Submitted:
20 November 2024
Posted:
21 November 2024
You are already at the latest version
Abstract
Suicide is a global phenomenon, with more than 700,000 people worldwide taking their own life yearly. Both natural and human-made disaster may have a detrimental effect on suicidal behaviors both in the short-term and in the long-term. Many studies focused on the acute impact of the COVID-19 pandemic on suicidality. The aim of the study was to analyze demographic and clinical features of subjects accessing the emergency rooms for suicidality during the second epidemic wave of COVID-19 in five emergency departments in Lombardy (Italy). A retrospective chart review was conducted in the five emergency departments for the period 4 June – 31 December 2020, and during the same time lapse in 2019. For all subjects accessing for suicidality, socio-demographic and clinical data were collected and compared between the two years. No differences between the two years were found for sex, triage priority level, history of substance abuse, factor triggering suicidality and discharge diagnosis. During 2020 a greater proportion of subjects did not show any previous mental disorder, however, more subjects were already taking anxiolytic medications before the admission. Among a range of possible risk factors, attempted suicide, depression diagnosis and taking medications before the admission were found to be predictor of admission to psychiatric inpatient units. Characterizing subjects prone to suicidality during the second wave of the COVID-19 pandemic, our study provides hints for mid-term causes of suicidality and possible preventive measures that could be helpful in the course and after massive infectious outbreaks.
Keywords:
1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of Subjects Accessing the ED for Suicidality During the Second Wave of COVID-19 in 2020
3.1.1. Distribution by District of Admission
3.1.2. Distribution Between Low-Epidemic and Peak-Epidemic Stage
3.1.3. Distribution by Sex
3.1.4. Risk for Admission to the Psychiatric Inpatient Care Unit
3.2. Comparison Between 2020 and 2019
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO, IASP.
- Klonsky ED, May AM, Saffer BY. Suicide, Suicide Attempts, and Suicidal Ideation. Annu Rev Clin Psychol. 2016 Mar 28;12(1):307–30.
- Bertolote, J.M.; Fleischmann, A. Suicide and psychiatric diagnosis: a worldwide perspective. World Psychiatry 2002, 1, 181–5.
- Nordentoft, M.; Mortensen, P.B.; Pedersen, C.B. Absolute Risk of Suicide After First Hospital Contact in Mental Disorder. Arch. Gen. Psychiatry 2011, 68, 1058–1064. [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Begum, N.; Saini, A.; Wang, S.; McGuire, P.; Fusar-Poli, P.; Lewis, G.; David, A.S. Suicide, self-harm and thoughts of suicide or self-harm in infectious disease epidemics: a systematic review and meta-analysis – CORRIGENDUM. Epidemiology Psychiatr. Sci. 2021, 30. [CrossRef]
- Kõlves K, Kõlves KE, De Leo D. Natural disasters and suicidal behaviours: A systematic literature review. J Affect Disord. 2013 Mar;146(1):1–14.
- Stratta, P.; Capanna, C.; Riccardi, I.; Carmassi, C.; Piccinni, A.; Dell'Osso, L.; Rossi, A. Suicidal intention and negative spiritual coping one year after the earthquake of L'Aquila (Italy). J. Affect. Disord. 2012, 136, 1227–1231. [CrossRef]
- Carmassi, C.; Stratta, P.; Calderani, E.; Bertelloni, C.A.; Menichini, M.; Massimetti, E.; Rossi, A.; Dell’osso, L. Impact of Mood Spectrum Spirituality and Mysticism Symptoms on Suicidality in Earthquake Survivors with PTSD. J. Relig. Heal. 2015, 55, 641–649. [CrossRef]
- Wasserman D, Iosue M, Wuestefeld A, Carli V. Adaptation of evidence-based suicide prevention strategies during and after the COVID -19 pandemic. World Psychiatry. 2020 Oct 15;19(3):294–306.
- Leaune, E.; Samuel, M.; Oh, H.; Poulet, E.; Brunelin, J. Suicidal behaviors and ideation during emerging viral disease outbreaks before the COVID-19 pandemic: A systematic rapid review. Prev. Med. 2020, 141, 106264–106264. [CrossRef]
- Zortea, T.C.; Brenna, C.T.A.; Joyce, M.; McClelland, H.; Tippett, M.; Tran, M.M.; Arensman, E.; Corcoran, P.; Hatcher, S.; Heise, M.J.; et al. The Impact of Infectious Disease-Related Public Health Emergencies on Suicide, Suicidal Behavior, and Suicidal Thoughts. 2021, 42, 474–487. [CrossRef]
- Yan, Y.; Hou, J.; Li, Q.; Yu, N.X. Suicide before and during the COVID-19 Pandemic: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Heal. 2023, 20, 3346. [CrossRef]
- Worldometers.
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. Qjm: Int. J. Med. 2020, 113, 531–537. [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: a Rapid review of the evidence. Lancet 2020, 395, 912–920. [CrossRef]
- Nordt, C.; Warnke, I.; Seifritz, E.; Kawohl, W. Modelling suicide and unemployment: a longitudinal analysis covering 63 countries, 2000–11. Lancet Psychiatry 2015, 2, 239–245. [CrossRef]
- Almaghrebi, A.H. Risk factors for attempting suicide during the COVID-19 lockdown: Identification of the high-risk groups. J. Taibah Univ. Med Sci. 2021, 16, 605–611. [CrossRef]
- Gesi, C.; Cafaro, R.; Achilli, F.; Boscacci, M.; Cerioli, M.; Cirnigliaro, G.; Loupakis, F.; Di Maio, M.; Dell’osso, B. The relationship among posttraumatic stress disorder, posttraumatic growth, and suicidal ideation among Italian healthcare workers during the first wave of COVID-19 pandemic. CNS Spectrums 2023, 29, 60–64. [CrossRef]
- Telles-Garcia, N.; Zahrli, T.; Aggarwal, G.; Bansal, S.; Richards, L.; Aggarwal, S. Suicide Attempt as the Presenting Symptom in a Patient with COVID-19: A Case Report from the United States. Case Rep. Psychiatry 2020, 2020, 1–3. [CrossRef]
- Purgato M, Gastaldon C, Papola D, van Ommeren M, Barbui C, Tol WA. Psychological therapies for the treatment of mental disorders in low- and middle-income countries affected by humanitarian crises. Cochrane Database of Systematic Reviews. 2018 Jul 5;2018(7).
- McAndrew, J.; O’leary, J.; Cotter, D.; Cannon, M.; MacHale, S.; Murphy, K.C.; Barry, H. Impact of initial COVID-19 restrictions on psychiatry presentations to the emergency department of a large academic teaching hospital. Ir. J. Psychol. Med. 2021, 38, 108–115. [CrossRef]
- Chatterjee, S.S.; Malathesh Barikar, C.; Mukherjee, A. Impact of COVID-19 pandemic on pre-existing mental health problems. Asian J. Psychiatry 2020, 51, 102071. [CrossRef]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Heal. 2017, 152, 157–171. [CrossRef]
- Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, Joiner TE. The interpersonal theory of suicide. Psychol Rev. 2010;117(2):575–600.
- Miller, I.W.; Camargo, C.A.; Arias, S.A.; Sullivan, A.F.; Allen, M.H.; Goldstein, A.B.; Manton, A.P.; Espinola, J.A.; Jones, R.; Hasegawa, K.; et al. Suicide Prevention in an Emergency Department Population. JAMA Psychiatry 2017, 74, 563–570. [CrossRef]
- Claassen, C.A.; Larkin, G.L. Occult suicidality in an emergency department population. Br. J. Psychiatry 2005, 186, 352–353. [CrossRef]
- Gesi, C.; Grasso, F.; Dragogna, F.; Vercesi, M.; Paletta, S.; Politi, P.; Mencacci, C.; Cerveri, G. How Did COVID-19 Affect Suicidality? Data from a Multicentric Study in Lombardy. J. Clin. Med. 2021, 10, 2410. [CrossRef]
- Brenner, J.M.; Marco, C.A.; Kluesner, N.H.; Schears, R.M.; Martin, D.R. Assessing psychiatric safety in suicidal emergency department patients. J. Am. Coll. Emerg. Physicians Open 2020, 1, 30–37. [CrossRef]
- International Business Machines Corporation. IBM SPSS Statistics for Data Analyses; Version 27.0; IBM Corp: Armonk. NY. USA. 2021.
- Er, S.T.; Demir, E.; Sari, E. Suicide and economic uncertainty: New findings in a global setting. SSM - Popul. Heal. 2023, 22, 101387. [CrossRef]
- Tachikawa, H.; Matsushima, M.; Midorikawa, H.; Aiba, M.; Okubo, R.; Tabuchi, T. Impact of loneliness on suicidal ideation during the COVID-19 pandemic: findings from a cross-sectional online survey in Japan. BMJ Open 2023, 13, e063363. [CrossRef]
- Adam, M.; Moran, J.K.; Kippe, Y.D.; Schouler-Ocak, M.; Bermpohl, F.; Gutwinski, S.; Goldschmidt, T. Increase in presentations with new-onset psychiatric disorders in a psychiatric emergency department in Berlin, Germany during the second wave of the COVID-19 pandemic – a retrospective cross-sectional study. Front. Psychiatry 2023, 14, 1240703. [CrossRef]
- Dubé, J.P.; Smith, M.M.; Sherry, S.B.; Hewitt, P.L.; Stewart, S.H. Suicide behaviors during the COVID-19 pandemic: A meta-analysis of 54 studies. Psychiatry Res. 2021, 301, 113998–113998. [CrossRef]
- A Mamun, M. Suicide and Suicidal Behaviors in the Context of COVID-19 Pandemic in Bangladesh: A Systematic Review. Psychol. Res. Behav. Manag. 2021, ume 14, 695–704. [CrossRef]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry 2020, 8, 130–140. [CrossRef]
- Schou, T.M.; Joca, S.; Wegener, G.; Bay-Richter, C. Psychiatric and neuropsychiatric sequelae of COVID-19 – A systematic review. Brain, Behav. Immun. 2021, 97, 328–348. [CrossRef]
- Serrano-Gimeno, V.; Diestre, A.; Agustin-Alcain, M.; Portella, M.J.; de Diego-Adeliño, J.; Tiana, T.; Cheddi, N.; Distefano, A.; Dominguez, G.; Arias, M.; et al. Non-fatal suicide behaviours across phases in the COVID-19 pandemic: a population-based study in a Catalan cohort. Lancet Psychiatry 2024, 11, 348–358. [CrossRef]
- Tanaka, T.; Okamoto, S. Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nat. Hum. Behav. 2021, 5, 229–238. [CrossRef]

| Year 2019 N = 379; [N(%)] |
Year 2020 N = 354; [N(%)] |
Chi-square | Sig. | |
|---|---|---|---|---|
|
Centre Milan Lodi Pavia Voghera Vigevano |
143 (37.7) 88 (23.2) 54 (14.2) 44 (11.6) 50 (13.2) |
104 (29.4) 117 (33.1) 63 (17.8) 33 (9.3) 37 (10.5) |
5.715 8.783 1.718 1.019 1.314 |
.017 .003 .190 .187 .256 |
|
Gender Female Male |
222 (58.6) 157 (41.4) |
210 (59.3) 144 (40.7) |
.042 |
.837 |
|
Nationality Italian Other |
307 (81) 72 (19) |
290 (81.9) 64 (18.1) |
.102 |
.749 |
|
Occupational Status Students Employed Unemployed Retired Other/Unknown |
31 (8.2) 59 (15.6) 133 (35.1) 31 (8.2) 125 (33) |
25 (7.1) 81 (22.9) 129 (36.4) 39 (11) 80 (22.6) |
.324 6.337 .145 1.706 9.794 |
.569 .012 .703 .191 .002 |
|
Marital Status Unmarried Married Separated/Divorced Widowed Other/Unknown |
169 (42.2) 72 (19) 27 (7.1) 14 (3.7) 105 (27.7) |
164 (46.3) 70 (19.8) 39 (11) 14 (4) 67 (18.9) |
8.299 1.254 .071 3.386 0.034 |
.263 .790 .066 .854 .004 |
|
Housing Institution Parents Spouse Alone Other/Unknown |
31 (8.2) 80 (21.1) 103 (27.2) 62 (16.3) 103 (27.2) |
22 (6.2) 93 (26.3) 101 (28.5) 79 (22.3) 59 (16.7) |
1.053 2.706 .167 4.182 11.744 |
.305 .100 .683 .041 <.001 |
|
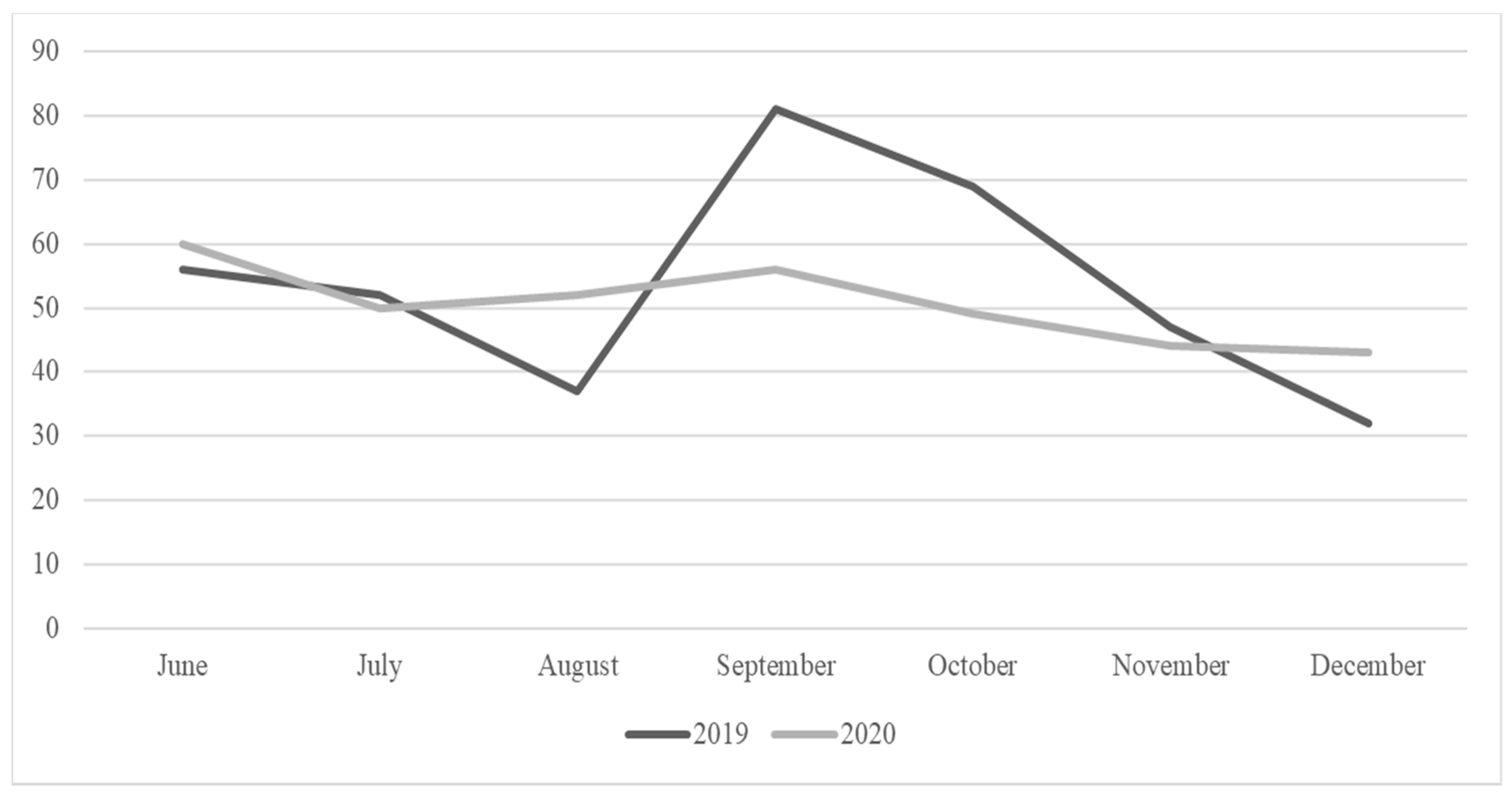
Pandemic phase June 4th – Sept 30th Oct 1st – Dec 31st |
231 (60.9) 148 (39.1) |
237 (66.9) 117 (33.1) |
2.854 |
.091 |
|
COVID-related stressor No Yes |
- - |
280 (78.6%) 74 (21.4%) |
||
|
Age (mean. SD) |
41.70 (±17.85) |
43.42 (±18.19) |
T -1.29 |
Sig. .198 |
| Year 2019 N = 379 [N(%)] |
Year 2020 N = 354 [N(%)] |
Chi-square | Sig. | |
|---|---|---|---|---|
|
Access to Emergency Department Voluntary EMSs Police Other |
142 (37.5) 207 (54.6) 24 (6.3) 6 (1.6) |
108 (30.5) 212 (59.9) 22 (6.2) 12 (3.4) |
5.925 |
.115 |
|
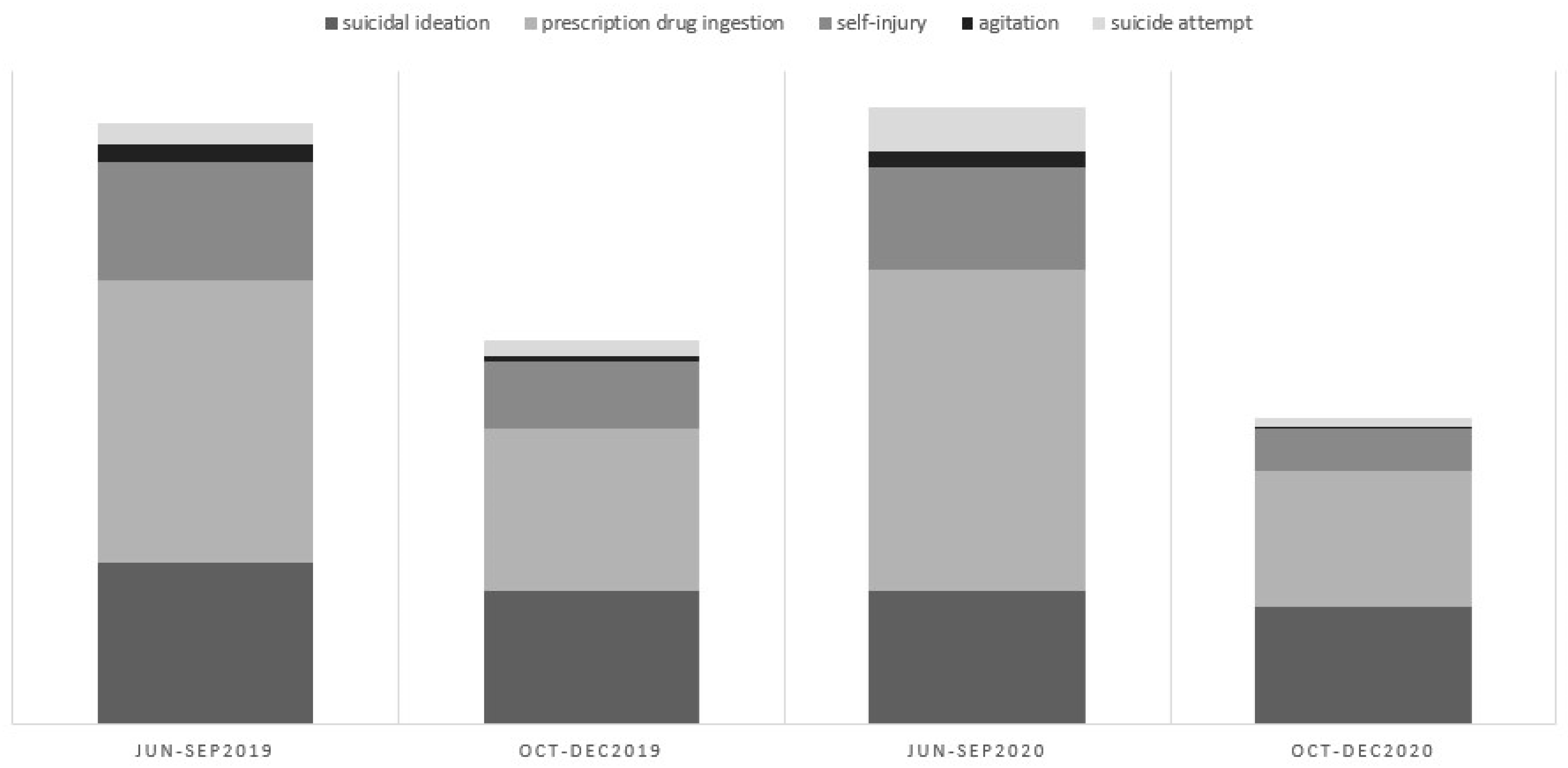
Reason for access Suicidal ideation Prescription drug ingestion Self-injury Agitation Suicide attempt |
113 (29.8) 170 (44.9) 71 (18.7) 9 (2.4) 14 (3.7) |
96 (27.1) 175 (49.4) 55 (15.5) 7 (2) 20 (5.6) |
.689 1.469 1.350 .139 1.565 |
.407 .225 .245 .709 .211 |
|
Consciousness Normal/Agitation Unconscious/Coma |
322 (85.2) 56 (14.8) |
308 (87.3) 45 (12.7) |
.655 |
.418 |
|
Triage priority level High/Red Low |
21 (5.9) 336 (94.1) |
32 (9) 322 (91) |
2.568 |
.109 |
|
Comorbidity No Yes |
209 (55.7) 166 (44.3) |
185 (52.3) 169 (47.7) |
.885 |
.347 |
|
Reason for suicidality Exacerbation Reactive Intoxication |
132 (35.7) 213 (57.6) 25 (6.8) |
142 (40.1) 191 (54) 21 (5.9) |
1.514 .957 .207 |
.218 .328 .649 |
|
Usual Care Provider None Public/private MHS Addiction Service |
132 (34.8) 230 (60.7) 17 (4.5) |
205 (57.9) 142 (40.1) 7 (2) |
39.25 30.99 3.636 |
<.001 <.001 .057 |
|
Substance Abuse No Yes |
276 (72.8) 103 (27.2) |
257 (73.2) 94 (26.8) |
.015 |
.904 |
|
Discharge diagnosis Personality Disorder Mood Disorder Anxiety Disorder Psychotic Disorder No Mental Disorder/harmful substance use |
140 (37.8) 91 (24.5) 38 (10.2) 15 (4) 87 (23.5) |
148 (42.4) 83 (23.7) 33 (9.5) 15 (4.3) 70 (20.1) |
1.635 .055 .125 .029 1.214 |
.201 .815 .723 .864 .156 |
|
Instructions at discharge Admission to psychiatric inpatient care Outpatient psychiatric service Outpatient addiction service Both psychiatric and addiction services Other/General Practitioner |
159 (42) 120 (31.7) 16 (4.2) 11 (2.9) 73 (19.3) |
129 (36.4) 129 (36.4) 11 (3.1) 31 (8.8) 54 (15.3) |
2.331 1.863 .641 11.61 2.052 |
.127 .172 .423 .001 .152 |
| Year 2019 N = 379 [N(%)] |
Year 2020 N = 354 [N(%)] |
Chi-square | Sig. | |
|---|---|---|---|---|
| Psychotropic treatment previous to ED1 consultation | ||||
| Any psychotropic treatment Anxiolytics Antidepressants Antipsychotics Mood stabilizers |
240 (63.3) 185 (50.8) 144 (39.5) 105 (28.8) 70 (19.3) |
240 (68.6) 206 (58.4) 161 (45.6) 104 (29.5) 45 (12.7) |
2.305 4.101 2.784 0.042 5.671 |
.129 .043 .095 .838 .017 |
| Psychotropic treatment administered during ED access | ||||
| Any psychotropic treatment Anxiolytics Antidepressants Antipsychotics Mood stabilizers |
128 (33.8) 115 (30.6) 7 (1.9) 28 (7.4) 0 (0) |
105 (29.7) 95 (26.8) 7 (2) 25 (7.1) 2 (0.6) |
1.427 1.251 .012 .036 2.136 |
.232 .263 .913 .849 .144 |
| Psychotropic treatment prescribed at discharge from ED | ||||
| Any psychotropic treatment Anxiolytics Antidepressants Antipsychotics Mood stabilizers |
183 (48.8) 154 (41.1) 117 (31.2) 84 (22.4) 61 (16.3) |
186 (52.5) 149 (42.1) 119 (33.6) 83 (23.4) 43 (12.1) |
1.020 .079 .485 .113 2.527 |
.312 .779 .486 .737 .112 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



