
Submitted:
17 November 2024
Posted:
19 November 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic disrupted routine child immunization efforts, threatening to reverse progress in controlling vaccine-preventable diseases. We analyzed the impact of COVID-19 on DTP3 vaccination in Europe by comparing trends before and after the pandemic using time series data from 2000 to 2023. Employing Joinpoint regression, chi-square tests, and segmented regression analysis, we assessed DTP3 vaccination trends and coverage changes. The findings revealed significant regional disparities across Europe. Statistical models indicated reductions in DTP3 coverage in countries like Ireland, Sweden, and Switzerland, whereas Ukraine and San Marino showed improvements. These variations indicate the need for targeted public health strategies to address vaccine hesitancy, logistical barriers, and systemic inequities.
Keywords:
DTP3 Vaccination
; COVID-19 Pandemic Impact
; Vaccination Trends
; Vaccine Hesitancy
; Europe
; Childhood Immunization
; Healthcare Disruptions
; Segmented Regression Analysis
; Immunity Debt
; Public Health Systems
; Vaccine Misinformation
; Routine Immunization
; Regional Disparities
; Vaccination Coverage
; Healthcare Access
; JoinPoint Regression
1. Introduction
The pandemic of covid 19 has disrupted DTP3 vaccination in Africa and the Americas[1,2]. The purpose of our study is to highlight its impact in Europe. The COVID-19 pandemic disrupted routine child immunization efforts, resulting in a concerning decline in vaccine uptake. This issue threatens to reverse years of progress in controlling vaccine-preventable diseases[3]. The pandemic greatly strained healthcare systems worldwide, disrupting routine immunization services. This situation was exacerbated by lockdowns, limited access to healthcare facilities, and the redirection of healthcare resources toward COVID-19 response efforts[4]. As a result, childhood immunization rates dropped globally, with some areas facing significant setbacks in vaccine coverage[5,6]. In 2020 alone, it was estimated that 30 million children missed the third dose of diphtheria, tetanus, and pertussis (DTP3) vaccine, and over 27 million missed the first dose of the measles-containing vaccine[7]. Routine immunization, crucial for reducing childhood mortality and morbidity, faced challenges as healthcare systems globally prioritized COVID-19 response measures, impacting other services. The global healthcare landscape has experienced unprecedented disruptions due to the COVID-19 pandemic, profoundly affecting routine immunization programs across many regions[8,9] DTP3 (Diphtheria, Tetanus, and Pertussis) vaccination, a cornerstone of childhood immunization programs, has significantly impacted various parts of the world. DTP3 coverage is crucial to overall immunization program performance and public health system efficacy[10,11]. Countries can maintain herd immunity against these life-threatening diseases by ensuring widespread coverage and preventing outbreaks that could lead to significant morbidity and mortality.
Historically, pandemics and epidemics have disrupted immunization programs by diverting resources and limiting healthcare access. The Ebola crisis, for instance, saw a significant reduction in vaccination coverage, resulting in a rise in preventable diseases, with measles fatalities surpassing those caused by Ebola itself.[12] Similarly, during COVID-19, lockdowns, physical distancing, and reallocating healthcare staff and resources led to declining child vaccination rates in both high- and low-income countries.[12] The concept of “immunity debt” emerged post-pandemic as reduced exposure to pathogens, like pertussis, led to increased population susceptibility[13]. This concept has underscored the critical need for consistent and timely immunization to prevent a resurgence of vaccine-preventable diseases and protect vulnerable populations, especially infants.
Historically, Europe has maintained high levels of DTP3 vaccination coverage through robust healthcare infrastructures and public health initiatives. However, the COVID-19 pandemic disrupted this stability. According to the World Health Organization (WHO), the European Region saw a slight decrease in immunization coverage during the pandemic, dropping from 95% in 2019 to 94% in 2020 for the third dose of the DTP vaccine. While this reduction may appear minimal, it highlights the strain on healthcare systems, with many European countries experiencing logistical challenges, healthcare worker shortages, and movement restrictions during the pandemic[14,15].
Globally, the impact of the pandemic was even more pronounced. The percentage of one-year-olds who received the DTP3 vaccine dropped worldwide. This decrease was from 86% in 2019 to 81% in 2021, though there was a partial recovery to 84% by 2023.[16] Despite this partial recovery, millions of children remained unvaccinated or under-vaccinated, revealing significant gaps in immunization efforts. These disruptions underscored disparities in healthcare access and delivery, which are crucial for understanding the long-term effects of the pandemic on vaccination coverage across regions[17,18,19]
In Europe, there are DTP vaccination programs in 42 countries[20]. This study examines whether the COVID-19 pandemic caused an abrupt decline in DTP3 coverage in Europe and assesses whether vaccination trends have returned to pre-pandemic levels. Specifically, by analyzing data from 2012 to 2023, this study seeks to explore whether the pandemic merely interrupted existing trends or introduced a significant shift in the trajectory of vaccination coverage. In doing so, the study will provide valuable insights into the immediate and sustained effects of the pandemic on routine childhood vaccination programs in Europe. Additionally, understanding variations in coverage across different regions of Europe can highlight disparities in recovery and identify potential areas where vaccine hesitancy or logistical challenges continue to hinder full recovery to pre-pandemic levels.
The pandemic also intensified vaccine hesitancy, partially driven by widespread misinformation on social media platforms. Misinformation and conspiracy theories about COVID-19 vaccines, particularly on platforms like Facebook and YouTube, may have spilled over to attitudes toward other vaccines, including those for children. This online “infodemic” fostered doubt and hesitancy among parents, potentially influencing decisions on routine childhood vaccinations[6].
The COVID-19 pandemic profoundly impacted healthcare systems globally, raising concerns about its immediate effect on routine vaccination programs, including DTP3[21] In addition to potential short-term disruptions caused by overwhelmed health services and logistical challenges, there is growing interest in understanding whether the pandemic influenced long-term vaccination trends[22,23,24,25,26,27] Researching vaccination is essential to understanding and mitigating the impacts of disruptions like those caused by COVID-19; our study on the pandemic’s effect on DTP3 coverage aims to provide insights that can inform recovery strategies and strengthen vaccination systems against future crises[28]. Specifically, we aim to assess if the pandemic caused an abrupt decline in DTP3 coverage and whether it altered or accelerated pre-existing trends in vaccination uptake. By analyzing vaccination data from 2000 to 2023, we seek to identify any significant changes in the trajectory of DTP3 coverage attributable to the pandemic, providing insights into both immediate and sustained effects.
The COVID-19 pandemic presented unprecedented challenges to healthcare systems worldwide. Lockdowns, travel restrictions, and reallocating healthcare resources to pandemic response efforts disrupted routine vaccination services in many countries. Additionally, concerns about contracting COVID-19 at healthcare facilities may have led to vaccine hesitancy among some parents. During the COVID-19 pandemic, skepticism about vaccines in general and the COVID-19 vaccine, in particular, became a[29]. For example, following the COVID-19 pandemic, Hungary experienced a rise in anti-vaccine sentiment[30].
Prior research has shown how the COVID-19 pandemic has affected DTP3 vaccination coverage in different regions. We investigated the effects of the pandemic on DTP3 vaccination trends in Africa[31], revealing disruptions and declines in coverage rates, and examined the impact of COVID-19 on DTP3 vaccination in the Americas, reporting similar trends[32]. These studies highlight the pandemic’s adverse effects on DTP3 vaccination programs in various regions.
In Europe, concerns have been raised about declining routine vaccination rates in children, including DTP3 [24]. The WHO has also reported an “alarming” rise in measles cases in Europe, likely linked to disruptions in vaccination coverage[33]. The results of this study highlight the need for further research into the pandemic’s impact on European vaccination trends and identifying strategies to mitigate negative consequences.
The COVID-19 pandemic may have disrupted routine DTP3 vaccination programs due to logistical challenges such as overwhelmed healthcare systems, movement restrictions, and interruptions in vaccine delivery. [22,23,24,33,34,35,36,37,38,39]While some European countries may have recovered to pre-pandemic vaccination levels, others might still struggle to regain coverage[27] as logistical issues persist, or vaccine hesitancy has increased.
We will compare DTP3 coverage in 2019 and 2023 to explore these potential changes, assessing whether vaccination rates have returned to pre-pandemic levels or remain affected. In some countries, vaccine hesitancy might prevent a full recovery, leaving coverage below pre-pandemic rates, as will be evaluated later using a chi-square analysis.
2. Materials and Methods
Information on vaccination DTP3 rates for European countries was obtained from the United Nations Children’s Fund’s databases, covering 2012 to 2023[40]. We consider European countries included in the United Nations geoscheme for Europe[41]. The analysis excluded several territories that, while geographically located within Europe, possess distinct political statuses not typically associated with independent sovereign nations (Åland Islands, Faroe Islands, Isle of Man, Svalbard and Jan Mayen Islands, Guernsey, Jersey, Sark, Gibraltar). These territories often function as dependencies, crown dependencies, or overseas territories of other European nations, exhibiting varying degrees of autonomy and self-governance. We also excluded the Vatican, the Republic of Kosovo, and Liechtenstein because no data was available. Regional data were also obtained from the UNICEF[40] repository.
2.1. European Regions Analysis
Consolidated data for Europe and West Europe were sourced from UNICEF. Because there were no regional data from North and South Europe in UNICEF, we computed it by weighting national countries’ DTP3 vaccination rates with the number of births. Annual newborn data was collected per country from the World Bank, United Nations, and UNICEF[42,43,44].
The analysis in this study was divided into four European regions. Eastern Europe encompasses Belarus, Bulgaria, Czechia, Hungary, Poland, Moldova, Romania, Slovakia, and Ukraine. The Russian Federation was also included in this group for statistical convenience, although it is a transcontinental country. The same happened with Türkiye. Northern Europe includes Estonia, Ireland, Finland, Sweden, United Kingdom, Latvia, Iceland, Lithuania, Norway and Denmark. Southern Europe contains Albania, Andorra, Bosnia and Herzegovina, Cyprus, Croatia, Greece, Italy, Malta, Montenegro, North Macedonia, Portugal, San Marino, Serbia, Slovenia, and Spain. Lastly, Western Europe includes Austria, Belgium, France, Germany, Luxembourg, Monaco, the Netherlands, and Switzerland.
2.2. Statistical Analysis
We used various statistical techniques to evaluate how the COVID-19 pandemic affected European vaccination trends. First, we used a JoinPoint regression to detect changes in DTP3 vaccination. After that, we computed a chi-square test to compare vaccination coverage in 2019 (pre-pandemic) and 2023 (post-pandemic), examining whether the pandemic caused significant shifts in vaccinated versus unvaccinated proportions. Additionally, we conducted a segmented regression analysis covering the period from 2000 to 2023 to detect changes in long-term vaccination trends, mainly focusing on potential interruptions caused by the pandemic.
The annual percentage change (APC) was computed using Joinpoint regression to quantify the magnitude of variation in DTP3 vaccination trends over time [44]. The Joinpoint regression models assumed constant variance. A Durbin-Watson test was computed to check for autocorrelation in the time series data [54]. If first-order autocorrelation was detected, it was accounted for in the analysis.
Joinpoint regression was utilized to find statistically significant results. JoinPoints, where abrupt changes in vaccination trends occurred, allowed us to pinpoint key moments linked to the pandemic’s impact. We considered that a Joinpoint was close to the pandemic when the joinpoint was located between 2019 and 2021. We must consider that joinpoints have a confidence interval; therefore, joinpoints of 2019 or 2021 could be located in 2020. These methods offer a comprehensive approach, combining hypothesis-driven and exploratory analyses to quantify the pandemic’s effect on vaccination coverage.
To complement the JoinPoint analysis, we compared each country’s DTP3 vaccination coverage between 2019 (the last pre-pandemic year) and 2023 (the most recent year in our dataset). Chi-square tests were employed to assess the statistical significance of any observed differences in coverage rates.
We employed segmented regression analysis to assess how the COVID-19 pandemic impacted DTP3 vaccination trends in Europe from 2000 to 2023. This methodology, also known as interrupted time series analysis, is a robust quasi-experimental approach well-suited for evaluating the effects of external events or interventions on time series data [55,56,57]. Our study period has spanned 23 years, with 20 years pre-pandemic (2000-2019) and three years post-pandemic (2020-2023).
The segmented regression model was defined as follows:
DTP3𝑡 = Intercept + 𝛽1Year + 𝛽2Pandemi c+ 𝜀𝑡
Where:
- “DTP3t” represents the DTP3 vaccination coverage in year t.
- Year is the year of the calendar.
- “Pandemic “is a dummy variable, taking 1 for the Covid-19 pandemic years (2020–2023) and 0 for pre-pandemic years.
The model allows us to estimate the change in the level (immediate effect) of DTP3 vaccination coverage following the onset of the COVID-19 pandemic. Following the initial models that included Year and Pandemic as independent variables, we extended the analysis by testing models incorporating an interaction term between Year and Pandemic to assess whether the effect of time on DTP3 vaccination coverage varied between the pre-pandemic and pandemic periods. The interaction term allows us to capture how the relationship between year and vaccination coverage was modified during the pandemic; for example, the coverage of DTP3 was increasing before and after the pandemic began to decrease.
2.3. Software and Tools
All statistical analyses were conducted using specialized software and programming tools. Joinpoint regression was computed with Joinpoint Trend Analysis Software (Version 5.0.2, May 2023) [45,46]. Vaccination rates between 2019 and 2023 were compared using IBM SPSS Statistics (Version 29, IBM Corp., Armonk, NY, USA). The Durbin-Watson statistic was also computed with IBM SPSS
The segmented regression analysis, a form of interrupted time series analysis, was implemented in the R statistical environment (Version 4.3.1, 2023-06-16 ucrt)[47] utilizing the “segmented” package[47,48,49,50,51]. Data visualization was enhanced with the “ggplot2” package [52], and the “readxl” package facilitated the importation of data from Excel files [53]
3. Results
No joinpoints were explicitly identified in Europe at the beginning of the COVID-19 pandemic (Table 1, Figure 1). There were joinpoints during the pandemic in South and West Europe. Europe exhibited no significant trend changes overall, maintaining a stationary annual percent change (APC) of 0.03%. In contrast, North Europe experienced three joinpoints. Southern and Western Europe had four joinpoints. East Europe had an upward trend with no joinpoint and an APC of 0.11%. (Table 1,). In South Europe and West Europe before the Covid-19 pandemic, the DTP3 coverage had a negative trend. After the pandemic, coverage increased in South Europe and remained static in Western Europe.
Figure 1.
The United Nations Classification of European Regions.
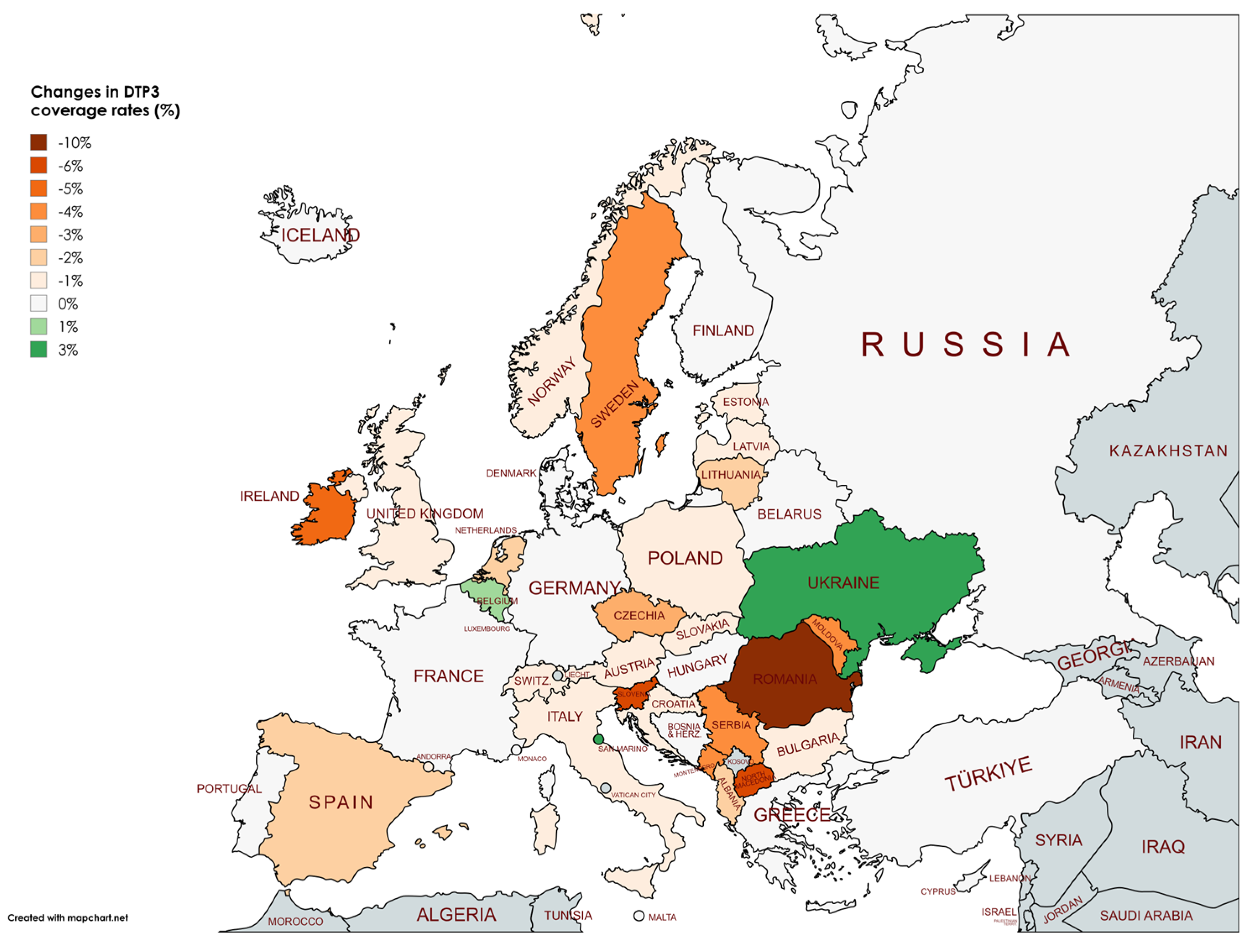
Figure 2.
Joinpoint graph of DTP3 in North Europe, 2000-2022.
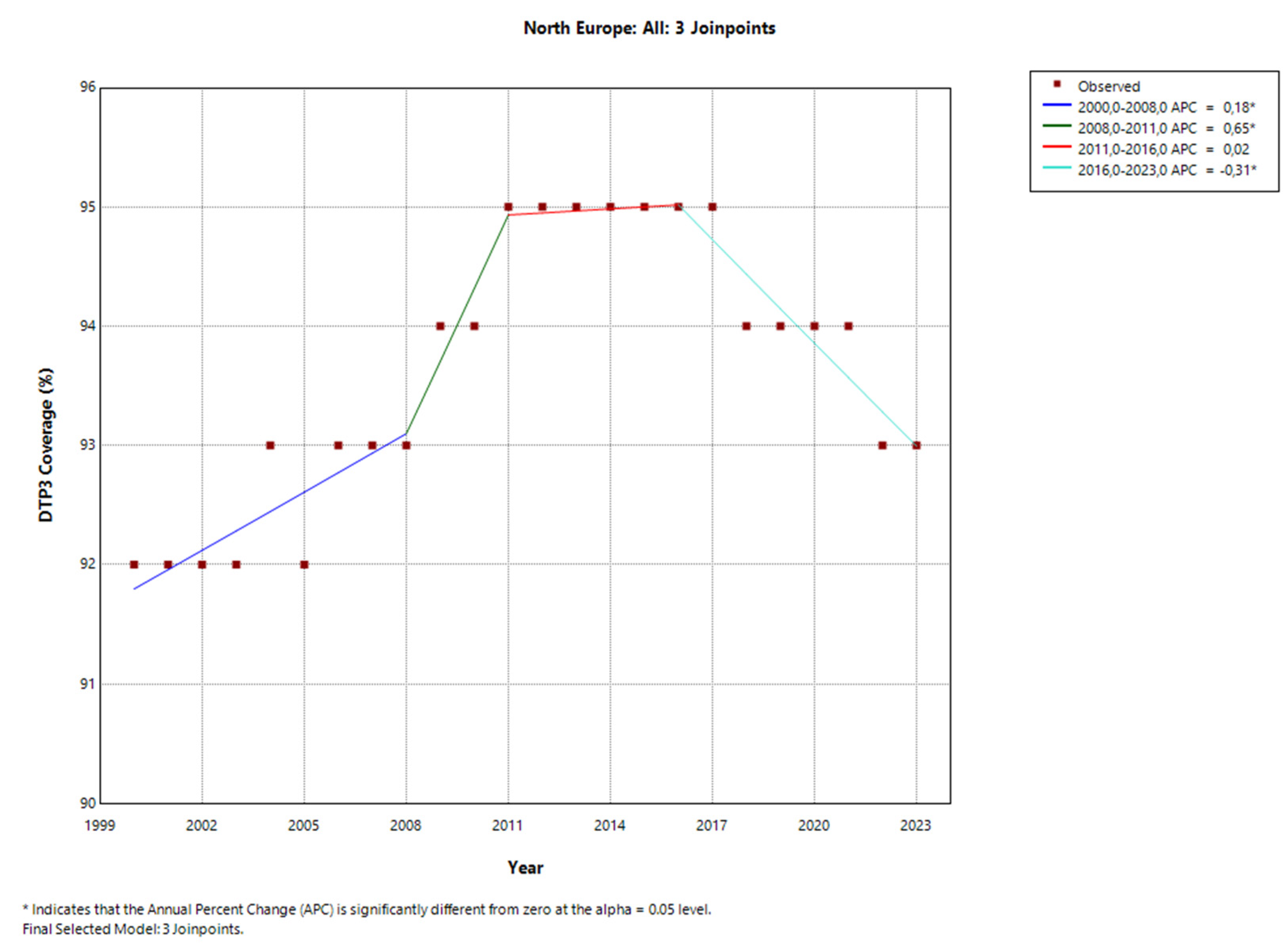
Figure 3.
Joinpoint graph of DTP3 in South Europe, 2000-2022.
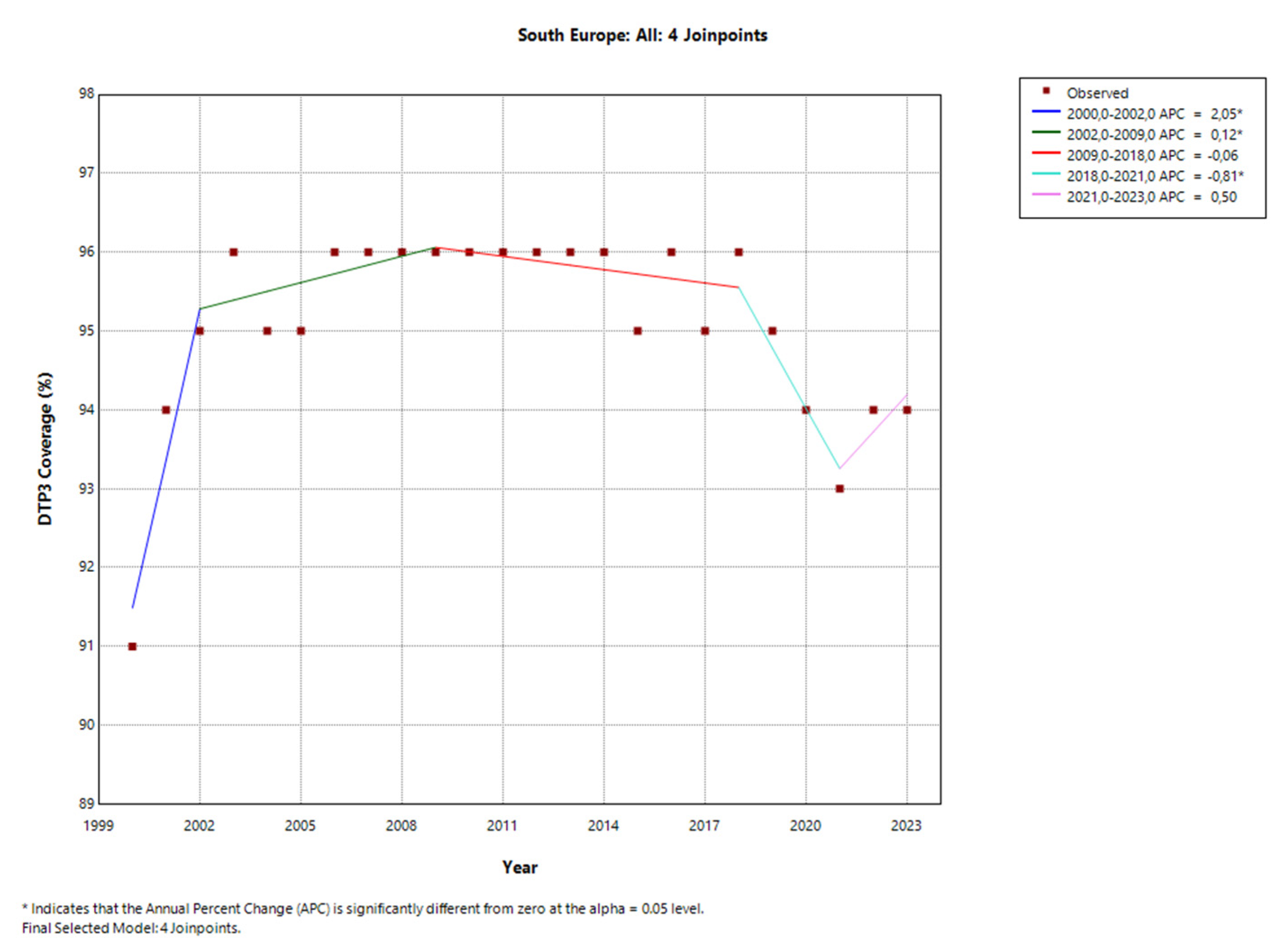
Figure 4.
Joinpoint graph of DTP3 in West Europe, 2000-2022.
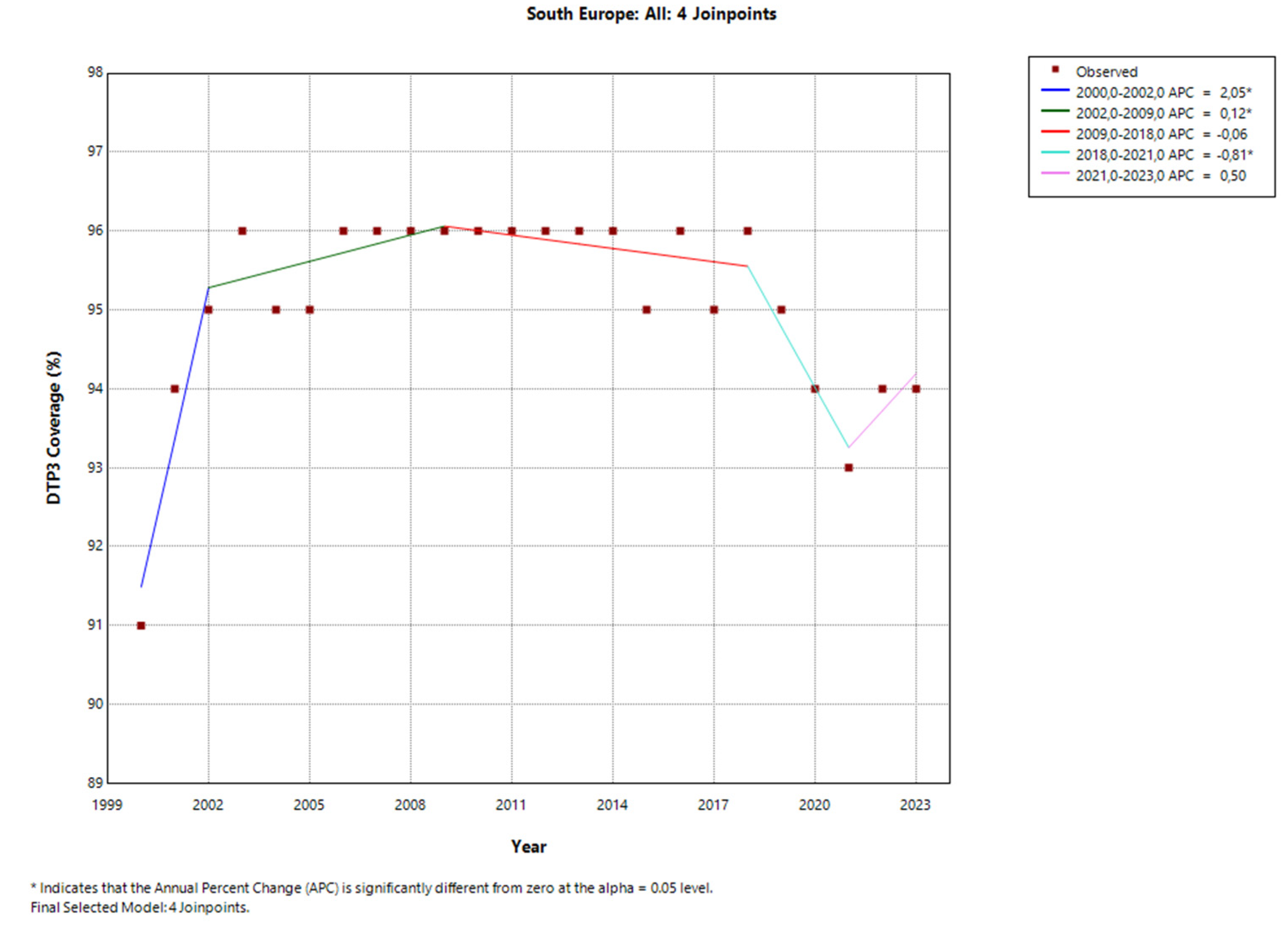
Figure 5.
Joinpoint regression of DTP3 in Europe: (a) Albania (b) Ireland (c) Poland (d) Slovakia (e) Sweden (f) Switzerland.
Figure 5.
Joinpoint regression of DTP3 in Europe: (a) Albania (b) Ireland (c) Poland (d) Slovakia (e) Sweden (f) Switzerland.
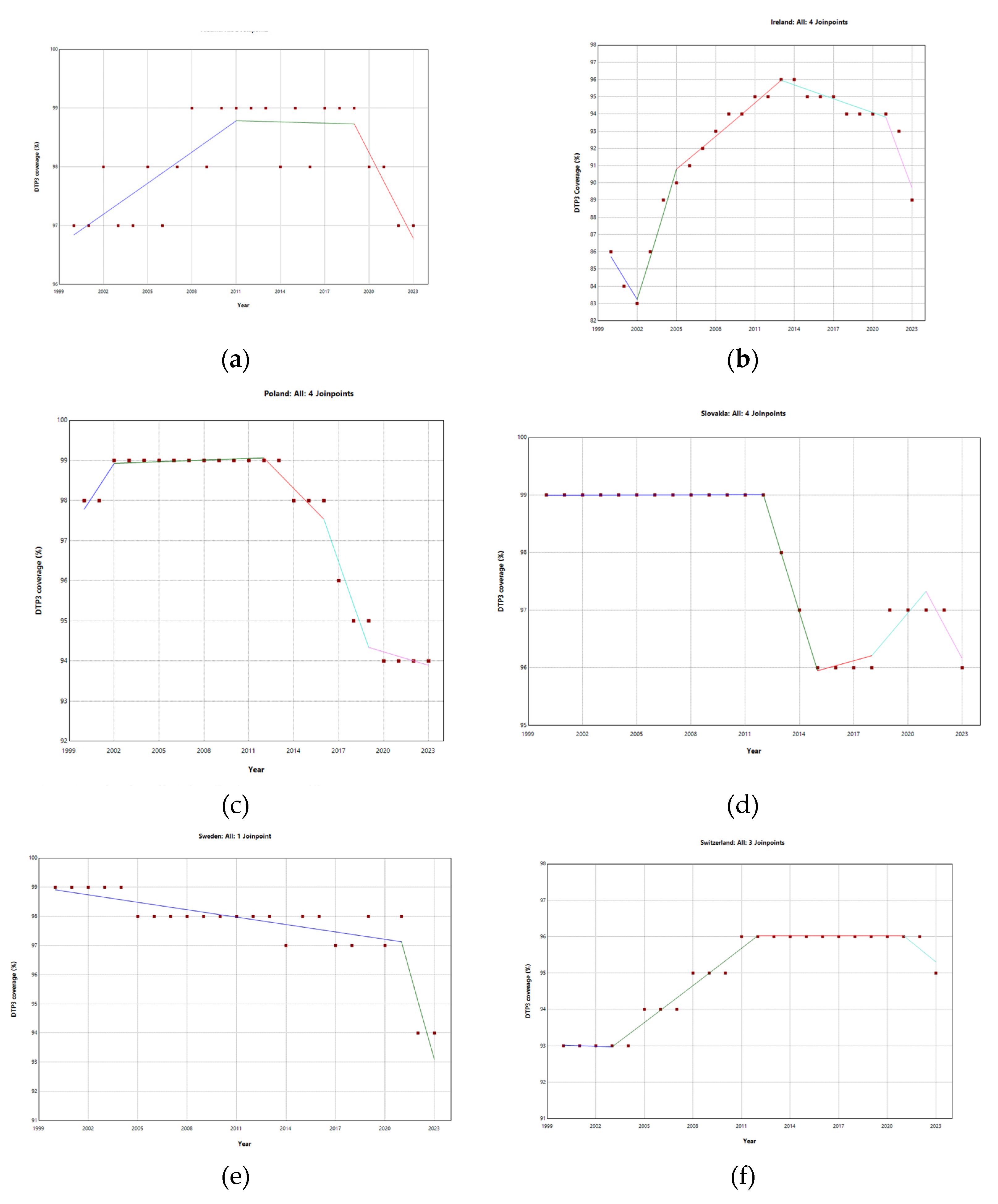
Albania, Ireland, Poland, Slovakia, Sweden, and Switzerland had joinpoints close to the pandemic and presented a negative trend after the pandemic.
In Belgium and Bosnia, where there were joinpoints close to the pandemic, DTP3 grew after the pandemic, with APCs of 0.24% and 3.87%, respectively. (Figure 6)
Table 3 shows the variation in DTP3 coverage rates between 2019 and 2023. Most countries experienced slight decreases, often around 1-2 %, due to the pandemic. The overall trend indicates a slight significative decline in vaccination rates across many European countries (Albania, Austria, Belgium, Bulgaria, Croatia, Czechia, Estonia, Ireland, Italy, Latvia, Lithuania, Montenegro, Netherlands, North Macedonia, Norway, Poland, Republic of Moldavia, Romania, Serbia, Slovakia, Slovenia, Spain, Sweden, Switzerland, Ukraine, United Kingdom). The most significant decrease was observed in Romania, with a drop of 10 percentage points. (Figure 7) Other notable decreases include North Macedonia and Slovenia (-6%), Ireland (-5%), Montenegro, Republic of Moldova, Serbia and Sweden with a -4% decrease.
The outcomes of the segmented regression, which examined the relationship between the pandemic and DTP3 coverage, are shown in Table 4. In Europe, the pandemic caused a minimal decrease in vaccination coverage that was not statistically significant (Figure 8). There was a decrease in coverage in Northen (-2.2%), Southern (-2.6%) and Western Europe. (-1.8%) (Figure 9).
Table 5 shows the parameters of the segmented regression and includes a column showing the interaction when it exists.
There were five countries where vaccination coverage increased slightly and significantly during the pandemic.: Germany, Russian Federation, San Marino, Iceland, Slovakia and Ukraine. The biggest increase took place in Ukraine (45.32%) and San Marino (4.92%) (Figure 10)
Segmented regressions show that the pandemic had an immediate negative effect on DTP3 vaccination coverage in Albania(-1.6%), Austria (-6.8%), Cyprus (-1.6%), Estonia (-0.9%), Ireland(-3.2%), Lithuania (-1.3%), Montenegro(-3.6), North Macedonia (-8.5%), Poland(-1.3%), Republic of Moldova (-1.9%), Slovenia(-3%), Spain(-2.4), Sweden(-1.3%), Switzerland (-1%), Türkiye (-1.8%) and the United Kingdom (-2.4%). (Table 5) (Figure 11 and Figure 12) In addition, there were negative interactions between the year and the pandemic in Ireland (-1.8%), Sweden (-1.2%) and Switzerland(-0.4%). This means that, for example, in the case of Switzerland, where the vaccination coverage was practically stagnant with an annual growth of 0.17%, there is a decrease in vaccination coverage of 3.2% in the year of the Pandemic and a negative trend begins with a decrease of 1.8% per year. In these three countries, Ireland, Sweden, and Switzerland, the pandemic has changed the trend, with a progressive reduction in DTP3 vaccination coverage.
4. Discussion
The COVID-19 pandemic caused disruptions to routine childhood vaccination programs. These disruptions included postponements, altered schedules, and, in some cases, complete suspensions of vaccination services[57,58,59]. Although the three statistical methods used identify the same countries, their interpretation differs. Segmented regression indicates if covid has an immediate effect, the comparison of rates between 2019 and 2023 indicates if the pandemic has an intermediate effect on rates or if the vaccine coverage recovered, while JoinPoint indicates if there was a change in the trend of the coverage in a certain point. In our opinion, combining the three methodologies increases the sensitivity and the ability to detect the impact of the pandemic.
4.1. Limitations
Our study has some limitations that should be acknowledged. Firstly, the reliance on publicly available data from organizations such as UNICEF and the World Bank might introduce limitations related to data completeness and accuracy, especially in the case of underreporting or data collection challenges during the pandemic due to resource constraints and reporting lags, especially in European low- and middle-income countries, such as some countries in the east or the south of Europe can further reduce the completeness of data[60,61] Routine immunization coverage is often measured using administrative data, which relies on registry information of administered doses. However, this method can have biases and inaccuracies, mainly if doses administered outside standard healthcare settings are not recorded consistently[13]. However, in Bosnia and Herzegovina, patient file data corroborates the official administrative data, showing consistent vaccination coverage levels, particularly for BCG, DTP, and MMR (measles, mumps, and rubella) vaccines, suggesting that the data for this region may be more reliable despite the challenges mentioned[62].
Although excluding certain European territories such as the Vatican, Liechtenstein, and other small countries or territories might initially seem to affect the overall results, their small size and unique characteristics mean they do not significantly influence the broader picture of vaccination coverage in Europe.
Another limitation is the use of country regional data, which may mask within-country variations in the impact of the pandemic, particularly in areas with lower healthcare service coverage or among ethnic groups that may reject vaccination or are difficult to reach due to their movement across borders[63,64] This is especially relevant in regions with diverse healthcare systems like Eastern Europe.
The study’s time, which focuses heavily on pre-pandemic trends, might not fully capture the long-term effects of the pandemic on vaccination rates as recovery continues to evolve, so we need to do follow-up studies to know the long-term effects of the pandemic.
Lastly, our statistical analysis does not consider the influence of confounding factors, such as concurrent public health interventions or political and economic changes during the pandemic, which may not have been fully accounted for, limiting the interpretation of direct pandemic-related effects.
4.2. Country by Country Analysis
A study investigating vaccine hesitancy across various regions in the European Union found that higher levels of aggregate vaccine hesitancy were significantly associated with lower immunization rates, particularly for childhood vaccines like DTP3. This analysis utilized data from the 2019 Eurobarometer survey on vaccine hesitancy and linked it to regional immunization coverage reported by the WHO. The findings suggest that regional differences in vaccination uptake are at least partially attributable to varying public attitudes toward vaccination[65]. The analysis of DTP3 vaccination trends during the COVID-19 pandemic across Europe reveals significant country-specific impacts shaped by unique sociopolitical, economic, and healthcare-related factors. Each country faced distinct challenges and exhibited various trends regarding vaccine uptake, influenced by historical hesitancy levels, the diversion of healthcare resources, public attitudes, and systemic responses to the pandemic. From Albania’s socioeconomic barriers and Austria’s pre-existing hesitancy to Cyprus’s education-linked confidence in vaccination and Serbia’s heightened skepticism fueled by misinformation, the spectrum of experiences underscores the complexity of maintaining routine immunizations during a global health crisis. Despite high immunization rates in some countries, such as Norway, regional or demographic pockets with low coverage present ongoing risks. Understanding these complex trends is essential for tailoring interventions to each context as countries continue working to restore and strengthen immunization programs in the post-pandemic era.
4.1.1. Albania
Albania experienced a significant impact on DTP3 vaccination coverage due to the pandemic; however, even prior to this, there was already a downward trend in vaccination rates. Despite universal health insurance and increasing healthcare expenditures, childhood immunization coverage declined, even though these services remain free of charge[66,67]. Low coverage was associated with socioeconomic and geographic factors [68], safety concerns, and unreliable information sources. Although vaccine hesitancy is low[69,70], mothers who rely on the internet or social media for health information are less likely to follow vaccination schedules[68]. Although nurses favor vaccination in Albania, more than 20% gave credence to hoaxes such as the association with autism or multiple sclerosis[71].
4.1.2. Austria
In Austria, low vaccine coverage has been limited to DTP3 and measles, making Austria second only to Romania in the number of reported measles cases[72]. The decrease in DTP3 vaccination coverage in Austria during the COVID-19 pandemic may be attributed to several factors related to vaccine hesitancy, which had already been observed before the pandemic. Studies have indicated that vaccine hesitancy and skepticism were significant in Austria, with a considerable proportion of the population expressing concerns about vaccine safety, particularly the fear of side effects[73]. In addition, this hesitancy contributed to a lack of sufficient health literacy and awareness about the importance of routine vaccinations and limited social marketing and promotion efforts to encourage vaccination. Furthermore, many parents in Austria became more hesitant after the pandemic [74]. The pandemic likely exacerbated these issues by straining healthcare systems and diverting attention from routine immunizations to COVID-19-related care.
4.1.3. Belgium
Although the only child compulsory vaccine in Belgium is the vaccine of Poliomyelitis[75,76], Belgium showed an increase in DTP3 coverage had implemented a pediatric vaccination program, recommended by the Superior Health Council, covering various childhood diseases with immunization coverage rates above 90%, overseen by regional authorities in Flanders, Wallonia, and Brussels[77] One explanation of this high coverage is that high vaccination coverage rates are positively influenced by urbanization, as seen in countries like Belgium, Israel, Japan, and Luxembourg, where over 90% of the population resides in urban areas[78,79].
4.1.4. Bosnia and Herzegovina
Gavi, the Vaccine Alliance, is a global organization that helps low- and middle-income countries increase access to life-saving vaccines by providing financial and technical support. Bosnia and Herzegovina transitioned from Gavi support in 2011, but this period saw instability in vaccination coverage[80]. The fluctuations in Bosnia’s vaccination coverage were attributed to several factors, including growing vaccine hesitancy, misinformation spread through social media, and challenges within the health system, such as a shortage of healthcare workers. This instability contributed to an outbreak of pertussis in 2018, during which Bosnia experienced many pertussis cases among unvaccinated children. Thanks to vaccination programs, the number of pertussis cases has been reduced from 93 cases in 2018 to 1 in 2021[66]. This data is consistent with the increase in DTP3 coverage that we detected in Bosnia.
4.1.5. Bulgaria
In our study, we detected that during the period from 2019 to 2023, Bulgaria experienced a significant decline in DTP3 (Diphtheria, Tetanus, and Pertussis) vaccination coverage, mirroring a broader trend observed in several European countries. This decline could be attributed to multiple factors, including the diversion of healthcare resources during the COVID-19 pandemic, the affluence of refugees[81], and a rise in vaccine hesitancy fueled by misinformation and low vaccine confidence [82]. The pandemic exacerbated existing challenges in Bulgaria’s immunization programs, particularly in underserved communities, where vaccination uptake was already vulnerable. A large-scale study across eighteen European countries before the pandemic found that Bulgaria and Poland had low vaccine confidence [83]. The resulting decrease in DTP3 coverage raises concerns about potential outbreaks of vaccine-preventable diseases and underscores the need for targeted public health interventions to rebuild trust in vaccines and restore routine immunization coverage[84].
4.1.6. Croatia
In Croatia, vaccine-hesitant individuals have reportedly employed tactics to bypass vaccination mandates, including falsifying vaccination records, using alternative substances, and bribing medical personnel[85]. Such behaviors were noted even before the COVID-19 pandemic, especially among parents resisting required childhood vaccinations. A qualitative research Croatian study highlighted similar strategies, such as altering medical documents, visiting a private physician, or offering bribes to pediatricians to evade compulsory vaccination requirements[86]. These challenges underscore the need for multidisciplinary strategies grounded in behavioral science to create more effective vaccination interventions[87]. Studies have observed that higher-education parents have good skills for assessing health information in Croatia, but these skills are lacking in the general population[88].
4.1.7. Cyprus
Our results on Cyprus agree with a study conducted in Cyprus during the COVID-19 pandemic that found that a significant proportion of mothers (57%) reported delaying their children’s vaccinations despite holding a generally positive view of vaccines. Mothers’ knowledge about vaccines varied, with only 13.6% achieving high accuracy in their responses, and knowledge levels were positively associated with higher education and income. A European study performed in 18 countries examined vaccine confidence among parents and found that confidence was notably highest in Portugal and Cyprus, with 78% of Cypriot parents having no hesitation about vaccines[83]. An article highlighted significant COVID-19 vaccine hesitancy among healthcare professionals in Cyprus, especially nurses and midwives[89]. This reluctance toward the COVID-19 vaccine could have contributed to a broader hesitancy toward other vaccines within this group.
Nevertheless, another study showed that in Cyprus, maternal attitudes toward childhood vaccination during the COVID-19 pandemic remained largely positive, with most mothers expressing confidence in vaccine safety, efficacy, and the protection vaccines provide against severe diseases. However, socio-demographic factors influenced these attitudes, with single mothers, those with secondary education, and lower-income households displaying comparatively less favorable views on vaccination[90]. These differences suggest that targeted public health efforts addressing specific socio-demographic barriers may be beneficial. Tailored interventions could enhance vaccine trust and ensure continued support for post-pandemic childhood immunization programs.
4.1.8. Czech Republic
Czechia’s healthcare operates on a mandatory health insurance system; childhood immunization is also compulsory. No vaccination can result in financial penalties and may even affect a child’s ability to attend preschool [91]. Despite high vaccination coverage, the Czech Republic has experienced occasional localized mumps outbreaks due to secondary vaccine failure [92]. Vaccine hesitancy is a notable public sentiment in the Czech Republic[30]. Although we lack specific data on vaccine hesitancy in Czechia, a study on the COVID-19 vaccine revealed that 70.2% of pregnant and lactating women showed a high level of vaccine acceptance[93].
4.1.9. Estonia
In Estonia, adopting a pay-for-performance system for family doctors has significantly improved vaccine coverage rates, as financial incentives encourage higher levels of childhood immunizations, such as the DTP3 vaccine. Factors such as some family doctors not participating in the pay-for-performance quality system reduce vaccine coverage in Estonia[94].
4.1.10. Ireland
Despite high overall self-reported uptake of childhood vaccinations in Ireland, the third dose of diphtheria, tetanus, and pertussis vaccine (DTP3) remains below World Health Organization targets due to vaccine hesitancy. Vaccine hesitancy among parents in Ireland is between 14 and 22%[95]. However, these figures could be even higher because another study found that 26% of respondents in Ireland were hesitant to receive a COVID-19 vaccine, and 9% were resistant.[96] Another study found that slightly over 30% of respondents indicated a possibility of vaccinating their child, while close to 18% stated they would not vaccinate their child[97]. Nevertheless, National surveys indicate parental solid support for vaccinations, yet concerns about vaccine safety and side effects are the most common reasons for missed DTP3 vaccinations. Trust in official vaccine information sources predicts vaccine acceptance; increased trust correlates with higher uptake[98,99,100]. Enhancing parental trust in healthcare professionals and public health authorities and addressing safety concerns are crucial strategies for improving DTP3 vaccination rates and achieving target coverage levels in Ireland.
4.1.11. Italy
Italy implemented a mandatory vaccination policy for school admission in 2017 [91]. In Italy, vaccination coverage for mandatory vaccines decreased in 2020 compared to 2019, with declines ranging from 1% to 2.7%. However, coverage for the chickenpox vaccine increased by 2.2% among 7-year-old children during the same periodRecommended vaccinations were moderately affected, with decreases between 1.4% and 8.5%, except for the Human papillomavirus vaccine (HPV) in males, the meningococcal conjugate vaccine against serogroups A, C, W, and Y (MenACWY), and rotavirus vaccination, which saw increases of 1.8%, 4.7%, and 9.4%, respectively. [101]. A study found that during the pandemic, 44% of parents have had children’s healthcare appointments delayed (29%) or canceled (15%)[102]. In Italy, problems have been like those in Croatia, such as vaccine-hesitant individuals bribing medical personnel[103]. The recent pertussis outbreak in Italy (January 2024) underscores the urgent need for enhanced maternal immunization, timely infant vaccinations, and post-exposure prophylaxis to protect vulnerable neonates and reduce severe complications and mortality[104]. There is also the problem of vaccine hesitancy. Research conducted in Italy suggests a strong link between anti-vaccination beliefs and a distrust of science[105]. Additionally, the study indicates that having unrealistic expectations of science can indirectly influence a person’s stance on vaccination.
4.1.12. Latvia
4.1.13. Lithuania
In Lithuania, one study found that 35.0% of parents did not vaccinate their children. Among the reasons for no vaccination was the cost of paid vaccinations, with 29.3% of parents saying it was too high[109]. Another study found that among vaccine-hesitant parents, information received from healthcare personnel during consultation has a higher impact on their opinion[110].
4.1.14. Moldova
Moldova faces challenges with vaccine hesitancy due to anti-vaccination campaigns and a lack of trust in the healthcare system, particularly regarding vaccine quality. This has led some parents to resist immunization mandates, and reports of falsified documents are being used to circumvent school entry requirements. Additionally, physicians are concerned about their legal protection should children experience adverse events following vaccination, whether real or perceived[111].
4.1.15. Montenegro
A study examining the impact of online media on parental attitudes towards childhood vaccination in Montenegro, Serbia, and Bosnia and Herzegovina revealed that specific parent demographics were more susceptible to online influence. These included women, younger parents (millennials), parents in common-law relationships, and those with larger families[112].
4.1.16. Netherlands
There has been an increase in parents with negative attitudes toward vaccination in the Netherlands. Some parents are reluctant to vaccinate their children, characterized by unfavorable attitudes toward immunization, skepticism about vaccine effectiveness, safety, potential side effects, preference for natural infection over-vaccination, and diminished trust in the National Immunization Program[113]. Despite high national vaccination rates, significant clusters of low vaccine coverage persist within specific school communities in the Netherlands. Notably, Orthodox Protestant and Anthroposophic schools exhibit substantially lower vaccination rates, dropping coverage to between 58% and 78% in these institutions[114]. The COVID-19 pandemic notably impacted vaccine-preventable diseases (VPDs) and vaccination rates in the Netherlands. Implementing measures such as social distancing and school closures significantly reduced the incidence of multiple VPDs by approximately 75–97%.
Additionally, the routine administration of vaccines experienced delays for children scheduled between March and September 2020, resulting in an initial decrease in vaccination participation by 6–14% compared to the previous year. Despite these delays, vaccination rates quickly rebounded through catch-up efforts, ultimately maintaining coverage levels with a slight decline of 1–2%. While COVID-19 response strategies effectively lowered the spread of VPDs, the disruption to the infant vaccination schedule was minimal and addressed mainly through subsequent vaccination initiatives[115].
4.1.17. North Macedonia
For years, the Republic of North Macedonia has had a successful immunization system in the country, confirmed by the high population coverage with mandatory vaccines and the evident results regarding eliminating and eradicating infectious diseases, but there has been stagnation in the population coverage ia with mandatory vaccines[116]. Negative trends initially emerged due to campaigns led by the anti-vaccine lobby. Later, these issues were compounded by the inconsistent enforcement of mandatory vaccination policies—which effectively became voluntary—and the absence of expected responses from relevant state agencies[116]. In North Macedonia, during the pandemic, there was a decrease in children’s coverage of the influenza vaccine. Data from the 2021/2022 influenza season indicate a substantial decline in vaccination coverage among children aged 6 months to 5 years, decreasing by 87.9% compared to 2020/2021[117]. Furthermore, fewer than 85% or 80% of specific vaccines in certain territories are worrying [116].
4.1.18. Norway
Even though the coronavirus pandemic has been very demanding on resources. According to the Folkehelseinstituttet, Norway had the same high global vaccination coverage as in previous years. This statement disagrees with our findings[118]. Norway’s children’s vaccination program has high and stable vaccine support [118]. In one study made in Australia, the USA, Norway, and the UK, Norway was where the population trusted more in the health authorities. This trust could also influence vaccinations[119]. Another study conducted in the UK, Australia, and Norway found that Norway had the lowest vaccine hesitancy concerning the COVID-19 vaccine[120]. Although vaccine coverage is high in Norway, it is lower among certain groups of immigrants. Children of parents from Somalia, Poland, and Lithuania have lower coverage of MMR, and those from East Europe have lower coverage of DTP and other vaccines than the national average[121,122,123].
4.1.19. Poland
In Poland, the healthcare system is built around compulsory insurance, yet a substantial portion of funding comes from private, primarily out-of-pocket, expenses. While certain vaccinations are required by law, others are merely suggested[124]. Poland, historically known for high childhood vaccination rates due to mandatory immunization laws from the communist era, is experiencing a concerning decline in vaccine uptake. Polish citizens have expressed significant concerns and doubts about the safety and efficacy of vaccines[30]. Increasing vaccine hesitancy has led more parents to refuse or delay mandatory vaccines despite potential fines and legal requirements enforced by family doctors[125]. The growing mistrust in authorities and minorities challenging vaccination laws contributes to this decline, putting public health at risk by potentially falling below essential immunity levels. Another study with Ukrainian economic migrants identified the main barriers experienced in accessing and utilizing Polish vaccination services. Two main barriers to vaccination were identified: challenges related to resources and those unrelated to resources (such as mismatched vaccine schedules, instances of discrimination, the optional status of the HPV vaccine, and a general lack of trust). The lack of sufficient resources, such as the lack of interpreters and healthcare resources, and the unresponsiveness and passivity of the system all contributed to the problem[126]. Regarding the price of vaccines, Ukrainian migrants clearly distinguished between mandatory and “optional.” The optional vaccines were considered less important[126].
4.1.20. Romania
A study in Romania found that 47.8% of postpartum mothers were vaccine hesitant. [127] Another study showed that Pertussis vaccine acceptancy (VA) dropped from 85% in 2019 to 44.4% in 2022[128]. In the case of MMR, Romania has a decreasing trend accelerated by the pandemic[129]. In another study in Romania, vaccine hesitancy was prevalent and negatively affected vaccination rates for infectious diseases, including Invasive Meningitis Diseases (IMD) [30].
4.1.21. Serbia
Under the Law on Population Protection from Communicable Diseases, vaccination against diphtheria, tetanus, and pertussis is required in Serbia[130]. Analysis of immunization trends in Serbia has revealed a significant decline in DTP and DTP3 vaccination coverage between 2000 and 2017 [130]. The evolution of DTP3 vaccination rates in children across the past two decades has likely been influenced by fluctuating levels of vaccine hesitancy among parents, a trend also observed in other European contexts[130,131]. Research indicates that parental attitudes toward vaccines play a significant role in immunization rates, with regions showing higher hesitancy correlating with lower uptake rates for childhood vaccines, such as DTP3. In Serbia, as in other countries, societal attitudes toward vaccination may have been further impacted by the global COVID-19 pandemic, which affected public trust in health interventions. This context underscores the importance of addressing vaccine hesitancy among parents to sustain and improve immunization coverage among children[131]. Serbia experienced measles outbreaks between 2015 and 2019, with a significant number of cases occurring in 2018., In 2018, the number of measles cases in Serbia tripled, making it the second highest in Europe after Ukraine[131]. Most cases involved unvaccinated children younger than five due to decreased MMR vaccination coverage below the recommended threshold[132]. During the pandemic, there was a decline in MMR coverage rates in Serbia, underscoring the pandemic’s broader impact on routine childhood vaccinations, paralleling trends seen with other essential vaccines like DTP3[133]. These disruptions emphasize the critical need for catch-up strategies to restore coverage levels and safeguard against preventable disease outbreaks.
During the COVID-19 pandemic, skepticism about vaccines in general and the COVID-19 vaccine became widespread in Serbia[29]. Public opposition to vaccination was observed in Serbia[30].
A growing public health challenge is posed by people becoming increasingly skeptical of the efficacy and safety of vaccines. A study in Serbia found that vaccine hesitancy and refusal are growing concerns[131]. This hesitancy is linked to distrust of medical science and institutions and a belief in conspiracy theories. The authors suggest that the abundance of misinformation on social media and the internet and distrust in official institutions contribute to this problem. Parents who endorse anti-vaccine conspiracy theories show a lower intention to vaccinate their children. The impact of vaccine refusal and the spread of misinformation can have harmful, even deadly, consequences[29].
A study in Serbia found that pediatricians play a key role in parents’ decisions to vaccinate their children with the MMR vaccine[134]. Other factors associated with higher MMR vaccination rates included having two children, previous vaccination of the child, and a higher parental vaccination knowledge score. Also, Research on HPV vaccination in Serbia demonstrated that a recommendation from a pediatrician was the strongest motivator for parents to vaccinate their children[135]. Most parents rely on pediatricians as their primary source of immunization information, highlighting the importance of pediatricians’ knowledge and attitudes toward vaccines in shaping parental decisions.
4.1.22. Slovenia
In Slovenia, vaccine hesitancy has been a factor in lower immunization rates against IMD[30]. A study involving nursing students in Slovenia, Poland, and Serbia highlighted the influence of healthcare professionals’ attitudes on public vaccination decisions. Factors such as perceived vaccine benefits, trust in institutions, and vaccine effectiveness significantly impacted students’ intentions to vaccinate and advise others to do so. The study found that greater trust in institutions and healthcare providers was associated with increased vaccination willingness[136].
4.1.23. Spain
The COVID-19 pandemic significantly disrupted pediatric vaccination coverage in Spain, impacting the continuity of immunization schedules, particularly during the early stages of lockdown when healthcare services were suspended. Confinement measures, closure of health facilities, and public fear of SARS-CoV-2 transmission contributed to reduced access to vaccination, mainly affecting children under two years of age. The COVID-19 pandemic has significantly impacted child vaccination coverage in Spain, affecting routine immunizations and campaigns. The shift to telemedicine, fear of infection, and restrictions on physical attendance at health centers reduced vaccination rates, with declines between 5% and 60% across regions, varying by age and vaccine type. [137] While essential vaccines like DTaP (diphtheria, tetanus, and acellular pertussis) in children under 15 months were somewhat maintained, declines included an 8-13% drop for primary doses at 2 and 4 months, 15% for 11-month boosters, 12% for MMR and meningococcal ACWY at 12 months, and 20% for varicella at 15 months. Unfunded vaccines saw the steepest drops, with meningococcal B down by 68.4% in April in Valencia and 39% in total doses in Andalusia. Vaccination for pregnant women remained largely unaffected[137]. School-based immunizations were suspended, and only certain critical vaccines, like DTP3 for pregnant women, were prioritized[137]. Although vaccination rates for infants recovered after initial disruptions, coverage for booster vaccines lagged, with MMR coverage notably falling below the threshold required to prevent measles outbreaks. In response, Spanish health authorities issued urgent recommendations to prioritize essential vaccinations, but regional disparities persisted in vaccination rates[138]. In Catalonia (Spain), vaccination coverage for DTP3 and other routine childhood vaccines decreased despite efforts to maintain essential immunization services. During the lockdown, healthcare services focused on vaccinating children under 15 months and vulnerable populations, but logistical challenges and restrictions hindered access for many. While some vaccines, like the PCV13, recovered, others, including DTP3, remained below pre-pandemic levels, highlighting the pandemic’s disruptive effect on vaccine coverage.
Our study detected decreased DTP3 coverage in Spain, but some regional studies describe increases. Contrary to what might be thought in Central Catalonia, Spain, the COVID-19 pandemic increased overall influenza vaccination, reducing the usual discrepancy between native and immigrant child vaccination rates[139]. In the same way, a study performed in Cantabria (Spain) showed that contrary to expectations, the COVID-19 pandemic did not significantly affect routine childhood vaccination rates, as these remained stable between the pre-pandemic and pandemic cohorts[140]. However, a substantial increase was observed in non-routine vaccinations, with mothers being three times more likely to opt for these additional vaccines during the pandemic period[140].
Another problem is vaccine hesitancy. A study in Spain on COVID-19 vaccine hesitancy found that it was influenced by concerns over vaccine safety, distrust in its expedited development, and perceived experimental nature. The hesitant commonly believed that vaccines were financially motivated or ineffective. Demographic factors such as younger age groups (mainly 18-40 years) showed lower uptake, partly due to structural issues and distrust in healthcare information sources, particularly among those relying on social media for information[141]. Another factor was believing or using alternative therapies[142]. High trust in Spain’s healthcare system, a culture supportive of vaccination, and universal healthcare access likely contributed to the overall success of vaccination campaigns[141]. Maternal education, employment, and income influenced vaccination choices, particularly for non-routine vaccines, which were more frequently chosen by higher-income and educated mothers[140].
4.1.24. Sweden
The COVID-19 pandemic influenced child immunization rates in Sweden, with various factors impacting vaccine uptake. Firstly, lockdowns and reallocating healthcare resources disrupted routine immunization services, leading to delays in childhood vaccinations. There was also increased vaccine hesitancy, partly fueled by misinformation and fears related to COVID-19 vaccines, which may have impacted overall trust in immunization programs. Like other European countries, DTP3 coverage faced setbacks in Sweden, impacting pertussis immunity. Additionally, post-pandemic immunity debt, resulting from reduced pathogen exposure, has been associated with increased susceptibility to diseases like pertussis, underscoring the importance of maintaining high immunization coverage to protect against resurgence in vaccine-preventable diseases.
4.1.25. Switzerland
A study on Swiss childhood vaccination from 2012 to 2021 highlights critical factors affecting vaccination rates, particularly the impact of the COVID-19 pandemic and regional variations. Despite high initial coverage, booster doses are often missed or delayed, resulting in an overall coverage below the Swiss Federal Office of Public Health target of 95%. The significant regional differences, with lower coverage in German-speaking and rural areas, are possibly due to varying vaccine hesitancy and logistical barriers [143]. Another study found that most Swiss parents intend to vaccinate their children more frequently, especially in Latin Switzerland, which was more affected by the pandemic than the German-speaking regions[144]. Amendments to the vaccination schedule in 2019, switching to a 2+1 scheme for the DTP-IPV-Hib vaccine (diphtheria, tetanus, pertussis, inactivated polio, and Haemophilus influenzae type b), led to improvements in timeliness and coverage. However, the pandemic’s effects were minimal in disrupting vaccination progress, with some vaccines, like MMR, experiencing delays due to possible vaccine hesitancy or reluctance to administer multiple vaccines concurrently[143]. Another study conducted in Geneva, Switzerland, on COVID-19, found that parental willingness to vaccinate children was related to socioeconomic factors that play a critical role: parents with secondary or primary education levels and those with middle or low household incomes show greater reluctance to vaccinate their children[145].
4.1.25. Türkiye
The COVID-19 pandemic led to substantial disruptions in routine childhood immunizations globally, and Türkiye was no exception. Initial lockdowns and movement restrictions made access to healthcare facilities challenging, leading to delays in vaccinations and coverage rates, including for the DTP3 vaccine [146]. Factors such as parental fear of exposing children to COVID-19 during healthcare visits, logistical challenges in vaccine distribution, and reduced healthcare accessibility have contributed to declines in immunization coverage[147], primarily due to restricted healthcare access and parental hesitancy influenced by concerns over virus transmission during hospital visits. In Ankara, vaccination rates for children under 24 months decreased by approximately 2-5%, with the most pronounced decline observed in vaccines scheduled for children over 18 months[148]. This decline aligns with broader global patterns observed in various countries, where vaccination coverage fell by over 10% in the first months of the pandemic[146]. The COVID-19 pandemic significantly impacted public perspectives on vaccination in the Republic of Türkiye, with a notable increase in vaccine hesitancy. In one study19.6% of participants reported hesitancy regarding routine childhood vaccines, a figure aligned with global studies that indicate similar hesitancy rates across different populations[149]. A study conducted at Trakya University Hospital in Edirne, Türkiye, showed that parental hesitancy towards routine childhood vaccines significantly increased as the pandemic progressed[150]. Among parents surveyed during two COVID-19 peak periods, vaccine hesitancy rose markedly, from 10.6% after the first peak to 20% after the second Additionally, mean scores on the WHO Vaccine Hesitancy Scale (were higher among parents after the second peak, indicating increased hesitancy This shift the overall rise in childhood vaccine hesitancy during the pandemic, suggesting a need for proactive public health communication strategies to maintain high vaccination coverage in Türkiye[151]. Another survey of parents of hospitalized children in Türkiye found vaccine Hesitancy in 9.38% of the parents[146].
4.1.26. Ukraine
In Ukraine, there have been recent public health sector reforms that may affect vaccination uptake[152]. A study previous to the 2022 war found that Prevailing mistrust in the healthcare system and limited access to trustworthy information contributed to the vaccine-related concerns expressed by many parents. [153] In addition, Roma parents encountered systemic obstacles to obtaining vaccines. Vaccine hesitancy in Ukraine is also a problem among refugees[154]. It also posed challenges to achieving high vaccination coverage for IMD[30].
The conflict in Ukraine has led to a significant displacement of children and adolescents, resulting in serious public health challenges in host countries. Many Ukrainian children arrive with low vaccination rates, including for preventable diseases such as measles, polio, and COVID-19, raising concerns about potential outbreaks. Vaccine hesitancy remains prevalent among Ukrainian refugees, further compounding efforts to catch up on vaccinations.[155,156,157]. Addressing these issues requires robust vaccination campaigns, public health education, and coordination among healthcare providers to ensure timely vaccinations, as well as psychological and medical support to mitigate the trauma and complex healthcare needs of these young refugees[154].
4.1.27. United Kingdom
The United Kingdom (UK) has a nationalized healthcare system in which vaccines are recommended and provided to the public through doctors’ offices[158]. The country has a significant history of debates surrounding childhood vaccinations, especially concerning the MMR vaccine[159,160,161,162,163,164]. The influence of previous controversies, such as the Wakefield study linking MMR vaccines to autism, still resonates, with parents citing these fears[165]. The vaccine uptake dropped by approximately 20% in the initial weeks of the lockdown.
The COVID-19 pandemic disrupted routine healthcare services in the UK, including child immunizations, as resources were redirected to COVID-19 responses. Lockdowns, fear of infection, and changes in healthcare accessibility led to delays and reductions in routine vaccination [165]. A study found that 47% of parents have had a children’s health care appointment delayed (24%) or canceled (23%)[102]. Public messaging focused on encouraging the public to “stay at home,” which inadvertently led parents to avoid healthcare facilities, fearing exposure to COVID-19 and a desire not to overburden the National Health Service (NHS). Reports indicated that 60% of families considered postponing or canceling immunizations due to these concerns[3]
During the pandemic, the acceptance of vaccinations decreased in the UK. A study found that 25% of respondents in the UK were hesitant to receive a COVID-19 vaccine, and 6%, respectively, were resistant. This hesitancy aligns with general trends of vaccination resistance observed for other vaccines, indicating an underlying public health concern that extends beyond COVID-19 and potentially impacts routine childhood vaccinations. In the UK, vaccine hesitancy and resistance are influenced by sociodemographic factors, including age, income level, and gender. Women, younger adults, and those in lower income brackets were found to be more vaccine-hesitant[96]. The COVID-19 pandemic highlighted a global challenge of misinformation that directly affects public willingness to vaccinate. Findings suggest that misinformation reduces vaccination intent by approximately six percentage points in the UK[5]. Misinformation affects different sociodemographic groups in varying ways, with females, lower-income groups, and some ethnic minorities more susceptible to altered vaccination intentions[5]. Parents from these demographics might similarly display hesitancy toward child immunizations if they perceive vaccination as unsafe or unnecessary[166].
In the UK, political affiliation influenced vaccine intentions, with Labour Party supporters showing higher vaccination intentions than Conservative Party supporters. This difference is partially attributed to the UK’s regulatory media environment, which is less polarized and is overseen by Ofcom, supporting more balanced public health messaging. This context suggests that political and media landscapes impact vaccine perceptions differently across regions[6]. In the UK, reliance on legacy media (like broadcast TV and newspapers) correlated positively with vaccine intentions, while social media, particularly platforms like Facebook and YouTube, correlated negatively. This negative association on social media may stem from misinformation and conspiracy theories regarding vaccines, especially COVID-19, which saw high engagement on these platforms[167]. Misinformation videos on COVID-19 vaccines spread primarily via Facebook and YouTube shares, and this content often received higher engagement than factual information.
Thus, public health campaigns in the UK may benefit from focusing on regulated media while addressing misinformation on social platforms[6]. Socioeconomic and ethnic factors also influenced vaccine intentions in the UK. Lower vaccine intentions were associated with minority ethnic groups and lower-income households.
Disparities in healthcare access exacerbated the reductions in vaccination coverage. Vaccination rates are typically lower in socioeconomically disadvantaged areas and among minority ethnic groups, who were disproportionately affected by COVID-19 and may hesitate to seek healthcare due to higher perceived risks. Areas with higher deprivation levels and households with lower incomes experienced more significant disruptions in immunization schedules due to increased logistical barriers and healthcare access challenges during COVID-19. Families in these communities were often hesitant or unable to attend catch-up campaigns when clinics reopened[165]. This situation also intersects with challenges in public communication, as health information is often not tailored to reach families with limited English proficiency, literacy, or digital access, such as recent migrants [3].
4.3. Strategies for Enhancing DTP3 Vaccination Coverage in Europe Amidst and Beyond COVID-19 Challenges
The COVID-19 pandemic significantly impacted routine childhood vaccination programs across Europe, including those for DTP3. In response to vaccine hesitancy and fluctuating coverage rates, several European countries have implemented mandatory or incentive-based vaccination policies, which have generally proven effective in increasing vaccine uptake and reducing the incidence of vaccine-preventable diseases. Studies from countries like France and Italy, which adopted stricter immunization policies before the pandemic, show that these mandates can sustain or even improve vaccination coverage despite the challenges posed by COVID-19[101].
Immunization programs are very rentable for the society and the health care system. The Polish immunization program is very effective. Each euro invested produces a return of 2 and 7 euros, from the perspective of health care and society.[168] Ensuring equitable access to childhood vaccinations, such as the DTP3 vaccine, is essential, as systemic biases against prioritizing children’s health can hinder fair healthcare access and compromise their well-being, especially when vaccine hesitancy and safety concerns are prevalent among parents[169]. To improve DTP3 vaccination coverage across Europe, a holistic approach is essential, integrating immunization into broader child health services and addressing practical barriers such as cost, accessibility, and scheduling, alongside fostering trust through enhanced e-health solutions that connect families with tailored support and information systems[170]. Expanding vaccination efforts to non-primary care settings for children could significantly improve immunization rates, especially among underserved populations. Like adults, parents often appreciate the convenience, accessibility, and reduced costs of receiving vaccines outside traditional clinics, such as community centers, schools, or mobile clinics. These locations can reduce logistical barriers, particularly for parents facing time or transportation challenges. However, parental concerns about vaccine safety, fear of side effects, and a strong preference for vaccinations administered by a primary pediatrician remain common barriers. Addressing these concerns through trusted community-based nurses, clear information about vaccine benefits, and flexible vaccination opportunities could support parents’ decisions to vaccinate their children. Broadening immunization access through non-traditional settings thus has the potential to enhance child vaccination rates, reduce disparities, and support public health goals for childhood immunization[171].
Home vaccination by nurses could be a feasible strategy to combat vaccine hesitancy and improve coverage. Home visits for vaccination have effectively boosted coverage among hard-to-reach populations, targeting under-vaccinated children in socioeconomically deprived areas. Offering home vaccinations via a trained team can increase coverage quickly [172]. To counteract this decline, healthcare professionals, especially nurses, should be encouraged to actively reach out to parents and pregnant women, especially in communities with historically low vaccination uptake.
Efforts include clear messaging to reassure families that vaccination services are safe and essential. Some healthcare facilities adapted to the pandemic by establishing drive-in vaccine clinics and other measures that minimize in-person contact.[3]. Misformation exposure often occurs in online environments where individuals can encounter exaggerated risks associated with vaccines. Thus, understanding these digital ecosystems and improving the visibility of reliable information is crucial for protecting child vaccination rates. Misinformation spreads more rapidly than factual information, a factor public health agencies must consider when designing countermeasures. Legacy media use, including broadcast and print media, has been linked with higher vaccine acceptance than social media, which has often hosted vaccine-skeptical narratives. During the pandemic, high reliance on social media for health information was correlated with greater hesitancy, whereas engagement with traditional media was associated with a more positive outlook on vaccines. This dichotomy suggests that public health campaigns must balance digital engagement with efforts to direct audiences toward reliable sources, especially for immunization information aimed at parents[6].
These points reflect how the challenges observed with COVID-19 vaccine misinformation may have broader implications for routine child immunization programs, emphasizing the need for vigilant public health strategies to sustain immunization rates among children.
The pandemic disrupted healthcare services globally, leading to delays in routine child immunizations. With vaccine hesitancy possibly fueled by pandemic-related distrust, the risk of a continued decline in child immunization rates is high. There is a need for renewed efforts to prioritize routine vaccinations post-pandemic, ensuring vaccine hesitancy does not impede the return to pre-pandemic immunization coverage levels.
Government support and investment in primary care infrastructure, community health initiatives, and more robust public health surveillance are essential to monitor and address vaccination gaps. Ensuring robust call-and-recall systems for missed vaccines, improving safety in clinical settings, and strengthening public trust in primary care are pivotal to restoring immunization levels and protecting child health in the long term[3]
Our paper has revealed critical vulnerabilities in routine immunization programs. E ensuring resilience in these programs during future health emergencies will require addressing the socioeconomic factors that drive disparities in vaccine access.
5. Conclusions
The COVID-19 pandemic has profoundly disrupted DTP3 vaccination programs across Europe, exposing significant regional disparities in coverage and recovery. While overall vaccination rates in Europe remain high, several countries have experienced declines, with regions like Eastern Europe facing more significant challenges in regaining pre-pandemic coverage levels compared to more resilient regions such as Southern and Western Europe. These variations underscore the need for targeted public health strategies to address vaccine hesitancy, logistical barriers, and systemic inequities exacerbated by the pandemic.
The pandemic has introduced immediate and sustained challenges to routine immunization efforts, with statistical models revealing shifts in vaccination trends in countries such as Ireland, Sweden, and Switzerland, which experienced reductions in coverage. Conversely, countries like Ukraine and San Marino reported notable improvements, highlighting the importance of localized healthcare strategies and robust public health interventions.
To mitigate the “immunity debt” caused by pandemic-related disruptions and to protect vulnerable populations from vaccine-preventable diseases, measures should be taken to enhance trust in vaccination, leverage community healthcare resources, and combat misinformation. While some healthcare systems have demonstrated resilience, sustained efforts to reinforce healthcare infrastructure and adapt immunization programs are essential to ensure equitable access and uptake, safeguard against future public health crises, and protect global health achievements.
Author Contributions
Conceptualization, ERV, FGG, IA, SGA; Methodology, IAO, MGA; Software, FGG, MGA; Data Curation, ERV, FGG, LGA, MGA; Investigator Resources, EAO, LGA; Formal Analysis, FGG, MGA, RAB; Visualization, FGG, MGA; Supervision, EAO, ERV, FGG, IAO, LO; Writing—Original Draft, EAO, FGG, IAO, LGA, LO, SGA; Writing—Review & Editing, EAO, ERV, FGG, IAO, LGA, LO, MGA, RAB, SGA;
Funding
This research received no external funding
Institutional Review Board Statement
The study did not require ethical approval.
Data Availability Statement
Data were obtained from the following resources available in the public domain: World Bank, United Nations, and UNICEF. https://data.worldbank.org/indicator/SP.POP.TOTL, https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=GLOBAL_DATAFLOW&ver=1.0&dq=.DM_BRTS..&startPeriod=2019&endPeriod=2023, https://population.un.org/wpp.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Aguinaga-Ontoso, I.; Guillen-Aguinaga, S.; Guillen-Aguinaga, L.; Alas-Brun, R.; Onambele, L.; Aguinaga-Ontoso, E.; Guillen-Grima, F. COVID-19 Impact on DTP Vaccination Trends in Africa: A Joinpoint Regression Analysis. Vaccines (Basel) 2023, 11, 1103. [Google Scholar] [CrossRef]
- Aguinaga-Ontoso, I.; Guillén-Aguinaga, S.; Guillén-Aguinaga, L.; Alas-Brun, R.; Aguinaga-Ontoso, E.; Rayón-Valpuesta, E.; Guillén-Grima, F. Has COVID-19 Affected DTP3 Vaccination in the Americas? Vaccines (Basel) 2024, 12, 238. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Skirrow, H.; Bedford, H. Routine Vaccination during Covid-19 Pandemic Response. BMJ 2020, m2392. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.U.; Haq, F.U.; Imran, M.; Shah, A.; Bibi, N.; Khurshid, R.; Romman, M.; Gaffar, F.; Khan, M.I. Impact of the COVID-19 Lockdown on Routine Vaccination in Pakistan: A Hospital-Based Study. Hum Vaccin Immunother 2024, 17, 4934–4940. [Google Scholar] [CrossRef]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the Impact of COVID-19 Vaccine Misinformation on Vaccination Intent in the UK and USA. Nat Hum Behav 2021, 5, 337–348. [Google Scholar] [CrossRef]
- Allington, D.; McAndrew, S.; Moxham-Hall, V.L.; Duffy, B. Media Usage Predicts Intention to Be Vaccinated against SARS-CoV-2 in the US and the UK. Vaccine 2021, 39, 2595–2603. [Google Scholar] [CrossRef] [PubMed]
- Cellini, M.; Pecoraro, F.; Rigby, M.; Luzi, D. Comparative Analysis of Pre-Covid19 Child Immunization Rates across 30 European Countries and Identification of Underlying Positive Societal and System Influences. PLoS One 2022, 17, e0271290. [Google Scholar] [CrossRef]
- Lassi, Z.S.; Naseem, R.; Salam, R.A.; Siddiqui, F.; Das, J.K. The Impact of the COVID-19 Pandemic on Immunization Campaigns and Programs: A Systematic Review. Int J Environ Res Public Health 2021, 18, 988. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Medic, S.; Cassimos, D.C.; Effraimidou, E.; Poland, G.A. Decreasing Routine Vaccination Rates in Children in the COVID-19 Era. Vaccine 2022, 40, 2525–2527. [Google Scholar] [CrossRef]
- Bramer, C.A.; Kimmins, L.M.; Swanson, R.; Kuo, J.; Vranesich, P.; Jacques-Carroll, L.A.; Shen, A.K. Decline in Child Vaccination Coverage During the COVID-19 Pandemic — Michigan Care Improvement Registry, May 2016–May 2020. MMWR Morb Mortal Wkly Rep 2020, 69, 630–631. [Google Scholar] [CrossRef]
- Dinleyici, E.C.; Borrow, R.; Safadi, M.A.P.; van Damme, P.; Munoz, F.M. Vaccines and Routine Immunization Strategies during the COVID-19 Pandemic. Hum Vaccin Immunother 2021, 17, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Spencer, N.; Nathawad, R.; Arpin, E.; Johnson, S. Pandemics, Epidemics and Inequities in Routine Childhood Vaccination Coverage: A Rapid Review. BMJ Paediatr Open 2020, 4, e000842. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Samara, A.; Campbell, H.; Ladhani, S.N.; Amirthalingam, G. Recent Increase in Infant Pertussis Cases in Europe and the Critical Importance of Antenatal Immunizations: We Must Do Better…now. International Journal of Infectious Diseases 2024, 146, 107148. [Google Scholar] [CrossRef]
- World Health Organization. Half a million children in WHO European Region not fully vaccinated in their first year of life: New 2023 data reveal both gaps and gains in immunization coverage https://www.who.int/europe/news/item/15-07-2024-half-a-million-children-in-who-european-region-not-fully-vaccinated-in-their-first-year-of-life--new-2023-data-reveal-both-gaps-and-gains-in-immunization-coverage (accessed 2024 -10 -19).
- World Health Organization. European Region achieves high routine immunization coverage, but falls short of pre-pandemic levels.
- Director-General WHO. Immunization Agenda 2030 Progress towards Global Immunization Goals and Implementation of the Immunization Agenda 2030.EXECUTIVE BOARD EB154/9 154th Session 4 December 2023 Provisional Agenda Item 9 Immunization Agenda 2030 Progress towards Global Immunization Goals and Implementation of the Immunization Agenda 2030 Report by the Director-General; Geneva, 2023.
- WHO The Global Health Observatory. Immunization and vaccine-preventable communicable diseases.
- WHO. Varied impact of COVID-19 on routine immunization in the European Region https://www.who.int/europe/news/item/16-07-2021-varied-impact-of-covid-19-on-routine-immunization-in-the-european-region.
- WHO. COVID-19 pandemic leads to major backsliding on childhood vaccinations, new WHO, UNICEF data shows https://www.who.int/news/item/15-07-2021-covid-19-pandemic-leads-to-major-backsliding-on-childhood-vaccinations-new-who-unicef-data-shows (accessed 2024 -10 -20).
- Effraimidou, E.; Cassimos, D.C.; Medic, S.; Topalidou, M.; Theodoridou, M.; Maltezou, H.C. Vaccination Programs for Children Aged up to 18 Years in Europe, 2020. Journal of Child Health Care 2023, 27, 336–350. [Google Scholar] [CrossRef]
- Saidu, Y. Exploring Barriers to Immunization Coverage within a Sub-Saharan African Setting, Università degli Studi di Siena, Siena, 2023.
- Ackerson, B.K.; Sy, L.S.; Glenn, S.C.; Qian, L.; Park, C.H.; Riewerts, R.J.; Jacobsen, S.J. Pediatric Vaccination During the COVID-19 Pandemic. Pediatrics 2021, 148. [Google Scholar] [CrossRef] [PubMed]
- Moura, C.; Truche, P.; Sousa Salgado, L.; Meireles, T.; Santana, V.; Buda, A.; Bentes, A.; Botelho, F.; Mooney, D. The Impact of COVID-19 on Routine Pediatric Vaccination Delivery in Brazil. Vaccine 2022, 40, 2292–2298. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Medic, S.; Cassimos, D.C.; Effraimidou, E.; Poland, G.A. Decreasing Routine Vaccination Rates in Children in the COVID-19 Era. Vaccine 2022, 40, 2525–2527. [Google Scholar] [CrossRef] [PubMed]
- Santoli, J.M.; Lindley, M.C.; DeSilva, M.B.; Kharbanda, E.O.; Daley, M.F.; Galloway, L.; Gee, J.; Glover, M.; Herring, B.; Kang, Y.; Lucas, P.; Noblit, C.; Tropper, J.; Vogt, T.; Weintraub, E. Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration — United States, 2020. MMWR Morb Mortal Wkly Rep 2020, 69, 591–593. [Google Scholar] [CrossRef]
- Ji, C.; Piché-Renaud, P.-P.; Apajee, J.; Stephenson, E.; Forte, M.; Friedman, J.N.; Science, M.; Zlotkin, S.; Morris, S.K.; Tu, K. Impact of the COVID-19 Pandemic on Routine Immunization Coverage in Children under 2 Years Old in Ontario, Canada: A Retrospective Cohort Study. Vaccine 2022, 40, 1790–1798. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.; Cabrera, M.; Moore, M.; Lomazzi, M. Driving Paediatric Vaccine Recovery in Europe. Vaccines (Basel) 2023, 11, 184. [Google Scholar] [CrossRef]
- Polašek, O.; Wazny, K.; Adeloye, D.; Song, P.; Chan, K.Y.; Bojude, D.A.; Ali, S.; Bastien, S.; Becerra-Posada, F.; Borrescio-Higa, F.; Cheema, S.; Cipta, D.A.; Cvjetković, S.; Castro, L.D.; Ebenso, B.; Femi-Ajao, O.; Ganesan, B.; Glasnović, A.; He, L.; Heraud, J.M.; Igwesi-Chidobe, C.; Iversen, P.O.; Jadoon, B.; Karim, A.J.; Khan, J.; Biswas, R.K.; Lanza, G.; Lee, S.W.; Li, Y.; Liang, L.-L.; Lowe, M.; Islam, M.M.; Marušić, A.; Mshelia, S.; Manyara, A.M.; Htay, M.N.; Parisi, M.; Peprah, P.; Sacks, E.; Akinyemi, K.O.; Shahraki-Sanavi, F.; Sharov, K.; Rotarou, E.S.; Stankov, S.; Supriyatiningsih, W.; Chan, B.T.; Tremblay, M.; Tsimpida, D.; Vento, S.; Glasnović, J.V.; Wang, L.; Wang, X.; Ng, Z.X.; Zhang, J.; Zhang, Y.; Campbell, H.; Chopra, M.; Cousens, S.; Krstić, G.; Macdonald, C.; Mansoori, P.; Patel, S.; Sheikh, A.; Tomlinson, M.; Tsai, A.C.; Yoshida, S.; Rudan, I. Research Priorities to Reduce the Impact of COVID-19 in Low- and Middle-Income Countries. J Glob Health 2022, 12, 09003. [Google Scholar] [CrossRef]
- Jovanović, V.; Lazić, M. Vaccination Attitudes Examination (VAX) Scale: A Bifactor-ESEM Approach in a Youth Sample (15–24 Years). BMC Psychol 2023, 11, 351. [Google Scholar] [CrossRef]
- Tzanakaki, G.; Cabrnochová, H.; Delić, S.; Draganescu, A.; Hilfanova, A.; Onozó, B.; Pokorn, M.; Skoczyńska, A.; Tešović, G. Invasive Meningococcal Disease in South-Eastern European Countries: Do We Need to Revise Vaccination Strategies? Hum Vaccin Immunother 2024, 20. [Google Scholar] [CrossRef] [PubMed]
- Aguinaga-Ontoso, I.; Guillen-Aguinaga, S.; Guillen-Aguinaga, L.; Alas-Brun, R.; Onambele, L.; Aguinaga-Ontoso, E.; Guillen-Grima, F. COVID-19 Impact on DTP Vaccination Trends in Africa: A Joinpoint Regression Analysis. Vaccines (Basel) 2023, 11, 1103. [Google Scholar] [CrossRef] [PubMed]
- Aguinaga-Ontoso, I.; Guillén-Aguinaga, S.; Guillén-Aguinaga, L.; Alas-Brun, R.; Aguinaga-Ontoso, E.; Rayón-Valpuesta, E.; Guillén-Grima, F. Has COVID-19 Affected DTP3 Vaccination in the Americas? Vaccines (Basel) 2024, 12, 238. [Google Scholar] [CrossRef] [PubMed]
- United Nations. WHO: “Alarming” rise of measles cases in Europe https://unric.org/en/who-alarming-rise-of-measles-cases-in-europe/ (accessed 2024 -09 -23).
- Mboussou, F.; Kada, S.; Danovaro-Holliday, M.C.; Farham, B.; Gacic-Dobo, M.; Shearer, J.C.; Bwaka, A.; Amani, A.; Ngom, R.; Vuo-Masembe, Y.; Wiysonge, C.S.; Impouma, B. Status of Routine Immunization Coverage in the World Health Organization African Region Three Years into the COVID-19 Pandemic. Vaccines (Basel) 2024, 12, 168. [Google Scholar] [CrossRef]
- Cardoso Pinto, A.M.; Ranasinghe, L.; Dodd, P.J.; Budhathoki, S.S.; Seddon, J.A.; Whittaker, E. Disruptions to Routine Childhood Vaccinations in Low- and Middle-Income Countries during the COVID-19 Pandemic: A Systematic Review. Front Pediatr 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- GAVI. Raising Generation Immunity The 2023 Mid-Term Review Report; Geneva,Switzerland, 2023.
- O’Leary, S.T.; Opel, D.J.; Cataldi, J.R.; Hackell, J.M.; O’Leary, S.T.; Campbell, J.D.; Ardura, M.I.; Banerjee, R.; Bryant, K.A.; Caserta, M.T.; Frenck, R.; Gerber, J.S.; John, C.C.; Kourtis, A.P.; Myers, A.; Pannaraj, P.; Ratner, A.J.; Shah, S.S.; Kimberlin, D.W.; Barnett, E.D.; Lynfield, R.; Sawyer, M.H.; Bernstein, H.H.; Cardemil, C.; Farizo, K.M.; Kafer, L.M.; Kim, D.; Medina, E.L.; Moore, D.; Panagiotakopoulos, L.; Romero, J.R.; Sauvé, L.; Starke, J.R.; Thompson, J.; Wharton, M.; Woods, C.R.; Frantz, J.M.; Gibbs, G.; Hackell, J.M.; Almendarez, Y.M.; Berhane, A.M.; Cantrell, P.E.; Kafer, L.M.; Latimer, T.; Warner, R.; Wiskind, R.H.; Schafer, K.; Skatrud, A.; Magnus, M.A.; Laventhal, N.T.; Geis, G.M.; Loeff, D.S.; Michelson, K.; Ott, M.; Elster, N.; Diekema, D.S.; Arora, K.; McGee, M.; Emanuel, A. Strategies for Improving Vaccine Communication and Uptake. Pediatrics 2024, 153. [Google Scholar] [CrossRef]
- Stepovic, M.; Dragojevic Simic, V.; Zivanovic Macuzic, I.; Simic, R.; Vekic, S.; Sekulic, M.; Radovanovic, S.; Maricic, M.; Sorak, M.; Suljagic, V.; Vojinovic, R.; Rancic, N. The Last 3 Decade of Vaccination Coverage in the Balkan and Eastern Europe Countries with Reference to the Impact of the COVID-19 Pandemic. Front Pharmacol 2024, 15. [Google Scholar] [CrossRef] [PubMed]
- Lindstrand, A.; Cherian, T.; Chang-Blanc, D.; Feikin, D.; O’Brien, K.L. The World of Immunization: Achievements, Challenges, and Strategic Vision for the Next Decade. J Infect Dis 2021, 224 (Supplement_4), S452–S467. [Google Scholar] [CrossRef] [PubMed]
- Data Warehouse - UNICEF DATA https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=IMMUNISATION&ver=1.0&dq=.IM_DTP3..&startPeriod=2000&endPeriod=2024 (accessed 2024 -07 -27).
- United Nations. Standard country or area codes for statistical use (M49) https://unstats.un.org/unsd/methodology/m49/ (accessed 2024 -07 -27).
- World Bank. Population, total | Data https://data.worldbank.org/indicator/SP.POP.TOTL (accessed 2024 -07 -28).
- UNICEF. Number of Births. Data Warehouse - UNICEF DATA https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=GLOBAL_DATAFLOW&ver=1.0&dq=.DM_BRTS..&startPeriod=2019&endPeriod=2023 (accessed 2024 -07 -28).
- United Nations, D. of E. and S. A. P. D. World Population Prospects 2022, Online Edition https://population.un.org/wpp (accessed 2024 -07 -28).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation Tests for Joinpoint Regression with Applications to Cancer Rates. Stat Med 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Joinpoint Regression Program Version 5.2.0. May, 2023; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute. 2023.
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing: Vienna, Austria. 2023.
- Muggeo, V.M.; Atkins, D.C.; Gallop, R.J.; Dimidjian, S. Segmented Mixed Models with Random Changepoints: A Maximum Likelihood Approach with Application to Treatment for Depression Study. Stat Modelling 2014, 14, 293–313. [Google Scholar] [CrossRef]
- Muggeo, V.M.R. Interval Estimation for the Breakpoint in Segmented Regression: A Smoothed Score-based Approach. Aust N Z J Stat 2017, 59, 311–322. [Google Scholar] [CrossRef]
- Muggeo, V.M.R. Testing with a Nuisance Parameter Present Only under the Alternative: A Score-Based Approach with Application to Segmented Modelling. J Stat Comput Simul 2016, 86, 3059–3067. [Google Scholar] [CrossRef]
- Fasola, S.; Muggeo, V.M.R.; Küchenhoff, H. A Heuristic, Iterative Algorithm for Change-Point Detection in Abrupt Change Models. Comput Stat 2018, 33, 997–1015. [Google Scholar] [CrossRef]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer-Verlag: New York, 2016. [Google Scholar]
- Wickham, H.; Bryan, J. Readxl: Read Excel Files_. R Package Version 1.4.3. 2023.
- MapChart Version 6.0.10. MapChart. November 30, 2024.
- Brewer, C.A.; Hatchard, G.W.; Harrower, M.A. COLORBREWER 2.0 Color Advice for Cartograph. 2013.
- Brewer, C.A.; Hatchard, G.W.; Harrower, M.A. ColorBrewer in Print: A Catalog of Color Schemes for Maps. Cartogr Geogr Inf Sci 2003, 30, 5–32. [Google Scholar] [CrossRef]
- Nelson, R. COVID-19 Disrupts Vaccine Delivery. Lancet Infect Dis 2020, 20, 546. [Google Scholar] [CrossRef] [PubMed]
- WHO. At least 80 million children under one at risk of diseases such as diphtheria, measles and polio as COVID-19 disrupts routine vaccination efforts, warn Gavi, WHO and UNICEF https://www.who.int/news-room/detail/22-05-2020-at-least-80-million-children-under-one-at-risk-of-diseases-such-as-diphtheria-measles-and-polio-as-covid-19-disrupts-routine-vaccination-efforts-warn-gavi-who-and-unicef (accessed 2024 -10 -23).
- Dinleyici, E.C.; Borrow, R.; Safadi, M.A.P.; van Damme, P.; Munoz, F.M. Vaccines and Routine Immunization Strategies during the COVID-19 Pandemic. Hum Vaccin Immunother 2021, 17, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Badker, R.; Miller, K.; Pardee, C.; Oppenheim, B.; Stephenson, N.; Ash, B.; Philippsen, T.; Ngoon, C.; Savage, P.; Lam, C.; Madhav, N. Challenges in Reported COVID-19 Data: Best Practices and Recommendations for Future Epidemics. BMJ Glob Health 2021, 6, e005542. [Google Scholar] [CrossRef] [PubMed]
- Rotulo, A.; Kondilis, E.; Thwe, T.; Gautam, S.; Torcu, Ö.; Vera-Montoya, M.; Marjan, S.; Gazi, Md. I.; Putri, A.S.; Hasan, R.B.; Mone, F.H.; Rodríguez-Castillo, K.; Tabassum, A.; Parcharidi, Z.; Sharma, B.; Islam, F.; Amoo, B.; Lemke, L.; Gallo, V. Mind the Gap: Data Availability, Accessibility, Transparency, and Credibility during the COVID-19 Pandemic, an International Comparative Appraisal. PLOS Global Public Health 2023, 3, e0001148. [Google Scholar] [CrossRef] [PubMed]
- Musa, S.; Bach Habersaat, K.; Jackson, C.; Kulo, A.; Primorac, E.; Smjecanin, M.; Funk, S. Tailoring Immunization Programmes: Using Patient File Data to Explore Vaccination Uptake and Associated Factors. Hum Vaccin Immunother 2021, 17, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Stanescu, A.; Ruta, S.M.; Cernescu, C.; Pistol, A. Suboptimal MMR Vaccination Coverages—A Constant Challenge for Measles Elimination in Romania. Vaccines (Basel) 2024, 12, 107. [Google Scholar] [CrossRef] [PubMed]
- Mayerová, D.; Abbas, K. Childhood Immunisation Timeliness and Vaccine Confidence by Health Information Source, Maternal, Socioeconomic, and Geographic Characteristics in Albania. BMC Public Health 2021, 21, 1724. [Google Scholar] [CrossRef] [PubMed]
- Stoeckel, F.; Carter, C.; Lyons, B.A.; Reifler, J. Association of Vaccine Hesitancy and Immunization Coverage Rates in the European Union. Vaccine 2021, 39, 3935–3939. [Google Scholar] [CrossRef]
- Bali, D.; Kuli-Lito, G.; Ceka, N.; Godo, A. Maternal and Child Health Care Services in Albania. J Pediatr 2016, 177, S11–S20. [Google Scholar] [CrossRef] [PubMed]
- Petro, E.; Perumal-Pillay, V.; Mantel-Teeuwisse, A.K.; van den Ham, H.A.; Suleman, F. Evaluation of Alignment of the Reimbursement Medicines List for Children in Albania with the WHO Essential Medicines List for Children. J Pharm Policy Pract 2024, 17. [Google Scholar] [CrossRef]
- Mayerová, D.; Abbas, K. Childhood Immunisation Timeliness and Vaccine Confidence by Health Information Source, Maternal, Socioeconomic, and Geographic Characteristics in Albania. BMC Public Health 2021, 21, 1724. [Google Scholar] [CrossRef] [PubMed]
- Gjini, E.; Moramarco, S.; Carestia, M.C.; Cenko, F.; Ylli, A.; Mehmeti, I.; Palombi, L.; Buonomo, E. Parents’ and Caregivers’ Role toward Childhood Vaccination in Albania: Assessment of Predictors of Vaccine Hesitancy. Ann Ig 2023, 35, 75–83. [Google Scholar] [CrossRef]
- Pojani, P.C.E.; Nelaj, E.; Ylli, A.P.M.A. Overview of the Immunization Situation in Albania. European Journal of Multidisciplinary Studies 2017, 5, 259. [Google Scholar] [CrossRef]
- Gjini, E.; Carestia, M.; Cenko, F.; Di Giovanni, D.; Mehmeti, I.; Moramarco, S.; Yulli, A.; Buonomo, E. Hesitancy toward Childhood Vaccinations: Preliminary Results from an Albanian Nursing Staff’s Investigation. Nurs Res Pract 2022, 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Measles on the Rise in the EU/EEA: Considerations for Public Health Response.; Stockholm, 2024. [CrossRef]
- Bauer, A.; Tiefengraber, D.; Wiedermann, U. Towards Understanding Vaccine Hesitancy and Vaccination Refusal in Austria. Wien Klin Wochenschr 2021, 133, 703–713. [Google Scholar] [CrossRef]
- Magyar, R.; Voitl, P.K.; Voitl, J.J.M.; Diesner-Treiber, S.C. Vaccine Hesitancy among Parents of Children in Their First Two Years of Life. Front Public Health 2024, 12. [Google Scholar] [CrossRef]
- Gobert, C.; Semaille, P.; Van der Schueren, T.; Verger, P.; Dauby, N. Prevalence and Determinants of Vaccine Hesitancy and Vaccines Recommendation Discrepancies among General Practitioners in French-Speaking Parts of Belgium. Vaccines (Basel) 2021, 9, 771. [Google Scholar] [CrossRef]
- Partouche, H.; Gilberg, S.; Renard, V.; Saint-Lary, O. Mandatory Vaccination of Infants in France: Is That the Way Forward? European Journal of General Practice 2019, 25, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Carrico, J.; Mellott, C.E.; Talbird, S.E.; Bento-Abreu, A.; Merckx, B.; Vandenhaute, J.; Benchabane, D.; Dauby, N.; Ethgen, O.; Lepage, P.; Luyten, J.; Raes, M.; Simoens, S.; Van Ranst, M.; Eiden, A.; Nyaku, M.K.; Bencina, G. Public Health Impact and Return on Investment of Belgium’s Pediatric Immunization Program. Front Public Health 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Glatman-Freedman, A.; Nichols, K. The Effect of Social Determinants on Immunization Programs. Hum Vaccin Immunother 2012, 8, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Varbanova, V.; Verelst, F.; Hens, N.; Beutels, P. Determinants of Basic Childhood Vaccination Coverage in European and OECD Countries. Hum Vaccin Immunother 2022, 18. [Google Scholar] [CrossRef] [PubMed]
- Kolesar, R.J.; Spruk, R.; Tsheten, T. Evaluating Country Performance After Transitioning From Gavi Assistance: An Applied Synthetic Control Analysis. Glob Health Sci Pract 2023, 11, e2200536. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Regional Office for Europe. Ukraine Crisis Strategic Response Plan for January–December 2023.; Copenhagen, 2023.
- Tull, K. Vaccine Hesitancy: Guidance and Interventions. ; 2019.
- Hadjipanayis, A.; van Esso, D.; del Torso, S.; Dornbusch, H.J.; Michailidou, K.; Minicuci, N.; Pancheva, R.; Mujkic, A.; Geitmann, K.; Syridou, G.; Altorjai, P.; Pasinato, A.; Valiulis, A.; Soler, P.; Cirstea, O.; Illy, K.; Mollema, L.; Mazur, A.; Neves, A.; Zavrsnik, J.; Lapii, F.; Efstathiou, E.; Kamphuis, M.; Grossman, Z. Vaccine Confidence among Parents: Large Scale Study in Eighteen European Countries. Vaccine 2020, 38, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Riad, A. COVID-19 Vaccine Hesitancy: A Tale of Two Pandemics, Charles University Faculty of Medicine in Pilsen, Pilsen, 2013.
- Vijest HIR. Krivotvorenje COVID potvrda postalo pravi mali biznis: Desetero palo u Zagrebu, lažno upisivali cijepljenja [Forgery of COVID certificates has become a real small business: Ten fell in Zagreb, falsely registering vaccinations] https://kaportal.net.hr/aktualno/vijesti/148105/krivotvorenje-covid-potvrda-postalo-pravi-mali-biznis-desetero-palo-u-zagrebu-lazno-upisivali-cijepljenja/ (accessed 2024 -10 -25).
- Tomljenovic, H.; Bubic, A.; Hren, D. Decision Making Processes Underlying Avoidance of Mandatory Child Vaccination in Croatia – a Qualitative Study. Current Psychology 2022, 41, 6210–6224. [Google Scholar] [CrossRef]
- Jerković, H.; Šitum, M. VACCINE HESITANCY - FROM PARENTAL DISTRUST TO COVID-19 CONSPIRACIES. Psychiatr Danub 2023, 35, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Pivac, I.; Markić, J.; Poklepović Peričić, T.; Aranza, D.; Marušić, A. Evaluating Health Claim Assessment Skills of Parents with Preschool Children: A Cross-Sectional Study Using Informed Health Choices Claim Evaluation Tool. J Glob Health 2023, 13, 04156. [Google Scholar] [CrossRef] [PubMed]
- Fakonti, G.; Kyprianidou, M.; Toumbis, G.; Giannakou, K. Attitudes and Acceptance of COVID-19 Vaccination Among Nurses and Midwives in Cyprus: A Cross-Sectional Survey. Front Public Health 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Kyprianidou, M.; Fakonti, G.; Tzira, E.; Pylli, M.; Giannakou, K. Associations between Socio-Demographic Characteristics and Maternal Attitudes towards Childhood Vaccination in Cyprus—A Cross-Sectional Survey. COVID 2023, 3, 1042–1051. [Google Scholar] [CrossRef]
- Vuolanto, P.; Almeida, A.N.; Anderson, A.; Auvinen, P.; Beja, A.; Bracke, P.; Cardano, M.; Ceuterick, M.; Correia, T.; De Vito, E.; Delaruelle, K.; Delicado, A.; Esposito, M.; Ferrara, M.; Gariglio, L.; Guerreiro, C.; Marhánková, J.H.; Hilário, A.P.; Hobson-West, P.; Iorio, J.; Järvinen, K.-M.; Koivu, A.; Kotherová, Z.; Kuusipalo, A.; Lermytte, E.; Mendonça, J.; Morais, R.; Numerato, D.; Polak, P.; Rudek, T.; Sbaragli, S.; Scavarda, A.; Silva, K.; da Silva, P.A.; Sivelä, J.; Moura, E.S.; Świątkiewicz-mośny, M.; Tipaldo, G.; Wagner, A. Trust Matters: The Addressing Vaccine Hesitancy in Europe Study. Scand J Public Health 2024, 52, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Macounová, P.; Macounová, D. Mumps and Its Occurrence in the Czech Republic and Slovakia. Epidemiol Mikrobiol Imunol 2021, 70, 253–263. [Google Scholar]
- Riad, A.; Jouzová, A.; Üstün, B.; Lagová, E.; Hruban, L.; Janků, P.; Pokorná, A.; Klugarová, J.; Koščík, M.; Klugar, M. COVID-19 Vaccine Acceptance of Pregnant and Lactating Women (PLW) in Czechia: An Analytical Cross-Sectional Study. Int J Environ Res Public Health 2021, 18, 13373. [Google Scholar] [CrossRef] [PubMed]
- Merilind, E.; Salupere, R.; Västra, K.; Kalda, R. The Influence of Performance-Based Payment on Childhood Immunisation Coverage. Health Policy (New York) 2015, 119, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Whelan, S.O.; Moriarty, F.; Lawlor, L.; Gorman, K.M.; Beamish, J. Vaccine Hesitancy and Reported Non-Vaccination in an Irish Pediatric Outpatient Population. Eur J Pediatr 2021, 180, 2839–2847. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; Levita, L.; Martinez, A.P.; Stocks, T.V.A.; Karatzias, T.; Hyland, P. Psychological Characteristics Associated with COVID-19 Vaccine Hesitancy and Resistance in Ireland and the United Kingdom. Nat Commun 2021, 12, 29. [Google Scholar] [CrossRef]
- Ceannt, R.; Vallieres, F.; Burns, H.; Murphy, J.; Hyland, P. Covid-19 Vaccine Hesitancy and Resistance amongst Parents of Children under 18 Years of Age in Ireland. Vaccine 2022, 40, 6196–6200. [Google Scholar] [CrossRef] [PubMed]
- Marron, L.; Ferenczi, A.; O’Brien, K.M.; Cotter, S.; Jessop, L.; Morrissey, Y.; Migone, C. Views on COVID-19 Vaccination of Young Children in Ireland, Results from a Cross-Sectional Survey of Parents. Vaccine 2022, 40, 5716–5725. [Google Scholar] [CrossRef] [PubMed]
- Marron, L.; Ferenczi, A.; O’Brien, K.M.; Cotter, S.; Jessop, L.; Morrissey, Y.; Migone, C. A National Survey of Parents’ Views on Childhood Vaccinations in Ireland. Vaccine 2023, 41, 3740–3754. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Moore, A.C.; Sahm, L.J.; Fleming, A. Parent Attitudes about Childhood Vaccines: Point Prevalence Survey of Vaccine Hesitancy in an Irish Population. Pharmacy 2021, 9, 188. [Google Scholar] [CrossRef] [PubMed]
- Kuznetsova, L.; Cortassa, G.; Trilla, A. Effectiveness of Mandatory and Incentive-Based Routine Childhood Immunization Programs in Europe: A Systematic Review of the Literature. Vaccines (Basel) 2021, 9, 1173. [Google Scholar] [CrossRef] [PubMed]
- Tan, L. (L. J.; Safadi, M.A.P.; Horn, M.; Regojo Balboa, C.; Moya, E.; Schanbaum, J.; Pimenta, P.; Lambert, E.; Soumahoro, L.; Sohn, W.-Y.; Bruce, T.; Ruiz García, Y. Pandemic’s Influence on Parents’ Attitudes and Behaviors toward Meningococcal Vaccination. Hum Vaccin Immunother 2023, 19. [Google Scholar] [CrossRef]
- Tondo, L. Italian Nurse Accused of Giving Fake Covid Jabs to Anti-Vaxxers Arrested. The Guardian 2022. [Google Scholar]
- Poeta, M.; Moracas, C.; Albano, C.; Petrarca, L.; Maglione, M.; Pierri, L.; Carta, M.; Montaldo, P.; Venturini, E.; De Luca, M.; Buonsenso, D.; Brambilla, I.; Giacomet, V.; Lo Vecchio, A.; Bruzzese, E.; Midulla, F.; Colomba, C.; Guarino, A. Pertussis Outbreak in Neonates and Young Infants across Italy, January to May 2024: Implications for Vaccination Strategies. Eurosurveillance 2024, 29. [Google Scholar] [CrossRef] [PubMed]
- Crescenzi-Lanna, L.; Valente, R.; Cataldi, S.; Martire, F. Predictors of Young People’s Anti-Vaccine Attitudes in the Context of the COVID-19 Pandemic. Public Understanding of Science 2024, 33, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Kassianos, G.; Cohen, J.-M.; Civljak, R.; Davidovitch, N.; Pecurariu, O.F.; Froes, F.; Galev, A.; Ivaskeviciene, I.; Kõivumägi, K.; Kristufkova, Z.; Kuchar, E.; Kyncl, J.; Maltezou, H.C.; Marković, M.; Nitsch-Osuch, A.; Ortiz de Lejarazu, R.; Rossi, A.; Schelling, J.; van Essen, G.A.; Zavadska, D. The Influenza Landscape and Vaccination Coverage in Older Adults during the SARS-Cov-2 Pandemic: Data from Several European Countries and Israel. Expert Rev Respir Med 2024, 18, 69–84. [Google Scholar] [CrossRef]
- Lucane, Z.; Kursite, M.; Sablinskis, K.; Gailite, L.; Kurjane, N. COVID-19 Vaccination Coverage and Factors Influencing Vaccine Hesitancy among Patients with Inborn Errors of Immunity in Latvia: A Mixed-Methods Study. Vaccines (Basel) 2023, 11, 1637. [Google Scholar] [CrossRef] [PubMed]
- Kraft, K.B.; Godøy, A.A.; Vinjerui, K.H.; Kour, P.; Kjøllesdal, M.K.R.; Indseth, T. Vaksinasjonsdekning Mot Covid-19 Etter Innvandrerbakgrunn. Tidsskrift for Den norske legeforening 2022. [Google Scholar] [CrossRef] [PubMed]
- Čeponytė, K.; Narkevičiūtė, E.; Beržanskytė, A.; Burokienė, S. Determinants of Parental Attitudes towards Children’s Vaccination in Lithuania: An Online Survey. Acta Med Litu 2024, 31, 23–34. [Google Scholar] [CrossRef]
- Svist, V.; Maciuleviciene, A.; Naudziunaite, S.; Petraitiene, S.; del Torso, S.; Grossman, Z.; Magelinskiene, G.; Valiulis, A. Vaccine-Hesitant Families Are More Susceptible to Verbal Communication Messaging. Cent Eur J Public Health 2023, 31, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, S.P.; Silver, D.; Domenti, O.; Gasoyan, H.; Paatashvili, E.; Gellin, B.G.; Gordon, J.L. Strengthening Legal Frameworks for Vaccination: The Experiences of Armenia, Georgia, and Moldova. Vaccine 2019, 37, 4840–4847. [Google Scholar] [CrossRef]
- Melovic, B.; Jaksic Stojanovic, A.; Vulic, T.B.; Dudic, B.; Benova, E. The Impact of Online Media on Parents’ Attitudes toward Vaccination of Children—Social Marketing and Public Health. Int J Environ Res Public Health 2020, 17, 5816. [Google Scholar] [CrossRef]
- Knijff, M.; van Lier, A.; Boer, M.; de Vries, M.; Hament, J.-M.; de Melker, H.E. Parental Intention, Attitudes, Beliefs, Trust and Deliberation towards Childhood Vaccination in the Netherlands in 2022: Indications of Change Compared to 2013. Vaccine 2024, 42, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Klinkenberg, D.; van Hoek, A.J.; Veldhuijzen, I.; Hahné, S.; Wallinga, J. Social Clustering of Unvaccinated Children in Schools in the Netherlands. Epidemiol Infect 2022, 150, e200. [Google Scholar] [CrossRef] [PubMed]
- Middeldorp, M.; van Lier, A.; van der Maas, N.; Veldhuijzen, I.; Freudenburg, W.; van Sorge, N.M.; Sanders, E.A.M.; Knol, M.J.; de Melker, H.E. Short Term Impact of the COVID-19 Pandemic on Incidence of Vaccine Preventable Diseases and Participation in Routine Infant Vaccinations in the Netherlands in the Period March-September 2020. Vaccine 2021, 39, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Shumanov, G.; Todosieva, J.; Nikolovska, E.; Shumanova, C.; Panova, G. Condition and Prospects of Vaccination of the Population in the Republic of Macedonia. KNOWLEDGE-International Journal 2018, 23, 461–466. [Google Scholar]
- Mustafa, Z.; Memeti, S.; Karadzovski, Z.; Arsova Sarafinovska, Z.; Mihajloska, E.; Anchevska Netkovska, K.; Grozdanova, A. The Influence of Covid-19 Pandemic on the Vaccination of the Population with the Influenza Vaccine in the Republic of North Macedonia. MEDIS – International Journal of Medical Sciences and Research 2022, 1, 49–53. [Google Scholar] [CrossRef]
- Berild, J.; Berg, A.; Bruun, T.; Christensen, A. Barnevaksinasjonsprogrammet i Norge. Rapport for 2021. Barnevaksinasjonsprogrammet i Norge; Oslo, 2022.
- Price, D.; Bonsaksen, T.; Leung, J.; McClure-Thomas, C.; Ruffolo, M.; Lamph, G.; Kabelenga, I.; Ostertun Geirdal, A. Factors Associated with Trust in Public Authorities Among Adults in Norway, United Kingdom, United States, and Australia Two Years after the COVID-19 Outbreak. Int J Public Health 2023, 68. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.; Price, D.; McClure-Thomas, C.; Bonsaksen, T.; Ruffolo, M.; Kabelenga, I.; Lamph, G.; Geirdal, A.Ø. Motivation and Hesitancies in Obtaining the COVID-19 Vaccine—A Cross-Sectional Study in Norway, USA, UK, and Australia. Vaccines (Basel) 2023, 11, 1086. [Google Scholar] [CrossRef] [PubMed]
- Nybru Gleditsch, R.; Skogset Ofitserova, T.; Aubrey White, R.; Karoline Råberg Kjøllesdal, M.; Dvergsdal, E.; Hansen, B.T.; Askeland Winje, B. Vaccine Coverage among Children Born to Immigrant Parents in Norway, 2000–2020. Vaccine 2024, 42, 3049–3056. [Google Scholar] [CrossRef]
- Melović, B.; Stojanović, A.J.; Vulić, T.B.; Baynazoğlu, M.E. Perceptions and Attitudes of Parents Toward Vaccination of Children in Western Balkan Countries: Trust in Function of Improving Public Health. Balkan Med J 2020. [Google Scholar] [CrossRef] [PubMed]
- Jenness, S.M.; Aavitsland, P.; White, R.A.; Winje, B.A. Measles Vaccine Coverage among Children Born to Somali Immigrants in Norway. BMC Public Health 2021, 21, 668. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Vaccination schedule for Poland https://immunizationdata.who.int/global/wiise-detail-page/vaccination-schedule-for-country_name?DISEASECODE=&TARGETPOP_GENERAL= (accessed 2024 -10 -25).
- Finnegan, G. MMR rates fall in Poland – despite mandatory vaccination rules https://www.vaccinestoday.eu/stories/mmr-rates-fall-poland-despite-mandatory-vaccination-rules/ (accessed 2024 -10 -25).
- Ganczak, M.; Kalinowski, P.; Pasek, O.; Duda-Duma, Ł.; Sobieraj, E.; Goławski, J.; Biesiada, D.; Jansen, D.; Vervoort, J.P.M.; Edelstein, M.; Kowalska, M. Health System Barriers to Child Mandatory and Optional Vaccination among Ukrainian Migrants in Poland in the Context of MMR and HPV Vaccines—A Qualitative Study. Int J Environ Res Public Health 2022, 20, 712. [Google Scholar] [CrossRef] [PubMed]
- Iova, C.F.; Badau, D.; Daina, M.D.; Șuteu, C.L.; Daina, L.G. Knowledge, Attitudes, Intentions and Vaccine Hesitancy among Postpartum Mothers in a Region from the Northwest of Romania. Vaccines (Basel) 2023, 11, 1736. [Google Scholar] [CrossRef]
- Herdea, V.; Tarciuc, P.; Ghionaru, R.; Lupusoru, M.; Tataranu, E.; Chirila, S.; Rosu, O.; Marginean, C.O.; Leibovitz, E.; Diaconescu, S. Vaccine Hesitancy Phenomenon Evolution during Pregnancy over High-Risk Epidemiological Periods—“Repetitio Est Mater Studiorum. ” Vaccines (Basel) 2023, 11, 1207. [Google Scholar] [CrossRef] [PubMed]
- Stanescu, A.; Ruta, S.M.; Cernescu, C.; Pistol, A. Suboptimal MMR Vaccination Coverages—A Constant Challenge for Measles Elimination in Romania. Vaccines (Basel) 2024, 12, 107. [Google Scholar] [CrossRef] [PubMed]
- Veljkovic, M.; Loncarevic, G.; Kanazir, M.; Kisic-Tepavcevic, D.; Gazibara, T. Trend in Mandatory Immunisation Coverage: Linear and Joinpoint Regression Approach, Serbia, 2000 to 2017. Eurosurveillance 2021, 26. [Google Scholar] [CrossRef] [PubMed]
- Milošević Đorđević, J.; Mari, S.; Vdović, M.; Milošević, A. Links between Conspiracy Beliefs, Vaccine Knowledge, and Trust: Anti-Vaccine Behavior of Serbian Adults. Soc Sci Med 2021, 277, 113930. [Google Scholar] [CrossRef]
- Aritonovic Pribakovic, J.; Katanic, N.; Ilic, A.; Stojanovic Tasic, M.; Mitic, N.R.; Mirkovic, M.; Radomirovic, D.; Milentijevic, M.; Mirkovic, M.; Katanic, R. The Measles Epidemic in Northern Kosovo and Metohija, Serbia, October 2017−August 2019. The Journal of Infection in Developing Countries 2022, 16, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Burgess, C.; Lisul, B.; Pawaskar, M.; Petigara, T.; Murtagh, J.; Kanazir, M.; Loncarevic, G.; Carias, C. Impact of the COVID-19 Pandemic on Measles Vaccination Coverage and Estimated Catch-up Efforts for Serbia. Pediatric Infectious Disease Journal 2024, 43, 1011–1017. [Google Scholar] [CrossRef]
- Loncarevic, G.S.; Jovanovic, A.L.; Kanazir, M.S.; Kisic Tepavcevic, D.B.; Maric, G.D.; Pekmezovic, T.D. Are Pediatricians Responsible for Maintaining High MMR Vaccination Coverage? Nationwide Survey on Parental Knowledge and Attitudes towards MMR Vaccine in Serbia. PLoS One 2023, 18, e0281495. [Google Scholar] [CrossRef]
- Štrbac, M.; Vuković, V.; Pustahija, T.; Nikolić, N.; Rajčević, S.; Ilić, S.; Dugandžija, T.; Patić, A.; Ristić, M.; Petrović, V. Motives and Attitudes of Parents toward HPV Vaccination: Results from the Initial Period of HPV Vaccine Rollout in Serbia. PLoS One 2023, 18, e0287295. [Google Scholar] [CrossRef]
- Kregar Velikonja, N.; Dobrowolska, B.; Stanisavljević, S.; Erjavec, K.; Globevnik Velikonja, V.; Verdenik, I. Attitudes of Nursing Students towards Vaccination and Other Preventive Measures for Limitation of COVID-19 Pandemic: Cross-Sectional Study in Three European Countries. Healthcare 2021, 9, 781. [Google Scholar] [CrossRef]
- Moraga-Llop, F.A.; Fernández-Prada, M.; Grande-Tejada, A.M.; Martínez-Alcorta, L.I.; Moreno-Pérez, D.; Pérez-Martín, J.J. Recuperando Las Coberturas Vacunales Perdidas En La Pandemia de COVID-19. Vacunas 2020, 21, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Garces-Sanchez, M.; Cilleruelo-Ortega, M.J.; Hernandez-Merino, A.; Alvarez-Garcia, F.J. The Impact of the Pandemic on Vaccination Coverage in Spain: A Challenge for Pediatrics and Public Health. Anales de Pediatría (English Edition) 2023. [Google Scholar] [CrossRef] [PubMed]
- Burgaya-Subirana, S.; Balaguer, M.; Miró Catalina, Q.; Sola, L.; Ruiz-Comellas, A. Influenza Vaccination Coverage in Children: How Has COVID-19 Influenced It? A Review of Five Seasons (2018–2023) in Central Catalonia, Spain. Vaccines (Basel) 2024, 12, 925. [Google Scholar] [CrossRef]
- Gómez-Acebo, I.; Barquín-Ruiz, A.; Llorente, S.; Alonso-Molero, J.; Llorca, J.; Cabero-Perez, M.J.; Dierssen-Sotos, T. The Impact of the COVID-19 Pandemic on Childhood Vaccination Rates and the Role of Sociodemographic Factors: A Cohort Study. Vaccine 2024, 42, 126207. [Google Scholar] [CrossRef] [PubMed]
- Falcon, M.; Rodríguez-Blázquez, C.; Romay-Barja, M.; Ayala, A.; Burgos, A.; De Tena-Dávila, M.J.; Forjaz, M.J. COVID-19 Vaccine Hesitancy in Spain and Associated Factors. Front Public Health 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Ganem, F.; Folch, C.; Colom-Cadena, A.; Bordas, A.; Alonso, L.; Soriano-Arandes, A.; Casabona, J. Determinants of COVID-19 Vaccine Hesitancy among Students and Parents in Sentinel Schools Network of Catalonia, Spain. PLoS One 2023, 18, e0282871. [Google Scholar] [CrossRef]
- Zürcher, S.J.; Signorell, A.; Léchot-Huser, A.; Aebi, C.; Huber, C.A. Childhood Vaccination Coverage and Regional Differences in Swiss Birth Cohorts 2012–2021: Are We on Track? Vaccine 2023, 41, 7226–7233. [Google Scholar] [CrossRef] [PubMed]
- Seiler, M.; Goldman, R.D.; Staubli, G.; Hoeffe, J.; Gualco, G.; Manzano, S. Parents’ Intent to Vaccinate against Influenza during the COVID-19 Pandemic Im Two Regions in Switzerland. Swiss Med Wkly 2021, 151, w20508. [Google Scholar] [CrossRef]
- Baysson, H.; Pullen, N.; De Mestral, C.; Semaani, C.; Pennacchio, F.; Zaballa, M.-E.; L’Huillier, A.G.; Lorthe, E.; Guessous, I.; Stringhini, S.; The Specchio-COVID19 study group. Parental Willingness to Have Children Vaccinated against COVID-19 in Geneva, Switzerland: A Cross-Sectional Population-Based Study. Swiss Med Wkly 2023, 153, 40049. [Google Scholar] [CrossRef] [PubMed]
- Durmaz, N.; Suman, M.; Ersoy, M.; Örün, E. Parents’ Attitudes toward Childhood Vaccines and COVID-19 Vaccines in a Turkish Pediatric Outpatient Population. Vaccines (Basel) 2022, 10, 1958. [Google Scholar] [CrossRef] [PubMed]
- Dinleyici, E.C.; Borrow, R.; Safadi, M.A.P.; van Damme, P.; Munoz, F.M. Vaccines and Routine Immunization Strategies during the COVID-19 Pandemic. Hum Vaccin Immunother 2021, 17, 400–407. [Google Scholar] [CrossRef]
- Kara, A.; İlbay, S.; Topaç, O.; Arabulan, E.A.; Tezer, H.; Tavukçu, N.; Şimşek, Ç. Alteration in Vaccination Rates and an Evaluation of Physicians’ Perceptions of the Possible Impact of the SARS-CoV-2 Pandemic on Childhood Vaccinations in Ankara, Turkey. Hum Vaccin Immunother 2021, 17, 3457–3462. [Google Scholar] [CrossRef]
- Akbulut, S.; Boz, G.; Ozer, A.; Sahin, T.T.; Colak, C. Evaluation of the Turkish Population’s Perspective on COVID-19 Vaccine Hesitancy and Routine Childhood Vaccine Applications: National Survey Study. Vaccines (Basel) 2023, 11, 779. [Google Scholar] [CrossRef]
- Ota, M.O.C.; Badur, S.; Romano-Mazzotti, L.; Friedland, L.R. Impact of COVID-19 Pandemic on Routine Immunization. Ann Med 2021, 53, 2286–2297. [Google Scholar] [CrossRef]
- Duran, S.; Duran, R.; Acunaş, B.; Şahin, E.M. Changes in Parents’ Attitudes towards Childhood Vaccines during COVID-19 Pandemic. Pediatrics International 2023, 65. [Google Scholar] [CrossRef]
- Romaniuk, P.; Semigina, T. Ukrainian Health Care System and Its Chances for Successful Transition from Soviet Legacies. Global Health 2018, 14, 116. [Google Scholar] [CrossRef] [PubMed]
- Osborne, J.; Goncharova, M.; Germanovich, M.; Koshalko, O.; Kutalek, R.; Dückers, M.; Rodyna, R. Locating Vaccine Uptake and Public Participation in Ukraine: An Exploratory Qualitative Study on Attitudes and Barriers to Early Childhood Vaccination. Glob Public Health 2023, 18. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Torchia, G.; Nardi, A. Vaccine Hesitancy among Ukrainian Refugees. Journal of preventive medicine and hygiene 2022, 63, E566–E572. [Google Scholar] [CrossRef]
- Vignier, N.; Halley des Fontaines, V.; Billette de Villemeur, A.; Cazenave-Roblot, F.; Hoen, B.; Chauvin, F.; Lepelletier, D.; Chidiac, C.; Billaud, E. Public Health Issues and Health Rendezvous for Migrants from Conflict Zones in Ukraine: A French Practice Guideline. Infect Dis Now 2022, 52, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Loboda, A. Systematic Review of Health and Disease in Ukrainian Children Highlights Poor Child Health and Challenges for Those Treating Refugees. Acta Paediatr 2022, 111, 1341–1353. [Google Scholar] [CrossRef]
- Rzymski, P.; Falfushynska, H.; Fal, A. Vaccination of Ukrainian Refugees: Need for Urgent Action. Clinical Infectious Diseases 2022, 75, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.; Pitchforth, E.; Edwards, N.; Alderwick, H.; McGuire, A.; Mossialos, E. United Kingdom: Health System Review. Health Syst Transit 2022, 24, 1–194. [Google Scholar]
- Vagnoni, C.; Rough, E.; Bunn, S. UK Vaccination Policy; House of Commons Library: London, 2022. [Google Scholar]
- Measles in These Days Can Cause a Lot of Anxiety. Lancet Microbe 5, e203.
- Hobson-West, P. Understanding Vaccination Resistance: Moving beyond Risk. Health Risk Soc 2003, 5, 273–283. [Google Scholar] [CrossRef]
- Petts, J.; Niemeyer, S. Health Risk Communication and Amplification: Learning from the MMR Vaccination Controversy. Health Risk Soc 2004, 6, 7–23. [Google Scholar] [CrossRef]
- Casiday, R.; Cresswell, T.; Wilson, D.; Panter-Brick, C. A Survey of UK Parental Attitudes to the MMR Vaccine and Trust in Medical Authority. Vaccine 2006, 24, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.A.; Mahgoub, H.; Shankar, A.G. Vaccine Acceptance: The UK Perspective. Hum Vaccin Immunother 2013, 9, 2658–2660. [Google Scholar] [CrossRef] [PubMed]
- Torracinta, L.; Tanner, R.; Vanderslott, S. MMR Vaccine Attitude and Uptake Research in the United Kingdom: A Critical Review. Vaccines (Basel) 2021, 9, 402. [Google Scholar] [CrossRef] [PubMed]
- Sythes, L.; Bedford, H. Motherhood and Vaccine Refusal in the United Kingdom: A New Examination of Gender, Identity and the Journey to Contemporary Non-vaccination. Child Care Health Dev 2022, 48, 979–989. [Google Scholar] [CrossRef]
- Cookson, D.; Jolley, D.; Dempsey, R.C.; Povey, R. A Social Norms Approach Intervention to Address Misperceptions of Anti-Vaccine Conspiracy Beliefs amongst UK Parents. PLoS One 2021, 16, e0258985. [Google Scholar] [CrossRef]
- Mellott, C.E.; Jaworski, R.; Carrico, J.; Talbird, S.E.; Dobrowolska, I.; Golicki, D.; Bencina, G.; Clinkscales, M.; Karamousouli, E.; Eiden, A.L.; Sabale, U. Public Health Impact and Return on Investment of the Pediatric Immunization Program in Poland. Expert Rev Vaccines 2023, 22, 1114–1125. [Google Scholar] [CrossRef]
- Autzen, B.; Dineen, K.; Vaughan, D. Vaccinating Children: Fairness and Childism. Lancet Infect Dis 2021, 21, 1354–1355. [Google Scholar] [CrossRef]
- Rigby, M.J.; Chronaki, C.E.; Deshpande, S.S.; Altorjai, P.; Brenner, M.; Blair, M.E. European Union Initiatives in Child Immunization— the Need for Child Centricity, e-Health and Holistic Delivery. Eur J Public Health 2020, 30, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Lentakis, E.; Seale, H.; Lazarus, R.; Mounier-Jack, S. Exploring the Attitudes and Practices of Adult Service Users and Providers towards Vaccination in Non-Primary Care Settings: A Mixed Methods Scoping Review. Vaccine 2024, 42, 126472. [Google Scholar] [CrossRef]
- Tesorone, M.; Ungaro, C.; Graziano, L.; Vitagliano, A.; Luminoso, I.; Corvino, M.; Papa, M.; Verdoliva, C. Vaccinations at Home: A New Strategy to Contain Vaccine Hesitancy? The Experience of ASL Napoli 1 Centro, Italy. Ann Ig 2024. [Google Scholar] [CrossRef]
Figure 6.
Joinpoint regression of DTP3 in Europe: (a) Belgium (b) Bosnia.
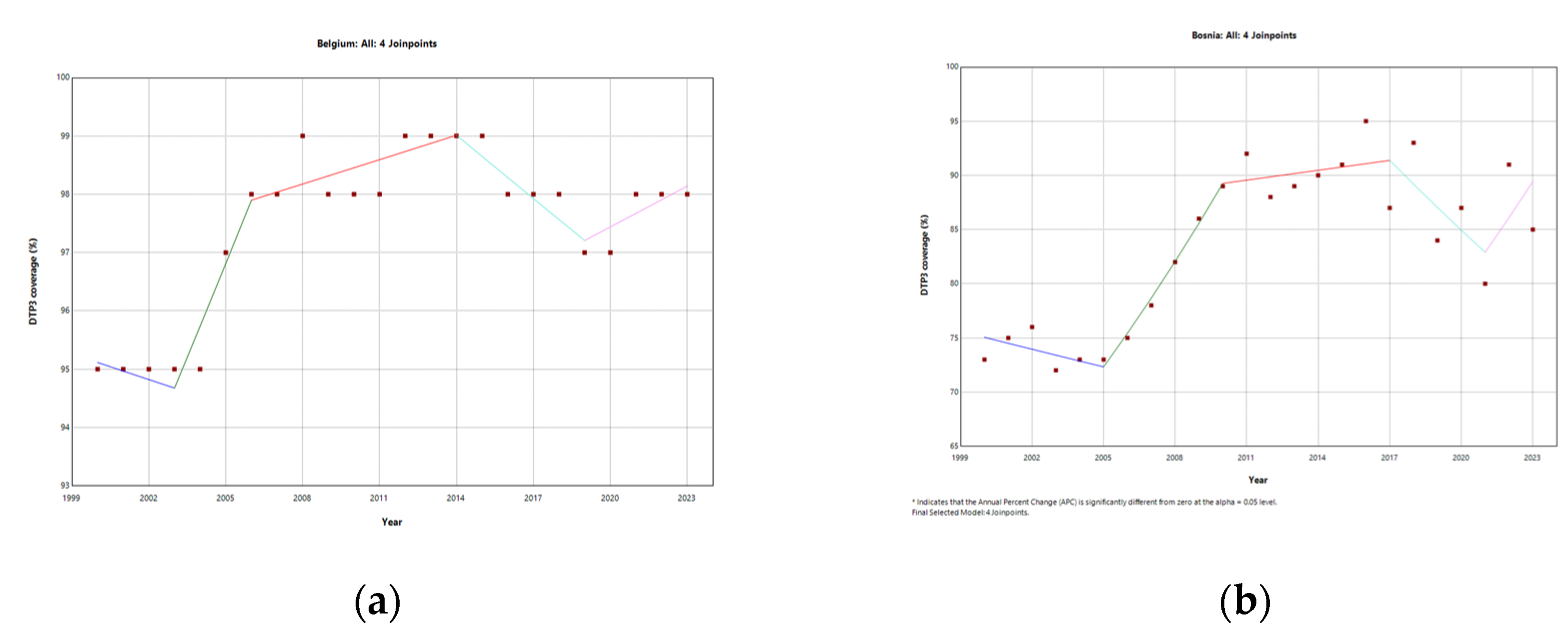
Figure 7.
DTP3 coverage rates (%) changes in Europe in 2019 and 2023.

Figure 8.
Segmented regression of DTP3 coverage in Europe.
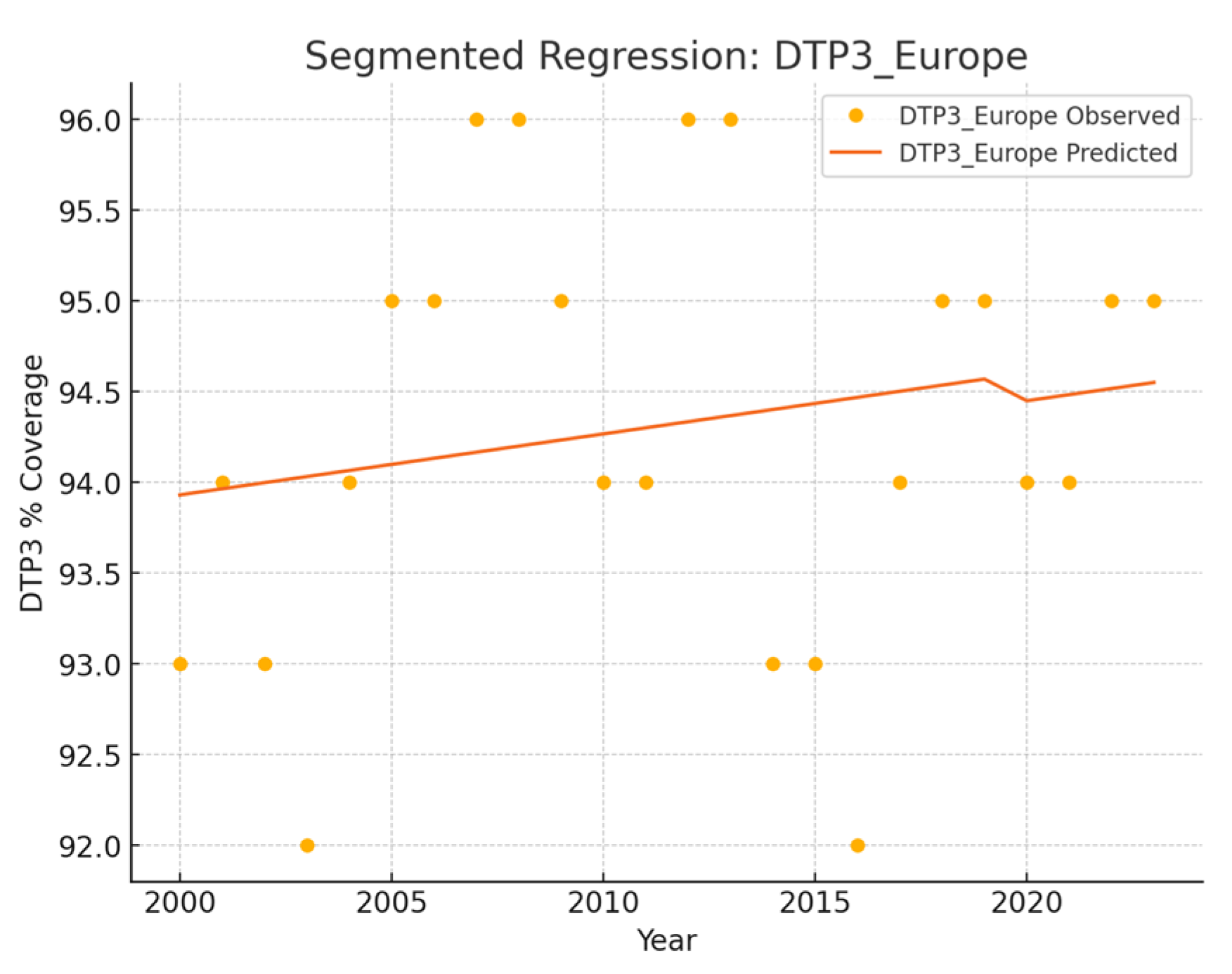
Figure 9.
Segmented regression of DTP3 coverage: (a) Northern (b) Southern Europe (c) Eastern Europe (d) Western Europe.
Figure 9.
Segmented regression of DTP3 coverage: (a) Northern (b) Southern Europe (c) Eastern Europe (d) Western Europe.
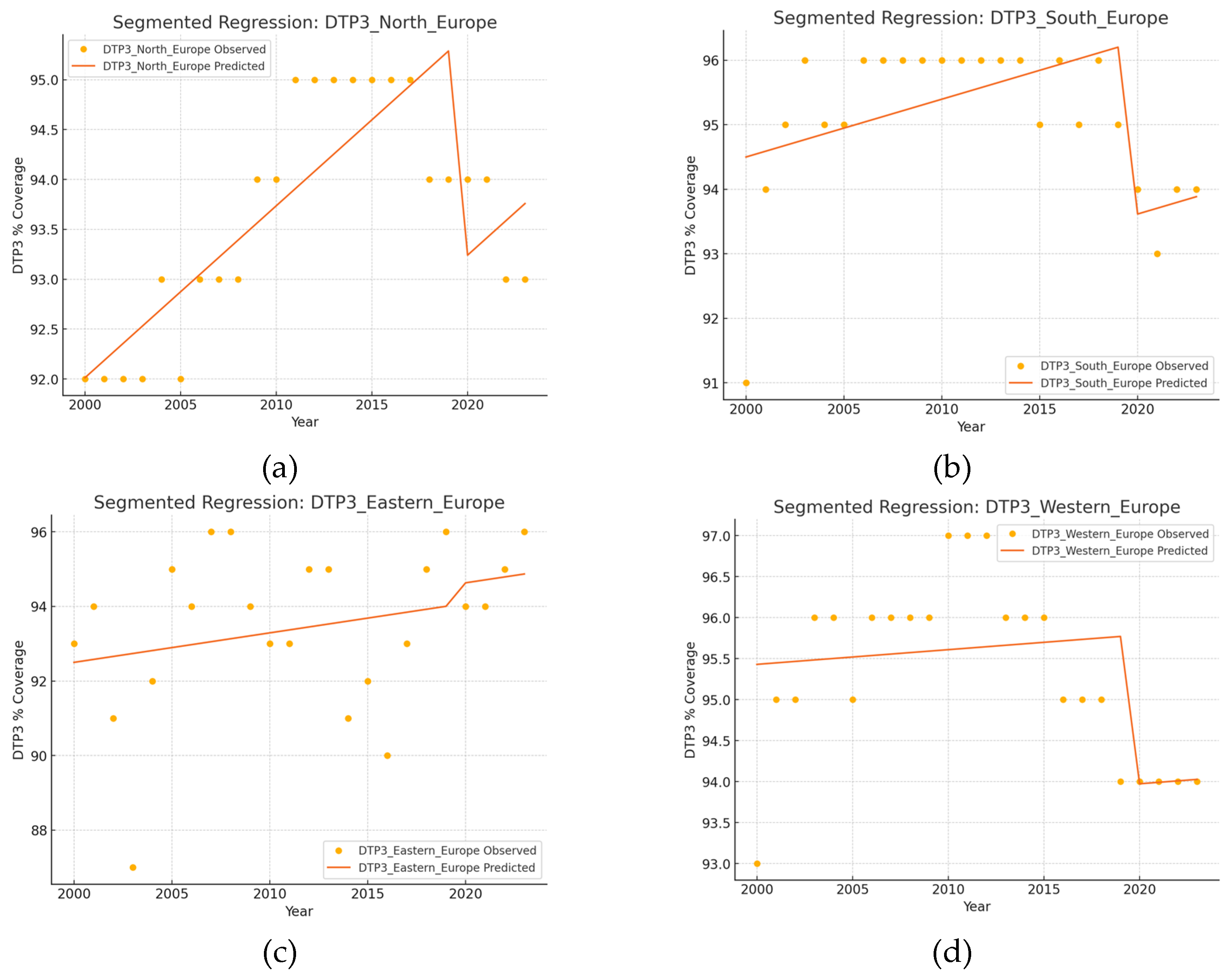
Figure 10.
Segmented regression of DTP3 coverage: (a) San Marino (b) Ukraine (c) Iceland (d) Slovakia.
Figure 10.
Segmented regression of DTP3 coverage: (a) San Marino (b) Ukraine (c) Iceland (d) Slovakia.
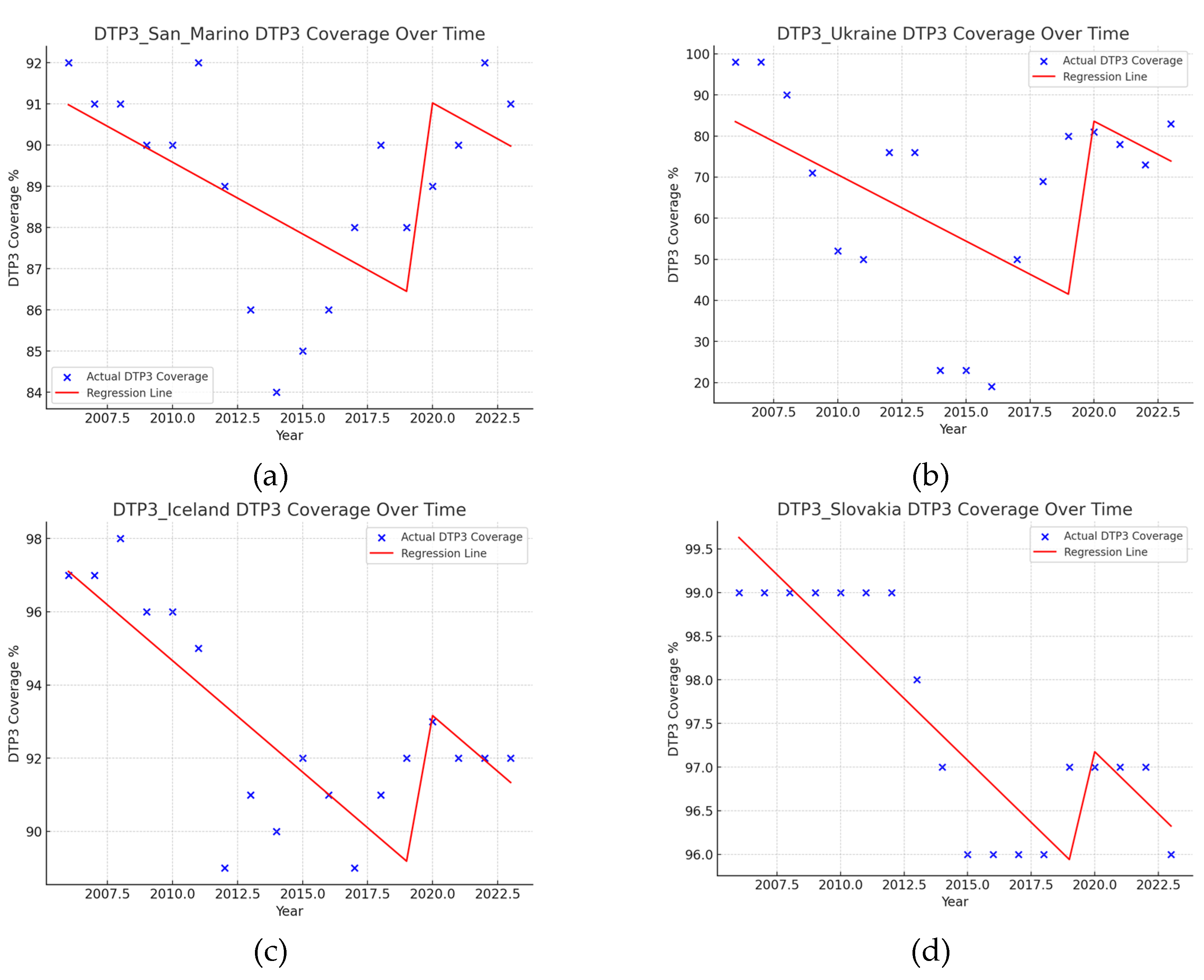
Figure 11.
Segmented regression of DTP3 coverage: (a) Albania (b) Austria (c) Cyprus (d) Estonia (e) Ireland (f) Lithuania.
Figure 11.
Segmented regression of DTP3 coverage: (a) Albania (b) Austria (c) Cyprus (d) Estonia (e) Ireland (f) Lithuania.
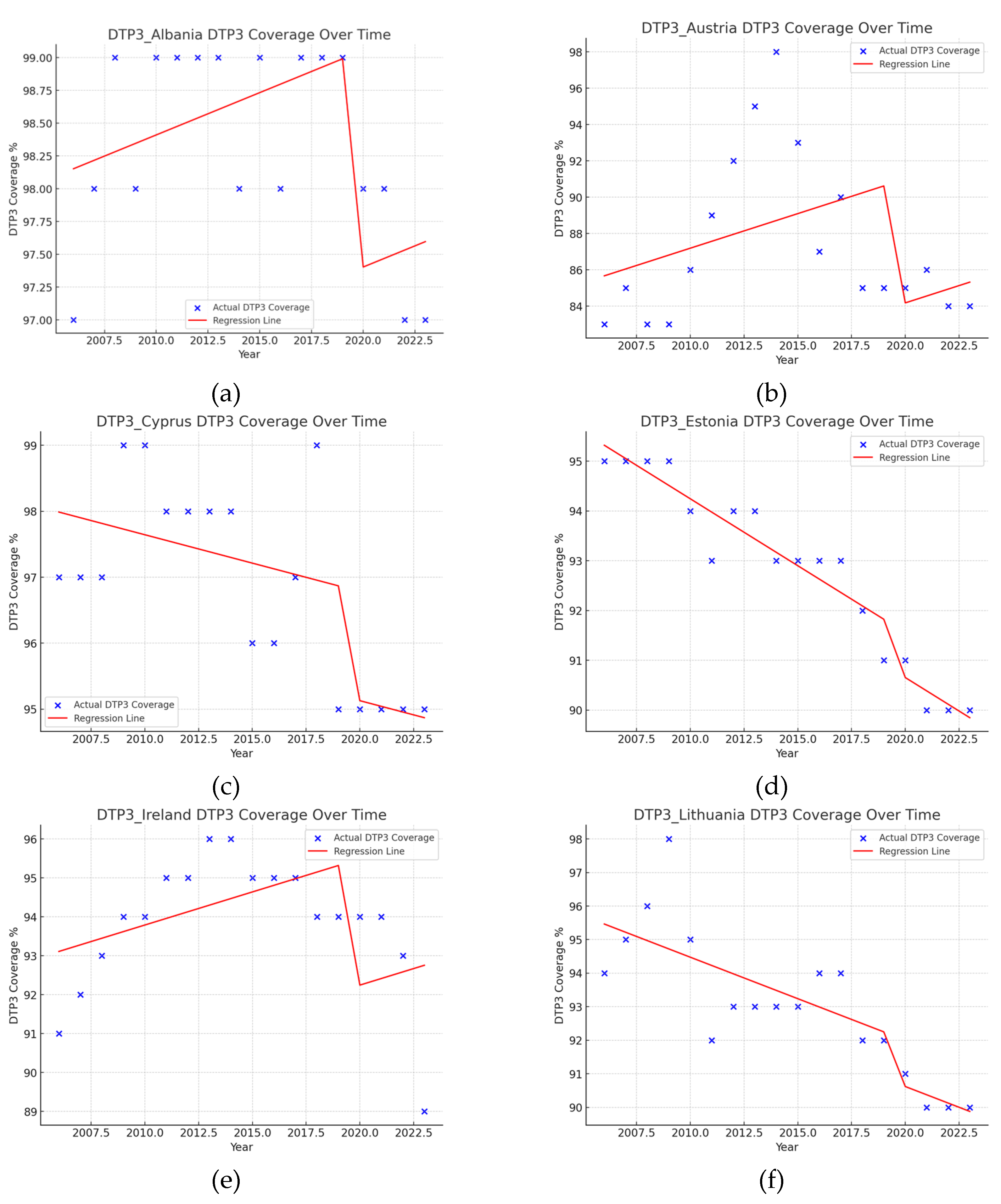
Figure 12.
Segmented regression of DTP3 coverage: (a) Montenegro (b) North Macedonia (c) Poland (d) Republic of Moldova (e) Slovenia (f) Lithuania (g) Türkiye (h) United Kingdom.
Figure 12.
Segmented regression of DTP3 coverage: (a) Montenegro (b) North Macedonia (c) Poland (d) Republic of Moldova (e) Slovenia (f) Lithuania (g) Türkiye (h) United Kingdom.
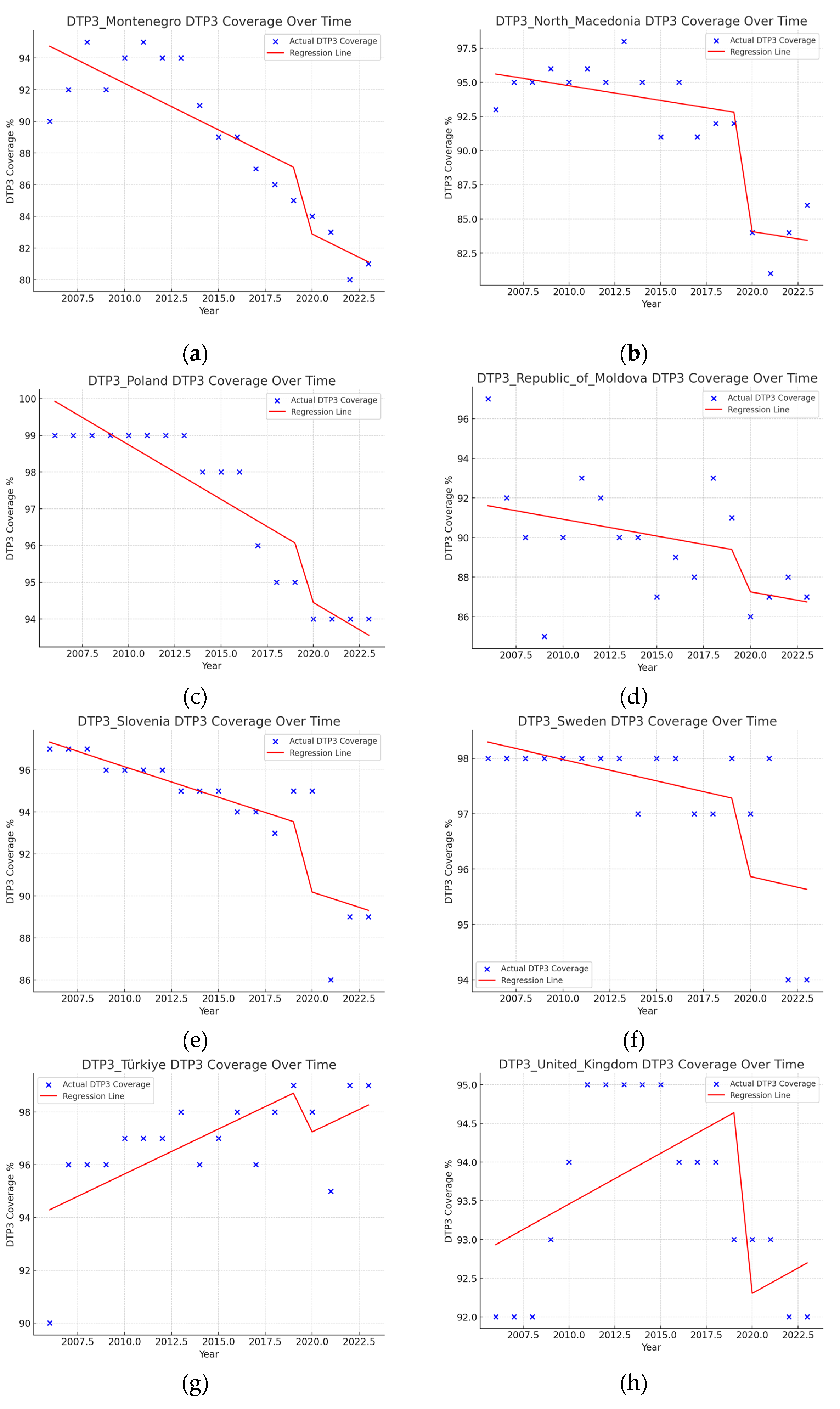

Table 1.
Joinpoint analysis for the DTP3 vaccination Regional rates in Europe, 2000–2023.
| Region | Number of Joint Points (Jointpoints) | APC Total Period | APC1 | APC2 | APC3 | APC4 | APC5 |
|---|---|---|---|---|---|---|---|
| Europe | 0 | 0.03 | - | - | - | - | - |
| North | 3 (2008, 2011, 2016) | 0,11* | 0,18* | 0,65* | 0,02 | -0,31* | - |
| South | 4 (2002, 2009, 2018, 2021) | -0.02 | 2.05* | 0.12* | -0.06 | -0.81* | 0.50 |
| East | 0 | 0.11 | - | - | - | - | - |
| West | 4 (2002, 2008, 2011, 2020) | -0,12 | 1,17* | 0,06 | 0,41 | -0,37* | 0,03 |
*Annual Percent Change (APC) p < 0.05.
Table 2.
Joinpoint analysis for the DTP3 vaccination rates in Europe, 2000–2023.
| Country | Number of Joint Points (Jointpoints) | APC Total Period | APC1 | APC2 | APC3 | APC4 | APC5 |
|---|---|---|---|---|---|---|---|
| Albania | 2 (2011, 2019) | 0.04 | 0.18* | -0.01 | -0.50* | ||
| Andorra | 0 | 0.06 | |||||
| Austria | 3 (2009, 2014, 2017) | 0.19 | 0.1 | 3.0* | -3.8* | -0.5 | |
| Belarus | 2 (2003, 2006) | 0.50 | -13.3* | 11.6* | -0.2 | ||
| Belgium | 4 (2003, 2006, 2014, 2019) | 0.12 | -0.15 | 1.12* | 0.14* | -0.37* | 0.24* |
| Bosnia | 4 (2005, 2010, 2017, 2021) | 0.96 | -0.74 | 4.30* | 0.34 | -2.41* | 3.87* |
| Bulgaria | 1 | -0.21* | 0.76 | -0.31* | |||
| Croatia | 1 (2008) | -0.12 | 0.41* | -0.34* | |||
| Cyprus | 1 (2011) | -0.10 | -0.14 | 0.31* | |||
| Czechia | 1 (2011) | -0.15 | 0.14 | -0.41* | |||
| Denmark | 3 (2004, 2007, 2018) | 0.13 | -0.38 | -2.88* | 0.91* | -0.06 | |
| Estonia | 1 (2007) | -0.21* | 0.33* | -0.37* | |||
| Finland | 2 (2014, 2017) | -0.46* | 0.06 | -3.11* | 0.17 | ||
| France | 4 (2003, 2006, 2013, 2016) | -0.09* | 0.04 | 0.58 | 0.02 | -1.00 | -0.00 |
| Germany | 3 (2003, 2010, 2017) | -0.21* | 2.18* | -0.05 | -0.76* | 0.02 | |
| Greece | 2 (2003, 2007) | 0.33 | 1.71* | 1.36 | -0.00 | ||
| Hungary | 0 | 0.00 | 0.27 | -2.55* | 0.18 | ||
| Iceland | 2 (2009, 2012) | -0.30* | 0.27 | -2.55* | 0.18 | ||
| Ireland | 4 (2002, 2005, 2013, 2021) | 0.40* | -1.49* | 2.95* | 0.69* | -0.28* | |
| Italy | 1 (2003) | 0.09 | 2.85* | -0.08 | |||
| Latvia | 1 (2011) | -0.01 | -0.55* | 0.46* | |||
| Lithuania | 1 (2009) | -0.21* | 0.14 | -0.40* | |||
| Luxembourg | 0 | 0.01 | |||||
| Malta | 3 (2005, 2008, 2012) | 0.60 | -0.77 | -9.17* | 9.46* | -0.06 | |
| Monaco | 0 | 0.00 | |||||
| Montenegro | 1 (2011) | -0.91* | 0.94* | -1.43* | |||
| Netherlands | 0 | 0.29 | |||||
| North Macedonia | 1 (2013) | -0.48* | 0.21 | -1.47* | |||
| Norway | 0 | 0.29 | |||||
| Poland | 2 (2013, 2020) | -0.23* | 0.06 | -0.76* | -0.03 | ||
| Portugal | 0 | 0.14 | |||||
| Republic of Moldova | 0 | -0.50 | |||||
| Romania | 0 | -0.83 | |||||
| Russian Federation | 2 (2007, 2011) | 0.01 | 0.36* | -0.32* | 0.00 | ||
| San Marino | 1 (2015) | -0.40* | -0.92* | 0.90* | |||
| Serbia | 0 | -0.02 | |||||
| Slovakia | 3 (2012, 2015, 2021) | -0.15 | 0.00 | -1.10* | 0.23* | -0.50* | |
| Slovenia | 1 (2008) | -0.16 | 0.86* | -0.57* | |||
| Spain | 1 (2012, 2016) | -0.16* | 1.24 | -0.07 | -0.61 | ||
| Sweden | 1 (2021) | -0.14* | -0.09* | -1.94* | |||
| Switzerland | 3 (2003, 2012, 2021) | 0.16* | -0.01 | 0.36* | 0.00 | -0.45* | |
| Türkiye | 2 (2003, 2006) | 0.89* | -6.17* | 9.35* | 0.18 | ||
| Ukraine | 3 (2012, 2015, 2018) | -2.63 | -3.75 | -35.32* | 56.47* | ||
| United Kingdom | 2 (2008, 2012) | 0.11* | 0.18 | 0.91* | -0.34* | ||
| * Annual Percent Change (APC) p < 0.05 |
Table 3.
DTP3 coverage rates (%) changes in European countries between 2019 and 2023.
| 2019 | 2023 | |||||
|---|---|---|---|---|---|---|
| Country | DTP3 (%) | Births (n) | DTP3 (%) | Births (n) | Change in DTP3 (%) | p † |
| Albania | 99 | 29773 | 97 | 28538 | -2 | <0.001 |
| Andorra | 99 | 590 | 98 | 569 | -1 | ns |
| Austria | 85 | 84744 | 84 | 84132 | -1 | <0.001 |
| Belarus | 98 | 93218 | 98 | 86154 | 0 | ns |
| Belgium | 97 | 116136 | 98 | 116823 | 1 | <0.001 |
| Bosnia and Herzegovina |
73 | 29754 | 73 | 26279 | 0 | ns |
| Bulgaria | 93 | 61637 | 92 | 55495 | -1 | <0.001 |
| Croatia | 94 | 36700 | 93 | 33537 | -1 | <0.001 |
| Cyprus | 95 | 13237 | 95 | 12348 | 0 | ns |
| Czechia | 97 | 109738 | 94 | 99736 | -3 | <0.001 |
| Denmark | 97 | 60455 | 97 | 65003 | 0 | ns |
| Estonia | 91 | 14158 | 90 | 13102 | -1 | 0.005 |
| Finland | 91 | 45790 | 91 | 47143 | 0 | ns |
| France | 96 | 701300 | 96 | 671363 | 0 | ns |
| Germany | 91 | 771867 | 91 | 755129 | 0 | ns |
| Greece | 99 | 81148 | 99 | 76080 | 0 | ns |
| Hungary | 99 | 92375 | 99 | 104762 | 0 | ns |
| Iceland | 92 | 4402 | 92 | 4553 | 0 | ns |
| Ireland | 94 | 60463 | 89 | 56728 | -5 | <0.001 |
| Italy | 96 | 418113 | 95 | 406243 | -1 | <0.001 |
| Latvia | 99 | 18693 | 98 | 15996 | -1 | <0.001 |
| Lithuania | 92 | 28075 | 90 | 25605 | -1 | <0.001 |
| Luxembourg | 99 | 6167 | 99 | 6724 | -2 | ns |
| Malta | 98 | 4318 | 98 | 4863 | 0 | ns |
| Monaco | 99 | 331 | 99 | 323 | 0 | ns |
| Montenegro | 85 | 7429 | 81 | 6773 | 0 | <0.001 |
| Netherlands (Kingdom of the) | 94 | 169827 | 92 | 182435 | -2 | <0.001 |
| North Macedonia | 92 | 20447 | 86 | 19769 | -6 | <0.001 |
| Norway | 97 | 54384 | 96 | 54464 | -1 | <0.001 |
| Poland | 95 | 382527 | 94 | 423741 | -1 | <0.001 |
| Portugal | 99 | 85439 | 99 | 79465 | 0 | ns |
| Republic of Moldova |
91 | 40266 | 87 | 49667 | -4 | <0.001 |
| Romania | 88 | 203903 | 78 | 214232 | -10 | <0.001 |
| Russian Federation |
97 | 1486730 | 97 | 1375609 | 0 | ns |
| San Marino | 88 | 209 | 91 | 199 | 3 | ns |
| Serbia | 97 | 69672 | 93 | 65195 | -4 | <0.001 |
| Slovakia | 97 | 57020 | 96 | 62451 | -1 | <0.001 |
| Slovenia | 95 | 19865 | 89 | 18520 | -6 | <0.001 |
| Spain | 95 | 354681 | 93 | 351908 | -2 | <0.001 |
| Sweden | 98 | 114109 | 94 | 113685 | -4 | <0.001 |
| Switzerland | 96 | 85930 | 95 | 86100 | -1 | <0.001 |
| Türkiye | 99 | 1303201 | 99 | 1214053 | 0 | ns |
| Ukraine | 80 | 353538 | 83 | 184455 | 3 | <0.001 |
| United Kingdom | 93 | 709079 | 92 | 677708 | -1 | <0.001 |
ns= no significant, †Chi-square Test.
Table 4.
Segmented regression of DTP 3 coverage in European Regions.
| Region | Intercept | Year | Pandemic |
|---|---|---|---|
| Europe | 26,77 | 0,0336 | -0,1530 |
| North Europe | -252,76 | 0,1724*** | -2,2187*** |
| South Europe | -84,61 | 0,0896* | -2,6746*** |
| Eastern Europe | -65,71 | 0,0791 | 0,5507 |
| Western Europe | 59,61 | 0,0179 | -1,8149* |
*p < 0.05 **p < 0.01 ***p < 0.001.
Table 5.
Segmented regression of DTP 3 coverage in European Countries.
| Nation | Intercept | Year | Pandemic | Interaction |
| Albania | -31.2673 | 0.0645 | -1.6521** | N/A |
| Andorra | -252.7788 | 0.1742 | -0.8535 | N/A- |
| Austria | -677.9055 | 0.3806 | -6.8187 | N/A- |
| Belarus | -23.6828 | 0.0602 | -0.2919 | N/A- |
| Belgium | 145.8932 | -0.0237 | -0.3228 | N/A- |
| Croatia | 687.9301 | -0.2946*** | 0.4016 | N/A- |
| Cyprus | 270.5469 | -0.0860 | -1.6544† | N/A- |
| Czechia | 569.6045 | -0.2344*** | -0.9975 | N/A- |
| Denmark | -1253.2089 | 0.6688*** | -1.8051 | N/A- |
| Estonia | 634.5661 | -0.2688*** | -0.9021* | N/A- |
| Finland | 1455.1928 | -0.6753*** | 0.1131 | N/A- |
| France | 643.1797 | -0.2710*** | 0.5816 | N/A |
| Germany | 1058.9201 | -0.4796*** | 1.5304* | N/A- |
| Greece | 42.6651 | 0.0280† | -0.1802 | N/A- |
| Hungary | 99.0000 | 0.0000*** | 0.0000 | N/A- |
| Iceland | 1317.9547 | -0.6086*** | 4.5846** | N/A- |
| Ireland | -247.6943 | 0.1699 | -3.2433* | -1.8087** |
| Italy | 355.2488 | -0.1290* | 0.0899 | N/A |
| Latvia | -494.0307 | 0.2925† | -0.7037 | N/A- |
| Lithuania | 591.5722 | -0.2473** | -1.3813 | N/A- |
| Luxembourg | 99.0000 | 0.0000 | 0.0000 | N/A- |
| Malta | -3965.2956 | 2.0150*** | -9.8854 | N/A- |
| Monaco | 99.0000 | 0.0000 | 0.0000 | N/A- |
| Montenegro | 1272.4608 | -0.5871** | -3.6447† | N/A- |
| Netherlands (Kingdom of the) | 667.1475 | -0.2839*** | 0.1977 | N/A- |
| North Macedonia | 527.0100 | -0.2151*** | -8.5288*** | N/A- |
| Norway | -368.5200 | 0.2301*** | 0.1076 | N/A- |
| Poland | 695.2581 | -0.2968*** | -1.3290† | N/A- |
| Portugal | -222.5545 | 0.1591*** | -0.1465 | N/A |
| Republic of Moldova | 432.4086 | -0.1699 | -1.9710 | N/A- |
| Romania | 1960.9631 | -0.9290*** | 1.0756 | N/A- |
| Russian Federation | 270.4040 | -0.0860*** | 0.4885* | N/A- |
| San Marino | 789.8433 | -0.3484* | 4.9212* | N/A- |
| Serbia | 179.9877 | -0.0430 | -0.0415 | N/A- |
| Slovakia | 669.0760 | -0.2839*** | 1.5191* | N/A- |
| Slovenia | 679.7028 | -0.2903* | -3.0657* | N/A- |
| Spain | 321.4823 | -0.1118* | -2.4221** | N/A- |
| Sweden | 253.5922 | -0.0774† | -1.3389† | -1.2494*** |
| Switzerland | -190.1452 | 0.1419*** | -1.0274** | -0.4516* |
| Türkiye | -587.3172 | 0.3398** | -1.8081 | N/A |
| Ukraine | 6563.0914 | -3.2301* | 45.3210* | N/A- |
| United Kingdom | -170.2197 | 0.1312† | -2.4664** | N/A- |
N/A= No interaction †p < 0.10 *p < 0.05 **p < 0.01 ***p < 0.001.
Table 6.
Comparison of the findings of Segmented Regression, Comparison of rates 2019-23 and Joint Point.
Table 6.
Comparison of the findings of Segmented Regression, Comparison of rates 2019-23 and Joint Point.
| Country | Segmented | Chi-Square | JoinPoint |
| Albania | - | - | - |
| Austria | - | - | |
| Belgium | + | + | |
| Bosnia | + | ||
| Bulgaria | - | ||
| Croatia | - | ||
| Cyprus | - | ||
| Czechia | - | ||
| Estonia | - | - | |
| Ireland | - | - | - |
| Italy | - | ||
| Latvia | |||
| Lithuania | - | - | |
| Moldavia | - | - | |
| Montenegro | - | - | |
| Netherland | - | ||
| North Macedonia | - | - | |
| Norway | - | ||
| Poland | - | - | - |
| Romania | - | ||
| Serbia | - | ||
| Slovakia | - | - | |
| Slovenia | - | - | |
| Spain | - | - | |
| Sweden | - | - | - |
| Switzerland | - | - | - |
| Türkiye | - | ||
| Ukraine | + | ||
| United Kingdom | - | - |
+ increase - decrease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



