Submitted:
20 November 2024
Posted:
21 November 2024
You are already at the latest version
Abstract
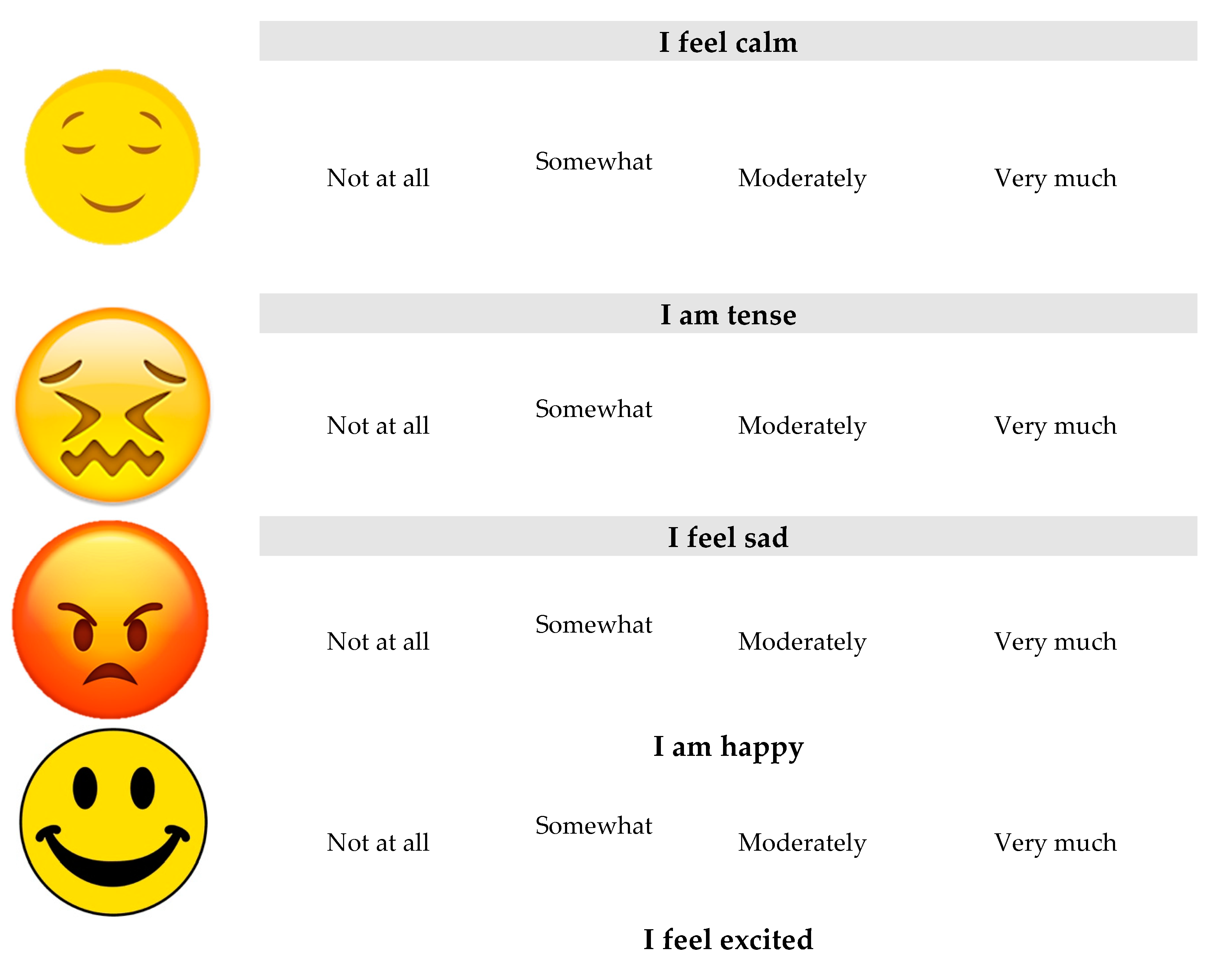
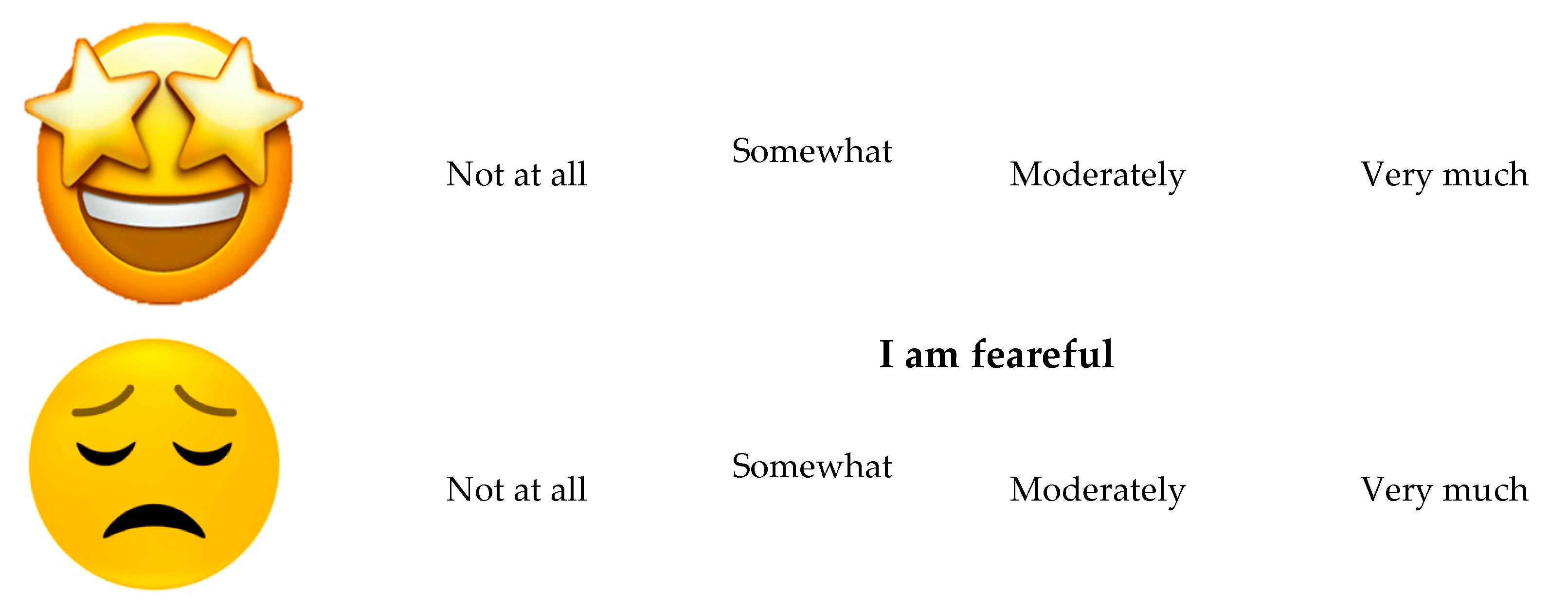
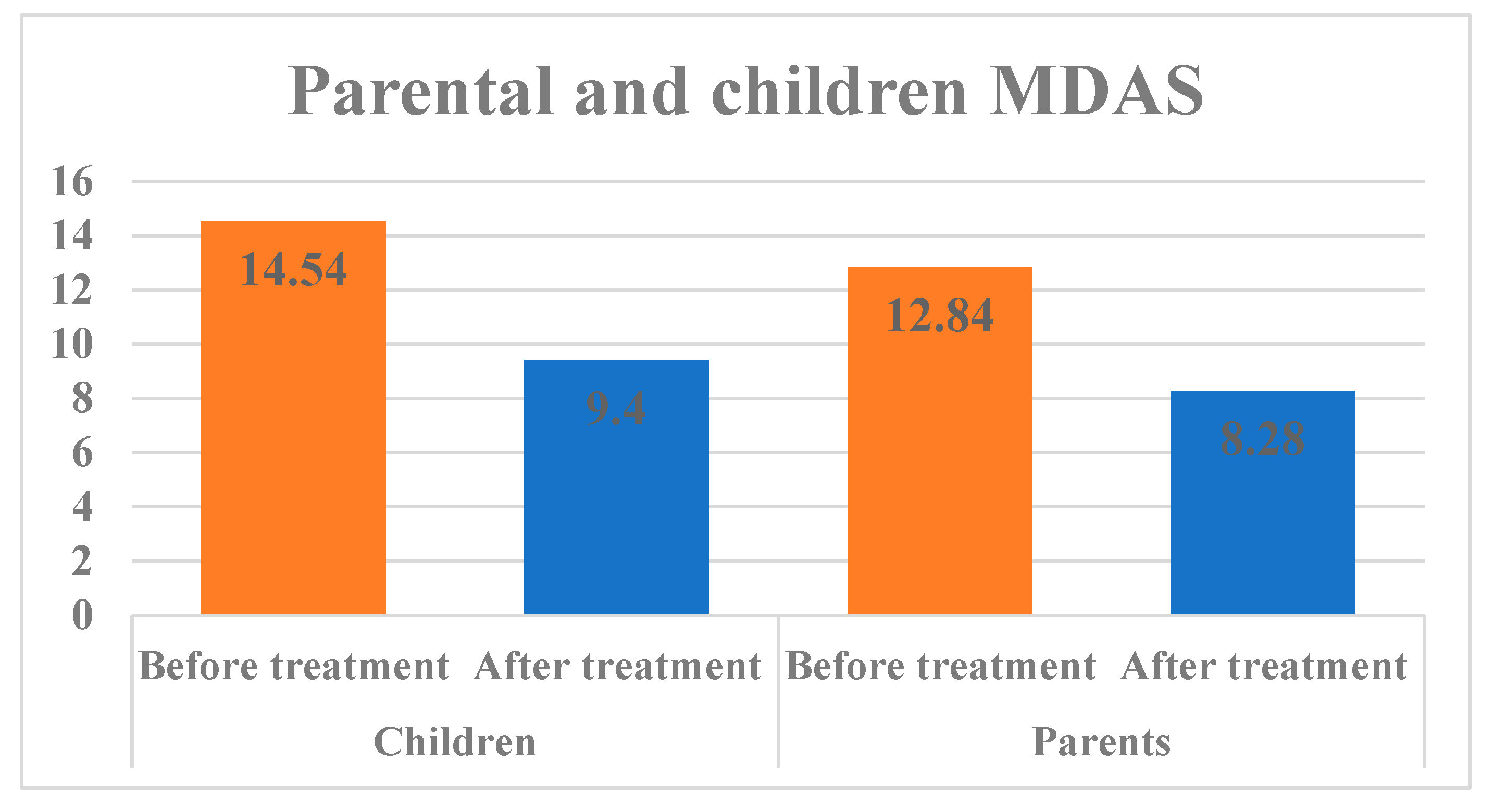
The study aimed to assess dental anxiety (self and proxy reported) using a modified dental Anxiety Scale(MDAS) and modified short state-trait anxiety inventory scale(Emoji). Methods: 200 children visiting the pediatric dental clinic at the College of Dentistry at Prince Sattam bin Abdulaziz University were recruited to assess their levels of anxiety. The anxiety score was measured before and after the treatment using a short STAI scale and MDAS of 200 children using a Modified Dental Anxiety Scale (MDAS) and a modified short STAI (Emoji) Scale. Results: The perception of children MDAS was found to have a highest mean score of 14.54±3.82 after the dental procedure than compared to the mean score of 9.40 ±2.90 before the dental procedure this difference was statistically significant (p<0.001). There was a statistically significant difference observed in MDAS after the dental procedure and in short STAI before the dental procedure. Conclusion: All children exhibited improvement in their levels of dental anxiety before and after the procedure. Therefore, procedural experience may improve the child's response.
Keywords:
1. Introduction
2. Materials and Methods

| Sl no | Questions |
|---|---|
| 1 | If you had to go to the dentist for checkup tomorrow, how would you feel? |
| 2 | If you were sitting in the waiting room, how would you feel? |
| 3 | If you were about to have a tooth drilled, how would you feel? |
| 4 | If you were about to have your teeth scaled and polished, how would you feel? |
| 5 | If you were about to receive local anaesthetic injection in your gum, how would you feel? |
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aartman IH1, van Everdingen T, Hoogstraten J, Schuurs AH, Aartman IH, Hoogstraten J, Schuurs AH. Self-report measurement of dental anxiety and fear in children: A critical assessment. ASDC J Dent Child. 1998, 65, 252–258. [Google Scholar]
- Appukuttan, DP. Strategies to manage patients with dental anxiety and dental phobia: literature review. ClinCosmetInvestig Dent. 2016, 8, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Chhabra N, Chhabra A, Walia G. Prevalence of dental anxiety and fear among five to ten year old children: a behaviour based cross sectional study. Minerva Stomatol. 2012, 61, 83–89. [Google Scholar]
- Lee CY, Chang YY, Huang ST. Prevalence of dental anxiety among 5- to 8-year-old Taiwanese children. J Public Health Dent. 2007, 67, 36–41. [Google Scholar] [CrossRef]
- Rantavuori K, Lahti S, Hausen H, Seppä L, Kärkkäinen S. Dental fear and oral health and family characteristics of Finnish children. ActaOdontol Scand. 2004, 62, 207–213. [Google Scholar]
- Armfield JM, Slade GD, Spencer AJ. Dental fear and adult oral health in Australia. Community Dent Oral Epidemiol. 2009, 37, 220–230. [Google Scholar] [CrossRef]
- Lockerl D, Liddell A, Dempster L, Shapirol D. Age of onset of dental anxiety. J Dent Res. 1999, 78, 790–796. [Google Scholar] [CrossRef]
- Corah, NL. Development of a dental anxiety scale. J Dent Res. 1969, 48, 596. [Google Scholar] [CrossRef]
- Humphris GM, Morrison T, Lindsay SJ. The Modified Dental Anxiety Scale: validation and United Kingdom norms. Community Dent Health. 1995, 12, 143–150. [Google Scholar]
- Spielberger, CD. Assessment of state and trait anxiety: conceptual and methodological issues. South Psychol. 1985, 2, 6–16. [Google Scholar]
- T. M. Marteau and H. Bekker, “The development of a sixitemshort-form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI),” British Journal of Clinical Psychology,vol. 31, part 3, pp. 301–306, 1992.
- Gustafsson A, Arnrup K, Broberg AG, Bodin L, Berggren U. Child dental fear as measured with the Dental Subscale of the Children’s Fear Survey Schedule: The impact of referral status and type of informant (child versus parent). Community Dent Oral Epidemiol. 2010, 38, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Porritt J, Buchanan H, Hall M, Gilchrist F, Marshman Z. Assessing children’s dental anxiety: A systematic review of current measures. Community Dent Oral Epidemiol. 2013, 41, 130–142. [Google Scholar] [CrossRef]
- Howard KE, Freeman R. Reliability and validity of a faces version of the modified child dental anxiety scale. Int J Paediatr Dent. 2007, 17, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Patel H, Reid C, Wilson K, Girdler NM. Inter-rater agreement between children’s self-reported and parents’ proxy-reported dental anxiety. Br Dent J. 2015, 218, E6–E6. [Google Scholar] [CrossRef]
- Klein U, Manangkil R, DeWitt P. Parents’ ability to assess dental fear in their six-to 10-year-old children. Pediatr Dent. 2015, 37, 436–441. [Google Scholar]
- Humphris GM, Dyer TA, Robinson PG. The modified dental anxiety scale: UK general public population norms in 2008 with further psychometrics and effects of age. BMC Oral Health. 2009, 9, 20.
- Klaassen MA, Veerkamp JS, Aartman IH et al. Stressful situations for toddlers: indications for dental anxiety? ASDC J Dent Child. 2002; 69: 306–309.
- Krikken JB, Veerkamp JS. Child rearing styles, dental anxiety and disruptive behaviour; an exploratory study. Eur Arch Paediatr Dent 2008; 9(Suppl. 1): 23–28.
- Afshar H, BaradaranNakhjavani Y, Mahmoudi-Gharaei J, Paryab M, Zadhoosh S. The effect of parental presence on the 5 year-old children’s anxiety and cooperative behavior in the first and second dental visit. Iran J Pediatr. 2011, 21, 193–200. [Google Scholar]
- Shinohara S, Nomura Y, Shingyouchi K, Takase A, Ide M, Moriyasu K et al. Structural relationship of child behavior and its evaluation during dental treatment. J Oral Sci. 2005, 47, 91–96. [Google Scholar] [CrossRef]
- Yamada MK, Tanabe Y, Sano T, Noda T. Cooperation during dental treatment: the Children’s Fear Survey Schedule in Japanese children. Int J Paediatr Dent. 2002, 12, 404–409. [Google Scholar] [CrossRef]
- Tönnies S, Mehrstedt M, Eisentraut I. Die Dental Anxiety Scale (DAS) und das Dental Fear Survey (DFS) – ZweiMessinstrumentezurErfassung von Zahnbehandlungsängsten. Z Med Psychol. 2002, 11, 63–72. [Google Scholar]
- Kothari S, Gurunathan D. Factors influencing anxiety levels in children undergoing dental treatment in an undergraduate clinic. J Family Med Prim Care. 2019, 8, 2036–2041. [Google Scholar] [CrossRef] [PubMed]
- Shindova MP, Belcheva AB. Dental fear and anxiety in children: a review of the environmental factors. Folia Med (Plovdiv). 2021, 63, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Gao X, Hamzah SH, Yiu CK, McGrath C, King NM. Dental fear and anxiety in children and adolescents: qualitative study using YouTube. J Med Internet Res. 2013, 15, e29. [Google Scholar] [CrossRef] [PubMed]
- Hussein TO, Akşit-Bıçak D. Management of Post-Traumatic Dental Care Anxiety in Pediatric Dental Practice-A Clinical Study. Children (Basel). 2022, 9, 1146. [Google Scholar]
- Saatchi M, Abtahi M, Mohammadi G, Mirdamadi M, Binandeh ES. The prevalence of dental anxiety and fear in patients referred to Isfahan Dental School, Iran. Dent Res J (Isfahan). 2015, 12, 248–253. [Google Scholar]
- Oliveira MMT, Colares V. The relationship between dental anxiety and dental pain in children aged 18 to 59 months: a study in Recife, Pernambuco state, Brazil. Cad SaudePublica 2009, 25, 743–750. [Google Scholar]
- Soares FC, Lima RA, Santos Cda F, de Barros MV, Colares V. Predictors of dental anxiety in Brazilian 5-7years old children. Compr Psychiatry. 2016, 67, 46–53. [Google Scholar] [CrossRef]
- Themessl-Huber M, Freeman R, Humphris G, MacGillivray S, Terzi N. Empirical evidence of the relationship between parental and child dental fear: A structured review and meta-analysis. Int J Paediatr Dent 2010, 20, 83–101. [Google Scholar] [CrossRef]
- Boman UW, Lundgren J, Elfström ML, Berggren U. Common use of a fear survey schedule for assessment of dental fear among children and adults. IntJ Paediatr Dent 2008, 18, 70–76. [Google Scholar] [CrossRef]
- Lee CY, Chang YY, Huang ST. The clinically related predictors of dental fear in Taiwanese children. Int J Paediatr Dent 2008, 18, 415–422. [Google Scholar] [CrossRef]
- Oppenheim MN, Frankl S. A behavioral analysis of the preschool child when introduced to dentistry by the dentist or hygienist. J Dent Child 1971, 38, 317–325. [Google Scholar]
- Rayen R, Muthu MS, Chandrasekhar Rao R, Sivakumar N. Evaluation of physiological and behavioral measures in relation to dental anxiety during sequential dental visits in children. Indian J Dent Res 2006, 17, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Setty JV, Srinivasan I, Radhakrishna S, Melwani AM, Dr MK. Use of an animated emoji scale as a novel tool for anxiety assessment in children. J Dent Anesth Pain Med. 2019, 19, 227–233. [Google Scholar] [CrossRef] [PubMed]
| Mean | Std. Deviation | |||
| Children | Before treatment | 14.54 | 3.82 | t = 5.75 p < 0.001 |
| After treatment | 9.40 | 2.90 | ||
| Parents | Before treatment | 12.84 | 1.50 | t = 10.49 p < 0.001* |
| After treatment | 8.28 | 2.79 | ||
| Mean | Std. Deviation | |||
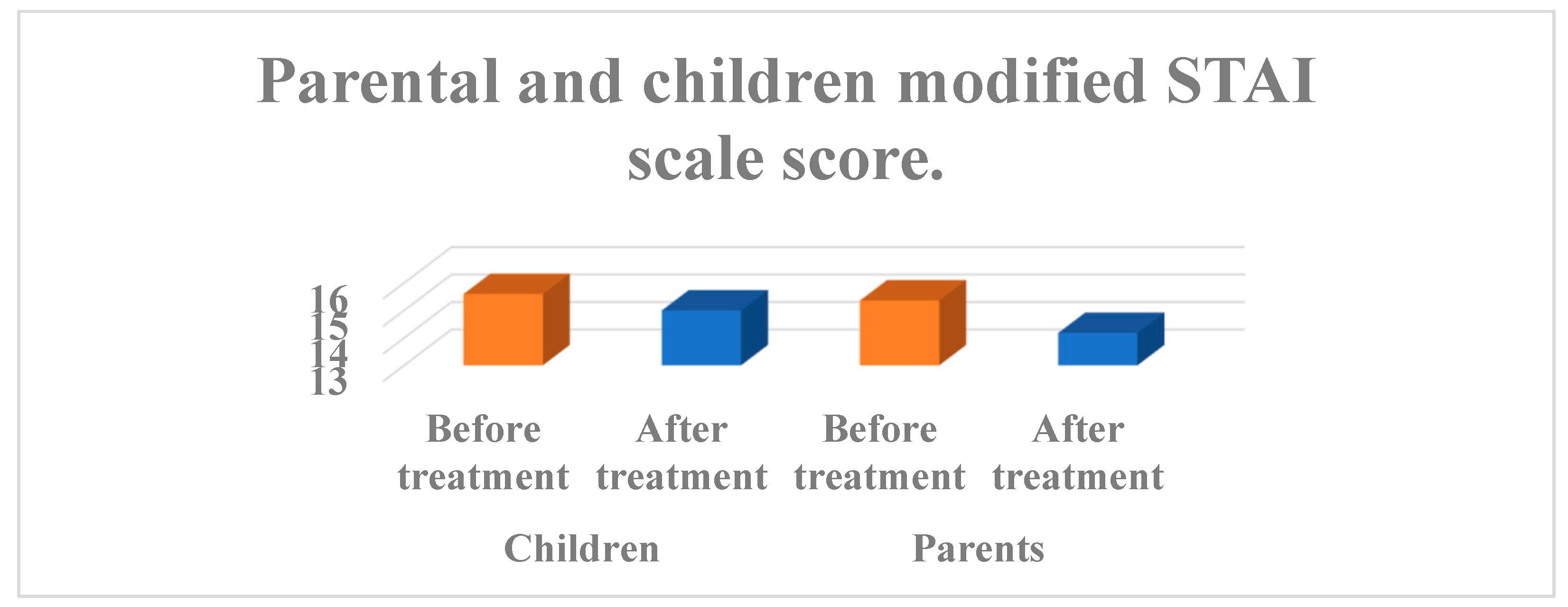
| Children | Before treatment | 15.60 | 1.67 | t = 1.967 p = 0.055 |
| After treatment | 15.00 | 1.10 | ||
| Parents | Before treatment | 15.36 | 1.83 | t = 4.65 p < 0.001* |
| After treatment | 14.18 | 1.45 | ||
| Mean | Std. Deviation | F value | ||
| Education | Up to diploma | 12.61 | 1.82 | 1.963 |
| Bachelors | 12.53 | 1.40 | ||
| Maters | 13.50 | 0.75 | ||
| Socio economic status | Middle class | 12.90 | 1.41 | 1.310 |
| Upper middle | 12.44 | 1.58 | ||
| Upper class | 12.33 | 1.49 | ||
| Before treatment | After treatment | ||
| Modified Dental Anxiety Scale | r | 0.248 | 0.580 |
| Significance | 0.082 | 0.001* | |
| Modified STAI scale | r | 0.424 | 0.231 |
| Significance | 0.002* | 0.107 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



