1. Introduction
A recent study showed that 22% of patients in retirement homes [
1] developed Acquired Deforming Hypertonia (ADH). Given the importance of the retirement home population, likely to be increasing in coming years due to the ageing of the population, the number of people affected by these deformations is growing. In France, in 2015, approximately 728,000 patients were cared for in residential care for the elderly [
2]. Some of theses ADH problems are accessible for botulinum toxin injections [
3] but others problems require surgical procedures.
Considerably less invasive surgical techniques for these patients have being developped, allowing them to return quickly to their usual setting and avoiding perioperative destabilisation [
4]. Previous research has underlined that these patients are particularly sensitive to the change of environment when they are institutionalised in a retirement home in particular. It has been shown in studies focusing particularly on femoral neck fractures in elderly patients with rates of over 42% postoperative confusion with behaviours that can become aggressive and have a risk of abuse [
5]. These techniques (percutaneous tenotomies in particular) are not recent since such gestures (today with analgesia in addition obviously) were already practised in the 18th century [
6]. Needle tenotomy have been developped, which is well tolerated and yields a significant increase in range of motion when tenotomise knee flexor [
4] and finger flexor [
7] with no unwanted effects [
4,
7]. This technique could be used in an ambulatory care setting or within institutions for severely disabled individuals [
7]. Skills of anaesthesiologists in deep sedation to avoid as much as possible general anaesthesia to these patients are very helfull (general anaesthesia can be complicated by hemodynamic repercussions with specially marked hypotension responsible for hypo cerebral perfusion, causing postoperative confusion, increased perioperative morbidity and length of stay of patients). Sedation is more successful in many centres, especially in elderly patients with comorbidity, such as cardiac valve surgery [
8].
To deploy such surgery without moving patients, it was considered attractive to explore the idea of developing a mobile unit such as ones already existing in different situations: for cataract treatment in India [
9], treatment of recent strokes in Europe [
10], vascular grafts in a truck equipped with a bioreactor in Germany [
11], or several learning units (Mobile Lab learning arthroscopy, Virtamed©), radiographic diagnosis or analysis laboratory (for instance sports events), mobile units in the nursing home: odontology, radiology. In literature, when searching on PubMed with the words « Mobile + Unit » in the title, it led to 108 papers. Most of these papers, except the papers cited behind, describe mobile units for diagnosing or following up chronic diseases (HIV, cancers, etc.). Additionally, we found several papers describing mobile units for treatment, in particular for stroke [
12], cardio-vascular support [
13,
14] and chronic wound [
15]. To our knowledge, none of the previous researches described mobile units for mini-invasive surgical treatment. For most of these mobile units, the purpose was the diagnosis. The mobile unit is a good alternative for diagnosis (and, in some cases, treatment) when the population cannot benefit from medical care easily. The low cost is also considered as an advantage. All these units have provided good management of these patients (particularly without additional risk of infection in the case of cataract treatment in India [
9]) and with a possibility of faster control for stroke, treated with mobile thrombolysis unit in Europe [
10], which is accompanied by a decrease in the sequelae of these patients. Regarding the experience of vascular grafting in an equipped truck [
11], the goal was mainly to have access to this technology in different institutions, possibly thanks to unit’s mobility. It is the same for the different units focused on learning and diagnosis.
However, the literature is poor on acquired deforming hypertonia for elderly patients: only two papers have been published to date on this topic. The first published is the study by Dehail et al. [
1] which evaluates the percentage of patients who developed uncomfortable ADH. The second [
16], from the same team, published in 2018, described etiological factors contributing to developing joint contractures and ADH in older people. The pathophysiologic mechanisms of joint contractures in animal models are also presented. Based on this review, in the case of ADH, several challenges have been identified by the main author in the design of a mobile unit to take care of all functional handicaps to allow:
- -
adaptation of technical aids (orthoses, sticks, adapted wheelchair, etc.),
- -
solutions addressing the deformations (Botulinum toxin injections, minimally invasive interventions like percutaneous tenotomy) to allow better AutoNOMy, installation in bed, chair, verticalization, nursing, and dressing,
- -
the reorientation, if necessary, of residents to a hospital unit,
- -
the possibility of giving ad hoc advice via an e-consulting office (telemedicine) for residents and elderly patients living around the structure (the retirement home can then be a real mobile health home).
Innovation is key in managing increasing constraints and constrained public spending [
17]. It has been underlined that healthcare innovation mainly focuses on diffusion and experimental evaluation of innovative existing technologies and medical processes [
18]. But when imagining several innovative organisational solutions to medical treatment, there is a strong need for a structured approach:
It is needed to precisely model the medical issue (here, the multiple ADH impacts on a population of aged persons) and to assess the remaining pain points corresponding to the existing organisational solution(s) of the medical treatment,
From this primary analysis, it is necessary to generate (or ideate) a number of a priori relevant scenarios of effective and efficient organisational solutions (here, solutions based on a mobile unit) to medical treatment,
From this latter enumeration, it is necessary to quickly and, a priori, assess the global value of these innovative organisational solutions in terms of their ability to alleviate the whole “quantities of pain” [
18] of the medical issue. It is also necessary to further validate the best a priori solutions in real conditions. Thus, it implies disposing of a decision-making method able to aggregate the capability of an organisational solution to alleviate the pains in the context of a medical issue.
This is why the main author of this article, involved in taking care of ADH people since 2015, decided to associate with, on the one hand, experts in logistics and healthcare systems to address point 2 properly, and on the other hand, an expert in innovation management and design science who is the inventor of the Radical Innovation Design (RID) methodology [
18] to address points 1 and 3 correctly. RID has already been used to improve dental radiologis
t’s activity [
19]. Innovative organisational solutions are explored with the double objective of addressing functional disabilities, improving the quality of life in the long-term care of patients, as well as the quality of the daily work of all the professionals working in retirement homes.
The aim of this research was to use a collective progress methodology (RID) to find innovative therapeutic process solutions, in order to advance therapeutic care in ADH problems in retirement homes in France.
2. Materials and Methods
1-. RID Methodology
Innovation in the healthcare sector is a critical activity. However, it has already been pointed out that the design approaches in healthcare are only beginning to develop and still need to be better adapted for the healthcare sector. Moreover, the focus on device development rather than the services (such as healthcare pathways design and modelling) has been underlined [
20]. Several approaches, such as user-centred design or design thinking, have already been implemented and adapted to the healthcare sector [
21,
22,
23,
24,
25].
Radical Innovation Design is a novel, complete and well-structured innovative design methodology that prioritizes the improvement of the user experience within a context of activity (here applied to the care of French patients suffering from ADH). RID considers innovative design as the improvement of the activity support solution (made of product, service, and organization parts) to augment the performances of a future activity. RID guides innovators who want to systematically explore users’ problems and unstated needs, and evaluate which ones are most pressing in terms of innovation, taking into account the effectiveness of existing solutions in contributing to a satisfactory practice of activity. RID renews the way to define innovation targets along with the obtention of a prioritized set of value buckets. Value buckets, the frequent usage situations where major problems are experienced and for which the current solutions provide little or no relief, are the starting point in the RID methodology to pose questions for starting the ideation sessions. The objective is that identification and solving problems defined by value bucket to create unaddressed usefulness value for users (here patients and medical staff). With its emphasis on problem exploration, RID differs from methods based on early prototyping and goes beyond “design thinking” approaches. The RID methodology has been validated in various industrial and business sectors. A complete and open access book on RID methodology can be found in [
18].
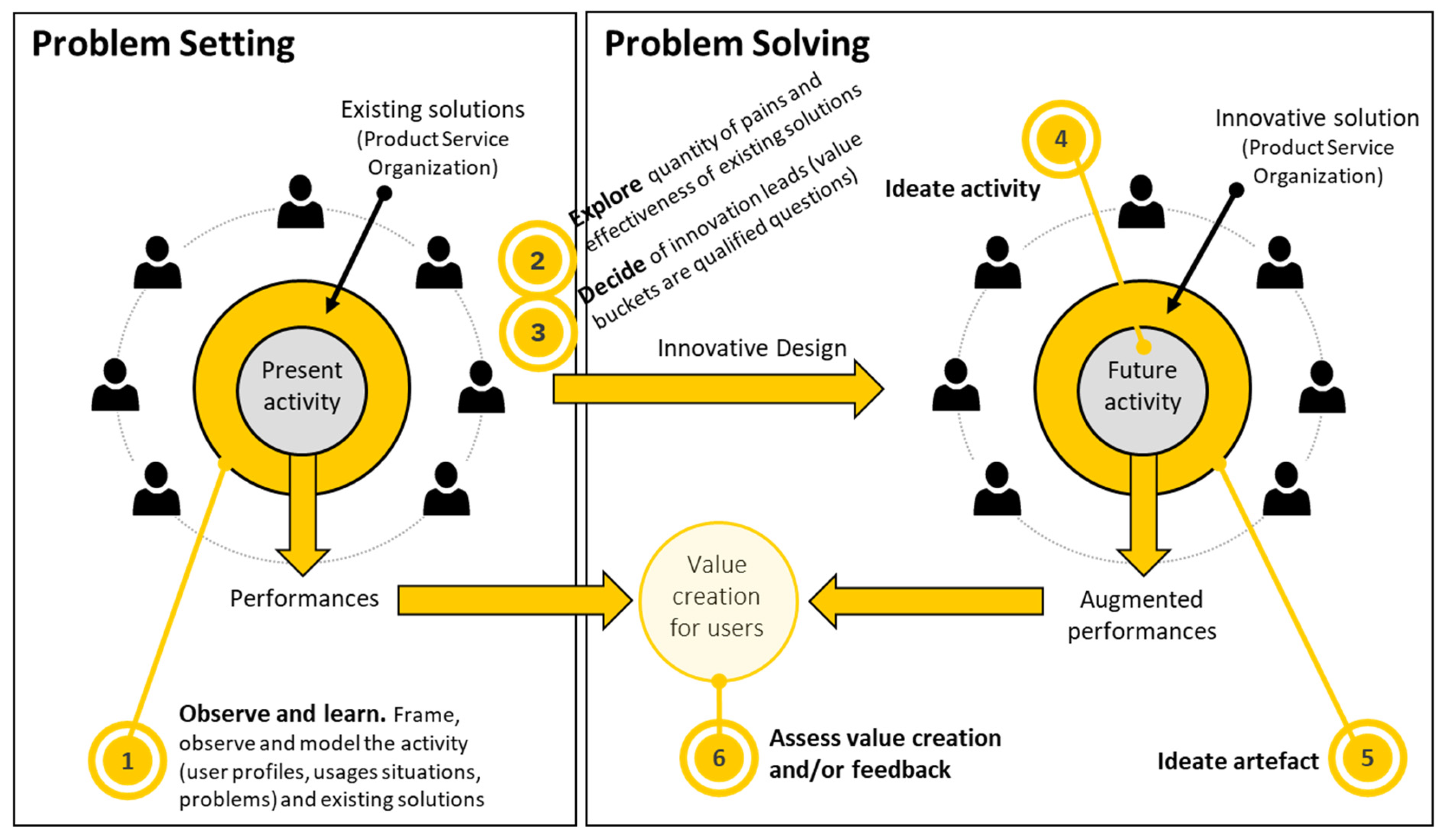
The RID process is the core of the Radical Innovation Design
® methodology [
18]. The generic RID process encompasses three key stages (see
Figure 1):
- -
-
Observe and learn (stage #1 of
Figure 1): A phase of observations and interviews allow to better comprehend the activity to:
- ○
First, parameterize the activity into distinct categories of user profiles, usage situations, problems, and existing solutions.
- ○
Second, learn from links between these categories by answering to seven simple questions on one, two or three activity dimensions at a time (among user profiles, usage situations, problems, existing solutions). These questions are very simple, and experts and users are appropriately queried on specific questions to contribute to a systemic representation of the activity practice; one speaks of building a cognitive model of the activity.
This process of activity investigation and learning is abundantly depicted by Salehy et al
. [
26].
- -
Explore and decide (stages #2 and #3): The cognitive model is investigated, particularly by determining useful targets for innovation, i.e., major problems experienced by number of people during frequent usage situations and for which the current solutions provide little or no relief. These innovation leads are called value buckets in RID and they are computed by dedicated algorithms in the RID compass method.
- -
Ideate, design and assess (Tags #4, #5 and #6): The most important value buckets are used as qualified questions—starting points—for brainstorming. Then, the new solution architecture (combination of products, services and organization) is designed, prototyped, and finally assessed in terms of its ability to (better) perform the activity. This assessment of the innovative solution is achieved by the RID comparator method (18) which allows comparing the usual solutions and the innovative one to effectively achieve the activity in all usage situations experimented by users in the scope of activity.
Previous publications on RID methodology focused on developing innovative product, service and/or organisation (
Table 1). In this paper, we propose applying the RID methodology to model the new scenario for medical treatment of ADH.
2- The Interviews (supplementary file 1)
Then, an observation stage based on interviews enabled us to determine user profiles, usage situations, problems, and existing solutions. Semi-structured interviews were organised as follows: 1) Presentation of the objectives of the study, 2) Questions about the causes that lead to difficulties in ADH management, and 3) Questions about their perceived expectation in designing and deploying a potential mobile unit. The duration of interviews was variable, but generally, it was around 40 min (especially for patients currently suffering from ADH). Minutes for discussions were created, and coding and analysis were done manually.
The discussions also helped us to define the cognitive model of the ADH detection and treatment activity. We obtained the value buckets from this stage (with RID compass method), which have been the ideation seeds for determining new potential solutions. We then built different solutions to manage patients, considering the guidelines obtained from the previous stages. Evaluation criteria were determined to assess these solutions: number of patients, overall costs, number of transportations, type of transportation, quality of healthcare, quality of work environment for the medical staff, number of retirement homes that can benefit from the proposed solution, and logistics difficulty.
3- RID comparator method
Once the best solution determined, we assessed it in terms of its effectiveness in different usage situations and compared it to present ADH detection and treatment solutions.
3. Results: Application of the RID Methodology on Mobile Unit for ADH Care
1- The RID process
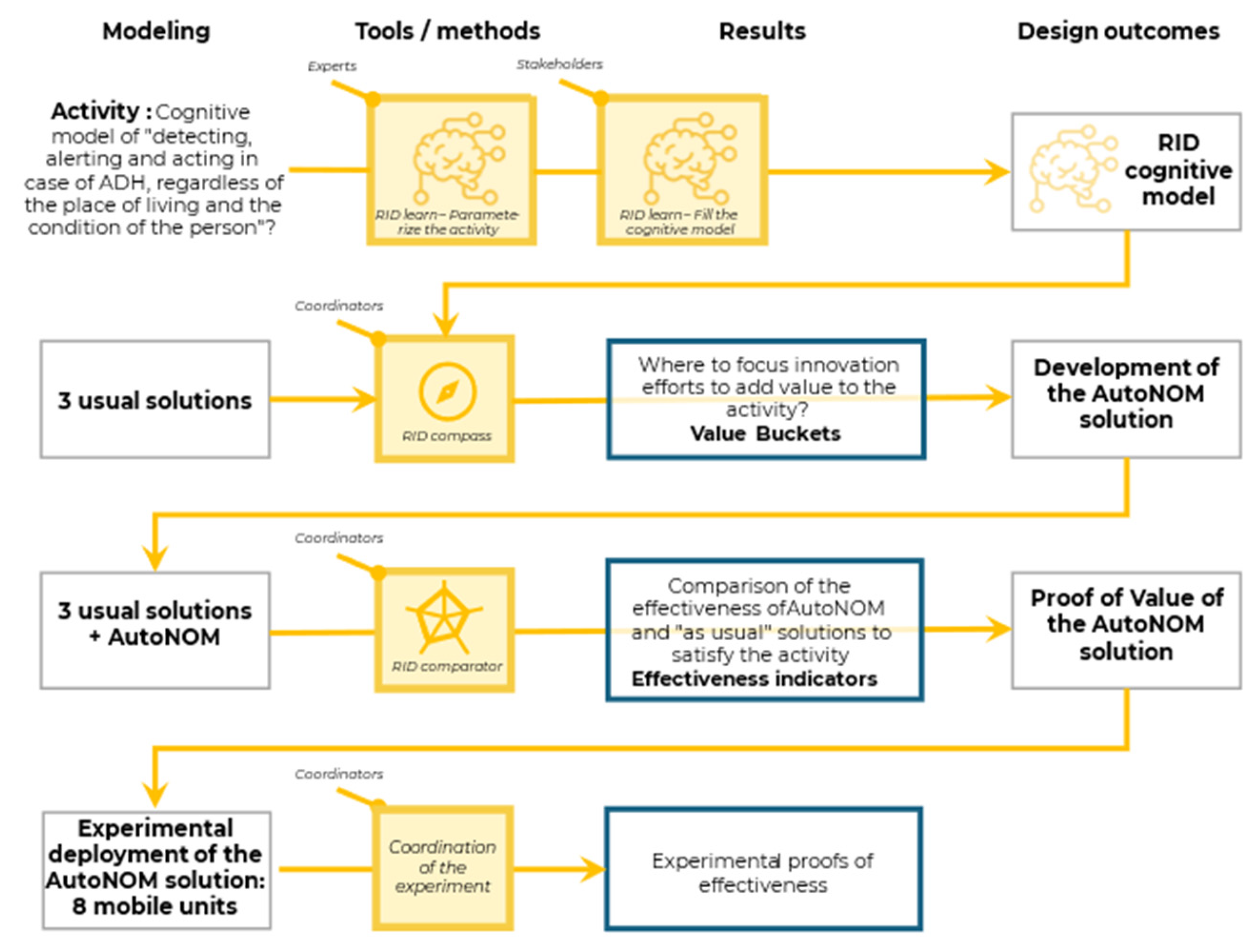
We used the RID methodology in all three stages (see
Figure 1) for the “AutoNOM” study (the project title addressing the ADH care). More refined RID process for this study can be seen in
Figure 2. We first defined the activity scope as “Detect, alert and act in case of ADH, whatever the place of living and the condition of the person” and the ideal goal of the activity as “Detect early enough any person developing ADH, whether or not that person is demented and dependent, regardless of where they live (home, retirement home), in order to treat them effectively while respecting their physical and cognitive state”.
Figure 2 shows the data collection process by defining the
“experts
” who are used to parameterize the cognitive model (find the categories) are the authors of this study working on ADH since 2015, the
“stakeholders
” who were used to fill in the data of the cognitive model are these same authors and two co-authors of the 2 main publications on ADH, and the
“coordinators
” who made the decisions at the level of the RID compass are all the authors, the RID comparator and
“idea
” an innovative solution.
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
2- The interviews
An interview-based methodology was proposed to identify different stakeholder pains and expectations. The stakeholders are further called user profiles and pains and expectations are gathered into the so-called problems. The stakeholders are the patients concerned, their entourage, retirement home staff, hospitals and other structures involved in managing functional disabilities. People interviewed have been all the people present and who have accepted the interviews during the various trips to the health site and to the retirement homes. These persons were:
- -
The operating room orthopaedic department of Raymond Poincaré Hospital (one anaesthesiologist, three nurse anaesthesiologists, two nurses, two surgeons, and one operating room manager),
- -
The consultation team of the orthopaedic department of Raymond Poincaré Hospital (a gypsotherapy nursing auxiliary, five nurses, a coordinating nurse, two nursing auxiliary, four Physical Medical Rehabilitator (PMR) doctors),
- -
The nursing team of the retirement home of Repotel Voisins-le-Bretonneux retirement home (one psychologist and one coordinating medical doctor),
- -
Three patients (two during a geriatric consultation in the Raymond Poincaré hospital and one during a retirement home visit).
These interviews have allowed us to identify and define user profiles in conjunction with the literature [
1]: patients and care team. We used three discriminating variables to generate and size twelve patient categories:
- -
-
Patient fragility/AutoNOMy regarding daily life:
- ○
Medium fragility for patients who have daily life activities without external aid.
- ○
High fragility for patients who need aid in their daily life activities.
- -
-
Life situation regarding the patient’s place of living:
- ○
In for patients living in a retirement home.
- ○
Out for patients living outside retirement homes.
- -
-
Medical needs after the diagnosis by the team:
- ○
Surgical (requiring surgical intervention)
- ○
Medical (requiring botulinum toxin injection)
- ○
Prescription (requiring rehabilitation or orthesis)
In addition, these interviews enabled us to identify the problems, their causes and their consequences. Five categories of problems are finally established:
Long lead times: time spend to wait for specialist consultation and treatment and during transport.
Patient discomfort: patient without treatment and discomfort during transport or treatment in a specialist hospital.
Lack of patient safety: the problem of transport safety, hospitalisation without landmark.
Patient & family’s fears: from the operating room, regarding the patient’s weight.
Lack of care: patient without treatment—no care—or too late because of lack of detection.
The causes of these problems were identified and further related to the given problems:
Lack of coordination: Difficulty in coordinating the patient care path from finding a specialist doctor to scheduling patient transportation.
Lack of knowledge: Lack of information about ADH and the existing solutions to treat it.
Current detection method: Lack of training and organisation to detect early ADH.
Current diagnosis method: Lack of training and organisation to diagnose ADH.
Current treatment method: Lack of training and organisation to treat ADH.
Medical care difficulty & complexity (in case of patient fragility): Overprotect the patient and refuse to disturb the patient regarding his/her age and comorbidities.
Operating room anxiety: fear of the operating room from the patient and all caregivers, including family.
The ultimate consequences are twofold:
Increase of morbidity and mortality: because of the lack of care, the lack of patient safety and the patient discomfort.
Increase in healthcare costs: because of the increase in dependence, treatment is more expensive if they are too late.
In our study, the usage situations are related to the patient care process steps. We then defined the usage situations as follows:
- -
Detection: First signs of ADH (for example flexum of knees, hands, elbow with little difficulties with hygiene, chair installation or walking).
- -
Diagnosis: Consultation step to provide prescriptions or medical procedures to the patient.
- -
Treatment: Surgery step to treat a patient requiring a surgical procedure or injection of botulinum toxin for people requiring it or prescription of physiotherapy or orthesis if requiring.
- -
Follow-up: The following step to provide the treatment follow up.
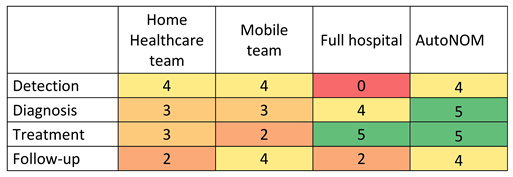
We identified three existing solutions that exist in the current healthcare system addressing the ADH: Full Hospital, Mobile Team and Home Healthcare Team. These existing solutions do not cover all the patient care process steps (
Table 2: Patient care process step carried out).
As explained, we used the RID compass method [
18] to compute a set of prioritized value buckets answering the question: “Where should I concentrate to develop innovations that merit to be developed (important quantities of pain) and where existing solutions are not much effective in average?”.
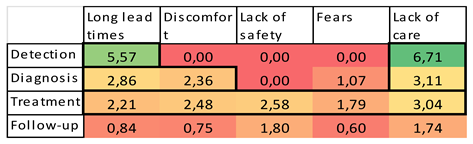
A first computation is done to get the so-called All-Users value bucket matrix (
Table 3)—computation formula is given and justified in [
18] -. This matrix displays prioritized (usage situations, problems) pairs which are quantitatively painful and for which the present ADH detection and treatment solutions are weak in average. After
Table 3, the value buckets most conducive to innovation are in the detection and diagnosis phases concerning the problems of long lead times and lack of care. These value buckets are considerably higher than other value buckets that have been identified in other patient care phases.
More in-depth analysis can be done with respect to a specific
user profile (see
Table 4 for the
high-out-surgical user value bucket matrix). This matrix reveals that significant value buckets are also identified in the treatment phase (Long Lead Time 2,2, Discomfort 2,48, Lack of safety 2,58, Fears 1,79 and Lack of care 3,04). The quantitative value has no meaning here, apart that their ratio is significant to a disproportion in an amount of non-addressed quantities of pain. If we examine the underlying plausible causes, we find that this phase is particularly difficult for “In” patients. Given that the ratio of “In” to “Out” is 20/80, this difficulty is less obvious when we consider the overall level of the care process.
3- Proposition of solutions
The focus of this study is to look for solutions to improve the care of patients living in retirement homes, as these patients have the least AutoNOMy. It is easier to identify and access them (by identifying and having agreements with the retirement homes). In this way, all the proposed solutions will be more accessible to patients living in retirement homes.
To build the AutoNOM solution according to the pains that have been identified, we took as our starting point the care process and, more specifically, the stages involved. The advantage of the RID method is that solutions that have been proposed not only proposed technological innovation but also healthcare services innovation [
21].
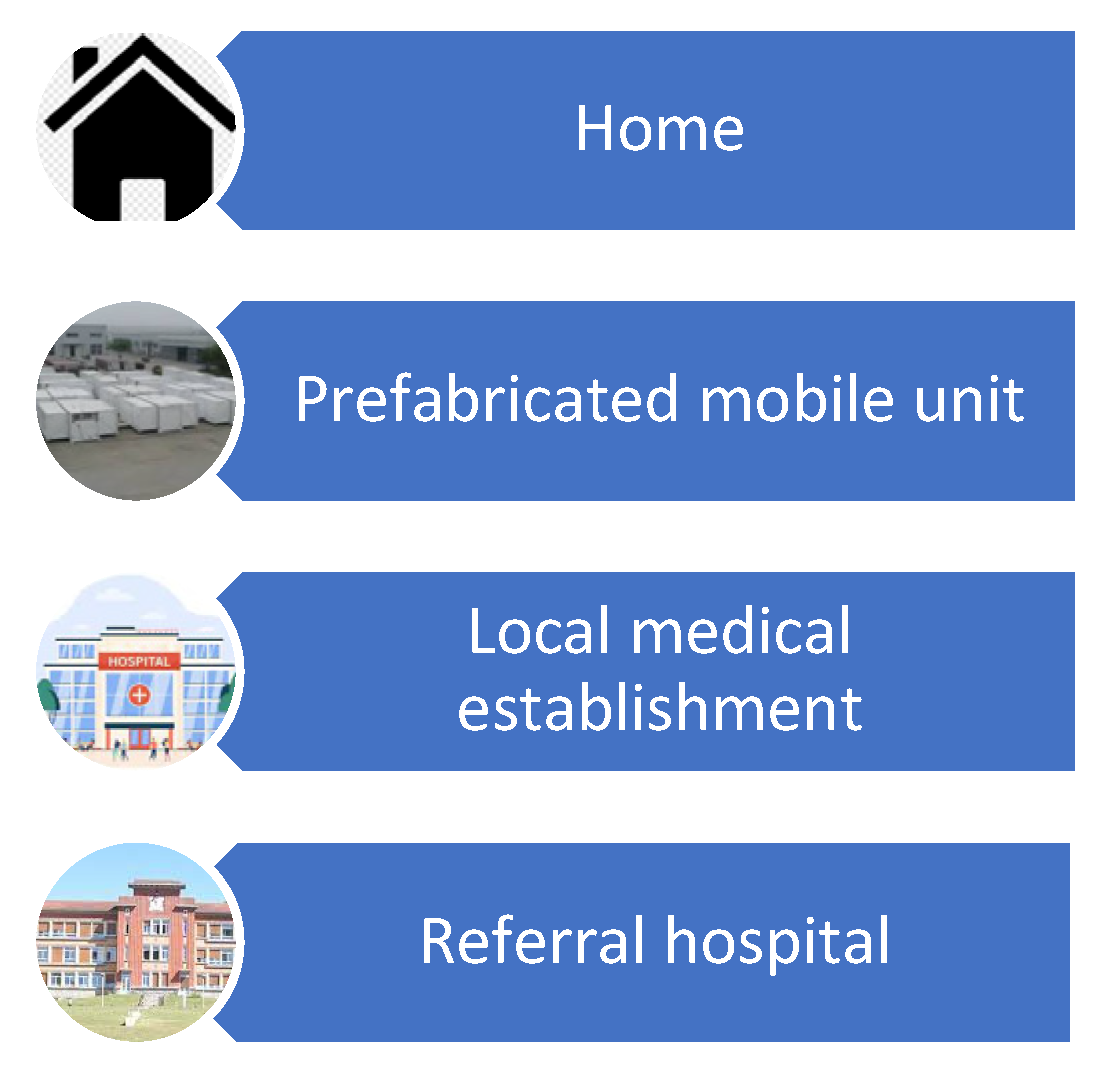
We identified four possible care locations for AutoNOM project (
Figure 3) and further 256 possible organizational solutions by crossing different locations possible for care (4 identified) and the 4 different stages of patients care: 4
4 = 256. Four of the 256 cases already exist: full hospital (two possibilities via detection in a local medical establishment or reference hospital), HAD and mobile unit. In discussion with experts of the question of ADH (team of health service involved in ADH care), two hundred forty-six options make no sense in terms of their use. For example, all the possibilities for the treatment phase are at home, while the other stages are carried out in the hospital or the prefabricated mobile unit. This leaves us with six possibilities, which we summarise in
Table 5: Potential solutions.
To evaluate the proposed solutions, several criteria have been discussed and defined: number of patients, overall costs, number of transportations, type of transportation, quality of healthcare, quality of work environment for the medical staff, number of retirement homes that can benefit from the proposed solution, logistics difficulty.
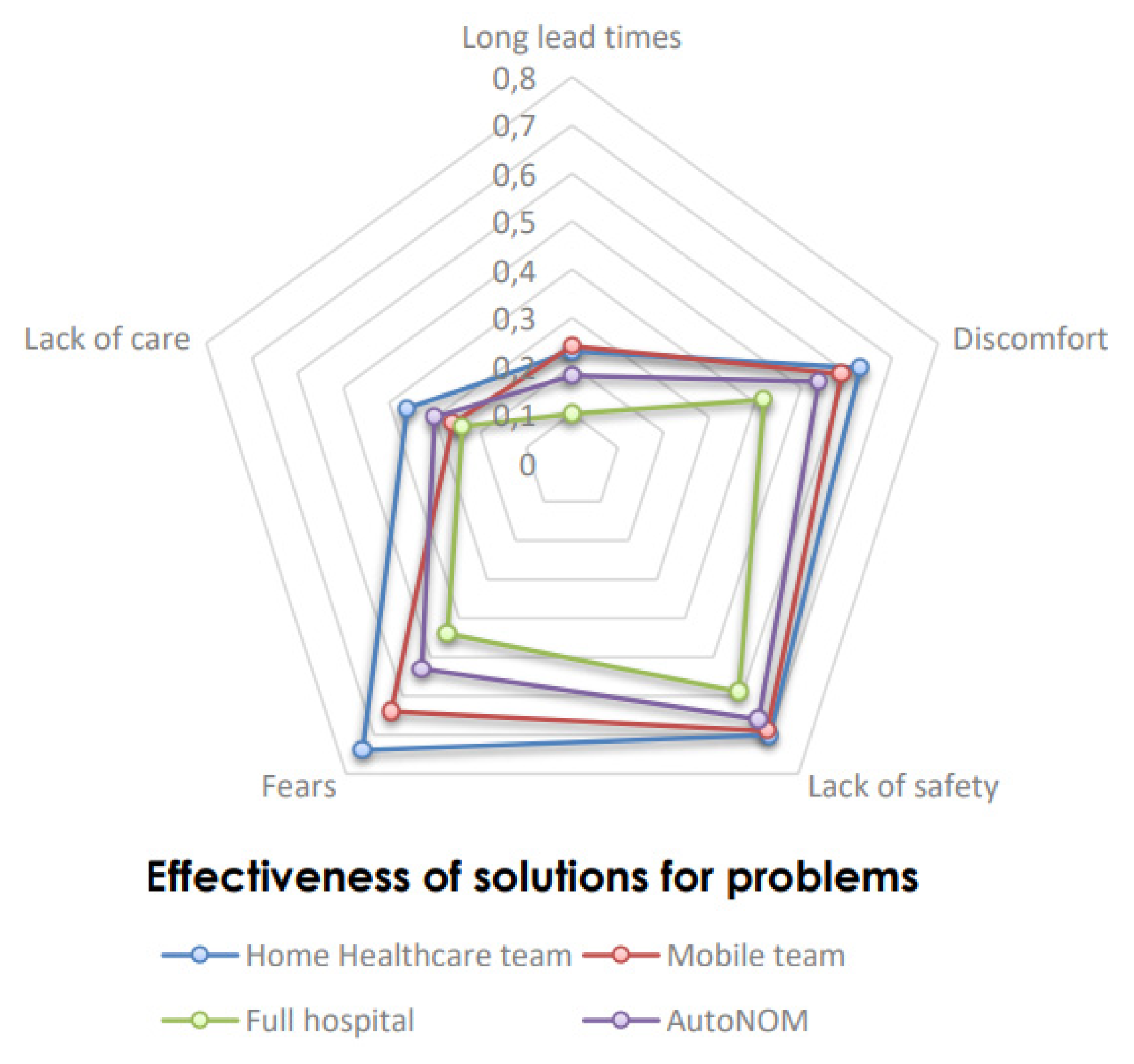
Out of previously identified solutions, a particular solution has been identified that we called the AutoNOM solution. This solution proposed to do the consultations and treatments within retirement homes, and follow-up phase on-site or by teleconsultation. The idea behind this solution is to address the long lead times and lack of care that have been identified and major value buckets in the detection and diagnosis phase. The objective is to offer a training module to staff to lower detection time and lack of care. This AutoNOM innovative solution has been qualitatively evaluated along with the three current existing solutions “Home healthcare team”, “Mobile team” and “Full Hospital” through the filling of three matrices, considering the adequacies of solutions toward problems (EsP matrix), usage situations (UsEs matrix) and user profiles (UpEs matrix). These matrices have been filled with numbers between 0 to 5 (this scale is a convention), function of the degree of completion of the asked question to the main author of the study and two other experts of the ADH question. The 2 first authors completed the matrix.
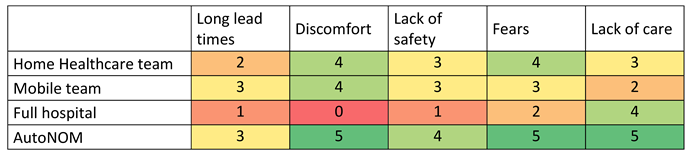
Matrix EsP (
Table 6) estimates how different existing solutions solve specific problems in responding to the following question: “To what extent does this solution eliminate or mitigate this problem?”. The hospital is not an easy solution for these patients who are difficult to move. Care by a mobile team and especially by Home Healthcare team is reassuring for the patients and the care team. The difficulty is especially for these last two modes of exercise the time for the care and thus the lack of care in addition to the safety which can be altered by displacement. The evaluation of the AutoNOM solution is designed in particular to reduce discomfort, fears, lack of safety and lack of care (which is clearly evaluated by experts giving value of 5 or 4 for each problem). The problems of discomfort, fears and lack of safety should be reduced because we avoid transporting patients and disturbing them, and the treatment is carried out on-site. Lack of care is addressed in particular by setting up training.
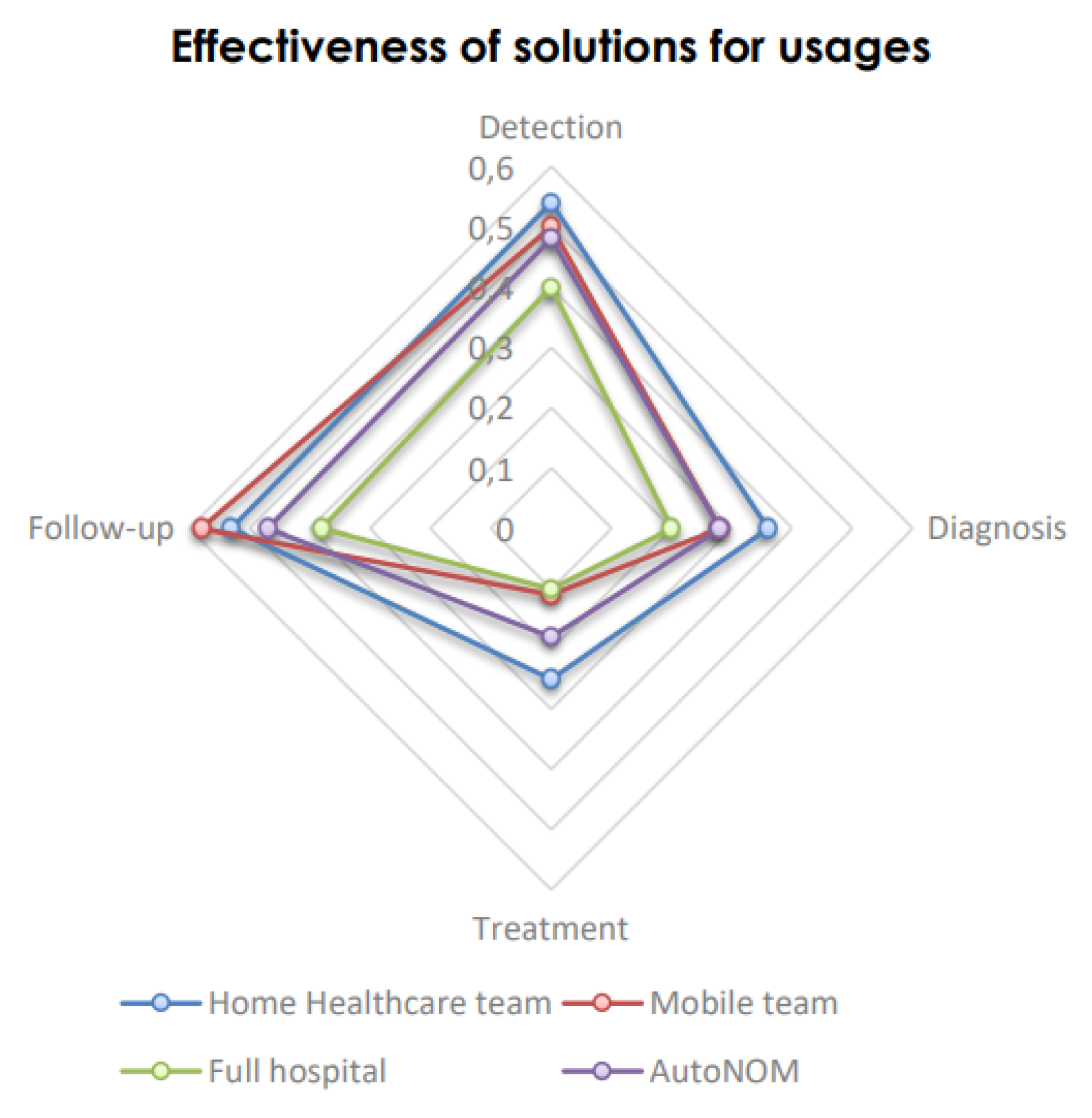
Matrix UsEs (
Table 7) estimates how different existing solutions are adapted to specific usage situations in responding to the following question: “To what extent does this solution facilitate this usage?”. Treatments and diagnoses are more easily done in the hospital. Follow-up and detection are more easily done by a mobile team. Home Healthcare team is a good means of detection (but often without a doctor, so no diagnosis could be done). AutoNOM solution has been developed to carry out the diagnostic and treatment stages at the patien
t’s bedside (value of 5 in these two usage situations for AutoNOM solution). In this way, it facilitates access to comprehensive care. The detection stage is enhanced by training sessions offered to healthcare teams travel (value of 4 for this usage situation with AutoNOM solution). The patient follow-up stage is also improved by teleconsultation, reducing the need to travel (value of 4 for this usage situation with AutoNOM solution).
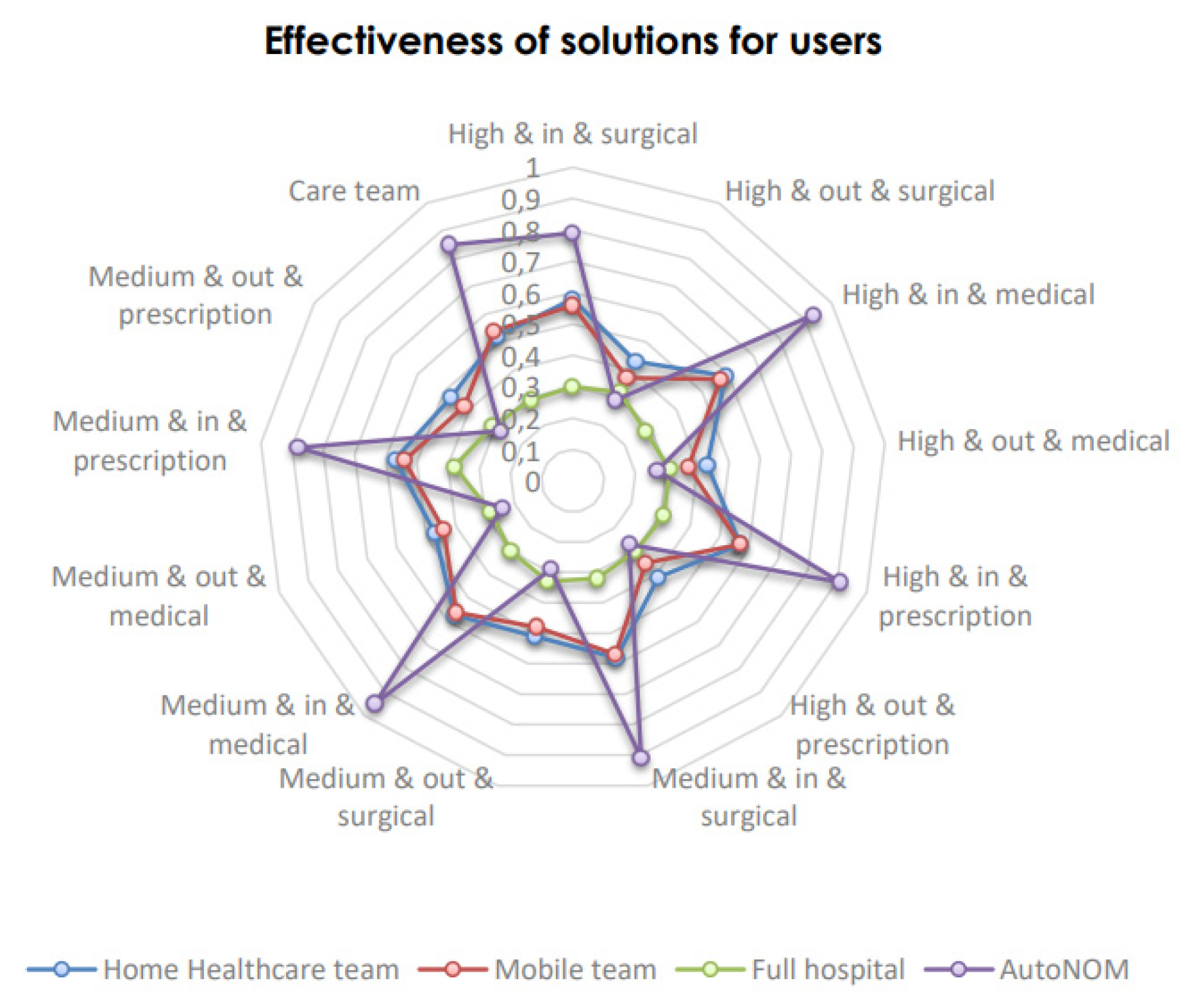
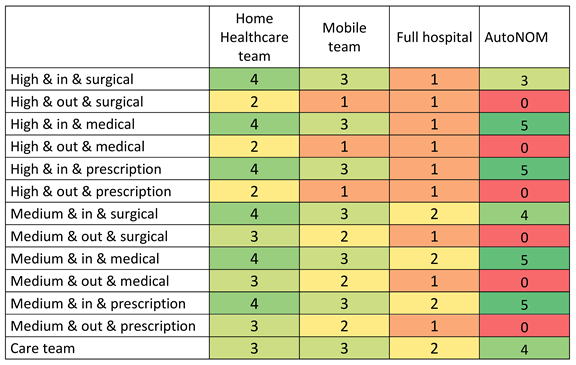
Matrix UpEs (
Table 8) estimates how different existing solutions are accessible, effectively used and adapted to specific user profiles in responding to the following question: “How effectively does this user access and use this solution?”. Out-type users
—outside of a retirement home
—have less access to care, especially to the hospital. This difference is less for the mobile team and especially Home Healthcare team, which has better coverage of the territory. The AutoNOM solution has been designed by experts to support patients living in nursing homes (values of 3 to 5 for these user profiles with AutoNOM solution). It targets patients requiring a medical procedure or recommendations for installation or rehabilitation. AutoNOM solution will also be used to treat patients requiring surgery, with the family’s agreement. Staff training will also enhance their knowledge and improve the quality of patient care.
4. Discussion
This RID deployment for the mobile unit for ADH treatment has underlined that the Radical Innovation Design (RID) methodology [
18] considers broader solutions scenario space. Some scenarios have been identified though they have yet to be initially considered (initially, only mobile unit development was considered, such as truck, and six solutions have been fully investigated and proposed). Identification of problems (pain points and expectations) have been critiqued in gaining an in-depth understanding of perceptions and acceptance of different solution scenarios. Moreover, discussion of possible solutions with French healthcare social security have been done, partly by the main author of these study, and based on the results of this study. One of the first possible enhancements that were discussed was related to botulinum toxin use and refund: since January 1st, 2021, in France, botulinum toxin can be refunded in home healthcare, which could be an interesting solution for several patients where the treatment with botulinum toxin has an interest. A list of expensive molecules eligible for a refund in home healthcare have been published. [
30]
In addition, discussions have started with the general directorate of health care in France (Direction Générale de l’Offre de Soins, DGOS) to evaluate a new program of management for these patients to minimise their transports, overall cost and manage more patients than today. In particular, with the results of this study, we were able to discuss with the French General Secretariat of Social Affair Ministry (Secrétariat général du ministère des affaires sociales) to find the most appropriate solution for these patients. An experimental solution has begun last year in 8 mobile unit called Auto-NOM, in France.
The interesting point is that RID methodology has brought more healthcare scenarios (for instance not only the truck solution in this case but also a prefabricated unit solution and others solutions described in the study before) and aims to evaluate a solution designed using pain points and defined regarding decision maker preferences over several criteria. The AutoNOM solution tries to respond to an ideal ADH detection and treatment activity and is the best solution, to date, to enhance the care process for patients living in retirement homes. Even though the study has yielded an interest in the French healthcare system, several questions persist:
- -
How can sedation be brought/stored in facilities other than hospitals to allow the same treatment as at the hospital but closer to the patient? Because all procedure could not be performed under local anaesthesia and sedation could be a step in at home care.
- -
How can patients living in their homes around the retirement home have access to this solution? To avoid medical deserts, it could be possible to proposed this care to all the patients living closed to the retirement home where the AutoNOM project is deployed.
- -
Can we consider allowing access to this care to people with disabilities and not only the elderly population (e.g., cerebral palsy in particular)? Elderly patient have some similar points to patients with important disabilities, even if it is not really ADH in their cases, they have similar deformity problems and could access to these solutions.
5. Conclusions
The aim of this research was to use a collective progress methodology (RID) to find innovative therapeutic process solutions, in order to advance therapeutic care in ADH problems in retirement homes in France which is a public health problem regarding the number of people reached.
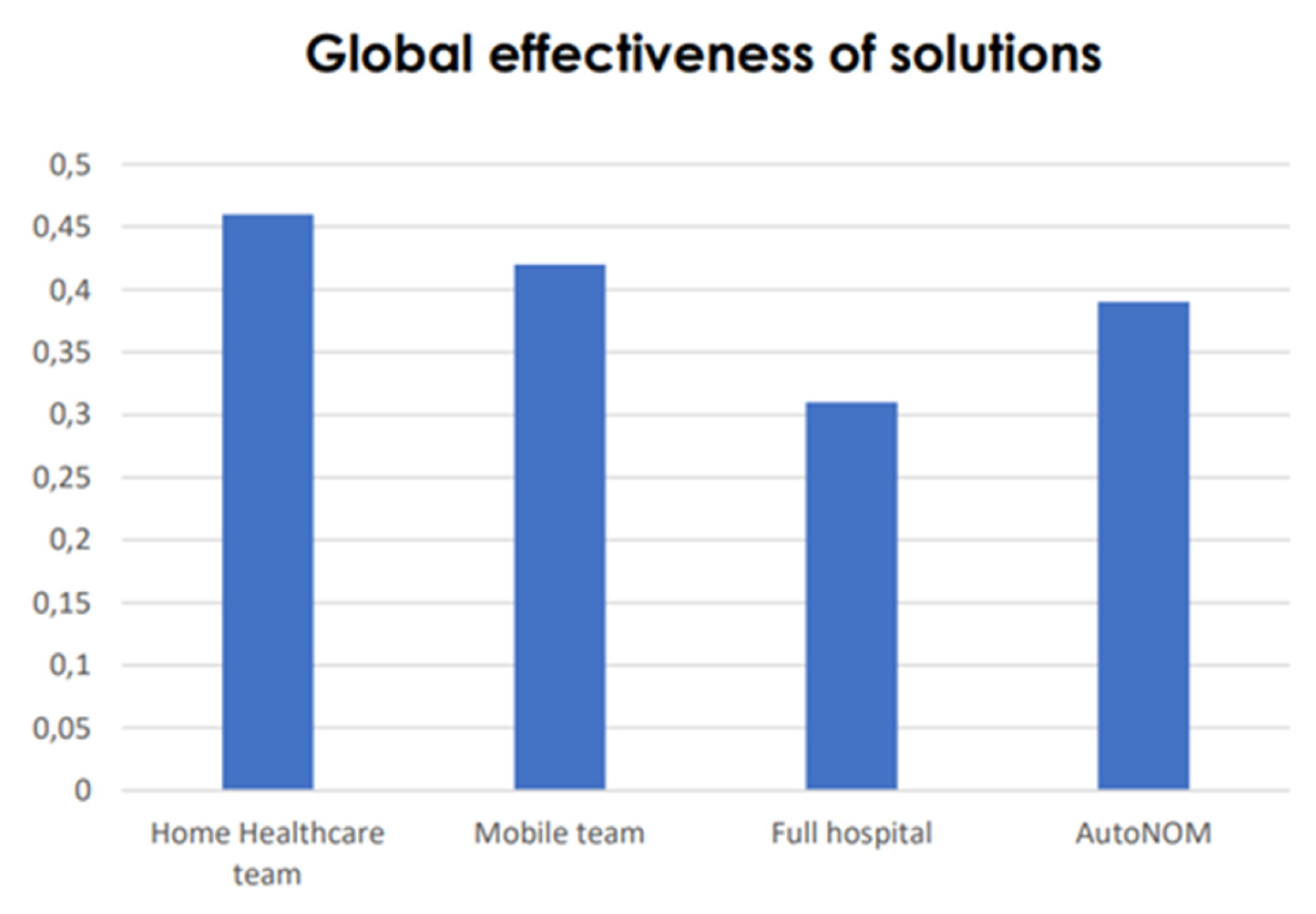
In this study, we propose to use the Radical Innovation Design methodology to support the innovation process related to ADH treatment. In particular, this study has been conducted to design and develop a mobile care unit where the minimal procedure that was developed can be used. The idea of mobile units is not new, and several other studies have been addressing diagnose, treatment or teaching. RID has been used to guide and structure the development process. One of the major advantages has been that this process gathers a refined understanding of the pain points encountered in ADH patients as well as for different stakeholders (medical staff, retirement home staff, and family). These explorations based upon interviewing and observations used as input for the RID methodology highlighted major value buckets such as long lead times and lack of patient care. The value buckets have been used as a basis for brainstorming. Six possible novel scenarios have been considered. AutoNOM solution has been selected and evaluated by RID methodology using effectiveness indicators. For instance, the effectiveness of the AutoNOM solution is the best for patients living in the retirement home. As discussed in the literature, RID has allowed us to identify healthcare service and product innovative scenarios.
Moreover, this study has been used to discuss possible implementation with Direction Générale de l’Offre de Soins (DGOS). In particular, botulinum toxin has been introduced as a possibility to be reimbursed in home healthcare situations. Discussions are currently being undergone with the French General Secretariat of Social Affair Ministry (Secrétariat général du ministère des affaires sociales), and implementation of the AutoNOM solution has been ongoing since September 2023 (authorization of the 22 December of 2022) in eight mobile unit in France.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, ADH-Elderly questionnaire
Author Contributions
L.G. wrote the main manuscript text, realized the study and reviewed the manuscript. N.A. and Y.B. participated to the study.E.S., M.J. and B.Y. designed the study, supervised the study and reviewed the manuscript.
Funding
This study was partially funded by a donation from Abbvie.
Informed Consent Statement
The need for ethics approval was unnecessary according to national regulations for this non-interventional procedure. In accordance with this law, we collected the non-opposition of people interviewed. (LOI n° 2012-300 du 5 mars 2012 relative aux recherches impliquant la personne humaine). An informed consent to participate from all participants had been collected.
Data Availability Statement
Data and materials (especially RID methodology) are available with corresponding author.
Acknowledgments
To Irénée, Reyes, Guilherme and Tarek, CentraleSupélec’s students. To Jean-René Camara and the students of Institut Supérieur des Matériaux du Mans who worked extensively on numerical models. To Clinalliance-Repotel’s group and especially Mr David Bouniol and Ms Nolwenn Mare.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. L.G. and Y.B. are consultants for IPSEN, MERZ and ABBVIE.
References
- Dehail P., Simon O., Godard A.L., Faucher N., Coulomb Y., Schnitzler A., Denormandie P. and Jeandel C. Acquired deforming hypertonia and contractures in elderly subjects: Definition and prevalence in geriatric institutions (ADH survey). Annals of physical and rehabilitation medicine 2014 57(1):11-23. [CrossRef]
- Available online: http://drees.solidarites-sante.gouv.fr/IMG/pdf/er1015.pdf (accessed on 22 11 2024).
- Barnes M.P. Spasticity: a rehabilitation challenge in the elderly. Gerontology 2001 47(6):295-9. [CrossRef]
- Schnitzler A., Genêt F., Diebold A., Mailhan L., Jourdan C. and Denormandie P. Lengthening of knee flexor muscles by percutaneous needle tenotomy: Description of the technique and preliminary results. PLoS ONE 2017 12(11): e0182062. [CrossRef]
- Freter S., Dunbar M., Koller K., MacKnight C. and Rockwood K. Risk of Pre-and Post-Operative Delirium and the Delirium Elderly at Risk (DEAR) Tool in Hip Fracture Patients. Can Geriatr J. 2015 23(18):212-6. [CrossRef]
- Delpech J. Considérations sur la déformité appellée pieds bots. In Chirurgie clinique de Montpellier ou observations et réflexions tirées des travaux de chirurgie clinique de cette école / 1. Jacques Delpech. Ed. Paris-Montpellier, Gabon. 1823 ; pp. 1777-1832.
- Schnitzler A., Diebold A., Parratte B., Tliba L., Genêt F., Denormandie P. An alternative treatment for contractures of the elderly institutionalized persons: Microinvasive percutaneous needle tenotomy of the finger flexors. Ann Phys Rehabil Med 2015 59(2):83-6. [CrossRef]
- Mayr N.P., Michel J., Bleiziffer S., Tassani P. and Martin K. Sedation or general anesthesia for transcatheter aortic valve implantation (TAVI). J Thorac Dis 2015 7(9):1518-26. [CrossRef]
- Sangameswaran R.-P., Verma G.-K., Raghavan N., Joseph J. and Sivaprakasam M. Cataract surgery in mobile eye surgical unit: Safe and viable alternative. Indian J Ophthalmol 2016 64(11):835-839. [CrossRef]
- Wei, D., Oxley T.-J., Nistal D.-A., Mascitelli J.-R., Wilson N., Stein L., Liang J., Turkheimer L.-M., Morey J.-R., Schwegel C., Awad A.-J., Shoirah H., Kellner C.-P., De Leacy R.-A., Mayer S.-A., Tuhrim S., Paramasivam S., Mocco J. and Fifi J.-T. Mobile Interventional Stroke Teams Lead to Faster Treatment Times for Thrombectomy in Large Vessel Occlusion. Stroke 2017 48(12):3295-3300. [CrossRef]
- Wolf, F., Rojas González D.-M., Steinseifer U., Obdenbusch M., Herfs W., Brecher C., Jockenhoevel S., Mela P. and Schmitz-Rode T. VascuTrainer: A Mobile and Disposable Bioreactor System for the Conditioning of Tissue-Engineered Vascular Grafts. Ann Biomed Eng 2018 46(4):616-626. [CrossRef]
- Renjen P.N. and Chaudhari D. Telemedicine and stroke: Stroke Emergency Mobile Unit—A new approach to stroke care. Neurol India 2016 64: S110-2. [CrossRef]
- Lesur D., Vincentelli A., Juthier F., Banfi C., and Coadou H. Mobile unit for cardio-respiratory support. Ann Fr Anesth Reanim 2011 30(Suppl 1):S27-9.
- Lacroix G., Pankert M., Nee L., Riberi A. and Kerbaul F. Interest of circulatory assistance mobile unit for cardiovascular surgical pathology support at distance of specialized centers: about a case of papillary muscle rupture. Ann Fr Anesth Reanim 2011 30(5):432-5. [CrossRef]
- Mitschler A., Roth B., Michel J.-M. and Guillaume J.-C. An innovative experience in clinical care management of chronic wounds: the wound and healing mobile unit of Centre Alsace. Ann Dermatol Venereol 2007 134(8-9):629-31.
- Dehail P., Gaudreault N., Zhou H., Cressot V., Martineau A., Kirouac-Laplante J. andTrudel G. Joint contractures and acquired deforming hypertonia in older people: Which determinants? Ann Phys Rehabil Med 2018 8(18):31482-9. [CrossRef]
- Varkey P., Horne A., Bennet K.-E. Innovation in Health Care: A Primer. Am J Med Qual 2008 1;23(5):382–8.
- Yannou B., and Cluzel F. Radical Innovation Design: A systematic and usage-driven innovation methodology to ensure usefulness for users and profitability for companies. Publisher : EDP Sciences, Paris, France, 2024 ; pp. 1-384.
- Lamé G., Yannou B., Cluzel F. Usage-driven problem design for radical innovation in healthcare. BMJ Innovations 2018 4(1):15–23. [CrossRef]
- Huynh-Dagher S., Lamé G., Duong T. A., and Jankovic M. Design research in healthcare: a systematic literature review of key design journals. Journal of Engineering Design 2022 33(8-9), 522-544. . [CrossRef]
- Yannou B., Cluzel F., Farel R. Capturing the relevant problems leading to pain and usage driven innovations: the DSM Value Bucket algorithm. Concurrent Engineering—Research And Applications (CERA) 2016 1-16.
- Duong T. A., Le Cardinal J. and Bocquet J.-C. Design of a healthcare service: Teledermatology. In 19th International Conference on Engineering Design, Seoul, South Korea 19 08 2013.
- Jean C., Duong T. A. , Stal Le Cardinal J., Jankovic M. and Bocquet J.-C. Sharing economic value between the stakeholders of a telehealth project: Methodological issues? European Research in Telemedicine 2016 5(2): 37-44. [CrossRef]
- Jean C., Jankovic M., Stal Le Cardinal J and Bocquet J.-C.. Predictive modeling of telehealth system deployment. Journal of Simulation 2015 9(2): 182-194. [CrossRef]
- Yannou B., Farel R., Cluzel F. The DSM value bucket tool. In 15th International Conference on Research into Design, Bangalore, India 07 01 2015.
- Salehy Y., Yannou B., Hoan H.-M. Cluzel F., Leroy Y., Fournaison L., and Delahaye A. Diagnosing the socio-technical refrigeration system with Radical Innovation Design methodology to target innovations. International Journal of Design Creativity and Innovation 2024 118-138. [CrossRef]
- Bekhradi A., Yannou B., Cluzel F., Vallette T. Categorizing users’ pains, usage situations and existing solutions in front end of innovation: The case of smart lighting project. In 21st International Conference on Engineering Design (ICED), Vancouver, Canada 21 08 2017.
- Lamé G., Leroy Y., Yannou B.. Ecodesign tools in the construction sector: Analyzing usage inadequacies with designers’ needs. Journal of Cleaner Production 2017 148:60–72. [CrossRef]
- Salehy Y., Yannou B., Leroy Y., Cluzel F., Fournaison L., Hoang H.-M., Lecomte R., Delahaye A. Diagnosis of development opportunities for refrigeration socio-technical system using the radical innovation design methodology. Proceedings of the Design Society 2021 1:1263–1272. [CrossRef]
- Available online: https://www.atih.sante.fr/specialites-pharmaceutiques-en-had-2021 (accessed on 22 11 2024).
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).