1. Introduction
Pediatric obesity is a global problem in countries with varying income levels [
1,
2,
3]. The prevalence of pediatric obesity has more than doubled since 1990; 390 million children and adolescents aged 5–19 years are overweight or obese by 2022 [
1]. Obesity is defined by the World Health Organization (WHO) as a weight greater than three standard deviations above the WHO Growth Reference Median in children under 5 years or two standard deviations above the WHO Growth Reference Median in children and adolescents between 5 and 19 years of age [
1].
Obesity is a chronic disease with multifactorial etiology [
1,
3]. Structural barriers to a healthy lifestyle, such as inadequate access to nutritious foods, lack of safe locations for physical activity, and lack of consistent healthcare access, contribute to children’s control [
1,
3,
4]. Exposure to high-calorie snacks and drinks, sedentary behavior [
1,
3,
4], excessive use of screens [
5,
6], and poor support for self-regulating behaviors further exacerbate weight gain [
4]. Obesity is associated with many medical conditions such as type 2 diabetes mellitus, cardiovascular disease, decline in bone health, endocrine abnormalities, increased risk of cancer [
1,
2], and autoimmune conditions associated with chronic inflammation [
2,
3,
6]. It also has strong psychosocial consequences for children; stigma, bullying, and discrimination can adversely affect school performance, mental well-being, and quality of life [
1,
3,
4]. Obesity in childhood is associated with a 500% increased risk of obesity in adulthood [
4]; therefore, early and effective medical treatment for pediatric obesity is paramount for improving lifelong health.
Current medical treatment guidelines for pediatric obesity center on behavioral interventions [
3,
4]. Dietary education is the mainstay of treatment, focusing on measures such as increased intake of fruits and vegetables and reduction in high-calorie snacks and drinks [
2,
3,
4]. Other lifestyle interventions include encouragement of moderate physical activity and decreased sedentary behaviors [
3,
4]. Pharmacotherapies such as orlistat and, more recently, liraglutide and other GLP-1 agonists have been approved by the United States Food and Drug Administration (US FDA) for adolescents older than 12 years [
2,
7]. Gastric bypass surgery can also be an effective intervention for certain adolescents, although the risk of remission of diabetes or mental health disorders after surgery is higher in this age group than in adults [
2,
3].
Complementary and alternative medical treatments are often of interest as a holistic approach to address obesity and its comorbidities [
6]. A variety of herbal supplements, such as
Camellia sinensis,
Hoodia gordonii,
Cynanchum auriculatum, hydroxycitric acid, chitosan, and chromium, have been proposed to aid weight loss by augmenting energy metabolism, binding fat in the intestines for faster excretion, and other unknown mechanisms [
6,
8]. Other available treatments include acupuncture and noninvasive body contouring (cryolipolysis and laser therapy) [
6,
8]. However, the body of literature evaluating the safety and efficacy of these treatments offers conflicting results [
6,
8], and most studies have been conducted in adults [
6,
8].
In this narrative review, we aimed to synthesize the available body of evidence regarding the use of complementary and alternative treatments as therapies for adolescent obesity, assess the efficacy of available adjunctive therapies in pediatric populations, and highlight areas that would be beneficial for further exploration.
2. Materials and Methods
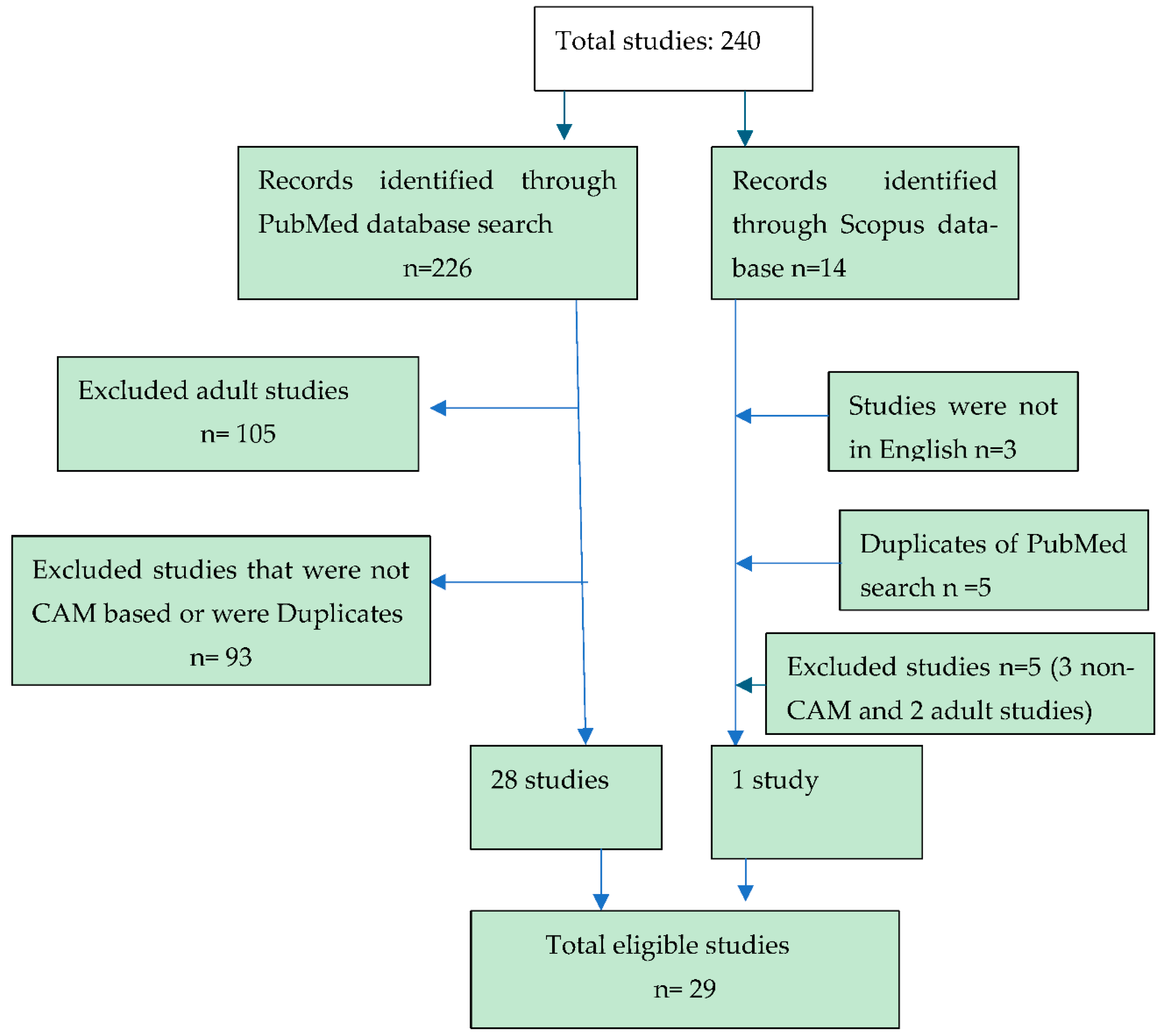
We performed a literature review on the use of complementary and alternative treatments (CAM) in adolescent obesity by searching the PubMed and Scopus databases for related English-language articles published on April 5, 2024.
We searched PubMed using the search terms ("Complementary Therapies"[Mesh] OR “complementary therap*”[tiab] OR “complementary medicine”[tiab] OR “alternative therap*”[tiab] OR “alternative medicine”[tiab]) AND ("Obesity"[Mesh] OR "Obesity/diet therapy"[Mesh] OR "Obesity/drug therapy"[Mesh] OR "Obesity/therapy"[Mesh] OR obesity[tiab]) AND ("Adolescent"[Mesh] OR adolescent[tiab] OR teen[tiab]) resulting in 226 records. . In Scopus, a title/abstract search for ("alternative medicine" OR "alternative therap*" OR "complementary medicine" OR "complementary therap*") AND obesity AND (adolescent OR teen) returned 14 results.
All observational studies, RCTs, systematic reviews, and meta-analyses were considered. The age range for inclusion was adolescents between 12 and 17 years; however, other studies that included these ages were also included. Although the effects were primarily examined for improvement in obesity parameters, such as BMI, weight, body fat, and metabolic aspects of obesity, such as improvement in lipid profile and glucose, were also included.
Studies were excluded if they were outside the adolescent age range (≥ 18 years), non-CAM studies, or non-English language studies. Of the 226 PubMed records, 105 articles were excluded because of age (≥ 18 years). Further examination of each study revealed that 93 studies were not CAM studies, leaving 28 that met our inclusion criteria. Of the 14 Scopus records, five studies were excluded because three studies were non-CAM studies and two were adult studies. Three non-English language studies and five duplicate records were excluded, leaving one that met our inclusion criteria. In total, 29 studies were included in the review.
Figure 1.
Study Flow Diagram.
Figure 1.
Study Flow Diagram.
3. Results
The initial search for CAM treatments for adolescent obesity yielded 240 results, and 29 studies matched our inclusion criteria (
Figure 2).
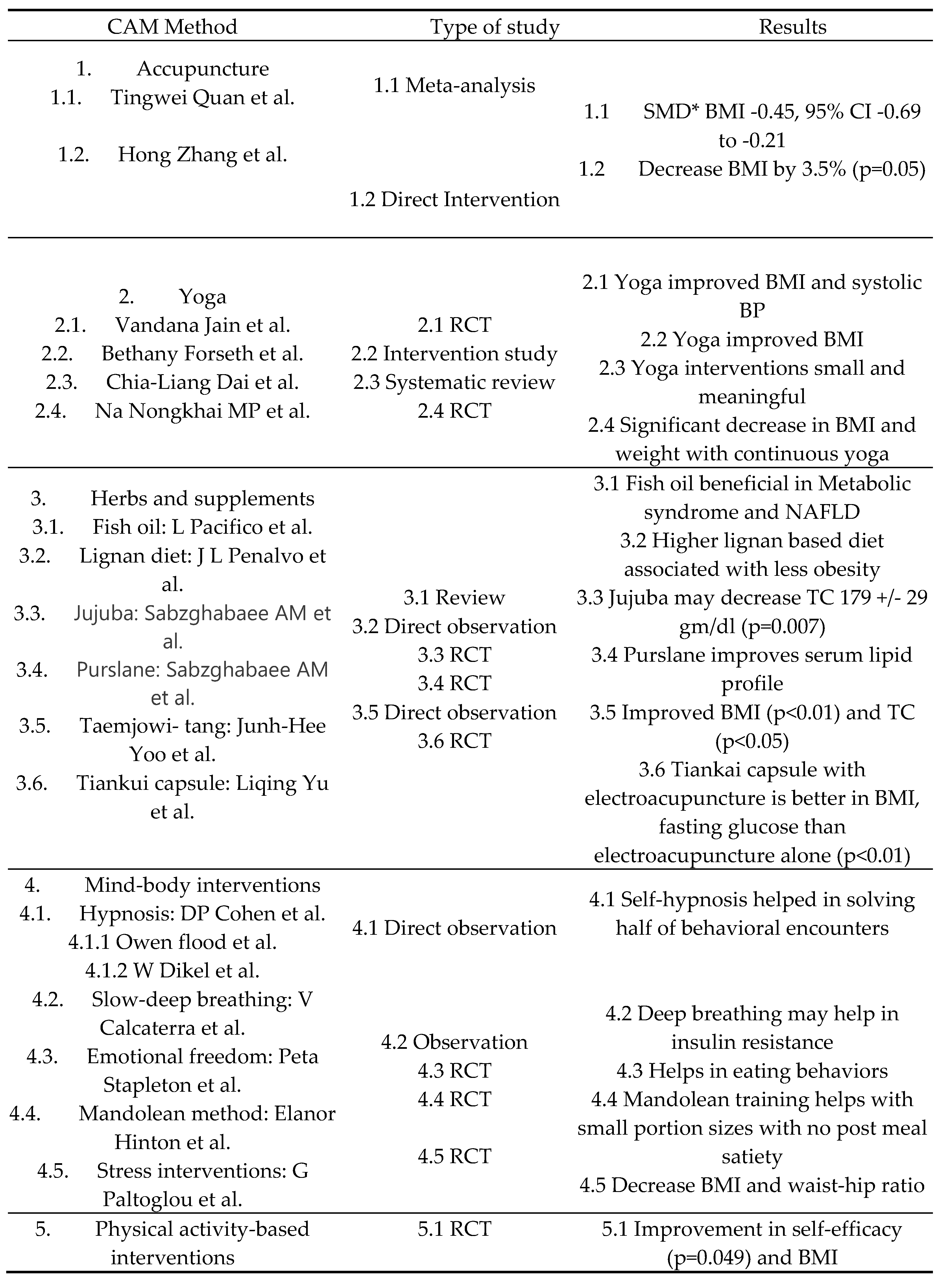
3.1. Acupuncture
The National Center of Complementary and Integrative Health defines acupuncture as a technique in which practitioners insert fine needles into the skin to treat health problems. The needles may be manipulated manually or stimulated with small electrical currents (electroacupuncture) [
9]. Two studies used acupuncture with different modalities to treat adolescent obesity. Quan et al [
10] examined 1288 overweight/obese children and teenagers between 7 and 16 years using a Randomized Control Trial (RCT) in China and Korea and found improved metabolic indicators with the use of acupuncture in BMI, body weight, and serum leptin. Hong Zhang et al. [
11] evaluated acupuncture therapy in 10 healthy obese children and adolescents between ages 10 and 13 years daily for a month and observed statistically significant improvements in Body Mass Index (BMI) and abdominal visceral abdominal tissue using magnetic resonance imaging (MRI) scans.
3.2. Yoga
Yoga is an ancient Indian science that emphasizes the attainment of complete health and well-being through various physical postures (
asanas), breathing techniques (
pranayama) and meditation [
12]. Jain et al. [
13] conducted a RCT in 165 obese children (ages 8-15 years) and concluded that yoga with dietary modification was effective in reducing BMI and systolic blood pressure (BP) compared to the control group and was as effective as standard weight management for BMI reduction. Forseth et al [
14] conducted a pilot study with 30 adolescents aged 8-18 years with obesity and incorporated PHIT (promoting health in teens) yoga into a 12-week pediatric weight management intervention. Fifty-four percent of the children in the PHIT yoga cohort and 65% of the children in the PHIT Kids cohort attended 75% or more of the intervention sessions. The survey results support the view that PHIT yoga is acceptable to both caregivers and children. Improvements in BMI were observed in 50% of the children in each cohort, and five of the seven health habits improved in both groups. In a systematic review by Chia-Liang Dai et al. [
15], nine studies were evaluated, and the authors found a small but meaningful impact. The limitations were the small number of studies and lack of follow-up. This review highlights the need for further research. Kongkhai Mp et al. conducted an RCT on 40 obese adolescents and studied the effect of continuous yoga (asanas, prayanama, and surya namaskar) and found a significant decrease in BMI and body fat mass in the yoga intervention group at weeks 8 and 12 and an increase in muscle mass [
16].
3.3. Herbs, Supplements, and Diet
There is an extensive history of people trying various herbs and supplements to treat various ailments. However, we did not find many studies on the use of herbs and supplements in adolescents compared to that in adults.
3.3.1. Fish Oil
The incidence of metabolic syndrome, including central obesity, is increasing. Non-alcoholic fatty liver disease (NAFLD) is a direct consequence of metabolic syndrome. Pacifico et al. [
17] reviewed observational and intervention studies to examine the beneficial effects of fish oil in the treatment of NAFLD and decrease in lipids in metabolic syndrome.
3.3.2. Lignan Diet
A lignan diet based on olive oil, wheat-based bread, and refined wheat is associated with improved health outcomes. Penalvo et al. [
18] determined that boys (aged 2–20 years) with the highest lignan-rich products were less likely to have obesity in Spanish children and adolescents.
3.3.3. Zizyphus Jujuba Fruit
Jujuba fruit has long been used in Chinese medicine for sleep disturbances, anxiety, appetite suppression, and digestion [
19]. Sabzghabaee et al [
20] conducted a triple blind RCT trial in 80 obese adolescents (ages 12-18 years) eating 5 g jujuba fruit three times a day for one month and found significant decreases in total cholesterol (19 +/- 37 mg/dl in controls vs. 170 +/- 29 mg/dl in cases, P = 0.007)and LDL.(114 +/- 38 mg/dl vs. 104 +/- 22 mg/dl, respectively, P = 0.004).
3.3.4. Purslane (Portulaca Oleracea)
Purslane has traditionally been used as an antioxidant and antiatherogenic agent. Sabzghabaee et al [
21] found a statistically significant improvement in total cholesterol (197.19 to 187.05 mg/dl), LDL-C(112.87 to 101.73 mg/dl) and triglycerides( 145.86 to 129.59 mg/dl) with p<= 0.001 in a RCT trial giving capsule containing 500 mg of Purslane seeds twice a day for one month in obese adolescents aged 12-18 years.
3.3.5. Taeumjowi-Tang
Yo et al. [
22] studied the use of Taeumjowi-tang, a traditional Korean herbal formula (KH), in 22 subjects (8 girls and 14 boys; average age, 11/- 2.62 years) for 30 days, and found a statistically significant improvement in BMI and a reduction in serum lipids. The short-term effects of KH on obese children were the reduction of their BMI from 24.34 +/- 3.10 to 23.26 +/- 3.00 kg/m2 of %RBW from 34.41 +/- 10.90 to 25.94 +/- 11.18% (p < 0.01) and their total cholesterol decreased from 195.38 +/- 31.39 to 183.25 +/- 33.27 mg/dl (p < 0.05). It was not associated with side effects or safety concerns.
3.3.6. Tiankui Capsule
Yu et al. [
23] compared Tiankui capsules, a traditional Chinese kidney-nourishing medicine with electroacupuncture, versus electroacupuncture only in 67 obese adolescents and adults (ages 17-39 years). BMI, body weight, waist-to-hip ratio, fasting plasma glucose, fasting insulin were lower, and adiponectin levels were higher in the medicine-acupuncture group than in the acupuncture group alone (p<0.01).
In a review of adult CAM therapies used for obesity by Batsis et al. [
8], many herbs, such as ephedra/caffeine, green tea (Camellia), chitosan, garcinia, and chocolate/cocoa, have been studied; however, no similar children/adolescent studies were found in our PubMed search.
3.4. Mind-Body Interventions
Different mind-body interventions have been attempted to improve adolescent obesity through self-hypnosis, stress management programs, and/or slow deep breathing.
3.4.1. Self-Hypnosis
Cohen et al. [
24] studied the use of self-hypnosis (relaxation mental imagery) in 505 children and adolescents aged 3–20 years for behavioral encounters, including obesity or bed wetting, and found a resolution of 51% of presenting problems and 32% saw significant improvement of their symptoms. Other articles involving self-hypnosis in adolescent obesity include A Owen-flood [
25] and W Dikel et al. [
26].
3.4.2. Slow-Deep Breathing
Calcaterra et al. [
27] showed that slow-deep breathing in 301 obese children and adolescents aged 9 to 13 years improved blunted baroreflex sensitivity in children with insulin resistance and diabetes and may help with their insulin levels.
3.4.3. Emotional Freedom Techniques
The rates of adolescent obesity have increased along with eating disorders. Emotional Freedom Techniques (EFT) are techniques that stimulate acupressure points by pressuring, tapping, or rubbing while focusing on situations that represent personal fear or trauma [
28]. Stapleton et al. [
29] compared 44 students (aged 12 to 18 years) with emotional freedom techniques versus controls for 6 weeks. Improved eating habits and self-esteem may ultimately help in weight-associated psychopathology.
3.4.4. Mandolean Method
The Mandolean principle is based on how people eat rather than how much by focusing on slow eating and small portion sizes. Hilton et al [
30] randomized 24 obese (BMI>95 the centile) adolescents (aged 11-18 years) into standard care for 6 months in an obesity clinic versus standard care with short term Mandolean training. Functional MRI data showed that the Mandolean training group had less activation of brain regions associated with food cue reactivity after a glucose meal and 22 % less portion size, with no change in food satiety.
3.4.5. Stress Management
Paltoglou et al. [
31] studied six RCTs on mindfulness and stress management in children and adolescents with obesity. There were 112 subjects in the intervention group and 137 subjects in the control group aged 8-17.9 years and interventions for mindfulness-based stress reduction therapy for 8 weeks (3 studies), mindfulness-based group program for adolescents (1 study), and mindful eating program for 6 and 10 weeks (1 study each). They found reduced adiposity markers such as BMI and waist-to-hip ratio in four out of six studies and supported that mindfulness-based interventions can play a role in decreasing BMI.
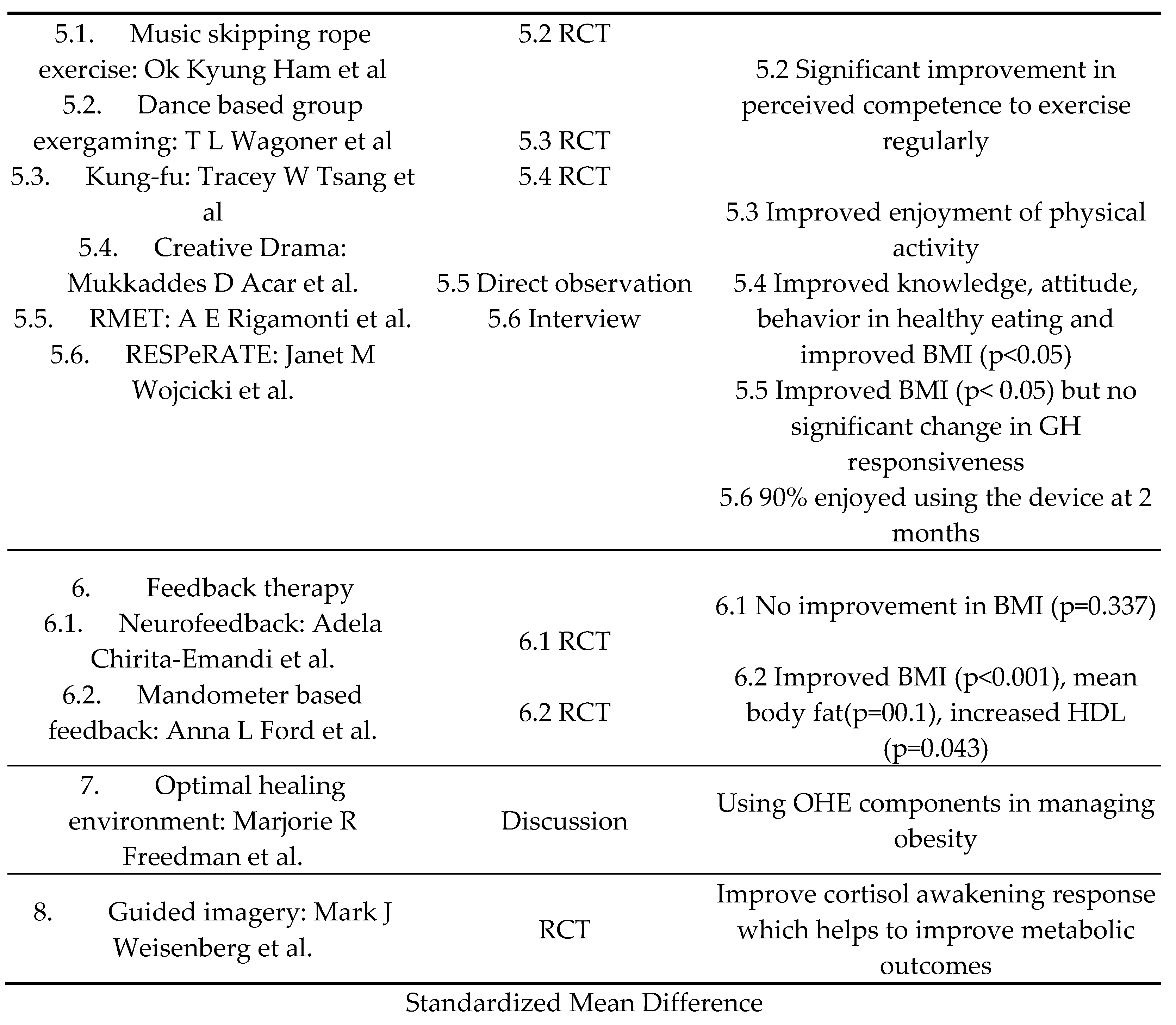
3.5. Physical Activity-Based Interventions
Different studies on adolescent obesity have used different methods of physical activity-based interventions to decrease weight, as highlighted below.
3.5.1. Music Skip Rope
Ham et al. [
32] conducted a RCT on 75 obese children and adolescents aged 8 to 13 years in Korea with exercise counseling and music skip rope exercise and found a statistically significant improvement in self-efficacy(p=0.49) and maintenance of BMI at 6 months (p>0.05). The control group showed an increase in BMI (p<0.05).
3.5.2. Dance Based Group Exergaming
Wagoner et al. [
33] performed a RCT on group dance-based exergaming for 10 weeks on 40 obese adolescents aged 12 to 18 years and showed a significant increase in self-reported competence to exercise regularly and significant improvement in relations with parents.
3.5.3. Kung-fu
Kung-fu is a Chinese martial art that requires training, discipline, and practice. Tsang et al [
34] performed a RCT with Kung-fu training versus placebo-exercise group in 20 overweight/obese adolescents 12 to 18 years for 6 month and showed an improved enjoyment of physical activity more than the placebo group.
3.5.4. Creative Drama
Acar et al [
35] conducted a RCT on 76 overweight/obese aged 12.5+/- 1 years old adolescents in Turkey evaluating 5 sessions of creative drama. There was a statistically significant improvement in knowledge, attitude, order of meals, and healthy diet exercise behavior (p< 0.05). Statistically significant improvements were observed in the BMI, body weight, and waist/hip ratio (p< 0.05).
3.5.5. Respiratory Muscle Endurance Training (RMET)
Obesity can cause hyposomatropism owing to blunted growth hormone (GH) responses. Adult studies have shown improvement with the use of the RMET using a commercially available device, SpiroTiger. Rigamonti et al [
36] evaluated incremental RMET to body weight reduction program in obese adolescents aged 12-17 years. Improvement in body weight (115.3±9.2 kg to 111.5±8.7 kg, p<0.05) was shown; but not in obesity-related hyposomatropism.
3.5.6. RESPeRATE Device
The RESPeRATE device helps in decreasing blood pressure through controlled breathing and has been shown to be an effective tool for high blood pressure in adults [
37]. Wojcicki et al [
38] studied the feasibility in obese children and adolescents 6 to 14 years and found that 90% still enjoyed using the device in 2 months and 80% stated they would recommend to a friend or relative.
3.6. Feedback Therapy
Feedback therapy using a feedback device that gives immediate visual or auditory feedback which helps control eating behaviors in obese patients
3.6.1. Neurofeedback
Neurofeedback is a type of biofeedback that teaches self-control by measuring brain waves and providing feedback signals in audio or video form [
39]. Chirita-Emandi et al. [
40] studied 34 obese subjects aged 6-18 years received 20 neurofeedback sessions, along with standard lifestyle measures. A statistically significant reduction in BMI was observed at 6 months (p=0.035).
3.6.2. Mandometer based feedback
A study by Ford et al. [
41] evaluated the Mandometer, a computerized device that provides real-time feedback to slow down eating and reduce the total food intake. A 12- month evaluation with reassessment at 18 months after intervention in 106 obese children and adolescents aged 9 to 17 years revealed statistically significant improvements in BMI, HDL, meal size, and mean fat at 18 months (p=0.001), suggesting a role of retraining feeding behavior using feedback devices as an adjunct to providing lifestyle changes.
3.7. Optimal Healing Environment (OHE)
The Samueli Institute coined the term
Optimal Healing Environment (OHE) in 2004 to describe a healthcare system designed to stimulate and support the inherent healing capacity of patients, families, and their care providers [
42]. Freedman et al [
43] focuses on the role and components of OHE that help in managing pediatric obesity: healing intention, healing relationships, health promotion and disease prevention, and healing spaces.
3.8. Guided Imagery (GI)
Changes in diurnal cortical salivary patterns are associated with poor metabolic outcomes. Weigensberg et al [
44] studied stress reduction GI and lifestyle behavior GI in 232 Latino adolescents aged 14-17 years and found small statistically significant increase in cortical awakening response and reduction in perceived stress scale suggesting it may help to improve stress response and improve metabolic outcomes.
4. Discussion
The total number of studies in adolescents is far fewer than that in adult studies of its kind [
8]. In most studies, the adolescent population ranged from 13 to 17 years old compared to adults ranging from 18 to 65 years. There could also be hesitancy with researchers to conduct children or adolescent-based studies with newer and untested treatments compared to adults, in addition to difficulty in obtaining approval from the Institutional Review Board (IRB). This is also highlighted by the fact that most adult studies have many different herbs and supplement-based studies, whereas adolescent-based studies are mostly physical activity-based. Green tea, ephedra or caffeine, chitosan, and cocoa-based adult studies are abundant in the literature [
8], while adolescent-based studies are more limited to physical activity-based interventions such as dance, trial, and yoga, although acupuncture-based studies are the most common study group for all ages [
8].
Many CAM studies in adolescents are region-based. Many acupuncture-based studies have been conducted in China or nearby Asian countries, such as Korea [
9,
10,
11]. Acupuncture therapy originated in China and had a deep inherent knowledge to try new interventions based on it. One trial even studied electroacupuncture therapy, a variation of acupuncture with the herb Tiankui capsule on adolescent obesity [
23]. Although yoga has origins in India, it has quickly attained adoption in many countries, including the USA. Although there have been some studies by Indian researchers [12-13}, other countries have also conducted yoga-based studies [
14,
15,
16]. Tests of other studies were conducted in different countries, including Europe and the USA. The lignan-based diet study was based in Spain [
18], Taumjowi-tang is an herbal tea based in Korea, and the Tiankui capsule and Zizyphus jujuba fruit are based in China, purslane seeds (Portulaca oleracea) study is based in Iran. An emotional freedom technique was studied in Australia, and a separate device study was conducted in the USA. It can be generalized that countries like China and Korea that adopt acupuncture freely do similar studies of familiarity, and similar inferences could be applied to some herb-based studies. Yoga-based studies are outliers and may be due to the widespread adoption of yoga in many countries. However, the number of studies was too small to make any significant associations.
Therefore, it is important to discuss the power and quality of these studies. Although there are many RCT based studies in the discussion and results that have statistically significant results, many of these RCTs and other individual studies have a small number of participants. This could be because some studies were pilot studies or because of the difficulty of enrolling adolescents in new untested therapies. Some of the studies based in China and Russia were in their native language or no English translation was available or even an abstract; they were either excluded, or a brief mention was made in the group. Although there have been few studies on herbs and supplements such as Taemjowi-tang and Tiankui capsules in adolescents, studies based on green tea, ephedra, caffeine, and cocoa that have shown promising results in adults have not been studied in adolescents.
5. Conclusions
Many studies, however, have small RCT based on observations or review studies and have statistically significant results, showing that acupuncture, yoga, and physical therapy-based interventions could play an important role in adolescent obesity. With the acknowledgement of obesity as a chronic disease and recent US FDA approval of many anti-obesity medications, there could be an important role for newer larger studies of herbs, supplements, and other CAM methods in adolescent obesity in the future.
Author Contributions
Conceptualization, Mahesh Shrestha, and Dilip Patel.; Methodology, Ann Harris, Mahesh Shrestha.; Writing—original draft preparation, Mahesh Shrestha and Urvi Savant: Writing—review and editing, Mahesh Shrestha, Ann Harris, Teresa Bailey, Dilip Patel.;. Supervision: Mahesh Shrestha, and Dilip Patel. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data will be available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Obesity and Overweight. World Health Organization. 1 March 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on October 26,2024).
- Marcus, C.; Danielsson, P.; Hagman, E. Pediatric Obesity-Long-Term Consequences and Effect of Weight Loss. J. Intern. Med. 2022, 292, 870-891. [CrossRef]
- Jebeile, H.; Kelly, A.S.; O'Malley, G.; Baur, L.A. Obesity in Children and Adolescents: Epidemiology, Causes, Assessment, and Management. Lancet Diabetes Endocrinol. 2022, 10, 351-365. [CrossRef]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351-378. [CrossRef]
- Robinson, T.N.; Banda, J.A.; Hale, L; Lu, A.S.; Fleming-Milici, F.; Calvert, S.L.; Wartella, E. Screen Media Exposure and Obesity in Children and Adolescents. Pediatrics. 2017, 140(Suppl 2), S97-S101. [CrossRef]
- Esteghamati, A; Mazaheri, T.; Vahidi Rad, M.; Noshad, S. Complementary and Alternative Medicine for the Treatment of Obesity: A Critical Review. Int. J. Endocrinol. Metab. 2015, 13, e19678. [CrossRef]
- FDA Approves Weight Management Drug. Center for Drug Evaluation and Research. U.S. Food and Drug Administration. 20 December 2020. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-weight-management-drug-patients-aged-12-and-older (accessed on October 26,2024).
- Batsis, J.A.; Apolzan, J.W.; Bagley, P.J.; Blunt, H.B.; Divan, V.; Gill, S.; Golden, A.; Gundumraj, S.; Heymsfield, S.B.; Kahan, S.; et al. A Systematic Review of Dietary Supplements and Alternative Therapies for Weight Loss. Obesity (Silver Spring). 2021, 29, 1102-1113. [CrossRef]
- Accupuncture: What You Need to Know. National Center for Complementary and Integrative Health. Available online: https://www.nccih.nih.gov/health/acupuncture-effectiveness-and-safety#:~:text=Acupuncture%20is%20a%20technique%20in,for%20at%20least%202%2C500%20years (accessed on 4 August 2024).
- Quan, T.; Su, Q.; Luo, Y.; Su, X.; Chen, Q.; Yang, J.; Tang, H. Does Acupuncture Improve the Metabolic Outcomes of Obese/Overweight Children and Adolescents?: A Systematic Review and Meta-Analysis. Medicine (Baltimore). 2023, 102, e34943. [CrossRef]
- Zhang, H.; Peng, Y.; Liu, Z.; Li, S.; Lv, Z.; Tian, L.; Zhu, J.; Zhao, X.; Chen, M. Effects of Acupuncture Therapy on Abdominal Fat and Hepatic Fat Content in Obese Children: A Magnetic Resonance Imaging and Proton Magnetic Resonance Spectroscopy Study. J. Altern. Complement. Med. 2011, 17, 413-420. [CrossRef]
- Nayak, N.N.; Shankar, K. Yoga: A Therapeutic Approach. Phys. Med. Rehabil. Clin. N. Am. 2004, 15, 783-vi. [CrossRef]
- Jain V, Kumar B, Sharma A, et al. A comprehensive yoga programme for weight reduction in children & adolescents with obesity: A randomized controlled trial. Indian J Med Res. 2022;155(3&4):387-396. [CrossRef]
- Forseth B, Hampl S, Dreyer Gillette M, et al. Incorporating Yoga into a Pediatric Weight Management Program: A Pilot Study. Child Obes. 2022;18(1):67-71. [CrossRef]
- Dai, C.L.; Sharma, M.; Chen, C.C.; Yesilyurt, E.; Godbey, S. Yoga as an Alternative Therapy for Weight Management in Child and Adolescent Obesity: A Systematic Review and Implications for Research. Altern. Ther. Health Med. 2021, 27, 48-55.
- Na Nongkhai MP; Yamprasert R; Punsawad C. Effects of Continuous Yoga on Body Composition in Obese Adolescents. Evid Based Complement Alternat Med. 2021, 2021, 6702767. [CrossRef]
- Pacifico, L.; Giansanti, S.; Gallozzi, A.; Chiesa, C. Long Chain Omega-3 Polyunsaturated Fatty Acids in Pediatric Metabolic Syndrome. Mini Rev. Med. Chem. 2014, 14, 791-804.
- Peñalvo, J.L.; Moreno-Franco, B.; Ribas-Barba, L., Serra-Majem, L. Determinants of Dietary Lignan Intake in a Representative Sample of Young Spaniards: Association with Lower Obesity Prevalence Among Boys But Not Girls. Eur. J. Clin. Nutr. 2012, 66, 795-798. [CrossRef]
- What We Know (And Don’t Yet Know) About Jujube Fruit Benefits. 26 May 2023. Cleveland Clinic. Available online: https://health.clevelandclinic.org/jujube-benefits (accessed on 6 August 2024).
- Sabzghabaee, A.M.; Khayam, I.; Kelishadi, R.; Ghannadi, A.; Soltani, R.; Badri, S.; Shirani, S. Effect of Zizyphus Jujuba Fruits on Dyslipidemia in Obese Adolescents: A Triple-Masked Randomized Controlled Clinical Trial. Med. Arch. 2013, 67, 156-159.
- Sabzghabaee, A.M.; Kelishadi, R.; Jelokhanian, H.; Asgary, S.; Ghannadi, A.; Badri S. Clinical Effects of Portulaca Oleracea Seeds on Dyslipidemia in Obese Adolescents: A Triple-blinded Randomized Controlled Trial. Med. Arch. 2014, 68, 195-199. [CrossRef]
- Yoo, J-H.; Lee, E-J.; Kwak, C-K.; Shon, E-H.; Koh, B-H.; Song, I-B.; Lee, K-S. Clinical Trial of Herbal Formula on Weight Loss in Obese Korean Children. Am. J. Chin. Med. 2005, 33, 713-722.
- Yu, L.; Liao, Y.; Wu, H.; Zhao, J.; Wu, L.; Shi, Y.; Fang, J. Effects of Electroacupuncture and Chinese Kidney-Nourishing Medicine on Polycystic Ovary Syndrome in Obese Patients. J. Tradit. Chin. Med. 2013, 33, 287-293. [CrossRef]
- Kohen, D.P.; Olness, K.N.; Colwell, S.O.; Heimel, A. The Use of Relaxation-Mental Imagery (Self-Hypnosis) in the Management of 505 Pediatric Behavioral Encounters. J. Dev. Behav. Pediatr. 1984, 5, 21-25.
- OWEN-FLOOD A. Slimming under hypnosis; the obese adolescent. Med World. 1960;93:310-312.
- Dikel, W.; Olness, K. Self-Hypnosis, Biofeedback, and Voluntary Peripheral Temperature Control in Children. Pediatrics. 1980, 66, 335-340.
- Calcaterra, V.; Vandoni, M.; Debarbieri, G.; Larizza, D.; Albertini, R.; Arpesella, M.; Bernardi, L. Deep Breathing Improves Blunted Baroreflex Sensitivity in Obese Children and Adolescents with Insulin Resistance. Int. J. Cardiol. 2013, 168, 1614-1615. [CrossRef]
- Wikipedia Contributors. Emotional Freedom Techniques. Wikipedia, The Free Encyclopedia. Available online: https://en.wikipedia.org/w/index.php?title=Emotional_Freedom_Techniques&oldid=1244239671 (accessed on 6 September 2024).
- Stapleton, P.; Chatwin, H.; William, M.; Hutton, A.; Pain, A.; Porter, B.; Sheldon, T. Emotional Freedom Techniques in the Treatment of Unhealthy Eating Behaviors and Related Psychological Constructs in Adolescents: A Randomized Controlled Pilot Trial. Explore (NY). 2016, 12, 113-122. [CrossRef]
- Hinton, E.C.; Birch, L.A.; Barton, J.; Holly, J.M.P.; Biernacka, K.M.; Leary, S.D.; Wilson, A.; Byrom, O.S.; Hamilton-Shield, J.P. Using Neuroimaging to Investigate the Impact of Mandolean® Training in Young People with Obesity: A Pilot Randomised Controlled Trial. BMC Pediatr. 2018, 18, 366. [CrossRef]
- Paltoglou, G.; Chrousos, G.P.; Bacopoulou, F. Stress Management as an Effective Complementary Therapeutic Strategy for Weight Loss in Children and Adolescents with Obesity: A Systematic Review of Randomized Controlled Trials. Children (Basel). 2021, 8, 670. [CrossRef]
- Ham, O.K.; Sung, K.M.; Lee, B.G.; Choi, H.W.; Im, E.O. Transtheoretical Model Based Exercise Counseling Combined with Music Skipping Rope Exercise on Childhood Obesity. Asian Nurs. Res. (Korean Soc. Nurs. Sci). 2016, 10, 116-122. [CrossRef]
- Wagener, T.L.; Fedele, D.A.; Mignogna, M.R.; Hester, C.; Gillaspy, S.R. Psychological Effects of Dance-Based Group Exergaming in Obese Adolescents. Pediatr. Obes. 2012, 7, e68-e74. [CrossRef]
- Tsang, T.W.; Kohn, M.R.; Chow, C.M.; Singh, M.F. Self-Perception and Attitude Toward Physical Activity in Overweight/Obese Adolescents: The "Martial Fitness" Study. Res. Sports. Med. 2013, 21, 37-51. [CrossRef]
- Demir Acar, M.; Bayat, M. The Effect of Diet-Exercise Trainings Provided to Overweight and Obese Teenagers through Creative Drama on Their Knowledge, Attitude, and Behaviors. Child Obes. 2019, 15, 93-104. [CrossRef]
- Rigamonti, A.E.; Agosti, F.; Patrizi, A.; Tringali ,G.; Fessehatsion R.; Cella, S.G.; Sartorio, A. GH Responsiveness Before and After a 3-Week Multidisciplinary Body Weight Reduction Program Associated with an Incremental Respiratory Muscle Endurance Training in Obese Adolescents. Horm. Metab Res. 2014, 46, 59-64. [CrossRef]
- Schein, M.H.; Gavish, B.; Baevsky, T.; Kaufman, M.; Levine, S.; Nessing, A.; Alter, A. Treating Hypertension in Type II Diabetic Patients with Device-Guided Breathing: A Randomized Controlled Trial. J. Hum. Hypertens. 2009, 23, 325-331. [CrossRef]
- Wojcicki, J.M.; Geissler, J.D.; Stokes, C.W.; Heyman, M.B.; Tran, C.T. The Use of the RESPeRATE Device to Lower Blood Pressure in Inner City Obese Adolescents and Children: A Pilot Feasibility Study. High Blood Press. Cardiovasc. Prev. 2013, 20, 89-92. [CrossRef]
- Marzbani, H.; Marateb, H.R.; Mansourian, M. Neurofeedback: A Comprehensive Review on System Design, Methodology and Clinical Applications. Basic Clin. Neurosci. 2016, 7, 143-58. [CrossRef]
- Chirita-Emandi, A.; Puiu, M. Outcomes of Neurofeedback Training in Childhood Obesity Management: A Pilot Study. J. Altern. Complement. Med. 2014, 20, 831-837. [CrossRef]
- Ford, A.L.; Bergh, C.; Södersten, P.; Sabin, M.A.; Hollinghurst, S.; Hunt, L.P.; Shield, J.P.H. Treatment of Childhood Obesity by Retraining Eating Behaviour: Randomised Controlled Trial. BMJ. 2009, 340, b5388. [CrossRef]
- Sakallaris, B.R.; MacAllister, L.; Voss, M.; Smith, K.; Jonas, W.B. Optimal Healing Environments. Glob. Adv. Health Med. 2015, 4, 40-45. [CrossRef]
- Freedman, M.R.; Stern, J.S. The Role of Optimal Healing Environments in the Management of Childhood Obesity. J. Altern. Complement. Med. 2004, 10 (Suppl 1), S231-S244.
- Weigensberg, M.J.; Wen, C.K.; Sanogo, F.; Toledo-Corral, C.; Ding, L. Imagine HEALTH: Changes In Diurnal Salivary Cortisol Patterns Following a 12-Week Guided Imagery RCT Lifestyle Intervention in Predominantly Latino Adolescents. Psychoneuroendocrinology. 2023, 151, 106053. [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).