
Submitted:
04 December 2024
Posted:
05 December 2024
You are already at the latest version
Abstract
Background/Objectives: Chronic exposure to stress has been considered a risk factor for hyper-tension, which is also associated with increased bone resorption. This review aimed to investigate the effect of acute and chronic stress, associated with hypertension, on the skeletal system. Methods: This narrative review was designed with searches in databases, mainly Pub-Med/MEDLINE, with emphasis on the following topics: bone disorders, emotional stress, arterial hypertension and relationship between emotional stress and bone disorders. The selection of manuscripts for detailed analysis was made, checked and inserted into a table by consensus of all authors. Results: The main topics include situations that favor bone loss, such as psychological stress, which can lead to osteoporotic fractures through immunological and endocrine mecha-nisms. The relationship between psychological stress and loss of bone density, as in osteoporosis, occurs due to the reduction in the number of osteoblasts and loss in the balance between physi-ological formation/resorption. Conclusions: Chronic stress significantly affects cardiovascular health and bone resorption. This narrative review study highlights the vulnerability of the skeletal system to prolonged stress, along with the cardiovascular system, highlighting the need for multidisciplinary strategies in preventing stress-related conditions. Effective stress management can help reduce the risks of cardiovascular disease and bone resorption, emphasizing their role in comprehensive health care.
Keywords:
hypertension
; psychological stress
; acute stress
; chronic stress
; bone density
; osteoporosis
; func-tional morphology
1. Introduction
Among cardiovascular diseases, hypertension is considered a serious and silent disease, associated with hypoalgesia [1]. Hypertension will be, among non-communicable diseases, according to the World Health Organization (WHO), the most important cause of functional disability in the coming decades. Risk factors increase high blood pressure, such as lifestyle, sedentary lifestyle, smoking, foods rich in fat, and non-restorative nights of sleep [2]. Psychosocial factors may also play an important role in increasing blood pressure. Exposure to chronic stress has been identified as a risk factor. Occupational stress, stressful aspects of the social environment and low socioeconomic status have been studied [3].
The impact of stress on the development of hypertension is believed to involve a sympathetic nervous system response, in which the release of catecholamines leads to increased heart rate, cardiac output, and blood pressure [4]. The literature indicates that individuals with a greater reaction to stressful tasks are 21% more likely to have high blood pressure than those with a lower reaction, which suggests the importance of stress control in the non-drug treatment of high blood pressure [5]. The effects of acute stressors have been demonstrated, but continued exposure to stress may be more plausibly linked to sustained elevations in blood pressure and the incidence of hypertension [6].
Therefore, changes in lifestyle, especially with the inclusion of physical exercise and the relationship with high blood pressure require attention. In addition to being a notable but modifiable risk factor for stroke and coronary artery disease, high blood pressure also leads to atrial fibrillation, congestive heart failure and kidney failure, in addition to being an important component of metabolic syndrome [7]. The beneficial effect of regular exercise not only leads to a reduction in blood pressure, but it has also been shown to reduce left ventricular hypertrophy and improve quality of life. When combined with dietary changes, regular exercise causes reduced oxidative stress, increases nitric oxide availability, and improves overall metabolic profile [8].
As for bone tissue, under the influence of gravity, it undergoes greater or lesser deformation according to the intensity of daily life activities. It is known that activities that result in impact are those that most stimulate osteogenesis and thus reduce the loss of bone mass. Knowing how bone cells recognize the mechanical deformation imposed on the bone and initiate a series of biochemical chain reactions is of fundamental importance for the development of therapeutic and preventive practices [9]. Furthermore, evidence indicates that high blood pressure is associated with abnormalities in calcium metabolism: calcium loss can lead to increased bone mineral loss in individuals with high blood pressure [10]. Essential or idiopathic or primary hypertension, the most common type of hypertension, has different effects on bone mineral density in different locations [11].
With societal trends toward aging and lifestyle changes (such as increased intake of high-fat foods and reduced physical activity), the prevalence rates of essential or primary hypertension and osteoporosis increase. each year. Both hypertension and osteoporosis are age-related diseases and result from the interaction of genetic and environmental factors [12].
Furthermore, the prevalence of chronic disorders, high blood pressure and bone pathologies, as well as emotional disorders, such as stress, in the general population, today demands a need for studies on these topics, with the aim of better understanding the aspects physiological, morphological and biochemical changes in these conditions. Therefore, investment in studies in this area aims to demand new future drug therapies that have “multi-targets”, so that patients in this profile suffer fewer side effects. Considering these propositions and needs, this project aims to characterize the influence of varied acute and chronic stress associated with arterial hypertension on the skeletal system.
2. Bone Disorders
Bone is a dynamic tissue and is in a constant process of remodeling to maintain ideal mass and integrity throughout life [13]. It has basic functions such as support, protection and locomotion and is under the control of systemic factors, such as hormones, and local factors, such as growth factors and cytokines [14].
The homeostasis of the skeletal system depends on balanced bone remodeling, that is, on the balanced dynamics between the activity of osteoblasts (bone formation cells) and osteoclasts (bone resorption cells). In addition to osteoblasts and osteoclasts, bone tissue also contains cells called osteocytes [15]. Osteocytes are the most abundant cell type in bone tissue and are considered essential for bone maintenance as well as bone remodeling, since it has been suggested that osteocyte apoptosis can attract and stimulate osteoclast activity [16].
Bone is made up of an organic part (consisting of type I collagen, proteoglycans and adhesive glycoproteins) and an inorganic part (phosphate ions, calcium and, to a lesser extent, bicarbonate, magnesium, potassium, sodium and citrate) [17]. The union of phosphate and calcium forms crystals with a hydroxyapatite structure that, associated with collagen fibers, provides the resistance and hardness characteristic of bone tissue [18]. An important group of glycoproteins, extracted from the demineralized bone matrix, are bone morphogenetic proteins (BMPs) and are responsible for bone induction. Research shows that, among the more than 20 BMPs discovered to date, there are differences between them in their ability to induce osteogenesis [19]. BMPs 2, 6 and 9 appear to have greater potential in inducing osteoblastic differentiation from mesenchymal progenitor cells [20].
When there is an imbalance in the activity of bone cells or matrix components associated with systemic and local factors, bone pathologies may arise [21]. Among the most common pathologies, osteoporosis, arthritis and osteosarcoma can be highlighted [22]. In the dental area, the presence of bone resorption associated with periodontal diseases, traumatic surgeries or even for physiological reasons due to lack of ridge function or inadequate prosthetic load is very common [23].
Thus, due to its importance in both the medical and dental areas, there is great development in approaches to bone disorders associated with other diseases, drug therapies, biomaterials, grafts [24].
3. Emotional Stress
Stress is a set of reactions of the organism, characterized by an imbalance in homeostasis, in response to threats and/or aggressions arising from environmental stimuli, of a psychic or physical nature, unusual or hostile [25]. Stress designates all non-specific effects of factors that can act on the organism and has been characterized as a general adaptation syndrome, composed of three phases: alarm reaction, adaptation phase and exhaustion phase [26].
Stress comprises daily events that increase physiological activities and consequently cause psychological exhaustion to a certain extent. Modern life events, such as family and work-related problems, social withdrawal, financial concerns and violence, are some factors that can predispose or increase stress [27].
Psychological stress is characterized by a particular relationship between the individual and the environment, which is interpreted by the individual as a process of overload that exceeds their possibilities of adaptation and threatens their well-being. Stress situations promote a series of physiological and behavioral changes that can affect hormonal and neurotransmitter systems, causing different responses in the same individual to each new situation [28].
To study the consequences of stress and its relationship with so-called stress-related disorders, animal models have been used [29]. This is because the absence of stress is a powerful indicator of the animal's well-being. In rats, stress also modulates reproductive function [30]. The chronic stress protocol has been applied to animal models and is widely used to investigate the physiological and behavioral consequences of long-term stressful conditions [31]. In evidence, the activity of the hypothalamic-pituitary adrenal (HPA) axis is directly linked to the body's physiological responses to stress. Knowing that the HPA axis is formed by adrenocorticotropic hormones (ACTH) and corticosterone, serum concentrations of these hormones are considered an important indicator of stress, including in animal models [32].
4. Arterial Hypertension
Arterial hypertension (AH) is part of the group of cardiovascular diseases that represent the highest percentage of causes of mortality, such as cerebrovascular accident (CVA) and acute myocardial infarction [33]. This multifactorial clinical entity is characterized by the presence of systolic blood pressure (SBP) levels persistently equal to or above 140 mmHg and/or diastolic blood pressure (DBP) levels persistently equal to or above 90 mmHg [34].
In individuals without preexisting heart disease, the proportion of unrecognized myocardial infarctions increases significantly with the severity of hypertension. Thus, hypertensive patients have an increased risk of myocardial infarction and of such an event not being recognized [35].
Arterial hypertension can be primary/essential or secondary [36]. The causes of primary arterial hypertension are not known in most cases, whereas secondary arterial hypertension must be investigated, since the etiological diagnosis means, in many cases, the possibility of specific treatment and cure or control by clinical or surgical intervention [37].
As for the known risk factors for hypertension, the most important are obesity, smoking, alcohol intake, family history of hypertension, psychological factors, certain personality traits and stress, which can be important triggers in the development of hypertension [38]. Genetic and environmental factors, such as physical inactivity and excessive sodium consumption, are also mentioned [39].
Arterial hypertension and osteoporosis are diseases considered predominant among the most prevalent chronic diseases in the elderly population [40]. Considering the aging of the Brazilian population and the increase in the life expectancy of these elderly people, there is an increase in the demand for specialized health services for this population and in studies aimed at bone and cardiovascular diseases.
Animal models using spontaneously hypertensive and normotensive rats have been used to study chronic conditions of arterial hypertension [41]. However, to date, few studies have used these models for investigating factors related to bone disorders and hypertension. Furthermore, reports on skeletal changes in hypertensive animal models are conflicting [42].
5. Relationship Between Emotional Stress and Bone Disorders
Emotional stress is closely related to abnormalities in bone metabolism and can lead to reduced bone mass and increased risk of fractures [43,44,45]. Bone metabolism is a physiological process regulated through the sympathetic nervous system by substances produced by the hypothalamus [46]. Also, in the hypothalamus where emotions are controlled [47]. Thus, changes in the central nervous system can induce changes in bone mass. The humoral mechanism initiated and orchestrated by the central nervous system has been perceived as a fundamental regulatory pathway from the nervous system to bone metabolism [48]. The regulatory pathway for bone metabolism arises from leptin. Leptin modulates bone mass, altering sympathetic tone after acting on the hypothalamus [49]. This causes peripheral nerves to release norepinephrine into the local microenvironment, which in turn activates β -adrenergic receptors expressed by osteoblasts [50]. Other molecules, such as neuromedin U, also regulate bone mass through signals processed in the hypothalamus. These signals, in turn, modulate sympathetic signals transmitted by peripheral nerves [51].
Intraosseous nerves are well distributed throughout the skeleton, including cortical and trabecular bone, bone marrow, and periosteum. Intraosseous motor nerves are mainly visceral motor nerves, which are divided into adrenergic and cholinergic nerves according to their released neurotransmitters. These peripheral nerves communicate with the skeleton to regulate bone metabolism through resident nerve cells, locally released neurotransmitters, neuropeptides, axon guidance factors, and neurotrophins [52]. Bone metabolism is regulated by signals generated by intraosseous nerves. These signals mediate bone mass and maintain bone micro- and macroarchitecture through regulation of bone deposition by osteoblasts and resorption by osteoclasts [53].
Depression is responsible for abnormal emotional and physical symptoms that include loss of interest and dysregulated sleep. Anxiety can be accompanied by physical symptoms, such as increased heart rate and shortness of breath. These mood disorders often have a common cause: psychological stress. In addition to osteoporosis, bone abnormalities related to psychological stress are also regulated by peripheral nerves [54].
Psychological stress can accelerate bone loss and osteoporotic fractures through immunological and endocrine mechanisms. The relationship between psychological stress and osteoporosis has been demonstrated with chronic mild stress, an established model in rodents that leads to depression, causing a reduction in the number of osteoblasts, bone loss and reduced bone formation. Peripheral nerves participate in the regulation of bone metabolism in individuals with psychological stress. One way in which psychological stress may impact the risk and severity of osteoporotic disease is through catecholamine-induced activation of β -adrenergic receptors on osteoblasts and osteoclasts, which may increase RANKL expression and result in osteoclast differentiation [55] (Figure 1 and Table 1).
Chronic stress protocol has already been studied in both experimental and clinical study models. It was observed that there is a relationship between emotional stress and bone resorption (Table 1). In addition to the chronic stress protocol, there is also the possibility of occasional stress, which is called acute stress. It is interesting to be able to investigate the action of acute stress on bone resorption, which is not yet available in literature.
The relationship between bone tissue and emotional stress is a complex and growing field of study in medical research. Chronic stress leads to an increase in the production of hormones such as cortisol. High cortisol levels have been linked to reduced bone mineral density, which may increase the risk of osteoporosis and fractures [79]. Cortisol can interfere with bone formation and promote bone resorption, where bone tissue is destroyed faster than it is formed. Chronic stress leads to an increase in the production of hormones such as cortisol. Elevated cortisol levels have been linked to reduced bone mineral density, which may increase the risk of osteoporosis and fractures [80]. Cortisol can interfere with bone formation and promote bone resorption, where bone tissue is destroyed faster than it is formed. Stress can also increase inflammation in the body. Elevated inflammatory markers are associated with bone loss and can exacerbate conditions such as arthritis. People under stress can adopt behaviors that are harmful to bone health, such as an inadequate diet, a sedentary lifestyle or excessive consumption of alcohol and tobacco [81].
These behaviors can contribute to the deterioration of bone health. Mental health conditions such as depression and anxiety, often associated with stress, can also impact bone health. Depression, for example, can be associated with a decrease in physical activity and a poor diet, both factors that affect bone health. Research has shown that chronic stress can have an adverse effect on bone health over time. Longitudinal studies indicate that prolonged exposure to stress can accelerate bone loss and increase susceptibility to fractures. Interventions that reduce stress, such as stress management techniques, therapy, and wellness practices, can have a positive impact on bone health by helping to mitigate some of the adverse effects of chronic stress [82]. Emotional stress can negatively influence bone health through hormonal, behavioral and psychosocial mechanisms. It is important to consider integrated approaches to managing stress and maintaining bone health to promote overall well-being [83].
The relationship between bone, stress and inflammatory markers is an important aspect of bone biology and the stress response. Chronic stress can trigger an inflammatory response, which in turn can negatively impact bone health. Chronic stress can increase the production of inflammatory cytokines, such as TNF-alpha (tumor necrosis factor alpha), IL-1 (interleukin-1), IL-6 (interleukin-6), and CRP (C-reactive protein). These cytokines are involved in the inflammatory response and can influence bone health. Inflammatory cytokines, especially IL-1 and IL-6, can stimulate the activity of osteoclasts, the cells responsible for bone resorption. Increased osteoclast activity leads to greater degradation of bone tissue, contributing to the loss of bone mass [84]. Chronic inflammation can promote an environment in which bone remodeling processes are unbalanced, with a predominance of resorption over bone formation. Inflammatory cytokines can affect the bone matrix, the structure in which osteoblasts deposit new bone, interfering with mineralization and bone integrity.
Chronic stress is associated with an increase in the production of inflammatory markers, which in turn negatively affect bone health. Inflammatory cytokines can increase osteoclast activity and inhibit osteoblast function, resulting in bone loss. Furthermore, chronic inflammation can unbalance the bone remodeling process and compromise bone integrity. Therefore, managing stress and reducing inflammation are important for maintaining bone health and preventing related diseases [85].
People under stress can adopt behaviors that are harmful to bone health, such as an inadequate diet, a sedentary lifestyle or excessive consumption of alcohol and tobacco. These behaviors can contribute to the deterioration of bone health. Bone loss is strongly influenced by different lifestyle habits. Daily habits can have a significant impact on bone health, affecting both bone formation and resorption. Calcium is essential for the formation and maintenance of bones. A diet low in calcium can lead to a decrease in bone density. Calcium-rich foods include dairy products, dark green leafy vegetables, and fortified foods. Vitamin D is crucial for calcium absorption. Vitamin D deficiencies can harm bone health. Sun exposure and foods fortified with vitamin D can help maintain adequate levels. High levels of caffeine and excessive alcohol consumption can interfere with calcium absorption and bone formation. Moderating your intake of these items can help maintain bone health.
A diet low in nutrients essential for bone health, such as magnesium and vitamin K, can contribute to bone loss. Physical exercise, especially weightlifting and weight-bearing activities such as walking and running, stimulates bone formation and improves bone density. Lack of physical activity can lead to loss of bone mass. Resistance exercises, such as weight training, are particularly beneficial for bone health as they help to strengthen muscles and bones [86].
In addition, we can mention lifestyle behaviors such as smoking and alcohol consumption. Smoking is associated with lower bone density and an increased risk of fractures. Smoking can harm bone formation and reduce calcium absorption. Excessive alcohol consumption can interfere with bone formation and increase the risk of fractures [87]. Alcohol can also affect the absorption of nutrients essential for bone health. Sun exposure is important for the production of vitamin D, which is necessary for the absorption of calcium and the maintenance of bone health. Recommendations to promote bone health associated with lifestyle habits are: Maintain a Balanced Diet: Include foods rich in calcium and vitamin D and avoid excess caffeine and alcohol. Exercise Regularly: Practice physical activities that include weight-bearing and resistance exercises. No Smoking: Avoid smoking and minimize alcohol consumption. Monitor Health Conditions: Manage medical conditions that may impact bone health and discuss the effects of medications with a healthcare professional. Check Nutrient Levels: Check and maintain adequate levels of calcium and vitamin D through diet and sun exposure. In summary, bone loss can be influenced by a series of lifestyle habits. Adopting a healthy lifestyle, which includes a balanced diet, regular physical activity and avoiding harmful behaviors, can help preserve bone health and reduce the risk of conditions such as osteoporosis [88].
Mental health conditions such as depression and anxiety, often associated with stress, can also impact bone health. Depression, for example, can be associated with a decrease in physical activity and a poor diet, both factors that affect bone health. Depression and anxiety often lead to decreased physical activity and can lead to poor diet. A lack of essential nutrients, such as calcium and vitamin D, can compromise bone health. Some medications used to treat depression, such as tricyclic antidepressants and serotonin reuptake inhibitors (SSRIs), can have side effects that impact bone health, although this relationship can vary. It is important to monitor and discuss any potential impacts with a healthcare professional [89].
Anxiety often causes sleep disturbances, and a lack of quality sleep can negatively affect bone health. Sleep is important for bone regeneration and maintenance. Seeking treatment for depression and anxiety through therapy, medication and psychological support can help improve quality of life and minimize the impact on bone health. Maintaining a balanced diet rich in calcium and vitamin D, exercising regularly and adopting stress management strategies are essential for bone health. Having regular bone density screenings and discussing with healthcare professionals the influence of mental health conditions and medications on bone health can help with early detection and prevention of bone problems [90]. In summary, depression and anxiety can impact bone health in several ways, primarily through reduced physical activity, a poor diet, and hormonal and behavioral changes. Addressing these conditions holistically and maintaining a healthy lifestyle can help protect and improve bone health.
In summary, emotional stress can negatively influence bone health through hormonal, behavioral and psychosocial mechanisms. It is important to consider integrated approaches to managing stress and maintaining bone health to promote overall well-being (Figure 2).
6. Conclusions
The findings of this study reinforce the growing evidence that chronic stress plays a significant role not only in the etiology of cardiovascular diseases but also in bone health. Our observations indicate a clear association between chronic stress and bone resorption, suggesting that the skeletal system, like the cardiovascular system, is highly vulnerable to the deleterious effects of prolonged stress. This finding broadens our understanding of the systemic impact of stress, highlighting the need for a multidisciplinary approach in the prevention and treatment of stress-related conditions.
Moreover, the interrelationship between the cardiovascular and skeletal systems under stress underscores the importance of therapeutic interventions aimed at both reducing stress levels and protecting these systems. Effective stress management may be a crucial strategy for mitigating the risks of both cardiovascular diseases and bone resorption, preventing more severe complications in patients experiencing chronic stress.
Author Contributions
Conceptualization, M.R.P. and J.P.M.I.; methodology, M.R.P., M.A., S.F., D.V.B., R.L.B. and J.P.M.I.; formal analysis, M.R.P., M.A., S.F., D.V.B., R.L.B. and J.P.M.I.; writing—original draft preparation, M.R.P. and J.P.M.I.; writing—review and editing, M.A., S.F., D.V.B. and R.L.B.; visualization, M.R.P., M.A., S.F., D.V.B., R.L.B. and J.P.M.I.; supervision, J.P.M.I.; funding acquisition, D.V.B. and R.L.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ferguson, M.; Slepian, M.; France, C.; Svendrovski, A.; Katz, J. Hypertensive Hypoalgesia in a Complex Chronic Disease Population. J. Clin. Med. 2021, 10, 3816. [Google Scholar] [CrossRef]
- Qiu, T.; Jiang, Z.; Chen, X.; Dai, Y.; Zhao, H. Comorbidity of Anxiety and Hypertension: Common Risk Factors and Potential Mechanisms. Int. J. Hypertens. 2023, 2023, 9619388. [Google Scholar] [CrossRef]
- Spruill, T.M. Chronic Psychosocial Stress and Hypertension. Curr. Hypertens. Rep. 2010, 12, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Liu, Y.; Chen, S.; et al. A GABAergic Neural Circuit in the Ventromedial Hypothalamus Mediates Chronic Stress-Induced Bone Loss. J. Clin. Invest. 2020, 130, 6539–6554. [Google Scholar] [CrossRef] [PubMed]
- Arroyave-Atehortua, D.; Cordoba-Sanchez, V.; Zambrano-Cruz, R. Perseverative Cognition as a Mediator Between Personality Traits and Blood Pressure. Vasc. Health Risk Manag. 2023, 19, 363–370. [Google Scholar] [CrossRef]
- Schaupp, J.; Hediger, K.; Wunderli, J.M.; Schäffer, B.; Tobias, S.; Kolecka, N.; Bauer, N. Psychophysiological Effects of Walking in Forests and Urban Built Environments with Disparate Road Traffic Noise Exposure: Study Protocol of a Randomized Controlled Trial. BMC Psychol. 2024, 12, 250. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Przysucha, E.; Klarner, T.; Zerpa, C.; Maransinghe, M.K. Bimanual Coordination in Individuals Post-stroke: Constraints, Rehabilitation Approaches and Measures: Systematic Review. Int. J. Exerc. Sci. 2024, 17, 831–851. [Google Scholar] [PubMed]
- Bletsa, E.; et al. Exercise Effects on Left Ventricular Remodeling in Patients with Cardiometabolic Risk Factors. Life 2023, 13, 1742. [Google Scholar] [CrossRef]
- Xu, P.; Zhao, N.; Wang, J. Knowledge, Attitude, and Practice Toward Osteoporosis Among Patients with Chronic Kidney Disease in Zhejiang. Medicine (Baltimore) 2024, 103, e38153. [Google Scholar] [CrossRef]
- Jolic, M.; Sharma, S.; Palmquist, A.; Shah, F.A. The Impact of Medication on Osseointegration and Implant Anchorage in Bone Determined Using Removal Torque—A Review. Heliyon 2022, 8, e10844. [Google Scholar] [CrossRef]
- Lu, H.; Lary, C.W.; Hodonsky, C.J.; Peyser, P.A.; Bos, D.; van der Laan, S.W.; Miller, C.L.; Rivadeneira, F.; Kiel, D.P.; Kavousi, M.; Medina-Gomez, C. Association Between BMD and Coronary Artery Calcification: An Observational and Mendelian Randomization Study. J. Bone Miner. Res. 2024, 39, 443–452. [Google Scholar] [CrossRef]
- Kassis, A.; et al. Nutritional and Lifestyle Management of the Aging Journey: A Narrative Review. Front. Nutr. 2023, 9, 1087505. [Google Scholar] [CrossRef] [PubMed]
- Hadjidakis, D.J.; Androulakis, I.I. Bone Remodeling. Ann. N.Y. Acad. Sci. 2006, 1092, 385–396. [Google Scholar] [CrossRef]
- Serim, T.M.; Amasya, G.; Eren-Böncü, T.; Şengel-Türk, C.T.; Özdemir, A.N. Electrospun Nanofibers: Building Blocks for the Repair of Bone Tissue. Beilstein J. Nanotechnol. 2024, 15, 941–953. [Google Scholar] [CrossRef]
- Al-Bari, A.A.; Al Mamun, A. Current Advances in Regulation of Bone Homeostasis. FASEB BioAdvances 2020, 2, 668–679. [Google Scholar] [CrossRef]
- Marahleh, A.; Kitaura, H.; Ohori, F.; Noguchi, T.; Mizoguchi, I. The Osteocyte and Its Osteoclastogenic Potential. Front. Endocrinol. (Lausanne) 2023, 14, 1121727. [Google Scholar] [CrossRef]
- Ansari, N.; Sims, N.A. The Cells of Bone and Their Interactions. Handb. Exp. Pharmacol. 2020, 262, 1–25. [Google Scholar]
- Ansari, M. Bone Tissue Regeneration: Biology, Strategies and Interface Studies. Prog. Biomater. 2019, 8, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Lofaro, F.D.; Costa, S.; Simone, M.L.; Quaglino, D.; Boraldi, F. Fibroblasts' Secretome from Calcified and Non-calcified Dermis in Pseudoxanthoma Elasticum Differently Contributes to Elastin Calcification. Commun. Biol. 2024, 7, 577. [Google Scholar] [CrossRef] [PubMed]
- Ke, K.X.; Gao, X.; Liu, L.; He, W.G.; Jiang, Y.; Long, C.B.; Zhong, G.; Xu, Z.H.; Deng, Z.L.; He, B.C.; Hu, N. Leptin Attenuates the Osteogenic Induction Potential of BMP9 by Increasing β-Catenin Malonylation Modification via Sirt5 Down-Regulation. Aging (Albany NY) 2024, 16, 7870–7888. [Google Scholar] [CrossRef]
- Vergatti, A.; Abate, V.; D'Elia, L.; De Filippo, G.; Piccinocchi, G.; Gennari, L.; Merlotti, D.; Galletti, F.; Strazzullo, P.; Rendina, D. Smoking Habits and Osteoporosis in Community-Dwelling Men Subjected to Dual-X-ray Absorptiometry: A Cross-Sectional Study. *J. Endocrinol. Invest.* 2024. Ahead of Print. [Google Scholar] [CrossRef]
- Hudhud, L.; Rozmer, K.; Kecskés, A.; Pohóczky, K.; Bencze, N.; Buzás, K.; Szőke, É.; Helyes, Z. Transient Receptor Potential Ankyrin 1 Ion Channel Is Expressed in Osteosarcoma and Its Activation Reduces Viability. Int. J. Mol. Sci. 2024, 25, 3760. [Google Scholar] [CrossRef]
- Tsuchida, S.; Nakayama, T. Recent Clinical Treatment and Basic Research on the Alveolar Bone. Biomedicines 2023, 11, 843. [Google Scholar] [CrossRef]
- Jiang, J.; Röper, L.; Fuchs, F.; Hanschen, M.; Failer, S.; Alageel, S.; Cong, X.; Dornseifer, U.; Schilling, A.F.; Machens, H.G.; Moog, P. Bone Regenerative Effect of Injectable Hypoxia Preconditioned Serum-Fibrin (HPS-F) in an Ex Vivo Bone Defect Model. Int. J. Mol. Sci. 2024, 25, 5315. [Google Scholar] [CrossRef]
- Chrousos, G.P. Stress and Disorders of the Stress System. Nat. Rev. Endocrinol. 2009, 5, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, J.K.; Engert, V.; Valk, S.L.; Singer, T.; Puhlmann, L.M.C. Mapping Pathways to Neuronal Atrophy in Healthy, Mid-Aged Adults: From Chronic Stress to Systemic Inflammation to Neurodegeneration? Brain Behav. Immun. Health 2024, 38, 100781. [Google Scholar] [CrossRef]
- Hammarström, A.; Westerlund, H.; Janlert, U.; Virtanen, P.; Ziaei, S.; Östergren, P.O. How Do Labour Market Conditions Explain the Development of Mental Health Over the Life-Course? A Conceptual Integration of the Ecological Model with Life-Course Epidemiology in an Integrative Review of Results from the Northern Swedish Cohort. BMC Public Health 2024, 24, 1315. [Google Scholar] [CrossRef]
- Kumar, A.; Rinwa, P.; Kaur, G.; Machawal, L. Stress: Neurobiology, Consequences and Management. J. Pharm. Bioallied Sci. 2013, 5, 91–97. [Google Scholar] [CrossRef]
- Atrooz, F.; Alkadhi, K.A.; Salim, S. Understanding Stress: Insights from Rodent Models. Curr. Res. Neurobiol. 2021, 2, 100013. [Google Scholar] [CrossRef]
- Patterson, Z.R.; Abizaid, A. Stress Induced Obesity: Lessons from Rodent Models of Stress. Front. Neurosci. 2013, 7, 130. [Google Scholar] [CrossRef]
- Tran, I.; Gellner, A.-K. Long-Term Effects of Chronic Stress Models in Adult Mice. J. Neural Transm. (Vienna) 2023, 130, 1133–1151. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, E.; Hatanaka, T.; Iijima, T.; Kimura, M.; Katoh, A. The Effects of Corticotropin-Releasing Factor on Motor Learning. Sci. Rep. 2024, 14, 17056. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The Global Epidemiology of Hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Picariello, C.; Lazzeri, C.; Attanà, P.; Chiostri, M.; Gensini, G.F.; Valente, S. The Impact of Hypertension on Patients with Acute Coronary Syndromes. Int. J. Hypertens. 2011, 2011, 563657. [Google Scholar] [CrossRef]
- Anthony, N.; Hassan, A.; Ghani, U.; Rahim, O.; Ghulam, M.; James, N.; Ashfaq, Z.; Ali, S.; Siddiqui, A. Age-Related Patterns of Symptoms and Risk Factors in Acute Coronary Syndrome (ACS): A Study Based on Cardiology Patients' Records at Rehman Medical Institute, Peshawar. Cureus 2024, 16, e58426. [Google Scholar] [CrossRef]
- Qiu, T.; Jiang, Z.; Chen, X.; Dai, Y.; Zhao, H. Comorbidity of Anxiety and Hypertension: Common Risk Factors and Potential Mechanisms. Int. J. Hypertens. 2023, 2023, 9619388. [Google Scholar] [CrossRef]
- Koszewicz, M.; Jaroch, J.; Brzecka, A.; Ejma, M.; Budrewicz, S.; Mikhaleva, L.M.; Muresanu, C.; Schield, P.; Somasundaram, S.G.; Kirkland, C.E.; Avila-Rodriguez, M.; Aliev, G. Dysbiosis Is One of the Risk Factors for Stroke and Cognitive Impairment and Potential Target for Treatment. Pharmacol. Res. 2021, 164, 105277. [Google Scholar] [CrossRef] [PubMed]
- Fabrazzo, M.; Cipolla, S.; Signoriello, S.; Camerlengo, A.; Calabrese, G.; Giordano, G.M.; Argenziano, G.; Galderisi, S. A Systematic Review on Shared Biological Mechanisms of Depression and Anxiety in Comorbidity with Psoriasis, Atopic Dermatitis, and Hidradenitis Suppurativa. Eur. Psychiatry 2021, 64, e71. [Google Scholar] [CrossRef]
- Pickering, T.G. The Effects of Environmental and Lifestyle Factors on Blood Pressure and the Intermediary Role of the Sympathetic Nervous System. J. Hum. Hypertens. 1997, 11, S9–18. [Google Scholar] [PubMed]
- Williams, J.S.; Egede, L.E. Differences in Medical Expenditures for Men and Women with Diabetes in the Medical Expenditure Panel Survey, 2008-2016. Womens Health Rep. (New Rochelle) 2020, 1, 345–353. [Google Scholar]
- Vetcher, A.A.; Zhukov, K.V.; Gasparyan, B.A.; Borovikov, P.I.; Karamian, A.S.; Rejepov, D.T.; Kuznetsova, M.N.; Shishonin, A.Y. Different Trajectories for Diabetes Mellitus Onset and Recovery According to the Centralized Aerobic-Anaerobic Energy Balance Compensation Theory. Biomedicines 2023, 11, 2147. [Google Scholar] [CrossRef]
- Ayala-Méndez, G.X.; Calderón, V.M.; Zuñiga-Pimentel, T.A.; Rivera-Cerecedo, C.V. Noninvasive Monitoring of Blood Pressure and Heart Rate during Estrous Cycle Phases in Normotensive Wistar-Kyoto and Spontaneously Hypertensive Female Rats. J. Am. Assoc. Lab. Anim. Sci. 2023, 62, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Ryan, K.R.; McDonald, L.T.; Jensen, N.R.; Sidles, S.J.; LaRue, A.C. Impacts of Psychological Stress on Osteoporosis: Clinical Implications and Treatment Interactions. Front. Psychiatry 2019, 10, 200. [Google Scholar]
- Jethwa, J.T. Musculoskeletal and Psychological Rehabilitation. Indian J. Orthop. 2023, 57 (Suppl 1), 260–266. [Google Scholar] [CrossRef]
- Coventry, P.A.; Meader, N.; Melton, H.; Temple, M.; Dale, H.; Wright, K.; Cloitre, M.; Karatzias, T.; Bisson, J.; Roberts, N.P.; Brown, J.V.E.; Barbui, C.; Churchill, R.; Lovell, K.; McMillan, D.; Gilbody, S. Psychological and pharmacological interventions for posttraumatic stress disorder and comorbid mental health problems following complex traumatic events: Systematic review and component network meta-analysis. PLoS Med. 2020, 17, e1003262. [Google Scholar] [CrossRef]
- Wawrzyniak, A.; Balawender, K. Structural and Metabolic Changes in Bone. Animals 2022, 12, 1946. [Google Scholar] [CrossRef]
- Idelevich, A.; Baron, R. Brain to Bone: What Is the Contribution of the Brain to Skeletal Homeostasis? Bone 2018, 115, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Qiao, W.; Wei, J.A.; Tao, Z.; Chen, C.; Wu, Y.; Lin, M.; Ng, K.M.C.; Zhang, L.; Yeung, K.W.; Chow, B.K.C. Secretin-Dependent Signals in the Ventromedial Hypothalamus Regulate Energy Metabolism and Bone Homeostasis in Mice. Nat. Commun. 2024, 15, 1030. [Google Scholar] [CrossRef]
- Chen, P.J.; Lu, Y.C.; Lu, S.N.; Liang, F.W.; Chuang, H.Y. Association Between Osteoporosis and Adiposity Index Reveals Nonlinearity Among Postmenopausal Women and Linearity Among Men Aged Over 50 Years. *J. Epidemiol. Glob. Health* 2024. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.; Jiang, B.; Xing, W.; Sun, J.; Greenblatt, M.B.; Zou, W. Skeletal Stem Cells: Origins, Definitions, and Functions in Bone Development and Disease. Life Med. 2022, 1, 276–293. [Google Scholar] [CrossRef]
- Xu, Y.; Xu, C.; Song, H.; Feng, X.; Ma, L.; Zhang, X.; Li, G.; Mu, C.; Tan, L.; Zhang, Z.; Liu, Z.; Luo, Z.; Yang, C. Biomimetic Bone-Periosteum Scaffold for Spatiotemporal Regulated Innervated Bone Regeneration and Therapy of Osteosarcoma. J. Nanobiotechnol. 2024, 22, 250. [Google Scholar] [CrossRef]
- Minoia, A.; et al. Bone Tissue and the Nervous System: What Do They Have in Common? Cells. 2022, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- Gisbert-Garzarán, M.; Gómez-Cerezo, M.N.; Vallet-Regí, M. Targeting Agents in Biomaterial-Mediated Bone Regeneration. Int. J. Mol. Sci. 2023, 24, 2007. [Google Scholar] [CrossRef] [PubMed]
- Ong, W.; Liu, R.W.; Makmur, A.; Low, X.Z.; Sng, W.J.; Tan, J.H.; Kumar, N.; Hallinan, J.T.P.D. Artificial Intelligence Applications for Osteoporosis Classification Using Computed Tomography. Bioengineering (Basel) 2023, 10, 1364. [Google Scholar] [CrossRef] [PubMed]
- Fricke, H.P.; Hernandez, L.L. The Serotonergic System and Bone Metabolism During Pregnancy and Lactation and the Implications of SSRI Use on the Maternal-Offspring Dyad. J. Mammary Gland Biol. Neoplasia 2023, 28, 7. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Zhang, Y.; Cao, Y.; Hu, C.H.; Zheng, C.X.; Jin, Y.; Sui, B.D. Autonomic Neural Regulation in Mediating the Brain-Bone Axis: Mechanisms and Implications for Regeneration Under Psychological Stress. QJM 2024, 117, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Indirli, R.; Lanzi, V.; Mantovani, G.; Arosio, M.; Ferrante, E. Bone Health in Functional Hypothalamic Amenorrhea: What the Endocrinologist Needs to Know. Front. Endocrinol. (Lausanne) 2022, 13, 946695. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Shao, J.; Gao, D.; Zhang, L.; Yang, F. Astrocytes in the Ventromedial Hypothalamus Involve Chronic Stress-Induced Anxiety and Bone Loss in Mice. Neural Plast. 2021, 2021, 7806370. [Google Scholar] [CrossRef]
- Ng, J.S.; Chin, K.Y. Potential Mechanisms Linking Psychological Stress to Bone Health. Int. J. Med. Sci. 2021, 18, 604–614. [Google Scholar] [CrossRef]
- Yang, F.; Liu, Y.; Chen, S.; et al. A GABAergic Neural Circuit in the Ventromedial Hypothalamus Mediates Chronic Stress-Induced Bone Loss. J. Clin. Invest. 2020, 130, 6539–6554. [Google Scholar] [CrossRef]
- Otto, E.; Knapstein, P.R.; Jahn, D.; Appelt, J.; Frosch, K.H.; Tsitsilonis, S.; Keller, J. Crosstalk of Brain and Bone—Clinical Observations and Their Molecular Bases. Int. J. Mol. Sci. 2020, 21, 4946. [Google Scholar] [CrossRef] [PubMed]
- Lopes Castro, M.M.; Nascimento, P.C.; Souza-Monteiro, D.; et al. Blood Oxidative Stress Modulates Alveolar Bone Loss in Chronically Stressed Rats. Int. J. Mol. Sci. 2020, 21, 3728. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Gao, X.; Hou, Y. Effects of Mindfulness-Based Stress Reduction Combined with Music Therapy on Pain, Anxiety, and Sleep Quality in Patients with Osteosarcoma. Braz. J. Psychiatry 2019, 41, 540–545. [Google Scholar] [CrossRef]
- Li, Q.; Zhao, Y.; Deng, D.; et al. Aggravating Effects of Psychological Stress on Ligature-Induced Periodontitis via the Involvement of Local Oxidative Damage and NF-κB Activation. Mediators Inflamm. 2022, 2022, 6447056. [Google Scholar] [CrossRef]
- Gomes, E.S.B.; Farias, L.C.; Silveira, L.H.; Jesus, C.Í.; Rocha, R.G.D.; Ramos, G.V.; Magalhães, H.T.A.T.; Brito-Júnior, M.; Santos, S.H.S.; Jham, B.C.; et al. Conditioned Fear Stress Increases Bone Resorption in Apical Periodontitis Lesions in Wistar Male Rats. Arch. Oral Biol. 2019, 97, 35–41. [Google Scholar] [CrossRef]
- Follis, S.L.; Bea, J.; Klimentidis, Y.; et al. Psychosocial stress and bone loss among postmenopausal women: results from the Women's Health Initiative. J Epidemiol Community Health 2019, 73, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Haffner-Luntzer, M.; Foertsch, S.; Fischer, V.; Prystaz, K.; Tschaffon, M.; Mödinger, Y.; Bahney, C.S.; Marcucio, R.S.; Miclau, T.; Ignatius, A.; Reber, S.O. Chronic Psychosocial Stress Compromises the Immune Response and Endochondral Ossification During Bone Fracture Healing via β-AR Signaling. Proc. Natl. Acad. Sci. U.S.A. 2019, 116, 8615–8622. [Google Scholar] [CrossRef] [PubMed]
- Foertsch, S.; Haffner-Luntzer, M.; Kroner, J.; Gross, F.; Kaiser, K.; Erber, M.; Reber, S.O.; Ignatius, A. Chronic Psychosocial Stress Disturbs Long-Bone Growth in Adolescent Mice. Dis. Model. Mech. 2017, 10, 1399–1409. [Google Scholar] [CrossRef]
- Okbay Güneş, A.; Alikaşifoğlu, M.; Şen Demirdöğen, E.; Erginöz, E.; Demir, T.; Kucur, M.; Ercan, O. The Relationship of Disordered Eating Attitudes with Stress Level, Bone Turnover Markers, and Bone Mineral Density in Obese Adolescents. J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 237–245. [Google Scholar] [CrossRef]
- Henneicke, H.; Li, J.; Kim, S.; Gasparini, S.J.; Seibel, M.J.; Zhou, H. Chronic Mild Stress Causes Bone Loss via an Osteoblast-Specific Glucocorticoid-Dependent Mechanism. Endocrinology 2017, 158, 1939–1950. [Google Scholar] [CrossRef] [PubMed]
- Kumano, H. Clin Calcium 2005, 15, 1544–1547.
- Azuma, K.; Adachi, Y.; Hayashi, H.; Kubo, K.Y. Chronic Psychological Stress as a Risk Factor of Osteoporosis. J. UOEH 2015, 37, 245–253. [Google Scholar] [CrossRef]
- Azuma, K.; Furuzawa, M.; Fujiwara, S.; Yamada, K.; Kubo, K.Y. Effects of Active Mastication on Chronic Stress-Induced Bone Loss in Mice. Int. J. Med. Sci. 2015, 12, 952–957. [Google Scholar] [CrossRef]
- Nahrendorf, M.; Swirski, F.K. Lifestyle Effects on Hematopoiesis and Atherosclerosis. Circ. Res. 2015, 116, 884–894. [Google Scholar] [CrossRef] [PubMed]
- Erez, H.B.; Weller, A.; Vaisman, N.; Kreitler, S. The Relationship of Depression, Anxiety and Stress with Low Bone Mineral Density in Post-Menopausal Women. Arch. Osteoporos. 2012, 7, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Li, Q.; Wu, S.; Sun, J.; Zhang, M.; Chen, Y.J. Psychological Stress Alters the Ultrastructure and Increases IL-1β and TNF-α in Mandibular Condylar Cartilage. Braz. J. Med. Biol. Res. 2012, 45, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Seferos, N.; Kotsiou, A.; Petsaros, S.; Rallis, G.; Tesseromatis, C. Mandibular Bone Density and Calcium Content Affected by Different Kinds of Stress in Mice. J. Musculoskelet. Neuronal Interact. 2010, 10, 231–236. [Google Scholar]
- Patterson-Buckendahl, P.; Pohorecky, L.A.; Kubovcakova, L.; Krizanova, O.; Martin, R.B.; Martinez, D.A.; Kvetnanský, R. Ethanol and Stress Activate Catech.
- García-Alfaro, P.; García, S.; Rodriguez, I.; Pascual, M.A.; Pérez-López, F.R. Association of Endogenous Hormones and Bone Mineral Density in Postmenopausal Women. J Midlife Health 2023, 14, 196–204. [Google Scholar] [CrossRef]
- Li, S.; Luo, X.; Lu, Z.; Chen, N. Association of Midnight Cortisol Level with Bone Mineral Density in Chinese Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study. Diabetes Metab Syndr Obes 2024, 17, 2943–2953. [Google Scholar] [CrossRef]
- Herbert, C. Enhancing Mental Health, Well-Being and Active Lifestyles of University Students by Means of Physical Activity and Exercise Research Programs. Front Public Health 2022, 10, 849093. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; Ryder-Burbidge, C.; McNeil, J. Physical activity, obesity and sedentary behavior in cancer etiology: epidemiologic evidence and biologic mechanisms. Mol Oncol 2021, 15, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.M.; Huang, P.; Chen, R.; Wang, Y.C. The relationship between physical activity and mental health of middle school students: the chain mediating role of negative emotions and self-efficacy. Front Psychol 2024, 15, 1415448. [Google Scholar] [CrossRef] [PubMed]
- Calcagni, E.; Elenkov, I. Stress system activity, innate and T helper cytokines, and susceptibility to immune-related diseases. Ann N Y Acad Sci 2006, 1069, 62–76. [Google Scholar] [CrossRef]
- Coletti, C.; Acosta, G.F.; Keslacy, S.; Coletti, D. Exercise-mediated reinnervation of skeletal muscle in elderly people: An update. Eur J Transl Myol 2022, 32, 10416. [Google Scholar] [CrossRef]
- Chang, X.; Xu, S.; Zhang, H. Regulation of bone health through physical exercise: Mechanisms and types. Front Endocrinol (Lausanne). 2022, 13, 1029475. [Google Scholar] [CrossRef]
- Jing, Z.; Li, Y.; Zhang, H.; et al. Tobacco toxins induce osteoporosis through ferroptosis. Redox Biol 2023, 67, 102922. [Google Scholar] [CrossRef] [PubMed]
- García-Maldonado, E.; Gallego-Narbón, A.; Zapatera, B.; Alcorta, A.; Martínez-Suárez, M.; Vaquero, M.P. Bone Remodelling, Vitamin D Status, and Lifestyle Factors in Spanish Vegans, Lacto-Ovo Vegetarians, and Omnivores. Nutrients 2024, 16, 448. [Google Scholar] [CrossRef]
- Al Hezaimi, K.; Rotstein, I.; Katz, J.; Nevins, M.; Nevins, M. Effect of Selective Serotonin Reuptake Inhibitor (Paroxetine) on Newly Formed Bone Volume: Real-Time In Vivo Micro-computed Tomographic Analysis. J Endod 2023, 49, 1495–1500. [Google Scholar] [CrossRef] [PubMed]
- Elkhenany, H.; AlOkda, A.; El-Badawy, A.; El-Badri, N. Tissue regeneration: Impact of sleep on stem cell regenerative capacity. Life Sci. 2018, 214, 51–61. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Illustrative diagram of the factors that cause emotional stress, such as a bad lifestyle (food rich in sodium, fat and lack of nutrients), alcohol, cigarettes, excessive work, non-restorative nights of sleep and a sedentary lifestyle contribute to depression and anxiety (emotional control). These factors influence the GABAergic neural circuit in the ventromedial hypothalamus (VMH), influencing bone loss induced by chronic stress. Created by Biorender.com.
Figure 1.
Illustrative diagram of the factors that cause emotional stress, such as a bad lifestyle (food rich in sodium, fat and lack of nutrients), alcohol, cigarettes, excessive work, non-restorative nights of sleep and a sedentary lifestyle contribute to depression and anxiety (emotional control). These factors influence the GABAergic neural circuit in the ventromedial hypothalamus (VMH), influencing bone loss induced by chronic stress. Created by Biorender.com.
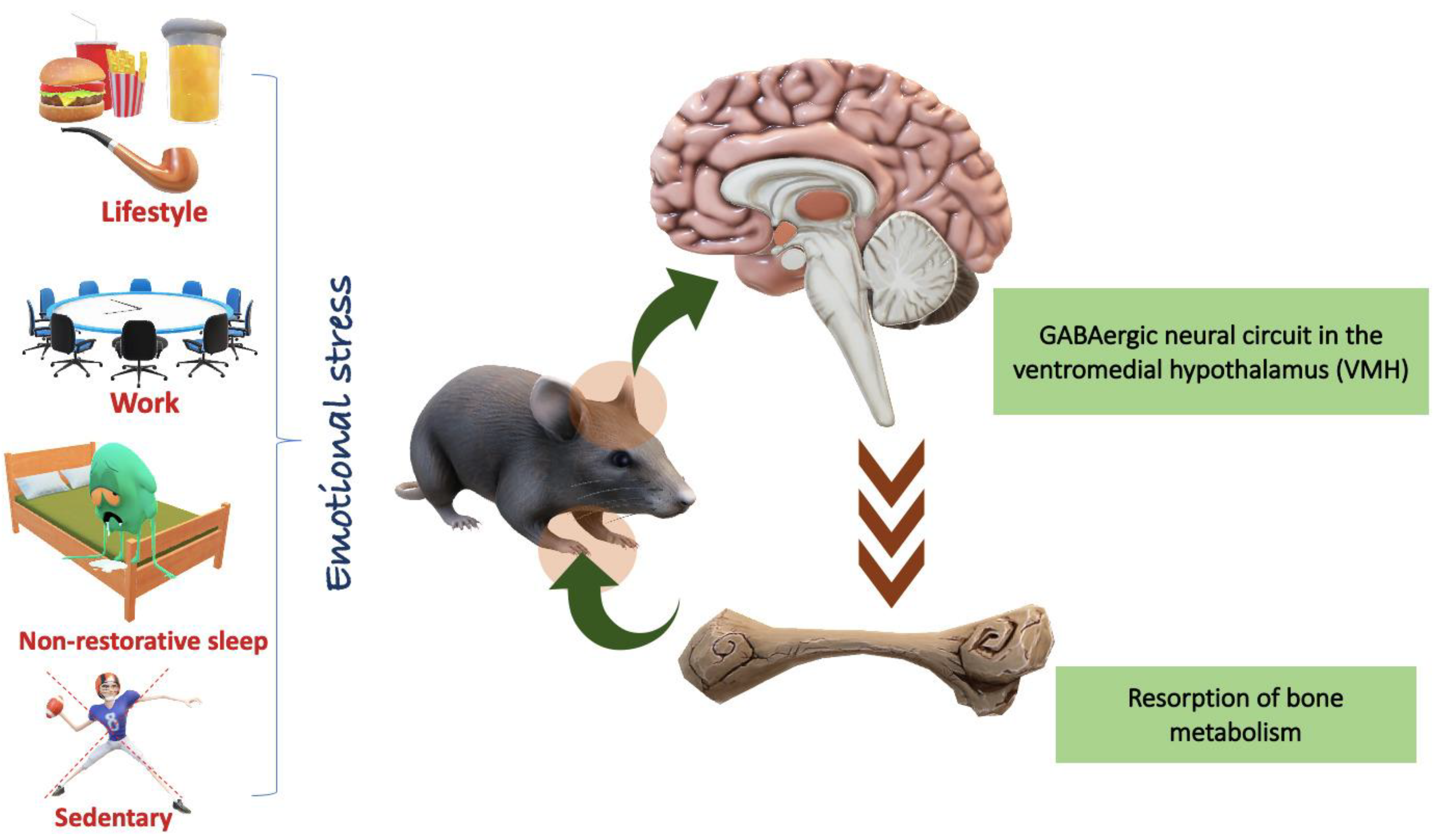
Figure 2.
Representative images of a chronic stress protocol in rat tibia. (A) Bone tissue stained with Masson's Trichrome. (B) Immunohistochemistry with osteocalcin that marks the presence of bone remodeling. (C) Immunohistochemistry with sialoprotein that marks osteoblastic activity. (D) Immunohistochemistry with tartrate-resistant acid phosphatase (TRAP) that marks osteoclast activity. Created by Biorender.com.
Figure 2.
Representative images of a chronic stress protocol in rat tibia. (A) Bone tissue stained with Masson's Trichrome. (B) Immunohistochemistry with osteocalcin that marks the presence of bone remodeling. (C) Immunohistochemistry with sialoprotein that marks osteoblastic activity. (D) Immunohistochemistry with tartrate-resistant acid phosphatase (TRAP) that marks osteoclast activity. Created by Biorender.com.
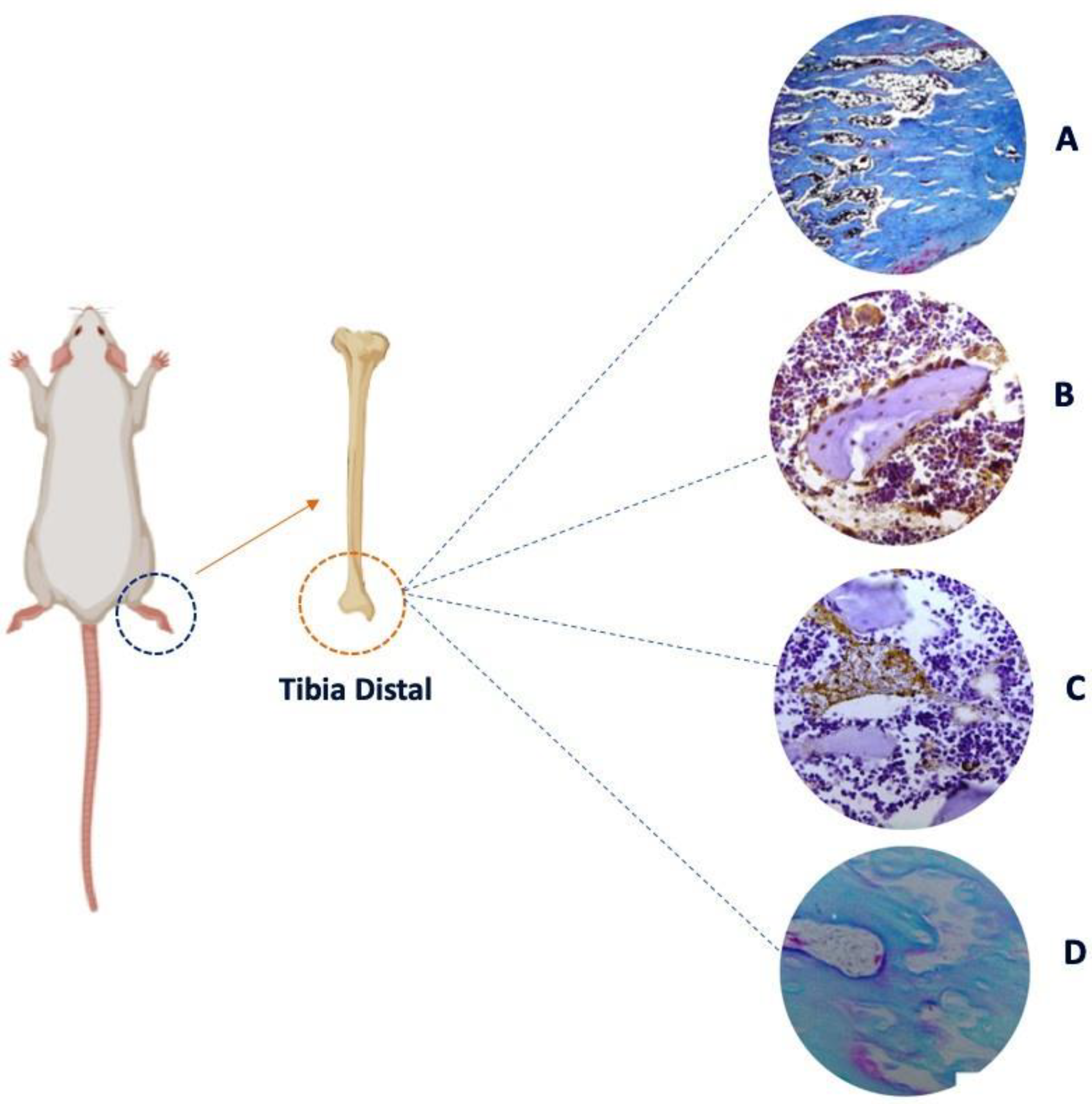

Table 1.
Relationship between emotional stress and bone resorption.
| Article title | Kind study | Authors | Year | Stress | Time | Effect |
|---|---|---|---|---|---|---|
| Autonomic neural regulation in mediating the brain-bone axis: mechanisms and implications for regeneration under psychological stress |
Review |
Ma, C et al. [56] |
2024 |
X |
X |
The autonomic neural basis of psychological stress-induced bone loss |
| Bone health in functional hypothalamic amenorrhea: What the endocrinologist needs to know |
Review |
Indirli, Rita et al. [57] |
2022 |
X |
X |
Functional hypothalamic amenorrhea causes stress and bone is severely affected |
| Astrocytes in the Ventromedial Hypothalamus Involve Chronic Stress-Induced Anxiety and Bone Loss in Mice | Experimental | Liu, Yunhui et al. [58] | 2021 | Chronic | 8 weeks | Glial-neuron microcircuit in VMH nuclei that mediates anxiety and bone loss induced by chronic stress |
| Potential mechanisms linking psychological stress to bone health | Review | Ng, Jia-Sheng, and Kok-Yong Chin [59] | 2021 | Chronic | X | Chronic psychological stress should be recognised as a risk factor of osteoporosis |
| GABAergic neural circuit in the ventromedial hypothalamus mediates chronic stress-induced bone loss | Experimental | Yang, Fan et al. [60] | 2020 | Chronic | 8 weeks | Chronic stress in crewmembers resulted in decreased bone density |
| Crosstalk of Brain and Bone—Clinical Observations and Their Molecular Bases | Review | Otto, Ellen et al. [61] | 2020 | X | X | The nervous system tightly modulates bone metabolism and regeneration |
| Blood Oxidative Stress Modulates Alveolar Bone Loss in Chronically Stressed Rats | Experimental | Lopes Castro, Micaele Maria et al. [62] | 2020 | Chronic | 30 days | Chronic stress induces oxidative blood imbalance, which can potentiate or generate morphological, structural and metabolic damage to the alveolar bone |
| Effects of mindfulness-based stress reduction combined with music therapy on pain, anxiety, and sleep quality in patients with osteosarcoma | Clinical | Liu, Haizhi et al. [63] | 2019 | Chronic | 8 weeks | Music therapy significantly alleviated clinical symptoms in patients with osteosarcoma |
| Aggravating Effects of Psychological Stress on Ligature-Induced Periodontitis via the Involvement of Local Oxidative Damage and NF- κ B Activation | Experimental | Li, Qiang et al. [64] | 2019 | Chronic | 4 weeks | Psychological stress aggravates inflammation in periodontitis tissues and leads to further activation of the nuclear factor kappa-B (NF-κB) signaling pathway |
| Conditioned fear stress increases bone resorption in apical periodontitislesions in Wistar male rats | Experimental | Gomes, Emisael Stênio Batista et al. [65] | 2019 | Chronic | 56 days | Stress caused by fear modifies a periapical lesion, increasing the size of bone loss and increasing the number of inflammatory cells |
| Psychosocial stress and bone loss among postmenopausal women: results from the Women's Health Initiative | Clinical | Follis, Shawna L et al. [66] | 2019 | Chronic | 6 years | High social stress was associated with decreased bone mineral density |
| Chronic psychosocial stress compromises the immune response and endochondral ossification during bone fracture healing via β-AR signaling | Experimental | Haffner-Luntzer, Melanie et al. [67] | 2019 | Chronic | 19 days | Chronic psychosocial stress leads to an imbalanced immune response after fracture via β-AR signaling |
| Chronic psychosocial stress disturbs long-bone growth in adolescent mice | Experimental | Foertsch, Sandra et al. [68] | 2017 | Chronic | 19 days | Chronic psychosocial stress negatively impacts endochondral ossification in the growth plate, affecting both longitudinal and appositional bone growth |
| The Relationship of Disordered Eating Attitudes with Stress Level, Bone Turnover Markers, and Bone Mineral Density in Obese Adolescents | Clinical | Okbay Güneş, Aslı et al. [69] | 2017 | X | X | Effect of stress caused by disordered eating habits harms bone remodeling |
| Chronic Mild Stress Causes Bone Loss via an Osteoblast-Specific Glucocorticoid-Dependent Mechanism | Experimental | Henneicke, Holger et al. [70] | 2017 | Chronic | 4 weeks | Bone loss during chronic stress is mediated through increased glucocorticoid signaling in osteoblasts (and osteocytes) and subsequent activation of osteoclasts |
| Osteoporosis and stress | Review | Kumano, Hiroaki. [71] | 2015 | X | X | Osteoporosis causes anxiety, depression, loss of social roles and social isolation, which leads to stress. |
| Chronic Psychological Stress as a Risk Factor of Osteoporosis | Review | Azuma, Kagaku et al. [72] | 2015 | X | X | Chronic stress activates the HPA axis and increases inflammatory cytokines, eventually leading to bone loss, inhibiting bone formation and stimulating bone resorption. |
| Effects of Active Mastication on Chronic Stress-Induced Bone Loss in Mice | Clinical | Azuma, Kagaku et al. [73] | 2015 | Chronic | 4 weeks | The stress group showed an increase in serum corticosterone levels and increased bone resorption |
| Lifestyle effects on hematopoiesis and atherosclerosis | Review | Nahrendorf, Matthias, and Filip K Swirski. [74] | 2015 | Chronic | X | Lifestyle (stress) changes the number of macrophages, diverting bone marrow production to the periphery |
| The relationship of depression, anxiety and stress with low bone mineral density in post-menopausal women | Clinical | Erez, Hany Burstein et al. [75] | 2012 | X | X | Supporting evidence for the existence of associations between mood variables and decreased bone |
| Psychological stress alters the ultrastructure and increases IL-1β and TNF-α in mandibular condylar cartilage | Experimental | Lv, Xin et al. [76] | 2012 | Chronic | 1,3 nad 5 weeks | Psychological stress increased plasma hormone levels and indicated increased expression of IL-1β and TNF-α in the TMJ |
| Mandibular bone density and calcium content affected by different kind of stress in mice | Experimental | Seferos, N et al. [77] | 2010 | Chronic | 137 days | The calcium content of the mandible and the ratio between calcium content and mandible volume was decreased |
| Ethanol and stress activate catecholamine synthesis in the adrenal: effects on bone | Experimental | Patterson-Buckendahl, Patricia et al. [78] | 2008 | Chronic | 6 weeks | Osteocalcin levels were reduced indicating inhibition of bone formation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



