
Submitted:
03 December 2024
Posted:
03 December 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background/Objectives: In this study we aimed to assess the impact of Covid-19 pandemic period on the epidemiological trend of thyroid pathology in a university hospital in Romania. Methods: We performed a 6-years retrospective study (2017-2022) including all patients who underwent thyroid surgery, registered in the Pathology Department, Emergency County Hospital, Târgu-Mureș, Romania (n=971). Thyroid lesions were grouped into 3 major categories: (1) benign, non-tumoral, (2) benign, tumoral and (3) malignant, tumoral. To assess the impact of Covid-19 pandemic on the annual rate of thyroid surgeries and thyroid pathology, data were analyzed in comparison: before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. Results: A significant decrease in the mean number of thyroid specimens per year was observed in the Covid-19 and post-Covid-19 period, compared to the previous period (131 versus 192 cases, p=0.0023). Thyroid benign lesions were the most frequent, but their prevalence was significantly lower during the pandemic period (50.8%), compared to the previous period (58.6%) (p=0.017). Benign tumors were rare, revealing similar occurrence rates in both periods. By contrast, the annual rate of malignant tumors increased significantly during Covid-19 and post-Covid-19 period (26.3% versus 35.4%, p=0.002), the most common histopathological type being papillary thyroid carcinoma. Conclusion: Along with Covid-19 pandemic (year 2020), due to reduced access to medical investigations, many thyroid cancers remained undiagnosed in our hospital. Consequently, this has led to an increased prevalence of malignant cases in the years that came after.
Keywords:
Covid-19
; pandemic
; thyroid
; cancer
; impact
1. Introduction
The Covid-19 pandemic, declared by the WHO (World Health Organization) on March 11th 2020, produced major changes worldwide on many different spheres of society, including the economy and public health [1,2]. The novel SARS-CoV-2 virus was first identified in an outbreak in the Chinese city of Wuhan in December 2019 [3]. Covid-19, also known as coronavirus disease, is the infectious illness caused by the SARS-CoV-2 virus, characterized by dry cough, loss of taste or smell, lung complications such as pneumonia and, in the most severe cases, acute respiratory distress syndrome. The virus has spread rapidly to more than 215 countries. Until March 2024 it had infected more than 704 million of people and caused the death of more than 7 million [4]. The new pandemic situation that allocated the medical resources to treat patients with severe forms of SARS-CoV-2 infection, imposed measures with a significant impact on public access to health services, on the quality of curative and preventive care provided for other conditions.
Literature data focused on the impact Covid-19 pandemic on thyroid pathology with a particular interest on neoplastic disorders are scarce [5,6,7]. SARS-CoV-2 infection has been associated with thyroid disorders that can manifest biochemically as thyrotoxicosis, hypothyroidism, as well as nonthyroidal illness syndrome. The virus can affect thyroid function either through a primary thyroid injury or through a secondary pituitary or hypothalamic lesion. The virus enters host cells using a molecular complex involving angiotensin-converting enzyme 2 (ACE2) and transmembrane protease serine 2 (TMPRSS2), both more extensively expressed in the thyroid gland than in the lungs [8,9,10,11]. The mechanisms involved in thyroid dysfunctions could be caused either by the direct effect of the virus, or by an indirect effect through a systemic abnormality of the inflammatory-immune response caused by SARS-CoV-2 infection [9,11].
Pathologies affecting the thyroid gland, and their management can significantly influence the patients’ long-term well-being. Of these, and the most threatening is thyroid cancer, which is the most common endocrine malignancy, accounting for ~2.1% of all cancer diagnoses worldwide.
The incidence of thyroid cancer has significantly increased over the past few decades. Most of this increase is attributed to papillary thyroid cancer (PTC). This trend has been observed in higher-income countries (Republic of Korea, Canada, Italy, France, Israel, Croatia, Austria, U.S.A.), middle-income countries, and even island nations and territories (Cyprus, Cabo Verde, French Polynesia) [12]. In the United States, thyroid cancer is estimated to be the 13th most commonly diagnosed cancer [12] and in urban areas in China it ranks 4th among all malignant tumors in women [13]. Currently, one in 55 U.S.A. women and one in 149 U.S.A. men are expected to be diagnosed with thyroid cancer during their lifetime [12]. The occurrence of thyroid cancer has been linked to radiation exposure, iodine intake, diabetes, obesity, Hashimoto thyroiditis, exogenous estrogen use, and dietary choices [14]. Moreover, the general population's easy access to medical imaging investigation methods has led to the discovery of small, indolent thyroid microcarcinomas.
In this study, we aimed to assess the impact of Covid-19 pandemic period on the epidemiological trend of thyroid pathology in a university hospital in Romania (Mureș County Emergency Hospital), with special emphasis on the diagnosis and outcome of thyroid cancer.
2. Materials and Methods
2.1. Database and Study Design
We performed a 6-years retrospective study including all patients who underwent thyroid surgery and who were registered in the Pathology Department, Emergency County Hospital, Târgu-Mureș, Romania, between January 2017 and December 2022, a time period centered by the year 2020, when the Covid-19 pandemic broke out.
The Ethics Committee of the Emergency County Hospital, Târgu-Mureş approved the study (Letter of Approval no.1727/26.01.2023).
2.2. Pathological Data and Study Groups
All patients who underwent thyroid surgery (total or partial thyroidectomy) between January 2017 and December 2022 were included in the study. Patient demographics (age, gender) and pathological data (complete histopathological diagnosis, tumor’s histology, lymph nodes involvement, extra-thyroidal extension, ect) were all retrieved from institutional database registries and pathological reports.
To assess the impact of Covid-19 pandemic on the annual rate of thyroid surgeries and thyroid pathology in our department data were analyzed in comparison: before Covid-19 (3 years, January 2017 - December 2019) versus Covid-19 and post-Covid-19 (3 years, January 2020- December 2022) period. Different types of thyroid lesions were divided the into 3 separate groups: 1. benign non-tumoral pathology (encompassing nodular and diffuse goiter, Basedow-Graves’ disease, autoimmune thyroiditis, subacute thyroiditis, thyroid tuberculosis, abscess and cysts), 2. benign tumors, 3. malignant tumors.
The histological type of tumor was established according to the 2017 World Health Organization (WHO) Classification of Tumors of Endocrine Organs (15). Benign tumors encompassed follicular adenoma (FA) cases and variants. Other entities including hyalinizing trabecular tumor and encapsulated follicular-patterned thyroid tumors: thyroid tumors of uncertain malignant potential, (TT-UMP) and noninvasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP) were also included in this category due to their indolent, benign biologic behavior, as well as a similar to follicular adenomas post-surgery management, which is clinical follow-up only. Malignant tumors included: (1) papillary thyroid carcinoma (PTC) cases (conventional and variants: follicular, infiltrative; follicular, encapsulated, invasive; papillary microcarcinoma; columnar cell; oncocytic; diffuse sclerosing; cribriform-morular; hobnail; solid-trabecular; spindle cell; clear cell and Warthin-like), (2) follicular thyroid carcinoma (FTC) cases (minimally invasive, encapsulated angioinvasive, widely invasive), (3) poorly differentiated thyroid carcinoma (PDTC) cases, (4) anaplastic thyroid carcinoma (ATC) cases and (5) medullary thyroid carcinoma (MTC) cases. PTCs with poorly differentiated areas were considered as PDTCs, since the presence of poorly differentiated areas in a background of well-differentiated thyroid carcinoma carries out a worse prognostic.
2.3. Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS, version 22, Chicago, USA), Excel 2021 and GraphPad Prism 7 programs. Descriptive statistical analyses were done. The data were expressed as nominal or quantitative variables. The nominal variables were characterized by means of frequencies. The frequencies of the nominal variables were compared using the Chi-squared test. The normal distribution of continuous variables was assessed using the Kolmogorov–Smirnov test or histograms. The distributed continuous variables were expressed as mean +/- standard deviation SD. The student test was applied to compare continuous values with Gaussian distribution. The ANOVA test was used to compare several mean values. We analyzed the data in a comparative way between two periods: before Covid-19 (3 years, 2017-2019) and Covid-19 and post-Covid-19 period (3 years, 2020-2022). To compare parametric data, the exact Fisher test was applied. The level of statistical significance was set at p<0.05.
3. Results
3.1. Patient Characteristics
A total of 971 thyroid specimens were registered in our department over the study period: 578 (59.5%) cases before Covid-19 period and 393 (40.5%) cases in the Covid-19 and post-Covid-19 period. Among the 578 cases registered between 2017-2019, 510 (88.1%) were women and 68 (11.9%) were men, the women/men (W/M) ratio being 7.5/1; the mean age at diagnosis was 52.37 years-old (range 18-85 years). With regard to the second study period (during Covid-19 and post Covid-19 period), among the 393 patients submitted to surgery, 339 (86.3%) were women and 54 (13.7%) were men (W/N ratio: 6.2/1); the mean age at diagnosis was 52.05 years-old (range 7-86 years). Interesting to note was that men who underwent surgery during Covid-19 pandemic were significantly older compared to those who underwent surgery before Covid-19 pandemic (60 years-old versus 54 years-old, p=0.002).
A significant decrease in the mean number of thyroid specimens per year was observed in the Covid-19 and post-Covid-19 period, compared to the previous period (131 cases [95%CI: 31.73-230.3] versus192 cases [95%CI: 153.1-232.3], p=0.0023). The most spectacular reduction in the number of thyroid surgeries occurred in 2020 (n=95 versus n=197 cases in the precedent year, 2019, p=0.001) (Figure 1). In 2022, the number of thyroid surgeries was again similar to those performed in 2017, prior to Covid-19 pandemic.
Table 1 summarizes the frequency of different thyroid lesions/tumors in comparison before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. During both study periods, the highest prevalence was observed for benign non-tumoral thyroid lesions, followed by malignant and benign thyroid tumors, respectively.
Figure 2 illustrates the prevalence and epidemiological trend of the three study groups (benign non-tumoral lesions, benign and malignant tumors, respectively) over the entire study period (between 2017-2022).
3.2.1. Benign Non-Tumoral Pathology Group
Benign non-tumoral thyroid lesions represented more than half of the cases in our study population. However, a consistent reduction in their percentage (among all thyroid lesion types) was observed during the pandemic period (50.8%), compared to the previous period (58.6%) (p=0.017).
The demographic characteristics of the patients belonging to this group are listed in Table 2. In both study periods, most of the cases occurred in women, but a slight decreasing trend of the gender gap was observed between 2020-2022 (W/M ratio 9.2/1 versus 7.3/1). The patients’ average age was 53 years-old for both periods. Interestingly, men who underwent surgery during the pandemic were significantly older compared to those admitted for surgical treatment between 2017-2019 (60 years-old versus 54 years-old, p=0.002).
3.2.2. Benign Thyroid Tumors Group
Benign thyroid tumors were rare, revealing similar occurrence rates in both periods: 87 cases (15.1%) in the first period versus 54 cases (13.8%) in the second period (p=0.579).
The demographic characteristics of the patients belonging to this group are listed in Table 2. No significant differences were observed between the two study periods. The patients’ mean age was 49 and 51 years-old between 2017-2019 and 2020-2022, respectively. In both study periods, most of the cases occurred in women (W/M ratio 7.7/1 versus 6.8/1).
Table 4 summarizes the frequencies of benign thyroid tumors and their different histology in comparison, before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. The most frequent tumor type in this category was follicular adenoma [52.9% (2017-2019) versus 40.7% (2020-2022), p=0.170], followed by encapsulated follicular-patterned thyroid tumors (non-invasive) (32.2% versus 44.4%, p= 0.154). Even though variations in the proportion of these cases were observed between the two study periods (decreasing trend for adenomas and increasing trend for encapsulated follicular-patterned thyroid tumors), no statistically significant differences in the annual rates were recorded.
Hürthle cell adenoma cases were less frequent and revealed a similar prevalence trend in the two study periods (14.9% versus 12.9%, p=0.808); hyalinizing trabecular tumor cases were extremely rare.
3.2.3. Malignant Thyroid Tumors Group
Two hundred ninety-one (n=291) cases of malignant thyroid tumors were registered in our department over the study period. The annual rate of malignant tumors increased significantly during Covid-19 and post-Covid-19 period (35.4%, CI (95%) [11.91 to 40.27] versus 26.3%, p=0.002), the most common histopathological type being PTC. The highest prevalence was observed in 2021 (41.1%) and 2022 (33.9%). Three years after the pandemic outbreak, the cancer prevalence remains higher than the average rate observed in the pre-Covid years (Figure 3).
Regarding demographic characteristics of the study cases (Table 2), our data revealed that male patients with malignant thyroid tumors during Covid-19 and post-Covid-19 period were younger compared to men diagnosed in the pre-Covid period (48.87 years-old versus 54.65 years-old), although the difference did not reach statistical difference (p=0.186). We also noticed that during Covid-19 and post-Covid-19 period, men diagnosed with malignant thyroid tumors were significantly younger than men diagnosed with benign, non-tumoral lesions in the same period (48.47 versus 60.83 years-old, p=0.002). The female gender was predominant but compared to the benign non-tumoral and tumoral lesions, the gender disparity was lower [the W/M ratio was 4.6/1 versus 9.2/1 or 7.7/1 (2017-2019) and 5.3/1 versus 7.3/1 or 6.8/1 (2020-2023), respectively].
The prevalence of different types of malignant thyroid tumors is shown in Table 5 in comparison, before Covid-19 versus Covid-19 and post-Covid-19 period.
The most common type of thyroid cancer was PTC in both study periods, accounting for 118 (77.6%) and 124 (89.2%) cases, respectively. A statistically significant increase in the annual rate of PTC was observed in the Covid-19 and post-Covid-19 period, compared to the previous years (p=0.011). Other malignant tumor types (FTC, Hurthle cell carcinoma, PDTC, ATC) were rare both periods. A significant decrease in the prevalence of medullary thyroid carcinoma, a rare tumor in general, was observed during the second period compared to 2017-2019 interval (4 cases - 2.9% versus 15 cases- 9.9%, p=0.017].
When analyzing the histology of PTC and its variants (Table 6), for both study periods, most PTC cases corresponded to conventional PTCs (51.8% versus 41.2%). The proportion of small thyroid tumors, namely papillary thyroid microcarcinomas (≤1 cm) remained constant throughout the two studied periods (19.5% versus 20.9%, p=0.873).
4. Discussion
Since the outbreak of the Covid-19 pandemic, many scientific articles were published about SARS-CoV-2 virus and its related pathology [2,16,17]. Nevertheless, there are still few that have assessed to the impact of this pandemic situation on the management of other pathologies, that do not represent life-threatening emergencies (eg. thyroid diseases). The aim of the present study was to investigate the impact of Covid-19 pandemic period on the epidemiological trend of thyroid pathology in a university hospital in Romania (Mureș County Emergency Hospital), with special emphasis on the diagnosis and outcome of thyroid cancer.
It is well known that the global prevalence of thyroid disease is high and continues to rise, thyroid goiter being by far the most common form of thyroid disorder. Most thyroid pathologies do not require surgical intervention and can be effectively managed through alternative approaches (oral treatment, clinical or imaging follow-up) and only a limited ratio of patients diagnosed with thyroid diseases experience oncological or clinically severe thyroid disorders. Surgical considerations are recommended in cases associated with symptoms of cervical compression, hyperthyroidism that is refractory to treatment, and high suspicion of malignancy.
In pandemic crisis, social distancing and/or social isolation were the most recommended and even imposed protection measures against the spread of Sars-CoV-2 virus [18]. The access of the general population to the medical services was limited [19,20,21,22]. According to the WHO guidelines, the medical services were classified as essential or non-essential, which allowed resources to be redirected to the pandemic response. This has caused cancellations or delays in elective and non-urgent procedures, like most of those involving thyroid pathology. Other important reasons why patients avoided medical services were: the fear of contagion [19,23,24], perception that the medical services will not be of a high standard [19,25] and not in the end, worsening socioeconomic situation of the population. Moreover, there was a rapid conversion of the classic face-to-face consultation to telemedicine (online consultation, telephone, video call, ect), which accounted for up to 80% of all consultations according to published data [26]. The remote examination of the patient with thyroid nodules, without a physical and ultrasound examination of the thyroid, is defective and involves the risk of missing the diagnosis of nodules that require surgical treatment. Further on, the pandemic has also led to a drastic reduction in the frequency of fine needle aspiration biopsies of the thyroid nodules. During Covid-19 pandemic, this procedure has become extremely rare, performed only for highly selected cases, which has led to a decrease of up to 98% of its frequency, as reported by previous studies [27].
In line with all these arguments, the results of our study also revealed a significant decrease in the number of thyroid surgeries performed during the Covid-19 period compared to the previous period. This decrease was particularly notable in the year 2020, the hotspot of the Covid-19 pandemic. Nevertheless, the annual rate of malignant tumors in our study increased significantly during Covid-19 and especially during post-Covid-19 period (p=0.002), PTC being the most common histopathological type. The highest prevalence of thyroid cancer was observed in 2021 (41.1%), the first year following the pandemic outbreak.
Our results are similar to those recently reported by other Romanian authors analyzing data from different territorial regions in Romania [28,29]. In their study, Popa O et al. also observed a significantly higher prevalence of more aggressive pathological thyroid tumor types in the POSTCOVID group (17.7%) compared to the PRECOVID group (7.6%; p=0.0006). In their study performed in South Korea (2019-2021), Seong Hoon Kim et al. have reported a persistent increasing trend in the incidence of thyroid malignant tumors despite the reduced thyroid surgical interventions [30]. Additionally, the authors of this study also emphasized that the proportion of worse prognostic factors (extrathyroidal extension, lymphatic invasion, vascular invasion, and neck lymph node metastasis) was significantly higher among PTC patients diagnosed the Covid-19 outbreak. A plausible explanation could be the delay in diagnosis and surgical interventions as healthcare systems were reorganized in accordance to the pandemic-related challenges, patients may have faced delays in seeking medical attention, diagnostic procedures and elective surgeries.
The proportion of small thyroid tumors, namely papillary thyroid microcarcinomas (≤1 cm) remained constant throughout the two studied periods, which can be explained by the indolent clinical behavior characteristic for these tumors. Thyroid microcarcinomas generally do not cause symptoms or complications that require immediate or urgent surgery. In many cases, these tumors are discovered accidentally, usually during imaging investigations for other conditions or during routine exams. Indeed, studies have reported an increasing thyroid tumor size in cases diagnosed in the pandemic study groups (4.0 ±1.9 cm- 2020 year, 4.3± 2.3 cm- 2021 year) compared to the group Before COVID-19 (3.5 ±2.2 cm- 2019 year) [30]. The more frequent diagnosis of larger tumors during the Covid-19 period may be associated with the onset of cervical compressive symptoms, leading to prompt surgical intervention without significant delays. On the other hand, cervical discomfort experienced by some individuals during the Covid-19 pandemic might have been associated with Sars-CoV-2 infection. This connection could have led to prompt diagnosis of thyroid tumors, subsequently resulting in timely referrals to surgical services.
It has been reported that thyroid gland is vulnerable to SARS-CoV-2 infection [9,11,31]. Many studies have analyzed the functional aspect of the thyroid and have observed thyroid dysfunctions in patients diagnosed with SARS-CoV-2 infections [5,6,9,32,33]. Histopathological studies on thyroid specimens from SARS-CoV-2 infected patients have revealed severe destruction of parafollicular and follicular epithelial cells leading to follicle rupture [8]. However, no study has demonstrated a direct association between SARS-Cov-2 infection and thyroid cancer. The increase proportion of malignant thyroid tumors during Covid-19 and post-Covid-19 period could be rather related to an improved screening of the patients with thyroid nodules who were referred for surgical evaluation in that period. Moreover, the patients seeking medical services during the Covid-19 period had specific and urgent reasons, rather than routine visits. The surge in cases of malignant tumors during the pandemic years when nearly all medical services were limited, does not represent a real increase. Rather, it reflects the fact that a considerable number of tumor cases were deferred and diagnosed later due to the reorganization of the health system and the prioritization of the Covid crisis instead of chronic diseases.
With regard to the gender distribution of thyroid pathology we did not observe significant changes before and after the appearance of the SARS-coV-2 virus. However, although women were the most affected in both periods, the gender disparity (W/M ratio) was lower in the malignant thyroid tumors group [4.6/1 vs. 7.7/1 vs. 9.2/1 (2017-2019) and 5.3/1 vs. 6.8/1 vs. 7.3/1 (2020-2023), respectively]. Thyroid cancer has always been more common in women than men. A large study (1983-2017, USA) aiming to examine the gender differences in thyroid cancer incidence has reported a W/M ratio of 4.28/1 in patients diagnosed with small localized PTCs, that was reduced to 2.41/1 when larger and higher stage PTCs were considered [34]. In a meta-analysis of 12 pooled study populations, the autopsy prevalence of subclinical PTC was 14.0% in women and 10.8% in men [34]. Some experts have proposed the link between female hormonal factors and thyroid cancer [35,36]. Systematic review, in vitro and experimental studies using animal models aiming to assess a possible link between estrogens and thyroid cancer have demonstrated weak and discordant data and no consistent association between thyroid cancer risk and estrogens [35,37,38]. Since the incidence rate are similar for both women and men, as cancer lethality increases, it has been suggested that higher rates of thyroid cancer could be attributed to women's greater engagement in health care and to gender differences in healthcare utilization and patterns of clinical thinking in which women are subject to over detection and men may be at risk of under detection. In line with these observations, in our study, we noticed a decreasing trend in the W/M ratio as the histopathological diagnosis became more and more severe. The highest W/M ratio was found in the benign non-tumoral lesions group, while the lowest W/M ratio was seen in the malignant tumors group, in both time periods.
In our study population, we also found that during Covid-19 and post-Covid-19 period, male patients diagnosed with malignant thyroid tumors were younger compared to men diagnosed with malignant tumors in the pre-Covid period. This observation might be attributed to the fact that surgeons may have selected younger patients to minimize the risk of serious illness from Covid-19 or the older patients opted against surgery hospitalization in a period when hospitals were considered hotspots for infection.
Thyroid cancer is the only type of cancer in which patient’s age is used as a prognostic factor included in the TNM staging system. With the same degree of cancer involvement, patients aged < 55 have a distinctly different prognosis than those aged > 55 [39]. The reasons for this age-based different prognosis are not entirely clear, but it is assumed that older age, in addition to the changes of the thyroid tissue, is also involved in the loss of radioiodine avidity [39].
5. Conclusions
Our study highlights how unexpected crises, like the Covid-19 pandemic, can have far-reaching effects on healthcare practices beyond their direct implications, herein including the management and prevalence trend of thyroid pathology.
After the onset of the Covid-19 pandemic, in the beginning of 2020, the number of thyroid surgeries decreased dramatically in our hospital and were mainly reserved for elective cases, with high suspicion for malignancy. Further on, due to reduced access to medical investigations by the end of 2020, many thyroid cancers remained undiagnosed. Consequently, this has led to an increased prevalence of malignant cases in the years that came after. This aspect should be monitored carefully because the delay in screening programmers and planned examinations impacts the outcome of thyroid cancer patient. Further, larger studies are needed to confirm our observations.
Author Contributions
Conceptualization, RTC, ANB and AB; Methodology, RTC, ANB and AB; Software: AZ; Validation, RTC, ANB and AB; Formal analysis: AZ; Investigation: RTC, ADM and and GNR; Resources: RTC, ANB, and AB; Data Curation: RTC, ANB, AZ, ADM and GNR; Writing – Orig-inal Draft Preparation: RTC; Writing – Review &Editing: ANB and AB; Visualization: ANB; Su-pervision: AB; Project Administration, RTC; Funding Acquisition, not applicable.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the Emergency County Hospital, Târgu-Mureş, Romania (Letter of Approval no.1727/26.01.2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions (personal data protection of the patients included in the study).
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomedica 2020, 91. [Google Scholar]
- Huang, X.; Wei, F.; Hu, L.; Wen, L.; Chen, K. Epidemiology and Clinical Characteristics of COVID-19. Arch Iran Med 2020, 23. [Google Scholar] [CrossRef]
- Pradesh, U.; Pandit, P.; Dayal, D.; Pashu, U.; Vigyan, C.; Evam, V.; Pradesh, U.; Zoonosis, S. De; Pereira, S.; Pereira, D.; et al. Coronavirus Disease 2019 – COVID-19 Kuldeep Dhama, Preprints (Basel) 2020.
- WHO Coronavirus Disease (COVID-19) Pandemic, World Health Organization (WHO).
- Darvishi, M.; Nazer, M.R.; Shahali, H.; Nouri, M. Association of Thyroid Dysfunction and COVID-19: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne) 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Lui, D.T.W.; Tsoi, K.H.; Lee, C.H.; Cheung, C.Y.Y.; Fong, C.H.Y.; Lee, A.C.H.; Tam, A.R.; Pang, P.; Ho, T.Y.; Law, C.Y.; et al. A Prospective Follow-up on Thyroid Function, Thyroid Autoimmunity and Long COVID among 250 COVID-19 Survivors. Endocrine 2023, 80. [Google Scholar] [CrossRef] [PubMed]
- Khoo, B.; Tan, T.; Clarke, S.A.; Mills, E.G.; Patel, B.; Modi, M.; Phylactou, M.; Eng, P.C.; Thurston, L.; Alexander, E.C.; et al. Thyroid Function Before, During, and after COVID-19. Journal of Clinical Endocrinology and Metabolism 2021, 106. [Google Scholar] [CrossRef] [PubMed]
- Duntas, L.H.; Jonklaas, J. COVID-19 and Thyroid Diseases: A Bidirectional Impact. J Endocr Soc 2021, 5. [Google Scholar] [CrossRef]
- Scappaticcio, L.; Pitoia, F.; Esposito, K.; Piccardo, A.; Trimboli, P. Impact of COVID-19 on the Thyroid Gland: An Update. Rev Endocr Metab Disord 2021, 22. [Google Scholar] [CrossRef]
- Naguib, R. Potential Relationships between COVID-19 and the Thyroid Gland: An Update. Journal of International Medical Research 2022, 50. [Google Scholar] [CrossRef]
- Murugan, A.K.; Alzahrani, A.S. Sars-Cov-2: Emerging Role in the Pathogenesis of Various Thyroid Diseases. J Inflamm Res 2021, 14. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Schneider, A.B. Epidemiology of Thyroid Cancer. Cancer Epidemiology Biomarkers and Prevention 2022, 31. [Google Scholar] [CrossRef]
- Wu, J.; Zhao, X.; Sun, J.; Cheng, C.; Yin, C.; Bai, R. The Epidemic of Thyroid Cancer in China: Current Trends and Future Prediction. Front Oncol 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Ashorobi, D.; Lopez, P.P. Cancer, Follicular Thyroid; 2020.
- Juan Rosai, R.Y.O.G.K.R.V.L. WHO Classification of Tumours of Endocrine Organs; 2017;
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Abrahao-Machado, L.F.; Dahal, S.; Kumar, H.; Kv, D. Origin, Transmission, Diagnosis and Management of Coronavirus Disease 2019 (COVID-19). Postgrad Med J 2020, 96. [Google Scholar]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. New England Journal of Medicine 2020, 382. [Google Scholar] [CrossRef] [PubMed]
- Correction to Lancet Infect Dis 2020; Published Online March 23. Https://Doi.Org/10.1016/S1473-3099(20)30162 (The Lancet Infectious Diseases, (S1473309920301626), (10.1016/S1473-3099(20)30162-6)). Lancet Infect Dis 2020, 20. [CrossRef]
- Pujolar, G.; Oliver-Anglès, A.; Vargas, I.; Vázquez, M.L. Changes in Access to Health Services during the COVID-19 Pandemic: A Scoping Review. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Zhang, Y.N.; Chen, Y.; Wang, Y.; Li, F.; Pender, M.; Wang, N.; Yan, F.; Ying, X.H.; Tang, S.L.; Fu, C.W. Reduction in Healthcare Services during the COVID-19 Pandemic in China. BMJ Glob Health 2020, 5. [Google Scholar] [CrossRef]
- Tsioufis, K.; Chrysohoou, C.; Kariori, M.; Leontsinis, I.; Dalakouras, I.; Papanikolaou, A.; Charalambus, G.; Sambatakou, H.; Siasos, G.; Panagiotakos, D.; et al. The Mystery of “Missing” Visits in an Emergency Cardiology Department, in the Era of COVID-19.; a Time-Series Analysis in a Tertiary Greek General Hospital. Clinical Research in Cardiology 2020, 109. [CrossRef]
- Diaz, A.; Sarac, B.A.; Schoenbrunner, A.R.; Janis, J.E.; Pawlik, T.M. Elective Surgery in the Time of COVID-19. Am J Surg 2020, 219. [Google Scholar] [CrossRef]
- Halley, M.C.; Stanley, T.; Maturi, J.; Goldenberg, A.J.; Bernstein, J.A.; Wheeler, M.T.; Tabor, H.K. “It Seems like COVID-19 Now Is the Only Disease Present on Earth”: Living with a Rare or Undiagnosed Disease during the COVID-19 Pandemic. Genetics in Medicine 2021, 23. [Google Scholar] [CrossRef]
- Karavadra, B.; Stockl, A.; Prosser-Snelling, E.; Simpson, P.; Morris, E. Women’s Perceptions of COVID-19 and Their Healthcare Experiences: A Qualitative Thematic Analysis of a National Survey of Pregnant Women in the United Kingdom. BMC Pregnancy Childbirth 2020, 20. [Google Scholar] [CrossRef]
- Hailemariam, S.; Agegnehu, W.; Derese, M. Exploring COVID-19 Related Factors Influencing Antenatal Care Services Uptake: A Qualitative Study among Women in a Rural Community in Southwest Ethiopia. J Prim Care Community Health 2021, 12. [Google Scholar] [CrossRef]
- Gilbert, A.W.; Billany, J.C.T.; Adam, R.; Martin, L.; Tobin, R.; Bagdai, S.; Galvin, N.; Farr, I.; Allain, A.; Davies, L.; et al. Rapid Implementation of Virtual Clinics Due to COVID-19: Report and Early Evaluation of a Quality Improvement Initiative. BMJ Open Qual 2020, 9. [Google Scholar] [CrossRef]
- Smulever, A.; Abelleira, E.; Bueno, F.; Pitoia, F. Thyroid Cancer in the Era of COVID-19. Endocrine 2020, 70. [Google Scholar] [CrossRef] [PubMed]
- Popa, O.; Barna, R.A.; Borlea, A.; Cornianu, M.; Dema, A.; Stoian, D. The Impact of the COVID-19 Pandemic on Thyroid Nodular Disease: A Retrospective Study in a Single Center in the Western Part of Romania. Front Endocrinol (Lausanne) 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Feier, C.V.I.; Muntean, C.; Faur, A.M.; Blidari, A.; Contes, O.E.; Streinu, D.R.; Olariu, S. The Changing Landscape of Thyroid Surgery during the COVID-19 Pandemic: A Four-Year Analysis in a University Hospital in Romania. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Min, E.; Hwang, Y.M.; Choi, Y.S.; Yi, J.W. Impact of COVID-19 Pandemic on Thyroid Surgery in a University Hospital in South Korea. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef]
- Chen, W.; Tian, Y.; Li, Z.; Zhu, J.; Wei, T.; Lei, J. Potential Interaction between SARS-CoV-2 and Thyroid: A Review. Endocrinology (United States) 2021, 162. [Google Scholar] [CrossRef]
- Jafarzadeh, A.; Nemati, M.; Jafarzadeh, S.; Nozari, P.; Mortazavi, S.M.J. Thyroid Dysfunction Following Vaccination with COVID-19 Vaccines: A Basic Review of the Preliminary Evidence. J Endocrinol Invest 2022. [Google Scholar] [CrossRef]
- Allam, M.M.; El-Zawawy, H.T.; Ahmed, S.M.; Aly Abdelhamid, M. Thyroid Disease and Covid-19 Infection: Case Series. Clin Case Rep 2021, 9. [Google Scholar] [CrossRef]
- LeClair, K.; Bell, K.J.L.; Furuya-Kanamori, L.; Doi, S.A.; Francis, D.O.; Davies, L. Evaluation of Gender Inequity in Thyroid Cancer Diagnosis. JAMA Intern Med 2021, 181. [Google Scholar] [CrossRef]
- Moleti, M.; Sturniolo, G.; Di Mauro, M.; Russo, M.; Vermiglio, F. Female Reproductive Factors and Differentiated Thyroid Cancer. Front Endocrinol (Lausanne) 2017, 8. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Rinaldi, S.; Biessy, C.; Tjønneland, A.; Halkjær, J.; Fournier, A.; Boutron-Ruault, M.C.; Mesrine, S.; Tikk, K.; Fortner, R.T.; et al. Reproductive and Menstrual Factors and Risk of Differentiated Thyroid Carcinoma: The EPIC Study. Int J Cancer 2015, 136. [Google Scholar] [CrossRef]
- Rahbari, R.; Zhang, L.; Kebebew, E. Thyroid Cancer Gender Disparity. Future Oncology 2010, 6. [Google Scholar] [CrossRef] [PubMed]
- Peterson, E.; De, P.; Nuttall, R. BMI, Diet and Female Reproductive Factors as Risks for Thyroid Cancer: A Systematic Review. PLoS One 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Haymart, M.R. Understanding the Relationship Between Age and Thyroid Cancer. Oncologist 2009, 14, 216–221. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Number of thyroid surgeries per year and their epidemiological trend over the study period (between 2017-2022). The most spectacular reduction in the number of thyroid surgeries occurred in 2020 (n=95).
Figure 1.
Number of thyroid surgeries per year and their epidemiological trend over the study period (between 2017-2022). The most spectacular reduction in the number of thyroid surgeries occurred in 2020 (n=95).
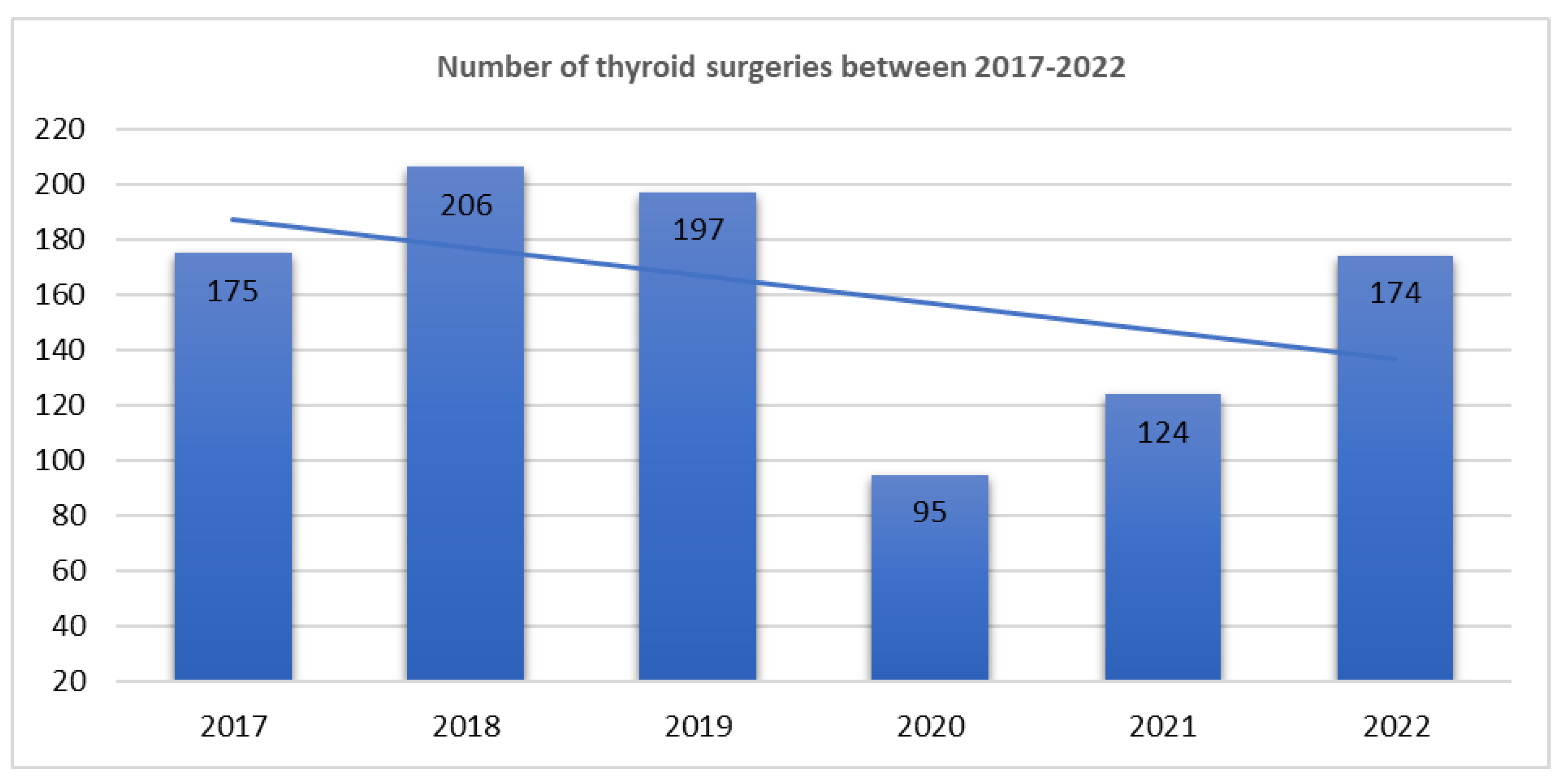
Figure 2.
Epidemiological trend of the three study groups (benign non-tumoral lesions, benign tumors and malignant tumors, respectively) over the study period (between 2017-2022).
Figure 2.
Epidemiological trend of the three study groups (benign non-tumoral lesions, benign tumors and malignant tumors, respectively) over the study period (between 2017-2022).
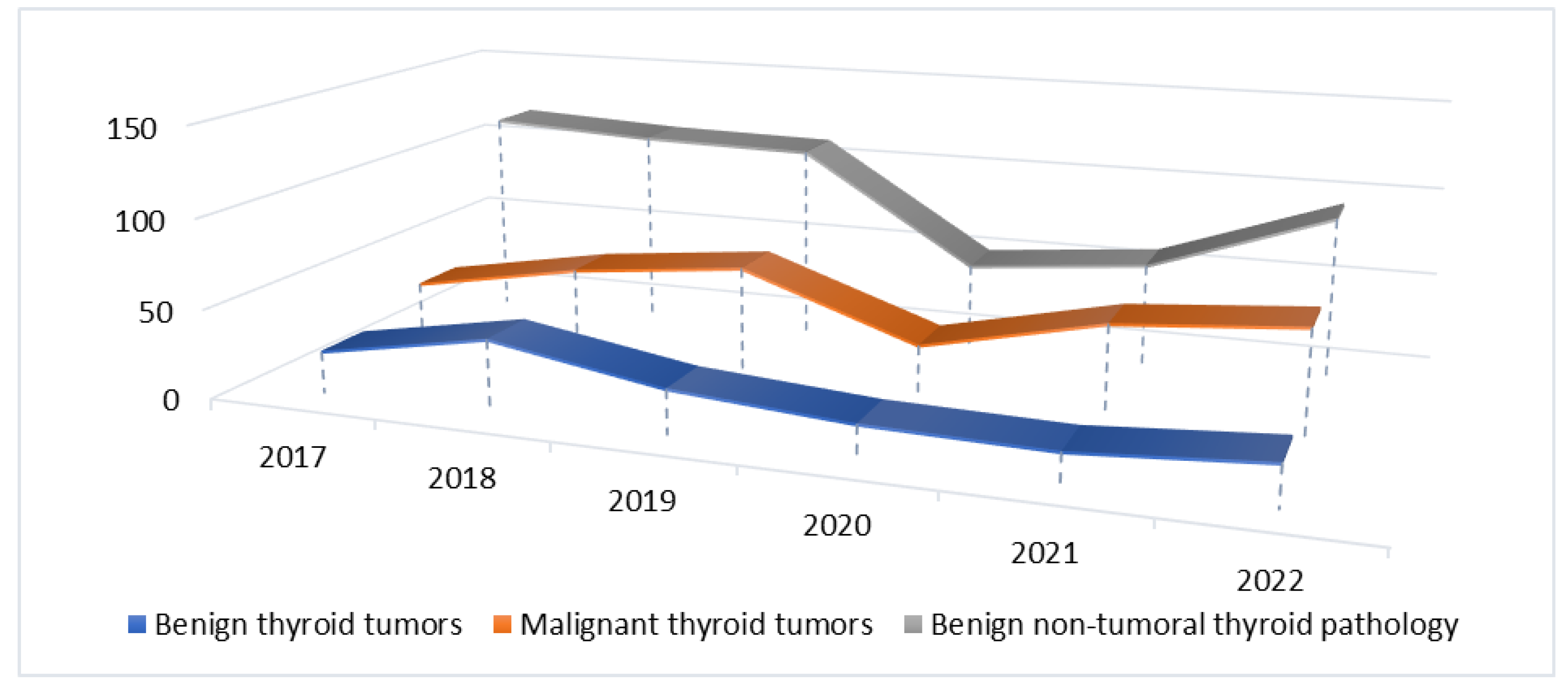
Figure 3.
Number of malignat thyroid tumor cases per year and their epidemiological trend over the study period (between 2017-2022) with respect to the number of thyroid surgeries.
Figure 3.
Number of malignat thyroid tumor cases per year and their epidemiological trend over the study period (between 2017-2022) with respect to the number of thyroid surgeries.
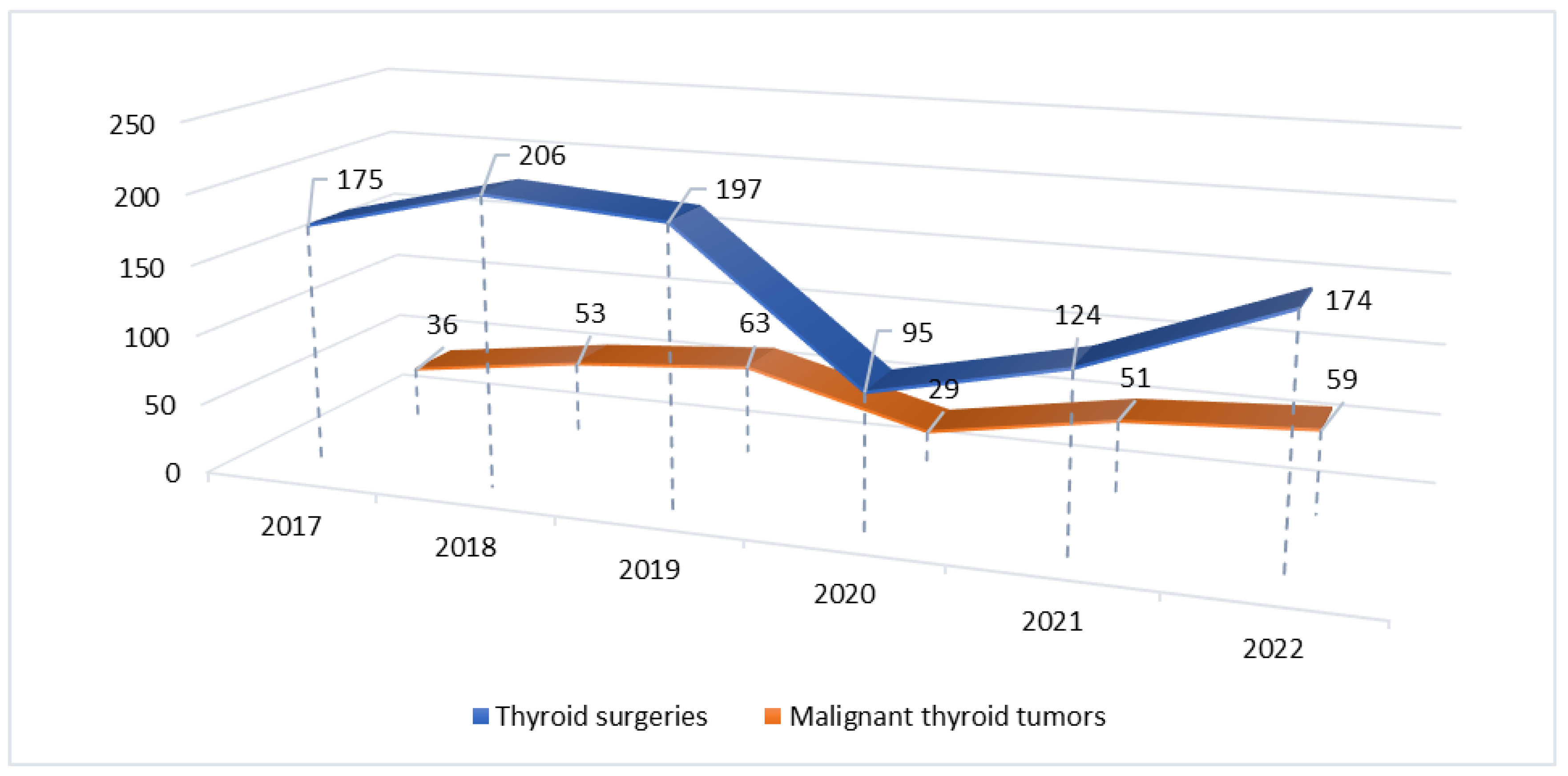

Table 1.
The frequency of different thyroid lesions/tumors in comparison before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period.
Table 1.
The frequency of different thyroid lesions/tumors in comparison before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period.
| Pathology group | 2017-2019 n (%) |
2020-2022 n (%) |
P* |
|---|---|---|---|
| Benign non-tumoral thyroid lesions | 339 (58.6) | 200 (50.8) | 0.017 |
| Benign thyroid tumors | 87 (15.1) | 54 (13.8) | 0.579 |
| Malignant thyroid tumors | 152 (26.3) | 139 (35.4) | 0.002 |
| Total | 578 (59.5%) | 393 (40.5%) |
Table 2.
Demographic characteristics of the patients included in the study, in comparison before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020 -2022) period, for the three study groups.The distribution of different types of benign, non-tumoral thyroid lesions is highlighted in Table 3, in comparison before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. The most frequent lesion was nodular goiter (79% versus 84.5%), followed by autoimmune thyroid disease: autoimmune thyroiditis (7.9% versus 7.5%) and Basedow-Graves’ disease (7.1% versus 5.5%). Cases of diffuse goiter (3.9% versus 1%), thyroid cysts (1.5% versus 1%) or subacute thyroiditis (0.3% versus 0%) were rare. No significant differences were observed in the annual rate for none of these thyroid lesions between the two studied periods.
Table 2.
Demographic characteristics of the patients included in the study, in comparison before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020 -2022) period, for the three study groups.The distribution of different types of benign, non-tumoral thyroid lesions is highlighted in Table 3, in comparison before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. The most frequent lesion was nodular goiter (79% versus 84.5%), followed by autoimmune thyroid disease: autoimmune thyroiditis (7.9% versus 7.5%) and Basedow-Graves’ disease (7.1% versus 5.5%). Cases of diffuse goiter (3.9% versus 1%), thyroid cysts (1.5% versus 1%) or subacute thyroiditis (0.3% versus 0%) were rare. No significant differences were observed in the annual rate for none of these thyroid lesions between the two studied periods.
|
Pathology group |
2017-2019 | 2020-2022 | p | ||||||||
|
Average age (years) |
W/ M ratio | Average age for men (years) | Average age for women (years) | Average age (years) | W/M ratio | Average age for men (years) | Average age for women (years) | Average age | Average age for men (years) | Average age for women (years) | |
| Benign non-tumoral thyroid pathology | 53.59 |
9.2/1 |
54.43 |
53.48 | 53.67 |
7.3/1 |
60.83 |
52.69 | 0.552 | 0.002 | 0.556 |
| Benign thyroid tumors | 49.73 |
7.7/1 |
50.90 |
49.58 | 51.90 |
6.8/1 |
51.68 |
53.42 | 0.363 | 0.694 | 0.419 |
| Malignant thyroid tumors | 50.96 |
4.6/1 |
54.64 |
50.10 | 49.57 |
5.3/1 |
48.47 |
48.71 | 0.356 | 0.186 | 0.542 |
Table 3.
Distribution of different types of benign, non-tumoral thyroid lesions in comparison, before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. .
Table 3.
Distribution of different types of benign, non-tumoral thyroid lesions in comparison, before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. .
| Benign, non-tumoral thyroid lesions | 2017-2019 N (%) |
2020-2022 N (%) |
P* |
|---|---|---|---|
| Nodular goiter | 268 (79) | 169 (84.5) | 0.139 |
| Diffuse goiter | 13 (3.9) | 2 (1) | 0.060 |
| Basedow-Graves’ disease | 24 (7.1) | 11 (5.5) | 0.588 |
| Autoimmune thyroiditis | 27 (7.9) | 15 (7.5) | 0.990 |
| Cysts | 5 (1.5) | 2 (1) | 0.990 |
| Subacute thyroiditis | 1 (0.3) | 0 | - |
| Thyroid tuberculosis | 1 (0.3) | 0 | - |
| Thyroid abscess | 0 | 1 (0.5) | - |
| Total | 339 (56.8) | 200 (50.8) | 0.017 |
*The parametric Fisher test was applied, the p-value was obtained by comparing the prevalence of different benign non-tumoral thyroid lesions in our institution between 2017-2019 versus 2020-2022.
Table 4.
Distribution of different types of benign thyroid tumors in comparison, before Covid- 19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period.
Table 4.
Distribution of different types of benign thyroid tumors in comparison, before Covid- 19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period.
| Benign thyroid tumors | 2017-2019 N (%) |
2020-2022 N (%) |
P* |
|---|---|---|---|
| Follicular adenoma | 46 (52.9) | 22 (40.7) | 0.170 |
| Hürthle cell adenoma | 13 (14.9) | 7 (12.9) | 0.808 |
| Hyalinizing trabecular tumor | 0 | 1 (2) | - |
| Other encapsulated follicular-patterned thyroid tumors (non-invasive) | 28 (32.2) | 24 (44.4) | 0.154 |
| Thyroid tumor of uncertain malignant potential (TT-UMP) | 9 (32.2) | 10 (41.6) | 0.151 |
| Noninvasive follicular thyroid neoplasm with papillary- like nuclear features (NIFTP) | 19 (67.8) | 14 (58.4) | 0.782 |
| Total | 87 (15.1) | 54 (13.8) | 0.579 |
* The parametric Fisher test was applied; the p-value was obtained by comparing the prevalence of different histopathological types of benign thyroid tumors in our institution between 2017-2019 versus 2020-2022.
Table 5.
Distribution of different types of malignant thyroid tumors in comparison, before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. .
Table 5.
Distribution of different types of malignant thyroid tumors in comparison, before Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period. .
| Malignant thyroid tumors | 2017-2019 N (%) |
2020-2022 N (%) |
P* |
|---|---|---|---|
| Papillary thyroid carcinoma | 118 (77.6) | 124 (89.2) | 0.011 |
| Follicular thyroid carcinoma | 1 (0.80) | 0 | - |
| Hürthle cell carcinoma | 0 | 2 (1.4) | - |
| Poorly differentiated thyroid carcinoma | 8 (5.2) | 5 (3.6) | 0.577 |
| Anaplastic thyroid carcinoma | 2 (1.3) | 0 | - |
| Medullary thyroid carcinoma | 15 (9.9) | 4 (2.9) | 0.017 |
| Metastasis | 3 (1.9) | 1 (0.7) | 0.623 |
| Other type (limphoma, angiosarcoma, plasmocitoma) | 5 (3.3) | 3 (2.2) | 0.725 |
| Total | 152 (26.3) | 139 (35.4) | 0.002 |
* The parametric Fisher test was applied, the p-value was obtained by comparing the prevalence of different histopathological types of malignant thyroid tumors in our institution between 2017-2019 versus 2020-2022.
Table 6.
Papillary thyroid carcinoma and its variants: number of cases and their prevalence before. Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period.
Table 6.
Papillary thyroid carcinoma and its variants: number of cases and their prevalence before. Covid-19 (2017-2019) versus Covid-19 and post-Covid-19 (2020-2022) period.
| Papillary thyroid carcinoma | 2017-2019 N (%) |
2020-2022 N (%) |
p |
|---|---|---|---|
| Conventional | 61 (51.8) | 51 (41.2) | 0.121 |
| Follicular variant | 18 (15.3) | 28 (22.7) | 0.189 |
| Papillary microcarcinoma | 23 (19.5) | 26 (20.9) | 0.873 |
| Encapsulated variant | 0 | 1 (0.8) | - |
| Oncocytic variant | 0 | 2 (1.6) | - |
| Warthin-like variant | 3 (2.5) | 6 (4.8) | 0.500 |
| Tall cell variant | 7 (5.9) | 6 (4.8) | 0.780 |
| Hobnail variant | 3 (2.5) | 2 (1.6) | 0.677 |
| Solid- trabecular variant | 3 (2.5) | 0 | - |
| Diffuse sclerosing variant | 0 | 2 (1.6) | - |
| Total | 118 | 124 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



