
Submitted:
03 December 2024
Posted:
04 December 2024
You are already at the latest version
Abstract
Background/Objectives: Stressors occurring across the life course are considered to have a cumulative impact on health, but there is no instrument for assessing lifetime stressor exposure in Korea. Therefore, we validated the Stress and Adversity Inventory (Adult STRAIN) in Korean. Methods: We translated the Adult STRAIN into Korean and examined its concurrent, predictive, and discriminate validity in 218 Korean adults (79 men, 139 women; Mage=29.5; 19–50 years old) recruited from a psychiatric setting. We assessed concurrent validity using Pearson’s correlations, predictive validity using multiple regression models, and discriminant validity using multivariate logistic regression to identify participants with lifetime psychiatric diagnoses. Results: The Korean STRAIN exhibited exceptional usability and acceptability; excellent concurrent validity with other measures of early adversity, life events, and perceived stress (rs=0.477–0.614); and strong predictive validity in relation to anxiety and depressive symptoms (β=0.08–0.47; ΔR2=0.109–0.206). The Korean STRAIN also significantly discriminated participants with psychiatric disorder based on stressor exposure timing, type, life domains, and social-psychological characteristics (odds ratios=1.20–4.85). Finally, the test–retest reliability for total lifetime stressor count and severity over four weeks was outstanding. Conclusions: The Korean STRAIN is a practical, valid, and reliable instrument for researchers and clinicians to efficiently assess lifetime stressor exposure.
Keywords:
early adversity
; childhood adversity
; life stress
; measurement
; assessment
; psychiatric disorders
; Korean STRAIN
1. Introduction
The concept of “stress,” defined by Han Selye in 1936 as “the non-specific response of the body to any demand for change” [1], has evolved to encompass the body’s response to any mental, emotional, or physical disturbance. Stress has recently become a central concept that poses a significant threat to both mental and physical health [2,3,4]. Moreover, recent studies have suggested that humans are affected by stress throughout their entire lives, and the potential health risks associated with stress are vast [5,6,7].
A stressor is defined as any event, situation, or stimulus that triggers a stress response [8,9]. According to Lazarus and Folkman’s model, individuals appraise stressors and manage them through coping strategies, with failures in this process associated with adverse psychological and physiological outcomes [3,9,10,11]. Since Thomas Holmes developed life event lists linking stressors to illness [12], research has shown that different stressor domains, such as work-related or interpersonal stress, elicit unique responses [8,13,14,15]. For instance, interpersonal and work stress are often strongly associated with depression, whereas traumatic experiences such as combat and sexual violence greatly increase the risk for developing post-traumatic stress disorder (PTSD) [16,17,18,19]. Furthermore, stressor effects vary by the exposure timing and specific stressors experienced, with evidence showing that these dimensions influence many health outcomes, including telomere shortening, neurodevelopmental risks, long-term immune dysfunction, malignancy, and even early mortality [2,4,5,6,7,20]. Although a comprehensive understanding of these diverse stressor effects is thus crucial, significant gaps have existed with respect to our ability to assess these different features of stressors across the life course.
More specifically, few instruments have historically existed that assess stressor exposure and its effects in high resolution. The Perceived Stress Scale (PSS), probably the most widely used stress measure [21], is commonly used in large cohort studies examining how stress impacts mental and physical health [22,23]. Although the PSS provides a simple quantification of perceived stress levels over the past month, it does not assess stressor exposure and is highly sensitive to mood and personality effects. The Life Events Checklist for DSM-5 (LEC-5) is another widely used scale [23], particularly in PTSD-related research, as it assesses the experience of traumatic events [24]. However, the LEC-5 also does not provide information on stressor exposure timing or on the domains of stressors experienced. Childhood maltreatment and adversity are frequently measured using the Childhood Trauma Questionnaire-Short Form (CTQ-SF) [25] and the Adverse Childhood Experiences (ACE) questionnaire [26], which focuses solely on specific early-life stressors, thus limiting its ability to evaluate adulthood stressors or the cumulative impact of stressors occurring across the life course. Indeed, a comprehensive and systemic tool for assessing multi-domain stressors across the lifespan has long been needed.
To address this critical measurement issue, in 2008, Slavich developed the Stress and Adversity Inventory for Adults (STRAIN) to assess lifetime stressor exposure. The STRAIN is designed as a highly affordable, user-friendly, scalable, and reliable tool that can be self- or interviewer-administered in an online system. This is the only stressor measurement system capable of evaluating a wide range of different lifetime stressors through a multidimensional structure that captures the perceived severity, frequency, specific exposure timing, primary life domain, core sociopsychological characteristics, and duration of the stressors experienced. The STRAIN has now been translated into more than 30 languages, and validation studies of the German, English, and Brazilian versions of STRAIN have demonstrated excellent usability and acceptability; test-retest reliability; concurrent, discriminant, and incremental validity; and predictive utility in relation to a wide variety of outcomes [27,28,29]. For example, research using the STRAIN has documented how cumulative exposure to specific lifetime stressors influences psychological outcomes (e.g., anxiety, depression, burnout, well-being) and physiological health (e.g., cortisol reactivity, inflammation, biological aging), personality traits (e.g., ambiguity tolerance, reward sensitivity), and behaviors (e.g., alcohol use, risk behaviors) [30,31,32,33,34,35].
The development of psychiatric disorders is often associated with chronic exposure to various stressors, leading to increased allostatic load or cumulative “wear-and-tear” on the body [36]. Recurrent and excessive stress progressively weakens the body’s ability to maintain homeostasis and increases the risk of mental disorders, including depression, anxiety, neurodevelopmental disorders, and PTSD [4,37,38,39]. The STRAIN’s ability to evaluating a broad array of stressors that can exert these cumulative effects over the lifetime is expected to be crucial in helping to clarify associations between stressor exposure and psychiatric disorders. However, research on lifetime stressor exposure using the STRAIN and psychiatric disorders is limited, and despite its importance and multifaceted and cumulative design, no appropriate tool is available in Korea.
To address this issue, we first translated the STRAIN into Korean. Then, we examined the usability, acceptability, test-retest reliability, and concurrent, predictive, and incremental validity of the Adult STRAIN in Korean. We hypothesized that the Adult STRAIN in Korean would demonstrate good usability/acceptability, and test-retest reliability, and be significantly correlated with other life stress measures. Furthermore, we hypothesized that cumulative lifetime stress exposure, as measured by the Korean STRAIN, would be associated with the lifetime psychiatric diagnosis but that these effects would vary by stressor type.
2. Materials and Methods
2.1. Participants and Procedure
Participants were 218 adults between 19–50 years old (79 men and 139 women) who were recruited through advertisements posted at the Korea University of Guro Hospital from June to November 2023. After providing informed consent, participants engaged in a survey of psychological factors (i.e., stress, anxiety, depression) and sociodemographic factors (e.g., demographics, medical history, and psychiatric history), including the Korean STRAIN.
Table 1 presents the participants’ characteristics. Participants in the initial survey had a mean age of 29.5 ± 6.02 years. A total of 171 participants (78.44%) in the sample were employed. Additionally, 66 participants reported a history of medical disorders, whereas 44 individuals reported a history of psychiatric disorders. Among these, depressive disorders were the most frequently reported, affecting 37 patients (16.97%). These were followed by anxiety disorder, reported by 31 patients (14.22%), and insomnia disorder, reported by 20 patients (9.17%). We re-administered the STRAIN to all participants approximately four weeks after enrollment (Mweeks = 5.33, SD = 3.20) to examine the test-retest reliability of the Korean STRAIN. In total, 177 participants completed the follow-up assessment. The study protocol was pre-approved by the Institutional Review Board of the Korea University Guro Hospital (IRB number: K2023-1381-001).
2.2. Measures
2.2.1. Lifetime Stressor Exposure
To evaluate participants’ cumulative lifetime stressor exposure, we first translated the STRAIN into Korean using the gold-standard translation/back-translation method. The process involved three key steps: first, the original English STRAIN interview was translated into Korean; second, this Korean version of the STRAIN was translated back into English; finally, we carefully compared the original English STRAIN and the back-translated STRAIN to ensure accuracy, and resolved any discrepancies via consensus discussion in order to confirm that the Korean STRAIN matched the English STRAIN with 100% fidelity. Critically, the first and second steps described above were carried out by two different, independent bilingual experts to ensure the accuracy and cultural appropriateness of the Korean STRAIN. The resulting Korean STRAIN maintains the structure of the original English version, encompassing an identical set of 55 core stressors [28]. Upon endorsing a stressor, respondents are prompted with tailored inquiries to gauge its perceived severity, frequency, exposure timing, and duration. This comprehensive approach enabled us to create highly nuanced and individualized lifetime stressor exposure profiles for each participant, while also synthesizing the data into various aggregate measures of lifetime stressor exposure. In this study, we concentrated on the STRAIN’s two primary outcomes: the (a) aggregate number of stressors experienced and (b) their cumulative severity over each participant’s entire lifetime.
2.2.2. Early Adversity
Early life adversity was evaluated using the Korean version of the CTQ-SF [26]. This 28-item measure assesses five dimensions of childhood maltreatment, including physical and emotional neglect and sexual, physical, and emotional abuse. Responses range from 1 (never true) to 5 (very often true), with higher average scores indicating greater early adversity. The Korean CTQ-SF has demonstrated high internal consistency in prior research (Cronbach’s α=0.88) [26] and excellent reliability in the present study (Cronbach’s α=0.93).
2.2.3. Life Events
Exposure to potentially traumatic life events was measured using the Korean version of the LEC-5 [24]. This self-report instrument screens for 16 events known to potentially result in PTSD or significant distress. Respondents indicate whether each event “happened to me,” was “witnessed,” or “does not apply.” The total number of directly experienced events provides an index of life event exposure. The Korean LEC-5’s reliability improved from prior studies (current Cronbach’s α=0.85, compared to 0.67 in prior research).
2.2.4. Perceived Stress
Recent perceived stress levels were assessed using the Korean PSS [21]. Participants reported their stress experiences over the past month using a five-point Likert scale, with higher scores indicating greater perceived stress. The Korean PSS maintained good reliability (Cronbach’s α=0.85), consistent with prior findings.
2.2.5. Anxiety and Depressive Symptoms
The Korean State-Trait Anxiety Inventory (STAI) [40,41] assessed both state (current) and trait (general) anxiety using 40 items rated on a four-point scale. Both subscales demonstrated excellent reliability (Cronbach’s α=0.95 and 0.94 for state and trait, respectively).
The Korean 7-item Generalized Anxiety Disorder scale (GAD-7) [42] evaluated symptoms of generalized anxiety over the past two weeks. It showed high internal consistency (Cronbach’s α=0.90), similar to prior findings (α=0.93).
Depressive symptoms were assessed using the Korean Patient Health Questionnaire-9 (PHQ-9) [43]. This nine-item measure assesses depressive symptoms over the past two weeks using a four-point Likert scale. The Korean PHQ-9 maintained excellent reliability (Cronbach’s α =0.91) compared to prior research (α=0.88).
2.3. Data Analyses
To analyze concurrent validity, we examined Pearson’s correlations between the Korean STRAIN and psychological factors, including CTQ-SF, LEC-5, and PSS scores. Predictive validity was assessed using multiple regression models by evaluating how well the Korean STRAIN predicts participants’ anxiety and depressive symptoms, measured by the STAI trait and state, GAD-7, and PHQ-9 scores. Additionally, we conducted multivariate logistic regression analyses to evaluate the discriminant validity of the Korean STRAIN to distinguish between participants with and without psychiatric disorders, examining the likelihood of diagnosis based on timing, type, domain, and core sociopsychological characteristics. All multiple regression models included the following covariates: age, sex, education level, and occupation. The test-retest reliability of the Korean STRAIN was evaluated using Pearson’s correlation coefficient. We applied Student’s t-tests to examine sex differences in specific primary life domains and core sociopsychological characteristics of lifetime stressor count. All analyses were conducted using R software (version 4.4.1; R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Usability and Acceptability
The Korean STRAIN assessment demonstrated efficient completion times across both administrations. During the initial assessment, participants completed the Korean STRAIN in a median time of 15 min 53 s (interquartile range [IQR]=9 min 55 s–21 min 51 s). The retest showed improved efficiency, with a median completion time of 12 min 17 s (IQR=8 min 1 s–16 min 33 s). The instrument exhibited remarkable acceptability among the study cohort. Indeed, all participants successfully completed the entire interview with no instances of premature termination. Furthermore, no participants reported any complaints or psychosocial distress stemming from engagement with the questions.
3.2. Descriptive Statistics for Lifetime Stressor Exposure for Men and Women
On average, participants reported 8.53 stressors over their life course (SD=9.90; range 0–55). Table 2 provides an analysis of lifetime stressor counts by sex. Women experienced more stressors (M=11.46, SD=11.63) than men (M=8.68, SD=6.61). This disparity was especially pronounced for stressors involving the primary life domains of housing, reproduction, and life-threatening situations (all p<0.05). Furthermore, examining the STRAIN’s core sociopsychological characteristics revealed sex-based differences that were particularly pronounced for stressors involving physical danger and role change/disruption (all p<0.05, Table 2).
3.3. Validity
3.3.1. Concurrent Validity
To evaluate the validity of the Korean STRAIN, we first investigated its concurrent validity by comparing it with other commonly used stress assessment tools. Our analysis focused on associations between the Korean STRAIN and three well-established stress measures: CTQ-SF for assessing early life adversity, LEC-5 for assessing significant life events, and PSS for assessing recent perceived stress levels.
The results revealed significant correlations between the Korean STRAIN’s two main outcomes—lifetime stressor count and lifetime stressor severity—and these commonly used, well-validated instruments. Indeed, both STRAIN indices demonstrated very strong, positive associations with childhood trauma as measured by the CTQ-SF (Count: r=0.614, p<0.05; Severity: r=0.604, p<0.05). Comparable patterns were observed with life events assessed using the LEC-5 (Count: r=0.487, p<0.05; Severity: r=0.473, p<0.01). Moreover, STRAIN metrics showed robust correlations with perceived stress levels quantified using the PSS (Count: r=0.477, p<0.05; Severity: r=0.509, p<0.05). Table 3 presents these correlation coefficients in detail.
3.3.2. Predictive Validity
Next, we assessed the Korean STRAIN’s predictive validity. Multiple separate regression models were used to examine the extent to which the Korean STRAIN predicted participants’ anxiety and depressive symptoms, as assessed using the STAI trait and state, GAD-7, and PHQ-9.
As shown in Table 4, the total lifetime stressor count was significantly associated with the STAI state scale (β=0.44; ΔR2=0.120, p<0.001), STAI trait scale (β=0.47; ΔR2=0.117, p<0.001), PHQ-9 scores (β=0.27; ΔR2=0.182, p<0.001), and GAD-7 scores (β=0.17; ΔR2=0.109, p<0.001). Similar results were found for models assessing lifetime stressor severity, wherein the total lifetime stressor severity was significantly associated with the STAI state scale (β=0.20; ΔR2=0.136, p<0.001), STAI trait scale (β=0.23; ΔR2=0.150, p<0.001), PHQ-9 scores (β=0.12; ΔR2=0.206, p<0.001), and GAD-7 scores (β=0.08; ΔR2=0.121, p<0.001).
3.3.3. Comparative Predictive Validity of Each Variable for Lifetime Psychiatric Diagnosis
To examine the comparative predictive validity of each domain of STRAIN for lifetime psychiatric diagnosis, we analyzed the likelihood of diagnosis based on the stressor timing, type, domains, and sociopsychological characteristics of the STRAIN, PSS, and CTQ-SF (Figure 1).
For stressor timing and stressor type, the odds ratios were high for early life stressor (odds ratio [OR]=1.29, 95% confidence interval [CI]=1.16–1.45, p<0.001) and chronic difficulties (OR=1.33, 95% CI=1.21–1.49, p<0.001) vs. adulthood stressors (OR=1.24, 95% CI=1.15–1.35, p<0.001) and acute life events (OR=1.20, 95% CI=1.11–1.30, p<0.001), respectively. In terms of the primary life domains, education (OR=4.85, 95% CI=1.57–18.87, p=0.010), treatment/health (OR=2.09, 95% CI=1.67–2.72, p<0.001), and work (OR=1.79, 95% CI=1.10–2.90, p<0.001) presented relatively high ORs. Regarding core sociopsychological characteristics, humiliation (OR=1.73, 95% CI=1.41–2.16, p<0.001) and entrapment (OR=1.66, 95% CI=1.24–2.26, p<0.001) were significantly associated with increased odds of being diagnosed with a lifetime psychiatric disorder. PSS (OR=1.05, 95% CI=1.03–1.08, p<0.001) and CTQ-SF (OR=1.22, 95% CI=1.13–1.33, p<0.001) scores were also significant.
3.4. Test-Retest Reliability
Finally, we assessed the test-retest reliability of all six of the Korean STRAIN’s main outcomes (i.e., Total Lifetime Stressor Count, Total Lifetime Stressor Severity, Acute Life Event Count, Chronic Difficulty Count, Acute Life Event Severity, Chronic Difficulty Severity) over a one-month period. All six of these outcomes exhibited very high test-retest reliability (r≥0.878, p<0.05) over one month. Among them, total lifetime stressor count and total lifetime stressor severity achieved outstanding test-retest reliability over time (r=0.910, p<0.05, and r=0.909, p<0.05, respectively) (Table S1).
4. Discussion
This study is the first to investigate the usability and acceptability, reliability, and validity of the Korean STRAIN, as well as how the various stressors dimensions assessed by the STRAIN relate to participants’ lifetime psychiatric diagnosis. Participants completed the Korean STRAIN in approximately 16 min in the first session and 12 min in the second session, with excellent overall usability and acceptability. The Korean STRAIN demonstrated strong concurrent validity with the CTQ-SF, LEC-5, and PSS, as well as excellent predictive validity with the STAI-Trait, STAI-State, GAD-7, and PHQ.
This study used various indices from the Korean STRAIN to examine sex differences in lifetime stressor exposure, revealing that women had higher overall stressor counts than men, particularly for stressors in the primary life domains of housing, reproduction, life-threatening situations, physical danger, and role change/disruption. Prior studies have suggested that women are exposed to more psychosocial and physiological stress during several life stages including, pregnancy, and menopause, leading to higher prevalence rates of psychiatric disorders, including perinatal mood and anxiety disorder and severe mental illness [44]. Women also traditionally face additional burdens from family caregiving responsibilities [45]. Furthermore, women are more vulnerable to intimate partner violence [46] and experience a greater fear of life-threatening and physical dangers than men, a phenomenon known as the “fear-gender gap” [47]. Using the Korean STRAIN, we were able to clearly observe differences in the specific types of stressors that may underlie these gender differences across the life course.
An analysis of the concurrent and predictive validity of the Korean STRAIN revealed strong correlations between the STRAIN scores and other scales assessing early adversity, adulthood life events, and recent perceived stress levels. Consistent with prior research examining the original Adult STRAIN (in English) and German Adult STRAIN, the CTQ-SF showed the strongest correlation with lifetime stressor count and severity [29], underscoring the critical role of early developmental stages in processing stressor exposure [4,6,48,49,50]. By capturing participants’ cumulative stressors from an early age, the Korean STRAIN provides a highly nuanced, comprehensive view of individuals’ lifelong stressor burden. Moreover, the STRAIN scores significantly predicted trait and state anxiety, as well as self-reported anxiety and depressive symptoms, supporting its strong predictive validity in relation to several key clinical outcomes. These findings are consistent with numerous prior studies reporting the onset of psychopathologies such as depression and anxiety following recent major life events and trauma [4,9,51,52,53], and the robust correlations between the Korean STRAIN and mental health highlight its potential utility for use assessing stress in clinical settings.
The findings of this study show that the STRAIN in Korean is consistent with prior studies of other stress assessments in relation to lifetime psychiatric diagnosis. Specifically, the data showed that chronic childhood stressors were associated with a significant elevated risk of lifetime psychiatric diagnosis, consistent with prior studies demonstrating that early life stress, measured using the ACE questionnaire, CTQ-SF, and clinical interviews increases the risk of developing conditions such as PTSD, depression, and conduct disorders [6,33,45,46]. The primary life domain results reflect Korean society’s characteristics, where academic stress leads to life dissatisfaction, highlighting prominent features in the educational domain [54,55].
Additionally, the study identified humiliation and entrapment as dimensions of stress that are highly relevant for the development of psychiatric disorders, supporting theories such as social safety theory [56,57,58], entrapment and defeat theory [59], social rank theory [60], and the interpersonal theory of suicide [61]. Although many models have hypothesized an association between specific categories of life stressors and psychopathology, few studies have comprehensively assessed the social characteristics of stressors, especially across the life course. By capturing the multidimensional characteristics and cumulative effects of psychological stressors, the Korean STRAIN could be highly beneficial to those looking to develop or refine theories of psychopathology and other health outcomes.
Finally, we found that the Korean STRAIN has excellent test-retest reliability over one month, even though achieving high test-retest reliability of a stressor scale requires participants to accurately (re-)remember not just which stressors they have experienced but also the specific severity, frequency, exposure timing, duration, and type (acute vs. chronic) of those stressors. Regardless, the test-retest reliability for the Korean STRAIN’s six main outcomes was very high, with total lifetime stressor count and total lifetime stressor severity exhibiting exceptional test-retest reliability at r=0.910 and r=0.909, respectively. These values are remarkably comparable to those observed for the original (English) Adult STRAIN (r=0.904 and 0.919, respectively) [26] and the Brazilian Adult STRAIN (r=0.936 and 0.953, respectively) [25], demonstrating the ability of the STRAIN to obtain consistent assessments of individuals’ lifetime stressor exposure over time.
4.1. Limitations
This study had several limitations. First, the primarily cross-sectional study design (except for the test-retest analyses) means that all findings are correlational, and causality cannot be inferred. Second, although the STRAIN has been shown to be insensitive to mood and self-report biases [29], the STRAIN is based on participants’ self-reports, and these biases cannot be fully ruled out. Third, no biological samples were collected in this study; therefore, further research is needed to validate STRAIN against health-related biomarkers. Fourth, the sample was drawn from a specific region in Korea and consisted of individuals with access to psychiatric care in the country, which may limit the generalizability of the findings. Finally, due to the limited sample size, limited information was available regarding the onset of specific clinical conditions. Future studies should evaluate the generalizability of the associations described here in more representative populations and specific clinical samples (e.g., anxiety, depression, cognitive decline, substance use).
4.2. Conclusion
In conclusion, the Korean STRAIN is a user-friendly and highly acceptable tool for assessing lifetime stressor exposure that demonstrates excellent concurrent, predictive, and discriminant validity, and outstanding test-retest reliability over one month. The Korean STRAIN’s multidimensional and cumulative nature could make it particularly useful for comprehensively assessing lifetime stressors to aid in case conceptualization and treatment planning in clinical settings. The Korean STRAIN may also help to identify individuals at high risk for psychiatric disorders, supporting the delivery of prevention programs for promoting resilience in high-risk individuals.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1. Test-retest reliability of the core 6-item of the STRAIN.
Author Contributions
Conceptualization: G.M.S. and J.K.; Data curation: K.S.O., Y.C.S., S.W.J., D.W.S., S.J.C., G.M.S., and J.K.; Formal analysis: E.S.K., Y.T.K., and J.K.; Visualization: J.K.; Writing – original draft: E.S.K., Y.T.K., and J.K.; Writing – review & editing: K.S.O., Y.C.S., S.W.J., D.W.S., S.J.C., G.M.S., and J.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Korean National Police Agency (KNPA, Korea), grant number 220222M03.
Institutional Review Board Statement
The study protocol was approved by the Institutional Review Board of the Korea University Guro Hospital (IRB number: K2023-1381-001). The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study prior to participation in any study procedures.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions.
Acknowledgments
We thank the participants for their time and effort.
Conflicts of Interest
The authors declare no conflicts of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Selye, H. The Stress of Life; McGraw Hill: New York, USA, 1978. [Google Scholar]
- Epel, E.S.; Blackburn, E.H.; Lin, J.; Dhabhar, F.S.; Adler, N.E.; Morrow, J.D.; Cawthon, R.M. Accelerated telomere shortening in response to life stress. Proc Natl Acad Sci 2004, 101, 17312–17315. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Litzelman, K.; Wisk, L.E.; Maddox, T.; Cheng, E.R.; Creswell, P.D.; Witt, W.P. Does the perception that stress affects health matter? The association with health and mortality. Health Psychol 2012, 31, 677. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.B.; Thayer, J.F.; Vedhara, K. Stress and health: a review of psychobiological processes. Annu Rev Psychol 2021, 72, 663–688. [Google Scholar] [CrossRef]
- Lautarescu, A.; Craig, M.C.; Glover, V. Chapter Two - Prenatal stress: Effects on fetal and child brain development. Int Rev Neurobiol 2020, 150, 17–40. [Google Scholar]
- Strathearn, L.; Giannotti, M.; Mills, R.; Kisely, S.; Najman, J.; Abajobir, A. Long-term cognitive, psychological, and health outcomes associated with child abuse and neglect. Pediatrics 2020, 146, e20200438. [Google Scholar] [CrossRef]
- Turner, A.I.; Smyth, N.; Hall, S.J.; Torres, S.J.; Hussein, M.; Jayasinghe, S.U.; Ball, K.; Clow, A.J. Psychological stress reactivity and future health and disease outcomes: a systematic review of prospective evidence. Psychoneuroendocrinology 2020, 114, 104599. [Google Scholar] [CrossRef] [PubMed]
- Monroe, S.; Slavich, G. Psychological stressors: overview. In Stress: Concepts, Cognition, Emotion, and Behavior; Elsevier, 2016; pp. 109–115.
- Biggs, A.; Brough, P.; Drummond, S. Lazarus and Folkman’s psychological stress and coping theory. In The Handbook of Stress and Health: A Guide to Research and Practice; Wiley Blackwell: Oxford, UK, 2017; pp. 349–364. [Google Scholar]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: psychological, behavioral, and biological determinants. Annu Rev Clin Psychol 2005, 1, 607–628. [Google Scholar] [CrossRef]
- Segerstrom, S.C.; Miller, G.E. Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychol Bull 2004, 130, 601. [Google Scholar] [CrossRef] [PubMed]
- Holmes, T.H. Life situations, emotions, and disease. Psychosomatics 1978, 19, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Nicolai, K.A.; Laney, T.; Mezulis, A.H. Different stressors, different strategies, different outcomes: how domain-specific stress responses differentially predict depressive symptoms among adolescents. J Youth Adolesc 2013, 42, 1183–1193. [Google Scholar] [CrossRef]
- Slavich, G.M.; O’Donovan, A.; Epel, E.S.; Kemeny, M.E. Black sheep get the blues: a psychobiological model of social rejection and depression. Neurosci Biobehav Rev 2010, 35, 39–45. [Google Scholar] [CrossRef]
- Epel, E.S.; Crosswell, A.D.; Mayer, S.E.; Prather, A.A.; Slavich, G.M.; Puterman, E.; Mendes, W.B. More than a feeling: A unified view of stress measurement for population science. Front Neuroendocrinol 2018, 49, 146–169. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, S.; Coggon, D.; Andersen, J.H.; Casey, P.; Flachs, E.M.; Kolstad, H.A.; Mors, O.; Bonde, J.P. Are depressive disorders caused by psychosocial stressors at work? A systematic review with metaanalysis. Eur J Epidemiol 2021, 36, 479–496. [Google Scholar] [CrossRef] [PubMed]
- Xue, C.; Ge, Y.; Tang, B.; Liu, Y.; Kang, P.; Wang, M.; Zhang, L. A meta-analysis of risk factors for combat-related PTSD among military personnel and veterans. PLoS One 2015, 10, e0120270. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M.; Irwin, M.R. From stress to inflammation and major depressive disorder: a social signal transduction theory of depression. Psychol Bull 2014, 140, 774–815. [Google Scholar] [CrossRef]
- Slavich, G.M.; Sacher, J. Stress, sex hormones, inflammation, and major depressive disorder: extending Social Signal Transduction Theory of Depression to account for sex differences in mood disorders. Psychopharmacology 2019, 236, 3063–3079. [Google Scholar] [CrossRef] [PubMed]
- Rentscher, K.E.; Carroll, J.E.; Mitchell, C. Psychosocial stressors and telomere length: a current review of the science. Annu Rev Public Health 2020, 41, 223–245. [Google Scholar] [CrossRef]
- Lee, J.; Shin, C.; Ko, Y.-H.; Lim, J.; Joe, S.-H.; Kim, S.; Jung, I.-K.; Han, C. The reliability and validity studies of the Korean version of the Perceived Stress Scale. Korean J Psychom Med 2012, 20, 127–134. [Google Scholar]
- Chandola, T.; Brunner, E.; Marmot, M. Chronic stress at work and metabolic syndrome: a prospective study. BMJ 2006, 332, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Janicki-Deverts, D. Who’s stressed? Distributions of psychological stress in the United States in probability samples from 1983, 2006, and 2009 1. J Appl Soc Psychol 2012, 42, 1320–1334. [Google Scholar] [CrossRef]
- Bae, H.; Kim, D.; Koh, H.; Kim, Y.; Park, J.S. Psychometric properties of the Life Events Checklist-Korean version. Psychiatry Investig 2008, 5, 163–167. [Google Scholar] [CrossRef]
- Armour, C.; Carragher, N.; Elhai, J.D. Assessing the fit of the dysphoric arousal model across two nationally representative epidemiological surveys: the Australian NSMHWB and the United States NESARC. J Anxiety Disord 2013, 27, 109–115. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am J Prev Med 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Park, S.C.; Yang, H.; Oh, D.H. Reliability and validity of the Korean version of the childhood trauma questionnaire-short form for psychiatric outpatients. Psychiatry Investig 2011, 8, 305–311. [Google Scholar] [CrossRef]
- Cazassa, M.J.; Oliveira, M. d. S.; Spahr, C.M.; Shields, G.S.; Slavich, G.M. The Stress and Adversity Inventory for Adults (Adult STRAIN) in Brazilian Portuguese: initial validation and links with executive function, sleep, and mental and physical health. Front Psychol 2020, 10, 3083. [Google Scholar] [CrossRef]
- Slavich, G.M.; Shields, G.S. Assessing lifetime stress exposure using the Stress and Adversity Inventory for Adults (Adult STRAIN): An overview and initial validation. Psychosom Med 2018, 80, 17–27. [Google Scholar] [CrossRef]
- Sturmbauer, S.C.; Shields, G.S.; Hetzel, E.-L.; Rohleder, N.; Slavich, G.M. The stress and adversity inventory for adults (adult STRAIN) in German: an overview and initial validation. PLoS One 2019, 14, e0216419. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.C.; Shields, G.S.; Trainor, B.C.; Slavich, G.M.; Yonelinas, A.P. Greater lifetime stress exposure predicts blunted cortisol but heightened DHEA responses to acute stress. Stress Health 2019, 35, 15–26. [Google Scholar] [CrossRef]
- Murphy, M.L.; Slavich, G.M.; Chen, E.; Miller, G.E. Targeted rejection predicts decreased anti-inflammatory gene expression and increased symptom severity in youth with asthma. Psychol Sci 2015, 26, 111–121. [Google Scholar] [CrossRef]
- Raio, C.M.; Lu, B.B.; Grubb, M.; Shields, G.S.; Slavich, G.M.; Glimcher, P. Cumulative lifetime stressor exposure assessed by the STRAIN predicts economic ambiguity aversion. Nat Commun 2022, 13, 1686. [Google Scholar] [CrossRef]
- Rosero-Pahi, M.; Andoh, J.; Shields, G.S.; Acosta-Ortiz, A.; Serrano-Gomez, S.; Slavich, G.M. Cumulative lifetime stressor exposure impairs stimulus–response but not contextual learning. Sci Rep 2024, 14, 13080. [Google Scholar] [CrossRef] [PubMed]
- Shields, G.S.; Ramey, M.M.; Slavich, G.M.; Yonelinas, A.P. Determining the mechanisms through which recent life stress predicts working memory impairments: precision or capacity? Stress 2019, 22, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M.; Stewart, J.G.; Esposito, E.C.; Shields, G.S.; Auerbach, R.P. The Stress and Adversity Inventory for Adolescents (Adolescent STRAIN): associations with mental and physical health, risky behaviors, and psychiatric diagnoses in youth seeking treatment. J Child Psychol Psychiatry 2019, 60, 998–1009. [Google Scholar] [CrossRef]
- McEwen, B.S. Stress, adaptation, and disease: allostasis and allostatic load. Ann N Y Acad Sci 1998, 840, 33–44. [Google Scholar] [CrossRef]
- Devi, F.; Shahwan, S.; Teh, W.L.; Sambasivam, R.; Zhang, Y.J.; Lau, Y.W.; Ong, S.H.; Fung, D.; Gupta, B.; Chong, S.A.; Subramaniam, M. The prevalence of childhood trauma in psychiatric outpatients. Ann Gen Psychiatry 2019, 18, 15. [Google Scholar] [CrossRef]
- Lutin, E.; Schiweck, C.; Cornelis, J.; De Raedt, W.; Reif, A.; Vrieze, E.; Claes, S.; Van Hoof, C. The cumulative effect of chronic stress and depressive symptoms affects heart rate in a working population. Front Psychiatry 2022, 13, 1022298. [Google Scholar] [CrossRef] [PubMed]
- Mayer, S.E.; Prather, A.A.; Puterman, E.; Lin, J.; Arenander, J.; Coccia, M.; Shields, G.S.; Slavich, G.M.; Epel, E.S. Cumulative lifetime stress exposure and leukocyte telomere length attrition: the unique role of stressor duration and exposure timing. Psychoneuroendocrinology 2019, 104, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Hahn, D. Korean adaptation of Spielberger’s STAI (K-STAI). Korean J Health Psychol 1996, 1, 1. [Google Scholar]
- Lim, Y.; Lee, S.; Kim, J. Distinct and overlapping features of anxiety sensitivity and trait anxiety: the relationship to negative affect, positive affect, and physiological hyperarousal. Korean J Clin Psychol 2005, 24, 439–449. [Google Scholar]
- Ahn, J.-K.; Kim, Y.; Choi, K.-H. The psychometric properties and clinical utility of the Korean versions of the GAD-7 and GAD-2. Front Psychiatry 2019, 10, 127. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Jo, S.A.; Kwak, J.-H.; Pae, C.-U.; Steffens, D.; Jo, I.; Park, M.H. Validation of the Patient Health Questionnaire-9 Korean version in the elderly population: the Ansan Geriatric study. Compr Psychiatry 2008, 49, 218–223. [Google Scholar] [CrossRef] [PubMed]
- McKee, K.; Admon, L.K.; Winkelman, T.N.; Muzik, M.; Hall, S.; Dalton, V.K.; Zivin, K. Perinatal mood and anxiety disorders, serious mental illness, and delivery-related health outcomes, United States, 2006–2015. BMC Womens Health 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Mussida, C.; Patimo, R. Women’s family care responsibilities, employment and health: a tale of two countries. J Fam Econ Issues 2021, 42, 489–507. [Google Scholar] [CrossRef] [PubMed]
- Madriz, E. Nothing Bad Happens to Good Girls: Fear of Crime in Women’s Lives; University of California Press: Berkeley/Los Angeles, USA, 2023. [Google Scholar]
- Johansson, S.; Haandrikman, K. Gendered fear of crime in the urban context: a comparative multilevel study of women’s and men’s fear of crime. J Urban Aff 2023, 45, 1238–1264. [Google Scholar] [CrossRef]
- Masten, A.S.; Gewirtz, A.H.; Sapienza, J.K. Resilience in Development: The Importance of Early Childhood; Centre of Excellence for Early Childhood Development: Montreal, Canada, 2006. [Google Scholar]
- Nelson, C.A.; Bhutta, Z.A.; Harris, N.B.; Danese, A.; Samara, M. Adversity in childhood is linked to mental and physical health throughout life. BMJ 2020, 371, m3048. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Kim, S.; Zhang, H.; Dobalian, A.; Slavich, G.M. Lifetime adversity predicts depression, anxiety, and cognitive impairment in a nationally representative sample of older adults in the United States. J Clin Psychol 2024, 80, 1031–1049. [Google Scholar] [CrossRef]
- Burani, K.; Brush, C.J.; Shields, G.S.; Klein, D.N.; Nelson, B.; Slavich, G.M.; Hajcak, G. Cumulative lifetime acute stressor exposure interacts with reward responsiveness to predict longitudinal increases in depression severity in adolescence. Psychol Med 2023, 53, 4507–4516. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.L.M.; Sichko, S.; Bui, T.Q.; Libowitz, M.R.; Shields, G.S.; Slavich, G.M. Intergenerational transmission of lifetime stressor exposure in adolescent girls at differential maternal risk for depression. J Clin Psychol 2023, 79, 431–448. [Google Scholar] [CrossRef] [PubMed]
- Poulton, R.; Moffitt, T.E.; Silva, P.A. The Dunedin Multidisciplinary Health and Development Study: overview of the first 40 years, with an eye to the future. Soc Psychiatry Psychiatr Epidemiol 2015, 50, 679–693. [Google Scholar] [CrossRef]
- Kwak, C.W.; Ickovics, J.R. Adolescent suicide in South Korea: risk factors and proposed multi-dimensional solution. Asian J Psychiatr 2019, 43, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M. Social safety theory: a biologically based evolutionary perspective on life stress, health, and behavior. Annu Rev Clin Psychol 2020, 16, 265–295. [Google Scholar] [CrossRef]
- Slavich, G.M. Social safety theory: understanding social stress, disease risk, resilience, and behavior during the COVID-19 pandemic and beyond. Curr Opin Psychol 2022, 45, 101299. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M.; Roos, L.G.; Mengelkoch, S.; Webb, C.A.; Shattuck, E.C.; Moriarity, D.P.; Alley, J.C. Social safety theory: conceptual foundation, underlying mechanisms, and future directions. Health Psychol Rev 2023, 17, 5–59. [Google Scholar] [CrossRef]
- Choi, C.; Lee, J.; Yoo, M.S.; Ko, E. South Korean children’s academic achievement and subjective well-being: the mediation of academic stress and the moderation of perceived fairness of parents and teachers. Child Youth Serv Rev 2019, 100, 22–30. [Google Scholar] [CrossRef]
- Wijbenga, L.; Reijneveld, S.A.; Almansa, J.; Korevaar, E.L.; Hofstra, J.; de Winter, A.F. Trajectories of stressful life events and long-term changes in mental health outcomes, moderated by family functioning? The TRAILS study. Child Adolesc Psychiatry Ment Health 2022, 16, 106. [Google Scholar] [CrossRef]
- Taylor, P.J.; Gooding, P.; Wood, A.M.; Tarrier, N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychol Bull 2011, 137, 391–420. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.; Allan, S. The role of defeat and entrapment (arrested flight) in depression: an exploration of an evolutionary view. Psychol Med 1998, 28, 585–598. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Kirtley, O.J. The integrated motivational-volitional model of suicidal behaviour. Phil Trans R Soc B Biol Sci 2018, 373, 20170268. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Likelihood of lifetime psychiatric diagnosis by stressor timing, type, primary domain, and core sociopsychological characteristic of the STRAIN, PSS, and CTQ-SF. CTQ-SF, Childhood Trauma Questionnaire–Short Form; PSS, Perceived Stress Scale; STRAIN, Stress and Adversity Inventory for Adults.
Figure 1.
Likelihood of lifetime psychiatric diagnosis by stressor timing, type, primary domain, and core sociopsychological characteristic of the STRAIN, PSS, and CTQ-SF. CTQ-SF, Childhood Trauma Questionnaire–Short Form; PSS, Perceived Stress Scale; STRAIN, Stress and Adversity Inventory for Adults.
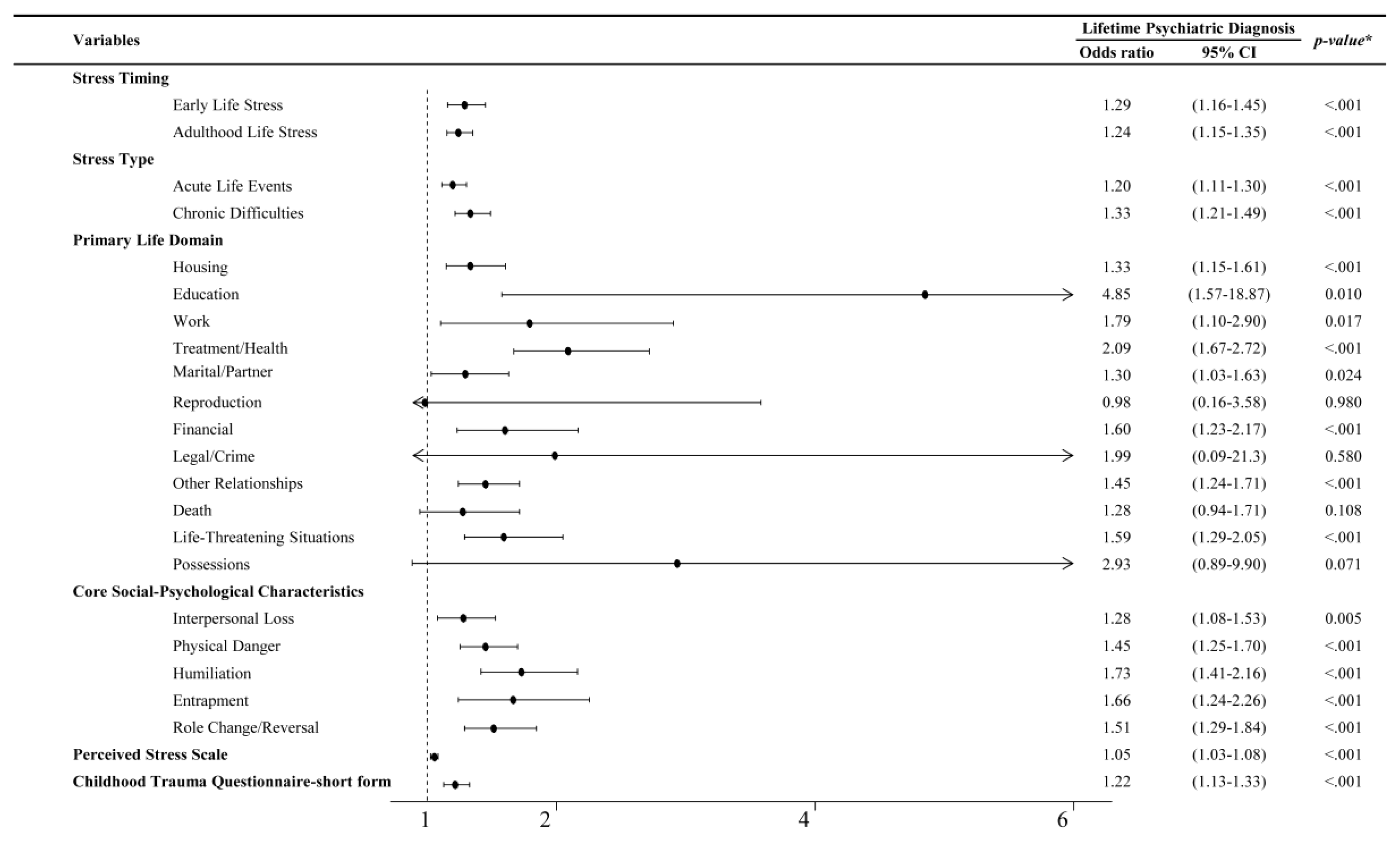

Table 1.
Participant characteristics.
| Characteristic | Total (N = 218) |
|
|---|---|---|
| Age (years) | 29.5±6.02 | |
| Sex | ||
| Male | 79 (36.24) | |
| Female | 139 (63.76) | |
| Level of education (years) | 14.90±1.73 | |
| Occupational status | ||
| Employed | 171 (78.44) | |
| Unemployed | 47 (21.56) | |
| Medical history | ||
| Any | 66 (30.28) | |
| Endocrine disorder | 24 (11.01) | |
| Gastrointestinal disorder | 23 (10.55) | |
| Nervous disorder | 6 (2.75) | |
| Musculoskeletal disorder | 6 (2.75) | |
| Respiratory disorder | 5 (2.29) | |
| Genitourinary disorder | 4 (1.83) | |
| Cardiovascular disorder | 3 (1.38) | |
| Others | 7 (3.21) | |
| None | 152 (69.72) | |
| Psychiatric history | ||
| Any | 44 (20.33) | |
| Depressive disorder | 37 (16.97) | |
| Anxiety disorder | 31 (14.22) | |
| Insomnia disorder | 20 (9.17) | |
| Panic disorder | 7 (3.21) | |
| Obsessive compulsive disorder | 2 (0.92) | |
| Bipolar disorder | 1 (0.46) | |
| Adjustment disorder | 1 (0.46) | |
| Post-traumatic stress disorder | 0 (0.00) | |
| Schizophrenia | 0 (0.00) | |
| Others | 1 (0.46) | |
| None | 174 (79.66) | |
Data are presented as mean ± standard deviation or number (%).
Table 2.
Lifetime stressor count by stressor category for men and women.
| Variables | Sex | p-value | ||
|
Men (n = 79) |
Women (n = 139) |
|||
| Total Lifetime Stressor Count | 8.68±6.61 | 11.46±11.63 | 0.052 | |
| Primary Life Domain | ||||
| Housing | 0.65±1.34 | 1.40±2.77 | 0.024* | |
| Education | 0.06±0.29 | 0.04±0.19 | 0.402 | |
| Work | 0.43±0.63 | 0.60±0.83 | 0.108 | |
| Treatment/Health | 1.49±2.19 | 1.55±2.01 | 0.856 | |
| Marital/Partner | 1.43±1.53 | 1.42±2.00 | 0.960 | |
| Reproduction | 0.00±0.00 | 0.12±0.42 | 0.015* | |
| Financial | 0.38±0.74 | 0.68±1.25 | 0.056 | |
| Legal/Crime | 0.06±0.29 | 0.01±0.12 | 0.084 | |
| Other Relationships | 1.70±2.13 | 2.09±2.54 | 0.241 | |
| Death | 0.96±1.32 | 0.76±1.16 | 0.246 | |
| Life-Threatening Situations | 0.65±1.39 | 1.32±2.53 | 0.030* | |
| Possessions | 0.03±0.16 | 0.08±0.30 | 0.136 | |
| Core Social-Psychological Characteristic | ||||
| Interpersonal Loss | 2.84±2.18 | 2.61±2.21 | 0.471 | |
| Physical Danger | 1.51±2.02 | 2.38±3.26 | 0.032* | |
| Humiliation | 1.25±1.83 | 1.47±2.00 | 0.433 | |
| Entrapment | 0.97±1.07 | 1.22±1.27 | 0.144 | |
| Role Change/Disruption | 1.65±2.05 | 2.81±4.32 | 0.025* | |
Data are presented as mean ± standard deviation. *p < 0.05.
Table 3.
Zero order correlation between the STRAIN indices and scales assessing early adversity, life events, and recent perceived stress.
Table 3.
Zero order correlation between the STRAIN indices and scales assessing early adversity, life events, and recent perceived stress.
| M±SD | 1 | 2 | 3 | 4 | 5 | ||
|---|---|---|---|---|---|---|---|
| 1 | STRAIN Lifetime Stressor Count | 10.45±10.17 | 0.949* | 0.614* | 0.487* | 0.477* | |
| 2 | STRAIN Lifetime Stressor Severity | 25.17±25.07 | 0.604* | 0.473* | 0.509* | ||
| 3 | CTQ-SF | 39.42±14.33 | 0.331* | 0.472* | |||
| 4 | LEC | 1.66±2.32 | 0.219* | ||||
| 5 | PSS | 17.16±5.91 |
M, mean; SD, standard deviation; CTQ-SF, Childhood Trauma Questionnaire–Short Form; LEC-5, Life Events Checklist for DSM-5; PSS, Perceived Stress Scale; STRAIN, Stress and Adversity Inventory for Adults. Total N = 218. * p < 0.05.
Table 4.
Multiple regression models parameters for the predictive validity for the STRAIN with the Subscales of the STAI, depressive, and anxiety symptoms levels.
Table 4.
Multiple regression models parameters for the predictive validity for the STRAIN with the Subscales of the STAI, depressive, and anxiety symptoms levels.
| STAI State | ||||||
| Model | Adj. R2 | Δ R2 | F | p | SE | β |
| Covariates | 0.23 | 13.97 | <0.001 | 9.64 | - | |
| Covariates + STRAIN Total Stressor Count | 0.35 | 0.12 | 20.47 | <0.001 | 8.86 | 0.44*** |
| Covariates + STRAIN Total Stressor Severity | 0.37 | 0.136 | 21.87 | <0.001 | 8.75 | 0.20*** |
| STAI Trait | ||||||
| Adj. R2 | Δ R2 | F | p | SE | β | |
| Covariates | 0.24 | 14.84 | <0.001 | 10.39 | - | |
| Covariates + STRAIN Total Stressor Count | 0.36 | 0.117 | 21.25 | <0.001 | 9.56 | 0.47*** |
| Covariates + STRAIN Total Stressor Severity | 0.39 | 0.15 | 24.28 | <0.001 | 9.31 | 0.23*** |
| PHQ-9 | ||||||
| Adj. R2 | Δ R2 | F | p | SE | β | |
| Covariates | 0.22 | 12.92 | <0.001 | 4.85 | - | |
| Covariates + STRAIN Total Stressor Count | 0.4 | 0.182 | 24.89 | <0.001 | 4.25 | 0.27*** |
| Covariates + STRAIN Total Stressor Severity | 0.42 | 0.206 | 27.35 | <0.001 | 4.17 | 0.12*** |
| GAD-7 | ||||||
| Adj. R2 | Δ R2 | F | p | SE | β | |
| Covariates | 0.12 | 6.84 | <0.001 | 4.25 | - | |
| Covariates + STRAIN Total Stressor Count | 0.23 | 0.109 | 11.64 | <0.001 | 3.98 | 0.17*** |
| Covariates + STRAIN Total Stressor Severity | 0.24 | 0.121 | 12.39 | <0.001 | 3.94 | 0.08*** |
Covariates: age, sex, level of education, occupation. STAI, State and Trait Anxiety Inventory; PHQ-9, Patient Health Questionaire-9; GAD-7, 7-item Generalized Anxiety Disorder; STRAIN, Stress and Adversity Inventory for Adults. *** p < 0.001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



