
Submitted:
25 November 2024
Posted:
26 November 2024
You are already at the latest version
Abstract
Cystic echinococcosis (CE) is a neglected tropical parasitic disease linked with significant social and economic burdens worldwide. The scientific community has minimal information on echinococcosis in Romanian people, and hospital medical recordings are the only sources that may be used to investigate its status. A 7-year retrospective clinical study on pediatric patients with CE from South-Eastern Romania was performed, and 39 children were included, 2-15 years old. They were hospitalized with cystic echinococcosis in the Pediatric Department and Pediatric Surgery Department from Constanta County Clinical Emergency Hospital "St. Apostle Andrew," between 1 January 2017 and 1 October 2024. Twenty-nine (74.36%) pediatric patients came from rural zones, and 10 (25.64%) had urban residences. 28 children (71.79%) had contact with four different animals (dogs, goats, pigs, and sheep); only 4 were from urban zones, and they had contact only with dogs. Data regarding length of hospital stay, cyst location, and complications were collected and analyzed. According to the medical files, the diagnosis was established using imaging techniques and serological tests for CE. IgE and IgG reported appreciable variations in correlation with all parameters, and significant differences (p<0.05) were recorded. IgE levels considerably increased in cases of no animal contact, pulmonary involvement, complications, surgical treatment, and multiple hospitalizations. Moderate IgE values were recorded in urban residences, pig and sheep contact, and hepatic involvement. The IgG concentration considerably increased sheep contact and moderately increased in patients from rural zones, hepatic involvement, complications, and surgical treatment. The results show that incidental discovery, symptoms, complications, multiple dissemination, pulmonary involvement, and dog and pig contact increase the hospitalization time. Extensive data analysis supports our results. Our findings highlight the complexity of managing E. granulosus infections in children and evidence the importance of a multidisciplinary approach, combining early diagnostic tools, tailored medical therapy, and careful surgical intervention when necessary.
Keywords:
Echinococcus granulosus
; hydatid cyst
; Romanian pediatric patients
; liver and lung involvement
; medical and surgical treatment
; IgG
; IgE
; eosinophilia
1. Introduction
The parasitic zoonotic infection known as human cystic echinococcosis (CE) is brought on by the larval stages of Echinococcus granulosus sensu lato [1]. E. granulosus, the causative agent of CE, is a tapeworm parasite transmitted from animals to humans, commonly affecting children in endemic areas. This parasitic infection leads to the formation of cysts, primarily in the liver and lungs, which can cause severe complications if it is untreated [2]. Cystic echinococcosis has been recognized since 1950 as a public health problem [3]. Echinococcosis belongs to the list of 17 neglected tropical diseases (NTD); it is also a prioritized neglected zoonotic disease, for which WHO advocates concert control efforts [4].
E. granulosus can be considered a cosmopolitan parasite, being found on all populated continents. The disease is widespread, especially in countries where agriculture, mainly sheep farming, occupies a bare place in the national economy, with a higher incidence recorded in the areas where hygiene and development standards are relatively low [5]. Globalization, including migration and tourism in recent years, has increased the interest in this pathology in countries with a low rate of Taenia echinococcus infection or where the disease was considered eradicated [6,7,8,9].
Numerous elements, such as education, agriculture, culture, socioeconomic status, and the environment, are essential in the disease's spread [10]. According to research on domestic animals from rural areas (sheep, goats, pigs, and dogs), up to 34% were found sick [11,12,13]; large quantities of Echinococcus eggs are transferred from animals to water, vegetables, or farmlands, being contagious for months [16]. Canids are the final host in the life cycle of E. granulosus, while ungulates are the intermediate host [2,12]. As unintentional hosts, humans contract the illness by contact with dogs, contaminated food or water consumption, or hand-to-mouth transmitting the parasite's eggs [14]. The oncospheres are released from the embryonated eggs by the action of stomach juices after ingestion. The hexacanth embryos cling to and penetrate the enteric mucosa in the small intestine. The blood flows through capillaries and then carries them to the other organs [15,16]. One or more hydatid cysts grow in the organs due to the infection [17,18]. Various patterns of hydatid cysts and multiple organ involvement have often been observed in children because of the undeveloped filtering mechanisms of the liver and lungs throughout infancy and childhood, as well as the role of intestinal lymphatic vessels in parasite transmission [19]. Usually, cysts develop in the liver (70%) and lungs (20%), yet they can also be found in other organs like the brain, bones, heart, urinary, and genital tract [20,21]. Children rarely manifest echinococcosis due to age. This disease, which primarily affects the liver, is often not included in differential diagnoses of abdominal diseases, and missing the diagnosis can have devastating consequences. Symptomatology in its early stages is mild or absent [18]. When complications occur, the symptomatology depends on the cyst's stage, number, localization, and size [18]. Cysts typically form in the lungs (20%) and liver (70%) but can also occur in the brain, bones, heart, urinary tract, and genital tract [21]. Nonspecific symptoms such as fever, chest discomfort, coughing, and dyspnea can indicate pulmonary involvement [24]. A pulmonary cyst is frequently found by accident on a chest X-ray or may be found due to respiratory symptoms after cyst rupture or cyst infection. Simple cysts, inflammatory masses, and benign or malignant tumors are among the many differential diagnoses for pulmonary cysts in children [22,23,24,25]. Multiple investigations are necessary for a reliable diagnosis, including histology, serology, imaging, and the polymerase chain reaction (PCR) approach [26,27,28].
The most typical location of an E. multilocularis infection is the liver. It has been proposed that over 90% of people with liver infections experience it. The right lobe usually develops cysts when liver disease occurs [29]. With a few notable exceptions, cystic lesions grow slowly and frequently have local effects in older children or teenagers, resulting in pressure or discomfort in the right hypochondrium [19]. Jaundice is an extremely rare symptom. During the disease, cholestasis, jaundice, and/or portal vein thrombosis/portal hypertension are expected since the parasite typically affects the liver arteries and bile ducts. Cholestasis or jaundice can be anticipated considerably earlier if the liver focuses on the hilum region [30]. Magnification techniques are critical in diagnosing CE and determining the cyst's location and stage. The two primary immunological testing modalities currently employed in CE patients are immunoblotting (IB), which is used as a confirming assay due to its higher specificity and sensitivity, and enzyme-linked immunosorbent assays (ELISAs), which are used as screening tests E. granulosus infection in children presents unique clinical and management challenges. Given the high prevalence and the risk of complications, especially in endemic areas, timely diagnosis and treatment are essential [8,9,21,31].
With 200.000 new cases previously identified worldwide, human CE accounts for over 95% of the estimated 2-3 million cases. However, because of the high expense of treatment, missed income, and productivity diminution linked to cattle, CE is a significant cause of healthcare and economic losses in many world regions. CE is endemic in southern and eastern nations like Spain, Italy, Greece, Macedonia, Bulgaria, Moldova, Romania, Serbia, and Turkey within the European Union (EU) and its neighboring countries [32,33].
In Romania, 52.16% of the population lives in the urban environment, while the rural population represents 47.83% [34]. The incidence of CE was 5.6 per 100,000 inhabitants/year, according to the studies conducted by Lupașcu et al. between 1953 and 1963 [35]. In 1991-1995, 1000 new cases per year were recorded, according to Ciuca et al., with an increased incidence in sheep farming zones (Sibiu, Dobrogea areas) [36].
In 2022, the estimated population in Constanta was 655.997 inhabitants [34]. Rural residents accounted for 34.01% of the population in Constanta County. The regional continental climate with Mediterranean influences – warm summers and mild winters - is ideal for developing technological plants and grains, and zonal geography with a predominant plain is favorable for sheep raising. The scientific community has minimal information on echinococcosis in Romanian people [37,38,39] because Romania has no national regulations to manage E. granulosus, and reporting new cases is not mandatory [40,41]. Hospital medical recordings are the only sources that may be used to investigate CE status in our country. Therefore, the present study aims to enrich the scientific database with concrete information regarding pediatric echinococcosis in Southeast Romania, based on data collected from Constanta County Clinical Emergency Hospital "St. Apostle Andrew."
2. Materials and Methods
According to the Ethical Committee of the Ovidius University of Constanta, Faculty of Medicine (protocol 21 approved on 15 November 2024), a retrospective clinical study was performed on pediatric patients with CE from Southeast Romania.
The 39 children included in the study were 2-15 years old. They were hospitalized with cystic echinococcosis in the Pediatric and Pediatric Surgery Departments of Constanta County Clinical Emergency Hospital "St. Apostle Andrew" between 1 January 2017 and 1 October 2024.
Hospital databases and medical charts were reviewed. Data regarding age, gender, area of residence, length of hospital stay, cyst location, and complications were collected and analyzed. According to the medical files, the diagnosis was established using imaging techniques (radiography, ultrasonography, computed tomography) and serological tests for CE (E. granulosus antibodies IgG, using the ELISA method). A negative result of antibodies does not exclude a hydatid; the test may indicate negative or equivocal results due to the low antibodies' level in the early stages of the infection. If there is a clinical suspicion, the test must be repeated after 2-4 weeks. Significant cross-reactivity with Taenia solium has been reported. A positive result does not exclude the influence of other pathogens [42,43].
Data Analysis
Extensive data analysis used different tools of XLSTAT Life Sciences v 2024.3.0. 1423 by Lumivero (Denver, CO, USA): descriptive analysis, ANOVA single factor, Kruskal-Wallis analysis, correlations between variable parameters and heat maps [44]. Following the descriptive statistics, the variable parameters are displayed as absolute frequency (number, N) and relative frequency (percentage) [45]. Statistical significance was established at p<0.05 [46].
3. Results
3.1. Sociodemographic and Epidemiological Characterization of Pediatric Patients
Data are recorded in Table 1. Significantly statistical differences are considered between both groups with rural and urban residences (p < 0.05).
Echinococcus sp. transmission was investigated, including residence in rural and urban zones, potential contact with animals, and animal type. Therefore, Table 1 shows that 29 (74.36%) pediatric patients came from rural zones, and 10 (25.64%) had urban residences. Twenty-eight children (71.79%) had contact with four animals (dogs, goats, pigs, and sheep). Animal contact was predominant in rural zones in 24/29 (82.76) patients. Only 40% of pediatric patients (4/10) with urban residence had contact with an animal, exclusively dogs. The children from rural regions had contact with various animals: goats (9/24, 37.50%), sheep (9/24, 37.50%), pigs (5/24, 20.83%), and dogs (1/24, 4.17%).
3.2. Main Symptoms at Presentation and Organ Involvement
The illness was incidentally discovered in 6 children (15,38%). The remaining 84.62% (33 children) manifested various general and specific symptoms, such as abdominal pain (alone and associated with 1 or 2 symptoms: fever, headache, nausea, vomiting) and cough (combined with 1 or 2 different symptoms: fever, hemoptysis, thoracic pain, thoracic back pain, shortness of breath). Other, and in the majority, atypical symptoms rarely manifested alone were axillary adenopathy, back pain, left thoracic pain, tachycardia, and vomiting; they are included in the "Other 1" category. These findings are presented in Table 2, grouped by hospitalization period (days). Several abbreviations are used to simplify the presentation. Abdominal pain = AP, AP +1 = Abdominal pain with fever, AP +2 = Abdominal pain + fever and headache, and Abdominal pain + nausea and vomiting. Cough + 1 = Cough associated with another symptom (fever. hemoptysis. shortness of breath. or thoracic back pain). Cough + 2 = Cough + fever and hemoptysis, Cough + fever and thoracic pain, Cough + shortness of breath and fever. Other 1 = axillary adenopathy, back pain, left thoracic pain, tachycardia, or vomiting alone.
The hospitalization period between 6-10 days significantly differs from the others (p< 0.05, Figure 1).
Abdominal pain was the most manifested symptom at presentation (16 children. 41.43%), alone (23%) associated with 1 or 2 other symptoms. Eleven children (28.21%) had a cough in the binary and triple combination. Finally, 6 children (15.38%) revealed only other symptoms. The main symptoms at the presentation in Emergency Service could help identify the organ involved in CE and eventually multiple organ dissemination (Figure 2). Figure 2A shows that AP, AP +1, and +2 are essential symptoms in liver involvement, while in pulmonary hydatidosis, the patient has Cough in double or triple combinations. Atypical symptoms could be found in both CE places, and ID may be possible.
3.3. Laboratory Analyses, Evolution and Treatment
Data recorded in Table 2 shows that 32 pediatric patients (82.05%) had IgE > 100 i.u./mL, 31/39 (79.49%) revealed IgG > 1.1 i.u./mL and 13/39 (33.33%) evidenced eosinophilia > 0.5 /µL. Pearson correlation evidenced a substantial correlation between all three parameters (r = 0.978-0.997, p<0.05). Moreover, they strongly correlate with many symptoms: AP +1, AP +2, Cough +1, and Other 1 (r = 0.969-0.997, p<0.05). They also significantly correlate with liver and lung involvement ± MD (r = 0.902 – 0.997, p<0.05) and TS ± Complications and Multiple hospitalizations (r = 0.948-0.999, p<0.05). They moderately correlate with Cough +2, ID, and TM (r = 0.832 – 0.504, p>0.05). IgE < 100 i.u./mL, Eos < 0.5/µL and IgG < 1.1 i.u./mL are remarkably correlated with AP (r = 0.983-0.990, p<0.05). Therefore, all three parameters are considerably associated with all CE aspects, being essential biomarkers for CE evolution, treatment, and prognostic.
Eighteen pediatric patients (46.15%) had various complications (Figure 3A).
The correlation between the different complications, the main symptoms at presentation, the organ involved, the laboratory parameters, and the treatment type is illustrated in Figure 3B-G.
The children with Other 1 symptoms (axillary adenopathy, back pain. left thoracic pain, tachycardia, or vomiting), Cough +2 (cough + fever and hemoptysis, cough + fever and thoracic pain, cough + shortness of breath and fever) and CE incidentally discovered are mostly implied to develop complications (Figure 3B). Lung involvement induces complications more frequently than liver involvement (Figure 3C). Ig E and IgG are highly related to complications, while Eos are poorly associated (Figure 3D, E, F). Surgical treatment is the first choice for patients with complications; thus, TS shows a high correlation (Figure 3G).
3.4. Correlation Between Sociodemographic Data and Clinical Findings
Residence zone (rural and urban) and animal contact are significant factors in CE symptoms and organ involvement (Figure 4).
Children from urban zones had no symptoms from the "other" category (Figure 4A). 36.36% of the children with no animal contact evidenced AP only; half of this percent is available in children with animal contact (Figure 1B). The number of children with "other" symptoms with animal contact is twice that of those without it (Figure 4B). Several particular aspects can be observed when analyzing the group of animal contact children (30 children, Figure 4C). The same percentage of incidental discovery (20%) is available for dog and pig contact. This percentage decreases by half (11.11%) in goat and sheep contacts. Atypical symptoms ("Other 1") were substantially developed in pig contacts (40%), followed by sheep and goats (22.22 and 11.11%). They are missing in dog contacts. Abdominal pain is in triple association with different symptoms (AP +2) and is significantly described in goat contacts (44.44%) and 20% of dog and pig contact children. Contrariwise, cough in triple association (Cough +2) is the main symptom in sheep (33.33%) and dog (20%) contacts and is absent in goat and pig ones (Figure 1C).
As expected, Figure 4D shows that abdominal pain (alone, +1 and +2) is prominent in hepatic involvement, and Cough +1 and +2 in pulmonary placement, with similar incidence (62.50% and, respectively, 66.67%).
Figure 5 illustrates that hepatic involvement occurs significantly in goat contacts (40%, Figure 5A), and pulmonary localization is frequent mainly in sheep (38.46%, Figure 5B).
Dogs and sheep are similarly responsible for liver involvement (20.00% and 26.67%. Figure 5A), while pigs and goats are equally involved in lung placement (23.08%, Figure 5B). Dogs are not implied in multiple dissemination (MD) of hydatidosis (Figure 5C), while sheep are associated with 50% of MD, followed by pigs (33.33%) and goats (16.67%). Dogs and sheep are appreciably implicated in abdominal and respiratory complications (Figure 5D).
Principal Component Analysis (Figure 6A, B) supports our findings by displaying the correlations between sociodemographics of pediatric patients with the main clinical manifestations, organ involvement, laboratory parameters, complications, treatment, days of hospitalization, and multiple hospitalizations. Moreover, the correlation biplots indicate the place of each animal type vs no animal contact (NA) linked with all variable parameters.
Figure 6A shows the correlations between sociodemographics, the main clinical manifestations, organ involvement, and laboratory parameters. Thus, the correlation biplot highlights a substantial correlation between hepatic involvement and males, MD-no, AP +2, IgE > 100, and Eos < 0.5 (r = 0.883 - 0.981, p<0.05). Pulmonary involvement is strongly associated with MD-yes (r = 0.895, p<0.05). MD-no is significantly correlated with males, AP +2, IgE > 100, Eos < 0.05, IgG < 1.1 (r = 0.910 – 0.981, p<0.05). MD-yes highly correlates with other 1 symptoms (r = 0.943, p<0.05).
Figure 6B displays the correlations of sociodemographics with organ involvement, laboratory parameters, complications, treatment, days of hospitalization, and multiple hospitalizations. Thus, the absence of complications is highly correlated with Eos < 0.5 and 6-10 days of hospitalization (r = 0.908 – 0.938, p<0.05), while various complications are substantially associated with TS and 11-15 days of hospitalization (r = 0.932 – 0.944, p<0.05). Multiple hospitalizations strongly correlate with rural residence and IgG > 1.1 ( r = 0.881 – 0.894, p<0.05). IgG > 1.1 also significantly correlates with females, Eos > 0.5, and IgE < 100 (r = 0.933 – 0.988, p<0.05).
Significant differences between pediatric patients with animal contact vs. those without animal contact are illustrated in Figure 6C.
4. Discussion
Cystic echinococcosis (CE) is a zoonotic infection. 100% preventable, produced by the larval stage (metacestodes) of E. granulosus sensu lato [47,48,49,50,51]. The definitive hosts are the carnivores (canids, cats), which harbor the adult forms of the parasite, and the intermediate ones are the herbivores (sheep. goats. pigs. cattle), which harbor the larval forms [52]. Humans are aberrant, accidental intermediate hosts infected by contact with parasite eggs in the stool of definitive hosts and cannot transmit the infection [53,54]. From the ingested eggs, oncospheres hatch in the intestine, which penetrate the intestinal mucosa and are located through the blood flow in the various organs, where the metacestodes develop [55,56]. Geographically widespread, CE causes significant public health concerns and economic losses in many endemic nations [57,58]. It is still a neglected zoonotic disease despite this worldwide impact [59].
Hydatidosis is the primary Romanian helminthic zoonosis in humans, among parasite illnesses that spread from animals to people because of its severe clinical manifestation and associated consequences [60]. Our study on Romanian patients confirms the previously published data. Of 39 patients diagnosed with CE, 28 have contact with animals (dogs, sheep, goats, and pigs).
The liver is most frequently affected, followed by the lung; other tissues, including bone, can be affected [61,62,63,64,65,66,67,68,69,70,71,72,73]. Cysts can grow between 1 mm and 50 mm per year or remain unchanged [55]. The higher incidence of liver involvement in pediatric patients may be attributed to the larger relative size of the liver in children and its role as a primary filter for bloodstream pathogens [74,75]. Our pediatric patients had hepatic and pulmonary CE.
These findings are consistent with global trends but underscore the need for heightened vigilance in endemic areas where multi-organ involvement can occur [76,77]. Most patients present a single lesion in a single organ [78], and our findings confirm it. Cystic echinococcosis becomes symptomatic in complications, such as local compressive effect, fistulization in adjacent structures (biliary tree, bronchi), rupture with the spread of infection, or anaphylactic shock [79]. Frequently, patients are diagnosed during imaging investigations performed for other morbidities [80]. Eighteen children had various complications, while 3 of them were incidentally discovered. Our study also found that most pediatric patients with E. granulosus infections presented with nonspecific symptoms, such as abdominal pain, coughing, and fever. This aspect aligns with existing literature, highlighting the difficulty in early diagnosis due to the often asymptomatic nature of hydatid cysts in the early stages [81,82,83].
There are several therapeutic alternatives accessible at the moment [84,85]. Smaller, simpler cysts (less than 5 cm) respond well to albendazole treatment [85,86]. Medication by itself only removes 30% of cysts [87]. Eleven patients were treated with Albendazole in the present study. For liver cysts > 10 cm, those in danger of rupturing, and/or those that are difficult, surgery is recommended [88]. Laparoscopic surgery is seldom used, reducing postoperative abdominal infection risk. In biliary fistula and commorbidities, the radical procedure (complete cystopericystectomy) is the preferred method [88,89]. Conservative methods are suitable when nonspecialist surgeons perform surgery in endemic areas. A novel approach is PAIR (puncture-aspiration-injection-reaspiration) as an alternative to surgery [90,91].
Twenty-eight patients had surgical treatment in the present study, and 12 had various complications. Combining medical and surgical approaches yields the best outcomes. It was using Albendazole as a preoperative and postoperative treatment that reduced cyst viability and recurrence rates, highlighting its role as an essential adjunct to surgery. Notably, a subset of patients responded well to a conservative drug-only regimen, particularly those with small and uncomplicated cysts. Given the promising outcomes of albendazole treatment, further research into optimizing non-surgical management strategies is warranted [92]. Invasive surgery might be avoidable in specific cases, thus reducing the morbidity associated with surgical interventions [93]. Moreover, it could be particularly beneficial in resource-limited settings where access to surgical facilities is restricted [94].
Eosinophilia is an increase in eosinophils in the peripheral blood above the normal limit (greater than 500/mm³) [95]. It is frequently associated with parasitic diseases, especially those involving tissue parasites or larval invasion, but may also occur in other pathological contexts [96]. In parasitic diseases, eosinophilia is an essential marker of the innate and adaptive immune response [97]. Eosinophilia was reported in 20–34% of instances with hydatid cysts [98]. In cysts ruptures, leukocyte and eosinophil levels were greater [98]. In our study, eosinophilia was present in 33.33% of the cases, similar to other studies [99].
Parasites of the genus Echinococcus (most commonly Echinococcus granulosus and E. multilocularis) cause a complex immune response in which eosinophilia and IgE play a central role. Both components reflect the activation of the TH2-type immune response, which is characteristic of parasitic infections [100]. Eosinophilia and elevated IgE levels are essential markers in echinococcosis, reflecting activation of the host immune response against the parasite [39]. Although the correlation between the two mechanisms is well documented, the severity of these responses depends on the stage of the disease and the complex interaction between host and parasite [100]. Numerous studies have demonstrated that the location of the cyst, particularly in a vital organ like the liver, influences the immune response more than other affected organs in the body [101]. Regarding the elevated IgE antibody level in individuals with hydatid cysts in the liver as opposed to different organs, the influence of the hydatid cyst size was reflected in the IgG and IgE antibody levels [102]. In our study, IgE and IgG are highly related to complications, while Eos is poorly associated.
An essential aspect of the present research was evaluating immune responses post-treatment. High levels of specific IgG and IgE antibodies persisted in patients after cyst removal, suggesting a prolonged immune response that could be a marker for monitoring recurrence [103]. The immune system's role in hydatid disease in children appears to be distinct from that in adults, necessitating further research into age-related immunological differences and their implications for treatment [27]. It could be particularly beneficial in resource-limited settings where access to surgical facilities is restricted. Understanding the immunological mechanisms may pave the way for new preventive measures, including vaccines [104,105,106].
Limitations
While our findings could be considered a substantial contribution to understanding E. granulossus in children, several limitations should be noted. (i) Sample size: the relatively small sample size may limit the generalizability of the results. More extensive multicenter studies are needed to validate these findings across diverse pediatric populations. (ii) Lack of long-term follow-up: the absence of long-term follow-up data restricted our ability to assess the recurrence rates and long-term complications. (iii) Potential bias in diagnosis: misdiagnosis is possible due to reliance on imaging and serological tests, especially atypical presentations.
5. Conclusions
The present study highlights the complexity of managing E. granulosus infections in children. Our findings evidence the importance of a multidisciplinary approach, combining early diagnostic tools, tailored medical therapy, and careful surgical intervention when necessary. Addressing the challenges identified in this research can lessen outcomes and diminish the burden of hydatid disease in pediatric populations. Future directions may explore the pediatric immune response to E. granulosus infection in greater detail, developing more sensitive and specific diagnostic markers essential for early detection, especially in asymptomatic cases.
Author Contributions
Conceptualization. C.M.M., T.C., V.P., and R.M.S.; methodology. T.C. and V.P.; software. T.C. and V.P.; validation. A.L.B., G.B., and S.C.C.; formal analysis. V.P.; investigation. C.M.M., T.C., A.L.B., G.B., V.V.L., F.D.E., S.C.C., and R.M.S.; resources. T.C., F.D.E., and S.C.C.; data curation. C.M.M., T.C., and A.L.B.; writing—original draft preparation. T.C., V.P., and R.M.S..; writing—review and editing. C.M.M., T.C., A.L.B., G.B., V.V.L., V.P., F.S., F.D.E., S.C.C., and R.M.S.; visualization. C.M.M., T.C., A.L.B., G.B., V.V.L., V.P., F.S., F.D.E., S.C.C., and R.M.S.; supervision. C.M.M., T.C., and R.M.S.; project administration. C.M.M., T.C., and R.M.S.; funding acquisition. C.M.M., T.C., A.L.B., G.B., V.V.L., V.P., F.S., F.D.E., S.C.C., and R.M.S.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki and approved by the Faculty of Medicine Ethics Committee, Ovidius University of Constanta. Protocol 21 was approved on 15 November 2024.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Paternoster, G.; Boo, G.; Wang, C.; Minbaeva, G.; Usubalieva, J.; Raimkulov, K.M.; Zhoroev, A.; Abdykerimov, K.K.; Kronenberg, P.A.; Müllhaupt, B.; et al. Epidemic Cystic and Alveolar Echinococcosis in Kyrgyzstan: An Analysis of National Surveillance Data. Lancet Glob Health 2020, 8, e603–e611. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Ahmed, H.; Simsek, S.; Afzal, M.S.; Cao, J. Spread of Cystic Echinococcosis in Pakistan Due to Stray Dogs and Livestock Slaughtering Habits: Research Priorities and Public Health Importance. Front Public Health 2020, 7, 412. [Google Scholar] [CrossRef] [PubMed]
- Casulli, A.; Abela-Ridder, B.; Petrone, D.; Fabiani, M.; Bobić, B.; Carmena, D.; Šoba, B.; Zerem, E.; Gargaté, M.J.; Kuzmanovska, G.; et al. Unveiling the Incidences and Trends of the Neglected Zoonosis Cystic Echinococcosis in Europe: A Systematic Review from the MEmE Project. Lancet Infect Dis 2023, 23, e95–e107. [Google Scholar] [CrossRef] [PubMed]
- WHO Ending the Neglected Tropical Diseases to Attain the Sustainable Development Goals. A Road Map for Neglected Tropical Diseases 2021–2030. Geneva: World Health Organization; 2020. 2020.
- Widdicombe, J.; Basáñez, M.-G.; Entezami, M.; Jackson, D.; Larrieu, E.; Prada, J.M. The Economic Evaluation of Cystic Echinococcosis Control Strategies Focused on Zoonotic Hosts: A Scoping Review. PLoS Negl Trop Dis 2022, 16, e0010568. [Google Scholar] [CrossRef]
- Mutwiri, T.; Magambo, J.; Zeyhle, E.; Muigai, A.W.T.; Alumasa, L.; Amanya, F.; Fèvre, E.M.; Falzon, L.C. Findings of a Community Screening Programme for Human Cystic Echinococcosis in a Non-Endemic Area. PLOS Global Public Health 2022, 2, e0000235. [Google Scholar] [CrossRef]
- Yaqub, S.; Jensenius, M.; Heieren, O.E.; Drolsum, A.; Pettersen, F.O.; Labori, K.J. Echinococcosis in a Non-Endemic Country – 20-Years' Surgical Experience from a Norwegian Tertiary Referral Centre. Scand J Gastroenterol 2022, 57, 953–957. [Google Scholar] [CrossRef]
- Bindi, E.; Nino, F.; Simonini, A.; Cobellis, G. Giant Hydatid Lung Cyst in Non-Endemic Area. J Pediatr Surg Case Rep 2021, 64. [Google Scholar] [CrossRef]
- Han, X.-M.; Cai, Q.-G.; Wang, W.; Wang, H.; Zhang, Q.; Wang, Y.-S. Childhood Suffering: Hyper Endemic Echinococcosis in Qinghai-Tibetan Primary School Students, China. Infect Dis Poverty 2018, 7, 71. [Google Scholar] [CrossRef]
- Petropoulos, A.S.; Chatzoulis, G.A. Echinococcus Granulosus in Childhood: A Retrospective Study of 187 Cases and Newer Data. Clin Pediatr (Phila) 2019, 58, 864–888. [Google Scholar] [CrossRef]
- Almalki, E.; Al-Quarishy, S.; Abdel-Baki, A.-A.S. Assessment of Prevalence of Hydatidosis in Slaughtered Sawakny Sheep in Riyadh City, Saudi Arabia. Saudi J Biol Sci 2017, 24, 1534–1537. [Google Scholar] [CrossRef]
- A Scientific Analysis of the Islamic Rules on the Uncleanliness of Dogs from the Perspective of Medical Parasitology. Journal of North Khorasan University of Medical Sciences 2023, 78–82. [CrossRef]
- Araujo, F.P.; Schwabe, C.W.; Sawyer, J.C.; Davis, W.G. Hydatid Disease Transmission in California: A Study of the Basque Connection. Am J Epidemiol 1975, 102. [Google Scholar] [CrossRef] [PubMed]
- Coello Peralta, R.D.; Coello Cuntó, R.A.; Yancha Moreta, C.; Guerrero Lapo, G.E.; Vinueza Sierra, R.L.; León Villalba, L.R.; Pazmiño Gómez, B.J.; Gómez Landires, E.A.; Ramallo, G. A Case of Hepatic Hydatid Cyst in a Woman Associated with the Presence of Echinococcus Granulosus in Her Domestic Dogs in a Marginal Urban Area from Ecuador. American Journal of Case Reports 2023, 24. [Google Scholar] [CrossRef]
- Wilson, C.S.; Jenkins, D.J.; Brookes, V.J.; Barnes, T.S. An Eight-Year Retrospective Study of Hydatid Disease (Echinococcus Granulosus Sensu Stricto) in Beef Cattle Slaughtered at an Australian Abattoir. Prev Vet Med 2019, 173, 104806. [Google Scholar] [CrossRef]
- Gareh, A.; Saleh, A.A.; Moustafa, S.M.; Tahoun, A.; Baty, R.S.; Khalifa, R.M.A.; Dyab, A.K.; Yones, D.A.; Arafa, M.I.; Abdelaziz, A.R.; et al. Epidemiological, Morphometric, and Molecular Investigation of Cystic Echinococcosis in Camel and Cattle From Upper Egypt: Current Status and Zoonotic Implications. Front Vet Sci 2021, 8. [Google Scholar] [CrossRef]
- Tüz, A.E.; Ekemen Keleş, Y.; Şahin, A.; Üstündağ, G.; Taşar, S.; Karadağ Öncel, E.; Kara Aksay, A.; Öztan, M.O.; Köylüoğlu, G.; Çapar, A.E.; et al. Hydatid Disease in Children from Diagnosis to Treatment: A 10-Year Single Center Experience. Turkish Journal of Parasitology 2022, 46, 189–194. [Google Scholar] [CrossRef]
- Dawit, G.; Shishay, K. Epidemiology, Public Health Impact and Control Methods of the Most Neglected Parasite Diseases in Ethiopia: A Review. World Journal of Medical Sciences 2014, 10. [Google Scholar] [CrossRef]
- Peters, L.; Burkert, S.; Grüner, B. Parasites of the Liver – Epidemiology, Diagnosis and Clinical Management in the European Context. J Hepatol 2021, 75, 202–218. [Google Scholar] [CrossRef]
- Pakala, T.; Molina, M.; Wu, G.Y. Hepatic Echinococcal Cysts: A Review. J Clin Transl Hepatol 2016, 4. [Google Scholar]
- Belhassen-García, M.; Romero-Alegria, A.; Velasco-Tirado, V.; Alonso-Sardón, M.; Lopez-Bernus, A.; Alvela-Suarez, L.; Perez Del Villar, L.; Carpio-Perez, A.; Galindo-Perez, I.; Cordero-Sanchez, M.; et al. Study of Hydatidosis-Attributed Mortality in Endemic Area. PLoS One 2014, 9. [Google Scholar] [CrossRef]
- Ahmed, M.E.; Abdalla, S.S.; Adam, I.A.; Grobusch, M.P.; Aradaib, I.E. Prevalence of Cystic Echinococcosis and Associated Risk Factors among Humans in Khartoum State, Central Sudan. Int Health 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Lawson, J.R.; Gemmell, M.A. Transmission of Taeniid Tapeworm Eggs via Blowflies to Intermediate Hosts. Parasitology 1990, 100. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Bernus, A.; Belhassen-García, M.; Carpio-Perez, A.; Perez Del Villar, L.; Romero-Alegria, A.; Velasco-Tirado, V.; Muro, A.; Pardo-Lledias, J.; Cordero-Sánchez, M.; Alonso-Sardón, M. Is Cystic Echinoccocosis Re-Emerging in Western Spain? Epidemiol Infect 2015, 143. [Google Scholar] [CrossRef]
- Gessese, A.T. Review on Epidemiology and Public Health Significance of Hydatidosis. Vet Med Int 2020, 2020. [Google Scholar] [CrossRef]
- Masih, Z.; Hoghooghirad, N.; Madani, R.; Sharbatkhori, M. Expression and Production of Protoscolex Recombinant P29 Protein and Its Serological Evaluation for Diagnosis of Human Hydatidosis. Journal of Parasitic Diseases 2022, 46, 377–383. [Google Scholar] [CrossRef]
- Trigui, A.; Toumi, N.; Fendri, S.; Saumtally, M.S.; Zribi, I.; Akrout, A.; Mzali, R.; Ketata, S.; Dziri, C.; Amar, M. Ben; et al. Cystic Echinococcosis of the Liver: Correlation Between Intra-Operative Ultrasound and Preoperative Imaging. Surg Infect (Larchmt) 2024, 25, 213–220. [Google Scholar] [CrossRef]
- Durhan, G.; Tan, A.A.; Düzgün, S.A.; Akkaya, S.; Arıyürek, O.M. Radiological Manifestations of Thoracic Hydatid Cysts: Pulmonary and Extrapulmonary Findings. Insights Imaging 2020, 11. [Google Scholar] [CrossRef]
- Barth, T.F.E.; Casulli, A. Morphological Characteristics of Alveolar and Cystic Echinococcosis Lesions in Human Liver and Bone. Pathogens 2021, 10, 1326. [Google Scholar] [CrossRef]
- Babadjanov, A.K.; Yakubov, F.R.; Ruzmatov, P.Y.; Sapaev, D.S. Epidemiological Aspects of Echinococcosis of the Liver and Other Organs in the Republic of Uzbekistan. Parasite Epidemiol Control 2021, 15, e00230. [Google Scholar] [CrossRef]
- Khan, A.; Naz, K.; Ahmed, H.; Simsek, S.; Afzal, M.S.; Haider, W.; Ahmad, S.S.; Farrakh, S.; Weiping, W.; Yayi, G. Knowledge, Attitudes and Practices Related to Cystic Echinococcosis Endemicity in Pakistan. Infect Dis Poverty 2018, 7, 4. [Google Scholar] [CrossRef]
- Tamarozzi, F.; Legnardi, M.; Fittipaldo, A.; Drigo, M.; Cassini, R. Epidemiological Distribution of Echinococcus Granulosus s.l. Infection in Human and Domestic Animal Hosts in European Mediterranean and Balkan Countries: A Systematic Review. PLoS Negl Trop Dis 2020, 14, e0008519. [Google Scholar] [CrossRef] [PubMed]
- Borhani, M.; Fathi, S.; Lahmar, S.; Ahmed, H.; Abdulhameed, M.F.; Fasihi Harandi, M. Cystic Echinococcosis in the Eastern Mediterranean Region: Neglected and Prevailing! PLoS Negl Trop Dis 2020, 14, e0008114. [Google Scholar] [CrossRef] [PubMed]
- Cracu, G.-M.; Schvab, A.; Prefac, Z.; Popescu, M.; Sîrodoev, I. A GIS-Based Assessment of Pedestrian Accessibility to Urban Parks in the City of Constanța, Romania. Applied Geography 2024, 165, 103229. [Google Scholar] [CrossRef]
- Hamrat K, Yahia A, Benaissa MH, C. V Histological Appearance of Echinococcus Granulosus in the Camel Species in Algeria. Bulletin UASVM Veterinary Medicine 2014, 71, 79–44.
- Ciuca, N. Studies on Echinococcosis/Hydatidosis in Men and in Animals TV Constanza County, Romania. Parasitol Int 1998, 47, 320. [Google Scholar] [CrossRef]
- Cobzaru, R.G.; Dumitrescu, A.M.; Ciobotaru, M.; Rîpǎ, C.; Leon, M.; Luca, M.; Iancu, L.S. Epidemiological Aspects of Hydatidosis in Children, in Some Areas of North-Eastern Romania. Rev Med Chir Soc Med Nat Iasi 2013, 117, 754–757. [Google Scholar]
- Mitrea, I.L.; Ionita, M.; Wassermann, M.; Solcan, G.; Romig, T. Cystic Echinococcosis in Romania: An Epidemiological Survey of Livestock Demonstrates the Persistence of Hyperendemicity. Foodborne Pathog Dis 2012, 9, 980–985. [Google Scholar] [CrossRef]
- Paduraru, A.A.; Lupu, M.A.; Lighezan, R.; Pavel, R.; Cretu, O.M.; Olariu, T.R. Seroprevalence of Anti-Echinococcus Granulosus Antibodies and Risk Factors for Infection in Blood Donors from Western Romania. Life 2023, 13, 871. [Google Scholar] [CrossRef]
- Paduraru, A.A.; Lupu, M.A.; Popoiu, C.M.; Stanciulescu, M.C.; Tirnea, L.; Boia, E.S.; Olariu, T.R. Cystic Echinococcosis in Hospitalized Children from Western Romania: A 25-Year Retrospective Study. Biomedicines 2024, 12, 281. [Google Scholar] [CrossRef]
- Paduraru, A.A.; Lupu, M.A.; Sima, L.; Cozma, G.V.; Olariu, S.D.; Chiriac, S.D.; Totolici, B.D.; Pirvu, C.A.; Lazar, F.; Nesiu, A.; et al. Cystic Echinococcosis in Hospitalized Adult Patients from Western Romania: 2007–2022. Microorganisms 2023, 11, 2388. [Google Scholar] [CrossRef]
- Garcia, L.S.; Arrowood, M.; Kokoskin, E.; Paltridge, G.P.; Pillai, D.R.; Procop, G.W.; Ryan, N.; Shimizu, R.Y.; Visvesvara, G. Practical Guidance for Clinical Microbiology Laboratories: Laboratory Diagnosis of Parasites from the Gastrointestinal Tract. Clin Microbiol Rev 2018, 31, e00025–17. [Google Scholar] [CrossRef] [PubMed]
- Mukarram Shah, S.M. ; Saira; Hussain, F. Molecular Techniques for the Study and Diagnosis of Parasite Infection. In Parasitic Infections; Wiley, 2023; pp. 176–204.
- Moroșan, E.; Dărăban, A.; Popovici, V.; Rusu, A.; Ilie, E.I.; Licu, M.; Karampelas, O.; Lupuliasa, D.; Ozon, E.A.; Maravela, V.M.; et al. Sociodemographic Factors, Behaviors, Motivations, and Attitudes in Food Waste Management of Romanian Households. Nutrients 2024, 16, 2738. [Google Scholar] [CrossRef] [PubMed]
- Streba, L.; Popovici, V.; Mihai, A.; Mititelu, M.; Lupu, C.E.; Matei, M.; Vladu, I.M.; Iovănescu, M.L.; Cioboată, R.; Călărașu, C.; et al. Integrative Approach to Risk Factors in Simple Chronic Obstructive Airway Diseases of the Lung or Associated with Metabolic Syndrome—Analysis and Prediction. Nutrients 2024, 16, 1851. [Google Scholar] [CrossRef] [PubMed]
- Mititelu, M.; Popovici, V.; Neacșu, S.M.; Musuc, A.M.; Busnatu, Ștefan S.; Oprea, E.; Boroghină, S.C.; Mihai, A.; Streba, C.T.; Lupuliasa, D.; et al. Assessment of Dietary and Lifestyle Quality among the Romanian Population in the Post-Pandemic Period. Healthcare 2024, 12, 1006. [CrossRef]
- Cucher, M.A.; Macchiaroli, N.; Baldi, G.; Camicia, F.; Prada, L.; Maldonado, L.; Avila, H.G.; Fox, A.; Gutiérrez, A.; Negro, P.; et al. Cystic Echinococcosis in South America: Systematic Review of Species and Genotypes of Echinococcus Granulosus Sensu Lato in Humans and Natural Domestic Hosts. Tropical Medicine & International Health 2016, 21, 166–175. [Google Scholar] [CrossRef]
- Kern, P.; Menezes da Silva, A.; Akhan, O.; Müllhaupt, B.; Vizcaychipi, K.A.; Budke, C.; Vuitton, D.A. The Echinococcoses. In Advances in Parasitology; 2017; Vol. 96, pp. 259–369.
- Alvi, M.A.; Alsayeqh, A.F. Food-Borne Zoonotic Echinococcosis: A Review with Special Focus on Epidemiology. Front Vet Sci 2022, 9. [Google Scholar] [CrossRef]
- Mandal, S.; Deb Mandal, M. Human Cystic Echinococcosis: Epidemiologic, Zoonotic, Clinical, Diagnostic and Therapeutic Aspects. Asian Pac J Trop Med 2012, 5, 253–260. [Google Scholar] [CrossRef]
- Budke, C.M.; Carabin, H.; Ndimubanzi, P.C.; Nguyen, H.; Rainwater, E.; Dickey, M.; Bhattarai, R.; Zeziulin, O.; Qian, M.-B. A Systematic Review of the Literature on Cystic Echinococcosis Frequency Worldwide and Its Associated Clinical Manifestations. The American Society of Tropical Medicine and Hygiene 2013, 88, 1011–1027. [Google Scholar] [CrossRef]
- Popa, G.L.; Tanase, I.; Popa, C.A.; Mastalier, B.; Popa, M.I.; Cretu, C.M. Medical and Surgical Management of a Rare and Complicated Case of Multivisceral Hydatidosis; 18 Years of Evolution. New Microbiologica 2014, 37, 387–391. [Google Scholar]
- Tao, Y.; Wang, Y.-F.; Wang, J.; Long, S.; Seyler, B.C.; Zhong, X.-F.; Lu, Q. Pictorial Review of Hepatic Echinococcosis: Ultrasound Imaging and Differential Diagnosis. World J Gastroenterol 2024, 30, 4115–4131. [Google Scholar] [CrossRef]
- Menschaert, D.; Hoyoux, M.; Moerman, F.; Daron, A.; Frere, J. Echinococcosis, a Global Economic and Health Burden. Tropical Medicine and International Health 2017, 22. [Google Scholar]
- Brunetti, E.; Kern, P.; Vuitton, D.A. Expert Consensus for the Diagnosis and Treatment of Cystic and Alveolar Echinococcosis in Humans. Acta Trop 2010, 114, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Luga, P.; Gjata, A.; Akshija, I.; Mino, L.; Gjoni, V.; Pilaca, A.; Zobi, M.; Martinez, G.E.; Richter, J. What Do We Know about the Epidemiology and the Management of Human Echinococcosis in Albania? Parasitol Res 2023, 122, 1811–1818. [Google Scholar] [CrossRef] [PubMed]
- Mihailescu, P.E.; Istrate, C.M.; Lazar, V. Echinococcus Species, Neglected Food Borne Parasites: Taxonomy, Life Cycle and Diagnosis. Biointerface Res Appl Chem 2020, 10, 5284–5295. [Google Scholar] [CrossRef]
- World Heath Organization Investing to Overcome the Global Impact of Neglected Tropical Diseases ... - World Health Organization - Google Books. Google books 2015, 3.
- da Silva, A.M. Human Echinococcosis: A Neglected Disease. Gastroenterol Res Pract 2010, 2010, 1–9. [Google Scholar] [CrossRef]
- Tamarozzi, F.; Akhan, O.; Cretu, C.M.; Vutova, K.; Akinci, D.; Chipeva, R.; Ciftci, T.; Constantin, C.M.; Fabiani, M.; Golemanov, B.; et al. Prevalence of Abdominal Cystic Echinococcosis in Rural Bulgaria, Romania, and Turkey: A Cross-Sectional, Ultrasound-Based, Population Study from the HERACLES Project. Lancet Infect Dis 2018, 18, 769–778. [Google Scholar] [CrossRef]
- Kosmidis, C.S.; Papadopoulos, K.; Mystakidou, C.M.; Sevva, C.; Koulouris, C.; Varsamis, N.; Mantalovas, S.; Lagopoulos, V.; Magra, V.; Theodorou, V.; et al. Giant Echinococcosis of the Liver with Suppuration: A Case Report and Review of the Literature. Medicina (B Aires) 2023, 59, 1070. [Google Scholar] [CrossRef]
- Jahanshahi, F.; Parsaei, A.H.; Naderi, D.; Davani, S.Z.N. Primary Isolated Extraluminal Hydatid Cyst of Left Pulmonary Artery. Int J Surg Case Rep 2023, 106. [Google Scholar] [CrossRef]
- Ewnte, B. Hydatid Cyst of the Foot: A Case Report. J Med Case Rep 2020, 14, 6. [Google Scholar] [CrossRef]
- Chaker, K.; Nouira, Y.; Ouanes, Y.; Bibi, M. A Simple Score for Predicting Urinary Fistula in Patients with Renal Hydatid Cysts. Libyan Journal of Medicine 2022, 17. [Google Scholar] [CrossRef] [PubMed]
- Jan, Z.U.; Ahmed, N.; Khan, M.Y.; Samin, Y.; Sohail, R. Hydatid Cyst of the Hepatopancreatic Groove - A Case Report. Int J Surg Case Rep 2023, 111, 108771. [Google Scholar] [CrossRef] [PubMed]
- Ahmady-Nezhad, M.; Rezainasab, R.; Khavandegar, A.; Rashidi, S.; Mohammad-Zadeh, S. Perineal and Right Femoral Hydatid Cyst in a Female with Regional Paresthesia: A Rare Case Report. BMC Surg 2022, 22, 64. [Google Scholar] [CrossRef] [PubMed]
- Khasawneh, R.A.; Mohaidat, Z.M.; Khasawneh, R.A.; Zoghoul, S.B.; Henawi, Y.M. Unusual Intramuscular Locations as a First Presentation of Hydatid Cyst Disease in Children: A Report of Two Cases. BMC Pediatr 2021, 21, 371. [Google Scholar] [CrossRef]
- Lakhdar, F.; Benzagmout, M.; Chakour, K.; Chaoui, M. el faiz Multiple and Infected Cerebral Hydatid Cysts Mimicking Brain Tumor: Unusual Presentation of Hydatid Cyst. Interdisciplinary Neurosurgery 2020, 22, 100802. [Google Scholar] [CrossRef]
- Tshering, S.; Dorji, N.; Wangden, T.; Choden, S. Pelvic Hydatid Cyst Mimicking Ovarian Cyst. Journal of South Asian Federation of Obstetrics and Gynaecology 2022, 14, 317–319. [Google Scholar] [CrossRef]
- Bouknani, N.; Kassimi, M.; Saibari, R.C.; Fareh, M.; Mahi, M.; Rami, A. Hydatid Cyst of the Uterus: Very Rare Location. Radiol Case Rep 2023, 18, 882–885. [Google Scholar] [CrossRef]
- Malakzai, H.A.; Baset, Z.; Ibrahimkhil, A.S.; Rahimi, M.S.; Khan, J.; Hanifi, A.N. Primary Hydatid Cyst of the Urinary Bladder with Associated Eosinophilic Cystitis: Report of a Unique Case. Urol Case Rep 2023, 46, 102296. [Google Scholar] [CrossRef]
- Ben Ismail, I.; Sghaier, M.; Boujmil, K.; Rebii, S.; Zoghlami, A. Hydatid Cyst of the Liver Fistulized into the Inferior Vena Cava. Int J Surg Case Rep 2022, 94, 107060. [Google Scholar] [CrossRef]
- Rahimi, M.T.; Hares, R.; Rahman, H.; Shinwari, M.A.; Khaliqi, S.; Hares, S. Primary Cervical Hydatid Cyst: A Rare Case Report. Int J Surg Case Rep 2023, 107, 108349. [Google Scholar] [CrossRef]
- Dziri, C.; Haouet, K.; Fingerhut, A.; Zaouche, A. Management of Cystic Echinococcosis Complications and Dissemination: Where Is the Evidence? World J Surg 2009, 33, 1266–1273. [Google Scholar] [CrossRef] [PubMed]
- Stojković, M.; Weber, T.F.; Junghanss, T. Clinical Management of Cystic Echinococcosis: State of the Art and Perspectives. Curr Opin Infect Dis 2018, 31, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Kiresi, D.A.; Karabacakoglu, A.; Odev, K.; Karakose, S. Pictorial Review. Uncommon Locations of Hydatid Cysts. Acta radiol 2003, 44, 622–636. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, B.; Akhavan, R.; Ghamari Khameneh, A.; Darban Hosseini Amirkhiz, G.; Rezaei-Dalouei, H.; Tayebi, S.; Hashemi, J.; Aminizadeh, B.; Darban Hosseini Amirkhiz, S. Computed Tomography and Magnetic Resonance Imaging of Hydatid Disease: A Pictorial Review of Uncommon Imaging Presentations. Heliyon 2021, 7, e07086. [Google Scholar] [CrossRef]
- Govindasamy, A.; Bhattarai, P.R.; John, J. Liver Cystic Echinococcosis: A Parasitic Review. Ther Adv Infect Dis 2023, 10. [Google Scholar] [CrossRef]
- Constantin, V.; Popa, F.; Socea, B.; Carâp, A.; Bǎlǎlǎu, C.; Motofei, I.; Banu, P.; Costea, D. Spontaneous Rupture of a Splenic Hydatid Cyst with Anaphylaxis in a Patient with Multi-Organ Hydatid Disease. Chirurgia (Romania) 2014, 109. [Google Scholar]
- Calu, V.; Enciu, O.; Toma, E.-A.; Pârvuleţu, R.; Pîrîianu, D.C.; Miron, A. Complicated Liver Cystic Echinococcosis—A Comprehensive Literature Review and a Tale of Two Extreme Cases. Tomography 2024, 10, 922–934. [Google Scholar] [CrossRef]
- Sánchez Infante, S.; Castellón Pavón, C.; Díaz García, G.; Pérez Domene, M.; Durán Poveda, M. Pancreatic Hydatidosis: Unusual Incidental Finding in the Surgical Specimen of a Cephalic Duodenopancreatectomy. Cirugía Andaluza 2023, 34, 468–470. [Google Scholar] [CrossRef]
- Arghir, O.; Dantes, E.; Toma, C.; Alexe, M. Bronchoscopic Diagnosis and Complete Treatment of a Ruptured Left Pulmonary Hydatid Cyst. Chest 2012, 142, 880A. [Google Scholar] [CrossRef]
- Collado-Aliaga, J.; Romero-Alegría, Á.; Alonso-Sardón, M.; Muro, A.; López-Bernus, A.; Velasco-Tirado, V.; Muñoz Bellido, J.L.; Pardo-Lledias, J.; Belhassen-García, M. Complications Associated with Initial Clinical Presentation of Cystic Echinococcosis: A 20-Year Cohort Analysis. Am J Trop Med Hyg 2019, 101, 628–635. [Google Scholar] [CrossRef]
- Paramita, A.A.K.Y.; Wibawa, I.D.N. Multimodal Treatment of Cystic Echinococcosis. The Indonesian Journal of Gastroenterology, Hepatology, and Digestive Endoscopy 2023, 24, 72–82. [Google Scholar] [CrossRef]
- Dehkordi, A.B.; Sanei, B.; Yousefi, M.; Sharafi, S.M.; Safarnezhad, F.; Jafari, R.; Darani, H.Y. Albendazole and Treatment of Hydatid Cyst, Review of Literature. Infect Disord Drug Targets 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Aydin, Y.; Ulas, A.B.; Ince, I.; Kalin, A.; Can, F.K.; Gundogdu, B.; Kasali, K.; Kerget, B.; Ogul, Y.; Eroglu, A. Evaluation of Albendazole Efficiency and Complications in Patients with Pulmonary Hydatid Cyst. Interact Cardiovasc Thorac Surg 2022, 34, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Eisenman, E.J.L.; Uhart, M.M.; Kusch, A.; Vila, A.R.; Vanstreels, R.E.T.; Mazet, J.A.K.; Briceño, C. Increased Prevalence of Canine Echinococcosis a Decade after the Discontinuation of a Governmental Deworming Program in Tierra Del Fuego, Southern Chile. Zoonoses Public Health 2023, 70, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Manouchehr Aghajanzadeh; Afshin Shafaghi; Mohammad Taghi Ashoobi; Mohamad Yosafee Mashhor; Omid Mosaffaee Rad; Mohaya Farzin Clinical Presentation, Diagnosis and Surgical Treatment of Intrabiliary Ruptured Hydatid Disease of the Liver. GSC Advanced Research and Reviews 2023, 16, 162–170. [CrossRef]
- Dogu, D.; Dincer, H.; Turan, T.; Akinci, D.; Parlak, E.; Dogrul, A.B. Diagnosis and Surgical Treatment of Cysto-Gastric Fistula out of an Hepatic Hydatid Cyst. Unusual Case. Ann Ital Chir 2023, 12, 1–3. [Google Scholar] [CrossRef]
- Chen, X.; Cen, C.; Xie, H.; Zhou, L.; Wen, H.; Zheng, S. The Comparison of 2 New Promising Weapons for the Treatment of Hydatid Cyst Disease. Surg Laparosc Endosc Percutan Tech 2015, 25, 358–362. [Google Scholar] [CrossRef]
- Ferrer-Inaebnit, E.; Molina-Romero, F.X.; Segura-Sampedro, J.J.; González-Argenté, X.; Morón Canis, J.M. A Review of the Diagnosis and Management of Liver Hydatid Cyst. Revista Española de Enfermedades Digestivas 2021, 114. [Google Scholar] [CrossRef]
- Tamarozzi, F.; Nicoletti, G.J.; Neumayr, A.; Brunetti, E. Acceptance of Standardized Ultrasound Classification, Use of Albendazole, and Long-Term Follow-up in Clinical Management of Cystic Echinococcosis. Curr Opin Infect Dis 2014, 27, 425–431. [Google Scholar] [CrossRef]
- Mahmoodi, S.; Ebrahimian, M.; Mirhashemi, S.H.; Soori, M.; Rashnoo, F.; Oshidari, B.; Shadidi Asil, R.; Zamani, A.; Hajinasrollah, E. A 20 Years Retrospective Descriptive Study of Human Cystic Echinococcosis and the Role of Albendazole Concurrent with Surgical Treatment: 2001-2021. Iran J Parasitol 2023, 18. [Google Scholar] [CrossRef]
- Ahmad, A.; Tania Mahar; Abdul Manan; Irfan Ahmad; Abdul Qadir; M. Usman; M. Waseem Cystobiliary Fistula in Hepatic Hydatid Cyst Disease; A Case Report and Literature Review. Medical Journal Of South Punjab 2021, 2. [CrossRef]
- Jafari, R.; Sanei, B.; Baradaran, A.; Kolahdouzan, M.; Bagherpour, B.; Yousofi Darani, H. Immunohistochemical Observation of Local Inflammatory Cell Infiltration in the Host-Tissue Reaction Site of Human Hydatid Cysts. J Helminthol 2019, 93, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Al-Sakee, H. Immunological Aspects of Cystic Echinococcosis in Erbil. Zanco J Med Sci 2011, 15, 1–9. [Google Scholar] [CrossRef]
- Hotz, J.F.; Kaczirek, K.; Stremitzer, S.; Waneck, F.; Auer, H.; Perkmann, T.; Kussmann, M.; Bauer, P.K.; Chen, R.-Y.; Kriz, R.; et al. Evaluation of Eosinophilic Cationic Protein as a Marker of Alveolar and Cystic Echinococcosis. Pathogens 2022, 11, 261. [Google Scholar] [CrossRef]
- Tartar, T.; Bakal, U.; Sarac, M.; Kazez, A. Laboratory Results and Clinical Findings of Children with Hydatid Cyst Disease. Niger J Clin Pract 2020, 23, 1008. [Google Scholar] [CrossRef] [PubMed]
- Lissandrin, R.; Tamarozzi, F.; Piccoli, L.; Tinelli, C.; De Silvestri, A.; Mariconti, M.; Meroni, V.; Genco, F.; Brunetti, E. Factors Influencing the Serological Response in Hepatic Echinococcus Granulosus Infection. The American Society of Tropical Medicine and Hygiene 2016, 94, 166–171. [Google Scholar] [CrossRef]
- Hotz, J.F.; Peters, L.; Kapp-Schwörer, S.; Theis, F.; Eberhardt, N.; Essig, A.; Grüner, B.; Hagemann, J.B. Evaluation of Serological Markers in Alveolar Echinococcosis Emphasizing the Correlation of PET-CTI Tracer Uptake with RecEm18 and Echinococcus-Specific IgG. Pathogens 2022, 11, 239. [Google Scholar] [CrossRef]
- Grimm, J.; Nell, J.; Hillenbrand, A.; Henne-Bruns, D.; Schmidberger, J.; Kratzer, W.; Gruener, B.; Graeter, T.; Reinehr, M.; Weber, A.; et al. Immunohistological Detection of Small Particles of Echinococcus Multilocularis and Echinococcus Granulosus in Lymph Nodes Is Associated with Enlarged Lymph Nodes in Alveolar and Cystic Echinococcosis. PLoS Negl Trop Dis 2020, 14. [Google Scholar] [CrossRef]
- KHABIRI, A.R.; BAGHERI, F.; ASSMAR, M.; SIAVASHI, M.R. Analysis of Specific IgE and IgG Subclass Antibodies for Diagnosis of Echinococcus Granulosus. Parasite Immunol 2006, 28, 357–362. [Google Scholar] [CrossRef]
- Maleki, F.; Akhlaghi, L.; Tabatabaie, F. Evaluation of Hydatid Cyst Antigen for Serological Diagnosis. Med J Islam Repub Iran 2023, 37. [Google Scholar] [CrossRef]
- Velasco-Tirado, V.; Alonso-Sardón, M.; Lopez-Bernus, A.; Romero-Alegría, Á.; Burguillo, F.J.; Muro, A.; Carpio-Pérez, A.; Muñoz Bellido, J.L.; Pardo-Lledias, J.; Cordero, M.; et al. Medical Treatment of Cystic Echinococcosis: Systematic Review and Meta-Analysis. BMC Infect Dis 2018, 18, 306. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Du, X.; Liu, K.; Wang, C.; Lv, Y.; Wang, M.; Yang, Z.; Yang, J.; Li, S.; Wu, C.; et al. Clinical Characteristics and Antibodies against Echinococcus Granulosus Recombinant Antigen P29 in Patients with Cystic Echinococcosis in China. BMC Infect Dis 2022, 22, 609. [Google Scholar] [CrossRef] [PubMed]
- Bethony, J.M.; Cole, R.N.; Guo, X.; Kamhawi, S.; Lightowlers, M.W.; Loukas, A.; Petri, W.; Reed, S.; Valenzuela, J.G.; Hotez, P.J. Vaccines to Combat the Neglected Tropical Diseases. Immunol Rev 2011, 239, 237–270. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The main differences between the hospitalization periods. Eos = Eosinophilia, C = complications, MD = multiple organ diffusion.
Figure 1.
The main differences between the hospitalization periods. Eos = Eosinophilia, C = complications, MD = multiple organ diffusion.
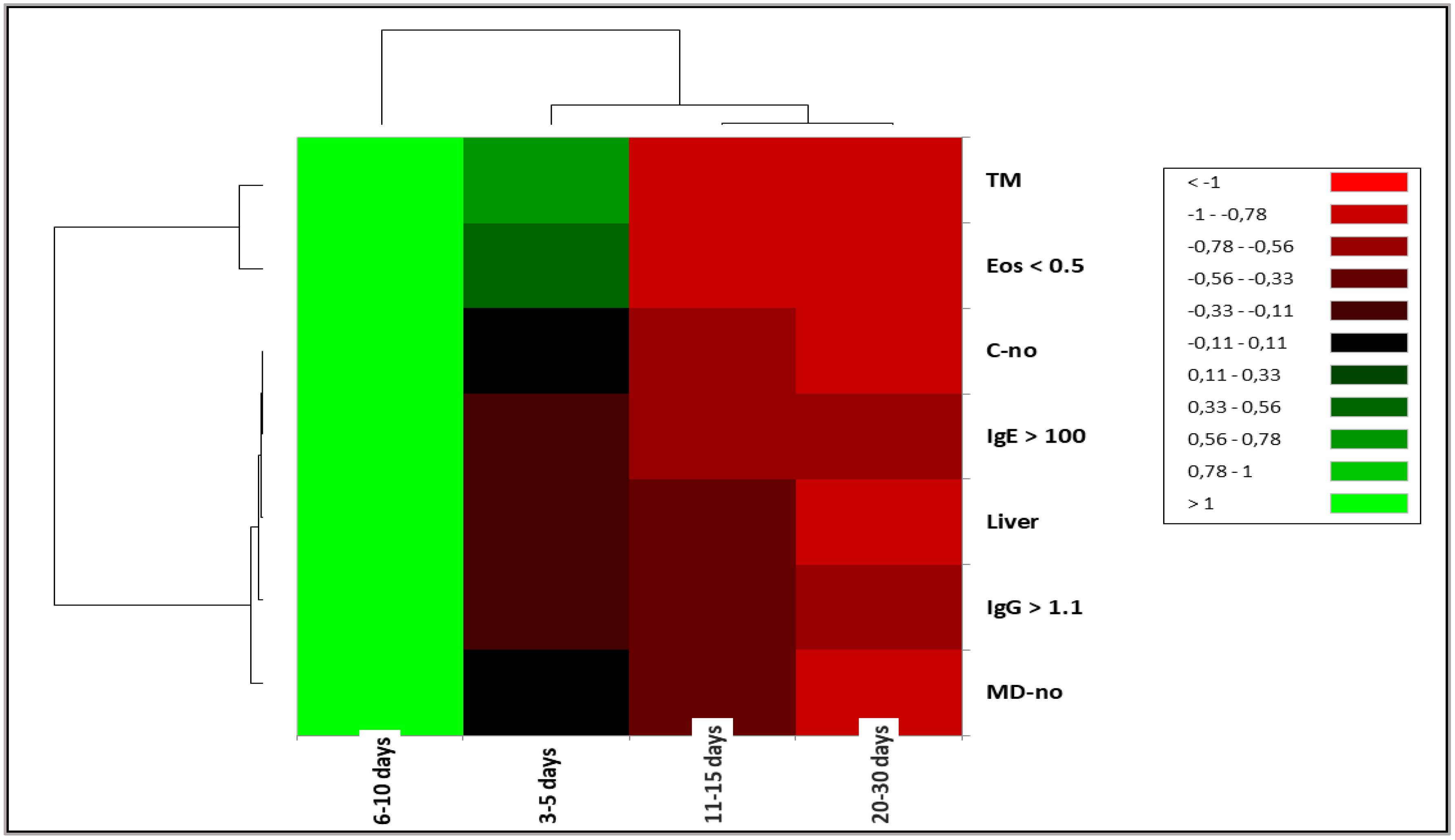
Figure 2.
The main symptoms associated with organs involved in CE in pediatric patients: Liver, Lung, and multiple organ diffusion (A and B). The organs correlated with MD (C) and its potential to generate complications (D) and the influence on the hospitalization period (E and F). AP = abdominal pain; AP +1 = Abdominal pain +1 = Abdominal pain with fever. AP +2 = Abdominal pain +2 = Abdominal pain + fever + headache and Abdominal pain + nausea and vomiting. Cough + 1 = Cough associated with one of the following symptoms: fever, hemoptysis, shortness of breath, or thoracic back pain. Cough + 2 = Cough + fever and hemoptysis, Cough + fever and thoracic pain, Cough + shortness of breath and fever. Other 1 = axillary adenopathy, back pain, left thoracic pain, tachycardia, or vomiting. ID = Incidental discovery; MD = Multiple organ diffusion; C = complications.
Figure 2.
The main symptoms associated with organs involved in CE in pediatric patients: Liver, Lung, and multiple organ diffusion (A and B). The organs correlated with MD (C) and its potential to generate complications (D) and the influence on the hospitalization period (E and F). AP = abdominal pain; AP +1 = Abdominal pain +1 = Abdominal pain with fever. AP +2 = Abdominal pain +2 = Abdominal pain + fever + headache and Abdominal pain + nausea and vomiting. Cough + 1 = Cough associated with one of the following symptoms: fever, hemoptysis, shortness of breath, or thoracic back pain. Cough + 2 = Cough + fever and hemoptysis, Cough + fever and thoracic pain, Cough + shortness of breath and fever. Other 1 = axillary adenopathy, back pain, left thoracic pain, tachycardia, or vomiting. ID = Incidental discovery; MD = Multiple organ diffusion; C = complications.
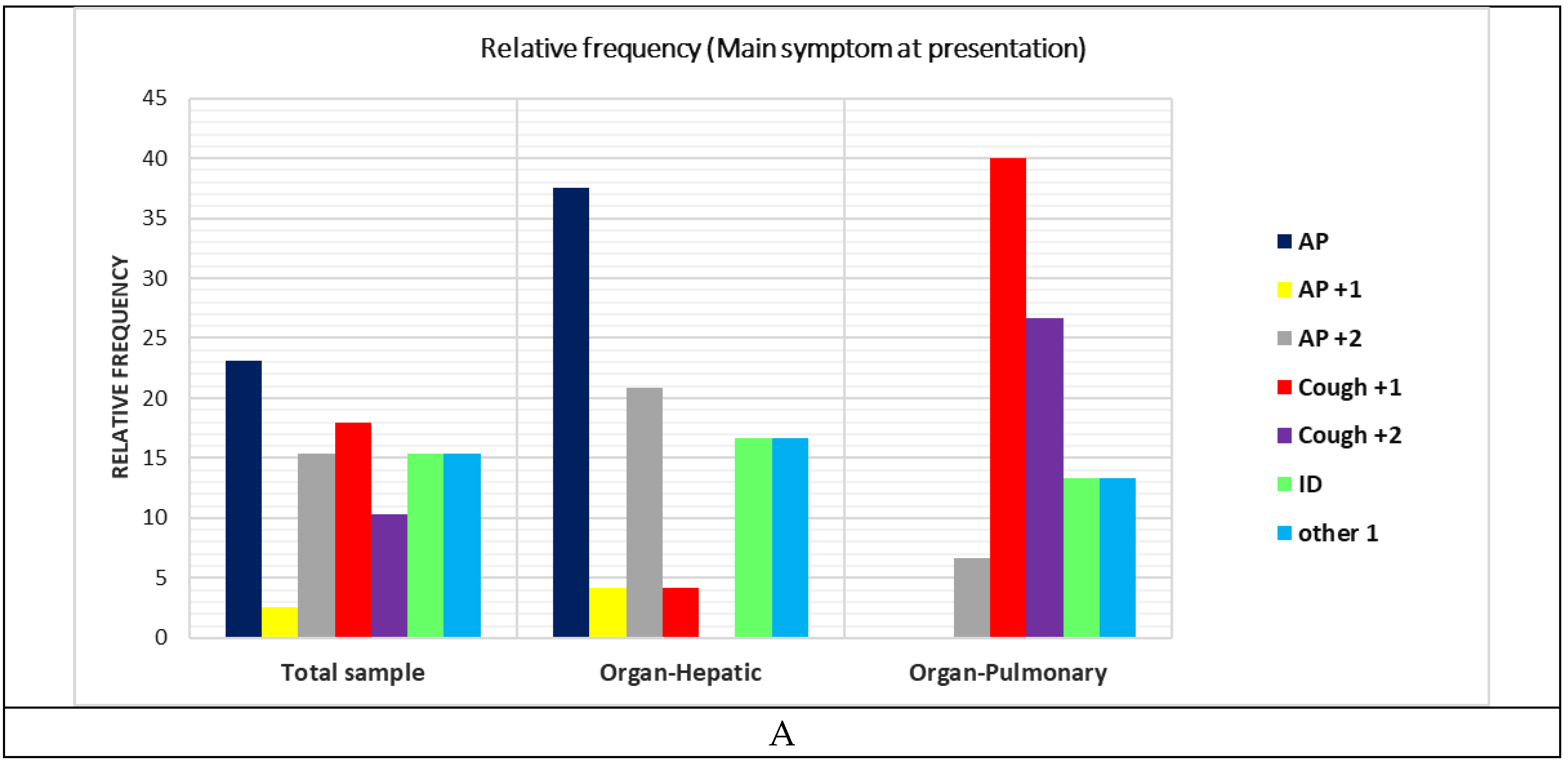
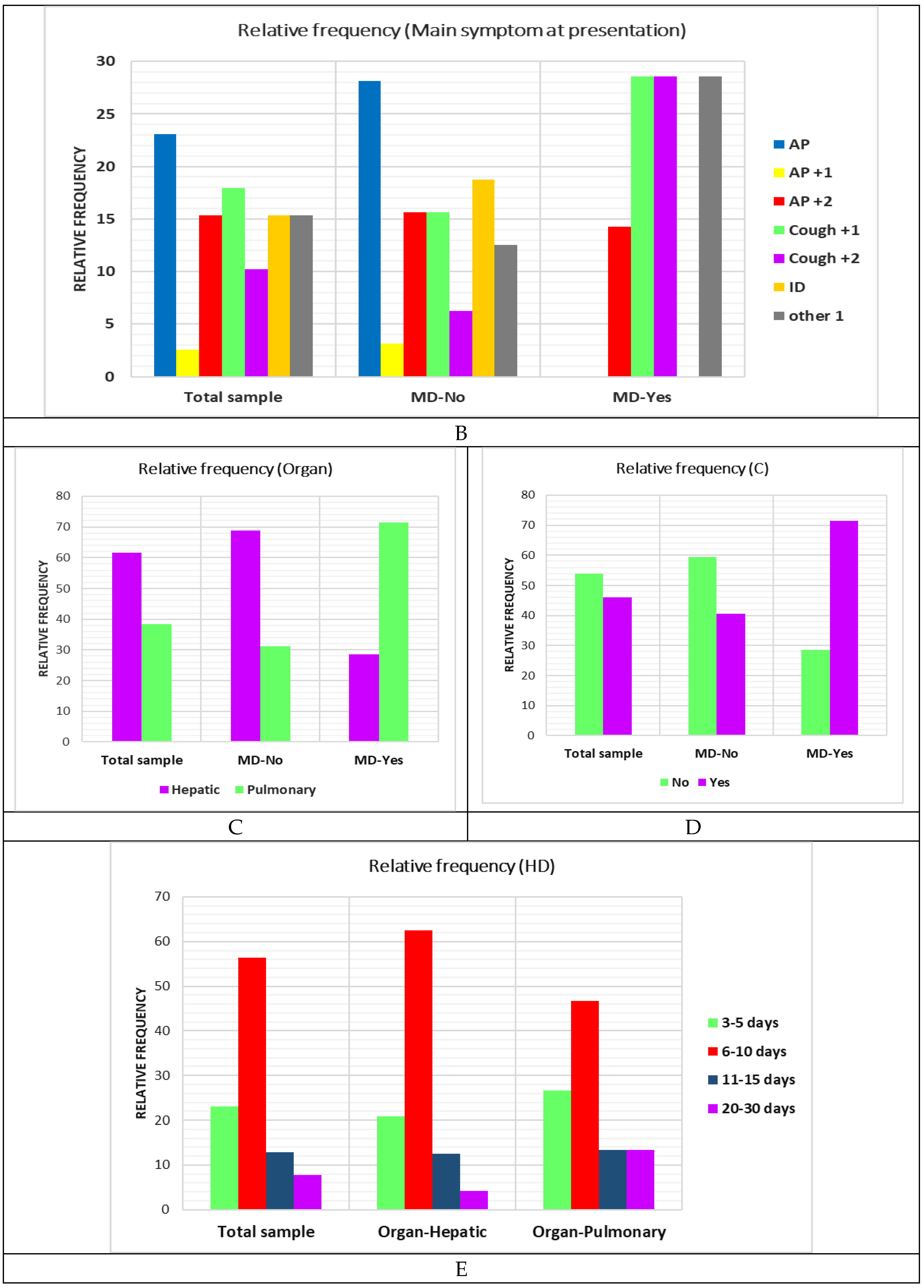
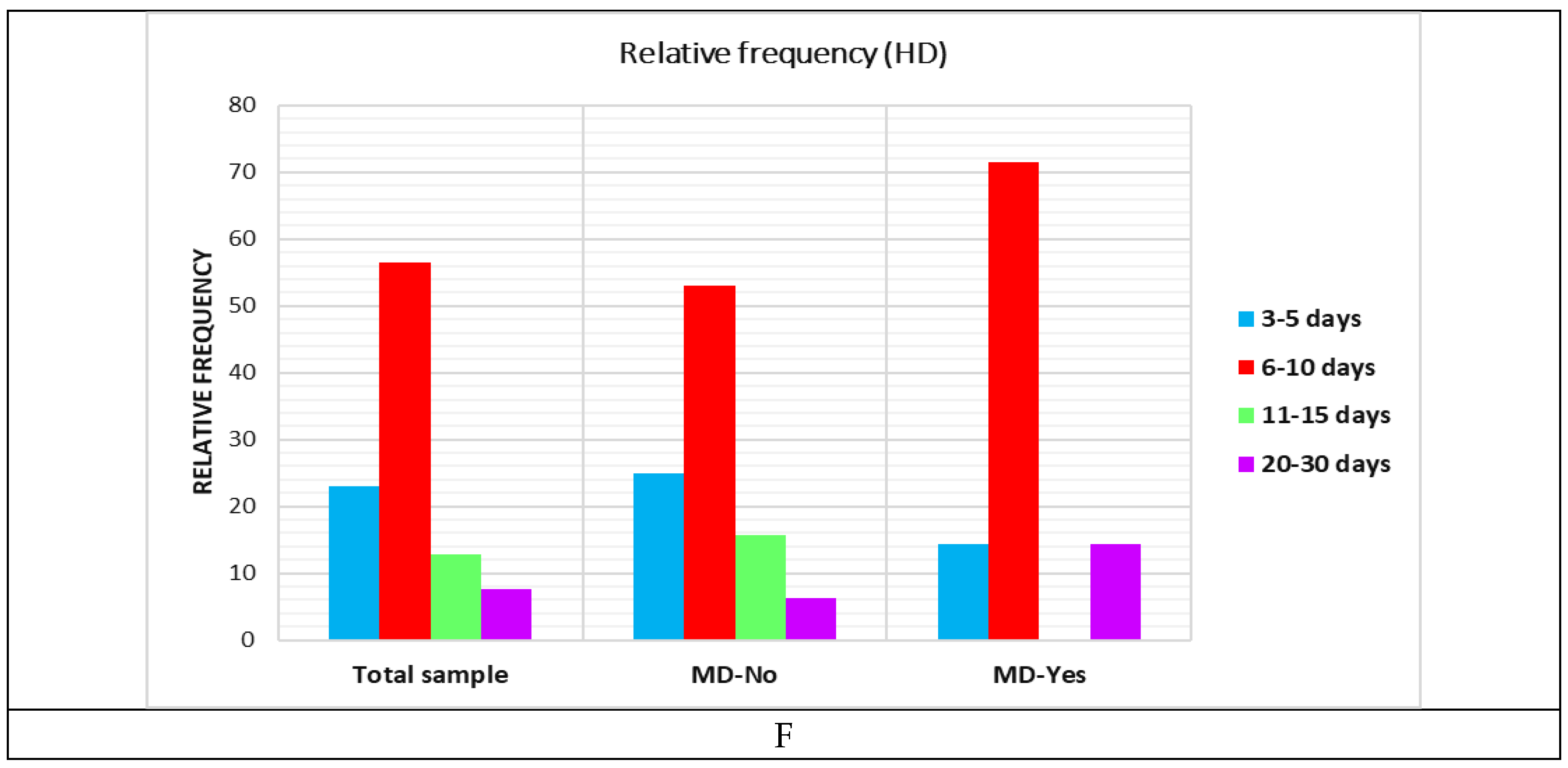
Figure 3.
CE complications and correlated factors: A. Complication type and relative frequency, B. Main symptoms at presentation (MSP), C. Organ involvement, D. IgE > 100, E. IgG > 1.1, F. Eos > 0.5, G. Treatment.
Figure 3.
CE complications and correlated factors: A. Complication type and relative frequency, B. Main symptoms at presentation (MSP), C. Organ involvement, D. IgE > 100, E. IgG > 1.1, F. Eos > 0.5, G. Treatment.
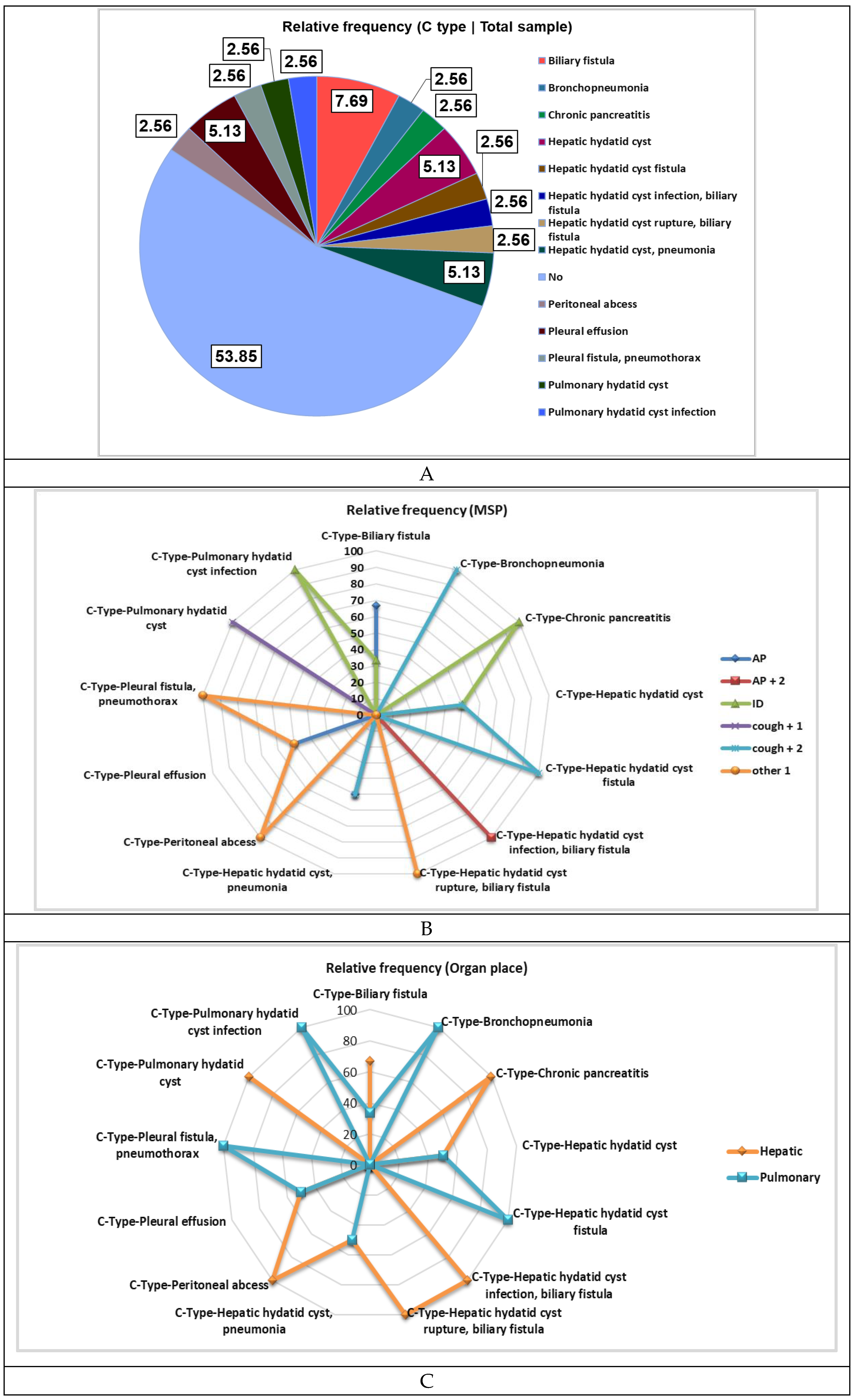
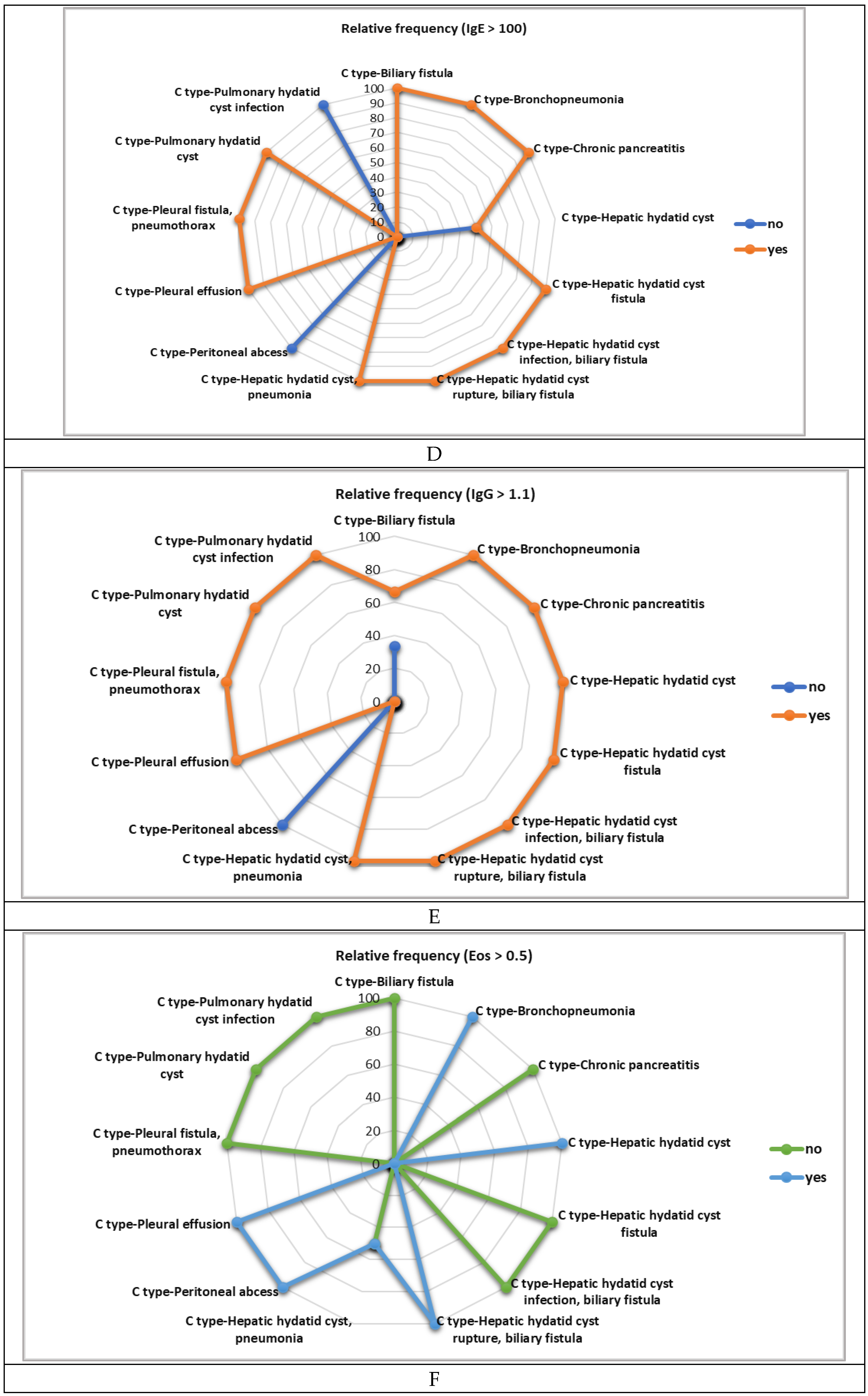
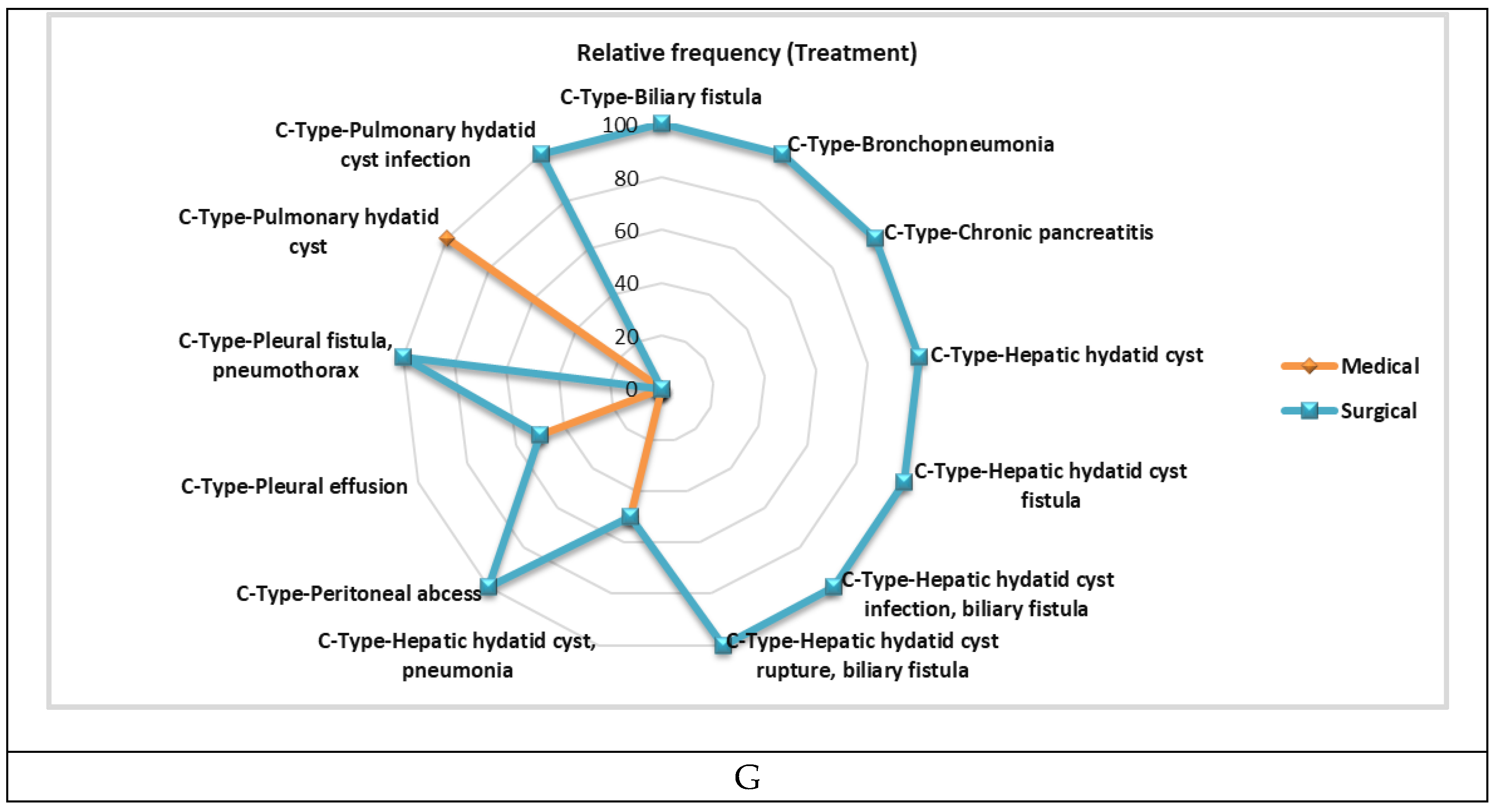
Figure 4.
The main symptoms manifested at presentation in pediatric emergency correlated with (A) rural/urban residence; (B) Animal contact; (C) Animal type; (D) Organ involved. AP = abdominal pain; AP +1 = Abdominal pain + 1 = Abdominal pain with fever. AP +2 = Abdominal pain + 2 = Abdominal pain + fever and headache and Abdominal pain + nausea and vomiting. Cough +1 = Cough associated with one of the following symptoms: fever, hemoptysis, shortness of breath, or thoracic back pain. Cough +2 = Cough + fever and hemoptysis, Cough + fever and thoracic pain, Cough + shortness of breath and fever. Other 1 = axillary adenopathy, back pain, left thoracic pain, tachycardia, or vomiting. ID = Incidental discovery.
Figure 4.
The main symptoms manifested at presentation in pediatric emergency correlated with (A) rural/urban residence; (B) Animal contact; (C) Animal type; (D) Organ involved. AP = abdominal pain; AP +1 = Abdominal pain + 1 = Abdominal pain with fever. AP +2 = Abdominal pain + 2 = Abdominal pain + fever and headache and Abdominal pain + nausea and vomiting. Cough +1 = Cough associated with one of the following symptoms: fever, hemoptysis, shortness of breath, or thoracic back pain. Cough +2 = Cough + fever and hemoptysis, Cough + fever and thoracic pain, Cough + shortness of breath and fever. Other 1 = axillary adenopathy, back pain, left thoracic pain, tachycardia, or vomiting. ID = Incidental discovery.
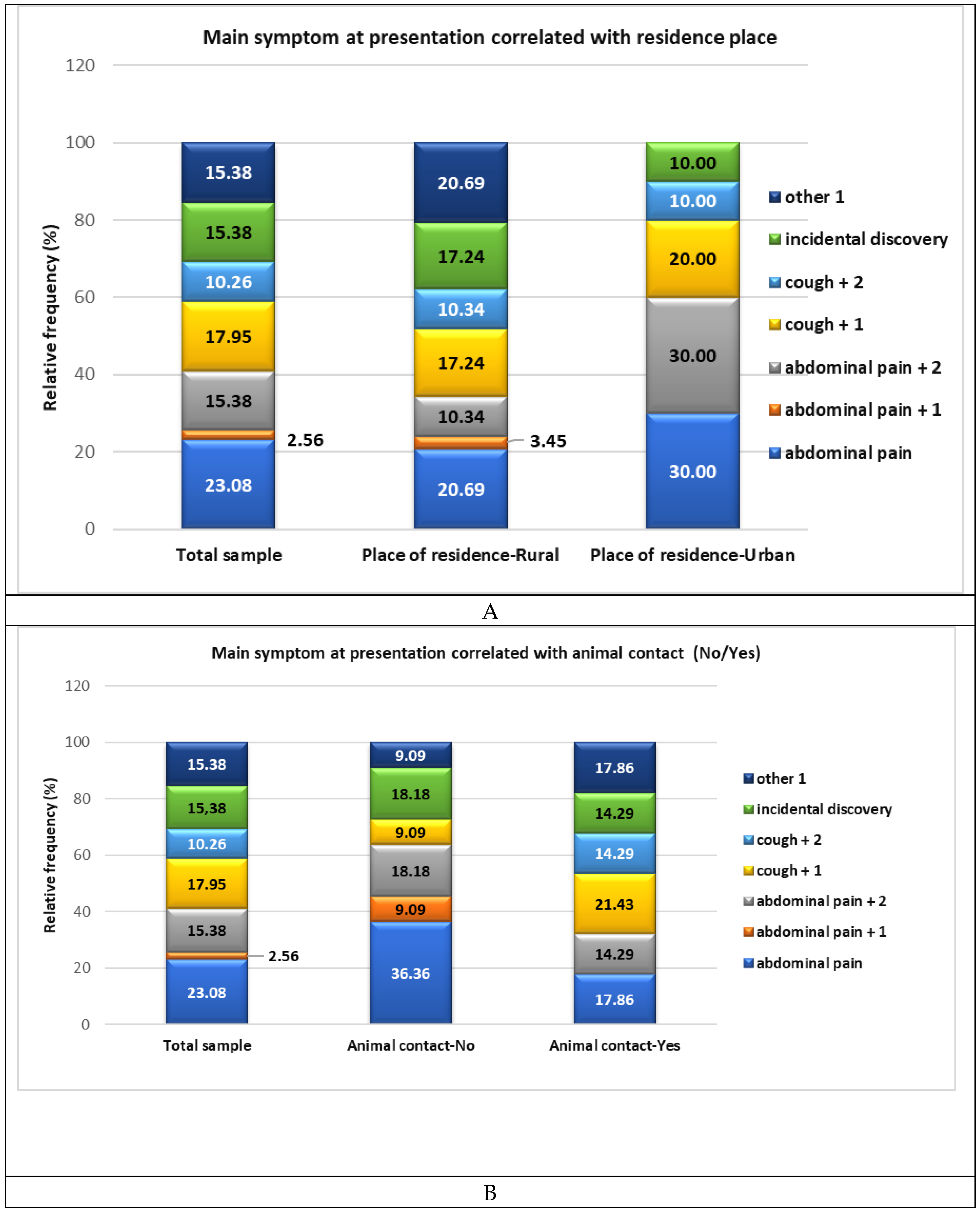
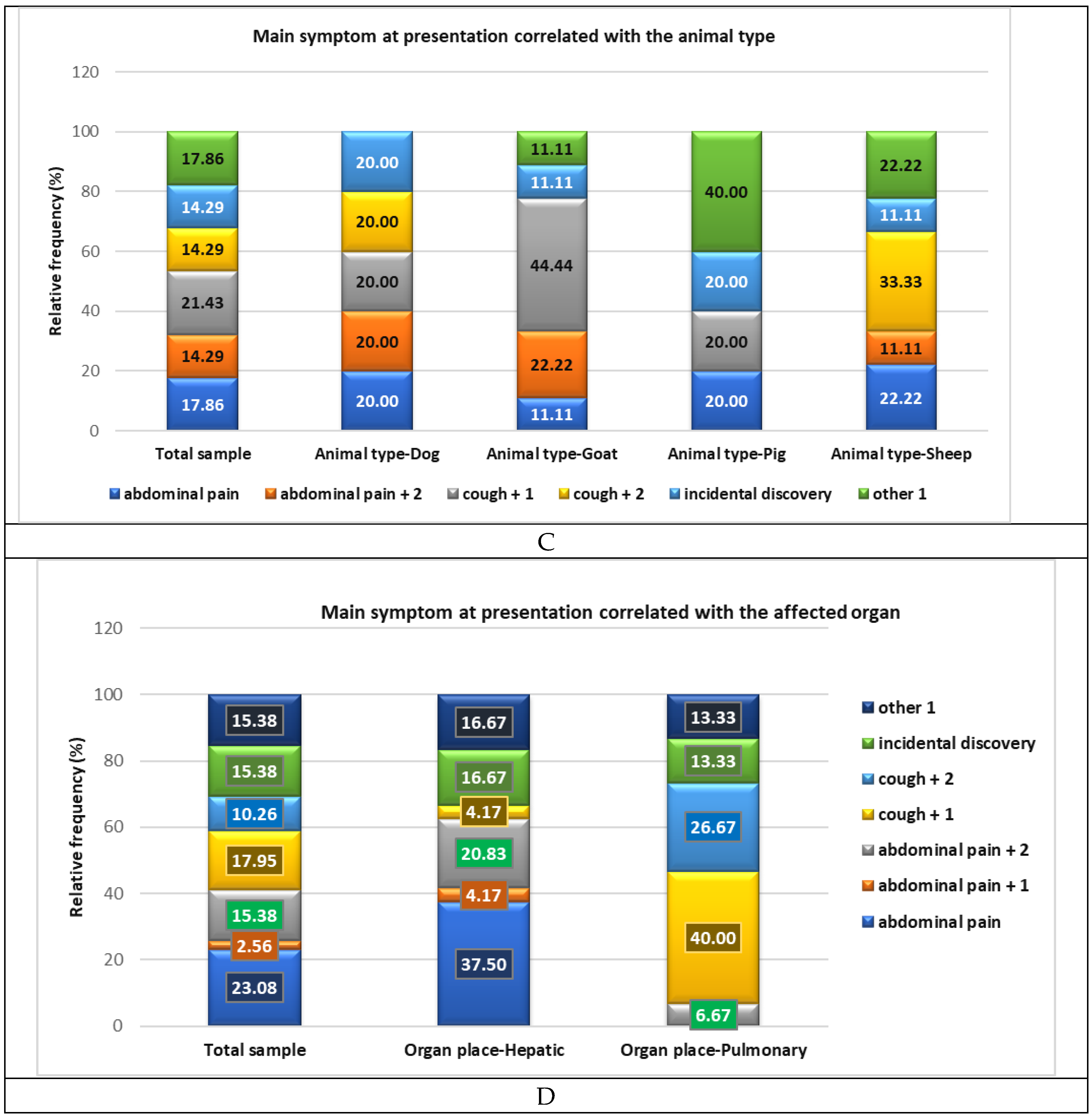
Figure 5.
Organ involvement correlated to animal-type contact (A-C): A. Hepatic. B. Pulmonary. C. Multiple organ dissemination; D. Animal-type contact correlated with complications.
Figure 5.
Organ involvement correlated to animal-type contact (A-C): A. Hepatic. B. Pulmonary. C. Multiple organ dissemination; D. Animal-type contact correlated with complications.
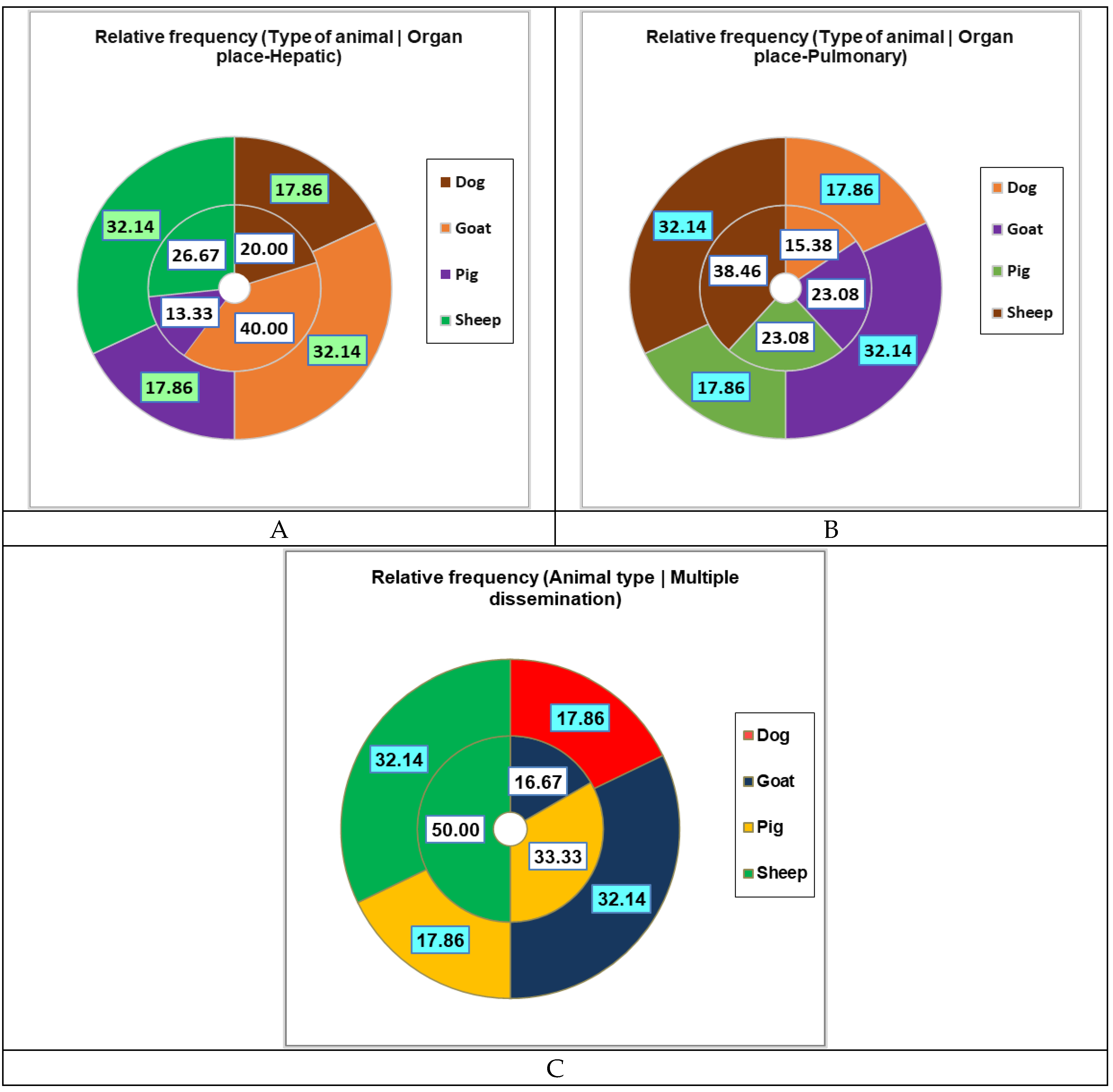
Figure 6.
Correlations between sociodemographics of pediatric patients with A. the main clinical manifestations and organ involvement; B. laboratory parameters, complications, treatment, days of hospitalization, and multiple hospitalizations; C. Heat map with significant statistical differences in pediatric patients correlated to animal contact. Abdominal pain + 1 = Abdominal pain with fever. Abdominal pain + 2 = Abdominal pain + fever and headache and Abdominal pain + nausea and vomiting. Cough + 1 = Cough associated with one of the following symptoms: fever, hemoptysis, shortness of breath, or thoracic back pain. Cough + 2 = Cough + fever and hemoptysis. Cough + fever and thoracic pain. Cough + shortness of breath and fever. Other 1 = axillary adenopathy, back pain, left thoracic pain, tachycardia, or vomiting. AC = animal contact; MD = multiple dissemination; C = complications; TS = surgical treatment; TM = medical treatment (Albendazole); MH = multiple hospitalizations; NA = no animal contact; Eos = Eosinophilia.
Figure 6.
Correlations between sociodemographics of pediatric patients with A. the main clinical manifestations and organ involvement; B. laboratory parameters, complications, treatment, days of hospitalization, and multiple hospitalizations; C. Heat map with significant statistical differences in pediatric patients correlated to animal contact. Abdominal pain + 1 = Abdominal pain with fever. Abdominal pain + 2 = Abdominal pain + fever and headache and Abdominal pain + nausea and vomiting. Cough + 1 = Cough associated with one of the following symptoms: fever, hemoptysis, shortness of breath, or thoracic back pain. Cough + 2 = Cough + fever and hemoptysis. Cough + fever and thoracic pain. Cough + shortness of breath and fever. Other 1 = axillary adenopathy, back pain, left thoracic pain, tachycardia, or vomiting. AC = animal contact; MD = multiple dissemination; C = complications; TS = surgical treatment; TM = medical treatment (Albendazole); MH = multiple hospitalizations; NA = no animal contact; Eos = Eosinophilia.
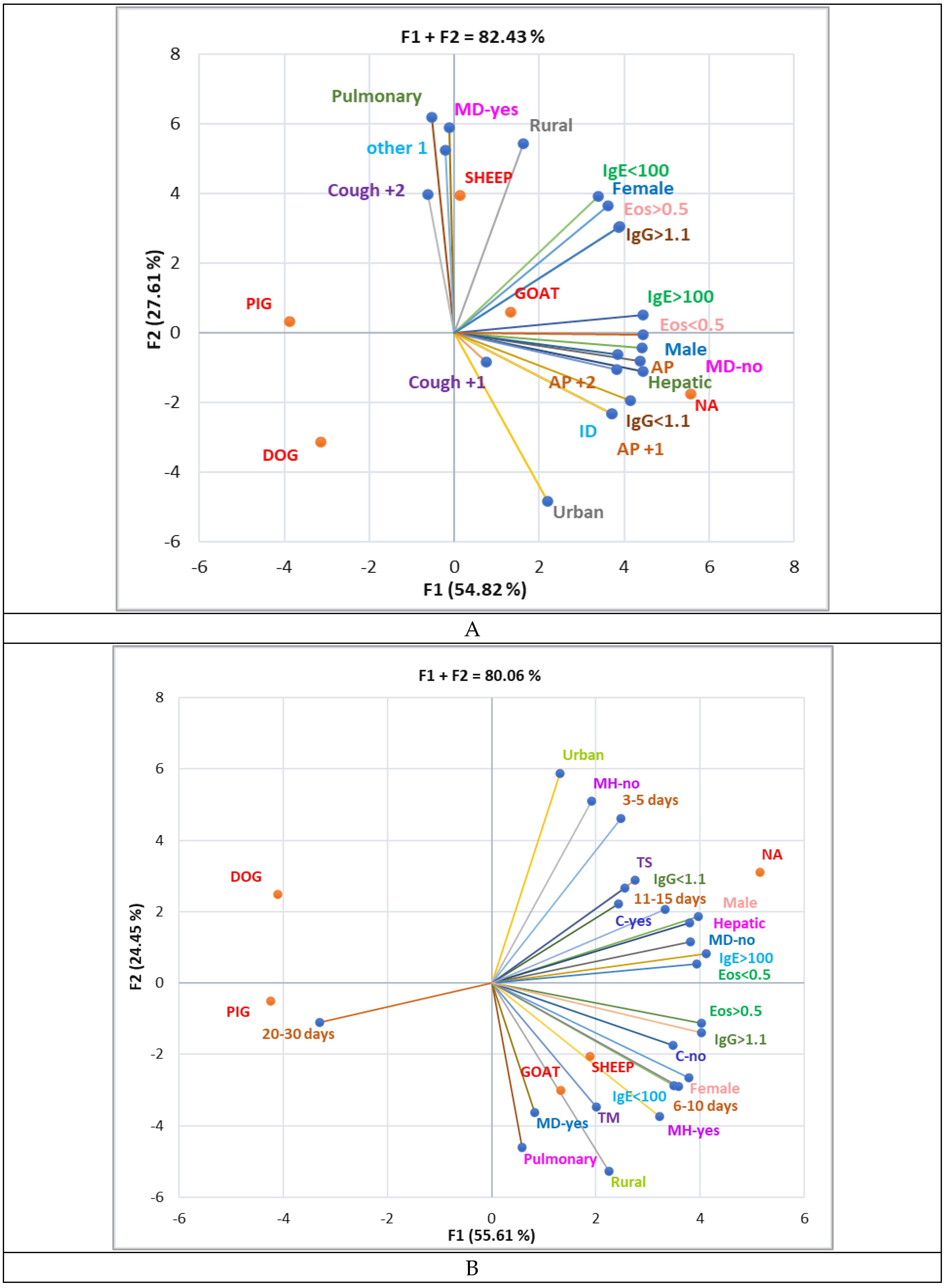
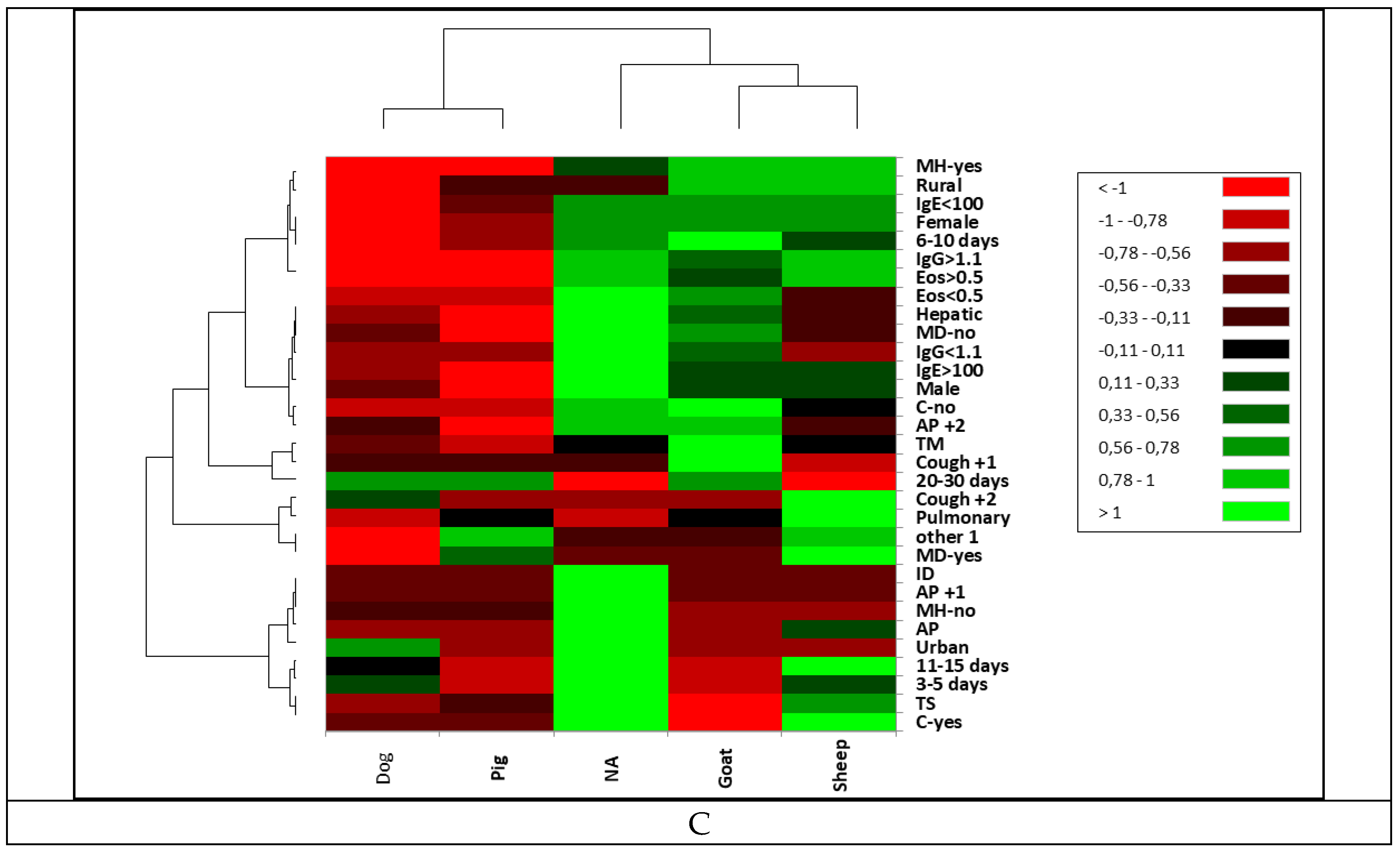

Table 1.
General data of the pediatric patients' group (n = 39)
|
Children 2-15 years (average age = 9.84 years) |
Total | Rural residence | Urban residence | p-value | ||||
| Nr | % | Nr | % | Nr | % | |||
| 39.00 | 100.00 | 29.00 | 74.36 | 10.00 | 25.64 | < 0.05 | ||
| Sex | Female | 15.00 | 38.46 | 13.00 | 44.83 | 2.00 | 20.00 | < 0.05 |
| Male | 24.00 | 61.54 | 16.00 | 55.17 | 8.00 | 80.00 | ||
| Animal contact |
No | 11.00 | 28.21 | 5.00 | 17.24 | 6.00 | 60.00 | < 0.05 |
| Yes | 28.00 | 71.79 | 24.00 | 82.76 | 4.00 | 40.00 | ||
| Animal type |
Dog | 5.00 | 17.86 | 1.00 | 4.17 | 4.00 | 100.00 | < 0.05 |
| Goat | 9.00 | 32.14 | 9.00 | 37.50 | 0.00 | 0.00 | ||
| Pig | 5.00 | 17.86 | 5.00 | 20.83 | 0.00 | 0.00 | ||
| Sheep | 9.00 | 32.14 | 9.00 | 37.50 | 0.00 | 0.00 | ||
Table 2.
The main aspects investigated in CE pediatric patients during hospitalization.
| Aspect | Total | Days of hospitalisation | |||||||||
| 3-5 days | 6-10 days | 11-15 days | 20-30 days | ||||||||
| N | % | N | % | N | % | N | % | N | % | ||
| Signs | AP | 9.00 | 23.08 | 3.00 | 33.33 | 5.00 | 22.73 | 1.00 | 20.00 | 0.00 | 0.00 |
| AP+1 | 1.00 | 2.56 | 0.00 | 0.00 | 1.00 | 4.55 | 0.00 | 0.00 | 0.00 | 0.00 | |
| AP+2 | 6.00 | 15.38 | 1.00 | 11.11 | 5.00 | 22.73 | 0.00 | 0.00 | 0.00 | 0.00 | |
| Cough+1 | 7.00 | 17.95 | 1.00 | 11.11 | 4.00 | 18.18 | 1.00 | 20.00 | 1.00 | 33.33 | |
| Cough+2 | 4.00 | 10.26 | 2.00 | 22.22 | 2.00 | 9.09 | 0.00 | 0.00 | 0.00 | 0.00 | |
| ID | 6.00 | 15.38 | 1.00 | 11.11 | 2.00 | 9.09 | 2.00 | 40.00 | 1.00 | 33.33 | |
| Other 1 | 6.00 | 15.38 | 1.00 | 11.11 | 3.00 | 13.64 | 1.00 | 20.00 | 1.00 | 33.33 | |
| Organ | Liver | 24.00 | 61.54 | 5.00 | 55.56 | 15.00 | 68.18 | 3.00 | 60.00 | 1.00 | 33.33 |
| Lung | 15.00 | 38.46 | 4.00 | 44.44 | 7.00 | 31.82 | 2.00 | 40.00 | 2.00 | 66.67 | |
| MD | no | 32.00 | 82.05 | 8.00 | 88.89 | 17.00 | 77.27 | 5.00 | 100.00 | 2.00 | 66.67 |
| yes | 7.00 | 17.95 | 1.00 | 11.11 | 5.00 | 22.73 | 0.00 | 0.00 | 1.00 | 33.33 | |
| C | no | 21.00 | 53.85 | 5.00 | 55.56 | 13.00 | 59.09 | 2.00 | 40.00 | 1.00 | 33.33 |
| yes | 18.00 | 46.15 | 4.00 | 44.44 | 9.00 | 40.91 | 3.00 | 60.00 | 2.00 | 66.67 | |
| Treatment | TM | 11.00 | 28.21 | 5.00 | 55.56 | 6.00 | 27.27 | 0.00 | 0.00 | 0.00 | 0.00 |
| TS | 28.00 | 71.79 | 4.00 | 44.44 | 16.00 | 72.73 | 5.00 | 100.00 | 3.00 | 100.00 | |
| MH | no | 21.00 | 53.85 | 5.00 | 55.56 | 11.00 | 50.00 | 3.00 | 60.00 | 2.00 | 66.67 |
| yes | 18.00 | 46.15 | 4.00 | 44.44 | 11.00 | 50.00 | 2.00 | 40.00 | 1.00 | 33.33 | |
| IgE > 100 | No | 7.00 | 17.95 | 2.00 | 22.22 | 4.00 | 18.18 | 1.00 | 20.00 | 0.00 | 0.00 |
| yes | 32.00 | 82.05 | 7.00 | 77.78 | 18.00 | 81.82 | 4.00 | 80.00 | 3.00 | 100.00 | |
| Eos > 0.5 | No | 26.00 | 66.67 | 8.00 | 88.89 | 12.00 | 54.55 | 3.00 | 60.00 | 3.00 | 100.00 |
| yes | 13.00 | 33.33 | 1.00 | 11.11 | 10.00 | 45.45 | 2.00 | 40.00 | 0.00 | 0.00 | |
| IgG > 1.1 | No | 8.00 | 20.51 | 3.00 | 33.33 | 4.00 | 18.18 | 1.00 | 20.00 | 0.00 | 0.00 |
| yes | 31.00 | 79.49 | 6.00 | 66.67 | 18.00 | 81.82 | 4.00 | 80.00 | 3.00 | 100.00 | |
Signs = main symptoms at presentation in the Emergency Service; AP = abdominal pain; AP +1 = Abdominal pain + 1 = Abdominal pain with fever. AP +2 = Abdominal pain + 2 = Abdominal pain + fever and headache and Abdominal pain + nausea and vomiting. Cough + 1 = Cough associated with one of the following symptoms: fever, hemoptysis, shortness of breath, or thoracic back pain. Cough + 2 = Cough + fever and hemoptysis, Cough + fever and thoracic pain, Cough + shortness of breath and fever. Other 1 = axillary adenopathy, back pain, left thoracic pain, tachycardia, or vomiting. ID = Incidental discovery; MD = Multiple organ diffusion; C = complications; TM = medical treatment (with Albendazole); TS = Surgical treatment; MH = multiple hospitalizations; Eos = Eosinophilia (N/µL), IgE (i.u./mL), IgG (i.u./mL).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



