
Submitted:
04 December 2024
Posted:
04 December 2024
You are already at the latest version
Abstract
Ectopic variceal bleeding is a rare, but regrettably life-threatening complication of hepatic cirrhosis. Throughout this paper, we present the case of a 52-year-old patient with decompensated alcoholic cirrhosis, who was admitted for melena. Upper and lower endoscopy failed to identify the source of bleeding. Ultimately, an evaluation with endoscopic capsule identified ileal varices. The patient was referred to surgery and the outcome was successful. In the discussion section, we approached the diagnostic and therapeutic arsenals in managing ectopic varices. In conclusion, although ectopic varices bleeding has a high fatal potential, prompt intervention in a multidisciplinary team could be the key for patient salvation.
Keywords:
cirrhosis
; ectopic varices
; variceal bleeding
; endoscopy
; case report
Introduction and Clinical Significance
Variceal hemorrhage is regarded as a critical decompensating event in cirrhotic patients which severely impacts the prognosis leading to a 5-year mortality rate of 80% when associated with other complications (ascites, hepatic encephalopathy) [1]. Management of esophagogastric variceal bleeding is clearly defined in the latest guidelines, but up to 5% of variceal hemorrhages occur from other sites, called ectopic varices [2]. Currently, there is no standardized approach to this potentially fatal event due to the heterogeneity of presentations and lack of randomized controlled trials. Immediate bleeding site identification is vital in order to proceed to hemostasis, either by endoscopic, radiologic or surgical techniques.
We present the case of a patient with challenging ectopic variceal hemorrhage where the multidisciplinary approach was of utmost importance in order to ensure the best possible care. Written consent was obtained from the patient in order to present this case.
Case Presentation
A 52-year-old female patient known with decompensated alcoholic cirrhosis (Child-Pugh C) and recurrent episodes of melena was transferred to our emergency department for another bleeding episode. She had previously been examined in another hospital unit through repeated upper and lower endoscopy procedures but without identification of any potential bleeding lesion.
The initial clinical examination revealed that the patient was in stable condition with a mild flapping tremor, but generally alert and oriented. Systolic blood pressure was 120 mmHg and tachycardia was noted (105 bpm, shock index 0.87). Lab tests showed moderate anemia with a hemoglobin level of 7.7 g/dL. We decided to repeat the endoscopic examinations and the EGD showed normal mucosa up to duodenum III. No varices had been detected even if other signs of portal hypertension (ascites, splenomegaly, thrombocytopenia) were present. During colonoscopy multiple blood clots were observed mainly in the ascending colon, cecum and terminal ileum. However, no potential bleeding site was detected. Therefore, we strongly thought that the site of bleeding was the small bowel and decided to investigate it. Unfortunately, after several hours from admission when the patient was apparently stable, hemodynamic instability (shock index >1), rapid clinical deterioration and altered mental status occurred. The patient was consequently admitted in the ICU department with a high APACHE II score of 30 points.
Due to the hemodynamically unstable status and signs of active bleeding, we decided to perform CT angiography. No active bleeding site was detected; nevertheless, several portocaval shunts in herniated ileal loops were noted (Figure 1). Afterwards, due to intensive care management and fluid resuscitation, the patient was stable enough to allow us to perform antegrade enteroscopy. Still, the bleeding spot was not detected.
We pursued to capsule endoscopy and the recordings showed multiple ileal protrusive enteral variceal cords with bleeding stigmata (Figure 2). Moreover, fresh blood was observed at the level of the cecum and proximal colon, highly suggestive of a recent bleeding episode which spontaneously ceased.
Transjugular intrahepatic portosystemic shunt (TIPS) was not available in our unit and its expertise mainly in the acute setting (salvage TIPS) is generally limited in the whole country.
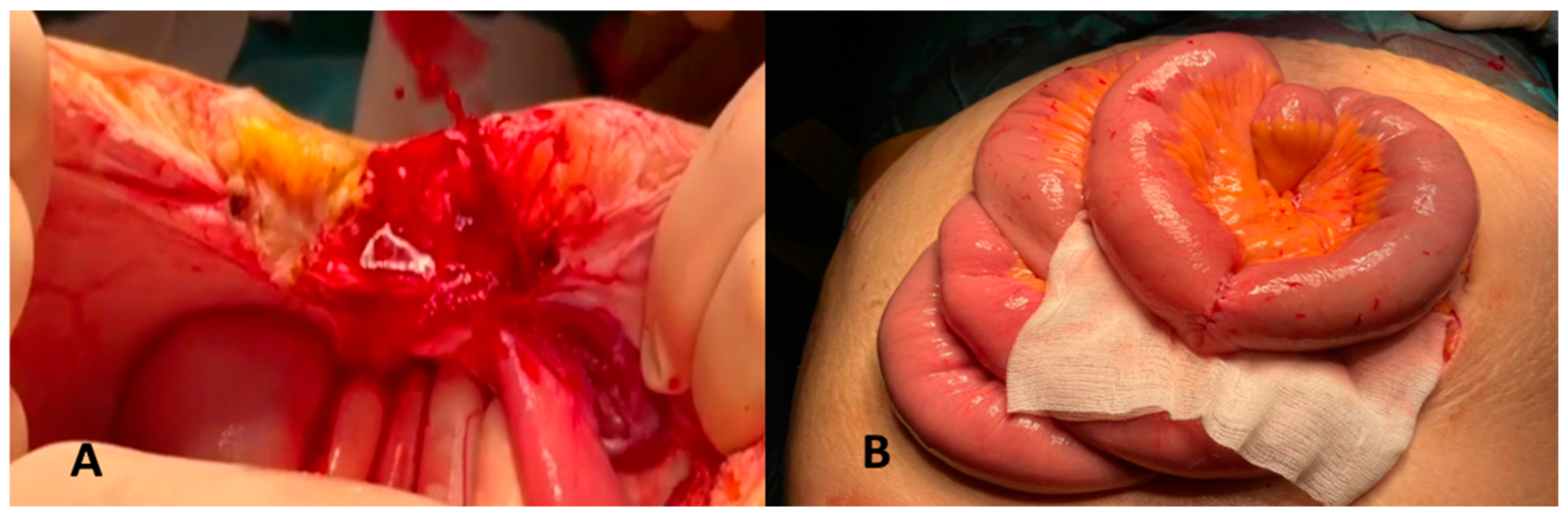
Due to the continuously deteriorating clinical status, surgery was considered the last resort and laparotomy identified an active bleeding variceal cord (Figure 3A). Segmental enterectomy and enterorrhaphy was performed with favorable outcome (Figure 3B). She was discharged 7 days after surgery, in good condition.
Discussions
Ectopic varices represent a rare and challenging complication, mainly caused by portal hypertension. They are dilated portosystemic collaterals located in unusual sites, different from the gastro-esophageal region, and account for up to 5% of all the variceal bleedings episodes [3]. In a study conducted on 169 patients admitted for bleeding from ectopic varices, those occurred from the small intestine accounted for 17% [4]. By comparison, in another study conducted on 46 patients, 8,7% of varices were located in the small bowel [5].
In spite of the advances in the fields of radiology and endoscopy with both diagnostic and therapeutic yields, it is still difficult to explore the ileo-jejunal varices and to estimate their true burden.
When it comes to exploration of overt gastrointestinal bleeding, it can be wise to consider second-look endoscopy and/or colonoscopy, since there are randomized controlled trials comparing outcome of capsule endoscopy and push enteroscopy which demonstrated that a significant proportion of patients (up to 36.7%) actually had a bleeding lesion in the stomach, duodenum and colon, regions that are visualized by standard endoscopy [6]. In our case report, both were negative, so we decided to investigate the small bowel, as current guidelines recommend.
Due to the unstable hemodynamic status, we proceeded to CT angiography. It is a fast and reliable examination with an overall 79% sensitivity and 95% specificity in the detection of active GI hemorrhage [7,8]. Intermittent GI hemorrhage is common and performing a CT angiographic examination when the bleeding is active is pivotal in localizing the incriminated lesion [9].
Capsule endoscopy can be the first line procedure as ACG guidelines recommend, with a 92% diagnostic rate in patients with active bleeding if hemodynamically stable [10]. Its main advantage is the capability of exploring the entire small bowel with minimal risks (1% risk of impactation), but there are also drawbacks such as lack of therapeutic potential and it may be limited by inadequate bowel preparation, limited field of view and poor visual clarity [11]. Another limitation of capsule endoscopy is the false-negative results which are up to 11% in hemorrhagic lesions [12].
Another diagnostic method which poses therapeutic hemostatic maneuvers with a relatively small rate of complication is enteroscopy, particularly the motorized spiral enteroscopy and balloon enteroscopy [13]. Motorized spiral enteroscopy can achieve complete intubation of the small bowel in about 35 minutes compared to balloon enteroscopy where the average time of complete intubation is 65 to 80 minutes. However, the rates of rebleeding seem to be significant and almost equal in the long term [14].
When it comes to managing bleeding from ectopic varices there are currently no established guidelines or randomized controlled trials. Therefore, it is recommended to adopt a multidisciplinary approach that includes expertise from gastroenterology, radiology and surgery fields. The management depends on several factors such as location of the hemorrhage, team expertise, available local equipment and the underlying cause [15].
There are various treatment options available for ectopic varices [16], including endoscopic band ligation (EBL) and endoscopic injection sclerotherapy (EIS) using different sclerosing agents [17]. While EBL has been found to be more effective than EIS in terms of lower rebleeding rates, mortality, complications and faster application, it has a higher rate of variceal recurrence compared to sclerotherapy. On the other hand, the latter may cause deep ulceration which can lead to rebleeding stricture formation or perforation [18,19]. To overcome these limitations a combination of EBL and EIS called endoscopic scleroligation (ESL) has been developed which has shown to be superior with decreased recurrence rates [20]. However, there is no established protocol for the use of these modalities in the management of ectopic varices and the choice often depends on the individual situation and expertise [15].
Balloon occluded retrograde transvenous obliteration (BRTO) is a retrograde shunt occlusion procedure used for controlling gastric variceal bleeding, as opposed to TIPS which actually creates a shunt [15]. BRTO at the site of an active bleeding will increase the portal hypertension which translates in a higher risk of variceal bleeding especially in the esophagus [21]. Consequently, combination of BRTO and TIPS can be done in order to prevent or to decrease the risk of hemorrhage from other variceal sites [22]. This combined method has a rate of success of 89% without significant side effects regarding hepatic function and without triggering encephalopathy [23]. Recent case reports of B-RTO have been successfully used in the treatment of varices in the small bowel are increasing [24,25]. However, the rebleeding rates are between 5-16% in hemorrhagic complications due to ectopic varices [26].
Multiple studies have highlighted the effectiveness of TIPS in managing bleeding ectopic varices in cirrhotic patients caused by intrahepatic portal hypertension. In terms of preventing recurrent esophageal bleeding TIPS is superior than other endoscopic therapy. A pressure gradient reduction of more than 50% is considered highly protective from rebleeding events and even a reduction of 25-50% can be effective [27]. Following TIPS, the cumulative rate of rebleeding was 23% at 1 year and 31% at 2 years [28].
Percutaneous embolization using a transhepatic approach has been successfully performed in tertiary centers but it carries a very high rebleeding rate (up to 65%) [29]. Percutaneous embolization has been reported for management of ectopic variceal bleedings but given the high rebleeding rates it is advised to be used in combination with other techniques like TIPS [30,31].
In terms of surgery, its role has been diminished in favor of modern management techniques and is nowadays considered a salvage option for patients when endoscopic and radiological procedures failed. Certainly, patients who have ectopic variceal bleedings are in a state of decompensated liver status and this represents a marker of high operative morbidity and mortality. Nevertheless, there are authors who reported successful partial ileal resection of the affected bowel in patients with bleeding varices with no further hemorrhagic events at a minimum of 1 year follow-up [32,33,34,35]. Furthermore, other studies had good results and advocate for a more direct approach with surgical management even in CHILD-PUGH B or C patients [36,37,38,39,40].
One of the downsides is that resection does not address the causative factor which is portal hypertension; therefore, a combined technique of enterectomy of the affected bowel and TIPS during the same hospitalization seems superior regarding long term rebleeding rates. Another argument for this integrated approach would be the fact that 25% of patients with cirrhosis and small intestinal varices had an episode of hemorrhage with frequent need for non-surgical second interventions and a high mortality rate [41].
Current literature does not offer a direction or a plan in managing ectopic variceal bleedings and the medical decisions should be made based on expert opinion for every case with interdisciplinary approach where input is made not only by surgeons, gastroenterologists, radiologist, intensivists, but also by the primary care physician who should closely monitor the patient and establish a personalized medical guidance plan.
Conclusions
Diagnosing and treating ectopic small bowel varices as a complication derived due to portal hypertension is a demanding task especially in acute settings and the currently presented case report is highlighting the importance of multidisciplinary approach. Randomized controlled trials and guidelines are expected to clarify and optimize the proper management.
Conflicts of interest
The authors declare no conflict of interest.
References
- D’Amico G, Pasta L, Morabito A, et al. Competing risks and prognostic stages of cirrhosis: a 25-year inception cohort study of 494 patients. Aliment Pharmacol Ther 2014;39:1180-1193. [CrossRef]
- Park SW, Cho E, Jun CH, et al. Upper gastrointestinal ectopic variceal bleeding treated with various endoscopic modalities: case reports and literature review. Medicine (Baltimore) 2017;96(1):e5860.
- Kinkhabwala M, Mousavi A, Iyer S, Adamsons R. Bleeding ileal varicosity demonstrated by transhepatic portography. AJR Am J Roentgenol. 1977;129:514–6. [CrossRef]
- Norton ID, Andrews JC, Kamath PS. Management of EcV. Hepatology. 1998;28:1154–8.
- Shou-jiang Tang MD, Simon Zanati, MD, Elena Dubcenco, MD, Maria Cirocco, MSc, Dimitrios Christodoulou, MD, Gabor Kandel, MD, Gregory B. Haber, MD, Paul Kortan, MD, Norman E. Marcon, MD,2004.
- Dev S Segarajasingam,1Stephen C Hanley,2Alan N Barkun,3,4Kevin A Waschke,3Pascal Burtin,5J Randomized Controlled Trial Comparing Outcomes of Video Capsule Endoscopy with Push Enteroscopy in Obscure Gastrointestinal Bleeding Can J Gastroenterol Hepatol Vol 29 No 2 March 2015.
- Kennedy DW , Laing CJ , Tseng LH et al. Detection of active gastrointestinal hemorrhage with CT angiography: a 4(1/2)-year retrospective review . J Vasc Interv Radiol 2010 ; 21 : 848 – 55.
- Yoon W, Jeong YY, Shin SS, et al. Acute massive gastrointestinal bleeding: detection and localization with arterial phase multi–detector row helical CT. Radiology 2006; 239:160 –167. [CrossRef]
- T.A Sos, J G Lee, D. Wixson, K.W. Sniderman, Intermittent bleeding from minute to minute in acute massive gastrointestinal hemorrhage,1978. [CrossRef]
- Pennazio M , Santucci R , Rondonotti E et al. Outcome of patients with obscure gastrointestinal bleeding aft er capsule endoscopy: report of 100 consecutive cases . Gastroenterology 2004 ; 126 : 643 – 53.
- Pasha SF , Leighton JA , Das A et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis . Clin Gastroenterol Hepatol 2008 ; 6 : 671 – 6. [CrossRef]
- Jones BH , Fleischer DE , Sharma VK et al. Yield of repeat wireless video capsule endoscopy in patients with obscure gastrointestinal bleeding . Am J Gastroenterol 2005 ; 100 : 1058 – 64.). [CrossRef]
- Mensink PB, Haringsma J, Kucharzik T, et al. Complications of double balloon enteroscopy: a multicenter survey. Endoscopy. 2007;39:613–5). [CrossRef]
- Samaha E, Rahmi G, Landi B, et al. Long-term outcome of patients treated with double balloon enteroscopy for small bowel vascular lesions. Am J Gastroenterol. 2012;107(2):240-246. [CrossRef]
- Nabeel M. Akhter, Ziv J. Haskal, Diagnosis and management of ectopic varices,2012. [CrossRef]
- D. Lebrec, J.P. Benhamou Ectopic varices in portal hypertension,1985.
- H. Hekmat, A. Al-toma, M.P. Mallant, C.J. Mulder, M.A. Jacobs, Endoscopic N-butyl-2-cyanoacrylate (Histoacryl) obliteration of jejunal varices by using the double balloon enteroscope,2007. [CrossRef]
- R.J. Schmitz, P. Sharma, A.S. Badr, M.T. Qamar, A.P. Weston Incidence and management of esophageal stricture formation, ulcer bleeding, perforation and massive hematoma formation from sclerotherapy versus band ligation,2001. [CrossRef]
- S. Seewald, U. Seitz, A.M. Yang, N. Soehendra,Variceal bleeding and portal hypertension: still a therapeutic challenge?,2001. [CrossRef]
- T. Tajiri, M. Onda, H. Yoshida, Y. Mamada, N. Taniai, M. Umehara, et al.,Endoscopic scleroligation is a superior new technique for preventing recurrence of esophageal varices,2002. [CrossRef]
- Y.H. Choi, C.J. Yoon, J.H. Park, J.W. Chung, J.W. Kwon, G.M. Choi Balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding: its feasibility compared with transjugular intrahepatic portosystemic shunt,2003.
- M.J. Kim, B.K. Jang, W.J. Chung, J.S. Hwang, Y.H. Kim Duodenal variceal bleeding after balloon-occluded retrograde transvenous obliteration: treatment with transjugular intrahepatic portosystemic shunt,2012.
- K.S. Park, Y.H. Kim, J.S. Choi, J.S. Hwang, J.H. Kwon, B.K. Jang, et al. Therapeutic efficacy of balloon-occluded retrograde transvenous obliteration in patients with gastric variceal bleeding,2006 al.
- K. Takamura, H. Miyake, H. Mori, Y. Terashima, T. Ando, M. Fujii, et al. Balloon occluded retrograde transvenous obliteration and percutaneous transhepatic obliteration for ruptured duodenal varices after operation for rectal cancer with multiple liver metastasis: report of a case,2005. [CrossRef]
- N. Hashimoto, T. Akahoshi, D. Yoshida, et al. The efficacy of balloon-occluded retrograde transvenous obliteration on small intestinal variceal bleeding,2010. [CrossRef]
- Keita Minowa, Shuhei Komatsu, Kenichiro Takashina, Sachie Tanaka, Tatsuya Kumano, Kenichiro Imura, Katsumi Shimomura, Jun Ikeda, Fumihiro Taniguchi, Yasuo Ueshima, Tecchuu Lee, Eito Ikeda, Eigo Otsuji, Yasuhiro Shioaki, Ectopic gastrointestinal variceal bleeding with portal hypertension Keita,2017.
- Martin Rossle, M.D., Volker Siegerstetter, M.D., Manfred Olschewski, Ph.D., Andreas Ochs, M.D., Elisabeth Berger, and Klaus Haag, M.D., How Much Reduction in Portal Pressure Is Necessary to Prevent Variceal Rebleeding? A Longitudinal Study in 225 Patients With Transjugular Intrahepatic Portosystemic Shunts, 2001. [CrossRef]
- V Vidal, L.Joly, P.Perreault, L.Bouchard, M.Lafortune, Usefulness of transjugular portosystemic shunt in the management of bleeding ectopic varices in cirrhotic patients,2006.
- G. Smith-Laing, J. Scott, R.G. Long, S. Sherlock Role of percutaneous transhepatic obliteration of varices in the management of bleeding from gastroesophageal varices,1981.
- Marcello Vangeli, David Patch, Natalia Terreni, John Tibballs, Anthony Watkinson, Andrew Kenneth Burroughs, Bleeding ectopic varices--treatment with transjugular intrahepatic porto-systemic shunt (TIPS) and embolization,2004.
- M. Sakai, A. Nakao, T. Kaneko, S. Takeda, S. Inoue, Y. Yagi, et al. Transhepatic portal venous angioplasty with stenting for bleeding jejunal varices,2005.
- Anis Haddad, Hazem Beji, Youssef Chaker, Houcine Maghrebi, Mohamed Jouini, Montassar Kacem, Surgical treatment for bleeding ileal varices: A case report,2021. [CrossRef]
- Hirotaka Konishi, Shojiro Kikuchi, Atsushi Miyashita, Daisuke Ichikawa, Hitoshi Fujiwara, Takeshi Kubota, Toshiya Ochiai, Yukihito Kokuba, Satoshi Yasukawa, Akio Yanagisawa & Eigo Otsuji, Minimally invasive surgery for obscure idiopathic ileal varices diagnosed by capsule endoscopy and double balloon endoscopy: report of a case, 2010. [CrossRef]
- Takahisa Suzuki, Mutsumi Murayama,Masataka Shinoda,Takafumi Ando et al, Rupture of ileal varices in a type C liver cirrhosis patient: a case report,2009.
- Satoshi Ambiru , Shunta Nakamura , Yasushi Mandai , Toru Sato , Takeichiro Kuwahara and Osamu Yokosuka, Ectopic Ileal Varices Associated with Recurrent Bleeding: Report of a Case,2011. [CrossRef]
- Junji Ueda,Hiroshi Yoshida, Yasuhiro Mamada,Takashi Tajiri et al., Successful emergency enterectomy for bleeding ileal varices in a patient with liver cirrhosis,2006. [CrossRef]
- Gianpaolo Carrafiello & Domenico Laganà & Andrea Giorgianni & Domenico Lumia & Monica Mangini & Edi Paragone & Carlo Fugazzola, Bleeding from peristomal varices in a cirrhotic patient with ileal conduit: treatment with transjugular intrahepatic portocaval shunt (TIPS),2007. [CrossRef]
- John V. Conte, M.D., Todd A. Arcomano, M.D., Mohammed A. Naficy, M.D., Richard W. Holt, M.D, Treatment of Bleeding Stomal Varices Report of a Case and Review of the Literature,2022.
- Kazuma Kobayashia, Junzo Yamaguchia, Akihiko Mizoea, Ichiro Isomotob, Tsuyoshi Koshiishib, Kunihide Izawaa and Takashi Kanematsuc, Successful treatment of bleeding due to ileal varices in a patient with hepatocellular carcinoma,2001. [CrossRef]
- Patrick Malleaa , Aaron Allenb , Maureen Kim Lynchc , Elsbeth Jensen-Otsud and David Tompkinse, Massive gastrointestinal bleeding due to ectopic varix in distal duodenum: a case report,2014. [CrossRef]
- Claire L Jansson-Knodell , Gerardo Calderon , Regina Weber , Marwan Ghabril ,Small Intestine Varices in Cirrhosis at a High-Volume Liver Transplant Center: A Retrospective Database Study and Literature Review,2021. [CrossRef]
Figure 1.
Ileal portocaval shunts.
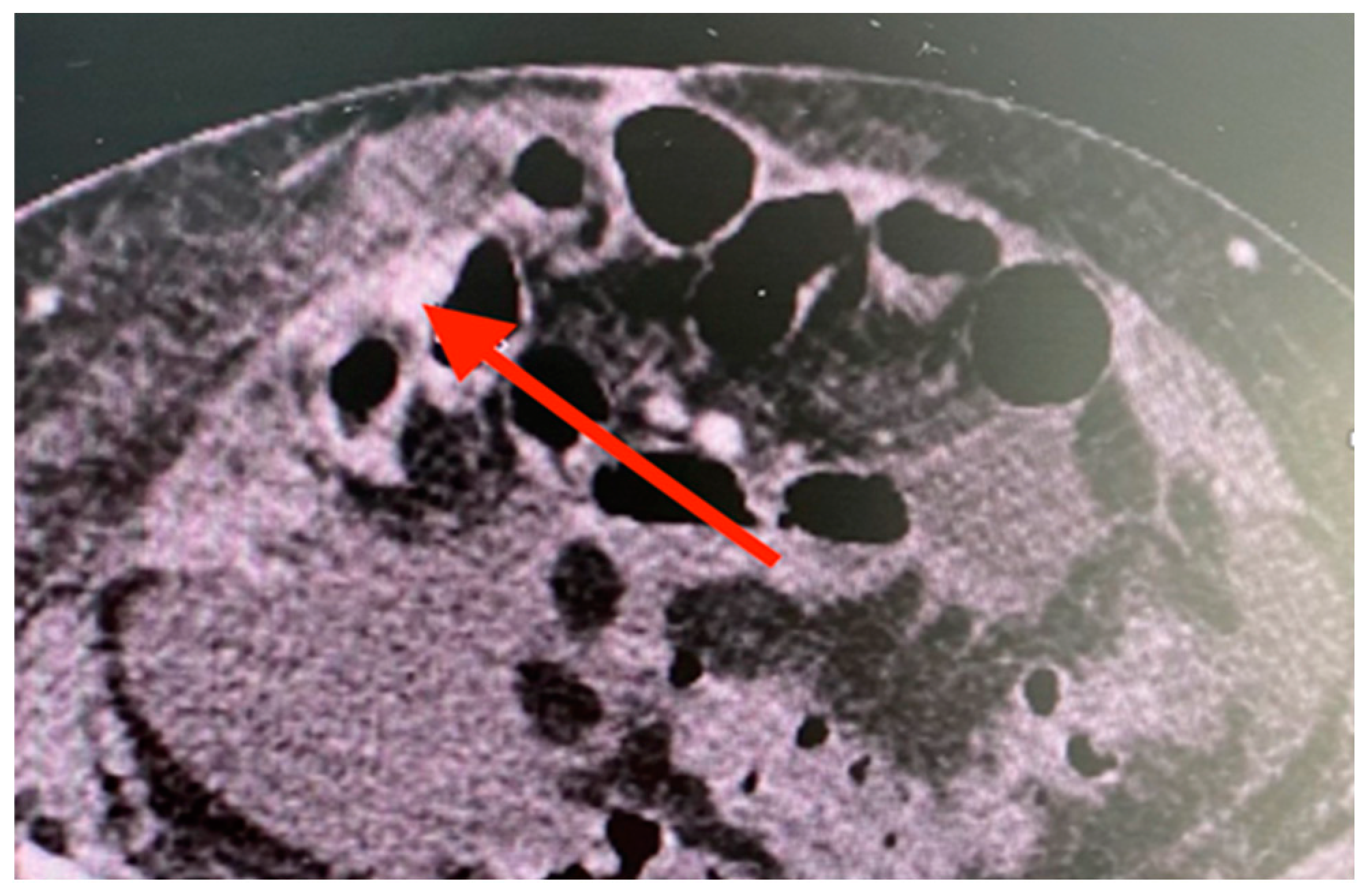
Figure 2.
Enteral variceal cords with bleeding stigmata.
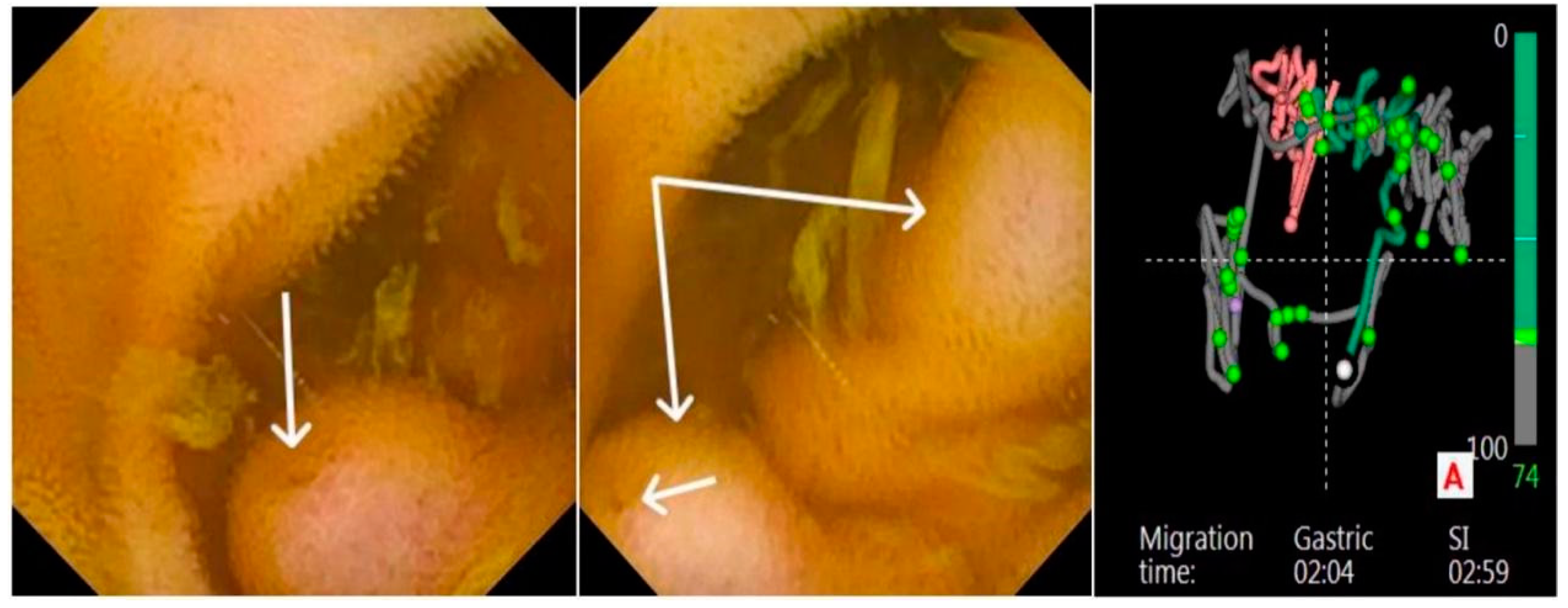
Figure 3.
A and 3B. Active variceal bleeding during laparotomy (A). Successful enterectomy followed by enterorrhaphy (B).
Figure 3.
A and 3B. Active variceal bleeding during laparotomy (A). Successful enterectomy followed by enterorrhaphy (B).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



