
Submitted:
26 November 2024
Posted:
26 November 2024
You are already at the latest version
Abstract
Background: The orthodontic therapy management in pediatric patients affected by rare diseases like Ectodermal Dysplasia (ED) and Osteogenesis Imperfecta (OI) requires complex protocols, for presence of dental anomalies in number and structure. Orthodontic management of those dental alterations is different form the traditional one, for anchoring deficiency due to dental anomalies, imposing a skeletal anchoring. Methods: Patients were treated with orthodontic therapy with Maxillary Skeletal Expander (MSE) with miniscrews at the Complex Operative Unit (UOC) of Pediatric Dentistry, Department of Oral and Maxillofacial Sciences, Sapienza, University of Rome, Policlinico Umberto I. After a medical anamnesis, a lateral cephalometric radiograph and a Cone Beam Computer Tomography (CBCT) were performed before therapy to obtain orthodontic diagnosis, verify bone quantity and quality, and create a customized hybrid device. At the end of treatment, the exams were performed again to verify MSE therapy effectiveness. Results: the orthodontic management in pediatric patients affected by rare diseases was achieved due to skeletal anchoring, with results comparable to those not affected. Conclusions: This study analyzes possible orthodontic strategy with aid of orthodontic miniscrews in various clinical cases. MSE with miniscrews therapy is an innovative therapy that finds different clinical applications, even in the most complex cases.
Keywords:
orthodontic miniscrew
; osteogenesis imperfecta
; ectodermal dysplasia
; maxillary skeletal expander (MSE)
1. Introduction
Ectodermal Dysplasia (ED) represents a group of hereditary conditions with prevalence of about 1 / 15,000, in which there are abnormalities of two or more structure of ectoderm, such as hair, teeth, nails, sweat glands, craniofacial structure, and fingers. On extraoral physical examination, these patients present sparse and brittle hair, prominent forehead, pronounced chin, and enlarged nose, abnormal development of some parts of the eye, deformed nails, and dry skin. Oral features are multiple agenesis, such as oligodontia (i.e. absence of 6 or more teeth) or complete anodontia, both of the deciduous and permanent series, enamel defects, malformed teeth, accompanied by problems with salivation [1,2].
ED Patients have a characteristic facial gestalt, which negatively affects self-esteem and quality of life [3]. An early diagnosis and a multidisciplinary approach could improve the quality of life of the patient affected by ED [4].
Osteogenesis Imperfecta (OI) are a heterogeneous group of inherited connective tissue disorders that share similar skeletal abnormalities causing bone fragility and deformity [5]. OI is a rare genetic disease with autosomal dominant transmission, due to anomalies in the synthesis of type I collagen by mutation of the genes COL1A1 and COL1A2. Typical features are increased skeletal fragility, decreased bone mass and other typical manifestations of an altered connective tissue, such as ligamentous laxity, scoliosis, blue sclera (pathognomonic sign), and hearing loss in adulthood, short stature and Dentinogenesis Imperfecta (DI). DI is a group of hereditary autosomal dominant disorders with an incidence of cases of 1: 6000, which causes abnormal dentin formation. The elective therapy of OI are bisphosphonates (BP) taken intravenously from birth, every 3 months. Bisphosphonates (BPs) are indicated in the treatment of OI because they inhibit bone resorption by osteoclasts, thus favoring bone formation over resorption during remodeling. [6].
BPs are synthetic analogues of pyrophosphate, which act by inhibiting number and activity of osteoclasts and reduce bone turnover, reducing risk of bone fracture. BPs are "life-saving" drugs for these children, but unfortunately, from a dental point of view, they present disadvantages: in fact, by inhibiting osteoclasts, they also inhibit orthodontic dental movements.
Patients with osteogenesis imperfecta (OI) are more affected by malocclusion than individuals without OI [7,8].
Orthodontic therapy in these cases of particular pathological conditions should be planned with a multidisciplinary treatment pathway.
Pediatric orthodontic treatment often requires evaluating the most effective anchoring system to ensure therapy success. Indeed, many conditions require anchoring for resolution of skeletal malocclusions, for dental displacements or because of trauma or lack of space. The clinician's task also consists in choosing the most appropriate and indicated method for the individual patient.
In pediatric dentistry, there are different clinical situations associated with the correction of skeletal malocclusions or the need for dental movements limited to pediatric dental emergency conditions that require skeletal anchoring in the planning of orthodontic treatment.
Checking the anchorage during orthodontic treatment is one of the main factors to ensure the success of the therapy. Correct maintenance of the anchorage is the purpose of orthodontic treatment to create appropriate force systems that allow the desired dental movements. Anchorage is the resistance that a tooth or group of teeth offers when subjected to a force [9]. The aim of orthodontic treatment is therefore to maintain sufficient anchorage control to create appropriate force systems that allow the desired tooth displacements. In pediatric dentistry, the main difficulties in using traditional anchoring systems consist in the patient collaboration, in the possible presence of concomitant pathologies and in the need of for multidisciplinary treatment, for example in patients with special needs.
In recent years, dental technology has developed new devices, such as temporary anchorage devices (TADs), which guarantee a stable and reliable skeletal anchorage, even regardless of the patient's collaboration, which have many clinical advantages in different situations. These devices have shown that the management of the anchorage in pediatric dentistry requires a careful approach to research and technological innovations: skeletal anchoring systems can offer valid support in many clinical cases, adapting to different necessity [10].
In cases of lack of space due to early loss of deciduous teeth caused by trauma, destructive carious lesions or systemic pathologies with oral manifestations (such as, for example, osteogenesis imperfecta and ectodermal dysplasia), predictable anchorage management is a determining factor for the success of the therapy and the stability of the long-term outcome.
In these cases, an orthodontic device with skeletal anchoring guarantees better results, fewer side effects and better management of the orthodontic treatment itself. These devices also allow the treatment of cases previously considered difficult, with relative ease of use and greater patient motivation.
Even in patients with special needs, these systems offer great advantages in terms of both compliance and reduction of the treatment duration combined with the safety and control of dental movements and the minimization of side effects, fundamental factors in the overall management of these patients. Indeed, these special need patients require orthodontic treatment to not only correct orofacial problems and improve function, but also aesthetics, and therefore the quality of their life [11]. TADs, including mini plates, implants and mini screws, are widely used to achieve skeletal anchoring and guarantee better control anchorage in orthodontic treatment, achieving more satisfactory and controlled results than could be achieved with conventional orthodontic mechanics, by supporting the anchor teeth or by being an independent anchor unit and are easily removed once their function has been completed.
Because TADs essentially provide an immediate absolute or stationary anchorage, it becomes possible for the clinician to deliver the desired force system using a TAD as anchorage without observing side effects on the anchor teeth. In these situations, anchorage could be set up directly through the use of a TAD (direct anchorage) or indirectly through connecting teeth to a TAD and making this segment of teeth virtually stationary (indirect anchorage). The stability of TADs during treatment and the bone-receiving site are critical in designing the proper appliance, delivering the appropriate force system.
TADs obtain their stability from mechanical retention and do not osseointegrate into bone. TADs are widely used in pediatric dentistry due to their effectiveness, ease of use and versatility of use in more complex cases, and above all for their characteristic of no-compliance appliances. In fact, these orthodontic devices are independent from pediatric patients’ collaboration and allows dental movements monitoring. In fact, these devices allow a correct management of orthodontic forces, transmitted directly to the bone site and are widely used to obtain skeletal maxillary expansion [12,13]. A recent review of the literature analyzes the effect and stability of miniscrew- assisted rapid palatal expansion (MARPE) for the clinical treatment of patients with maxillary transverse deficits (MTD). The authors demonstrate that MARPE could represent an effective treatment for patients with MTD, guaranteeing transverse skeletal expansion even in late adolescence and with less periodontal side effects than conventional rapid palatal expander (RPE) and presenting numerous clinical advantages [14].
For these reasons we decided to use miniscrew- assisted rapid palatal expansion (MARPE) with modified or hybrid TAD-assisted expanders with both dental and skeletal anchoring in special needs pediatric patients. This study describes the orthodontic management using orthodontic miniscrews in pediatric patients with special needs with lack of anchorage, due to systemic diseases associated with widespread agenesis or structural defects dentinal enamel, such as osteogenesis imperfecta and ectodermal dysplasia.
2. Materials and Methods
At the Complex Operative Unit (UOC) of Pediatric Dentistry, Department of Oral and Maxillofacial Sciences, Sapienza, University of Rome, Policlinico Umberto I, we managed two different patients of similar age, growing, in mixed dentition, with maxillofacial alterations and with anchoring deficiencies due to systemic pathologies with oral manifestations, such as Ectodermal Dysplasia (ED) and Osteogenesis Imperfecta (OI). The orthodontic treatment required a Maxillary Skeletal Expander (MSE) with skeletal anchoring.
The patients’ parents provided written informed consent agreeing to undergo the procedure. We accurately planned the protocol of orthodontic expansion and insertion of the mini screws.
In the first phase, we analyzed each case individually through the patient's systemic and physiological anamnesis with also an assessment of the patient's degree of cooperation. Then we evaluated with the pediatrician collaboration the patients’ pharmacological therapies for systemic pathologies and any contraindications to orthodontic treatments.
The therapeutic approach we applied required two clinical phases: the first surgical one, and the second orthodontic. Through clinical and radiographic physical examination such as orthopanoramic and lateral cephalometric radiograph, we performed the orthodontic diagnosis. We carried out the cephalometric analysis on telecranial radiography in a latero-lateral projection and alginate dental impressions for the study models and putty and light silicone impressions for the creation of the customized MSE anchored to the mini screws.
We requested also second level radiographic examinations: a cone beam computer tomography (CBCT). In fact, CBCT analysis allowed evaluation of quality and quantity bone and the design of customized surgical guides for the correct insertion of orthodontic miniscrews.
It was necessary to perform a thermoformed template with two palatal holes filled with gutta-percha to perform CBCT to evaluate the amount of cortical bone available.
The same thermotemplate was then used as a guide for miniscrews’ insertion and a precision silicone impression was taken to create a hybrid MSE.
The designed modified MSE was a hybrid type: dental anchoring given by two bands positioned on the upper first molars and skeletal anchoring provided by miniscrews positioned in the anterior portion of the palate (Miniscrews Imtec ORTHO Implant® of 6 mm in length and 1.8 mm in diameter).
The surgical protocol applied was execution of local anesthesia with vasoconstrictor, perforation of the mucosa with a rosette bur using the thermoformed template, use of a helical drill (0.9 mm or 1.1 mm) with perforation of the first 2-3 mm of the cortex alveolar and orientation in the same direction of screw insertion. We then performed the insertion of the mini screw (self-tapping) manually with the appropriate screwdriver, without exceeding the torsional loads. Disarming was performed manually and without anesthesia. After obtaining primary stability, the implant is immediately loaded with forces from 50g to 250g.
The activation protocol of MSE, cemented with glass ionomer cement, consisted of two activations per day for 15 days, giving instruction to patients' parents to activate the expansion. The expander was kept in place for 6 months for retention.
Occlusal radiographs were taken at the end of active RME therapy to assess the opening of the midpalatal suture suture [13] and after 1 year from the end of active expansion therapy to evaluate the reossification and reorganization of the midpalatal suture and verify the orthodontic therapy efficacy.
3. Cases Reports
3.1. MSE Treatment in Patient with Ectodermal Dysplasia
Ectodermal Dysplasia (ED) represents a group of hereditary conditions with prevalence of about 1 / 15,000, in which there are abnormalities of two or more ectodermal structures, such as hair, teeth, nails, sweat glands, craniofacial structure, and fingers. On extraoral physical examination, these patients present sparse and brittle hair, prominent forehead, pronounced chin, enlarged nose, abnormal development of some parts of the eye. Oral features are multiple agenesis, both of the deciduous and permanent series, enamel defects, malformed teeth.
An 8 y.o. male patient, with hypohydrotic ED and oral respiration came at Complex Operative Unit (UOC) of Pediatric Dentistry, Department of Oral and Maxillofacial Sciences, Sapienza, University of Rome. Extraoral clinical examination showed brachifacial typology, small chin, acute nasolabial angle, protruded lips, prominent and square forehead, protruding superciliary arches, wrinkles and pigmentation of the periocular area, small nose with hypoplastic wings and enlarged root, large ears with low implantation, blonde hair, sparse and thin. Intraoral examination revealed presence of multiple agenesis of both deciduous and permanent series, confirmed by orthopanoramic radiography, hypotrophy of both maxillaries, and in particular, of the upper jaw, contracted in transverse and sagittal planes (Figure 1).
The cephalometric analysis performed on telecranial radiography in a latero-lateral projection showed a first skeletal class with a mild tendency to the third class, hypodivergence and anticlockwise growth and reduced anterior facial height. The designed modified palatal expander was a hybrid type, realized with the same phases previously described.
After the activation, the MSE was kept inactive for 9 months to allow bone apposition at the median palatal suture site. Subsequently, two Schwarz appliance were realized with dental elements added to ensure function and aesthetics (Figure 2).
3.2. MSE Treatment in Patients with Osteogenesis Imperfecta and Dentinogenesis Imperfecta
Osteogenesis Imperfecta (OI) is a rare genetic disease with autosomal dominant transmission due to anomalies in the synthesis of type I collagen due to mutation of genes ColA1 and 2. Typical features are increased skeletal fragility, decreased bone mass and other typical manifestations of an altered connective tissue, such as ligamentous laxity, scoliosis, blue sclerae (pathognomonic sign), and hearing loss in adulthood, short stature and Dentinogenesis Imperfecta (DI). DI is a group of hereditary autosomal dominant disorders with an incidence of cases of 1: 6000, which causes abnormal dentin formation.
The elective OI therapy are bisphosphonates (BPs) taken intravenously from birth, every 3 months. These drugs are synthetic analogues of pyrophosphate, which act by inhibiting number and activity of osteoclasts and reducing bone turnover, decreasing bone fracture risk. BP are "life-saving" drugs for these children, but unfortunately, from a dental point of view, they present many disadvantages: in fact, by inhibiting osteoclasts, they also inhibit orthodontic dental movements.
A validated protocol has been applied at the Complex Operative Unit (UOC) of Pediatric Dentistry, Department of Oral and Maxillofacial Sciences, Sapienza, University of Rome with the Department of Pediatrics, Policlinico Umberto I, for patients who take BP and who should carry out an expansion rapid palatal for orthodontic treatment. In fact, under pediatric medical supervision, BP suspension is carried out for three months. Therefore, orthodontic treatment could be performed, like a rapid maxillary expansion obtaining a good opening of the palatine suture, physiological healing and formation of callus.
A 9 y.o. female patient, affected by OI and Dentinogenesis Imperfecta (DI) and taking intravenous BP from 3 months of age was treated at the Complex Operative Unit (UOC) of Pediatric Dentistry, Department of Oral and Maxillofacial Sciences, Sapienza, University of Rome. Extraoral examination demonstrated blue sclerae, upper jaw hypotrophy, dolic facial type and a concave profile. Intraoral examination showed: DI of deciduous and permanent tooth series, mixed dentition with permanence of tooth elements 5.3, 6.3, 7.3, 7.4, 7.5, 8.3 and 8.5, upper jaw contraction with right lateroposterior crossbite, III skeletal class malocclusion, negative overjet (OJ) and overbite (OB), atypical swallowing and lingual inclination of lower incisors (Figure 3).
The orthopanoramic radiography showed characteristic presence of very large pulp chambers in teeth affected by DI and agenesis of 1.5, 3.5 and 4.5 dental element. The cephalometric analysis carried out on the telecranium in latero-lateral projection confirmed the hypothesis of III class malocclusion of both dental and skeletal type with ANB values of -5.03 ° and Wits index of -3. Maxilla hypotrophy was confirmed by the ANS value of 71.6 °.
In agreement with his pediatrician, BPs intake was suspended for three months with monitoring of Computerized Bone Mineralometry (CBM) values for bone density. The lack of anchorage due to DI was resolved with MSE with palatal orthodontic miniscrews.
A precision silicone impression was taken for realization of a thermoformed template with two palatal holes filled with gutta-percha to perform CBCT to evaluate the amount of cortical bone available
And to realize a hybrid type orthodontic device: two bands on the first molars and connecting eyelets with miniscrews and cemented with glass ionomer cement (Figure 4).
Therefore, a CBCT was performed with an upper template and gutta-percha landmarks. Despite the patient's low bone thickness due to BPs prolonged use, it was possible to insert two orthodontic mini screws 8 mm long (Sweden Signature diameter 1.8 mm).
Then, after antibiotic prophylaxis and BPs infusion suspension for three months according with pediatrician, it was performed palatal anesthesia with vasoconstrictor and miniscrews insertion with the guide of the template.
The activation protocol of MSE, cemented with glass ionomer cement, consisted of two activations per day for 15 days [15], giving instruction to patients' parents to activate the expansion. Then a Petit's mask was applied with 14oz diameter ¾ rubber bands for use for at least 14 hours between day and night. At 3 months, clear improvements were noted with an increase in OJ and OB. At 9 months, the III class malocclusion was completely corrected with maxilla advancement, OJ and OB increased and completion of dental exchange. Transverse correction allowed resolution of right lateroposterior crossbite and bite opening [16].
After the activation, the MSE was kept inactive for 9 months to allow bone apposition at the level of the the midpalatal suture and then removed.
Follow-up at 12 months orthopanoramic, we observed exfoliation delay of 6.3 dental element, so we planned 6.3 dental element extraction to facilitate eruption of 2.3 dental element. Cephalometric analysis on control lateral cephalometric radiograph showed an increase in ANS and an ANB value of 0. The mandibular length remained constant, numerically monitored with new radiographic checks following the menarche that occurred this year. Follow-up at 12 months showed a completed permanent dentition with physiological eruption of 2.3. Orthodontic therapy continued with Frankel Type III myofunctional appliance. Given the patient low cooperation, we registered a lack of lingual posture control with a high risk of relapse malocclusion. Meanwhile, systemic therapy for OI was modified with a sperimental protocol with the intake of Denosumab: a new anti-RANK ligand antibody drug that inhibits osteoclasts formation and bone resorption. This new drug is degraded within 3-4 months and has no long-term systemic accumulation like BPs. These advantageous features together with the fewer side effects allow a safer therapy for OI patient, in the growth phase who have to start an orthodontic treatment.
Nowadays we have scheduled follow-up visits to monitor patient growth and increase motivation and collaboration for other orthodontic treatment, if needed.
4. Results
We treated each case individually and the orthodontic therapy was agreed in detail with the pediatrician. According to the article by Hartono et al. [12], we achieved a resolution of malocclusion, with clear opening of the palatine suture and movement of the dental elements with effective cross-sectional problem resolution, without side effects. There was never any mobility or subsidence of the miniscrews, but they were easily removed at the end of the treatment along with the MSE. CBCT was a particularly important help for these patients, because it avoided damage to the permanent teeth, or the one not yet erupted and highlighted areas mostly represented by type D1-2 bone.
The therapy goal was achieved also due to patients’ collaboration, necessary both for the various phases of therapy and for oral hygiene, which always had to be very accurate to avoid failure of the miniscrews and treatment. The surgical phase for the insertion of the miniscrews were managed according to the technique called “tell, show, do”, to obtain greater compliance. The surgical technique adopted was simple and effective and well accepted by all patients treated. The results obtained remained stable over time (Figure 10A: results in ED patient; 10B: results in OI patient) and nowadays we ensure appropriate follow- up of patients.
5. Discussion
After an accurate medical history anamnesis, an orthodontic therapy should correctly manage and identify which forces apply and which counterbalance to use for the orthodontic purpose. Orthodontic treatment should be carried out evaluating several factors, including medical history anamnesis.
Orthodontic therapy is based on dental or bone anchor. Anchoring is the "resistance of unwanted tooth movement" [17] and plays an important role in orthodontic mechanics since the third principle of dynamics enunciated by Newton is valid, according to which, "every action corresponds a reaction of the same intensity, but in the opposite direction" [18]. The dental elements, therefore, which are subject to a desired tooth displacement are called "active units", while those that do not want to move "reactive units" [17]. Moyers argues that: "the usual precautions include: base the anchoring as far as possible outside the arches, for example on the mucous membranes, muscles, skull etc.; extend the anchoring to as many teeth as possible, vary the extent, direction and method of applying the force between the active and resistance elements " [19] and therefore enunciate the search for a non-dental anchor.
The anchor could be classified according to the point of application into intraoral or extraoral. Based on the possibility of displacement of reactive unit teeth is classified in: maximum, when teeth must not undergo any unwanted displacement; medium, when teeth of active unit and those of reactive unit make a displacement of the same amount; minimum, when all the teeth, both of active unit and of reactive unit, are left free to move without any constraints. Based on the number of units involved in the reactive unit, it is divided into single, when the anchor is located on a single dental element; compound, when one or more teeth are used for anchoring; reinforced, when extraoral structures are exploited [20].
The maximum skeletal anchorage is the orthodontic, orthopedic and prosthetic anchorage provided by devices inserted into the bone, such as TADs [21]. These devices, temporarily fixed in the bone, provide direct or indirect anchorage, and are removed when the orthodontic therapy has been finalized [22]. Orthodontic miniscrews are biocompatible TADs with mechanical retention [21], which are used for skeletal anchoring and as bone fixation screws [23]. The more correct term for miniscrews is miniscrews implant [24]. They are widely considered one of the most important revolutions in orthodontics due to their undoubted qualities of versatility, efficiency, ease of use and safety [25].
TADS could also be used in cases where the dental anchor is absent due to a lack of dental elements caused by previous traumatic dental injuries (TDI) or carious lesions. In the assessment of TDI, timely diagnosis and treatment are essential to assess Oral Health-Related Quality of Life (OHRQoL) [26].
Each clinical case should therefore be carefully evaluated, investigating the modalities of the TDI in relation to the dental age of the child in order to effectively solve the problem.
Even in cases of space alterations in the arch, miniscrews could be applied to ensure effective orthodontic anchoring, such as for example in the early loss of deciduous teeth for extractions for destructive carious lesions. Indeed, interceptive orthodontic treatment is essential to manage space for permanent teeth [27]. In recent years, orthodontic miniscrews have also been used in resolution of palatal contraction. In fact, the maxilla expansion is one of the most commonly used procedures in orthodontics in order to correct the deficits of the skeletal transverse diameters of the upper jaw. Our results are in agreement with different studies. Ierardo et al. demonstrated the efficacy of orthodontic treatment with MSE in growing patients affected by OI and receiving treatment with BPs with a standard protocol, with no complications after a 1-year follow-up [28].
In fact, orthodontic mini-screws are devices that allow the achievement of the malocclusion resolution with fewer undesirable effects if compared to traditional orthodontic techniques. Skeletal anchoring is a valid substitute for conventional anchoring in situations where anchoring is difficult, critical, insufficient or at risk of causing unwanted side effects [31]. Skeletal anchoring is indicated where the forces acting on the reactive units are undesirable and cannot be neutralized by occlusal forces.
The success of the TADs ’use depends on different factors: anatomical structure and characteristics of the receiving site (cortical bone quality and quantity, soft tissues features), surgical protocol, tissue management, devices features (length, type, shape and diameter), clinical management and home oral hygiene, maxillary or mandibular location and position, gender, age, sagittal skeletal classification, discrepancy in the length of the arch and side [29,30,31,32,33,34,35,36].
Attention should be paid to numerous variables during planning orthodontic therapy using miniscrews, such as those relating to the site and bone tissue and those relating to the patient [37]. The evaluation in a first phase, therefore through second level exams such as site CBCT, is fundamental [38,39] and a second evaluation to verify the effectiveness of orthodontic MSE therapy.
The insertion of mini-implants for orthodontic purposes in fact requires a careful analysis of the receiving bone site, which should have a bone thickness adequate to the screw length and a width of at least 2.5 mm to avoid damage to the dental roots or other anatomical structures [14,22,23]. The areas with greater bone thickness are in the mandible, the vestibular interradicular area between the first and second molars, and in the maxillary bone between the canine and the lateral incisor. In the upper jaw, other suitable areas are represented by the interradicular spaces between the first molar and the second premolar, both buccally and palatally [15]. Another area with adequate bone thickness is at the level of the interradicular areas between the first and second maxillary molars, but the correct preparation of the site and the insertion of the miniscrew are difficult [23]. From a vertical point of view, the insertion of the miniscrews is carried out at or above the mucogingival line, depending on the desired action. Positioning above the mucogingival line is indicated in cases where a distalizing and intrusive vector is required. If the primary movement is distalization, an insertion at the level of the mucogingival line is recommended. Another consideration regarding positioning relates to the inclination of the axis of the screw body: the higher the insertion site, the greater the horizontal inclination of the axis (perpendicular to the bone surface) must be; if you opt for a positioning at the level of the mucogingival line, the inclination must be 30-45 ° with respect to the interradicular bone.
Patient bone turnover could be influenced by different factors [35]. General and local bone turnover greatly influences the treatment success. High bone turnover could lead to miniscrew failures. This high bone turnover is observed in patients with endocrinological alterations such as hyperthyroidism. On the other hand, in patients in therapy with drugs that reduce bone turnover for systemic diseases (e.g. bisphosphonates, immunosuppressants, etc.), the bone adaptation that occurs in relation to the screw is different. In these cases, an examination and a medical history are necessary to rule out any contraindications to the treatment [25].
Special attention should be paid to the medical history; in fact, some systemic pathologies show alterations of the craniofacial area as in the case of OI. In some cases of OI, the oral manifestation is dentinogenesis imperfect (DI), a hereditary dentin defect characterized by structural anomalies of the dentin responsible for abnormal tooth development.
In OI patients, a diagnostic and therapeutic program with the collaboration of dentist, orthodontist, neurologist and otolaryngologist are necessary for effective management [40].
In accordance with the study conducted by Messineo D. et al. [41] the correct orthodontic therapy in OI patients should be carefully evaluated and personalized for each case, with a level II radiological examinations such as CBCT to avoid complications and guarantee the efficacy of the therapy.. The increasing demand to treat decreased maxillary transverse diameters and prevent or alleviate obstructive sleep apnea (OSA) symptoms in both adults and children has led to an increase in the number of studies evaluating RME outcomes in terms of nasal cavity dimensions and upper airway patency using CBCT [42].
Our study demonstrated that the correct management of an orthodontic therapy with a hybrid MSE could be achieved also in patient affected by OI or by ectodermal dysplasia, in accordance with the study conducted by Ierardo et al [43,44].
The effectiveness of the TADs therefore depends on the patient's compliance, especially in pediatric dentistry [45].
In fact, fundamental is home oral hygiene to which the patient should be carefully instructed, especially if in the growth phase as pointed out by Wu TY [46].
Limitation of the Study
In accordance with this study, further studies with greater samples are essential to understand the efficacy of orthodontic therapy supported by MSE in different kind of cases, including special need patients, with lack of anchorage due to different clinical situation in pediatric dentistry.
6. Conclusions
This study therefore aimed to demonstrate the wide clinical applications of orthodontic miniscrews. Our results clearly show the effectiveness of these devices in orthodontic therapy even in complex cases both from a systemic and a dental point of view. These devices should be considerate safety and easily to apply even in special need pediatric patients.
The success of the therapy requires a collaborative network between specialists and others: dentist, orthodontist, pediatrician, dental hygienist, patients, and their legal guardians.
Author Contributions
Conceptualization, M.F.,V.L., V.I., G.I. ; methodology, M.F., V.L., V.I., G.I;; software, M.F.; validation, M.F., G.I., V.I., V.L..; formal analysis, M.F, M.C., G.I; investigation: M.F., G.I., M.G.; resources, M.F., V.L., V.I., G.I; data curation, M.F., V.L., V.I., G.I.; writing—original draft preparation, M.F., V.L., M. S., L.C., M.C., V.I., G.I; writing—review and editing, M.F., V.L., V.I., G.I; visualization, M.F., V.L., V.I., G.I; supervision, V.L., V.I., M.C., G.I.; project administration, M.F., V.L., V.I., G.I.; funding acquisition, M.F., V.L., V.I., G.I. All authors have read and agreed to the published version of the manuscript.
Funding
The Department of Oral and Maxillo-Facial Science, Pediatric Dentistry Unit, Policlinico Umberto I, Rome, Italy supported the study.
Institutional Review Board Statement
The study was conducted in accordance with 1975 Helsinki Declaration and its later amendments or comparable ethical standards and approved by the Institutional Local Review Board of Sapienza University of Rome (approval code: 2609/19; date of approval: 3 July 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed online consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Data available upon request due to restrictions. The data presented in this study are available upon request. The data is not publicly available for privacy reasons.
Conflicts of Interest
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
References
- Reyes-Reali J, Mendoza-Ramos MI, Garrido-Guerrero E, Méndez-Catalá CF, Méndez-Cruz AR, Pozo-Molina G. Hypohidrotic ectodermal dysplasia: clinical and molecular review. Int. J Dermatol 2018;57:965–972. [CrossRef]
- Sfeir E, Nassif N, Moukarzel C. Use of mini dental implants in ectodermal dysplasia children: follow-up of three cases. Eur J Paediatr Dent 2014 Jul;15(2 Suppl):207-12.
- Hashem A, Kelly A, O'Connell B, O'Sullivan M. Impact of moderate and severe hypodontia and amelogenesis imperfecta on quality of life and self-esteem of adult patients. J Dent. 2013 Aug;41(8):689-94.Epub 2013 Jun 15. PMID: 23778130. [CrossRef]
- Kratochvilova L, Dostalova T, Schwarz M, Macek M Jr, Marek I, Malíková M, Míšová E. Ectodermal dysplasia: important role of complex dental care in its interdisciplinary management. Eur J Paediatr Dent. 2022 Jun;23(2):140-146. [CrossRef]
- Forlino A, Marini JC. Osteogenesis imperfecta. Lancet. 2016 Apr 16;387(10028):1657-71. Epub 2015 Nov 3. PMID: 26542481; PMCID: PMC7384887. [CrossRef] [PubMed]
- Maines E, Monti E, Doro F, Morandi G, Cavarzere P, Antoniazzi F. Children and adolescents treated with neridronate for osteogenesis imperfecta show no evidence of any osteonecrosis of the jaw. J Bone Miner Metab 2012;30:434-8.
- Prado HV, Teixeira SA, Rabello F, Vargas-Ferreira F, Borges-Oliveira AC, Abreu LG. Malocclusion in individuals with osteogenesis imperfecta: A systematic review and meta-analysis. Oral Dis. 2022 Mar;28(2):314-325. Epub 2020 Nov 22. PMID: 33222339. [CrossRef]
- Nguyen MS, Binh HD, Nguyen KM, Maasalu K, Kõks S, Märtson A, Saag M, Jagomägi T. Occlusal features and need for orthodontic treatment in persons with osteogenesis imperfecta. Clin Exp Dent Res. 2017 Feb 9;3(1):19-24. PMID: 29744175; PMCID: PMC5839216). [CrossRef]
- Shroff, B., & Lindauer, S. J. Temporary Anchorage Devices: Biomechanical Opportunities and Challenges. Current Therapy in Orthodontics, 2010; 278-290).
- Melsen B., Mini-implants: where are we? J Clin Orthod 39 (9): 539-547, 2005.
- Carvalho Ferreira FP, Barbosa Lima AP, de Paula EC, Ferreira Conti AC, Valarelli DP, de Almeida-Pedrin RR. Orthodontic Protocol Using Mini-Implant for Class II Treatment in Patient with Special Needs. Case Rep Dent. 2016; 2016: 1057263. Epub 2016 Oct 26. PMID: 27847652; PMCID: PMC5101373. [CrossRef]
- Hartono N., Soegiharto B.M., Widayati R. The difference of stress distribution of maxillary expansion using rapid maxillary expander (RME) and maxillary skeletal Expander (MSE) - a finite element analysis. Prog Orthod 2018; 19: 33).
- Annarumma F., Aghazada H., Pandolfi S. L’espansione scheletrica mascellare in epoca post-puberale attraverso l’utilizzo delle miniviti palatali. Ortho Specialized.
- Baumgaertel S, Hans MG. Buccal cortical bone thickness fr mini-implant placement. Am J Orthod Dentofacial Orthop 2009; 136: 230-5.
- Carano A, Velo S, Incorvati C, Poggio P. Clinical applications of the Mini-Screw-Anchorage-System (M.A.S.) in the maxillary alveolar bone. Prog Orthod. 2004; 5 (2): 212-35. English, Italian. PMID: 15546013.
- McNamara Jr. J.A., Sigler L.M., Franchi L, Guest SS, Baccetti T. Changes in occlusal relationships in mixed dentition patients treated with rapid maxillary expansion. A prospective clinical study. Angle Orthod 2010;80:230–8.
- Daskaloggianakis J. Glossary of orthodontic terms. Leipzig: Quintessence Publishing Co:2000.
- Derton N., Gracco A., Greco A.M., Luzi C. Le miniviti ortodontiche – guida all’utilizzo clinico –Edizioni Martina 2015.
- Moyers R.E. Manuale di ortodonzia 1991. Cap 13, pag 329.
- Cope JB. Temporary devices in orthodontic: a paradigm shift. Semin Orthod 2005;11:3-9.
- Wehrbein H., Gollner P. Skeletal anchorage in orthodontics – basics and clinical application. J Orofac Orthop 2007;68:443-461.
- Kakali L, Alharbi M, Pandis N, Gkantidis N, Loukos D. Success of palatal implants or miniscrews placed median or paramedian for the reinforcement of anchora during orthodontic treatment: a systematic review. Eur J Ortho; 2019: 9-20.
- Bernhart T, Vollgruber A, Gahleitner A, Dortbudak O, Haas R. Alternative to the median region of the palate for placement of an orthodontic implant. Clin Oral Implants Res 2000; 11: 595-601.
- Papadopoulos M.A., Tarawneh F. The use of miniscrews implants for temporary skeletal anchorage in orthodontics: a comprehensive review. Oral Surg Oral Med Oral Pathol Oral Radiol 2007; 103; e6-e15rew.
- Leo M., Cerroni L., Pasquantonio G., Condò S.G., Condò R. Temporary anchorage deviced (TADs) in orthodontics: review of the factors that influence the clinical success rate of the mini-implants. Clin Ter 2016; 167 (£):e70-77).
- Di Giorgio G., Zumbo G., Saccucci M., Luzzi V., Ierardo G., Biagi R., Bossù M. Root Fracture and Extrusive Luxation in Primary Teeth and Their Management: A Case Report. Dent J (Basel). 2021 Sep 11;9(9):107. PMID: 34562981; PMCID: PMC8471370. [CrossRef]
- Luzzi V., Fabbrizi M., Coloni C., Mastrantoni C., Mirra C., Bossù M., Vestri A., Polimeni A. Experience of dental caries and its effects on early dental occlusion: a descriptive study. Ann Stomatol (Roma). 2011 Jan;2(1-2):13-8. Epub 2011 Jul 18. PMID: 22238717; PMCID: PMC3254384.
- Ierardo G, Calcagnile F, Luzzi V, Ladniak B, Bossu M, Celli M, Zambrano A, Franchi L, Polimeni A. Osteogenesis imperfecta and rapid maxillary expansion: Report of 3 patients. Am J Orthod Dentofacial Orthop. 2015 Jul;148(1):130-7. PMID: 26124036. [CrossRef]
- Manni A., Cozzani M., Tamborrino F. Factors influencing the stability of miniscrews. A retrospective study on 300 miniscrews. Eur J Orthod 2011 Aug; 33(4):388-95.
- Moon C.H., Park H.K., Nam J.S., et al. Am J Orthod Dentofacial Orthop. Relationship between vertical skeletal pattern and success rate of orthodontic mini-implants. 2010 Jul;138(1):51-7. [CrossRef]
- Giancotti A., Germano F., Muzzi F.A miniscrew-supported intrusion auxiliary for open-bite treatment with Invisalign. J Clin Orthod 2014 Jun;48(6):348-58.
- Janssen KI, Raghoebar GM, Vissink A, Sandham A. Skeletal anchorage in orthodontics--a review of various systems in animal and human studies. Int J Oral Maxillofac Implants. 2008 Jan-Feb;23(1):75-88. PMID: 18416415.
- Giancotti A., Greco M., Mampieri G.Palatal-implant anchorage in an adult class II patient. J Clin Orthod 2011 Nov; 45(11):627-34.
- Justens E., De Bruyn H. Clinical outcome of mini-screws used as orthodontic anchorage. Clin Implant Dent Relat Res. 2008 Sep;10(3):174-80. Epub 2008 Apr 1. [CrossRef]
- Lee S.J., Ahn S.J., Lee J.W. Survival analysis of orthodontic mini-implants. Am J Orthod Dentofacial Orthop. 2010 Feb;137(2):194-9. [CrossRef]
- Jaramillo-Bedoya D., Villegas-Giraldo G., Agudelo-Suárez A.A., Ramírez-Ossa D.M. A Scoping Review about the Characteristics and Success-Failure Rates of Temporary Anchorage Devices in Orthodontics. Dent J (Basel). 2022 May 6;10(5):78. PMID: 35621531; PMCID: PMC9139455. [CrossRef]
- Cassetta M., Sofan A.A., Altieri F., Barbato E. Evaluation of alveolar cortical bone thickness and density for orthodontic mini-implant placement. J Clin Exp Dent. 2013 Dec 1;5(5):e245-52. PMID: 24455090; PMCID: PMC3892271.). [CrossRef]
- Altieri F., Iezzi G., Luzzi V., Di Giorgio G., Polimeni A., Cassetta M. Computer-Guided Bone Biopsy: A Technical Note with the Description of a Clinical Case. Bioengineering (Basel). 2021 Dec 15;8(12):214. PMID: 34940367; PMCID: PMC8698291. [CrossRef]
- Reznikov N., Dagdeviren D., Tamimi F., Glorieux F., Rauch F., Retrouvey J.M. Cone-Beam Computed Tomography of Osteogenesis Imperfecta Types III and IV: Three-Dimensional Evaluation of Craniofacial Features and Upper Airways. JBMR Plus. 2019 Feb 7;3(6):e10124. PMID: 31346560; PMCID: PMC6636768. [CrossRef]
- Ierardo G, Luzzi V, Nardacci G, Vozza I, Polimeni A. Minimally invasive orthodontics: elastodontic therapy in a growing patient affected by Dentinogenesis Imperfecta. Ann Stomatol (Roma). 2017 Jul 3;8(1):34-38. PMID: 591 28736605; PMCID: PMC5507165. [CrossRef]
- Messineo D., Luzzi V., Pepe F., Celli L., Turchetti A., Zambrano A., Celli M., Polimeni A., Ierardo G. New 3D Cone Beam CT Imaging Parameters to Assist the Dentist in Treating Patients with Osteogenesis Imperfecta. Healthcare (Basel). 2020 Dec 10;8(4):546. PMID: 33321783; PMCID: PMC7764058. [CrossRef]
- Di Carlo G, Saccucci M, Ierardo G, Luzzi V, Occasi F, Zicari AM, Duse M, Polimeni A. Rapid Maxillary Expansion and Upper Airway Morphology: A Systematic Review on the Role of Cone Beam Computed Tomography. Biomed Res Int. 2017;2017:5460429. Epub 2017 Jul 16. PMID: 28791305; PMCID: PMC5534278. [CrossRef]
- Ierardo G., Calcagnile F, Luzzi V, Ladniak B, Bossu M., Celli M., Zambrano A., Franchi L., Polimeni A. Osteogenesis imperfecta and rapid maxillary expansion: Report of 3 patients. Am J Orthod Dentofacial Orthop. 2015 Jul;148(1):130-7. [CrossRef]
- Ierardo G, Luzzi V, Sfasciotti GL, Nardacci G, Polimeni A, Vozza I. Using of modified rapid palate expander with miniscrews in a patient affected by ectodermic dysplasia. Clin Ter. 2019 May-Jun;170(3):e168-e173. MID: 31173044.
- Uribe F., Mehr R., Mathur A. Prog Orthod. Failure rates of mini-implants placed in the infrazygomatic region 2015;16:31. Epub 2015 Sep 15. [CrossRef]
- Wu T.Y., Kuang S.H., Wu C.H. Factors associated with the stability of mini-implants for orthodontic anchorage: a study of 414 samples in Taiwan. J Oral Maxillofac Surg 2009 Aug;67(8):1595-9. https://doi.org/10.1016/j.joms.2009.04.015. [CrossRef]
Figure 1.
Intraoral examination of hypihydrotic ED patient.

Figure 2.
Design and application of orthodontic miniscrews in ED patient.
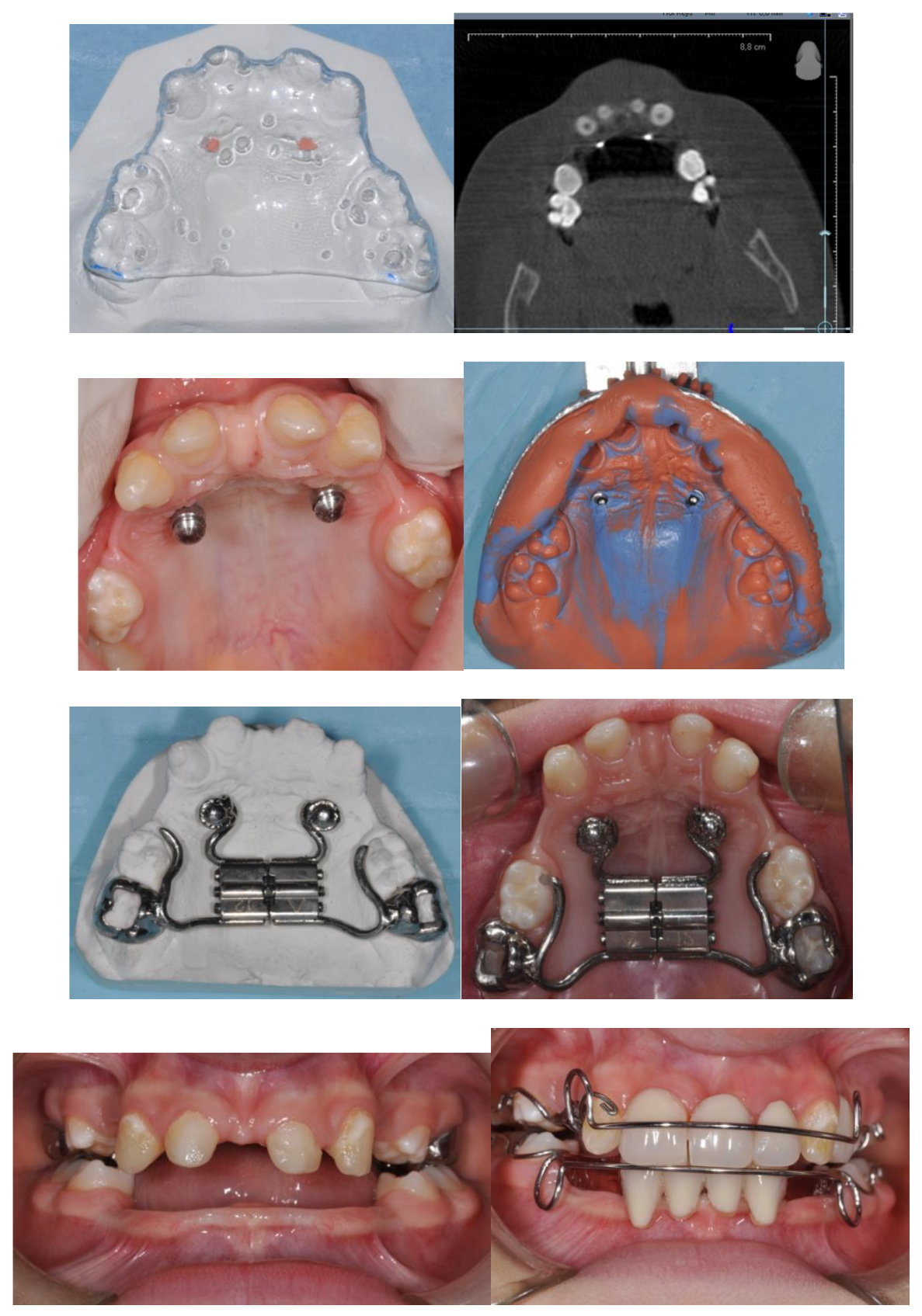
Figure 3.
Intraoral examination of OI patient.

Figure 4.
Design and application of orthodontic miniscrews in OI patient.
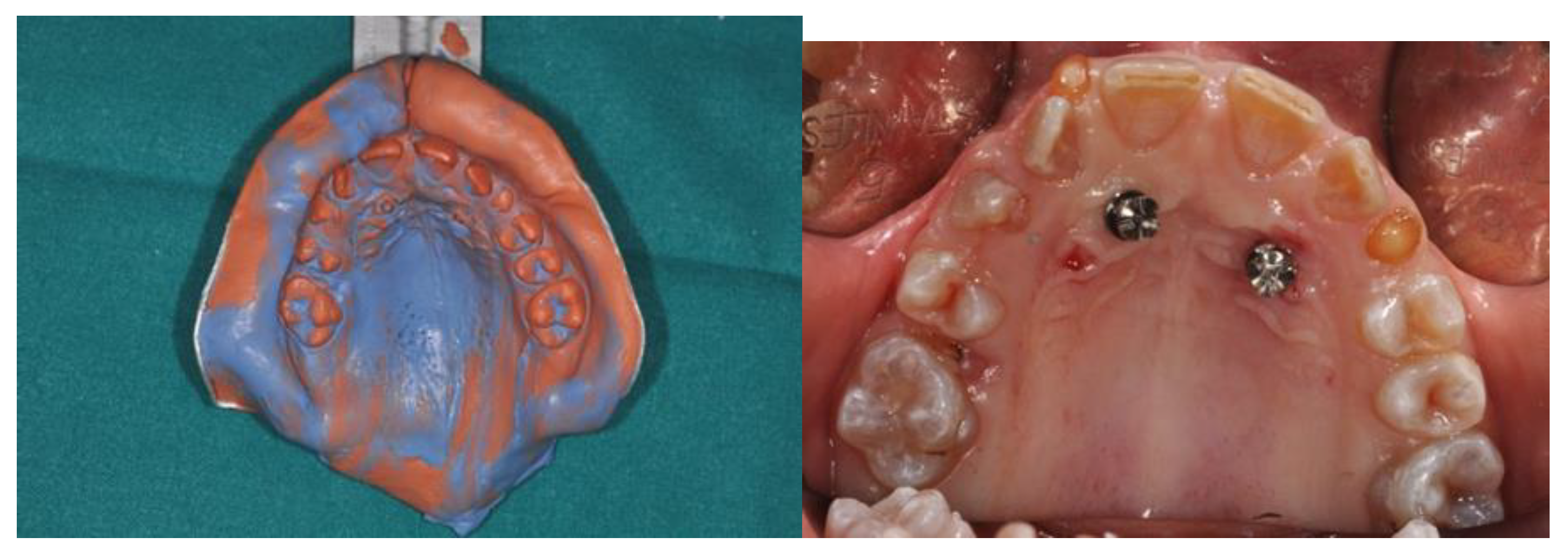
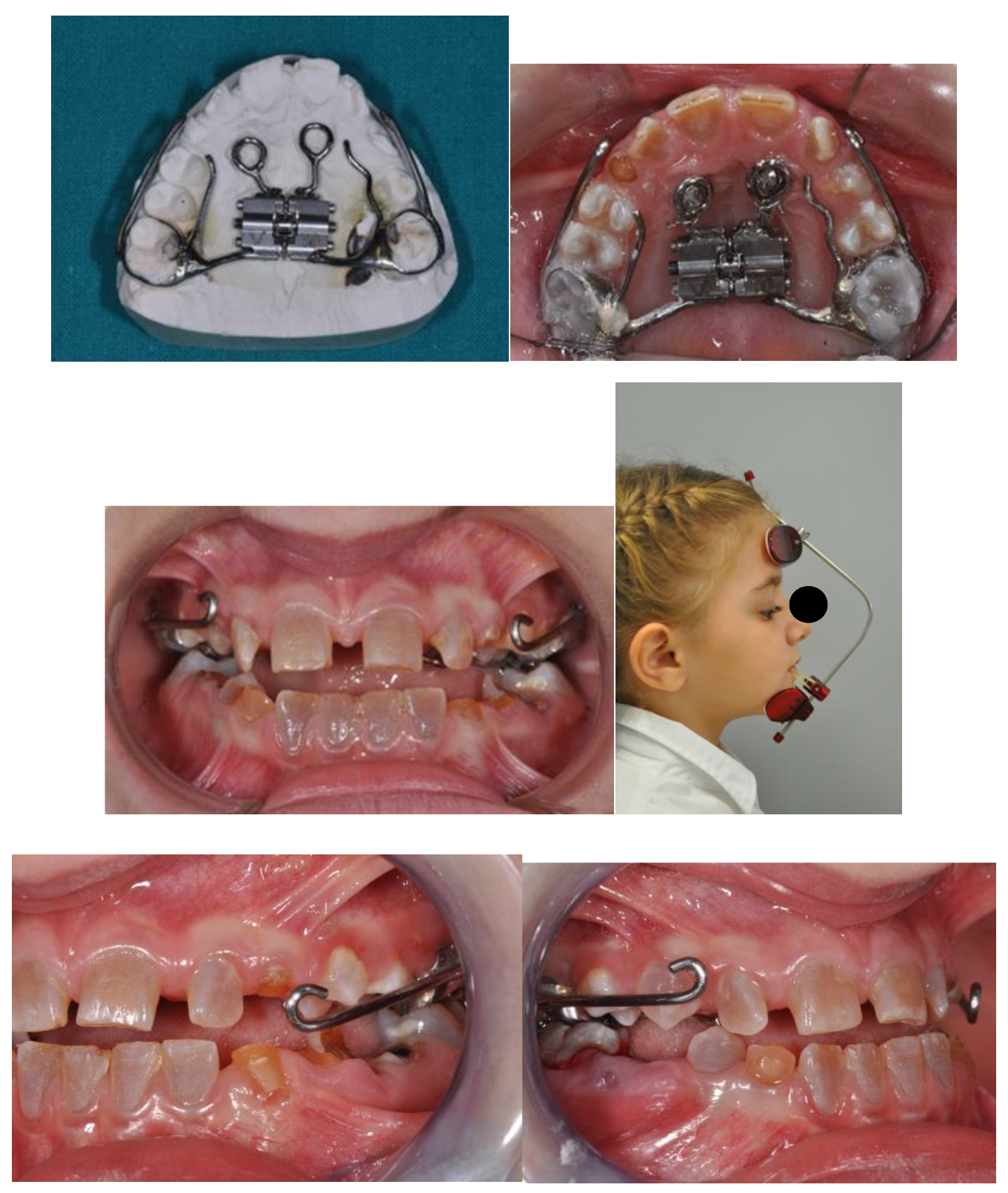

Figure 10.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



