
Submitted:
25 November 2024
Posted:
26 November 2024
You are already at the latest version
Abstract
Patient-provider communication is a crucial aspect of the work conducted in healthcare settings. Studies have shown that spoken and written language used by providers during healthcare conversations can positively or negatively impact health outcomes. A scoping review was conducted to map peer-reviewed research articles focused on the use of spoken/written language in healthcare settings, identify and clarify key related concepts, and find best practices for decreasing the use of harmful and biased language among healthcare professionals. Peer-reviewed articles published in English from 2003 to 2023 were identified through ProQuest Sociological Abstracts, PubMed, and ScienceDirect databases. Covidence was used to perform screening and data extraction. The search initially identified 128 records for title and abstract screening, with 33 articles deemed relevant for a full-text screen. A total of nine articles met the review’s inclusion criteria. Findings indicated a need for increasing and expanding inclusive language training for healthcare providers to enhance patient care quality and health equity and to ensure the next generation of healthcare providers adopt these practices. Training healthcare providers in inclusive language is crucial to improving patient care and addressing systemic biases in the healthcare system. Integrating this training into educational curriculums and continuing education opportunities can help reduce biases, empower patients, and support better health outcomes.
Keywords:
Bias
; Inclusive Language
; Spoken and Written Language
; Stigma
; Healthcare Workers
; Public Health
; Patient-Centered Care
1. Introduction
There is a long history of remarks about the power of the tongue, of the language we use. In the Book of Proverbs, it is stated “The tongue has the power of life and death” [1]. This statement resonates strongly when examining the impact of communication between healthcare professionals and people receiving their care. The language used in healthcare-related communications is crucial, as written and spoken language used in these interactions can either empower or harm individuals and communities. Stigmatizing words like “addict” or “substance abuser” contribute to bias and negative outcomes, as shown in the field of substance use disorder [2]. Words that are written or spoken hold immense power and are a prime vehicle for the expression of bias, stigma and discrimination in society, which in turn result in social determinants of health factors that disproportionately affect marginalized groups. Furthermore, “there is a causal, vicious cycle between disadvantages due to social determinants of health and poor health outcomes” [3].
Existing systematic reviews about language in healthcare settings focus on it as part of the multifaceted concept of communication, linguistic barriers such as dominant language proficiency (e.g., English proficiency) or use of dialects, global migration and linguistic diversity, and/or language usage in the context of cultural competence [4,5,6,7,8]. This review was conducted to address the scarcity of reviews focusing on research on spoken and written language practices in healthcare settings and interventions for improving these practices.
Background
Person-centered language (PCL), endorsed by institutions such as the American Medical Association Manual of Style and the American Psychological Association, is crucial to reducing stigma and promoting inclusive care [9] and is integral to effective patient-provider communication. In contrast, biased language can perpetuate stigma and limit healthcare access, particularly for marginalized groups [10]. Furthermore, promoting inclusive language aligns with efforts to address structural inequalities and improve health equity [3]. However, inclusive language adoption in healthcare settings has been hindered by a lack of inclusivity guidelines and the availability of practical steps for healthcare providers [3].
Providing patient or person-centered care is widely recognized as a fundamental principle for ensuring quality care and patient satisfaction. In the context of the person-centered approach, inclusive language refers to the use of communication that puts the patient in the driver’s seat and seeks to be culturally sensitive, gender-neutral, and respectful [11]. The purpose of inclusive language is to acknowledge and respect the diverse identities, backgrounds, and experiences of all persons receiving care [11]. Despite the growing need and emphasis on person-centered approaches, the use of non-inclusive and/or biased language in healthcare interactions poses a significant barrier to achieving true person-centered care [10]. Further, although inclusive oriented “person-first language is taught in most health professions programs…it is often not practiced by health care practitioners” [12]. As a response to inclusive language usage issues, there has been a concerted effort to move away from including racial and ethnic identifiers in oral clinical presentations, written clinical notes and summaries, as well as published case reports, especially in their opening narrative. This is due to the way these terms have been used to associate race/ethnicity with negative behaviors or socioeconomic status [13].
A background literature review on language usage in healthcare settings revealed three key characteristics among publications: unstandardized use of related conceptual framework terminology; a limited number of health issues for which the use of inclusive language is addressed; and a need to integrate inclusive language practice in healthcare educational settings.
The need for clarity and standardization of terminology used to conceptualize language usage inquiry can be exemplified by the uses of the terms Person-Centered Care and Patient-Centered Care. Some studies differentiate the terms, while others choose to use them interchangeably. A patient-centered perspective requires considering what is known about the patient and having a clear understanding of their history before forming a diagnosis. This perspective is based on defining a patient as “someone who suffers” [14]. In contrast, the concept of person-centered care was developed to put less of a focus on the sick role “and more on the unique individual with an illness” [14]. This approach considers the individual seeking treatment or care as having a myriad of complex attributes, intersectionality, and preferences while a current condition or potential condition (in the case of preventive care) is only a singular aspect embedded within this greater context. However, based on the literature, it is unclear whether the two terms should be used separately or interchangeably.
People-first language is another concept that lacks consensus when used in the context of inclusive language in healthcare settings. The People First movement emerged in 1974 as the first major self-advocacy disability rights movement [12] in the United States. Subsequently, during the early 1980s, the National Association of People with AIDS (NAPWA) was established [15] as a response to stigmatizing phrases like ‘AIDS victims’ and ‘AIDS patients’ and launching the HIV/AIDS movement [16]. The movement's principles, outlined in the 1983 Denver Principles [15,17], initiated the promotion of what we now recognize as person-first language [16]. The formal introduction of person-first language was done by the American Psychological Association in 1992 to be “a means to separate the individual from their diagnosis or impairments” [12]. Person-first language has faced criticism within the disability community, with some arguing that “if language is needed to separate them (the disability community) from a trait, then that suggests the trait is negative” [15], thus preferring the identity-first language which “views the individual’s disability as an integral part of the individual’s identity” [12].
Current studies also demonstrate that only a handful of healthcare medical areas have focused on inclusive language usage. Literature searches on language usage in healthcare settings resulted in most relevant articles related to dementia or weight loss. The focus of inclusive language research on dementia could be related to the fact that the theory of person-centered care was formed in the context of dementia care and the need to “see the person” [14]. According to Kim and Park, the aim of person-centered care, in the context of dementia, is to “maintain well-being and quality of life” [18]. In their article, they conducted a systematic literature review and meta-analysis and found intensive person-centered care significantly improved the quality of life in patients with dementia [18]. A similar systematic literature review and meta-analysis conducted by Lee et al., aimed to “review person-centered interventions used in the context of dementia care and analyze their effectiveness” [19]. A third study identified 25 articles focusing on the delivery of person-centered dementia care. In this study, they concluded that delivering person-centered dementia care fostered a “positive environment for meaningful interactions between caregivers and care recipients” [20].
Studies focusing on the use of inclusive language and communication practices when discussing obesity have for example aimed to evaluate the literature on the perspectives of patients and healthcare professionals on preferred/least offensive terms (‘weight’ and ‘Body Mass Index (BMI)’) versus stigmatizing and blameful ones (‘obese’, ‘large sized’, and ‘fatness’) [21]. Other obesity studies have looked at adherence to person-centered language terminology guidelines in articles published in weight-focused journals [8] and bariatric surgery patients’ preferences for weight and eating-related terminology [22].
Other health fields or topics in which language-related research has been done include amputation research (current adherence to PCL in scientific journals related to individuals with limb or digit amputations) [23] and patients with medically unexplained symptoms (quantification of language usage differences amongst practitioners and relationship to inducing patient anxiety) [24].
Regarding the third characteristic among publications documenting language usage in healthcare, our background literature review revealed a scarcity of interventions addressing language in healthcare, with most publications focusing on correlations or differences in patient outcomes, yet few discussing solutions. Examples of articles that mention interventions and calls to action are Auckburally et al.’s call for more support and training for healthcare providers in communicating weight status [21] and Truong et al’s offered solutions to address historical biases in healthcare language [25]. The issue of inclusive language in healthcare is recognized but remains complex, necessitating further research and interventions to create inclusive environments. Past reviews note a correlation between language use and patient outcomes, underscoring the importance of addressing biased language practices.
This scoping review aimed to identify and synthesize best practices and raise awareness about the importance of using inclusive spoken and written language in healthcare practice settings to support health equity. The objectives of this review were to (i) map and synthesize efforts to use appropriate and sensitive spoken or written language/terminology in healthcare settings, (ii) identify and clarify key related concepts, and (iii) identify and summarize best practices for strategies or interventions for decreasing harmful and biased spoken or written language/terminology usage among healthcare professionals in their interactions with patients. This review also identified gaps in the literature and future areas of research regarding best practices for decreasing biased language among health professionals.
2. Methods
We chose to use the scoping review method [26] as the results of a preliminary literature review pointed to inclusive language practices in healthcare settings as an emerging field of research. The scoping review method is designed to assess the breadth of available research literature and identify the “nature and extent of research evidence” [27], an appropriate approach for broader research questions seeking to qualitatively describe synthesized evidence by combining the strengths of a critical review with a thorough search process [28]. This review included studies employing qualitative and quantitative methods as well as randomized controlled trial, cross-sectional, and randomized vignette study designs. Given the differences in design of the included studies and that this type of review does not require a quality appraisal, our review did not conduct a quality assessment of the identified articles.
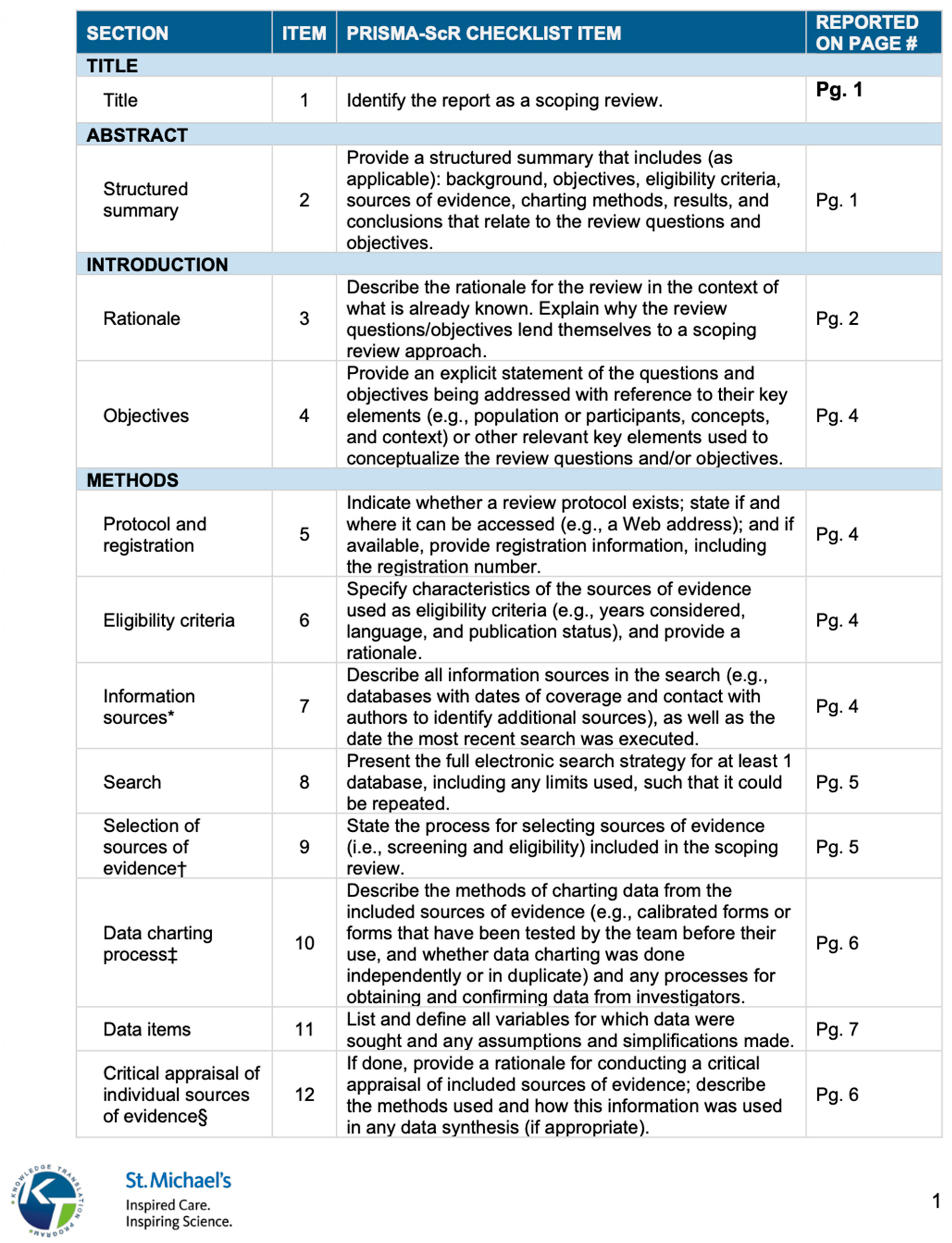
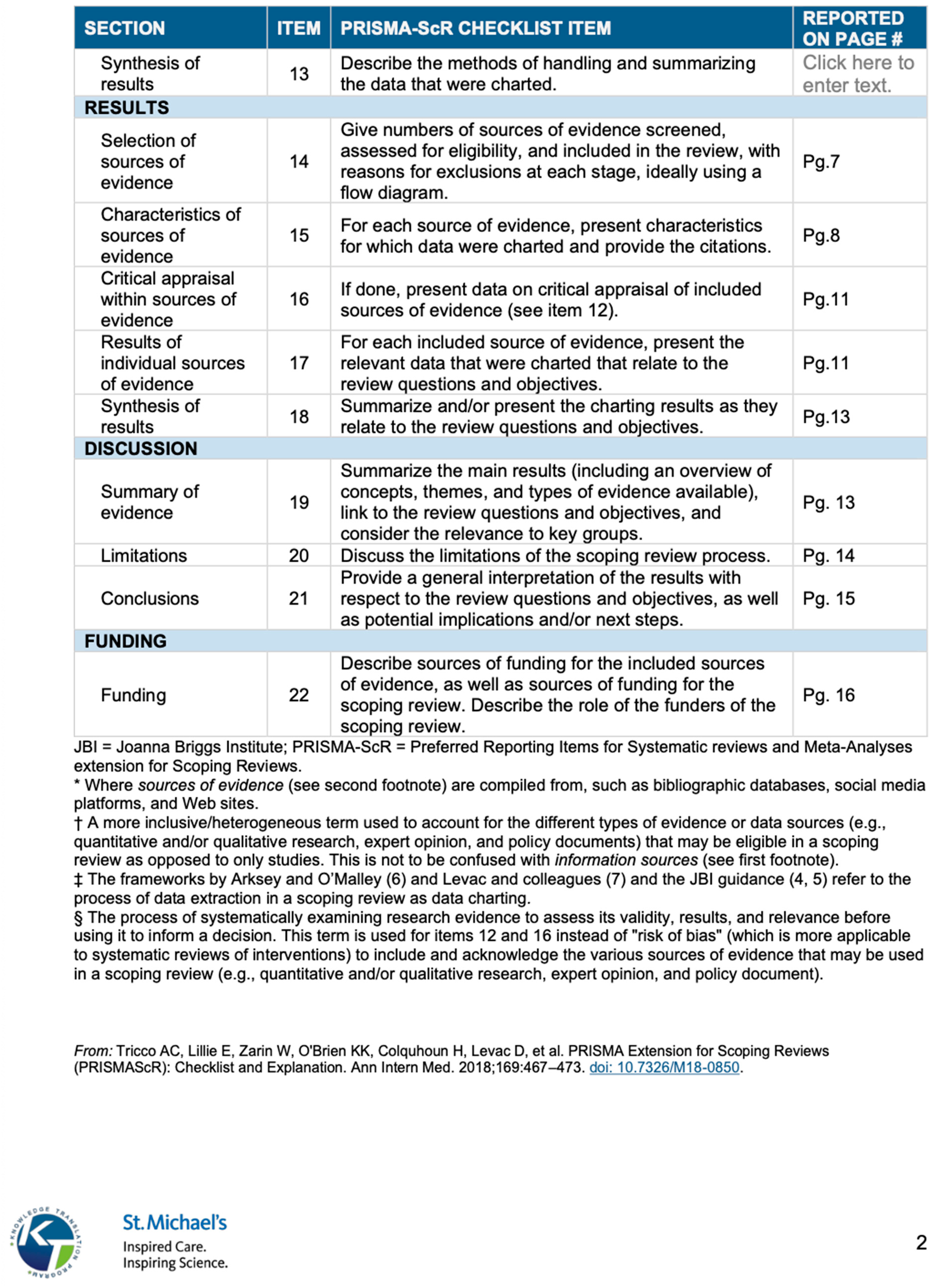
A Priori Review Protocol: Our review procedures initiated by determining the goal, aims, objectives, method, and reporting of findings, as well as inclusion/exclusion criteria for sources of evidence and to identify and extract relevant data [26]. To avoid duplication, before initiating the review we did an initial search for existing reviews with similar aims and objectives as ours. We then used Cochrane’s Population, Intervention, Comparison, Outcomes, Context (PICOC) strategy and developed a comprehensive list of key terms related to each category of the PICOC. The Cochrane Review Method [29] was employed to guide the inclusion and exclusion criteria for this review. We adhered to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Statement standards, identifying studies against the eligibility criteria while enhancing transparency and accuracy [30]. We also used the PRISMA extension for Scoping Reviews (PRIMA ScR) checklist (see Appendix A).
Peer-reviewed articles were identified from three major databases: ProQuest Sociological Abstracts, PubMed, and ScienceDirect. The procedure for choosing these three databases consisted of systematically testing the already defined sets of key terms in several social and biomedical sciences databases (CINAHL, Web of Science, Anthrosource, Embase, and Scopus) to identify the ones yielding the highest number of relevant results.
2.1. Inclusion and Exclusion Criteria
The review adapted Cochrane’s Population, Intervention, Comparison, Outcomes, and Context (PICOC) strategy for “defining review criteria, formulating questions and search strategies, and for characterizing included studies” [29], determining all key criteria before identifying and extracting data [31]. The population of interest (P) was identified as Health Sciences (medicine, nursing, allied health) Professionals (i.e., healthcare providers), seeking to identify healthcare professionals’ perceptions and perceived effects of using inclusive and/or non-inclusive written or verbal language in healthcare settings. Studies not involving professionals or professionals in training from healthcare fields were excluded. Interventions (I) included in the review mentioned programming or educational approaches to reduce biased language usage. Both qualitative and quantitative studies were included. Studies were excluded if they lacked mention of spoken or written language usage. The comparison (C) criterion does not apply to this study as a comparative analysis was not the purpose of this study. Study outcomes (O) were included if there was documentation and measurement of language bias (changes in communication patterns, attitude shift, change in patient outcomes), including interventional studies employing qualitative or quantitative assessments. Studies not documenting language bias and/or measuring/intervening regarding a change in behavior or the use of biased language among health professionals were excluded. Lastly, studies were included if their context (C) was noted as conducted in healthcare-related settings, such as hospitals/clinics, health education environments/programs, and/or universities. Original research studies of any design type published in peer-reviewed literature were eligible. Additionally, studies must have been conducted in English to minimize translation errors. Papers published before 2003 were not included. Grey literature was excluded.
2.2. Literature Search Strategy
A list of key terms related to each section of the PICOC strategy was used to identify relevant literature. The search included terms within the titles and/or abstracts. The following keywords were used in our systematic search: bias language, healthcare, stigmatizing language, and stigma. See Appendix B for a full list of the keywords used. Searches were filtered to only include research articles from 2003 to 2023 and were sorted in order of relevance. The first 80 returned titles and abstracts in each of the three databases were screened. Relevant articles matching the inclusion criteria were then exported to a citation manager program (EndNote) and from there exported again to a web-based literature review platform (Covidence) to streamline the process for abstract and full-text review.
2.3. Screening, Extraction, and Review of Identified Literature
2.3.1. Data Screening
The screening process was done using Covidence, a literature review platform and tool for academic research [32]. Key platform features include importation of literature, initial and full-text screening, data extraction, risk of bias assessment, and customization and reporting. To begin the Covidence review process, the platform requires users to input information about their review, giving the option to input specified eligibility (inclusion/exclusion) criteria, following the Cochrane method of review. Covidence’s settings were selected for two reviewers required for screening, two reviewers required for full-text review, and one reviewer required for data extraction. The platform also allows reviewers to set their preferred data extraction tool. For this review, “Extraction 2” was used because it supports single reviewer extractions. Due to Covidence using the Cochrane method, it also formats its eligibility criteria section under the Cochrane acronym PICOC. Covidence’s “study tags” function was used to help organize and categorize literature or highlight specific aspects of an article.
After choosing Covidence settings, the selected literature was imported. Covidence kept track of the number of sources used at each stage of the review process and automatically removed any duplicated items. An initial title and abstract screening were conducted through Covidence by two independent reviewers (first author, B.P., and a review collaborator). The two reviewers marked articles as “Yes, Maybe, or No” for inclusion and added explanatory notes and tags where relevant. All studies marked by Covidence as having “conflicts” or marked as “maybe” fitting the eligibility criteria were then reevaluated and decided on by consensus between the two reviewers. The next step consisted of a full-text review. This stage was also conducted independently by the same two reviewers. Reviewers again left notes and study tags on each of the remaining articles, as well as specific reasons for exclusion. Any conflicting reviews by researchers were resolved by consensus, as in the previous review stage.
2.3.2. Data Extraction
Data extraction from the selected studies was carried out systematically using the Covidence web-based extraction tool. Author B.P. independently conducted the data extraction process using Covidence's Extraction 2 tool, capturing various study characteristics such as authors’ names, country of study, study design, sample size, participant demographics, intervention details, and outcome measures.
2.3.3. Data Synthesis and Analysis
Using Covidence’s data extraction template, data were collated and reduced by sorting them into “General Information”, “Study Characteristics”, “Participants”, and “Outcomes” categories.
The General Information category consisted of a study ID, title, lead author name, country where the study was conducted, type of publication, funding source(s), author conflicts of interest, and additional notes. The Study Characteristics category consisted of study aim(s), study design, start and end date of the study, method of recruitment, theoretical frameworks used, training or intervention implemented, and inclusion of person-centered language in the text. The general information and study characteristics sections were later consolidated to create key characteristics found in the included studies (see Table 1, Results section).
The Participants category (see Table 2, Results section) consisted of the study’s population demographic characteristics (including age, sex, race/ethnicity), health conditions, study inclusion and exclusion criteria, total number of participants, and general characteristics of health professionals and/or patients. The Outcomes category (see Table 3, Results section) included method(s), outcomes measured, primary and secondary outcomes reported, key conclusions, and references to relevant studies. Any information not found in the studies was listed in the table as not applicable (“N/A”).
Studies were analyzed by qualitatively describing and critically assessing the synthesized data and inductively identifying general thematic categories from the nine included articles.
2.4. Ethical Considerations
Reporting of this systematic review was guided by the standards of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Statement [33]. PRISMA guidelines advise best practices for conducting and reporting systematic reviews. Using the PRISMA standard for systematic reviews ensures transparency, completeness, and accuracy in reporting, thereby promoting ethical conduct in research.
3. Results
A total of 128 articles were initially screened, later excluding 95 of these due to title or abstract not meeting the inclusion criteria and leaving 33 articles for the next stage of the review process. Of these, 24 studies did not meet the inclusion criteria for various reasons as seen in Figure 1. Ultimately, nine articles met the full eligibility criteria for inclusion in the review.
All of the nine included studies addressed the effects of language usage in healthcare settings. Seven studies focused on the impact of language used with patient populations and two on physicians and medical trainees’ perception of their language usage and its impact on patients. Two studies specifically aimed to address how bias plays a role amongst those in recovery. While other articles did not specifically mention bias, they did aim to assess the attitude of health professionals and how that may affect a person’s care and recovery. Four of the reviewed studies centered on specific health conditions such as diabetes, hypertension, pediatric asthma, chronic pain, and substance use disorder (SUD), while the remaining five did not specify a particular health condition. None of the studies included a clear definition of person- or patient-centered care.
Three studies employed a cross-sectional design, three used qualitative research methods such as interviews, one utilized a semi-qualitative approach, one employed a randomized control trial design, and one conducted a randomized vignette. Recruitment methods for human participants included email outreach, snowball sampling, and random selection. Three studies used medical records and notes to determine how healthcare providers document patient health conditions using positive or negative descriptors. Four of the reviewed studies centered on specific health conditions such as diabetes, hypertension, pediatric asthma, chronic pain, and substance use disorder (SUD), while the remaining five did not specify a particular health condition.
3.1. Recruitment and Data Collection of Included Studies
Participant recruitment methods varied among the nine included studies. Three studies relied on email as their primary recruitment tool, while two studies accessed data from a data mart or national registry to identify eligible patients. Additionally, two studies employed purposive sampling, selecting participants based on specific characteristics representing their target population.
3.2. Study Participant Characteristics of Included Studies
Among the nine articles meeting the inclusion criteria, seven were based on research conducted in the United States, one in Europe, and one in Canada. Six studies aimed to have sample sizes and characteristics representative of the population of the country of study. Five studies mentioned having participants identifying as white/Caucasian, followed by Black/African American, and then Hispanic. Three studies also mentioned most of their participants identifying as female. Five of the nine articles included healthcare workers and patients as participants in their study, while three solely focused on healthcare workers. Participants across studies also varied in age, ranging from 25 years old to 47 years old.
3.3. Inclusion and Exclusion Criteria of Included Studies
Inclusion criteria listed in the nine articles consisted of patients, health professionals, or a mixture of both. Three studies included health professionals (including medical residents). Six of the nine studies involved patients or the medical records of patients. All nine of the articles had unique exclusion criteria such as specific dates, not speaking English, or not working in a community healthcare setting. Other exclusion criteria included age specification, health condition qualifications, or a specific setting (for example, a community healthcare setting) that led to disqualification from their study.

Table 2.
Participant Characteristics and Inclusion/Exclusion Criteria.
| Table 2. Participant Characteristics and Inclusion/Exclusion Criteria of Included Studies | ||||
|---|---|---|---|---|
| Lead Author (Year) | Method of Recruitment of Participants | Population Characteristics | Inclusion criteria | Exclusion criteria |
| Zota et al. (2023) | About 64% of the sample was female. Most participants were employed in Greece (21.2%). The majority were physicians (45%), followed by nurses, other allied health professionals (i.e., psychologists, paramedics, health administration staff, nursing assistants, social workers, dentists/dental hygienists, dietitians/nutritionists, health promotion specialists, public health specialists) and students from health-related sectors. | Physicians, nurses, other allied health professionals (i.e., psychologists, paramedics, health administration staff, nursing assistants, social workers, dentists/dental hygienists, dietitians/nutritionists, health | Participants who did not specify health specialty/training or age | |
| Sun et. al (2022) | COVID-19 Data Mart | Almost one-third (29.7 percent) of the patients were White, 60.6 percent were Black, 6.2 percent were Hispanic or Latino, and 3.5 percent were categorized as other. The mean age was 47.4 years (SD23.0; data not shown) | All patients treated in an ED or inpatient setting between April 30, 2020 and October 1, 2020. | Patients with International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10), codes for dementia (n = 647), |
| Raney et al. (2021) | Not Specified | The target population is broad, including any provider, trainee, or staff member who works with patients in a clinical environment. | All health professionals caring for patients and documenting in the electronic medical record, including novice learners | Health professionals not documenting in electronic medical records |
| Park et al. (2021) | Random selection | Most patients were identified in the medical record as female (n = 350 [69%]). Most patients were identified as Black/African American (n = 406 [80%]), and 76 (15%) were identified as White | Patient medical records that had been written by physicians (attendings and residents) in 2017 at an ambulatory internal medicine setting at an urban academic medical center | Patient medical records not written in 2017 |
| Himmelstein et al. (2022) | Free-text admission notes of all patients admitted to a large academic medical center in 2018 | the 29,783 patients had a mean (SD) of 46.9 (27.7) years and 17 334 (58.2) were female, 840 (2.8%) were Hispanic patients, 1033 (3.5%) non-Hispanic Asian patients, 2498 (8.4%) were non-Hispanic Black patients, 18 956 (63.6%) were non-Hispanic White patients, and 1394 (4.7%) were another race (including American Indian or Alaskan Native and Hawaiian or Pacific Islander), and 2939 (9.9%) preferred a language other than English | All patients admitted to a large academic medical center in 2018 | Patients admitted to a non-academic medical center or patients not admitted in the year 2018 |
| DeMaria et al. (2023) | Email, Purposive Sampling, Snowball Sampling | Average Age- 25.8 ± 5.3; Race: White/Caucasian- 12 (54.5%); Black/African American - 7 (31.8%) Education: Some College or Undergraduate Degree - 13 (59.1%); Graduate Degree- 5 (22.7%) Employment: Student- 10 (45.5%); Full-Time- 11 (50.0%) |
- Women were eligible to participate in the study if they were 18–45 years of age and had ever sought reproductive healthcare at a community health center or program in Indiana - Non-physician healthcare professionals (i.e., NP, RN, CNM, doula, pharmacist, chiropractor) were eligibale if they were Iliving in Indiana who worked in a community healthcare setting |
Not working in a community healthcare setting |
| Deb Finn et al. (2021) | Purposive Sampling | Of the participants that completed the rating activity (n= 72), 41 participants identified as racialized health care users, 23 participants identified as non-racialized health care users, and 11 participants identified as either a ra- cialized or non-racialized health care provider. Of the 41 racialized health care users, 25 participants identified as female and 22 identified as Canadian-born | Recruited health care users were participants who had had a negative experience in Toronto or the GTA health care system within the past 5 years, age 16 years or older, and were able to write in English Recruited health care providers were front line providers (e.g. nurse, doctor, social worker, and pharmacist) who had at least 1 year of practice experience working in Toronto or the GTA |
Participant eligibility was group specific |
| Ashford et al. (2019) | Research Match- a national health volunteer registry. An email was sent to participants found in the registry | Participants had a mean age of 46.29 years (SD = 15.19), with the majority identifying as female (n = 225 / 75.3%), white (n = 271 / 90.6%), and either married or in a domestic partnership (n = 155 / 51.8%). Many participants had either a post-graduate degree (n = 135 / 45.2%) or a 4-year degree (n = 103 / 34.4%), were employed (n = 210 / 70.2%), and had a last year income over $50,000 (n = 200 / 66.9%). Less than a third of participants were in recovery (n = 87 / 29.1%) | Volunteers that elected to receive more information about the study | Random volunteers who did not respond |
| Goddu et al. (2018) | Of the 413 study participants (54% response rate), 42.8% were female, 43.5% were residents, and 14% were Hispanic/Latino. Most respondents were white (54.7%), 26.9% were Asian, and 10.4% identified as black or African American. | Residents in the medical center’s two internal medicine (IM) programs and one emergency medicine (EM) program | Non-residents | |
3.4. Measures and Outcomes of Studies
The nine eligible articles encompassed a variety of measured outcomes (refer to Table 3 for details). Studies examining physician or healthcare worker notes, such as those by Park et al. and Himmelstein et al. [34,35], identified negative descriptors in medical records such as "questioning credibility," "disapproval," and "difficult patient." Additionally, one study noted that "black patients had 2.54 times the odds of being described with one or more negative descriptors" [36]. Lastly, only one study focused on implementing a training workshop that provided "actionable skills for replacing biased language in clinical presentations and electronic health records" [14].
3.5. Key Conclusions of Included Studies
Four of the nine studies mention the need for training aimed at using person-centered language. The study by Zota et al. concluded that many healthcare professionals have not received health communication training, which was proven beneficial to “patient relations, professional satisfaction, patient satisfaction, trust, and medication adherence” [37]. Also, four studies mentioned race playing a role in the language used by healthcare professionals (Deb Finn et al.; Sun et al.; Park et al.; Himmelstein et al.). Though, the study by Deb Finn et al., is the only one that directly aims to determine the effects of racial bias (participants reported race/ethnic based discrimination as a large contributor to the challenges experienced when receiving care) [11], three other studies also mentioned race playing a role in the language used by healthcare professionals (Sun et al.; Park et al.; Himmelstein et al.). Sun et al., mentioned that the difference in occurrence of negative descriptors used to describe Black patients opposed to Caucasian patients may not only indicate racial bias among individual healthcare providers, but also amongst the broader attitudes maintained by the healthcare system [36]. Findings in Himmelstein et al. showed that stigmatizing language appeared in patient admission notes more often when describing non-Hispanic Black patients than non-Hispanic White patients [35].
4. Discussion
This scoping review aimed to identify, synthesize, and assess peer-reviewed research articles focused on investigating the use of spoken and/or written language in healthcare settings and on best practices (strategies and interventions) for inclusive language usage by healthcare professionals. The findings regarding inclusive language usage among the nine eligible studies can be broken into two large categories: a) the need to develop more interventions for healthcare providers (e.g., educational workshops and trainings) that can effectively target language used in the communication between healthcare providers and people receiving care; and b) the saliency of racial bias on language used in United States healthcare settings and the need to focus on addressing this kind of bias.
4.1. Increased Training and Research on Inclusive Language
Three of the nine included studies highlighted that there is a great need for training on inclusive language practices for current and future healthcare workers. This type of training is important because of its potential to increase the quality of care a patient may receive. As discussed in the background literature review, action-oriented interventions aimed at transitioning from non-person-centered language to person-centered language are lacking [6,11,14,22,38]. Similarly, the Raney et al. article, part of the nine articles reviewed for this study, concluded that workshops need to provide actionable skills for replacing biased language [14]. The articles in this scoping review showed that when offered workshops and trainings, healthcare professionals were more willing to apply the skills they learned into practice. Implementing workshops could be as simple as hospitals hosting trainings to help healthcare professionals meet or keep accreditations, inclusive language workshops at conventions or conferences, and inclusive language pamphlets or guidebooks that professionals could keep on their lanyards, ID badges, or in their pockets. Further, implementation science research should be conducted to identify the effectiveness and appropriateness of inclusive language tools and the overall success of related interventions.
Cultivating and sustaining trust was another important element related to this category, as it has been demonstrated that patient-provider trust is essential because of increased chances for better health outcomes such as for example correct medicine usage [14,37]. A call to action by authors from the nursing field suggests beginning communication with neutrally related terms and asking patients about their language preferences as a good practice for inclusive communication in healthcare settings [25]. Supporting patients in expressing their preferences can build trust and demonstrate they have agency in their healthcare journey and process.
4.2. Racial Bias on Language Usage in US Healthcare Settings
Lastly, there is pressing need to address systematic racism in the healthcare system in the United States, where seven of the nine included studies took place. Of these seven, four studies mentioned race playing a role in the language used by healthcare professionals (Deb Finn et al.; Sun et al.; Park et al.; Himmelstein et al.). Historically inaccurate stereotypes and biases have harmed marginalized and minority communities in U.S. healthcare settings, stigmatizing them with, for example, the use of negative descriptors in medical notes, as shown by the findings of one of the articles included in this review by Sun et al., which showed black patients having “2.54 times the odds of being described [in medical notes] with one or more negative descriptors” [36]. Implicit bias and negative language, whether spoken or written, can harm patient recovery, patient-provider trust, and overall quality of care. This is exemplified in the recent push to omit racial and ethnic identifiers from clinical presentations and case reports due to concerns about the association of race/ethnicity with negative traits or socioeconomic factors [7].
Patients are unlikely to return to providers who they feel do not have their best interest at hand or who they may perceive as discriminating and disrespectful. Another of the four articles mentioning the role of race, discusses how patients who have difficult interactions with clinicians may perceive that they are not receiving quality care and are at risk of distrusting their care team [34]. This could lead to prolonged periods before seeking treatment, leading to worse health outcomes or distrust in the healthcare system overall. Sensitivity to and awareness of cultural differences and related racial bias becomes critical to overcome issues of non-inclusive spoken and written language. As mentioned in the book chapter by Mahdi and Fiedler titled “Culture, language, and health care professionals”, cultural competence (also referred as cultural proficiency) training is essential for health professionals [39]. This type of training or curriculum can help address stigmatizing or harmful language usage in healthcare settings. Despite the growing increase in knowledge amongst healthcare providers on person-centered language, this review suggests that much more research and training interventions are needed to achieve greater inclusivity in healthcare settings.
5. Review Limitations
A possible limitation of this review is an incomplete retrieval of studies. Only the first 80 relevant studies resulting from each database search were reviewed. While the article search was set to display “most relevant first”, it is recognized that studies past 80 could have still been relevant to the search criteria. A second study limitation is the constant update of knowledge. While this literature review is based on the availability of literature at the time of search (December 2023), it is important to recognize that literature is constantly evolving and what may be available in the present is likely to be more than what was present at the time of search. It is also important to note that key search terms could have been missed. While comprehensive and expansive keywords and terms were used to conduct this literature search, it is plausible that different word combinations could have brought retrievals that yielded eligible information. Finally, it should be acknowledged that only English literature was surveyed. Retrieval of literature in different languages could have also provided eligible articles for review.
6. Public Health Implications and Recommendations
Enhancing inclusive language usage in healthcare settings carries significant implications for patient-provider dynamics and overall healthcare outcomes. It allows a provider to see the person as a complete being and not as a few identity labels. This cultivates a more trusting and solid therapeutic relationship that can widen the diagnostic scope when considering possible causes of illness. Embracing language that acknowledges and respects individuals' identities and experiences also fosters trusting environments where patients feel valued and understood. Research indicates that this approach can enhance treatment adherence, mitigate healthcare disparities, and boost patient satisfaction. Additionally, using inclusive language can contribute to dismantling systemic barriers that historically perpetuated inequality and healthcare disparities.
Implementing person-centeredness in healthcare requires a multifaceted approach in which communication skills are an essential aspect. Comprehensive communication training programs are essential for healthcare professionals. These programs should encompass cultural humility, ongoing bias training, and effective and practical communication techniques and skills for healthcare providers which should be tailored to diverse patient populations. Clear guidelines and policies on using inclusive language, especially in patient interactions and documentation, should complement these training initiatives. The reviewed studies underscore the significance of providing training and support to both current healthcare professionals and those in training to successfully integrate inclusive language strategies into healthcare settings.
6. Conclusions
It is crucial to equip both new and experienced healthcare providers with training on using inclusive language. While the initial steps may appear challenging, this transition holds immense potential to enhance the quality of patient care. Influential organizations such as the American Medical Association and the World Health Organization have urged healthcare professionals to adopt inclusive language. However, how can we expect the next generation of healthcare providers to effect this change without adequate education and training to integrate this into their professional practice? Integrating inclusive language practices into the curriculum for healthcare practitioners in training provides a key strategy for a future generalized adoption of inclusive language in healthcare practices. Similarly, continuing education for current healthcare providers through a variate of educational opportunities such as workshops, seminars, healthcare conventions or continuing education events can effectively introduce inclusive care language into their practice.
Moreover, systemic racism within the United States healthcare system has perpetuated biases, erected barriers, and deepened divides, disproportionately impacting minority populations. These biases often manifest in healthcare providers’ spoken and written language usage and patient treatment, leading to adverse health outcomes. Inclusive language is essential in healthcare to foster trust, support, and optimal health outcomes for patients.
For far too long, the power dynamic of the clinical relationship between the patient and healthcare provider has lied in the hands of the provider. Inclusive language reframes the traditional power imbalance by empowering the patient. There is a pressing need for further efforts to ensure that future healthcare providers receive comprehensive training, practices, and terminology essential for implementing inclusive, person-centered care across all societal groups.
Author Contributions
Conceptualization, B.P. and C.E.O.; methodology, C.E.O. and B.P.; software, B.P.; formal analysis, B.P. and C.E.O.; writing—original draft preparation, B.P.; writing—review and editing, B.P., C.E.O., V.C.M. and J.O.; visualization, B.P.; supervision, C.E.O. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Acknowledgments
We like to acknowledge Alondra Zamora for her contributions as a review collaborator (second reviewer for data screening and abstraction) and for her continuous encouragement, insightful ideas, and constructive criticism.
Conflicts of Interest
V.C.M. has received investigator-initiated research grants (to the institution) and consultation fees from Eli Lilly, Bayer, Gilead Sciences, Merck, and ViiV. V.C.M has also received funding support from the Emory Center for AIDS Research (P30AI050409) for work related to this manuscript.
Appendix A. Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist
Appendix B. Word Combinations used in Data Search.
| Appendix B. Data Search | |||
| Database: ScienceDirect | |||
| Keyterms: | Number of Original Return | Number of Filtered for Research Articles | Number of Articles Exported |
| Bias language AND Healthcare | 43,754 | 27,657 | 5 |
| Bias language AND Healthcare Workers | 10,830 | 6,732 | 0 |
| Bias language AND Infectious Diseases | 15,734 | 8,645 | 5 |
| Public Health AND bias language | 92,573 | 61,723 | 8 |
| Public Health AND Stigmatizing Language | 11,527 | 7,603 | 13 |
| Healthcare Workers AND Stigmatizing Language | 2,304 | 1,451 | 8 |
| Healthcare Workers AND Stigma | 7,607 | 4,750 | 12 |
| Healthcare AND Stigma AND Sexually Transmitted Diseases | 2,009 | 1,604 | 5 |
| Hospitals AND Stigma AND Sexually Transmitted Diseases | 3,435 | 1,816 | 11 |
| Database: PubMed | |||
| Keyterms: | Number of Original Returns | Number of Filtered for Research Articles | Number of Articles Exported |
| Bias language AND Healthcare | 1,693 | 1,351 | 3 |
| Bias language AND Healthcare Workers | 521 | 373 | 0 |
| Bias language AND Infectious Diseases | 350 | 310 | 0 |
| Public Health AND bias language | 7,150 | 5,494 | 2 |
| Public Health AND Stigmatizing Language | 407 | 253 | 12 |
| Healthcare Workers AND Stigmatizing Language | 126 | 63 | 8 |
| Healthcare Workers AND Stigma | 4,264 | 2,593 | 2 |
| Healthcare AND Stigma AND Sexually Transmitted Diseases | 2,773 | 2,412 | 7 |
| Hospitals AND Stigma AND Sexually Transmitted Diseases | 1,311 | 1,021 | 1 |
| Database: ProQuest Socioligcal Abstract | |||
| Keyterms: | Number of Original Return | Number of Filtered for Research Articles | Number of Articles Exported |
| Bias language AND Healthcare | 5,434 | 3,567 | 7 |
| Bias language AND Healthcare Workers | 3,463 | 3,216 | 1 |
| Bias language AND Infectious Diseases | 1,321 | 852 | 3 |
| Public Health AND bias language | 20,549 | 15,723 | 7 |
| Public Health AND Stigmatizing Language | 2,601 | 549 | 1 |
| Healthcare Workers AND Stigmatizing Language | 680 | 367 | 12 |
| Healthcare Workers AND Stigma | 3,382 | 2,270 | 0 |
| Healthcare AND Stigma AND Sexually Transmitted Diseases | 740 | 509 | 2 |
| Hospitals AND Stigma AND Sexually Transmitted Diseases | 779 | 523 | 0 |
| All Databases and Keyterms searched on December 26, 2023. Present day searches may vary | |||
| Database: CINAHL | |||
| Keyterms: | Number of Original Return | Number of Filtered for Research Articles | Number of Articles Exported |
| Bias language AND Healthcare | 37 | 34 | 3 |
| Bias language AND Healthcare Workers | 3 | 3 | 0 |
| Bias language AND Infectious Diseases | 0 | 0 | 0 |
| Public Health AND bias language | 4 | 4 | 0 |
| Public Health AND Stigmatizing Language | 9 | 9 | 1 |
| Healthcare Workers AND Stigmatizing Language | 3 | 3 | 0 |
| Healthcare Workers AND Stigma | 868 | 832 | 11 |
| Healthcare AND Stigma AND Sexually Transmitted Diseases | 149 | 142 | 0 |
| Hospitals AND Stigma AND Sexually Transmitted Diseases | 13 | 13 | 4 |
| All Databases and Keyterms searched on June 26, 2024. Present day searches may vary | |||
References
- Bible, New International Version. Proverbs 18:21. Biblica 2011.
- Ashford, R.D.; Brown, A.M.; McDaniel, J.; Curtis, B. Biased labels: An experimental study of language and stigma among individuals in recovery and health professionals. Subst Use Misuse 2019, 54(8), 1376–1384. [CrossRef]
- Marjadi, B.; Flavel, J.; Baker, K.; Glenister, K.; Morns, M.; Triantafyllou, M.; Gardiner, P.A. Twelve Tips for Inclusive Practice in Healthcare Settings. Int J Environ Res Public Health 2023, 20(5), 4657. [CrossRef]
- Gerchow, L.; Burka, L.R.; Miner, S.; Squires, A. Language barriers between nurses and patients: A scoping review. Patient Educ Couns 2021, 104(3), 534–553. [CrossRef]
- Hsueh, L.; Hirsh, A.T.; Maupomé, G.; Stewart, J.C. Patient-Provider Language Concordance and Health Outcomes: A Systematic Review, Evidence Map, and Research Agenda. Med Care Res Rev 2021, 78(1), 3-23. [CrossRef]
- Vella, E.; White, V. M.; Livingston, P. Does cultural competence training for health professionals impact culturally and linguistically diverse patient outcomes? A systematic review of the literature. Nurse Education Today 2022, 118, 105500. [CrossRef]
- Robling, K., Cosby, C., Parent, G., Gajjar, S., Chesher, T., Baxter, M., & Hartwell, M. (2023). Person-centered language and pediatric ADHD research: a cross-sectional examination of stigmatizing language within medical literature. Journal of osteopathic medicine, 123(4), 215–222. [CrossRef]
- Griffin, Z.; Long, P.; Peña, A.; Jacobsen, S.; Johnson, A. L.; Ottwell, R.; Torgerson, T.; Walters, C.; Ghebrehiwet, M.; Vassar, M.; Hartwell, M. Obesity, stigma, and person-centered language: A serial cross-sectional analysis of scientific literature.
- Harney, B.L.; Korchinski, M.; Young, P.; Scow, M.; Jack, K.; Linsley, P.; Bartlett, S.R. It is time for us all to embrace person-centred language for people in prison and people who were formerly in prison. Int J Drug Policy 2022, 99, 103455. [CrossRef]
- Goddu, A.P.; O'Conor, K.J.; Lanzkron, S.; Saheed, M.O.; Saha, S.; Peek, M.E.; Haywood, C., Jr; Beach, M.C. Do Words Matter? Stigmatizing Language and the Transmission of Bias in the Medical Record. J Gen Intern Med 2018, 33(5), 685–691. [CrossRef]
- Columbia University. Using Inclusive Language. Columbia University Department of Pediatrics 2022. Available online: https://www.pediatrics.columbia.edu/using-inclusive-language#:~:text=Inclusive%20language%20is%20a%20framework,person%20rather%20than%20their%20characteristics (accessed on 29 May 2024).
- Crocker, A. F., & Smith, S. N. (2019). Person-first language: are we practicing what we preach?. Journal of multidisciplinary healthcare, 12, 125–129. [CrossRef]
- Blum, A. (2022). Remove Race as an Initial Identifier From Clinical Presentations. American Family Physician, 106(2), 120–121.
- Håkansson Eklund, J.; Holmström, I. K.; Kumlin, T.; Kaminsky, E.; Skoglund, K.; Höglander, J.; ... Summer Meranius, M. "Same same or different?" A review of reviews of person-centered and patient-centered care. Patient Educ Couns 2019, 102(1), 3-11. [CrossRef]
- Murphy, K. (2013, February 15). HIV/AIDS movement has lost historic voice in NAPWA. NMAC. https://www.nmac.org/hivaids-movement-has-lost-historic-voice-in-napwa/#:~:text=NAPWA%20was%20founded%20in%201983,discussions%20that%20impacted%20their%20lives.
- U.S. Department of Health and Human Services. (2023, April 12). Writing respectfully: Person-first and identity-first language. National Institutes of Health. https://www.nih.gov/about-nih/what-we-do/science-health-public-trust/perspectives/writing-respectfully-person-first-identity-first-language.
- UNAIDS. (2023, June 26). The Denver principles: 40 Years on. UNAIDS. https://www.unaids.org/en/resources/presscentre/featurestories/2023/june/20230626_denver-principles-40-years-on.
- Kim, S.K.; Park, M. Effectiveness of person-centered care on people with dementia: a systematic review and meta-analysis. Clin Interv Aging 2017, 12, 381-397. [CrossRef]
- Lee, K. H.; Lee, J. Y.; Kim, B. Person-Centered Care in Persons Living With Dementia: A Systematic Review and Meta-analysis. The Gerontologist 2022, 62(4), e253–e264. [CrossRef]
- Wu, Q.; Qian, S.; Deng, C.; Yu, P. Understanding Interactions Between Caregivers and Care Recipients in Person-Centered Dementia Care: A Rapid Review. Clinical interventions in aging 2020, 15, 1637–1647. [CrossRef]
- Auckburally, S.; Davies, E.; Logue, J. The Use of Effective Language and Communication in the Management of Obesity: the Challenge for Healthcare Professionals. Curr Obes Rep 2021, 10(3), 274-281. [CrossRef]
- Ivezaj, V.; Lydecker, J. A.; Grilo, C. M. Language Matters: Patients' Preferred Terms for Discussing Obesity and Disordered Eating with Health Care Providers After Bariatric Surgery. Obesity (Silver Spring, Md.) 2020, 28(8), 1412–1418. https://doi.org/10.1002/oby.22868. Headley, S., Potter, I., Ottwell, R., Rogers, T., Vassar, M., & Hartwell, M. (2022). Adherence rates of person-centered language in amputation research: A cross-sectional analysis. Disabil Health J, 15(1), 101172. [CrossRef]
- Headley, S.; Potter, I.; Ottwell, R.; Rogers, T.; Vassar, M.; Hartwell, M. Adherence rates of person-centered language in amputation research: A cross-sectional analysis. Disabil Health J 2022, 15(1), 101172. [CrossRef]
- Stortenbeker, I. A.; Houwen, J.; Lucassen, P.; Stappers, H. W.; Assendelft, W. J. J.; van Dulmen, S.; ... Das, E. Quantifying positive communication: Doctor's language and patient anxiety in primary care consultations. Patient Educ Couns 2018, 101(9), 1577-1584. [CrossRef]
- Truong, M.; Lazarus, M.; Ochoa, G. G.; Brand, G. Resisting and unlearning dehumanising language in nursing and healthcare practice, education and research: A call to action. Nurse Educ Today 2022, 116, 105458. [CrossRef]
- Peters, Micah & Godfrey, Christina & Mcinerney, Patricia & Munn, Zachary & Trico, Andrea & Khalil, Hanan. (2020). Chapter 11: Scoping Reviews. 10.46658/JBIMES-20-12.
- Sutton, A., Clowes, M., Preston, L., & Booth, A. (2019). Meeting the review family: exploring review types and associated information retrieval requirements. Health information and libraries journal, 36(3), 202–222. [CrossRef]
- Khalil, H., Peters, M. D., Tricco, A. C., Pollock, D., Alexander, L., McInerney, P., Godfrey, C. M., & Munn, Z. (2021). Conducting high quality scoping reviews-challenges and solutions. Journal of clinical epidemiology, 130, 156–160. [CrossRef]
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane 2021. Available from train-ing.cochrane.org/handbook.
- Sarkis-Onofre, Rafael; Catalá-López, Ferrán; Aromataris, Edoardo; Lockwood, Craig. How to properly use the PRISMA Statement. Systematic Reviews 2021, 10. [CrossRef]
- Uman L. S. Systematic reviews and meta-analyses. Journal of the Canadian Academy of Child and Adolescent Psychiatry = Journal de l'Academie canadienne de psychiatrie de l'enfant et de l'adolescent 2011, 20(1), 57–59.
- Covidence. (2022). About Us. Retrieved from https://www.covidence.org/about-us-covidence/.
- PRISMA. (2022). Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Retrieved from https://www.prisma-statement.org/.
- Park, J.; Saha, S.; Chee, B.; Taylor, J.; Beach, M. C. Physician Use of Stigmatizing Language in Patient Medical Records. JAMA Netw Open 2021, 4(7), e2117052. [CrossRef]
- Himmelstein, G.; Bates, D.; Zhou, L. Examination of Stigmatizing Language in the Electronic Health Record. JAMA Netw Open 2022, 5(1), e2144967. [CrossRef]
- Sun, M.; Oliwa, T.; Peek, M. E.; Tung, E. L. Negative Patient Descriptors: Documenting Racial Bias In The Electronic Health Record. Health Affairs 2022, 41(2), 203-208. [CrossRef]
- Zota, D.; Diamantis, D. V.; Katsas, K.; Karnaki, P.; Tsiampalis, T.; Sakowski, P.; Linos, A. Essential Skills for Health Communication, Barriers, Facilitators and the Need for Training: Perceptions of Healthcare Professionals from Seven European Countries. Healthcare 2023, 11(14), 2058. [CrossRef]
- Raney J, Pal R, Lee T, Saenz SR, Bhushan D, Leahy P, Johnson C, Kapphahn C, Gisondi MA, Hoang K. Words Matter: An Antibias Workshop for Health Care Professionals to Reduce Stigmatizing Language. MedEdPORTAL. 2021;17:11115. [CrossRef]
- Mahdi, D.A.; Fiedler, B.A. Culture, language, and health care professionals. In Three Facets of Public Health and Paths to Improvements; Academic Press 2020, pp. 213-237. [CrossRef]
Figure 1.
PRISMA Flowchart- Screening Process.
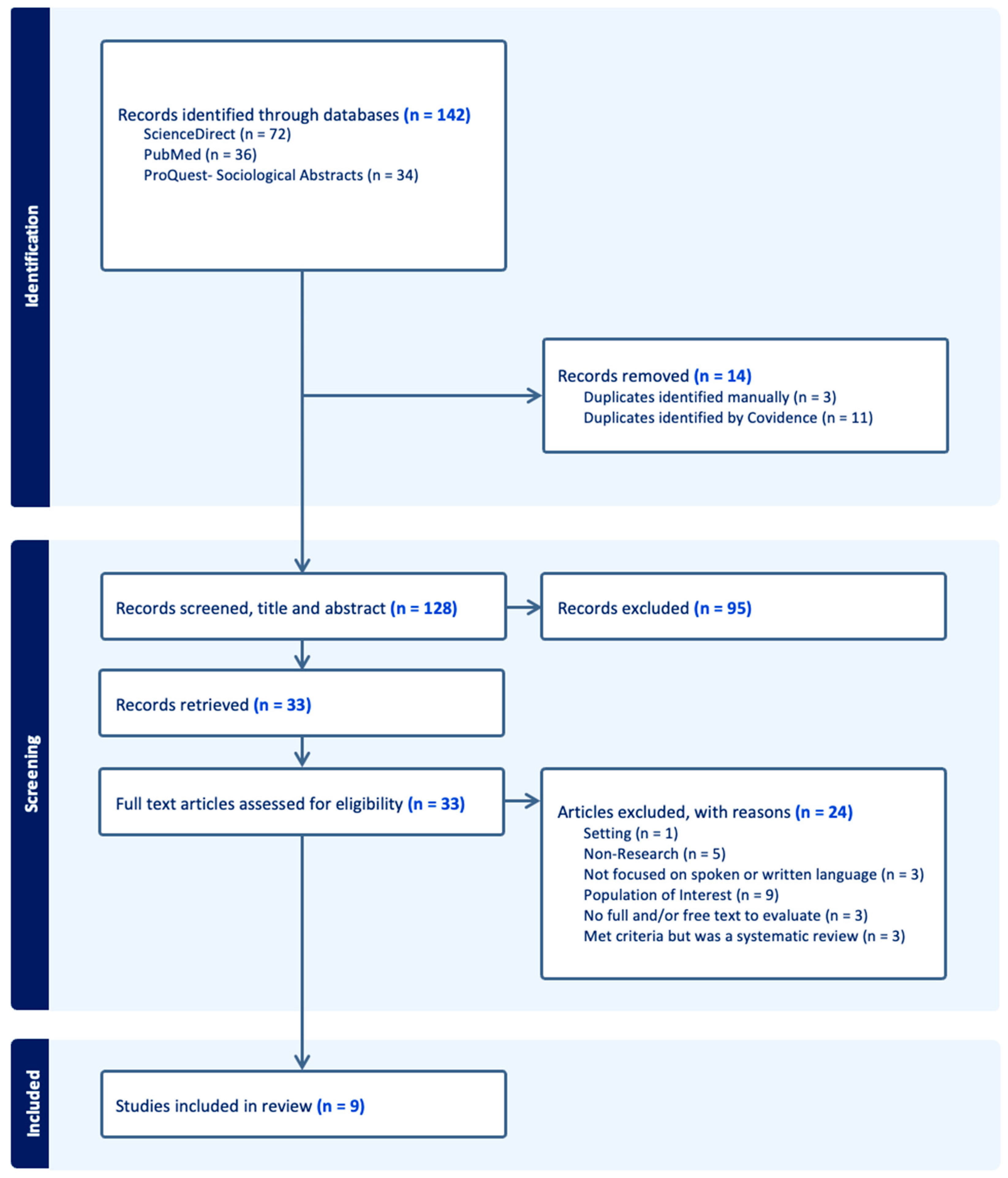
Table 1.
Key Characteristics Found in Included Studies.
| Lead Author (Year) | Title | Country in Which the Study Conducted | Study Design | Total Number of Participants | Health Condition |
|---|---|---|---|---|---|
| Zota et al. (2023) |
Essential Skills for Health Communication, Barriers, Facilitators and the Need for Training: Perceptions of Healthcare Professionals from Seven European Countries |
Europe: Cyprus, Germany, Greece, Poland, Spain | Cross Sectional Study | N = 702 Patients | N/A |
| Sun et. al (2022) |
Negative Patient Descriptors: Documenting Racial Bias In The Electronic Health Record |
United States | Cross Sectional Study | N = 18,459 Patients | N/A |
| Raney et al. (2021) | Words Matter: An Antibias Workshop for Health Care Professionals to Reduce Stigmatizing Language | United States | Qualitative Study | N = 66 Participants | N/A |
| Park et al. (2021) |
Physician Use of Stigmatizing Language in Patient Medical Records |
United States | Qualitative Study | N = 138 Clinicians (attendings and residents) | Not Specfied |
| Himmelstein et al. (2022) |
Examination of Stigmatizing Language in the Electronic Health Record |
United States | Cross Sectional Study | N1 = 29,783 Patients N2 = 1,932 Clinicians | Diabetes, Substance Use Disorder, and Chronic Pain |
| DeMaria et al. (2023) | The role of community healthcare professionals in discussing sexual assault experiences during obstetrics and gynecological healthcare appointments | United States | Qualitative Study | N = 22 Women | Sexual Trauma |
| Deb Finn et al. (2021) | Experiences of everyday racism in Toronto's health care system: a concept mapping study | Canada | Semi-Qualitative Study | Size varies based on activity | N/A |
| Ashford et al. (2019) | Biased labels: An experimental study of language and stigma among individuals in recovery and health professionals | United States | Randomised Controlled Trial | N = 299 Participants | Substace Use Disorder (SUD) |
| Goddu et al. (2018) |
Do Words Matter? Stigmatizing Language and the Transmission of Bias in the Medical Record |
United States | Randomized Vignette Study | N = 413 physicians-in-training | Sickle Cell Disease |
Table 3.
Measurements and Outcomes in Included Studies.
| Table 3. Measurements and Outcomes of Included Studies | |||||
|---|---|---|---|---|---|
| Lead Author (year) | Method of Outcome | Outcomes Measured | Primary Outcomes Reported | Secondary Outcomes Reported | Key Conclusions of Authors |
| Zota et al. (2023) | Online questionnaire, comprising 35 close-ended questions | Benefits, barriers and outcomes of effective health communication from the point of view of healthcare professionals | Physicians appear to be less concerned about communication skills, the barriers and facilitators of effective communication and perceived outcomes of successful communication | N/A | - Many healthcare professionals have yet to receive HCT, even though almost everyone identifies the beneficial effect of successful health communication on improved professional–patient relations, professional satisfaction and patient satisfaction, trust and medication adherence |
| Sun et. al (2022) | Natural language processing and machine learning | The occurrence of at least one negative descriptor in a patient’s history and physical note | In total, 8.2 percent of patients had one or more negative descriptors recorded in the history and physical notes in their EHR | Black patients had 2.54 times the odds of being described with one or more negative descriptors in the history and physical notes of their EHRs, even after we adjusted for their sociodemographic and health characteristic | This difference may indicate implicit racial bias not only among individual providers but also among the broader beliefs and attitudes maintained by the health care system |
| Raney et al. (2021) | Course Evaluation | Data familiarization, identifying themes, developing and applying a coding scheme, and organizing codes and themes. | Most believed the workshop met its objectives (4.8 out of 5.0) and strongly agreed that they would apply skills learned (4.8) | N/A | Workshop provided actionable skills for replacing biased language in clinical presentations and electronic health records |
| Park et al. (2021) | Encounter notes | Common linguistic characteristics reflecting an overall positive or negative attitude toward the patient | Five negative language categories: questioning credibility, disapproval, stereotyping, difficult patient, and unilateral decisions Six positive language categories: compliment, approval, self-disclosure, minimizing blame, personalize, and bilateral decision making |
N/A | This qualitative study found that physicians express negative and positive attitudes toward patients when documenting in the medical record Patients who have difficult interactions with a clinician may perceive that they are not receiving high-quality, patient-centered care, and may be at risk of distrusting or disengaging from care |
| Himmelstein et al. (2022) | Admission Notes | Stigmatizing language | Stigmatizing language appeared in 1197 of all 48 651 notes (2.5%); diabetes-specific stigmatizing language appeared in 599 notes for patients with diabetes (6.9%); language stigmatizing substance use appeared in 209 notes for patients with substance use disorder (3.4%); 37 notes for patients with chronic pain included stigmatizing language regarding pain (0.7%) | Across all medical conditions studied, stigmatizing language appeared more frequently in notes written about non-Hispanic Black patients | Although the stigmatizing language we assessed appeared infrequently, it has the potential to unnecessarily alienate patients and influence subsequent clinicians. Findings suggest that stigmatizing language appears in patients’ EHR admission notes, varies by medical condition, and is more often used to describe non-Hispanic Black than non-Hispanic White patients. Therefore, efforts to understand and minimize the use of stigmatizing language might improve patients’ care and their trust in their clinicians |
| DeMaria et al. (2023) | Semi-structured protocol focus groups and key-informant interviews | perspectives, novel experiences, and shared knowledge | There were three resulting themes: (1) healthcare professionals’ approaches to screening for a history of sexual assault varied depending on the providers’ work setting and their field; (2) healthcare experiences can compound traumatic experiences and create professional distrust with survivors; (3) sexual assault impacts patient healthcare experiences through the services they seek, how professionals interact with them, and type of professional they are willing to see. | N/A | One strength of this study was the inclusion of doulas. Doulas may gain additional patient context that a healthcare professional can use, with patient permission, to increase sensitivity to women’s needs in their birth experience Incorporating healthcare professionals’ and patients experiences and preferences for sexual assault-related discussions during routine obstetrical and gynecological care can assist in sexual assault prevention and treatment efforts, improve patient-professional rapport, and yield better health outcomes |
| Deb Finn et al. (2021) | Concept Mapping using Concept System® Global MAXTM software | Understanding complex the experiences of the target population | Racialized health care users reported that access to and quality of medical care are challenges cur- rently experienced in Toronto’s health care system | N/A | - Racialized health care users from Toronto (Canada’s largest city) and the Greater Toronto Area, reported ‘race’/ethnic based discrimination as largely contributory to the challenges experienced when receiving care. - Racialized health care users also prioritized unequal access to medical care for taking action/change |
| Ashford et al. (2019) | Scoring of the GNATs was done using the d-prime (d’) method. The method calculates sensitivity, indexed by d’, by converting the proportion of correct responses for signal items and incorrect responses for noise items into z-scores and then calculating the difference between the z-score value | Recovery status and employment types effects on views of SUD terminology | Descriptive statistics showed that while participants not in recovery had stronger associations than participants in recovery with most linguistic choices (addict + good M = 1.66; SUD + good M = 1.61, SUD + bad M = 2.10), that participants in recovery had stronger associations than participants not in recovery for addict + bad (M = 2.58). | health professional participants had stronger associations than non-health professional participants for all linguistic choices, with mean differences of .511 for substance abuse + good, .431 for substance abuse + bad, .248 for SUD + good, and .145 for SUD + bad. |
- The labels that are often used to identify and describe individuals with a SUD or in recovery can often be stigmatizing. - Terms such as “addict’ and “substance abuser” are also associated with greater levels of bias among individuals in recovery and health professionals. - Health professionals, having greater levels of negative association with stigmatizing terms, should commit to improving their linguistic choices in all manner of communication. |
| Goddu et al. (2018) | Qualtrics survey platform | Attitudes towards the hypothetical patient and pain management decisions (residents only | Exposure to the stigmatizing language note was associated with more negative attitudes towards the patient (20.6 stigmatizing vs. 25.6 neutral, p < 0.001) | reading the stigmatizing language note was associated with less aggressive management of the patient’s pain (5.56 stigmatizing vs. 6.22 neutral, p = 0.003) |
Stigmatizing language used in medical records to describe patients can influence subsequent physicians-in-training in terms of their attitudes towards the patient and their medication prescribing behavior |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



