982, 218, 474–475. [Google Scholar] [CrossRef]
- Substance Evaluation Conclusion as Required by REACH Article 48 and Evaluation Report for Silver EC No 231-131-3 CAS No 7440-22-4, Evaluating Member State(s): The Netherlands, 2018, REACH. Available online: https://echa.europa.eu/documents/10162/776ad739-c591-16fd-2e2c-62b9e50169ee (accessed on 20.11.2024).
- Steppan, J.J.; Roth, J.A.; Hall, L.C.; Jeannotte, D.A.; Carbone, S.P. A review of corrosion failure mechanisms during accelerated tests: electrolytic metal migration. Journal of the electrochemical society 1987, 134, 175–188. [Google Scholar] [CrossRef]
- Vu, K. Silver migration–The mechanism and effects on thick-film conductors. Mater Sci Eng 2003, 234, 1–21. [Google Scholar]
- Reclaru, L.; Meyer, J. M. Zonal coulometric analysis of the corrosion resistance of dental alloys. Journal of Dentistry 1995, 23, 301–311. [Google Scholar] [CrossRef]
- Graig, R.G. Reaction of fibroblast to various dental casting alloy. J. Oral Pathol 1988, 17, 341–347. [Google Scholar]
- Craig, R. G.; Hanks, C. T. Cytotoxicity of experimental casting alloys evaluated by cell culture tests. Journal of Dental Research 1990, 69, 1539–1542. [Google Scholar] [CrossRef] [PubMed]
- Bumgardner, J. D.; Lucas, L. C.; Tilden, A. B. Toxicity of copper-based dental alloys in cell culture. Journal of Biomedical Materials Research, 1989, 23, 1103–1114.
- Kuhn, A. T.; Rae, T. Aqueous corrosion of Ni-Cr alloys in biological environments and implications for their biocompatibility. British Corrosion Journal 1988, 23, 259–268. [Google Scholar] [CrossRef]
- Wataha J., C.; Hanks C., T.; Craig R., G. In vitro synergistic, antagonistic, and duration of exposure effects of metal cations on eukaryotic cells. J. Biomed. Mater. Res. 1992, 26, 1297–1309. [Google Scholar] [CrossRef]
- Wataha, J. C.; Malcolm, C. T.; Hanks, C. T. Correlation between cytotoxicity and the elements released by dental casting alloys. International Journal of Prosthodontics, 1995, 8, 9–14.
- Wataha, J. C.; Craig, R. G.; Hanks, C. T. The release of elements of dental casting alloys into cell-culture medium. J. Dent. Res, 1991, 70, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Takashi, K.; Imaeda, T.; Kwazoe, Y. Effect om metals ions on the adaptive response induced by methyl-N-Nitrosourea in Escherichia Coli, Biochemical and Biophysical Research Communications 1988, 157, 1124–1130.
- Olivier, P.; Marzin, D. Study of Genotoxic Potential 48 Inorganic Derivatives whit the SOS Chromotest, Muation Research 1987, 189, 263–269.
- Kanematsu, N.; Hara, M.; Kada, T. Rec assay and mutagenicity studies on metal compounds. Mutation Research/Genetic Toxicology, 1980, 77, 109–116. [Google Scholar] [CrossRef]
- Dusinska, M. , Slamenova D., Effect of Silver Compounds on Invitro Cultured Mammalian Cells, II Study of Genotoxicity and the Effect of DiammineSilver TetraBorate on Macromolecular Synthesis of V79 Cells. Biologia 1990, 45, 211–218. [Google Scholar]
- Denizeau, F. , Marion, M. . Genotoxic effects of heavy metals in rat hepatocytes. Cell biology and toxicology 1989, 5, 15–25. [Google Scholar] [PubMed]
- Rodriguez-Garraus, A.; Azqueta, A.; Vettorazzi, A.; Lopez de Cerain, A. Genotoxicity of silver nanoparticles. Nanomaterials 2020, 10, 251. [Google Scholar] [CrossRef]
- McShan, D.; Ray, P.C.; Yu, H. Molecular toxicity mechanism of nanosilver. J. Food Drug Anal. 2014, 22, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Abdal Dayem, A.; Hossain, M.; Lee, S.; Kim, K.; Saha, S.; Yang, G.; Choi, H.; Cho, S. The Role of Reactive Oxygen Species (ROS) in the Biological Activities of Metallic Nanoparticles. Int. J. Mol. Sci. 2017, 18, 120. [Google Scholar] [CrossRef] [PubMed]
- Dakal, T.C.; Kumar, A.; Majumdar, R.S.; Yadav, V. Mechanistic Basis of Antimicrobial Actions of Silver Nanoparticles. Front. Microbiol. 2016, 7, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Genchi, G.; Carocci, A.; Lauria, G.; Sinicropi, M. S.; Catalano, A. Nickel: Human health and environmental toxicology. h Int. J. Environ. Res. Public Health 2020, 2020 17, 679. [Google Scholar] [CrossRef]
- MDD93/42 EEC: Council Directive 93/42/EEC of 14 June 1993 concerning medical devices. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A31993L0042 (accessed on 17.11.2024).
- Soma, T.; Iwasaki, R.; Sato, Y.; Kobayashi, T.; Ito, E.; Matsumoto, T.; Kimura, A.; Homma, F.; Saiki, K.; Takahashi, Y.; et al. An ionic silver coating prevents implant-associated infection by anaerobic bacteria in vitro and in vivo in mice. Sci. Rep. 2022, 12, 18387. [Google Scholar] [CrossRef]
- Boutinguiza, M.; Fernández-Arias, M.; del Val, J.; Buxadera-Palomero, J.; Rodríguez, D.; Lusquiños, F.; Gil, F.; Pou, J. Synthesis and deposition of silver nanoparticles on cp Ti by laser ablation in open air for antibacterial effect in dental implants. Mater. Lett. 2018, 231, 126–129. [Google Scholar] [CrossRef]
- Esteves, G.M.; Esteves, J.; Resende, M.; Mendes, L.; Azevedo, A.S. Antimicrobial and Antibiofilm Coating of Dental Implants—Past and New Perspectives. Antibiotics 2022, 11, 235. [Google Scholar] [CrossRef]
- Chen, M.; Yang, L.; Zhang, L.; Han, Y.; Lu, Z.; Qin, G.; Zhang, E. Effect of nano/micro-Ag compound particles on the bio-corrosion, antibacterial properties and cell biocompatibility of Ti-Ag alloys. Mater. Sci. Eng. C 2017, 75, 906–917. [Google Scholar] [CrossRef]
- Alshammari, H.; Bakitian, F.; Neilands, J.; Andersen, O.Z.; Stavropoulos, A. Antimicrobial Properties of Strontium Functionalized Titanium Surfaces for Oral Applications, A Systematic Review. Coatings 2021, 11, 810. [Google Scholar] [CrossRef]
- Noga, M.; Milan, J.; Frydrych, A.; Jurowski, K. Toxicological aspects, safety assessment, and green toxicology of silver nanoparticles (AgNPs)—critical review: state of the art. International Journal of Molecular Sciences 2023, 24, 5133. [Google Scholar] [CrossRef]
- Mast, J.; Van Miert, E.; Siciliani, L.; Cheyns, K.; Blaude, M.N.; Wouters, C.; Waegeneers, N.; Bernsen, R.; Vleminckx, C.; Van Loco, J.; Verleysen, E. Application of silver-based biocides in face masks intended for general use requires regulatory control. Science of the Total Environment 2023, 870, 161889. [Google Scholar] [CrossRef]
- Regulation (EU) No 528/2012 of the European Parliament and of the Council of 22 May 2012 concerning the making available on the market and use of biocidal products, Official Journal of the European Union L 167, 27 June 2012, pp. 1–123. Avilable online: https://eur-lex.europa.eu/eli/reg/2012/528/oj (accessed on 17.11.2024).
Figure 1.
Alloy 11.8Au 47.7Ag22.8Pd6.7In6.8Zn: a, prior to corrosion test; b, after first corrosion test; c, after dissolution of silver chloride; d, after second test. Phase Au-Ag (1); Phase Pd-In (2).
Figure 1.
Alloy 11.8Au 47.7Ag22.8Pd6.7In6.8Zn: a, prior to corrosion test; b, after first corrosion test; c, after dissolution of silver chloride; d, after second test. Phase Au-Ag (1); Phase Pd-In (2).
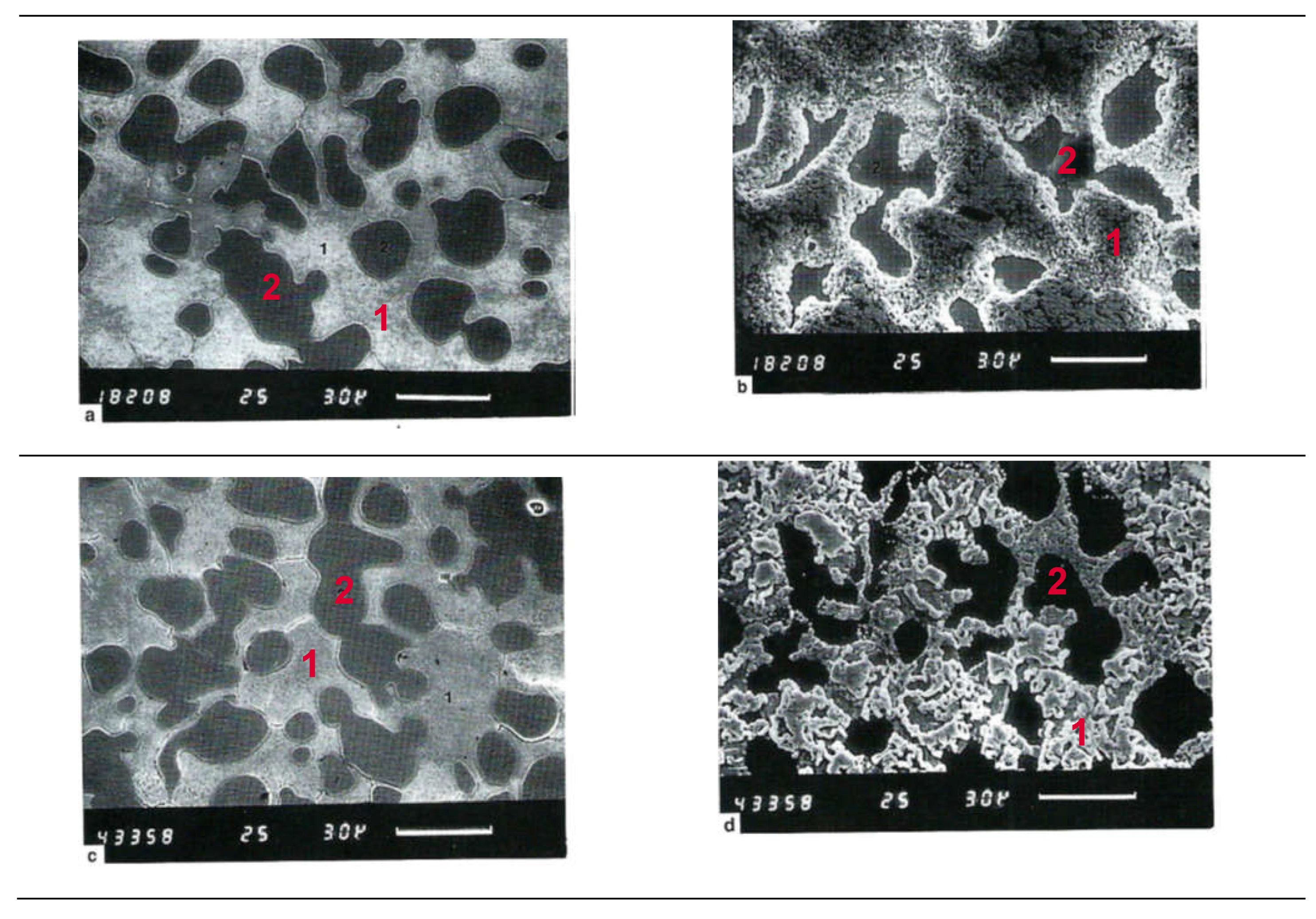
Figure 2.
Alloy 1.6Au 62.7Ag 22.5 Pd 1.8InCu10.6 Zn0.8: a, prior to corrosion test; b, after first corrosion test; c, after dissolution of silver chloride. Phase Au-Ag-Cu (1); Phase Pd-In (2).
Figure 2.
Alloy 1.6Au 62.7Ag 22.5 Pd 1.8InCu10.6 Zn0.8: a, prior to corrosion test; b, after first corrosion test; c, after dissolution of silver chloride. Phase Au-Ag-Cu (1); Phase Pd-In (2).
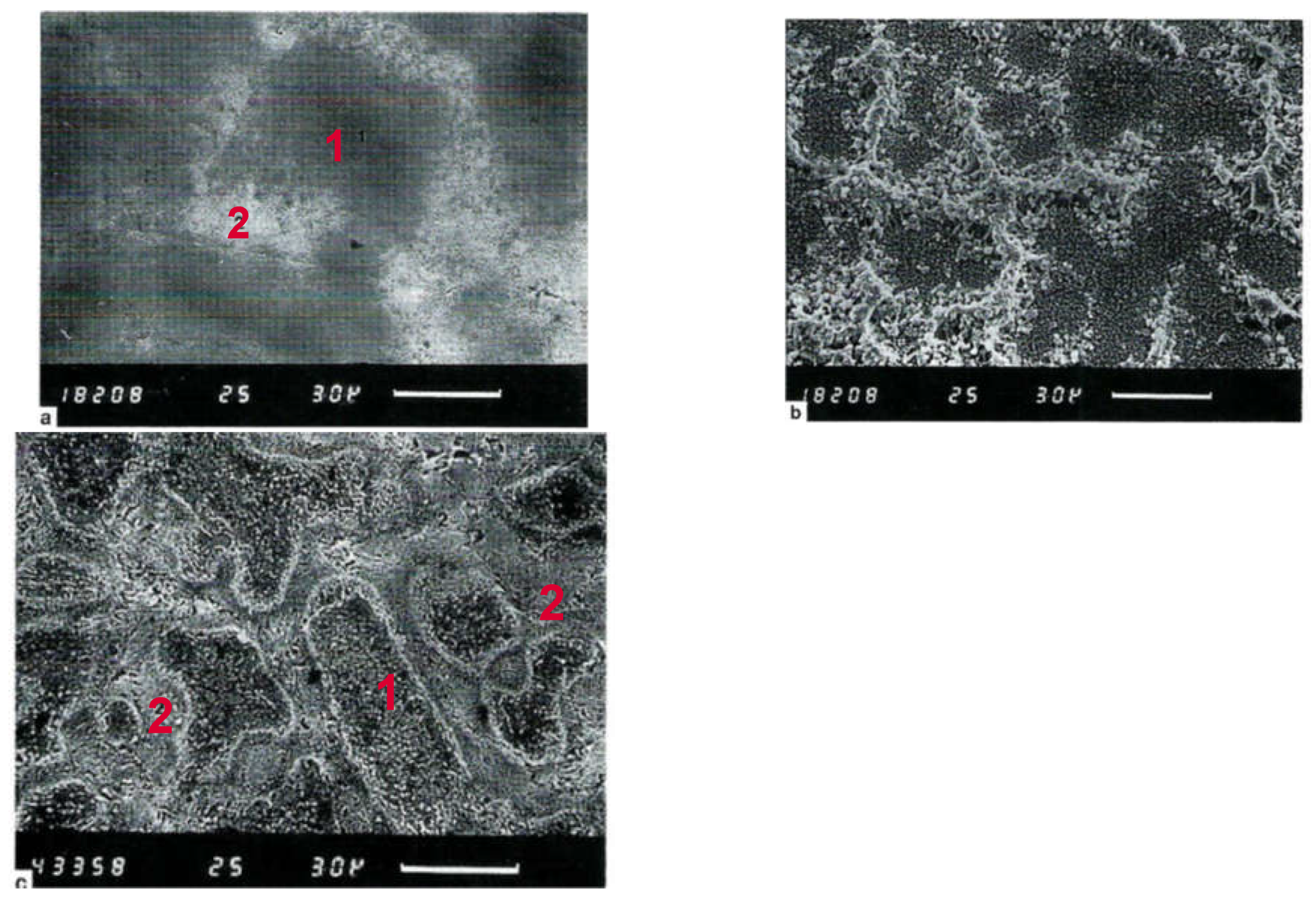
Figure 3.
MTT reduction of human primary isolated fibroblasts after a 24 h incubation with extracts (extract dilution series: Ix—8x, 1 : 1 v/v dilution) of alloy sample coded #8 (24 h medium extraction). Comparison to references: negative: silicone extract and medium control, positive: copper extract dilution series. No cytotoxic effect of the alloy. (mean ISD, n = 4). BIA-data, values given in relative absorbance at 550 nm.
Figure 3.
MTT reduction of human primary isolated fibroblasts after a 24 h incubation with extracts (extract dilution series: Ix—8x, 1 : 1 v/v dilution) of alloy sample coded #8 (24 h medium extraction). Comparison to references: negative: silicone extract and medium control, positive: copper extract dilution series. No cytotoxic effect of the alloy. (mean ISD, n = 4). BIA-data, values given in relative absorbance at 550 nm.
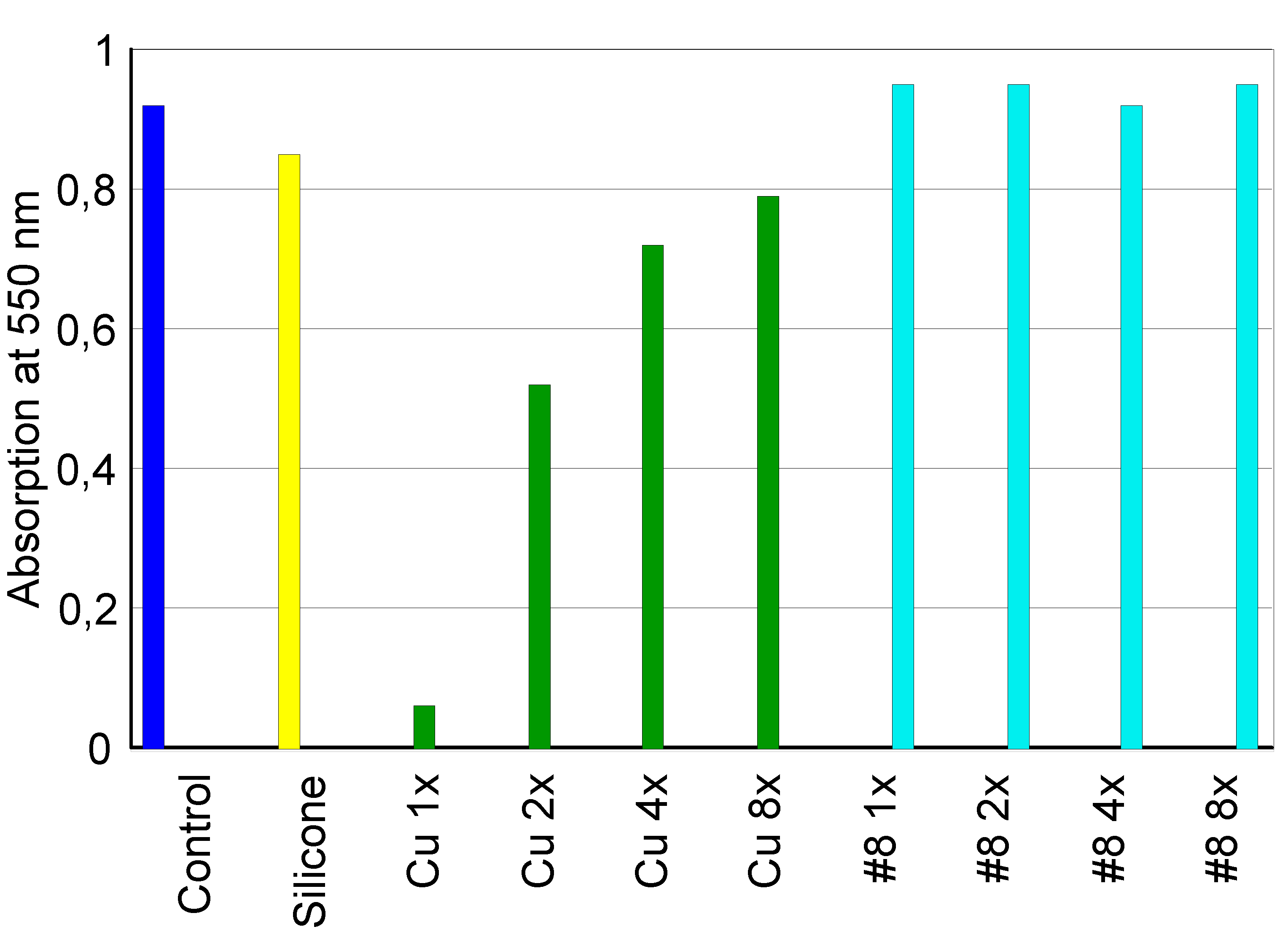
Figure 4.
BrdU-incorporation by HeLa-cells after a 24 h incubation with extracts (extract dilution series: Ix—8x, 1:1 v/v dilution) of alloy sample coded #8 (24 h medium extraction). Comparison to references: negative: silicone extract and medium control, positive: defined molar concentration of Zn/Ni ions. No cytotoxic effects of the tested alloy (mean ISD, n = 4). EIA-data, values given in relative absorbance at 405 nm.
Figure 4.
BrdU-incorporation by HeLa-cells after a 24 h incubation with extracts (extract dilution series: Ix—8x, 1:1 v/v dilution) of alloy sample coded #8 (24 h medium extraction). Comparison to references: negative: silicone extract and medium control, positive: defined molar concentration of Zn/Ni ions. No cytotoxic effects of the tested alloy (mean ISD, n = 4). EIA-data, values given in relative absorbance at 405 nm.
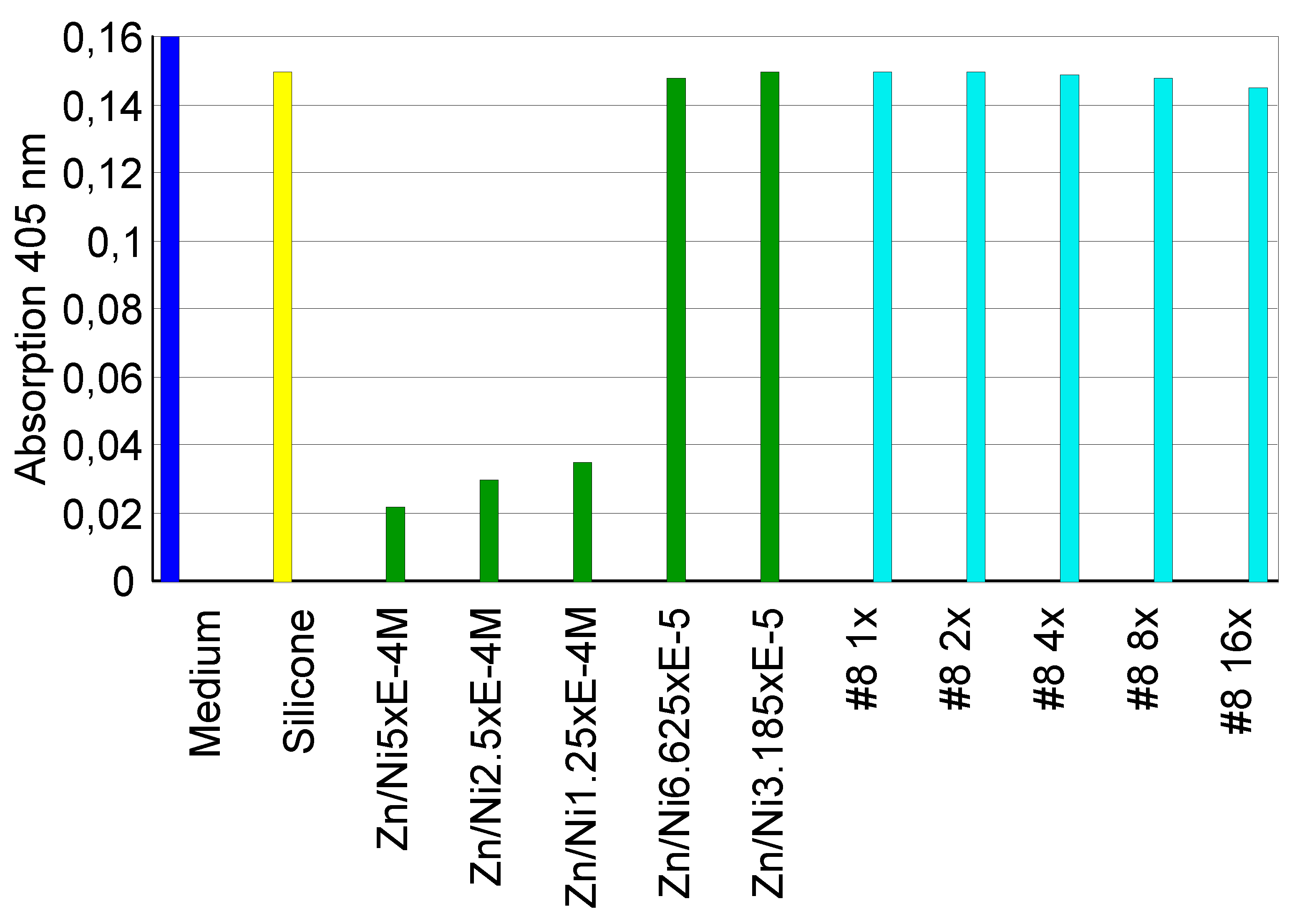
Figure 3.
Negative control: Human fibroblasts cultured under standard culture conditions on Thermanox tissue culture plates. Results of light microscopical analysis: unaffected, confluent monolayer structure (magnification x 65).
Figure 3.
Negative control: Human fibroblasts cultured under standard culture conditions on Thermanox tissue culture plates. Results of light microscopical analysis: unaffected, confluent monolayer structure (magnification x 65).
Figure 4.
Positive control: Human fibroblasts cultured under standard culture conditions on copper. Results of light microscopical analysis by reflected-light darkfield illumination: severe cytotoxic effects, rounded-up cells (magnification x 130).
Figure 4.
Positive control: Human fibroblasts cultured under standard culture conditions on copper. Results of light microscopical analysis by reflected-light darkfield illumination: severe cytotoxic effects, rounded-up cells (magnification x 130).
Figure 5.
Silicone reference: Human fibroblasts cultured under standard culture conditions on silicone. Results of light microscopical analysis; colony-like growth, with no evidence of cytotoxicity (magnification x 65).
Figure 5.
Silicone reference: Human fibroblasts cultured under standard culture conditions on silicone. Results of light microscopical analysis; colony-like growth, with no evidence of cytotoxicity (magnification x 65).
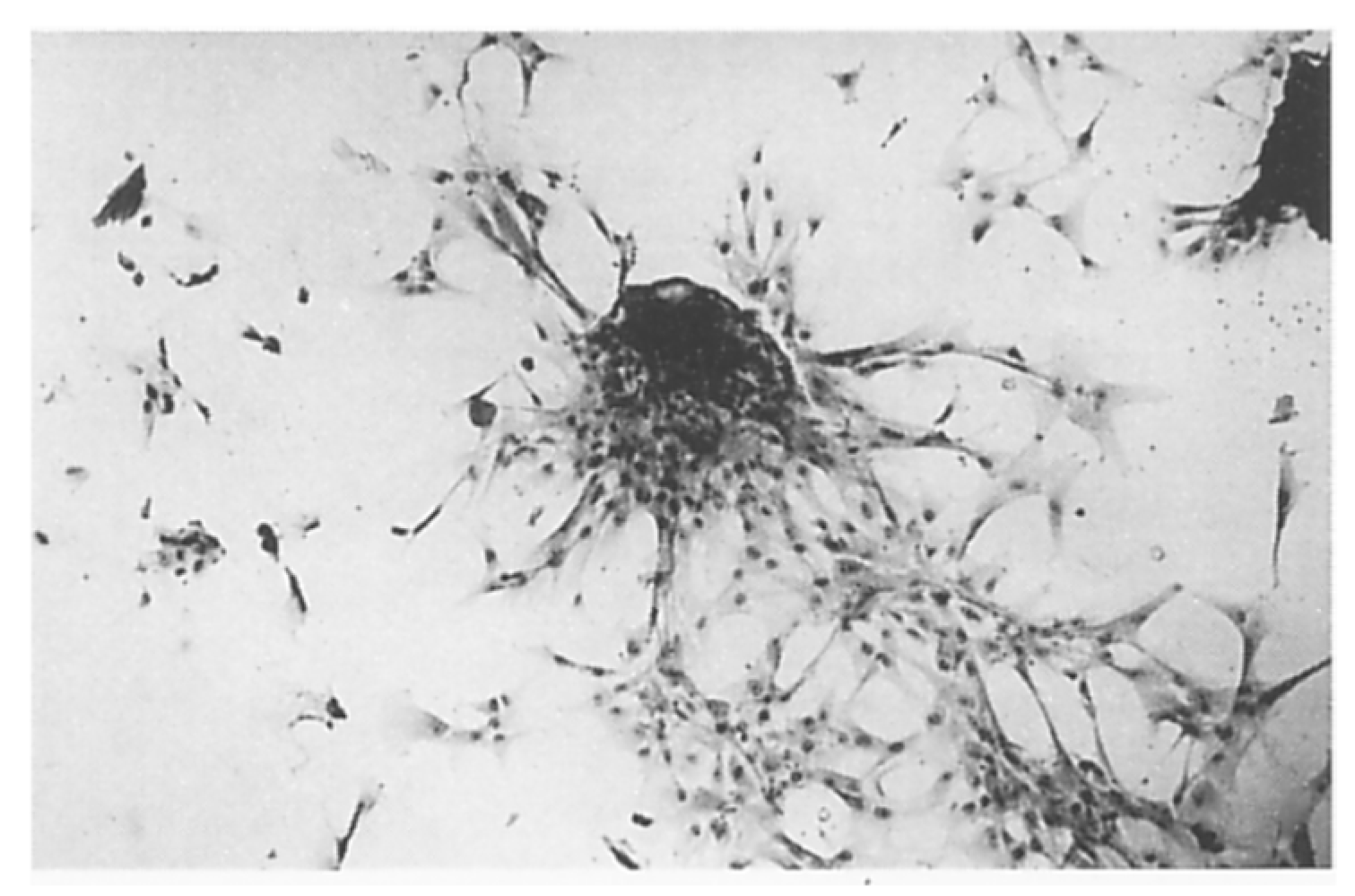
Figure 6.
Human fibroblasts cultured under standard culture conditions on #10. Results of Eight microscopical analysis by reflected-light darkfield illumination: monolayer growth, no evidence of cytotoxicity (magnification x 65).
Figure 6.
Human fibroblasts cultured under standard culture conditions on #10. Results of Eight microscopical analysis by reflected-light darkfield illumination: monolayer growth, no evidence of cytotoxicity (magnification x 65).
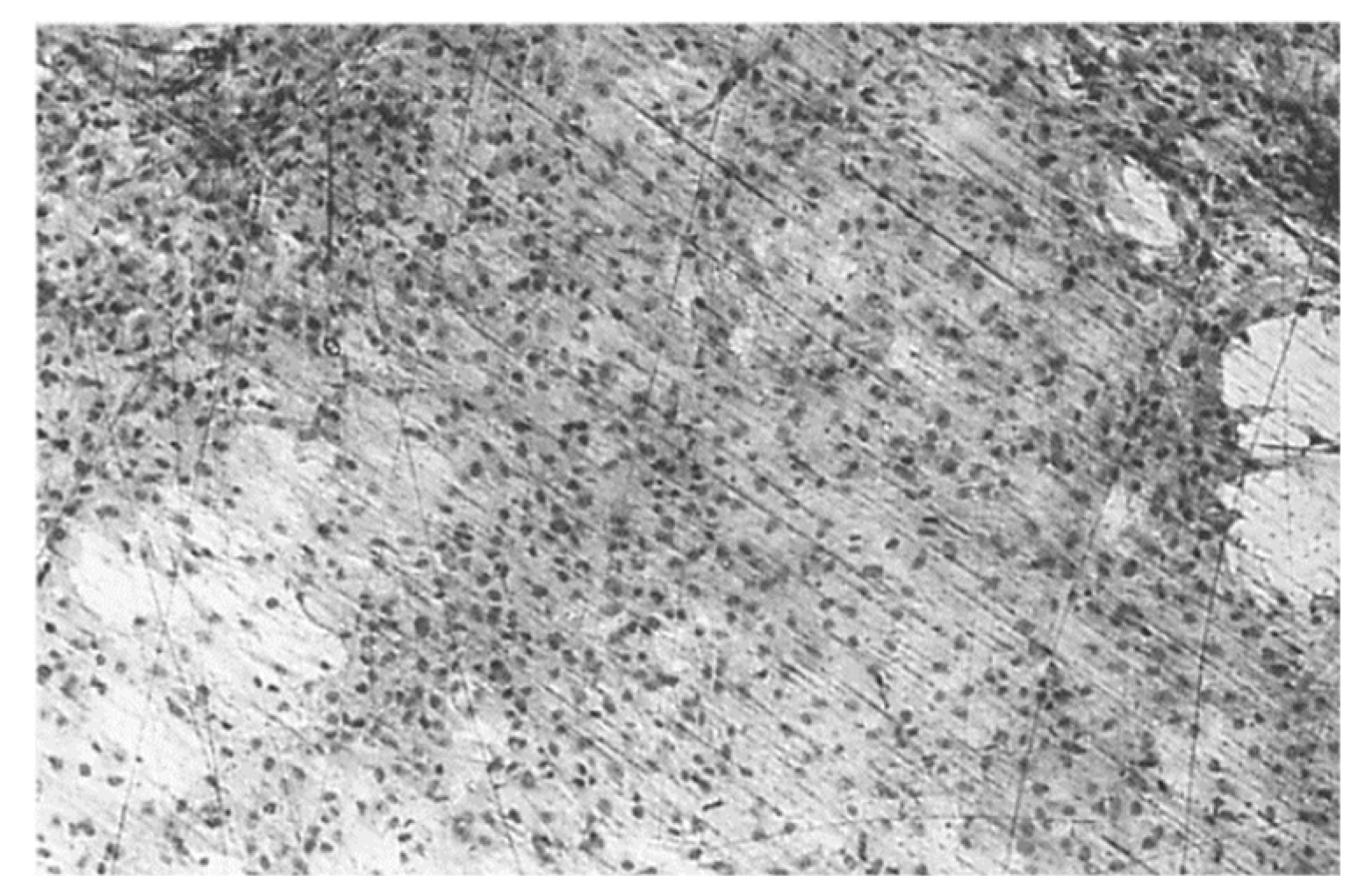
Figure 7.
Cytotoxicity evaluation of the tested silver-based alloys, according to ISO 10993-5 [62].
Figure 7.
Cytotoxicity evaluation of the tested silver-based alloys, according to ISO 10993-5 [62].
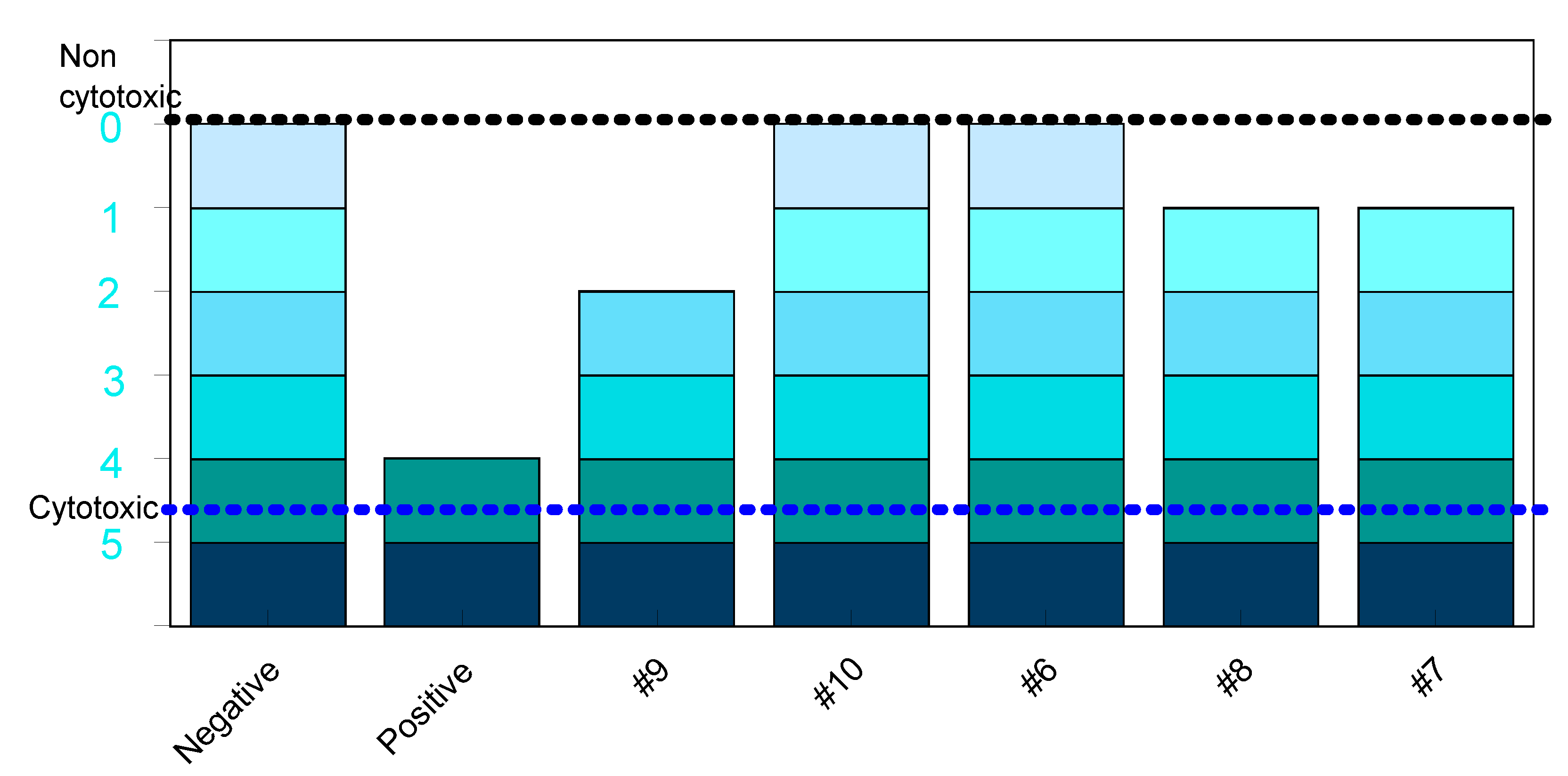

Table 1.
Chemical composition of dental alloys tested for extraction (#1-#5) and cytotoxicity (#6-#10).
Table 1.
Chemical composition of dental alloys tested for extraction (#1-#5) and cytotoxicity (#6-#10).
| Alloy code | Chemical composition in % weight | |||||
| Au | Pt | Pd | Ag | Cu | Zn | |
| #1 | 75.0 | 9.0 | - | 9.2 | 3.0 | - |
| #2 | 72.0 | 3.0 | - | 13.6 | 10.4 | - |
| #3 | 56 | - | 12.0 | 28.0 | - | - |
| #4 | 51 | - | 7.0 | 27.0 | 0.14 | - |
| #5 | 2.0 | - | 32.9 | 58 | 3.5 | - |
| #6 | 3.0 | 4.0 | 20.6 | 59.0 | 11.3 | 2.0 |
| #7 | 2.0 | 0.1 | 27.4 | 58.5 | 10.4 | 1.5 |
| #8 | - | - | 24.9 | 59.0 | 14.0 | 2.0 |
| #9 | 54.8 | - | 6.2 | 26.0 | 10.9 | 2.1 |
| #10 | 58.8 | - | 4.8 | 22.4 | 12.9 | 1.1 |
Table 2.
The results of the extraction tests for the dental alloys coded #1- #5.
| Alloy #1 | Alloy #2 | Alloy #3 | Alloy #4 | Alloy #5 | |||||||||||
| [*] | [**] | σ | [*] | [**] | σ | [*] | [**] | σ | [*] | [**] | σ | [*] | [**] | σ | |
| Ag | 55 | 0.20 | 0.01 | 82 | 0.31 | 0.01 | 103 | 0.38 | 0.01 | 314 | 1.17 | 0.15 | 243 | 0.90 | 0.13 |
| Cu | 92 | 0.34 | 0.01 | - | - | - | 83 | 0.31 | 0.07 | ||||||
| Fe | 64 | 0.24 | 30 | 0.11 | - | 24 | 0.09 | 0.01 | 66 | 0.25 | 0.20 | 60 | 0.22 | ||
| Mo | 12 | 0.04 | - | 10 | 0.04 | ||||||||||
| Zn | 30 | 0.11 | - | ||||||||||||
| Au | 1.0 | 0.004 | 0.000 | 0.7 | 0.002 | 0.000 | 0.7 | 0.003 | 0.001 | 0.7 | 0.003 | 0.00 | 0.4 | 0.001 | 0.00 |
| Cr | 4.8 | 0.02 | 0.01 | 3.8 | 0.01 | 0.00 | 4.5 | 0.02 | 0.00 | 7.5 | 0.03 | 0.02 | 5.4 | 0.02 | 0.01 |
| In | 0.4 | 0.001 | 0.001 | 6.3 | 0.02 | 0.00 | 0.4 | 0.001 | 5.5 | 0.02 | 0.00 | 3.9 | 0.01 | 0.00 | |
| Pd | 2.2 | 0.01 | 0.00 | 2.0 | 0.01 | 0.00 | 1.4 | 0.01 | 0.00 | 2.1 | 0.01 | 0.00 | 4.4 | 0.02 | 0.00 |
| Pt | 0.3 | 0.001 | 0.00 | 0.2 | 0.001 | 0.000 | |||||||||
| Sn | 0.4 | 0.002 | 0.000 | 0.2 | 0.001 | 8.1 | 0.03 | 0.00 | 18 | 0.07 | 0.01 | ||||
[*] in µg/L ; [**] in mg/cm2/week ; σ : standard deviation.
Table 3.
Silver in the chemical composition and the released silver corresponding to the tested. dental alloys (coded #1- #5)
Table 3.
Silver in the chemical composition and the released silver corresponding to the tested. dental alloys (coded #1- #5)
| Alloy code | Quantity of Ag in the chemical composition | Quantity of the released Ag | |
| % weight | [µg/L] | µg/cm2/week | |
| #1 | 9.2 | 55 | 0.20 |
| #2 | 13.6 | 82 | 0.31 |
| #3 | 28.0 | 103 | 0.38 |
| #4 | 27.0 | 314 | 1.17 |
| #5 | 58.0 | 243 | 0.90 |
Table 4.
Cations concentration in composition of Fusayama solution after first corrosion test. Adapted from [69].
Table 4.
Cations concentration in composition of Fusayama solution after first corrosion test. Adapted from [69].
| Alloy | Concentration (µ/L) | |||||
| Au | Ag | Pd | In | Cu | Zn | |
| 11.8Au 47.7Ag 22.8Pd 6.7In 6.8Zn (Figure 1) | 10 | 330 | 15 | 1.5 | 13 | 85 |
| 1.6Au 62.7Ag 22.5 Pd 1.8In Cu10.6 Zn0.8 (Figure 2) | 53 | 640 | 1680 | - | 465 | 80 |
Table 5.
The tested dental alloys according to the grade of positivity acquired.
| Code | Direct#break#contact | By extracts (elution test) | Ranking #break#According ISO 10993-5 | ||
| Cell#break#Viability | Cell#break#Proliferation | Grade of positivity | |||
| #9 | + | +1dil | - | 2nd level | 3 |
| #10 | - | - | - | 0 | 0 |
| #6 | - | - | - | 0 | 0 |
| #8 | - | +1dil | - | 1st level | 1 |
| #7 | - | +1dil | - | 1st level | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



