
Submitted:
04 December 2024
Posted:
04 December 2024
You are already at the latest version
Abstract
Chronic lymphocytic leukemia (CLL) treatment has undergone a significant evolution with a shift from historical chemotherapeutic regimens to targeted therapies such as Bruton tyrosine kinase (BTK) and BCL-2 inhibitors. These advancements have been associated with a notable improvement in survival rates with a transformation of CLL into a chronic and manageable condition for most persons with this disease.
However, as a consequence of improved outcomes long-term CLL survivors now face emergent challenges which include a risk of infections, cardiovascular complications and secondary malignancies. In this changed scenario, holistic models of care are essential to address emergent health risks. Such models of care for CLL patients require a multidisciplinary approach that integrates CLL treatment with proactive management of frailty, comorbidities, and psychosocial well-being to enhance both survival and quality of life (QoL).
CLL predominantly affects older persons, many of whom present with concurrent frailty and comorbidities that may complicate CLL treatment and impact QoL. Comprehensive geriatric assessments (GA) may play a critical role in the identification of persons at heightened risk of treatment-related toxicity and may help guide rational therapy selection, particularly in very frail persons.
In addition to the assessment of hematological responses the prospective assessment of patient-reported outcomes (PROs) and frailty metrics may offer a more nuanced understanding of global treatment benefits. A survivorship-focused care model is crucial to address the multifaceted needs of CLL patients with the extension of patient care into the broader domain of long-term health maintenance with associated improvements in QoL.
Keywords:
CLL
; disease care
; beyond treatment
; long-survivors
; long-term monitoring
Introduction
Chronic lymphocytic leukemia (CLL) affects over 200,000 people in the United States and has is a significant public health concern, particularly amongst older persons [1]. Historically, treatment outcomes were constrained by the toxicities and limited efficacy of chemoimmunotherapy with poor prognoses for a proportion patients [2]. However, over the past decade the advent of targeted therapies such as inhibitors of Bruton tyrosine kinase (BTK) and BCL-2 has transformed the management of CLL [2]. These innovations have been associated substantial improvements in survival and shifted the natural history of the disease from an often fatal condition to a chronic, manageable illness [3,4,5].
However, despite these therapeutic advancements and improved treatment outcomes, new challenges in patient management have emerged [6,7]. Long-term survivors of CLL may experience a range of secondary health complications such as infections, cardiovascular comorbidities and psychosocial challenges which are sometimes distinct from predictable treatment-related toxicities [7]. As a result, healthcare providers must now prioritize the development of comprehensive survivorship care plans to address the evolving needs of this patient group.
The Changing Treatment Landscape of CLL: A Success Story
Before the advent of targeted therapies, patients with CLL had limited treatment options which were primarily based upon chemotherapy regimens [8,9,10]. Agents such as chlorambucil, bendamustine or fludarabine were commonly used, but these treatments offered only modest improvements in survival and were associated with significant toxicities, including prolonged myelosuppression and increased susceptibility to infection [8,9,10].
The introduction of the anti-CD20 monoclonal antibody rituximab produced a pivotal shift in CLL management [11,12,13,14]. This breakthrough led to the development of chemoimmunotherapeutic approaches, notably the combination of fludarabine, cyclophosphamide and rituximab (FCR) [11,14]. The FCR regimen produced deep and durable responses in patients who were young and fit enough to tolerate the associated toxicities and this treatment represented a significant advancement in CLL therapy. An updated analysis from the MD Anderson Cancer Center (MDACC) demonstrated that among patients with immunoglobulin heavy chain chain (IGHV)-mutated (IGHV-M) CLL, those treated with FCR experienced a median progression-free survival (PFS) of 14.6 years. Remarkably, disease progression ten years beyond therapy was rare, which suggests that a subset of patients may achieve what is referred to as a "functional cure" of their CLL [15]. However, despite these promising outcomes, FCR is associated with significant risks, most notably the development of secondary malignancies such as myelodysplastic syndromes (MDS) or acute myeloid leukemia (AML), as well as prolonged immunosuppression with associated increased infection rates [15].
As the CLL treatment landscape has evolved, recent therapeutic developments have prompted a critical reappraisal of the role of FCR, particularly in light of the advent of targeted therapies [16]. A major driver of this reevaluation was the COVID-19 pandemic, which highlighted the vulnerability of immunosuppressed patients [17,18]. FCR-induced myelosuppression is associated with impaired immune responses, reduced vaccination efficacy and a heightened risk of major infections [18]. These risks underscored the need for alternative treatment strategies that offer efficacy while minimizing immune suppression and the attendant complications.
Recent clinical trials have provided evidence in support of the superiority of targeted therapies over FCR. For example, the US ECOG-ACRIN E1912 trial demonstrated that continuous treatment with the BTK inhibitor (BTKi) ibrutinib, in combination with rituximab, resulted in a progression free survival (PFS) advantage over FCR in young, fit CLL patients, including those with IGHV-M disease. The trial also reported a five-year overall survival (OS) benefit for patients treated with ibrutinib-based therapy [19]. Similarly, the GAIA/CLL13 trial highlighted the significantly prolonged PFS with both venetoclax-obinutuzumab (VO) and ibrutinib-venetoclax-obinutuzumab in comparison to chemoimmunotherapy (FCR or BR) and venetoclax-rituximab in previously untreated, fit patients [20]. In clinical practice, FCR remains a reasonable treatment option for a subset of young, fit patients with IGHV-M CLL, especially in regions where access to targeted therapies may be limited [21].
Currently, CLL targeted therapies are the preferred treatment options in the setting of either treatment-naïve or relapsed/refractory CLL [21,22]. The use of BTKi such as ibrutinib, acalabrutinib, and zanubrutinib, or the BCL-2 inhibitor venetoclax, either as monotherapy or in combination with anti-CD20 monoclonal antibodies, has consistently been associated with superior clinical outcomes when compared to chemoimmunotherapy across various CLL patient populations, including those who are elderly or less fit [19,20,23,24,25,26,27,28,29,30,31,32,33,34,35] .
Long-term outcome and safety data for a targeted agent in elderly CLL patients have recently been presented. The final ten year analysis of the landmark RESONATE-2 trial, which compared ibrutinib to chlorambucil in elderly or unfit, previously untreated CLL patients, revealed a median PFS of 8.9 years for ibrutinib-treated patients. Notably, 27% of patients continued ibrutinib treatment for at least ten years, with a median treatment duration of 6.2 years [36].
Such findings underscore the long-term efficacy and tolerability of ibrutinib whilst also highlighting the emergence of a new cohort of CLL patients who survive well beyond their initial diagnosis. Significantly, 70% of patients treated with ibrutinib in the RESONATE-2 trial achieved the 10-year survival milestone. Additionally, combined analyses of relevant clinical trials have demonstrated considerable improvements in OS amongst previously untreated CLL patients, including those aged 65 and older [37]. This progress has substantially narrowed the survival gap between CLL patients and the general population of similar age which is a major achievement for modern medicine[38].
Challenges Faced by Long-Term CLL Survivors
As the life expectancy of persons with CLL increases, healthcare providers must address emergent issues in this populations such as secondary cancers, cardiovascular complications and the consequences of ongoing immunosuppression. Additionally, patients may experience treatment-related fatigue, neurocognitive changes, or psychological distress, all of which can significantly impact upon QoL[7].
The management of these long-term effects may require a multidisciplinary approach. In addition to the expertise of hematologists and oncologists, the involvement of other healthcare professionals—including infectious disease specialists, cardiologists, and mental health providers is often necessary. Patient counseling is crucial to help individuals navigate the complexities of living with CLL and its treatments. Support groups and resources for both patients and caregivers can also offer emotional support and practical guidance. In some cases, psychiatric care may be warranted to address anxiety, depression, or other mental health challenges that can arise during the long-term management of CLL.
The Management of CLL-Related Immune Dysfunction
The heightened risk of infection in CLL is driven by several factors which include disease-induced immune dysregulation, secondary hypogammaglobulinemia and impaired cell-mediated immunity due to T-cell dysfunction [39]. Serious infections, which may also occur in individuals with monoclonal B-cell lymphocytosis (MBL), are frequently observed in patients with symptomatic CLL. The infectious risk is further exacerbated in patients treated with targeted therapies, as such treatments can compromise immune responses [40,41].
A recent meta-analysis of clinical trials of targeted therapies in persons with CLL highlights the risk of infection across various treatment regimens, with infection rates from 13% to 45% of trial participants. The overall incidence of infection was similar between patients treated with BTKi and BCL2 inhibitors (19.8% versus 17.4%). However, amongst those treated with BTKi, the rate of severe infections was increased in those with relapsed or refractory CLL (25.8%) compared to treatment-naïve patients (16.2%)[42]. These findings emphasize the importance of vigilant infection monitoring and the implementation of robust prevention strategies for a subset of CLL patients at higher risk of developing severe infections while undergoing targeted therapies.
Although vaccine responses are impaired in patients with CLL, immunization remains a critical strategy for the prevention of infections due to the favorable risk-benefit profile of this approach when compared to other infection-preventive measures such as prophylactic antimicrobials and immunoglobulin replacement [43]. Much of the recent understanding in relation to the protective effect vaccination in persons with CLL is derived from the period of the COVID-19 pandemic [18]. In the large observational European Research Initiative on CLL (ERIC) cohort, CLL patients vaccinated against COVID-19 had lower hospitalization rates and improved OS when compared to unvaccinated individuals. However, vaccination was not identified as an independent factor influencing hospitalization or survival which indicates that other patient-related factors are likely contributors to CLL patient outcomes. Notably, older age, comorbidities, and CLL-directed treatment were identified as significant risk factors for mortality, whilst vaccination status was not [44].
The European Conference on Infections in Leukaemia (ECIL) group recommends that CLL patients receive an annual single dose of an inactivated influenza vaccine and pneumococcal vaccination, preferably administered before the commencement of CLL-directed therapy. A similar approach is recommended for herpes zoster vaccination [45]. In a recent position paper proposing a model of care for long-term survivors of CLL patients, the strength of the recommendation for influenza, pneumococcal, COVID-19, and varicella herpes zoster vaccines is classified as 'strong (class 1),' provided that inactivated vaccines are used [7].
Interestingly, amongst patients treated with ibrutinib, those who had interrupted BTK inhibitor (BTKi) treatment at the time of vaccination exhibited significantly higher antibody titers compared to those who continued their BTKi regimen [46].
Additionally, in CLL long-term survivors who respond to targeted therapies, there is evidence of immunological recovery, which may lead to improved vaccine responses. Data from patients enrolled in the RESONATE and RESONATE2 trials suggest that ibrutinib significantly restored T-cell proliferative capacity, degranulation, and cytokine secretion [47]. Preliminary evidence for the restoration of circulating adaptive and innate immune cells has also been observed in treatment-naïve CLL patients treated with fixed-duration ibrutinib venetoclax therapy in the CAPTIVATE trial [48]. These findings underscore the need for systematic efforts to improve immune-restorative interventions, especially for long-term survivors of CLL.
An early intervention trial, the PreVent-ACaLL study (NCT03868722), is currently investigating a new scoring system to identify untreated CLL patients who do not meet treatment criteria but are at high risk of infection. These patients are randomized to either observation or 12 weeks of therapy with acalabrutinib and venetoclax. The primary endpoint is the rate of grade ≥3 infection-free survival at 24 weeks, with a possible extension of the observation period to two years post-enrollment.
Persistent hypogammaglobulinemia, a hallmark of CLL regardless of disease activity, is strongly associated with an increased risk of infection [49]. Immunoglobulin replacement therapy with polyvalent human immunoglobulin G (IgG) is recommended for patients experiencing recurrent severe bacterial infections and with low IgG levels [50]. A meta-analysis of randomized clinical trials in patients with hematologic malignancies and hypogammaglobulinemia demonstrated that immunoglobulin replacement therapy reduced the incidence of clinically documented infections but did not prevent microbiologically documented infections or infection-related deaths [51].
Cardiovascular Complications of BTKis: Risks and Management
CLL primarily affects older adults, with a median age at diagnosis of 72 years [2]. In this demographic group there is a relatively high prevalence of cardiovascular disease (CVD) compared to younger populations. Before the introduction of BTKi therapy, studies indicated that approximately one-third of CLL patients presented with significant CVD at diagnosis and treatment initiation [52,53]. This is concerning, as BTKis may further elevate the risk of cardiovascular events, particularly in those with pre-existing CVD [54]. A recent single-center study suggests that patients with pre-existing CVD have significantly higher odds of experiencing new or worsening atrial fibrillation (AF). This association persisted even after adjusting for comorbidities, the type of BTKi, and baseline medications. These findings underscore the importance of standardized strategies to prevent and promptly detect CVAEs during BTKi treatment, particularly in patients with pre-existing CVD [55].
Early clinical trials highlighted the association between hypertension and atrial arrhythmias with exposure to the BTKi ibrutinib [56]. In a large cohort of CLL patients (n=4,958), those treated with ibrutinib (6% of the cohort) experienced a 1.91-fold increased risk of stroke and a 3.65-fold increased risk of AF. A pooled analysis of four randomized controlled trials revealed that the incidence of AF was 6.5% in the ibrutinib group compared to 1.6% in the comparator group, with a median time to AF onset of 2.8 months (range: 0.3-26.6 months).
Amongst patients with lymphoid malignancies treated with ibrutinib, the incidence of hypertension was reported to be nearly 72%. Notably, the development of new or worsened hypertension following the initiation of ibrutinib is associated with more than a twofold increase in the risk of other cardiac events [57].
Three phase 3 trials which compared ibrutinib with the second-generation BTK inhibitors acalabrutinib or zanubrutinib, have been conducted [58,59,60]. Both acalabrutinib and zanubrutinib consistently demonstrated a two- to four-fold reduction in the risk of AF compared to ibrutinib [59,60]. Additionally, acalabrutinib was associated with significantly lower rates of hypertension (9% versus 23% with ibrutinib) [58]. While hypertension rates were similar across patients enrolled in the ALPINE study (24% with zanubrutinib vs. 23% with ibrutinib), they were quantitatively lower with zanubrutinib in the ASPEN trial which enrolled patients with Waldenström macroglobulinemia (15% vs. 26% with ibrutinib) [59,60]. Interestingly, in the ALPINE trial mean changes from baseline in systolic blood pressure over time were generally lower in patients treated with zanubrutinib vs ibrutinib [61]. In these studies treatment with antihypertensive medications was linked to a decrease in major adverse cardiovascular events [54].
Ventricular arrhythmias (VAs) and sudden death have emerged as potential class-wide side effects of BTK inhibitors. Ibrutinib is associated with an incidence of VAs of 0.6 to 0.8 per 100 person-years, whereas acalabrutinib and zanubrutinib have reported rates of 0.4 and 0.1 per 100 person-years, respectively. However, the rarity of these events and the limited data on newer agents make these statistics uncertain, emphasizing the need for ongoing monitoring and follow-up [62,63,64].
In early clinical trials of BTKi therapy heart failure was not found to be a complication of treatment. However, recent data from pooled long-term follow-ups of several later-phase ibrutinib trials suggest a potential increased risk of heart failure. In these analyses, heart failure was reported in up to 5% of patients, often emerging years after the commencement of treatment [64]. In a large retrospective study involving 860 patients treated with ibrutinib for CLL, a significantly higher risk of developing heart failure was identified compared to chemotherapy treatment (7.7% vs 3.6%)[65]. Similarly, a pharmacovigilance database study on ibrutinib indicated a more than three-fold increase in the reported odds of heart failure compared to all other drugs in the database [66].
For the second-generation BTKis limited long-term follow-up precludes an estimation of the risk of heart failure which generally occurs after prolonged drug exposure. In a pooled analysis of 760 patients treated with acalabrutinib, less than 1% experienced any grade of symptomatic congestive heart failure [67]. Evidence concerning heart failure associated with other next-generation agents, including reversible BTK inhibitors, is very limited due to the infrequent reporting of this outcome.
In conclusion, when selecting a BTKi, it is important to take the patient's cardiac risk profile into account, especially for those with pre-existing cardiovascular risk factors. Proactive management of modifiable cardiovascular risks and routine monitoring for cardiac toxicity related to the treatment should be implemented for all patients [68]. Of note, BTKi treatment should be avoided in patients with a history of heart failure, history of ventricular arrhythmias, or uncontrolled hypertension [69].
Second Primary Malignancies: Prevalence and Implications for Screening and Long-Term Care
The development of second primary malignancies (SPMs) is associated with increased morbidity amongst CLL patients [70]. A population-based study in the Netherlands demonstrated that CLL patients face a 63% higher risk of developing a SPM compared to an age- and sex-matched population. This increased risk includes both solid tumors and hematological malignancies, with the highest incidence occurring more than five years after CLL diagnosis. The spectrum of SPMs in CLL is broad and squamous cell carcinoma of the skin, melanoma, lung cancer, colorectal cancer, soft-tissue sarcoma, acute myeloid leukemia (AML), and thyroid cancer are the most commonly observed disorders [71].
In a recent international retrospective study of 19,705 CLL patients, 4,134 (21%) developed a second malignancy. Of these, 3,088 patients (15.7%) were diagnosed with one or more solid tumors, 834 patients (4.2%) developed a secondary hematological malignancy and 212 patients (1%) had both types. The median time from CLL diagnosis to the development of a secondary hematological malignancy was 4.7 years. Amongst secondary hematological malignancies, the most prevalent were myelodysplastic syndromes (MDS) (0.4%), AML (0.2%) and myeloma (0.13%). Solid tumors developed at a median of 4.4 years (interquartile range, 2.0–7.6 years) after CLL diagnosis, with non-melanoma skin and prostate cancers being the most common, followed by colorectal (1.9%) and breast cancers (1.7%)[72].
Patients with CLL who developed a SPM had inferior survival when compared to those without a second malignancy. Secondary AML and MDS were associated with the poorest survival outcomes. The FCR regimen was associated with an increased risk of AML and MDS, whereas patients treated exclusively with newer agents such as BTKi or venetoclax were not noted to develop these disorders [72]. These results align with findings from the German CLL Study Group (GCLLSG) registry, which demonstrated a higher-than-expected incidence of hematological SPMs in treated versus untreated CLL patients, likely due to fludarabine-based therapies [73].
Recent studies suggest that among patients treated with Bruton’s tyrosine kinase inhibitors (BTKis), the spectrum of SPMs is similar to that observed following chemotherapy or chemoimmunotherapy [74,75]. However, extended follow-up is necessary to fully understand the impact of targeted CLL treatments on the risk of secondary malignancies.
Since therapy with targeted agents has improved life expectancy for CLL patients, the long-term risk of developing SPMs will also increase as a function of increased longevity. Therefore a structured SPM screening program should be offered. These patients should be eligible for annual skin examinations, and screening for colon, breast, cervical and prostate cancers. Smoking cessation counseling and lung cancer screening should also be included in long-term care plans [7].
Bone Health in CLL: Addressing Fracture Risk and the Potential of BTK Inhibitors
Recent evidence suggests an interaction between bone tissue and CLL cells [76]. Abnormalities of bone metabolism in CLL are associated with elevated serum levels of tumor necrosis factor α, interleukin-6, interleukin-8, and chemokine (C-C motif) ligand 3 (CCL3) [77,78,79].
These abnormalities are also associated with the increased expression of the receptor activator of nuclear factor κ-B ligand (RANKL) and vitamin D insufficiency [80,81]. Of note, changes in bone metabolism contribute to a higher risk of axial fragility fractures, even in patients without osteoporosis [76].
A retrospective case-control study using the Surveillance, Epidemiology, and End Results (SEER) registry linked to Medicare which included 16,344 cases of CLL, reported a13% incidence of fractures. Notably, the increased fracture risk amongst CLL patients is specific to axial fractures, which supports the concept that cell-cell interactions between leukemic infiltrates and the bone marrow microenvironment may weaken the marrow-rich cancellous bone whilst sparing cortical bone [76].
The increased fracture risk in CLL highlights the need for preventive measures focused on bone health in addition to monitoring of bone mineral density in both asymptomatic and symptomatic CLL patients. A comprehensive approach could include osteoporosis prevention strategies such as calcium and vitamin D supplementation and regular exercise [7]. Accumulating evidence indicates that vitamin D insufficiency affects approximately 30% of CLL patients. Importantly, vitamin D deficiency has been associated with an increased risk of progression of early stage CLL to a symptomatic phase [82]. Finally, for CLL patients with signs of osteoporosis on bone densitometry early initiation of antiresorptive therapy is recommended [7].
Recent data suggests that second-generation Bruton's tyrosine kinase (BTK) inhibitors, such as acalabrutinib and tirabrutinib, may inhibit osteoclast formation by the inhibition of RANKL-induced osteoclast differentiation [83,84]. With the growing clinical use of these second-generation BTK inhibitors, there could be a potential for a reduced risk of bone fractures in CLL patients in response to these agents [85].
Managing Frailty in CLL
CLL patients are typically above 70 years old and often have comorbidities such as reduced mobility, cognitive impairment, and psychological disorders [86]. These age-related comorbidities are associated with negative health outcomes. In CLL it has been suggest that prospective evaluation of markers of frailty should be performed to identify those wo are at risk of treatment toxicity [87].
Recent data suggests that targeted therapies for CLL may improve frailty in older adults which implies that frailty is a dynamic condition with elements of reversibility [88]. HOVON139/GiVe has been the first trial to comprehensively examine geriatric assessments (GA) and frailty in the context of modern targeted CLL therapy. This study which included frail patients treated with the venetoclax-obinutuzumab combination did not fully address questions in relation to the benefits of targeted therapy in the most elderly population (≥80 years) [89]. In a retrospective analysis of CLL patients older than 80 years old who received ibrutinib the median PFS and OS were 42.5 and 51.8 months, respectively and 22.8% experienced a cardiovascular event [90]. The CLL-Frail trial prospectively evaluated the efficacy and safety of acalabrutinib monotherapy in patients ≥80 years of age and/or a FRAIL scale score of ≥3. The first interim analysis of this international phase II study of the evaluation of acalabrutinib in the elderly frail CLL population did not show any unexpected safety signals. At a median observation times of eight months, 21 patients remained on therapy. Reasons for discontinuation were adverse events in five (56%) and death and withdrawn consent in two (22%) patients each, respectively [91].
These findings highlight two key priorities for clinical trials of elderly frail CLL patients. Firstly, baseline evaluations should incorporate geriatric assessments (GA) to measure frailty and other age-related comorbidities, alongside traditional metrics such as chronological age, Eastern Cooperative Oncology Group Performance Status (ECOG PS), and general illness severity scales. This multi-dimensional approach can provide a clearer picture of an older patient's health status and suitability for various therapies [92].
Next, tracking outcomes related to frailty and quality of life, in addition to standard hematologic response metrics, is essential. This enables a more holistic understanding of how treatments impact upon patients’ overall well-being and functionality in addition to their cancer status. Alterations in frailty should be regularly assessed and reported, as such changes can be as important to patients’ quality of life as hematologic outcomes [93].
Without these measures, important benefits of modern CLL therapies could be missed, particularly those that might impact on frailty and sometimes improve overall function in older adults. Furthermore, the incorporation of GA into routine clinical practice could facilitate the identification of patients who may be at heightened risk of drug-related toxicities [94].
Finally, societal factors such as the absence of a caregiver, distance from the hematology center, and socio-economic factors, may pose barriers to achieving health equity in the management of frail CLL patients. All of these sociodemographic factors should be considered when selecting the most appropriate therapy to ensure improved treatment outcomes [95,96].
Enhancing Quality of Life for CLL Patients
Individuals with CLL report lower QoL across most domains when compared to their healthy counterparts [97]. Levels of depression, anxiety, and overall QoL are comparable between patients under watchful waiting and those who are actively treated [98]. However, younger patients managed with a watchful waiting approach often experience depression, diminished emotional and social QoL, and heightened anxiety whilst older patients tend to report poorer function in physical QoL domains [99].
Routine screening for emotional QoL elements is essential for all patients. Recommended tools to facilitate such assessments include the Geriatric Depression Scale (GDS)-5 and the PROMIS-Anxiety 4-item questionnaire, though alternative screening tools may also be appropriate. Access to psychosocial support from psychologists is critical, irrespective of treatment status [100]. Furthermore, the psychosocial burden on families and caregivers is frequently overlooked and warrants consistent communication and personalized support.
Effective CLL management requires a multidisciplinary, patient- and family-centered approach that addresses both physical and emotional well-being [101]. The shift from chemotherapy to targeted agents has favorably impacted the QoL of persons with CLL [99]. A recent study suggests that ibrutinib-treated patients receiving had better QoL and treatment satisfaction compared to patients receiving chemo-immunotherapy, irrespective of line of therapy [102]. The improvement of QoL observed with ibrutinib was also noted with second-generation BTKi. Patients with R/R CLL treated with zanubrutinib in the context of ALPINE trial demonstrated improvements in the global health status compared to ibrutinib treated patients [103]. Frontline fixed-duration VO improves overall patient reported outcomes (PROs) in older, unfit patients with CLL with and without geriatric impairments. The improvement was based on patients' HRQoL, as measured by Patient-Reported Outcomes (PROs). These included assessments of function, depression, cognition, nutrition, physical performance, muscle parameters, and comorbidities, along with evaluations using the European Organization for Research and Treatment of Cancer (EORTC) C30 and CLL17 questionnaires. [89].
Finally, anticipated improvements in clinical outcomes rarely fully translate into tangible, patient-centered benefits. Results from an exploratory cross-sectional quantitative survey assessing the quality of relationships between physicians, nurses, and patients, the impact of CLL on daily life, and patient satisfaction with care management suggest significant areas for improvement in these fields [104] . Future studies in CLL should prioritize patient needs, particularly psychosocial and behavioral factors, and focus on improving communication and shared decision-making.
Conclusions
Advancements in therapies specifically targeting CLL have significantly improved patient outcomes, offering promising prospects for extended survival [37,38,105]. However, it is becoming increasingly clear that improving survival rates for CLL patients will not solely depend on innovations in disease-directed treatments. Instead, the focus must expand to address competing causes of mortality that affect this patient population [106].
While progress in CLL treatment continues to evolve, there is a growing recognition that CLL patients are at elevated risk for comorbidities and complications that substantially impact their overall health and survival . These include cardiovascular disease, infections, SPMs and other health conditions not directly related to the leukemia itself [107]. To optimize long-term outcomes, it is essential to shift toward a more comprehensive model of care that goes beyond managing the malignancy alone. This model, grounded in the principles of survivorship, would incorporate proactive monitoring and management of these additional health risks, especially in long-term survivors [7]. Key components of this model would include regular surveillance for comorbidities, preventive healthcare strategies, and individualized interventions aimed at mitigating the risks associated with non-CLL-related factors. This broader focus requires a collaborative, multidisciplinary approach to care, involving oncologists, cardiologists, geriatric specialists, infectious disease experts, and other healthcare providers.
In this model, care would be tailored to each patient's unique needs, acknowledging the varied challenges they face as CLL survivors. Emphasizing the integration of personalized care plans, which address not only CLL but also the full spectrum of health risks, will be critical in improving both the survival and the quality of life of these patients [7]. By embracing this holistic, patient-centered approach, we can ensure that CLL patients live not only longer, but also healthier lives [108].
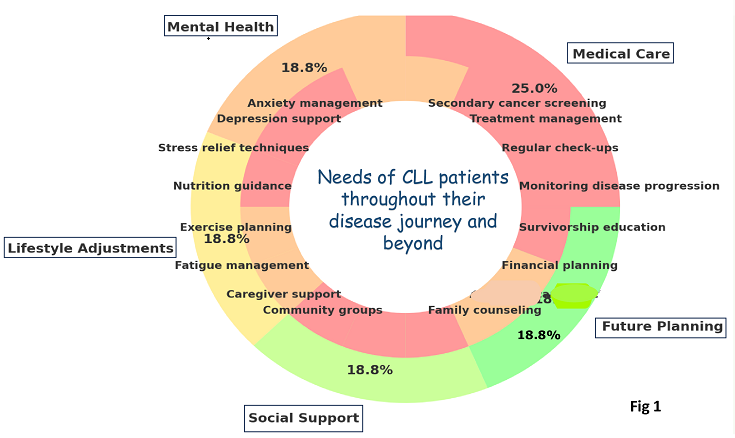
Figure 1.
A conceptual graph illustrating the needs of CLL patients throughout their disease journey and beyond, with a particular emphasis on long-term survivors. The outer ring highlights the primary categories of survivor care, while the inner ring provides a detailed breakdown of specific components within each category.
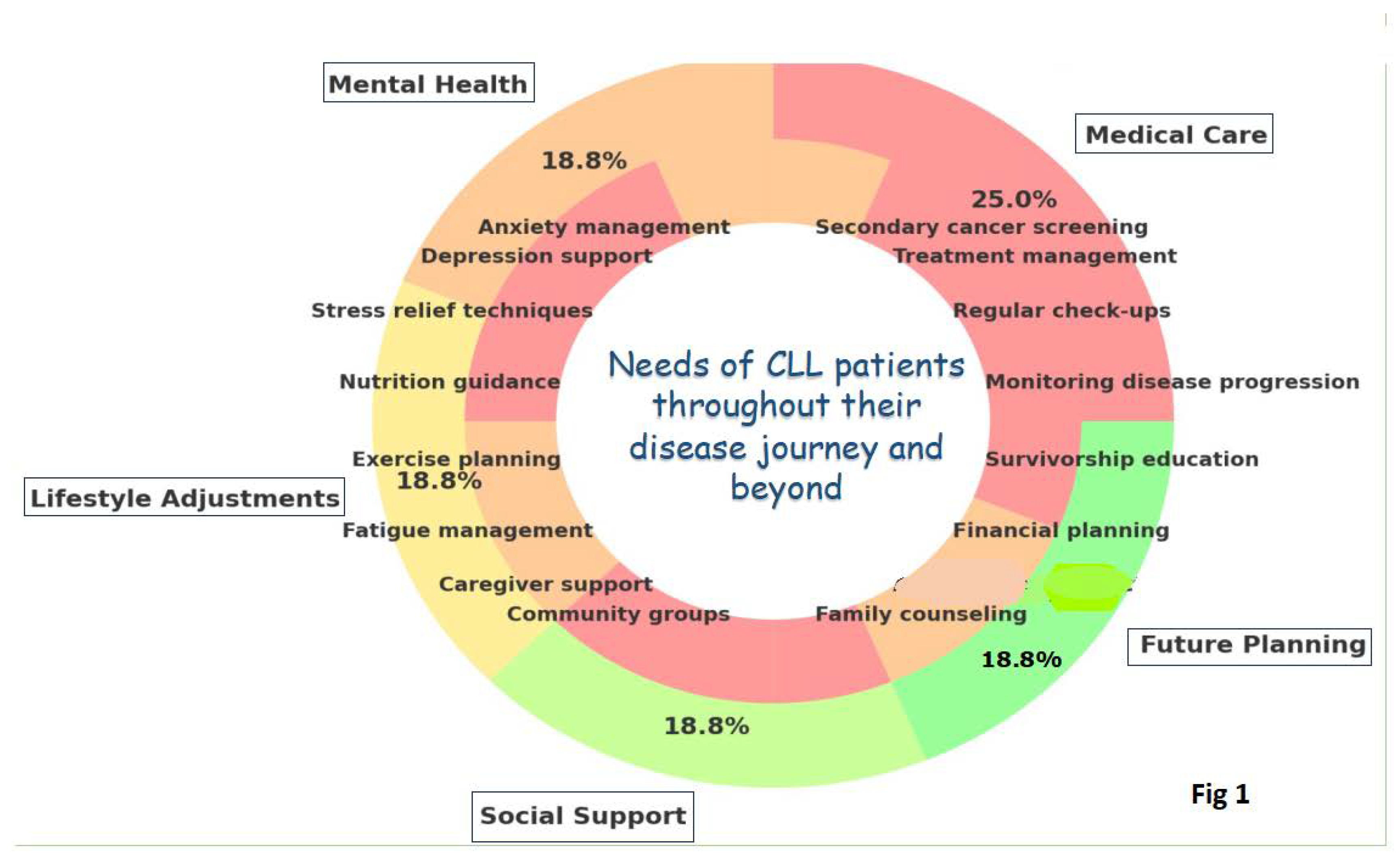
Figure 1.
A conceptual graph illustrating the needs of CLL patients throughout their disease journey and beyond, with a particular emphasis on long-term survivors. The outer ring highlights the primary categories of survivor care, while the inner ring provides a detailed breakdown of specific components within each category.
Funding
This research received no external funding.
Data Availability Statement
Data available on request from the authors.
Conflicts of Interest
S.M. received honoraria from Janssen, Abbvie, and AstraZeneca. D.A. received honoraria from Gilead, Roche, CSL Behring and Sobi.
References
- SEER*Explorer: An Interactive Website for SEER Cancer Statistics. Surveillance Research Program, National Cancer Institute; 2023. https://seer.cancer.gov/statistics-network/explorer/. Data source(s): SEER Incidence Data, November 2022 Submission (1975-2020), SEER 22 registries.
- Jain N, Wierda WG, O'Brien S Chronic lymphocytic leukaemia. Lancet. 2024, 404, 694–706. [CrossRef] [PubMed]
- Hemminki K, Hemminki J, Försti A, et al: Survival trends in hematological malignancies in the Nordic countries through 50 years. Blood Cancer J 2022, 12, 150. [CrossRef]
- van der Straten L, Maas C, Levin MD, et al: Long-term trends in the loss in expectation of life after a diagnosis of chronic lymphocytic leukemia: A population-based study in the Netherlands, 1989-2018. Blood Cancer J 2022, 12, 72. [CrossRef]
- Kajuter H, Wellmann I, Khil L, et al: Survival of patients with chronic lymphocytic leukemia before and after the introduction of chemoimmunotherapy in Germany. Blood Cancer J 2021, 11, 174. [CrossRef] [PubMed]
- Wang Y, Achenbach SJ, Rabe KG, et al: Cause of death in patients with newly diagnosed chronic lymphocytic leukemia (CLL) stratified by the CLL-International Prognostic Index. Blood Cancer J 2021, 11, 140. [CrossRef] [PubMed]
- Fedele PL, Opat S. Chronic Lymphocytic Leukemia: Time to Care for the Survivors. J Clin Oncol. 2024, 42, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Catovsky D, Richards S, Matutes E, et al. Assessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukaemia (the LRF CLL4 Trial): a randomised controlled trial. Lancet 2007, 370, 230–239. [Google Scholar] [CrossRef]
- Eichhorst BF Busch R, Hopfinger G, et al. Fludarabine plus cyclophosphamide versus fludarabine alone in first-line therapy of younger patients with chronic lymphocytic leukemia. Blood 2006, 107, 885–891. [Google Scholar]
- Flinn IW, Neuberg DS. , Grever MR et al. Phase III trial of fludarabine plus cyclophosphamide compared with fludarabine for patients with previously untreated chronic lymphocytic leukemia: US Intergroup Trial E2997. J Clin Oncol 2007, 25, 793–798. [Google Scholar] [CrossRef]
- Fischer K, Bahlo J, Fink AM, et al. Long-term remissions after FCR chemoimmunotherapy in previously untreated patients with CLL: updated results of the CLL8 trial. Blood. 2016, 127, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Fischer K, Cramer P, Busch R, et al. Bendamustine in combination with rituximab for previously untreated patients with chronic lymphocytic leukemia: a multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol. 2012, 30, 3209–3216. [Google Scholar] [CrossRef] [PubMed]
- Goede V, Fischer K, Busch R, et al Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med 2014, 370, 1101–1110. [CrossRef] [PubMed]
- Hallek M, Fischer K, Fingerle-Rowson G, et al Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet 2010, 376, 1164–1174. [CrossRef]
- Thompson PA, Bazinet A, Wierda WG, et al Sustained remissions in CLL after frontline FCR treatment with very-long-term follow-up. Blood 2023, 142, 1784–1788. [CrossRef]
- Davids, MS. Functional cure reported in CLL. Blood 2023, 142, 1761–1763. [Google Scholar] [CrossRef] [PubMed]
- Scarfò L, Chatzikonstantinou T, Rigolin GM, et al COVID-19 severity and mortality in patients with chronic lymphocytic leukemia: a joint study by ERIC, the European Research Initiative on CLL, and CLL Campus. Leukemia 2020, 34, 2354–2363. [CrossRef]
- Molica S, Tam C, Polliack A. Current perspectives regarding SARS-CoV-2 vaccination in chronic lymphocytic leukemia. Hematol Oncol 2022, 40, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt TD, Wang XV, Hanson CA, et al Long-term outcomes for ibrutinib-rituximab and chemoimmunotherapy in CLL: updated results of the E1912 trial. Blood 2022, 140, 112–120. [CrossRef]
- Eichhorst B, Niemann CU, Kater AP, et al First-Line Venetoclax Combinations in Chronic Lymphocytic Leukemia. N Engl J Med 2023, 388, 1739–1754. [CrossRef] [PubMed]
- Eichhorst B, Ghia P, Niemann CU, et al ESMO Clinical Practice Guideline interim update on new targeted therapies in the first line and at relapse of chronic lymphocytic leukaemia. Ann Oncol 2024, 35, 762–768. [CrossRef]
- https://www.nccn.org/professionals/physician_gls/pdf/cll.pdf NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Version 1.2025 — October 1, 2024 Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma.
- Burger JA, Tedeschi A, Barr PM, et al. Ibrutinib as initial therapy for patients with chronic lymphocytic leukemia. N Engl J Med 2015, 373, 2425–2437. [Google Scholar] [CrossRef] [PubMed]
- Barr PM, Owen C, Robak T, et al. Up to 8-year follow-up from RESONATE-2: first-line ibrutinib treatment for patients withchronic lymphocytic leukemia. Blood Adv 2022, 6, 3440–3450. [Google Scholar] [CrossRef] [PubMed]
- Moreno C, Greil R, Demirkan F, et al. Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in firstline treatment of chronic lymphocytic leukaemia (iLLUMINATE): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 2019, 20, 43–56. [Google Scholar] [CrossRef]
- Moreno C, Greil R, Demirkan F, et al. First-line treatment of chronic lymphocytic leukemia with ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab: final analysis of the randomized,phase III iLLUMINATE trial. Haematologica 2022, 107, 2108–2020. [Google Scholar] [CrossRef] [PubMed]
- Woyach JA, Ruppert AS, Heerema NA, et al. Ibrutinib regimens versu chemoimmunotherapy in older patients with untreated CLL. N Engl J Med 2018, 379, 2517–2528. [Google Scholar] [CrossRef] [PubMed]
- Woyach JA, Ruppert AS, Heerema NA, et al. Long-term results of Alliance A041202 show continued advantage of ibrutinib-based regimens compared with bendamustine plus rituximab (BR) chemoimmunotherapy. Blood 2024, 143, 1616–1627. [Google Scholar]
- Shanafelt TD, Wang XV, Kay NE, et al. Ibrutinib-rituximab or chemoimmunotherapy for chronic lymphocytic leukemia. N Engl J Med 2019, 381, 432–443. [Google Scholar] [CrossRef]
- Sharman JP, Egyed M, Jurczak W, et al. Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzumab for treatment-naive chronic lymphocytic leukaemia (ELEVATE TN): a randomised, controlled, phase 3 trial. Lancet 2020, 395, 1278–1291. [Google Scholar] [CrossRef] [PubMed]
- Sharman JP, Egyed M, Jurczak W, et al. Acalabrutinib ± obinutuzumab vs obinutuzumab + chlorambucil in treatment-naïve chronic lymphocytic leukemia: 6-year follow-up of Elevate-TN. Blood 2023, 142 (Suppl. 1). [Google Scholar]
- Tam CS, Brown JR, Kahl BS, et al. Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and smalllymphocytic lymphoma (SEQUOIA): a randomised, controlled,phase 3 trial. Lancet Oncol 2022, 23, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and Obinutuzumab in patients with CLL and coexisting conditions. N Engl J Med 2019, 380, 2225–2236. [Google Scholar] [CrossRef]
- Munir T, Cairns DA, Bloor A, et al. Chronic lymphocytic leukemia therapy guided by measurable residual disease. N Engl J Med 2024, 390, 326–337. [Google Scholar] [CrossRef]
- Al-Sawaf O, Zhang C, Jin HY, et al. Transcriptomic profiles and 5-year results from the randomized CLL14 study of venetoclax plus obinutuzumab versus chlorambucil plus obinutuzumab in chronic lymphocytic leukemia. Nat Commun 2023, 14, 2147–2156. [Google Scholar] [CrossRef]
- Burger J, Barr P, Robak T, et al Final Analysis of the RESONATE-2 Study: Up to 10 Years of Follow-Up of First-Line Ibrutinib Treatment in Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. Clin Lymphoma Myeloma Leukemia Volume 2024, 24 (Suppl. 1), S1–S678.
- Ghia P, Owen C, Allan JN, et al. First-line ibrutinib treatment in patients with chronic lymphocytic leukemia is associated with overall survival rates similar to those of an age-matched general population: A pooled post hoc analysis. Hemasphere. 2024, 8, e74. [Google Scholar] [CrossRef] [PubMed]
- Molica S, Shanafelt T, Allsup D, et al. Impact of targeted agents on survival of CLL patients age > 65 relative to age and sex matched population. Am J Hematol. 2023, 99, 480–483. [Google Scholar]
- Forconi F, Moss P. Perturbation of the normal immune system in patients with CLL. Blood. 2015, 126, 573–581. [Google Scholar] [CrossRef]
- Moreira J, Rabe KG, Cerhan JR, et al Infectious complications among individuals with clinical monoclonal B-cell lymphocytosis (MBL): a cohort study of newly diagnosed cases compared to controls. Leukemia 2013, 27, 136–141. [CrossRef]
- Galitzia A, Maccaferri M, Mauro FR, et al Chronic Lymphocytic Leukemia: Management of Adverse Events in the Era of Targeted Agents. Cancers (Basel). 2024, 16, 1996. [CrossRef]
- Vassilopoulos S, Shehadeh F, Kalligeros M, et al Targeted therapies in CLL/SLL and the cumulative incidence of infection: A systematic review and meta-analysis. Front Pharmacol 2022, 13, 989830. [CrossRef]
- Chong EA, Kumashie KG, Chong ER, et al Immunologic Predictors of Vaccine Responsiveness in Patients With Lymphoma and Chronic Lymphocytic Leukemia. J Infect Dis 2024, 230, 15–27. [CrossRef] [PubMed]
- Visentin A, Chatzikonstantinou T, Scarfò L, et al The evolving landscape of COVID-19 and post-COVID condition in patients with chronic lymphocytic leukemia: A study by ERIC, the European research initiative on CLL. Am J Hematol 2023, 98, 1856–1868. [CrossRef]
- Mikulska M, Cesaro S, de Lavallade H, et al: Vaccination of patients with haematological malignancies who did not have transplantations: Guidelines from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis 2019, 19, e188–e199. [CrossRef]
- Tomasulo E, Paul S, Mu R, et al Interruption of BTK inhibitor improves response to SARS-CoV-2 booster vaccination in patients with CLL. Leuk Lymphoma. 2023, 64, 2306–2315. [CrossRef] [PubMed]
- Solman IG, Blum LK, Hoh HY, et al Ibrutinib restores immune cell numbers and function in first-line and relapsed/refractory chronic lymphocytic leukemia. Leuk Res 2020, 97, 106432. [CrossRef]
- Moreno C, Solman IG, Tam CS, et al Immune restoration with ibrutinib plus venetoclax in first-line chronic lymphocytic leukemia: the phase 2 CAPTIVATE study. Blood Adv 2023, 7, 5294–5303. [CrossRef] [PubMed]
- Parikh SA, Leis JF, Chaffee KG, et al Hypogammaglobulinemia in newly diagnosed chronic lymphocytic leukemia: Natural history, clinical correlates, and outcomes. Cancer 2015, 121, 2883–2891. [CrossRef]
- Khan S, Allsup D, Molica S. An updated perspective on immunoglobulin replacement in chronic lymphocytic leukaemia in the era of targeted therapies. Front Oncol 2023, 13, 1135812. [Google Scholar] [CrossRef]
- Chai KL, Wong J, Weinkove R, et al Interventions to reduce infections in patients with hematological malignancies: a systematic review and meta-analysis. Blood Adv 2023, 7, 20–31. [CrossRef]
- Larsson K, Mattsson M, Ebrahim F, et al: High prevalence and incidence of cardiovascular disease in chronic lymphocytic leukaemia: A nationwide population-based study. Br J Haematol 2020, 190, e245–e248.
- Larsson K, Soderling J, Hoglund M, et al: Cardiovascular disease in patients with chronic lymphocytic leukemia: A Swedish nationwide register study with matched comparators. Am J Hematol 2022, 97, E255–E257.
- Dickerson T, Wiczer T, Waller A, et al Hypertension and incident cardiovascular events following ibrutinib initiation. Blood 2019, 134, 1919–1928. [CrossRef]
- Fernandez Turizo MJ, Kim E, Zhang C, et al Pre-existing cardiovascular disease is associated with an increased risk of cardiovascular events during Bruton tyrosine kinase inhibitor therapy. Oncologist 2024, oyae229. [CrossRef] [PubMed]
- Brown JR, Moslehi J, O'Brien S, et al. Characterization of atrial fibrillation adverse events reported in ibrutinib randomized controlled registration trials. Haematologica. 2017, 102, 1796–1805. [Google Scholar] [CrossRef] [PubMed]
- Diamond A, Bensken WP, Vu L, et al Ibrutinib Is Associated With Increased Cardiovascular Events and Major Bleeding in Older CLL Patients. JACC CardioOncol. 2023, 5, 233–243. [CrossRef] [PubMed]
- Byrd JC, Hillmen P, Ghia P, et al. Acalabrutinib versus ibrutinib in previously treated chronic lymphocytic leukemia: results of the first randomized phase III trial. J Clin Oncol. 2021, 39, 3441–3452. [Google Scholar] [CrossRef] [PubMed]
- Tam CS, Opat S, D'Sa S, et al. A randomized phase 3 trial of zanubrutinib vs ibrutinib in symptomatic Waldenström macroglobulinemia: the ASPEN study. Blood. 2020, 136, 2038–2050. [Google Scholar] [CrossRef]
- Brown JR, Eichhorst B, Hillmen P, et al. Zanubrutinib or ibrutinib in relapsed or refractory chronic lymphocytic leukemia. N Engl J Med. 2023, 388, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Brown JR, Eichhorst B, Lamanna N, et al Sustained Benefit of Zanubrutinib vs Ibrutinib in Patients With R/R CLL/SLL: Final Comparative Analysis of ALPINE. Blood, 2024.
- Lampson BL, Yu L, Glynn RJ, et al Ventricular arrhythmias and sudden death in patients taking ibrutinib. Blood. 2017, 129, 2581–2584. [CrossRef]
- Sharman JP, Ghia P, Miranda P, et al Analysis of ventricular arrhythmias and sudden death from prospective, randomized clinical trials of acalabrutinib. Br J Haematol. 2024, 205, 529–533. [CrossRef]
- Sanam Habib A, Shaaban A, Kola-Kehinde O, et al Cardiovascular Toxicities of BTK Inhibitors in Chronic Lymphocytic Leukemia: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol 2023, 5, 570–590.
- Abdel-Qadir, H. , Sabrie N., Leong D., et al. Cardiovascular risk associated with ibrutinib use in chronic lymphocytic leukemia: a population-based cohort study. J Clin Oncol. 2021, 39, 3453–3462. [Google Scholar] [CrossRef]
- Zheng Y, Guo X, Chen C, et al Cardiovascular Toxicities of Ibrutinib: A Pharmacovigilance Study Based on the United States Food and Drug Administration Adverse Event Reporting System Database. Pharmaceuticals (Basel) 2023, 16, 98. [CrossRef]
- Brown, J.R. , Byrd J.C., Ghia P., et al. Cardiovascular adverse events in patients with chronic lymphocytic leukemia receiving acalabrutinib monotherapy: pooled analysis of 762 patients. Haematologica. 2022, 107, 1335–1346. [Google Scholar] [CrossRef]
- Lyon AR, López-Fernández T, Couch LS, et al: 2022 ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J 2022, 43, 4229–4361.
- Awan FT, Addison D, Alfraih F, et al International consensus statement on the management of cardiovascular risk of Bruton's tyrosine kinase inhibitors in CLL. Blood Adv 2022, 6, 5516–5525. [CrossRef] [PubMed]
- Kumar V, Ailawadhi S, Bojanini L, et al Trends in the risk of second primary malignancies among survivors of chronic lymphocytic leukemia. Blood Cancer J 2019, 9, 75. [CrossRef] [PubMed]
- van der Straten L, Levin MD, Dinnessen MAW, et al Risk of second primary malignancies in patients with chronic lymphocytic leukemia: a population-based study in the Netherlands, 1989-2019. Blood Cancer J. 2023, 13, 15. [CrossRef] [PubMed]
- Chatzikonstantinou T, Scarfò L, Karakatsoulis G, et al Other malignancies in the history of CLL: an international multicenter study conducted by ERIC, the European Research Initiative on CLL, in HARMONY. EClinicalMedicine 2023, 65, 102307. [CrossRef] [PubMed]
- Cramer P, Isfort S, Bahlo J, et al Outcome of advanced chronic lymphocytic leukemia following different first-line and relapse therapies: a meta-analysis of five prospective trials by the German CLL Study Group (GCLLSG). Haematologica 2015, 100, 1451–1459. [CrossRef]
- Bond DA, Huang Y, Fisher JL, et al Second cancer incidence in CLL patients receiving BTK inhibitors. Leukemia 2020, 34, 3197–3205. [CrossRef] [PubMed]
- Falchi L, Vitale C, Keating MJ, et al: Incidence and prognostic impact of other cancers in a population of long-term survivors of chronic lymphocytic leukemia. Ann Oncol 2016, 27, 1100–1106. [CrossRef]
- Olszewski AJ, Gutman R, Eaton CB: Increased risk of axial fractures in patients with untreated chronic lymphocytic leukemia: A population-based analysis. Haematologica 2016, 101, e488–e491. [CrossRef]
- Ferrajoli A, Keating MJ, Manshouri T, et al. The clinical significance of tumor necrosis factor-alpha plasma level in patients having chronic lymphocytic leukemia. Blood 2002, 100, 1215–1219. [Google Scholar] [CrossRef]
- Lai R, O'Brien S, Maushouri T, et al. Prognostic value of plasma interleukin-6 levels in patients with chronic lymphocytic leukemia. Cancer. 2002, 95, 1071–1075. [Google Scholar] [CrossRef]
- Yan XJ, Dozmorov I, Li W, et al. Identification of outcome-correlated cytokine clusters in chronic lymphocytic leukemia. Blood. 2011, 118, 5201–5210. [Google Scholar] [CrossRef]
- Schmiedel BJ, Scheible CA, Nuebling T, et al: RANKL expression, function, and therapeutic targeting in multiple myeloma and chronic lymphocytic leukemia. Cancer Res 2013, 73, 683–694. [CrossRef] [PubMed]
- Shanafelt TD, Drake MT, Maurer MJ, et al. Vitamin D insufficiency and prognosis in chronic lymphocytic leukemia. Blood. 2011, 117, 1492–1498. [Google Scholar] [CrossRef]
- Molica S, Digiesi G, Antenucci A, et al Vitamin D insufficiency predicts time to first treatment (TFT) in early chronic lymphocytic leukemia (CLL). Leuk Res 2012, 36, 443–447. [CrossRef] [PubMed]
- Ariza, Y. , Murata M., Ueda Y., Yoshizawa T. Bruton’s tyrosine kinase (Btk) inhibitor tirabrutinib suppresses osteoclastic bone resorption. Bone Rep. 2019, 10, 100201. [Google Scholar] [CrossRef] [PubMed]
- Pokhrel, N.K. , Kim Y.G., Kim H.J., Kim H.J., Lee J.H., Choi S.Y., Kwon T.G., Lee H.J., Kim J.Y., Lee Y. A novel Bruton’s tyrosine kinase inhibitor, acalabrutinib, suppresses osteoclast differentiation and Porphyromonas gingivalis lipopolysaccharide-induced alveolar bone resorption. J. Periodontol. 2019, 90, 546–554. [Google Scholar]
- Giannoni P, Marini C, Cutrona G, et al Unraveling the Bone Tissue Microenvironment in Chronic Lymphocytic Leukemia. Cancers (Basel) 2023, 15, 5058. [CrossRef] [PubMed]
- Molica S, Brugiatelli M, Morabito F, et al Treatment of elderly patients with chronic lymphocytic leukemia: an unmet cinical need. Expert Rev Hematol. 2013, 6, 441–449. [CrossRef] [PubMed]
- Molica, S. Defining treatment success in chronic lymphocytic leukemia: exploring surrogate markers, comorbidities, and patient-centered endpoints. Expert Rev Hematol. 2024, 17, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Goede, V. Frailty is also a target for targeted drugs in CLL. Blood 2023, 142, 1107–1108. [Google Scholar] [CrossRef] [PubMed]
- van der Straten L, Stege CAM, Kersting S, et al. Fixed-duration venetoclax plus obinutuzumab improves quality of life and geriatric impairments in FCR-unfit patients with CLL. Blood 2023, 142, 1131–1142. [Google Scholar] [CrossRef] [PubMed]
- Martino EA, Mauro FR, Reda G, et al Ibrutinib as first line therapy in chronic lymphocytic leukemia patients over 80 years old: A retrospective real-life multicenter Italian cohort. Hematol Oncol 2024, 42, e3249. [CrossRef] [PubMed]
- Simon F, Ligtvoet R, Nösslinger T, et al Safety of acalabrutinib treatment in very old (≥80 y) and/or frail patients with chronic lymphocytic leukemia - interim safety analysis of the ongoing phase II CLL-Frail trial. Hematological Oncology 2023, 41, 468–469. [CrossRef]
- González-Gascón-Y-Marín I, Ballesteros-Andrés M, Martínez-Flores S, et al The Five "Ws" of Frailty Assessment and Chronic Lymphocytic Leukemia: Who, What, Where, Why, and When. Cancers (Basel) 2023, 15, 4391. [CrossRef] [PubMed]
- Crowder SL, Hoogland AI, Small BJ, et al Associations among frailty and quality of life in older patients with cancer treated with chemotherapy. J Geriatr Oncol 2022, 13, 1149–1155. [CrossRef]
- Johnson PC, Woyach JA, Ulrich A, et al Geriatric assessment measures are predictive of outcomes in chronic lymphocytic leukemia. J Geriatr Oncol. 2023, 14, 101538. [CrossRef] [PubMed]
- Soumerai JD, Barrientos JC, Ahn IE, et al Consensus Recommendations from the 2024 Lymphoma Research Foundation Workshop on Treatment Selection and Sequencing in CLL or SLL. Blood Adv 2024.
- S. Molica, D. Allsup, A. Polliack, D. Giannarelli. The net clinical benefit of targeted agents in the upfront treatment of elderly/unfit chronic lymphocytic leukemia patients: Results of network meta-analysis. Eur. J. Haematol. 2023, 110, 774–777. [Google Scholar] [CrossRef]
- Shanafelt TD, Bowen D, Venkat C, et al Quality of life in chronic lymphocytic leukemia: an international survey of 1482 patients. Br J Haematol 2007, 139, 255–264. [CrossRef] [PubMed]
- Holzner B, Kemmler G, Kopp M, et al: Quality of life of patients with chronic lymphocytic leukemia: Results of a longitudinal investigation over 1 yr. Eur J Haematol 2004, 72, 381–389. [CrossRef] [PubMed]
- Waweru C, Kaur S, Sharma S, et al: Health-related quality of life and economic burden of chronic lymphocytic leukemia in the era of novel targeted agents. Curr Med Res Opin 2020, 36, 1481–1495. [CrossRef] [PubMed]
- Russell K, Moghaddam N, Tickle A: Examining anxiety and depression in haematology cancer patients in ongoing treatment and under watchful waiting: A systematic review and meta-analysis. Eur J Cancer Care 2022, 31, e13678.
- Fifer S, Godsell J, Opat S, et al Understanding the experience, treatment preferences and goals of people living with chronic lymphocytic leukemia (CLL) in Australia. BMC Cancer 2024, 24, 831.
- Deering KL, Sundaram M, Harshaw Q,et al. Health-related quality of life and treatment satisfaction in Chronic Lymphocytic Leukemia (CLL) patients on ibrutinib compared to other CLL treatments in a real-world US cross sectional study. PLoS One 2022, 17, e0270291. [Google Scholar]
- Tam CS, Lamanna N, O'Brien SM, et al Health-related quality of life outcomes associated with zanubrutinib versus ibrutinib monotherapy in patients with relapsed/refractory chronic lymphocytic leukemia and small lymphocytic lymphoma: results from the ALPINE Trial. Curr Med Res Opin. 2023, 39, 1497–1503.
- Molica S, Bombaci F, Cuneo A, et al. LIVING WITH CHRONIC LYMPHOCYTIC LEUKEMIA (CLL): A QUANTITATIVE CROSS-SECTIONAL STUDY OF ITALIAN PATIENTS' EXPERIENCES ON BEHALF OF AIL (ASSOCIAZIONE ITALIANA CONTRO LE LEUCEMIE-LINFOMI E MIELOMI). EHA, 2020; EP1743.
- Molica S, Shanafelt TD, Allsup D, Giannarelli D. Impact of Targeted Agents on Survival of Chronic Lymphocytic Leukemia Patients Fit for Fludarabine, Cyclophosphamide, and Rituximab (FCR) Relative to Age- and Sex-Matched Population. Cancers (Basel) 2024, 16, 1085. [Google Scholar] [CrossRef] [PubMed]
- Wang Y, Achenbach SJ, Rabe KG, et al Cause of death in patients with newly diagnosed chronic lymphocytic leukemia (CLL) stratified by the CLL-International Prognostic Index. Blood Cancer J 2021, 11, 140. [CrossRef]
- Villavicencio A, Solans M, Zacarías-Pons L, et al Comorbidities at Diagnosis, Survival, and Cause of Death in Patients with Chronic Lymphocytic Leukemia: A Population-Based Study. Int J Environ Res Public Health 2021, 18, 701. [CrossRef] [PubMed]
- Shanafelt TD, Kay NE. Comprehensive management of the CLL patient: a holistic approach. Hematology Am Soc Hematol Educ Program. 2007, 324–331.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



