
Submitted:
12 November 2024
Posted:
15 November 2024
You are already at the latest version
Abstract
Retinal diseases are characterized by progressive damage to retinal cells, leading to irreversible vision loss. Among these, glaucoma stands out as a multifactorial neurodegenerative disease involving elevated intraocular pressure, retinal ganglion cell apoptosis, and optic nerve damage, ultimately resulting in blindness in both humans and dogs. Stem cell-based therapies have emerged as a promising therapeutic option for such conditions due to their regenerative and neuroprotective potential. These therapies, particularly those based on mesenchymal stem cells, offer the potential to repair and protect retinal tissues through the bioactive molecules (growth factors, cytokines, chemokines) secreted, their secretome. However, research in this field, especially on the use of umbilical cord mesenchymal stem cells’ secretome, remains sparse. Most clinical trials focus on human glaucomatous patients, leaving a significant gap in veterinary patients’ application, especially in dogs, additional research being needed to determine its usefulness in canine glaucoma treatment. Future studies should aim to evaluate these therapies across both human and veterinary contexts, broadening treatment possibilities for glaucoma.
Keywords:
glaucoma
; stem cell-based therapies
; mesenchymal stem cells
; secretome
; umbilical cord mesenchymal stem cells
; regenerative medicine
; veterinary ophtalmology
; veterinary medicine
1. Introduction
1.1. Description and Epidemiology
Retinal pathologies are a wide group of heterogenous degenerative and ischemic conditions that cause retinal cells apoptosis and loss of integrity. Within this diversity of diseases, the retinal degenerative ones (retinitis pigmentosa, diabetic retinopathy, age-related macular degeneration and glaucoma) stand out, since they are the main causes of irreversible vision loss and blindness worldwide, with a special emphasis in glaucoma in both humans and dogs [1,2,3,4,5]. Nowadays, glaucoma affects approximately 80 million people around the globe, and this number is expected to rise to more than 111 million by the year 2040 [2]. Likewise, around 1% of the dogs (2624 affected animals from a total of 294314 purebred dogs included in the study) in North America and more than 50 different pure breeds are affected by this disease [5]. Unfortunately, despite the several therapeutic options available, success rates are very limited, especially in dogs where in advanced stage chronic cases enucleation is sometimes required to improve animals’ welfare and comfort, as this condition is often extremely painful [6].
Glaucoma is a progressive multifactorial neurodegenerative disease known in medicine since antiquity. Hippokrates defined “glaykoseis” as blindness that arises in older individuals and Donders found that elevated intraocular pressure (IOP) caused blindness and named the disease “Glaukoma simplex”, in 1862 [7]. The normal IOP values for dogs and cats usually vary between 15 mmHg and 25 mmHg [8]. Glaucoma is diagnosed when the IOP measured using a tonometer [9] exceeds 30 mmHg [10].
Previously, glaucoma was mainly defined by elevated IOP. However, it is now well established that while increased IOP is a major risk factor, other factors also play a significant role in the disease’s progression and the damage it causes, such as abnormalities in the extracellular matrix of the lamina cribrosa and defects in the blood flow to the optic nerve head (ONH). A notable example is normotensive glaucoma, which exhibits all the characteristics of glaucoma—such as retinal ganglion cell dysfunction and apoptosis, optic nerve damage and degeneration, and progressive vision loss—despite normal IOP [11]. This form of glaucoma is acknowledged in both human [12] and non-human primates [13] and might also occur in dogs as well, although there is lack of published data on this.
1.2. Pathophysiology
Concerning glaucoma pathophysiology, IOP increases due to inadequate drainage of the aqueous humour, which corresponds to the fluid in the anterior and posterior chambers produced by the ciliary body, located behind the iris. This fluid passes through the pupil and exits from the anterior chamber via the iridocorneal angle, which is positioned at the intersection between the cornea and the iris and includes the trabecular meshwork and Schlemm’s canal, this corresponding to the conventional outflow pathway. The unconventional route, or uveoscleral outflow, is estimated to carry 3-82% of total aqueous humor drainage across various species [14].
The production and drainage of aqueous humour occurs nearly at the same rate, ensuring a constant IOP. Glaucoma develops because of inappropriate aqueous humour outflow, and the continuous high IOP promotes retinal ganglion cells’ (RGCs) apoptosis, resulting in functional vision loss due to retinal degeneration [15]. Apoptosis of the RGCs, once initiated, is irreversible. The optic nerve head suffers structural and functional damage over time, including cupping of the optic disc, sectoral retinal nerve fiber layer and neuroretinal rim thinning, confirming the progressive course of the disease [15].
1.3. Types of Glaucoma
Canine glaucoma can be either congenital, primary or secondary. Secondary glaucoma is quite common in veterinary medicine and occurs as a result of other ocular or systemic diseases.
Congenital glaucoma is present at birth (Figure 1), being diagnosed in newborn animals through a complete and comprehensive ophthalmological exam, including gonioscopy on all littermates [10,16,17]. Typically, affected animals display abnormalities in the iridocorneal angle and pectinate ligament dysplasia. In these cases, treatment typically involves laser ciliary body ablation or enucleation, while evisceration and silicone prosthesis implantation can be an option when buphthalmos is mild and the fibrous tunica is preserved [8,10,17]. If the eyes are enucleated, the globes should be examined histologically to confirm the glaucoma’s cause.
Primary glaucoma, the most common presentation in dogs, can also be classified as primary open-angle glaucoma (POAG) or primary angle-closure glaucoma (PACG), being responsible for the major of primary glaucoma cases (Figure 2) [18]. POAG can occur with both elevated and normal IOPs. When the IOP is considered normal (40% of POAG cases), it is referred to as a normotensive glaucoma [11].
Many breeds are predisposed to primary glaucoma in general, including the American Cocker Spaniel, Basset Hound, Beagle, Bouvier des Flandres, Dandie Dinmont Terrier, English Springer Spaniel, Irish Setter, Toy Poodle, Siberian Husky, Alaskan Malamute, Samoyed, Chow Chow, and American Eskimo [19].
POAG is characterized by a typical imbalance between the production and drainage of aqueous humor within the eye. Despite the drainage angle remaining open, impaired drainage leads to a gradual increase in the IOP. A study revealed that some dog breeds, such as the American Cocker Spaniel, Basset Hound, and Siberian Husky, are particularly predisposed to POAG [20].
On the other hand, PACG is characterized by a reduction or closure of the drainage angle or a sudden blockage. This results in a compromised drainage of aqueous humor, causing a rapid increase in the IOP. The elevated pressure damages RGCs, paving the way for the onset of severe and painful eye conditions, including buphthalmia. Notably, PACG is the less common of the two primary glaucoma forms. Dog breeds such as English Springer Spaniel and Chow Chow, may be particularly predisposed to this form of the disease [20].
1.4. Prevalence and Risk Factors
Studies on the prevalence of glaucoma in dogs reveal significant variations across breeds and regions. Research from veterinary medical teaching institutions in North America, using data from the Veterinary Medical Data Base (VMDB) from 1964 to 2002, found substantial breed predispositions to primary glaucoma [21]. During the 38-year research period, the prevalence of primary glaucoma in pure-bred dogs climbed from 0.29% to 0.89% within selected breeds, such as the American Cocker Spaniel and Basset Hound, having notably high prevalence rates of 5.52% and 5.44%, respectively, by the end of the study [21]. These findings highlight the relevance of hereditary variables in the development of glaucoma, especially in breeds like the American Cocker Spaniel, Basset Hound, Boston Terrier, and Wire Fox Terrier, which were consistently amongst the most afflicted [21].
A study from the Veterinary College Hospital in Bangalore (2016-2019) found that glaucoma was responsible for 7.86% of the cases of ocular diseases in dogs, with the highest incidences in crossbred dogs (25%), Pomeranians (21.43%), and Labrador Retrievers (14.29%). Adult dogs (32.14%) and males (60.71%) were more frequently affected [22]. Recognizing these breed- and age-specific risks is crucial for early glaucoma detection, correct and appropriate diagnose and management, underscoring the need for targeted monitoring and potentially specialized therapeutic approaches across different regions or breeds.
Secondary glaucoma is a serious complication that can develop after intraocular disease such as uveitis, neoplasia, anterior lens luxation or following post-cataract surgery in dogs. In the last case the incidence of this condition has been reported to range from 5% to 19% within a two-year postoperative period [23,24,25]. However, in certain dog breeds, such as Boston Terriers, Shih Tzus, and Labrador Retrievers, the likelihood of developing secondary glaucoma after cataract surgery can increase significantly, reaching levels between 29% and 38% [23,24,25,26,27,28,29]. This elevated incidence in specific breeds points to the possibility of a hereditary component influencing the development of this condition. This suggests that genetic factors may play a significant role in the increased risk observed in these breeds.
Glaucoma symptoms vary depending on the stage of the illness, with acute and chronic phases exhibiting different symptoms. Early recognition of these symptoms, which vary from ocular discomfort, conjunctival and episcleral congestion and mydriasis in the acute phase to more severe structural alterations including optic nerve cupping, corneal Haabs striae and buphthalmia in the chronic phase (Figure 3), is critical for prompt management and preventing irreversible vision loss [16,30,31].
Human genetic testing in glaucoma has progressed substantially, shedding light on disease mechanisms, enhanced diagnose accuracy and patient management, and identification of potential therapeutic targets. Genes, such as myocilin (MYOC), optineurin (OPTN), and TANK-binding kinase 1 (TBK1), have been associated with early-onset glaucoma, while other genetic loci are associated with adult-onset types like POAG and PACG [32], although its use remains questionable [33]. The MYOC.mt1 variant’s role in POAG is still controversial, with mixed evidence on its impact [33]. Understanding the genetic keystones of glaucoma may facilitate the development of targeted therapies and improve the identification of individuals at higher risk [34].
1.5. Therapeutic Options (Medical and Surgical)
Current therapeutic interventions, including medical, physical, pharmacological, laser, and surgical procedures targeting IOP reduction, are limited and unsatisfactory. Despite their ability to delay the progression of the disease, none can effectively prevent vision loss and inevitable blindness, requiring the investigation of novel therapeutic possibilities, particularly those focusing on neuroprotection and neuroregeneration [35]. Emergency treatment used to start with the use of hyperosmotic agents like mannitol (1-2g/kg IV over 20 minutes) to rapidly lower IOP. Since this effect is only temporary and the drug has potential side effects, this approach has been abandoned. It is critical to initiate longer-acting medications, such as carbonic anhydrase inhibitors and prostaglandin analogues, to lower the IOP [36]. Both topical and systemic carbonic anhydrase inhibitors (e.g., dorzolamide, brinzolamide, and methazolamide) decrease aqueous humor production, but systemic options like methazolamide may cause adverse side effects, such as, metabolic acidosis and gastrointestinal issues [37]. Topical agents, such as dorzolamide and brinzolamide have fewer side effects.
Prostaglandin analogues are potent topical pharmaceuticals that should be used carefully in animals that have concomitant ocular disorders, such as severe uveitis or anterior lens luxation, since they induce miosis and exacerbate both conditions [38]. For long-term glaucoma management, maintaining low IOP is the crucial point to slower the progression of the disease. Prostaglandin analogues, such as latanoprost, aid to increase uveoscleral outflow by activating prostaglandin F receptors, inducing miosis, leading to the relaxation of the ciliary body muscle and enhancing fluid drainage [37].
In human medicine, beta-adrenergic antagonists like 0.5% timolol maleate are commonly used but are generally less effective in veterinary patients due to their mild impact on lowering IOP [37]. Considering this and the fact that medical management offers only temporary relieve, surgical intervention might be necessary, both in animals and in humans [37]. Among the last U.S. Food and Drug Administration (FDA)-approved medications for human glaucoma treatment (2017-2023) are Latanoprostene Bunod (Vyzulta™) and Netarsudil (Rhopressa™) [39] approved in November and December of 2017, respectively. Latanoprostene bunod, a nitric oxide-donating prostaglandin F2α agonist, has shown superior IOP-lowering effects compared to latanoprost, particularly in specific canine models of POAG [40,41,42,43]. This medication can improve uveoscleral and trabecular outflow pathways [40,41,42,43]. Netarsudil, a Rho kinase (ROCK) inhibitor, targets the trabecular meshwork cells, reducing cell stiffness and contractility, and lowering episcleral venous pressure, thereby increasing the outflow capacity and lowering IOP [44,45,46,47,48]. Although its effectiveness in dogs is still being studied, netarsudil appears promising when used in combination with latanoprost for improved control of IOP, as observed in human trials [44,45,46,47,48,49]. In March 2019, FDA approved Rocklatan™ [50], a fixed-dose combination of netarsudil and latanoprost that enhances IOP-lowering by combining both the ROCK inhibition pathway and the uveoscleral outflow pathway. One year later, Durysta™ [51] was approved, an implant containing bimatoprost that slowly releases the medication over time to lower IOP. This implant is designed for patients with POAG and provides an alternative to daily eye drops. Afterwards, approved in September 2022, Omlonti™ (Omidenepag Isopropyl) [52] works as a receptor agonist of prostaglandin EP2, increasing aqueous humor drainage. This drug was also designed for the treatment of POAG, specifically. Finally, FDA approved iDose® TR [53] in 2023, a travoprost intracameral implant delivering continuous medication directly into the eye for up to three years.
Researchers are developing innovative approaches such as preservative-free formulations, improved delivery methods, and new formulations to boost patient adherence and address common treatment barriers [54]. Erythropoietin (EPO), known for its anti-apoptotic, antioxidant, and anti-inflammatory effects, has shown promise for neuroprotection in glaucoma [55]. This hormone is also being tested, through different formulations, in animal pre-clinical trials to access its efficacy for the treatment of veterinary glaucomatous patients [56,57,58,59,60]. Additionally, bis(7)-tacrine, nimodipine, and mirtogenol are being considered as adjunct therapies to counteract oxidative stress, vascular dysfunction, and retinal cell apoptosis [61]. Memantine, an N-methyl-D-aspartate receptor blocker, also holds potential as a neuroprotectant for glaucoma, with studies noting a favorable safety profile [62]. Together, these emerging therapies may offer more effective glaucoma management and reduce the disease’s progression-related morbidity and economic impact [62].
Contrary to human medicine, medical treatment options in dogs are not very effective. Moreover, one of the main challenges of canine glaucoma treatment is ensuring that the prescribed treatment (usually, eye drops) regimen is followed consistently and correctly by the tutors. Non-compliance can greatly reduce the effectiveness of glaucoma management and its one of the reasons for treatment failure. To overcome this issue, sustained-release drug delivery systems, that offer the potential to provide more consistent therapeutic outcomes and reduce the frequency of eye drop administration, are being investigated [63,64,65,66,67,68,69,70,71,72]. Unfortunately, these procedures are not yet widely studied and adopted in veterinary medicine.
As previously mentioned, in human medicine, medical treatment is usually effective. On the contrary, in dogs, medical treatment alone is not sufficient and surgical options are necessary. These procedures aimed two targets: to enhance aqueous humor outflow [73], such as anterior chamber gonioimplants, and reduce its production through laser photocoagulation, endolaser or cyclocryotherapy [74]. In severe nonresponsive cases of glaucoma leading to blind painful eyes, the treatment involves evisceration and intrascleral prosthesis implantation or enucleation [75].
Secondary glaucoma is treated similarly, with the goal of restoring or preserving aqueous humor outflow, which might be blocked at the iridocorneal angle or at the pupil. The etiology may differ, making diagnosis and therapy more challenging [75]. In these cases, it is important to identify and address the cause of the glaucoma.
Recent medical treatments for glaucoma, designed primarily for the human eye, may prove ineffective when applied to dogs’ eyes. It underscores the significance of comprehending the anatomical and physiological characteristics of the aqueous humor outflow pathways in both species. Glaucoma in dogs is similar to humans in terms of RGC loss and optic nerve neuropathy, although the aqueous humor outflow pathways differ between these species. For instance, conditions like pectinate ligament dysplasia, which is recognized as a significant risk factor for the development of POAG in dogs, do not hold the same relevance in humans [76]. Another important distinction between the human and the dog eyes relies in the post-trabecular meshwork outflow pathways, specifically the human Schlemm’s canal compared to the canine angular aqueous plexus. While the human Schlemm’s canal has been extensively studied, there is still much to be discovered about the function of the canine angular aqueous plexus and its role in the development of glaucoma [76]. Moreover, there is a need to expand our understanding of the risk factors and mechanisms of canine glaucoma, including the differences between dogs and other species, and even between each dog breed. This highlights the species-specific factors in glaucoma pathogenesis, underscoring the importance of targeted research for better understanding and treating glaucoma in canine patients. In summary, stem cell-based therapies are still in their experimental stages for dogs, and there is an urgent need for more robust and diverse veterinary studies. The available treatments and clinical trials are designed for humans mainly, with limited or no adaptations for veterinary use, despite the similarities in the progression of the disease across species [12]. This inconsistency leaves a significant gap in understanding how stem cell therapies can be optimized for dogs, where glaucoma is equally painful and progressive leading to irreversible blindness.
Another critical factor influencing treatment effectiveness includes diagnostic tools, disease recognition and staging. Early detection and precise diagnosis are closely linked to heightened therapeutic efficacy in preventing visual loss [77].
Given the limitations of current treatment options for canine glaucoma, such as the temporary relief (IOP-lowering mechanisms) or the invasive procedures, there is a growing need for novel therapeutic strategies.
Regenerative Medicine and cell-based therapies are emerging as a promising solution, with the use of stem cells’ and their biofactors as a potential tool to regenerate damaged ocular tissues and address the root causes of glaucoma, ideally avoiding vision impairment. This approach not only offers hope for more effective long-term management but also represents a significant advancement in veterinary medicine ophthalmology.
2. Stem Cells Basics (Types, Sources, Advantages and Limitations)
Cell-based therapies have emerged as a prominent area of focus within regenerative medicine research. Stem cells can be classified according to their source as embryonic, adult [hematopoietic stem cells (HSCs) and non-hematopoietic/mesenchymal stem/stromal cells (MSCs)] or induced pluripotent Scs (iPSCs) [78,79], and considering their stage of development and differentiation as totipotent, pluripotent or multipotent cells [80].
MSCs can be defined as adult multipotent cells with mesodermal origin capable to replicate as undifferentiated cells, differentiate into various cell lineages (related to adipose, tendon, muscle, cartilage, bone, skin and connective tissues) and self-renew [81,82,83,84,85]. These characteristics, the ease and success of harvesting along with few ethical restraints and the potential therapeutic application of these stem cells, have given them wide popularity in many clinical and laboratory investigation areas.
The appeal of MSCs lies not only in their differentiation abilities but also in their interaction with the immune system. MSCs can modulate immune responses by secreting a range of bioactive molecules, collectively known as the secretome, which includes cytokines, growth factors, and chemokines. The secretome can prevent apoptosis [86] and reduce fibrosis [87], promote wound healing, support proliferation and angiogenesis and the differentiation of cells in situ [88]. It can also reduce the inflammatory response and, consequently, enhance MSCs’ maintenance and the regeneration environment [89], making these cells highly valuable in therapeutic applications.
As previously mentioned, stem cells’ therapeutic effect is, nowadays, essentially attributed to their secretome. Studies have been conducted to understand if it is crucial or not to apply stem cells in injured tissues, once their secretome can lead to similar regenerative outcomes [90,91]. MSCs’ culture supernatant, obtained after subjecting cells to specific culture conditions and rich in specific bioactive factors secreted to the extracellular space (cytokines and growth factors – secretome –), is known as Conditioned Media (CM). CM’s composition fluctuates according to cells’ stimulation, stem cells type and tissue [92]. Using CM, instead of stem cells in regenerative treatments, diminish the risk of applying cells with malignant characteristics, as well as the risk of rejection. Similarly, cell dosage and storage requirements may be reduced with an increased response capacity in emergency/acute situations – off-the-shelf secretome therapies – [93].
In veterinary medicine, MSCs have been sourced from various tissues in cats, dogs, and horses, such as the umbilical cord stroma and blood [94], dental pulp and periodontal ligament [95], bone marrow [96], adipose tissue [96], synovial membrane and fluid [97] and peripheral blood [98]. Remarkably, MSCs were isolated from mice bone-marrow [99] for the first time ever and their first application in veterinary medicine history was performed in a horse with suspensory ligament desmitis [100].
Bone marrow (BM-) and adipose tissue (AD-) are the most common sources of MSCs for therapeutic purposes, even though MSCs can be virtually isolated from any body tissue niches or organ [101]. This is primarily since these sources yield a higher number of cells for collection and isolation. However, harvesting, for example, bone marrow mesenchymal stem cells (BM-MSCs) is an invasive and painful process. Additionally, studies have shown that due to aging, there is a decline in the therapeutic potential of BM-MSCs and adipose-derived MSCs (AD-MSCs) [102]. Given these considerations, the umbilical cord (UC) is increasingly recognized as an outstanding alternative source of MSCs, gaining significant attraction in regenerative medicine. The collection of UC tissue immediately after a cesarean section is a straightforward, noninvasive procedure that circumvents the ethical issues associated with bone marrow extraction. Historically, the umbilical cord was discarded as medical waste, underscoring the fact that its use in stem cell therapies has no adverse effects on either the mother or the newborn. Moreover, the umbilical cord tissue is an excellent reservoir of young stem cells (less mature when compared to other MSCs’ sources), with high proliferative, growth and differentiation potential [103,104]. Umbilical cord mesenchymal stem cells (UC-MSCs) are also known for long-term viability at higher passages and for having low immunogenicity [104]. As a result, UC-MSCs are well tolerated in allogeneic cell-therapies (use of stem cells obtained from a donor who is different from the recipient, but from the same specie) [105]. Another great advantage of UC-MSCs is that they are non-tumorigenic [106].
Conversely, obtaining umbilical cord tissue or matrix in veterinary medicine can be challenging. Cesarean sections are infrequently performed, typically only when medically necessary, such as in cases of dystocia. Additionally, many pet owners today prioritize sterilizing their animals, further limiting opportunities to collect this material [107]. Moreover, during natural births, the mother’s maternal instinct often results in the ingestion of birth materials, including the umbilical cord. In other species, like horses, it is not practical to collect this tissue in a sterile manner because births occur in the field. Despite these challenges, the availability of stem cell banking options, both public and private, has increased globally over time [108], making it easier to get canine umbilical cord mesenchymal stem cells (cUC-MSCs) and enabling a quicker response to therapeutic needs.
So far, in veterinary medicine, MSCs have been principally studied and used in horses and dogs, for the treatment of orthopedic disorders [109]. Nevertheless, encouraging results prompted the pursuit of new studies about MSCs’ therapeutic potential application in other diseases (ocular, liver, renal, dermal, neuronal, olfactory, respiratory, reproductive, and digestive diseases) [110].
The Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy (ISCT) established three minimal criteria to standardize human MSCs characterization. Briefly, human MSCs can be defined by their capacity to adhere to plastic surfaces and their fibroblastic-like morphology when cultured in flasks (Figure 4); their ability to differentiate into at least three different cell lineages (chondrogenic, osteogenic and adipogenic) when cultured in appropriate differentiation culture conditions; and expression of clusters of differentiation (CD) like CD105, CD73, and CD90 and reduced/non-expression of hematopoietic markers [CD45, CD34, CD14 or CD11b, CD79ɑ or CD19, and major histocompatibility complex- (MHC-) II/human leukocyte antigen- (HLA-) DR] [83].
Unfortunately, to date, no standardized guidelines have been approved for characterizing veterinary MSCs and their bioproducts, as the antibodies commonly used are specific to human stem cells. As a result, human guidelines remain the only reference available. Even though, human MSCs-based therapies are deeply studied, and uniformed factors were established to consider them as effective and safe [111], the diversity of veterinary species, their biological differences and MSCs’ heterogeneous phenotypes and behavior in vitro, makes it difficult to describe specific patterns for MSCs therapeutic use and their safety in veterinary medicine. Currently, research focus on finding new critical surface markers, such as CD271 and STRO-1, with the aim of establishing standardized and reliable guidelines for veterinary medicine MSCs’ characterization [112,113].
MSCs found in fetal tissues, placenta, umbilical cord, and various adult tissues such as bone marrow and adipose tissue [114,115], offer additional advantages: they secrete specific bioactive molecules of interest, such as growth factors (EGF, VEGF-A, FGF), cytokines (TNF-α, IL-6, IL-8), and other survival-promoting agents like insulin growth factor (IGF-1) and transforming growth factor (TGF)-β1; they express homing receptors to migrate to damaged or inflamed areas [116,117]. A limitation of MSCs is their short lifespan post-transplantation, which may reduce their effectiveness, and once differentiated, they can increase immunogenicity by expressing MHC-I and MHC-II molecules. In systemic transplantation, many MSCs are also trapped in the lungs, increased risk of pulmonary thrombi which may further limit their therapeutic potential. It is also known that MSCs tend to be attracted to places where some level of inflammation is occurring, which can lead to non-specific systemic dispersion and reduce the load of cells that reach the place where the therapeutic action is expected. Compared to BM- and AD- stem cells, or even umbilical cord blood (UCB) stem cells, UC-MSCs represent a promising therapeutic option in veterinary regenerative medicine, though they have received relatively little research attention to date.
Considering glaucoma therapy, stem cells have numerous beneficial characteristics: 1. the capacity to differentiate into different cell types, allowing for selective replacement of RGCs; 2. the neuroprotective and immunomodulatory properties, particularly MSCs [118]; 3. the low immunogenicity, especially in pluripotent stem cells; 4. the secretome which aids in injury repair and immunomodulation, often achieving therapeutic benefits without the need for full integration into host tissue [119]; 5. the potential to serve as delivery systems for neurotrophic and growth factors, and anti-apoptotic factors [118].
Preclinical studies using pluripotent stem cells, such as embryonic stem cells (ESCs) and iPSCs, have paved the way for their consideration in clinical applications for glaucoma. Pluripotent stem cells are particularly advantageous since they remain undifferentiated for extended periods in culture and can differentiate into every somatic cell type. Takahashi et al. reported iPSCs in 2007 [120], which are generated from adult somatic tissues via genetic engineering, having the potential to prevent immune rejection and reduce the requirement for immunosuppressive drugs. Nevertheless, ESCs and iPSCs oppose obstacles such as genetic instability and the potential of developing teratomas [121], and iPSCs need more work to grow properly rather than adult stem cells.
3. Stem Cells in Glaucoma Treatment
The neuroprotective and differentiation skills of MSCs place them as a potential therapeutic strategy for glaucoma treatment. Research has shown that MSCs can support RGCs survival and resistance and may even differentiate into these cells, integrating the retina [122,123], by releasing growth factors, cytokines, and chemokines - collectively known as the secretome – (paracrine signaling), regulation of the cellular environment, and mitigating tissue damage caused by excessive immune responses [124,125]. Likewise, other studies have proven that BM-MSCs could integrate into retinal tissue after intravitreal injection and last for several weeks [126,127,128,129]. This provided significant IOP reduction and was related to neurotrophic factors secretion, as Brain-Derived Neurotrophic Factor (BDNF) and Ciliary Neurotrophic Factor (CNTF), which may inhibit RGCs and photoreceptors apoptosis, maintaining functional vision and avoiding progressive blindness [126,127,128,129].
Along with laser-induced regeneration, MSC therapies in glaucoma models also exhibit temporary increases in RGC numbers and axons, promoting functional recovery as demonstrated by enhanced performance on visual-guided tasks [130,131,132]. Moreover, a study conducted by Jiang et al., 2019, showed that iPSC-derived MSCs had the capacity to transfer their mitochondria to RGCs of mice, promoting cells’ survival and lowering in situ inflammation after injection.
In advanced stages of glaucoma, the only potential possibility to restore vision or at least impede the progression of the disease, lies in the regeneration of the optic nerve, making stem cell-based therapies a promising yet very challenging approach, with numerous related difficulties.
One of the first challenges is identifying a reliable source of stem cells capable of differentiating into RGCs. Once the appropriate stem cells are selected, these cells must be transplanted into the eye and integrated into the retina, and this process requires a permissive environment for axonal regrowth. Unfortunately, in the central nervous system (CNS), glial scarring - formed in response to injury - acts as a significant barrier to neural repair [133]. In glaucoma, this problem is exacerbated by the altered biochemical microenvironment, where activated astrocytes in the lamina cribrosa and Müller cells in the retina hinder axon regeneration [133].
Addressing these environmental and cellular changes is critical to promoting successful axon growth through the ONH. Beyond the mechanical challenges, the transplanted cells must also establish functional synaptic connections with retinal interneurons and corresponding neurons in the brain. Only through this precise integration can the visual function be preserved or restored.
Despite the theoretical potential of stem cell-based therapies, translating success from preclinical studies in animal models to human clinical applications has proven difficult. Most animal studies are conducted using induced models of glaucoma, where the damage is acute and less extensive compared to the chronic, progressive nature of glaucoma [134]. In these models, the therapeutic environment may be more favorable, allowing for better outcomes than what can be realistically achieved in humans, where optic nerve degeneration often takes years to develop [134]. Moreover, as previously mentioned, biological differences between animal models and humans, such as glial scarring and the cellular microenvironment, further complicate this translation [135].
One of the significant challenges in addressing veterinary patients’ glaucoma, especially dogs, is the lack of preclinical studies focused on animals. While there has been distinguished progress in the application of stem cell-based therapies for treating human ocular conditions, the application of these therapies for glaucoma remains underexplored in animal models, particularly in canine patients.
As mentioned above, human clinical trials for glaucoma, although limited, are more prevalent. These trials often involve small participant groups and have not yet demonstrated long-term efficacy or significant benefits [136,137]. Severe complications, including retinal detachment and proliferative vitreoretinopathy, have also been reported in human trials [138], which further highlights the limitations and risks associated with these emerging treatments.
The following table (Table 1) summarizes clinical studies registered on various platforms, including the WHO International Clinical studies Registry Platform (ICTRP), ClinicalTrials.gov, and the European Clinical Trials Register, with an emphasis on the use of stem cells for glaucoma treatment. These studies investigate the ability of stem cell therapies to regenerate ocular tissues, preserve the optic nerve, and restore vision due to glaucoma. Studies are in diverse phases, ranging from early preclinical trials evaluating safety and efficacy in animal models to human clinical trials looking into therapeutic results. This table summarizes the current global research activities in this novel field of glaucoma therapy.
Regrettably, there are only a few registered clinical trials, and many have not yet reported results. Most trials involve small patient samples, with the exception of SCOT1 and SCOT2, which focused on using autologous BM-MSCs for different retinal and optic nerve diseases where the inclusion of glaucoma patients in these studies has been relatively limited. NCT06200727 also includes a significant patient population; however, the number of glaucoma patients enrolled in this trial remains relatively low.
The clinical trial NCT06498440 provides the most extensive results concerning specifically glaucoma, though its’s focused on the effectiveness of steroid and non-steroid anti-inflammatory drugs, highlighting the need for more research and investigation of the potential of cell-based therapies. Among the other trials, NCT02330978 is the only one that has produced outcomes on the use of MSCs for glaucoma treatment. Results showed no improvement in visual acuity or field [153]. One patient developed retinal detachment and was removed, while the other maintained stable retinal function without significant changes during the study [153].
Despite the limited number of animal studies using stem cell-based therapies for glaucoma treatment, Roubeix et al. (2015) conducted a study to assess the potential of BM-MSCs in a rat model of ocular hypertension. In this study, cells were administered into the anterior chamber of 20 hypertensive Long-Evans rats [161]. The results revealed a significant and long-lasting reduction of the IOP and meaningful neuroprotective effects on RGCs [161]. These findings highlight the potential of MSCs for the treatment of glaucoma in veterinary patients and the need for further studies on this matter.
4. Conclusions
Glaucoma has a substantial influence on dogs’ quality of life, being an extremely painful condition and causing gradual visual loss with inevitably general deterioration in well-being. Despite its ubiquity, long-term therapeutic options are limited, especially due to tutors’ compliance, highlighting the need for novel treatments. Stem cell-based therapies demonstrate potential in the management of this condition. Current research into the use of stem cells for the treatment of glaucoma, particularly umbilical cord mesenchymal stem cells and their secretome, is limited. The bulk of research have been undertaken on humans or animal models to evaluate potential human therapy, with relatively few conducted on veterinary patients such as dogs. Given the intriguing potential of these medicines, more extensive studies should be conducted in the future, particularly to investigate their use in veterinary medicine, where glaucoma treatment options remain scarce.
Author Contributions
All authors (A.D.S.M., B.L., A.C.S., A.C., P.S., A.A., E.D., R.A. and A.C.M.) made significant contributions to this work, with a clearly defined division of responsibilities. They all reviewed and approved the final version of the manuscript for submission. Each author accepts personal responsibility for their own contributions and for ensuring that any issues related to the accuracy or integrity of the work, even in parts they were not directly involved in, are properly investigated, addressed, and documented in the literature. All authors have read and approved the final published version of the manuscript.
Funding
The work was supported through the PhD Scholarships: Alícia Moreira (2023.00544.BD), Bruna Lopes (2021.05265.BD), Ana Catarina Sousa (SFRH/BD/146689/2019), André Coelho (2023.00428.BD), Patrícia Sousa (2023.00246.BD),and through the project UIDB/00211/2020 funded by FCT/MCTES through national funds and through the project 2022.04501.PTDC (Olfabionerve—Olfactory Mucosa Mesenchymal StemCells and Biomaterials Promoting Peripheral Nerve Regeneration).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Not applicable.
Acknowledgments
The author, Rui D. Alvites, acknowledges the Centro de Estudos de Ciência Animal (CECA), Instituto de Ciências, Tecnologias e Agroambiente (ICETA), Porto University (UP) and Fundação para a Ciência e Tecnologia (FCT) for the funding and availability of all technical, structural, and human resources necessary for the development of this work
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AD- | Adipose Tissue |
| AD-MSCs | Adipose Tissue Mesenchymal Stem Cells |
| ADRC | Adipose-Derived Regenerative Cells |
| BDNF | Brain-Derived Neurotrophic Factor |
| BM- | Bone Marrow |
| BM-MSCs | Bone Marrow Mesenchymal Stem Cells |
| CD | Clusters of Differentiation |
| CM | Conditioned Media |
| CNS | Central Nervous System |
| CNTF | Ciliary Neurotrophic Factor |
| cUC-MSCs | Canine Umbilical Cord Mesenchymal Stem Cells |
| EGF | Epidermal Growth Factor |
| ESCs | Embryonic Stem Cells |
| FDA | Food and Drug Administration |
| FGF | Fibroblast Growth Factor |
| HLA | Human Leukocyte Antigen |
| HSCs | Hematopoietic Stem Cells |
| ICTRP | International Clinical studies Registry Platform |
| IGF-1 | Insulin-like Growth Factor 1 |
| IL-6/-8 | Interleukin-6/8 |
| IOP | Intraocular Pressure |
| iPSCs | Induced Pluripotent Stem Cells |
| ISCT | International Society for Cellular Therapy |
| MHC-I/-II | Major histocompatibility complex I/II |
| MSCs | Mesenchymal Stem Cells |
| MYOC | Myocilin |
| ONH | Optic Nerve Head |
| OPTN | Optineurin |
| PACG | Primary Angle-Closure Glaucoma |
| POAG | Primary Open-Angled Glaucoma |
| PRF | Platelet-rich Fibrin |
| RGCs | Retinal Ganglion CellsTBK1 |
| TANK-binding kinase 1 | |
| TGF-β1 | Transforming Growth Factor-beta 1 |
| TNF-α | Tumor Necrosis Factor Alpha |
| UC | Umbilical Cord |
| UC-MSCs | Umbilical Cord Mesenchymal Stem Cells |
| UCB | Umbilical cord blood |
| VEGF-A | Vascular Endothelial Growth Factor A |
| VMDB | Veterinary Medical Data Base |
References
- Quigley, H. A. Glaucoma: Macrocosm to Microcosm. The Friedenwald Lecture. Invest Ophthalmol Vis Sci 2005, 46 (8), 2663–2670. [CrossRef]
- Tham, Y. C.; Li, X.; Wong, T. Y.; Quigley, H. A.; Aung, T.; Cheng, C. Y. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040: A Systematic Review and Meta-Analysis. Ophthalmology 2014, 121 (11), 2081–2090. [CrossRef]
- Quigley, H.; Broman, A. T. The Number of People with Glaucoma Worldwide in 2010 and 2020. British Journal of Ophthalmology 2006, 90 (3), 262–267. [CrossRef]
- Gelatt, K. N.; MacKay, E. O. Secondary Glaucomas in the Dog in North America. Vet Ophthalmol 2004, 7 (4), 245–259. [CrossRef]
- Gelatt, K. N.; MacKay, E. O. Prevalence of the Breed-Related Glaucomas in Pure-Bred Dogs in North America. Vet Ophthalmol 2004, 7 (2), 97–111. [CrossRef]
- Gelatt, K. N.; Whitley, R. D. Surgery of the Orbit. Veterinary Ophthalmic Surgery 2011, 51–88. [CrossRef]
- Frezzotti, R. The Glaucoma Mystery from Ancient Times to the 21st Century. The Glaucoma Mystery: Ancient Concepts. Acta Ophthalmol Scand Suppl 2000, 78 (232), 14–18. [CrossRef]
- Reinstein, S. L.; Rankin, A. J.; Allbaugh, R. Canine Glaucoma: Pathophysiology and Diagnosis. Compend Contin Educ Vet 2009, 31 (10).
- Wrześniewska, K.; Madany, J.; Winiarczyk, D. Comparison of Intraocular Pressure Measurement with Schiotz Tonometer and Tono-Pen Vet Tonometer in Healthy Dogs. J Vet Res 2018, 62 (2), 243–247. [CrossRef]
- Pizzirani, S. Definition, Classification, and Pathophysiology of Canine Glaucoma. Vet Clin North Am Small Anim Pract 2015, 45 (6), 1127–1157. [CrossRef]
- Dielemans, I.; Vingerling, J. R.; Wolfs, R. C. W.; Hofman, A.; Grobbee, D. E.; de Jong, P. T. V. M. The Prevalence of Primary Open-Angle Glaucoma in a Population-Based Study in The Netherlands. The Rotterdam Study. Ophthalmology 1994, 101 (11), 1851–1855. [CrossRef]
- Trick, G. L. Visual Dysfunction in Normotensive Glaucoma. Doc Ophthalmol 1993, 85 (2), 125–133. [CrossRef]
- Komaromy, A. M.; Sherwood, M. B.; Dawson, W. W.; Sapp, H. L.; Nelson, G.; Kubilis, P. S.; Brooks, D. E. Diurnal Intraocular Pressure Curves in Healthy Rhesus Macaques (Macaca Mulatta) and Rhesus Macaques With Normotensive and Hypertensive Primary Open-Angle Glaucoma. J Glaucoma 1998, 2 (7), 131.
- Johnson, M.; McLaren, J. W.; Overby, D. R. Unconventional Aqueous Humor Outflow: A Review. Experimental Eye Research. Academic Press May 1, 2017, pp 94–111. [CrossRef]
- Chang, E. E.; Goldberg, J. L. Glaucoma 2.0: Neuroprotection, Neuroregeneration, Neuroenhancement. Ophthalmology 2012, 119 (5), 979. [CrossRef]
- Maggio, F. Glaucomas. Top Companion Anim Med 2015, 30 (3), 86–96. [CrossRef]
- Morgan, R. Glaucoma in Dogs and Cats. https://veterinarypartner.vin.com/doc/?id=6097123&pid=19239.
- Slater, M. R.; Erb, H. N. Effects of Risk Factors and Prophylactic Treatment on Primary Glaucoma in the Dog. J Am Vet Med Assoc 1986, 188 (9), 1028–1030.
- Mendicino, M.; Bailey, A. M.; Wonnacott, K.; Puri, R. K.; Bauer, S. R. Cell Stem Cell Forum MSC-Based Product Characterization for Clinical Trials: An FDA Perspective. 2014. [CrossRef]
- Gelatt, K. N.; MacKay, E. O. Prevalence of the Breed-Related Glaucomas in Pure-Bred Dogs in North America. Vet Ophthalmol 2004, 7 (2), 97–111. [CrossRef]
- Gelatt, K. N.; Mackay, E. O. Prevalence of the Breed-Related Glaucomas in Pure-Bred Dogs in North America; 2004; Vol. 7.
- Soundarya, T. C.; Kshama, M. A.; Aishwarya, N. Studies on Occurrence of Ocular Diseases in Dogs with Emphasis on Occurrence of Glaucoma. Int J Curr Microbiol Appl Sci 2020, 9 (2), 2787–2795. [CrossRef]
- Sigle, K.; Nasisse, M. Long-Term Complications after Phacoemulsification for Cataract Removal in Dogs: 172 Cases (1995–2002); 2006.
- Biros, D.; Gelatt, K.; Brooks, D.; Kubilis, P.; Andrew, S.; Strubbe, D.; Whigham, H. Development of Glaucoma after Cataract Surgery in Dogs: 220 Cases (1987–1998); 2000.
- Lannek, EB.; Miller, P. Development of Glaucoma after Phacoemulsification for Removal of Cataracts in Dogs: 22 Cases (1987–1997); 2001.
- Scott, E. M.; Esson, D. W.; Fritz, K. J.; Dubielzig, R. R. Major Breed Distribution of Canine Patients Enucleated or Eviscerated Due to Glaucoma Following Routine Cataract Surgery as Well as Common Histopathologic Findings within Enucleated Globes. Vet Ophthalmol 2013, 16 (SUPPL.1), 64–72. [CrossRef]
- Foote, B. C.; Pederson, S. L.; Welihozkiy, A.; Stine, J. M.; Carastro, S. M.; Andrew, S. E.; Michau, T. M. Retinal Detachment and Glaucoma in the Boston Terrier and Shih Tzu Following Phacoemulsification (135 Patients): 2000–2014. Vet Ophthalmol 2018, 21 (3), 240–248. [CrossRef]
- Newbold, G. M.; Kelch, W. J.; Chen, T.; Ward, D. A.; Hendrix, D. V. H. Phacoemulsification Outcomes in Boston Terriers as Compared to Non-Boston Terriers: A Retrospective Study (2002–2015). Vet Ophthalmol 2018, 21 (4), 353–361. [CrossRef]
- Moeller, E.; Blocker, T.; Esson, D.; Madsen, R. Postoperative Glaucoma in the Labrador Retriever: Incidence, Risk Factors, and Visual Outcome Following Routine Phacoemulsification. Vet Ophthalmol 2011, 14 (6), 385–394. [CrossRef]
- Beamer, G.; Reilly, C. M.; Pizzirani, S. Microscopic Lesions in Canine Eyes with Primary Glaucoma. Vet Clin North Am Small Anim Pract 2015, 45 (6), 1213–1233. [CrossRef]
- Miller, P. E.; Bentley, E. Clinical Signs and Diagnosis of the Canine Primary Glaucomas. Vet Clin North Am Small Anim Pract 2015, 45 (6), 1183–1212. [CrossRef]
- Wiggs, J. L.; Pasquale, L. R. Genetics of Glaucoma. Human Molecular Genetics. Oxford University Press August 1, 2017, pp R21–R27. [CrossRef]
- Cohen, C. S.; Allingham, R. R. The Dawn of Genetic Testing for Glaucoma; 2004. www.theorator.
- Challa, P. Glaucoma Genetics: Advancing New Understandings of Glaucoma Pathogenesis.
- Almasieh, M.; Zhou, Y.; Casanova, C.; Polo, A. Di. Structural and Functional Neuroprotection in Glaucoma: Role of Galantamine-Mediated Activation of Muscarinic Acetylcholine Receptors. Cell Death Dis 2010, 27. [CrossRef]
- Mandell, D. C. Ophthalmic Emergencies. Clin Tech Small Anim Pract 2000, 15 (2), 94–100. [CrossRef]
- Alario, A. F.; Strong, T. D.; Pizzirani, S. Medical Treatment of Primary Canine Glaucoma. Vet Clin North Am Small Anim Pract 2015, 45 (6), 1235–1259. [CrossRef]
- Willis, A. M.; Diehl, K. A.; Robbin, T. E. Advances in Topical Glaucoma Therapy. Vet Ophthalmol 2002, 5 (1), 9–17. [CrossRef]
- U.S. Food and Drug Administration. Latanoprostene Bunod (VyzultaTM) and Netarsudil (RhopressaTM): Drug Approval Package. https://www.fda.gov/drugs/development-approval-process-drugs/drug-approvals-and-databases (accessed 2024-09-25).
- Krauss, A. H. P.; Impagnatiello, F.; Toris, C. B.; Gale, D. C.; Prasanna, G.; Borghi, V.; Chiroli, V.; Chong, W. K. M.; Carreiro, S. T.; Ongini, E. Ocular Hypotensive Activity of BOL-303259-X, a Nitric Oxide Donating Prostaglandin F2α Agonist, in Preclinical Models. Exp Eye Res 2011, 93 (3), 250–255. [CrossRef]
- Borghi, V.; Bastia, E.; Guzzetta, M.; Chiroli, V.; Toris, C. B.; Batugo, M. R.; Carreiro, S. T.; Chong, W. K. M.; Gale, D. C.; Kucera, D. J.; Jia, L.; Prasanna, G.; Ongini, E.; Krauss, A. H. P.; Impagnatiello, F. A Novel Nitric Oxide Releasing Prostaglandin Analog, NCX 125, Reduces Intraocular Pressure in Rabbit, Dog, and Primate Models of Glaucoma. J Ocul Pharmacol Ther 2010, 26 (2), 125–131. [CrossRef]
- Impagnatiello, F.; Borghi, V.; Gale, D. C.; Batugo, M.; Guzzetta, M.; Brambilla, S.; Carreiro, S. T.; Chong, W. K. M.; Prasanna, G.; Chiroli, V.; Ongini, E.; Krauss, A. H. P. A Dual Acting Compound with Latanoprost Amide and Nitric Oxide Releasing Properties, Shows Ocular Hypotensive Effects in Rabbits and Dogs. Exp Eye Res 2011, 93 (3), 243–249. [CrossRef]
- Cavet, M. E.; Decory, H. H. The Role of Nitric Oxide in the Intraocular Pressure Lowering Efficacy of Latanoprostene Bunod: Review of Nonclinical Studies. J Ocul Pharmacol Ther 2018, 34 (1–2), 52–60. [CrossRef]
- Lin, C. W.; Sherman, B.; Moore, L. A.; Laethem, C. L.; Lu, D. W.; Pattabiraman, P. P.; Rao, P. V.; Delong, M. A.; Kopczynski, C. C. Discovery and Preclinical Development of Netarsudil, a Novel Ocular Hypotensive Agent for the Treatment of Glaucoma. J Ocul Pharmacol Ther 2018, 34 (1–2), 40–51. [CrossRef]
- Rao, P. V.; Pattabiraman, P. P.; Kopczynski, C. Role of the Rho GTPase/Rho Kinase Signaling Pathway in Pathogenesis and Treatment of Glaucoma: Bench to Bedside Research. Exp Eye Res 2017, 158, 23–32. [CrossRef]
- Wang, S. K.; Chang, R. T. An Emerging Treatment Option for Glaucoma: Rho Kinase Inhibitors. Clin Ophthalmol 2014, 8, 883–890. [CrossRef]
- Rao, P. V.; Deng, P.-F.; Kumar, J.; Epstein, D. L. Modulation of Aqueous Humor Outflow Facility by the Rho Kinase-Specific Inhibitor Y-27632.
- Kiel, J. W.; Kopczynski, C. C. Effect of AR-13324 on Episcleral Venous Pressure in Dutch Belted Rabbits. J Ocul Pharmacol Ther 2015, 31 (3), 146–151. [CrossRef]
- Miyagi, H.; Kim, S.; Li, J.; Murphy, C. J.; Thomasy, S. M. Topical Rho-Associated Kinase Inhibitor, Y27632, Accelerates Corneal Endothelial Regeneration in a Canine Cryoinjury Model. Cornea 2019, 38 (3), 352–359. [CrossRef]
- U.S. Food and Drug Administration. RocklatanTM: Drug Approval Package. https://www.fda.gov/drugs/development-approval-process-drugs/drug-approvals-and-databases (accessed 2024-09-25).
- U.S. Food and Drug Administration. DurystaTM: Drug Approval Package. https://www.fda.gov/drugs/development-approval-process-drugs/drug-approvals-and-databases (accessed 2024-10-01).
- U.S. Food and Drug Administration. OmlontiTM (Omidenepag Isopropyl): Drug Approval Package. https://www.fda.gov/drugs/development-approval-process-drugs/drug-approvals-and-databases (accessed 2024-10-01).
- U.S. Food and Drug Administration. iDose® TR: Drug Approval Package. https://www.fda.gov/drugs/development-approval-process-drugs/drug-approvals-and-databases (accessed 2024-10-03).
- Schehlein, E. M.; Novack, G.; Robin, A. L. New Pharmacotherapy for the Treatment of Glaucoma. Expert Opinion on Pharmacotherapy. Taylor and Francis Ltd. December 12, 2017, pp 1939–1946. [CrossRef]
- Lin, T. Y.; Lai, Y. F.; Chen, Y. H.; Lu, D. W. The Latest Evidence of Erythropoietin in the Treatment of Glaucoma. International Journal of Molecular Sciences. MDPI December 1, 2022. [CrossRef]
- Silva, B.; Gonçalves, L. M.; Braz, B. S.; Delgado, E. Chitosan and Hyaluronic Acid Nanoparticles as Vehicles of Epoetin Beta for Subconjunctival Ocular Delivery. Mar Drugs 2022, 20 (2). [CrossRef]
- Silva, B.; Gonçalves, L. M.; Braz, B. S.; Delgado, E. Topical Administration of a Nanoformulation of Chitosan-Hyaluronic Acid-Epoetin Beta in a Rat Model of Glaucoma. Pharmaceuticals (Basel) 2023, 16 (2). [CrossRef]
- Silva, B.; Marto, J.; Braz, B. S.; Delgado, E.; Almeida, A. J.; Gonçalves, L. New Nanoparticles for Topical Ocular Delivery of Erythropoietin. Int J Pharm 2020, 576. [CrossRef]
- Silva, B.; Gonçalves, L. M.; São Braz, B.; Delgado, E. Topical Ocular Delivery of Nanoparticles with Epoetin Beta in Wistar Hannover Rats. Sci Rep 2023, 13 (1). [CrossRef]
- Resende, A. P.; Rosolen, S. G.; Nunes, T.; São Braz, B.; Delgado, E. Functional and Structural Effects of Erythropoietin Subconjunctival Administration in Glaucomatous Animals. Biomed Hub 2018, 3 (2), 1–11. [CrossRef]
- Beidoe, G.; Mousa, S. A. Current Primary Open-Angle Glaucoma Treatments and Future Directions. Clinical Ophthalmology. October 19, 2012, pp 1699–1707. [CrossRef]
- Mckinnon, S.; Goldberg, L. D.; Peeples, P.; Walt, J.; Bramley, T. Current Management of Glaucoma and the Need for Complete Therapy. American Journal of Managed Care 2008.
- Okeke, C. O.; Quigley, H. A.; Jampel, H. D.; Ying, G. shuang; Plyler, R. J.; Jiang, Y.; Friedman, D. S. Adherence with Topical Glaucoma Medication Monitored Electronically the Travatan Dosing Aid Study. Ophthalmology 2009, 116 (2), 191–199. [CrossRef]
- Friedman, D. S.; Quigley, H. A.; Gelb, L.; Tan, J.; Margolis, J.; Shah, S. N.; Kim, E. E.; Zimmerman, T.; Hahn, S. R. Using Pharmacy Claims Data to Study Adherence to Glaucoma Medications: Methodology and Findings of the Glaucoma Adherence and Persistency Study (GAPS). Invest Ophthalmol Vis Sci 2007, 48 (11), 5052–5057. [CrossRef]
- Miller, P. E.; Schmidt, G. M.; Vainisi, S. J.; Swanson, J. F.; Herrmann, M. K. The Efficacy of Topical Prophylactic Antiglaucoma Therapy in Primary Closed Angle Glaucoma in Dogs: A Multicenter Clinical Trial. J Am Anim Hosp Assoc 2000, 36 (5), 431–438. [CrossRef]
- Aref, A. A. Sustained Drug Delivery for Glaucoma: Current Data and Future Trends. Curr Opin Ophthalmol 2017, 28 (2), 169–174. [CrossRef]
- Brandt, J. D.; DuBiner, H. B.; Benza, R.; Sall, K. N.; Walker, G. A.; Semba, C. P. Long-Term Safety and Efficacy of a Sustained-Release Bimatoprost Ocular Ring. Ophthalmology 2017, 124 (10), 1565–1566. [CrossRef]
- Lee, S. S.; Burke, J.; Shen, J.; Almazan, A.; Orilla, W.; Hughes, P.; Zhang, J.; Li, H.; Struble, C.; Miller, P. E.; Robinson, M. R. Bimatoprost Sustained-Release Intracameral Implant Reduces Episcleral Venous Pressure in Dogs. Vet Ophthalmol 2018, 21 (4), 376–381. [CrossRef]
- Komaromy, A. M.; Koehl, K.; Harman, C. D.; Stewart, G.; Wolinski, N.; Norris, T. N.; Valade, D.; Chekhtman, I.; Lambert, J. N.; Donohue, A. C.; Tait, R. Long-Term Intraocular Pressure (IOP) Control by Means of a Novel Biodegradable Intracameral (IC) Latanoprost Free Acid (LFA) Implant. Invest Ophthalmol Vis Sci 2017, 58 (8), 4591–4591.
- Robeson, R.; Verhoeven, R. S.; Garcia, A.; Das, S.; Hamby, K.; Hernandez, M.; Gum, G. G.; Yerxa, B. R.; Navratil, T. A 12-Month Study of the ENV515 (Travoprost) Intracameral Implant on Intraocular Pressure in Beagle Dogs. Invest Ophthalmol Vis Sci 2017, 58 (8), 1072–1072.
- Seal, J. R.; Robinson, M. R.; Burke, J.; Bejanian, M.; Coote, M.; Attar, M. Intracameral Sustained-Release Bimatoprost Implant Delivers Bimatoprost to Target Tissues with Reduced Drug Exposure to Off-Target Tissues. J Ocul Pharmacol Ther 2019, 35 (1), 50–57. [CrossRef]
- Barachetti, L.; Rampazzo, A.; Mortellaro, C. M.; Scevola, S.; Gilger, B. C. Use of Episcleral Cyclosporine Implants in Dogs with Keratoconjunctivitis Sicca: Pilot Study. Vet Ophthalmol 2015, 18 (3), 234–241. [CrossRef]
- Graham, K. L.; Hall, E. J. S.; Caraguel, C.; White, A.; Billson, F. A.; Billson, F. M. Comparison of Diode Laser Trans-Scleral Cyclophotocoagulation versus Implantation of a 350-Mm2 Baerveldt Glaucoma Drainage Device for the Treatment of Glaucoma in Dogs (a Retrospective Study: 2010-2016). Vet Ophthalmol 2018, 21 (5), 487–497. [CrossRef]
- Bras, D.; Maggio, F. Surgical Treatment of Canine Glaucoma: Cyclodestructive Techniques. Vet Clin North Am Small Anim Pract 2015, 45 (6), 1283–1305. [CrossRef]
- Pumphrey, S. Canine Secondary Glaucomas. Vet Clin North Am Small Anim Pract 2015, 45 (6), 1335–1364. [CrossRef]
- Komáromy, A. M.; Bras, D.; Esson, D. W.; Fellman, R. L.; Plummer, C. E.; Sapienza, J. S.; Storey, E. S.; Teixeira, L. B.; Toris, C. B.; Webb, T. R.; András Komáromy, C. M. The Future of Canine Glaucoma Therapy. 2019. [CrossRef]
- Komáromy, A. M.; Bras, D.; Esson, D. W.; Fellman, R. L.; Grozdanic, S. D.; Kagemann, L.; Miller, P. E.; Moroi, S. E.; Plummer, C. E.; Sapienza, J. S.; Storey, E. S.; Teixeira, L. B.; Toris, C. B.; Webb, T. R. The Future of Canine Glaucoma Therapy. Vet Ophthalmol 2019, 22 (5), 726–740. [CrossRef]
- Evans, M. J.; Kaufman, M. H. Establishment in Culture of Pluripotential Cells from Mouse Embryos. Nature 1981 292:5819 1981, 292 (5819), 154–156. [CrossRef]
- Takahashi, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Mouse Embryonic and Adult Fibroblast Cultures by Defined Factors. Cell 2006, 126 (4), 663–676. [CrossRef]
- Wagers, A. J.; Weissman, I. L. Plasticity of Adult Stem Cells. Cell 2004, 116 (5), 639–648. [CrossRef]
- Barry, F. P.; Murphy, J. M. Mesenchymal Stem Cells: Clinical Applications and Biological Characterization. Int J Biochem Cell Biol 2004, 36 (4), 568–584. [CrossRef]
- Bianco, P.; Robey, P. G.; Simmons, P. J. Cell Stem Cell Commentary Mesenchymal Stem Cells: Revisiting History, Concepts, and Assays. Cell Stem Cell 2008, 2 (4), 313–319. [CrossRef]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F. C.; Krause, D. S.; Deans, R. J.; Keating, A.; Prockop, D. J.; Horwitz, E. M. Minimal Criteria for Defining Multipotent Mesenchymal Stromal Cells. The International Society for Cellular Therapy Position Statement. Cytotherapy 2006, 8 (4), 315–317. [CrossRef]
- Mendicino, M.; Bailey, A. M.; Wonnacott, K.; Puri, R. K.; Bauer, S. R. Cell Stem Cell Forum MSC-Based Product Characterization for Clinical Trials: An FDA Perspective. 2014. [CrossRef]
- Pittenger, M. F.; Mackay, A. M.; Beck, S. C.; Jaiswal, R. K.; Douglas, R.; Mosca, J. D.; Moorman, M. A.; Simonetti, D. W.; Craig, S.; Marshak, D. R. Multilineage Potential of Adult Human Mesenchymal Stem Cells. Science (1979) 1999, 284 (5411), 143–147. [CrossRef]
- Tögel, F.; Weiss, K.; Yang, Y.; Hu, Z.; Zhang, P.; Westenfelder, C. Vasculotropic, Paracrine Actions of Infused Mesenchymal Stem Cells Are Important to the Recovery from Acute Kidney Injury. Am J Physiol Renal Physiol 2007, 292, 1626–1635. [CrossRef]
- Suga, H.; Eto, H.; Shigeura, T.; Inoue, K.; Aoi, N.; Kato, H.; …; Yoshimura, K. IFATS Collection: Fibroblast Growth Factor-2-Induced Hepatocyte Growth Factor Secretion by Adipose-Derived Stromal Cells Inhibits Postinjury Fibrogenesis Through a c-Jun N-Terminal Kinase-Dependent Mechanism. Stem Cells 2009, 27 (1), 238–249. [CrossRef]
- Blobe, G. C.; Schiemann, W. P.; Lodish, H. F. Role of Transforming Growth Factor β in Human Disease. N Engl J Med 2009, 342 (18), 1350–1358. [CrossRef]
- Kalinski, P. Regulation of Immune Responses by Prostaglandin E2. Journal of Immunology 2012, 188 (1), 21–28. [CrossRef]
- Pereira, T.; Armada-Da Silva, P. A. S.; Amorim, I.; Rêma, A.; Caseiro, A. R.; Gärtner, A.; Rodrigues, M.; Lopes, M. A.; Bártolo, P. J.; Santos, J. D.; Luís, A. L.; Maurício, A. C.; Frias, R. Effects of Human Mesenchymal Stem Cells Isolated from Wharton’s Jelly of the Umbilical Cord and Conditioned Media on Skeletal Muscle Regeneration Using a Myectomy Model. Stem Cells Int 2014, 2014, 16. [CrossRef]
- Carvalho, M. M.; Teixeira, F. G.; Reis, R. L.; Sousa, N.; Salgado, A. J. Mesenchymal Stem Cells in the Umbilical Cord: Phenotypic Characterization, Secretome and Applications in Central Nervous System Regenerative Medicine. Curr Stem Cell Res Ther 2011, 6 (3), 221–228. [CrossRef]
- Vizoso, F. J.; Eiro, N.; Cid, S.; Schneider, J.; Perez-Fernandez, R. Molecular Sciences Mesenchymal Stem Cell Secretome: Toward Cell-Free Therapeutic Strategies in Regenerative Medicine. J. Mol. Sci 2017, 18 (8), 1852. [CrossRef]
- Volarevic, V.; Simovic Markovic, B.; Gazdic, M.; Volarevic, A.; Jovicic, N.; Arsenijevic, N.; Armstrong, L.; Djonov, V.; Lako, M.; Stojkovic, M. Ethical and Safety Issues of Stem Cell-Based Therapy. Int. J. Med. Sci 2018, 15 (1), 36–45. [CrossRef]
- Carrade, D. D.; Owens, S. D.; Galuppo, L. D.; Vidal, M. A.; Ferraro, G. L.; Librach, F.; Buerchler, S.; Friedman, M. S.; Walker, N. J.; Borjesson, D. L. Clinicopathologic Findings Following Intra-Articular Injection of Autologous and Allogeneic Placentally Derived Equine Mesenchymal Stem Cells in Horses. Cytotherapy 2011, 13 (4), 419–430. [CrossRef]
- Mensing, N.; Gasse, H.; Hambruch, N.; Haeger, J. D.; Pfarrer, C.; Staszyk, C. Isolation and Characterization of Multipotent Mesenchymal Stromal Cells from the Gingiva and the Periodontal Ligament of the Horse. BMC Vet Res 2011, 7, 1–13. [CrossRef]
- Webb, T. L.; Quimby, J. m.; Dow, S. W. In Vitro Comparison of Feline Bone Marrow-Derived and Adipose Tissue-Derived Mesenchymal Stem Cells. J Feline Med Surg 2012, 14 (2), 165–168. [CrossRef]
- Prado, A. A. F.; Favaron, P. O.; da Silva, L. C. L. C.; Baccarin, R. Y. A.; Miglino, M. A.; Maria, D. A. Characterization of Mesenchymal Stem Cells Derived from the Equine Synovial Fluid and Membrane. BMC Vet Res 2015, 11 (1), 1–13. [CrossRef]
- Sato, K.; Yamawaki-Ogata, A.; Kanemoto, I.; Usui, A.; Narita, Y. Isolation and Characterisation of Peripheral Blood-Derived Feline Mesenchymal Stem Cells. The Veterinary Journal 2016, 216, 183–188. [CrossRef]
- Friedenstein, A. J.; Piatetzky-Shapiro, I. I.; Petrakova, K. V. Osteogenesis in Transplants of Bone Marrow Cells. J Embryol Exp Morphol 1966, 16 (3), 381–390.
- Herthel DJ. Suspensory Desmitis Therapies. Proc 12th ACVS Vet Sympo 2002, 165–167.
- da Silva Meirelles, L.; Chagastelles, P. C.; Nardi, N. B. Mesenchymal Stem Cells Reside in Virtually All Post-Natal Organs and Tissues. J Cell Sci 2006, 119 (11), 2204–2213. [CrossRef]
- Wu, L. W.; Wang, Y. L.; Christensen, J. M.; Khalifian, S.; Schneeberger, S.; Raimondi, G.; Cooney, D. S.; Lee, W. P. A.; Brandacher, G. Donor Age Negatively Affects the Immunoregulatory Properties of Both Adipose and Bone Marrow Derived Mesenchymal Stem Cells. Transpl Immunol 2014, 30 (4), 122–127. [CrossRef]
- Richardson, S. M.; Kalamegam, G.; Pushparaj, P. N.; Matta, C.; Memic, A.; Khademhosseini, A.; Mobasheri, R.; Poletti, F. L.; Hoyland, J. A.; Mobasheri, A. Mesenchymal Stem Cells in Regenerative Medicine: Focus on Articular Cartilage and Intervertebral Disc Regeneration. Methods 2016, 99, 69–80. [CrossRef]
- Kim, J. H.; Jo, C. H.; Kim, H. R.; Hwang, Y. Il. Comparison of Immunological Characteristics of Mesenchymal Stem Cells from the Periodontal Ligament, Umbilical Cord, and Adipose Tissue. Stem Cells Int 2018, 2018. [CrossRef]
- Fong, C. Y.; Subramanian, A.; Gauthaman, K.; Venugopal, J.; Biswas, A.; Ramakrishna, S.; Bongso, A. Human Umbilical Cord Wharton’s Jelly Stem Cells Undergo Enhanced Chondrogenic Differentiation When Grown on Nanofibrous Scaffolds and in a Sequential Two-Stage Culture Medium Environment. Stem Cell Rev Rep 2012, 8 (1), 195–209. [CrossRef]
- Gauthaman, K.; Fong, C. Y.; Suganya, C. A.; Subramanian, A.; Biswas, A.; Choolani, M.; Bongso, A. Extra-Embryonic Human Wharton’s Jelly Stem Cells Do Not Induce Tumorigenesis, Unlike Human Embryonic Stem Cells. Reprod Biomed Online 2012, 24 (2), 235–246. [CrossRef]
- Sultana, T.; Lee, S.; Yoon, H. Y.; Lee, J. I. Current Status of Canine Umbilical Cord Blood-Derived Mesenchymal Stem Cells in Veterinary Medicine. Stem Cells Int 2018, 2018. [CrossRef]
- Arutyunyan, I.; Fatkhudinov, T.; Sukhikh, G. Umbilical Cord Tissue Cryopreservation: A Short Review. Stem Cell Res Ther 2018, 9 (1), 1–7. [CrossRef]
- Fortier, L. A.; Travis, A. J. Stem Cells in Veterinary Medicine. Stem Cell Research & Therapy 2011 2:1 2011, 2 (1), 1–6. [CrossRef]
- Voga, M.; Adamic, N.; Vengust, M.; Majdic, G. Stem Cells in Veterinary Medicine—Current State and Treatment Options. Front Vet Sci 2020, 7 (May), 1–20. [CrossRef]
- de Girolamo, L.; Lucarelli, E.; Alessandri, G.; Antonietta Avanzini, M.; Ester Bernardo, M.; Biagi, E.; Teresa Brini, A.; D’Amico, G.; Fagioli, F.; Ferrero, I.; Locatelli, F.; Maccario, R.; Marazzi, M.; Parolini, O.; Pessina, A.; ; Italian Mesenchymal Stem Cell Group (GISM), M. Mesenchymal Stem/Stromal Cells: A New “Cells as Drugs” Paradigm. Efficacy and Critical Aspects in Cell Therapy. Curr Pharm Des 2013, 19 (13), 2459–2473. [CrossRef]
- Álvarez-Viejo, M.; Menéndez-Menéndez, Y.; Otero-Hernández, J. CD271 as a Marker to Identify Mesenchymal Stem Cells from Diverse Sources before Culture. World J Stem Cells 2015, 7 (2), 470–476. [CrossRef]
- Fitter, S.; Gronthos, S.; Ooi, S. S.; Zannettino, A. C. W. The Mesenchymal Precursor Cell Marker Antibody STRO-1 Binds to Cell Surface Heat Shock Cognate 70. Stem Cells 2017, 35 (4), 940–951. [CrossRef]
- Bianco, P. “Mesenchymal” Stem Cells. Annu Rev Cell Dev Biol 2014, 30 (Volume 30, 2014), 677–704. [CrossRef]
- Cen, L. P.; Ng, T. K.; Liang, J. J.; Zhuang, X.; Yao, X.; Yam, G. H. F.; Chen, H.; Cheung, H. S.; Zhang, M.; Pang, C. P. Human Periodontal Ligament-Derived Stem Cells Promote Retinal Ganglion Cell Survival and Axon Regeneration After Optic Nerve Injury. Stem Cells 2018, 36 (6), 844–855. [CrossRef]
- Trounson, A.; McDonald, C. Stem Cell Therapies in Clinical Trials: Progress and Challenges. Cell Stem Cell 2015, 17 (1), 11–22. [CrossRef]
- Musiał-Wysocka, A.; Kot, M.; Majka, M. The Pros and Cons of Mesenchymal Stem Cell-Based Therapies. Cell Transplant 2019, 28 (7), 801–812. [CrossRef]
- Johnson, T. V.; Bull, N. D.; Martin, K. R. Stem Cell Therapy for Glaucoma: Possibilities and Practicalities. Expert Rev Ophthalmol 2011, 6 (2), 165–174. [CrossRef]
- Phelps, J.; Sanati-Nezhad, A.; Ungrin, M.; Duncan, N. A.; Sen, A. Bioprocessing of Mesenchymal Stem Cells and Their Derivatives: Toward Cell-Free Therapeutics. Stem Cells Int 2018, 2018 (1), 9415367. [CrossRef]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T.; Tomoda, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Adult Human Fibroblasts by Defined Factors. Cell 2007, 131 (5), 861–872. [CrossRef]
- De Almeida, P. E.; Ransohoff, J. D.; Nahid, A.; Wu, J. C. Immunogenicity of Pluripotent Stem Cells and Their Derivatives. Circ Res 2013, 112 (3), 549–561. [CrossRef]
- Ding, D. C.; Shyu, W. C.; Lin, S. Z. Mesenchymal Stem Cells. Cell Transplant 2011, 20 (1), 5–14. [CrossRef]
- Johnson, T. V.; Martin, K. R. Cell Transplantation Approaches to Retinal Ganglion Cell Neuroprotection in Glaucoma. Curr Opin Pharmacol 2013, 13 (1), 78–82. [CrossRef]
- Jin, S.; Trope, G. E.; Buys, Y. M.; Badley, E. M.; Thavorn, K.; Yan, P.; Nithianandan, H.; Jin, Y. P. Reduced Social Participation among Seniors with Self-Reported Visual Impairment and Glaucoma. PLoS One 2019, 14 (7), e0218540. [CrossRef]
- Jiang, D.; Xiong, G.; Feng, H.; Zhang, Z.; Chen, P.; Yan, B.; Chen, L.; Gandhervin, K.; Ma, C.; Li, C.; Han, S.; Zhang, Y.; Liao, C.; Lee, T. L.; Tse, H. F.; Fu, Q. L.; Chiu, K.; Lian, Q. Donation of Mitochondria by IPSC-Derived Mesenchymal Stem Cells Protects Retinal Ganglion Cells against Mitochondrial Complex I Defect-Induced Degeneration. Theranostics 2019, 9 (8), 2395–2410. [CrossRef]
- Emre, E.; Yüksel, N.; Duruksu, G.; Pirhan, D.; Subaşi, C.; Erman, G.; Karaöz, E. Neuroprotective Effects of Intravitreally Transplanted Adipose Tissue and Bone Marrow–Derived Mesenchymal Stem Cells in an Experimental Ocular Hypertension Model. Cytotherapy 2015, 17 (5), 543–559. [CrossRef]
- Inoue, Y.; Iriyama, A.; Ueno, S.; Takahashi, H.; Kondo, M.; Tamaki, Y.; Araie, M.; Yanagi, Y. Subretinal Transplantation of Bone Marrow Mesenchymal Stem Cells Delays Retinal Degeneration in the RCS Rat Model of Retinal Degeneration. Exp Eye Res 2007, 85 (2), 234–241. [CrossRef]
- Jiang, Y.; Zhang, Y.; Zhang, L.; Wang, M.; Zhang, X.; Li, X. Therapeutic Effect of Bone Marrow Mesenchymal Stem Cells on Laser-Induced Retinal Injury in Mice. International Journal of Molecular Sciences 2014, Vol. 15, Pages 9372-9385 2014, 15 (6), 9372–9385. [CrossRef]
- Zhang, Y.; Wang, W. Effects of Bone Marrow Mesenchymal Stem Cell Transplantation on Light-Damaged Retina. Invest Ophthalmol Vis Sci 2010, 51 (7), 3742–3748. [CrossRef]
- Harper, M. M.; Grozdanic, S. D.; Blits, B.; Kuehn, M. H.; Zamzow, D.; Buss, J. E.; Kardon, R. H.; Sakaguchi, D. S. Transplantation of BDNF-Secreting Mesenchymal Stem Cells Provides Neuroprotection in Chronically Hypertensive Rat Eyes. Invest Ophthalmol Vis Sci 2011, 52 (7), 4506–4515. [CrossRef]
- Hu, Y.; Tan, H. B.; Wang, X. M.; Rong, H.; Cui, H. P.; Cui, H. Bone Marrow Mesenchymal Stem Cells Protect against Retinal Ganglion Cell Loss in Aged Rats with Glaucoma. Clin Interv Aging 2013, 8, 1467–1470. [CrossRef]
- Manuguerra-Gagné, R.; Boulos, P. R.; Ammar, A.; Leblond, F. A.; Krosl, G.; Pichette, V.; Lesk, M. R.; Roy, D. C. Transplantation of Mesenchymal Stem Cells Promotes Tissue Regeneration in a Glaucoma Model Through Laser-Induced Paracrine Factor Secretion and Progenitor Cell Recruitment. Stem Cells 2013, 31 (6), 1136–1148. [CrossRef]
- Hernandez, M. R.; Miao, H.; Lukas, T. Astrocytes in Glaucomatous Optic Neuropathy. Prog Brain Res 2008, 173, 353–373. [CrossRef]
- Karl, M. O. The Potential of Stem Cell Research for the Treatment of Neuronal Damage in Glaucoma. Cell Tissue Res 2013, 353 (2), 311–325. [CrossRef]
- Evangelho, K.; Mogilevskaya, M.; Losada-Barragan, M.; Vargas-Sanchez, J. K. Pathophysiology of Primary Open-Angle Glaucoma from a Neuroinflammatory and Neurotoxicity Perspective: A Review of the Literature. Int Ophthalmol 2019, 39 (1), 259–271. [CrossRef]
- Fang, C. E. H.; Guo, L.; Hill, D.; Yap, T. E.; Cordeiro, M. F. Neuroprotective Strategies in Glaucoma-Translation to Clinical Trials. OBM Neurobiology. LIDSEN Publishing Inc 2020. [CrossRef]
- Storgaard, L.; Tran, T. L.; Freiberg, J. C.; Hauser, A. S.; Kolko, M. Glaucoma Clinical Research: Trends in Treatment Strategies and Drug Development. Front Med (Lausanne) 2021, 8. [CrossRef]
- Kuriyan, A. E.; Albini, T. A.; Townsend, J. H.; Rodriguez, M.; Pandya, H. K.; Leonard, R. E.; Parrott, M. B.; Rosenfeld, P. J.; Flynn, H. W.; Goldberg, J. L. Vision Loss after Intravitreal Injection of Autologous “Stem Cells” for AMD. N Engl J Med 2017, 376 (11), 1047–1053. [CrossRef]
- Özmert, E.; Arslan, U. Management of Retinitis Pigmentosa by Wharton’s Jelly Derived Mesenchymal Stem Cells: Preliminary Clinical Results. Stem Cell Res Ther 2020, 11 (1). [CrossRef]
- Zhao, T.; Liang, Q.; Meng, X.; Duan, P.; Wang, F.; Li, S.; Liu, Y.; Yin, Z. Q. Intravenous Infusion of Umbilical Cord Mesenchymal Stem Cells Maintains and Partially Improves Visual Function in Patients with Advanced Retinitis Pigmentosa. Stem Cells Dev 2020, 29 (16), 1029–1037. [CrossRef]
- Sung, Y.; Lee, S. M.; Park, M.; Choi, H. J.; Kang, S.; Choi, B. I.; Lew, H. Treatment of Traumatic Optic Neuropathy Using Human Placenta-Derived Mesenchymal Stem Cells in Asian Patients. Regenerative Med 2020, 15 (10), 2163–2179. [CrossRef]
- Weiss, J. N.; Levy, S.; Malkin, A. Stem Cell Ophthalmology Treatment Study (SCOTS) for Retinal and Optic Nerve Diseases: A Preliminary Report. Neural Regen Res 2015, 10 (6), 982–988. [CrossRef]
- Weiss, J. N.; Levy, S.; Benes, S. C. Stem Cell Ophthalmology Treatment Study (SCOTS) for Retinal and Optic Nerve Diseases: A Case Report of Improvement in Relapsing Auto-Immune Optic Neuropathy. Neural Regen Res 2015, 10 (9), 1507–1515. [CrossRef]
- Weiss, J. N.; Benes, S. C.; Levy, S. Stem Cell Ophthalmology Treatment Study (SCOTS): Improvement in Serpiginous Choroidopathy Following Autologous Bone Marrow Derived Stem Cell Treatment. Neural Regen Res 2016, 11 (9), 1512–1516. [CrossRef]
- Weiss, J. N.; Levy, S.; Benes, S. C. Stem Cell Ophthalmology Treatment Study (SCOTS): Bone Marrow-Derived Stem Cells in the Treatment of Leber’s Hereditary Optic Neuropathy. Neural Regen Res 2016, 11 (10), 1685–1694. [CrossRef]
- Weiss, J. N.; Levy, S.; Benes, S. C. Stem Cell Ophthalmology Treatment Study: Bone Marrow Derived Stem Cells in the Treatment of Non-Arteritic Ischemic Optic Neuropathy (NAION). Stem Cell Investig 2017, 4 (11). [CrossRef]
- Weiss, J. N.; Levy, S. Stem Cell Ophthalmology Treatment Study: Bone Marrow Derived Stem Cells in the Treatment of Retinitis Pigmentosa. Stem Cell Investig 2018, 5 (June). [CrossRef]
- Weiss, J. N.; Levy, S. Dynamic Light Scattering Spectroscopy of the Retina-a Non-Invasive Quantitative Technique to Objectively Document Visual Improvement Following Ocular Stem Cell Treatment. Stem Cell Investig 2019, 6 (April). [CrossRef]
- Weiss, J. N.; Levy, S. Stem Cell Ophthalmology Treatment Study (SCOTS): Bone Marrow Derived Stem Cells in the Treatment of Usher Syndrome. Stem Cell Investig 2019, 6 (September). [CrossRef]
- Weiss, J. N.; Levy, S. Stem Cell Ophthalmology Treatment Study (SCOTS): Bone Marrow Derived Stem Cells in the Treatment of Dominant Optic Atrophy. Stem Cell Investig 2019, 6. [CrossRef]
- Weiss, J. N.; Levy, S. Stem Cell Ophthalmology Treatment Study (SCOTS): Bone Marrow-Derived Stem Cells in the Treatment of Age-Related Macular Degeneration. Medicines (Basel) 2020, 7 (4), 16. [CrossRef]
- Weiss, J. N.; Levy, S. Stem Cell Ophthalmology Treatment Study (SCOTS): Bone Marrow-Derived Stem Cells in the Treatment of Stargardt Disease. Medicines (Basel) 2021, 8 (2), 10. [CrossRef]
- Vilela, C. A. P.; Messias, A.; Calado, R. T.; Siqueira, R. C.; Silva, M. J. L.; Covas, D. T.; Paula, J. S. Retinal Function after Intravitreal Injection of Autologous Bone Marrow-Derived Mesenchymal Stromal Cells in Advanced Glaucoma. Doc Ophthalmol 2021, 143 (1), 33–38. [CrossRef]
- Weiss, J. N.; Levy, S.; Malkin, A. Stem Cell Ophthalmology Treatment Study (SCOTS) for Retinal and Optic Nerve Diseases: A Preliminary Report. Neural Regen Res 2015, 10 (6), 982–988. [CrossRef]
- Weiss, J. N.; Levy, S.; Benes, S. C. Stem Cell Ophthalmology Treatment Study (SCOTS) for Retinal and Optic Nerve Diseases: A Case Report of Improvement in Relapsing Auto-Immune Optic Neuropathy. Neural Regen Res 2015, 10 (9), 1507–1515. [CrossRef]
- Weiss, J. N.; Benes, S. C.; Levy, S. Stem Cell Ophthalmology Treatment Study (SCOTS): Improvement in Serpiginous Choroidopathy Following Autologous Bone Marrow Derived Stem Cell Treatment. Neural Regen Res 2016, 11 (9), 1512–1516. [CrossRef]
- Kasetty, M. A.; Hedges, T. R.; Witkin, A. J. BILATERAL EPIRETINAL MEMBRANE FORMATION AFTER INTRAVITREAL INJECTIONS OF AUTOLOGOUS MESENCHYMAL STEM CELLS. Retin Cases Brief Rep 2022, 16 (5), 561–564. [CrossRef]
- Weiss, J. N.; Levy, S.; Benes, S. C. Stem Cell Ophthalmology Treatment Study (SCOTS): Bone Marrow-Derived Stem Cells in the Treatment of Leber’s Hereditary Optic Neuropathy. Neural Regen Res 2016, 11 (10), 1685–1694. [CrossRef]
- Yang, N.; Zeng, S.; Yang, J.; Lu, G.; Du, L. Application of Platelet-Rich Fibrin Transplantation for Large Macular Hole. Curr Eye Res 2022, 47 (5), 770–776. [CrossRef]
- Yang, N.; Xing, Y.; Zhao, Q.; Zeng, S.; Yang, J.; Du, L. Application of Platelet-Rich Fibrin Grafts Following Pterygium Excision. Int J Clin Pract 2021, 75 (10). [CrossRef]
- Roubeix, C.; Godefroy, D.; Mias, C.; Sapienza, A.; Riancho, L.; Degardin, J.; Fradot, V.; Ivkovic, I.; Picaud, S.; Sennlaub, F.; Denoyer, A.; Rostene, W.; Sahel, J. A.; Parsadaniantz, S. M.; Brignole-Baudouin, F.; Baudouin, C. Intraocular Pressure Reduction and Neuroprotection Conferred by Bone Marrow-Derived Mesenchymal Stem Cells in an Animal Model of Glaucoma. Stem Cell Res Ther 2015, 6 (1). [CrossRef]
Figure 1.
Congenital unilateral glaucoma in the right eye of a kitten with development of severe buphthalmia.
Figure 1.
Congenital unilateral glaucoma in the right eye of a kitten with development of severe buphthalmia.

Figure 2.
Comparison of Open-Angle and Angle-Closure Glaucoma. In open-angle glaucoma, the drainage angle remains open, but the trabecular meshwork gradually becomes less efficient at allowing aqueous humor to exit, leading to increased intraocular pressure. In angle-closure glaucoma, the drainage angle is blocked, preventing the outflow of aqueous humor and causing a rapid rise in intraocular pressure. Images were used with permission from Servier Medical Art by Servier, licensed under a Creative Commons Attribution 4.0 International License.
Figure 2.
Comparison of Open-Angle and Angle-Closure Glaucoma. In open-angle glaucoma, the drainage angle remains open, but the trabecular meshwork gradually becomes less efficient at allowing aqueous humor to exit, leading to increased intraocular pressure. In angle-closure glaucoma, the drainage angle is blocked, preventing the outflow of aqueous humor and causing a rapid rise in intraocular pressure. Images were used with permission from Servier Medical Art by Servier, licensed under a Creative Commons Attribution 4.0 International License.
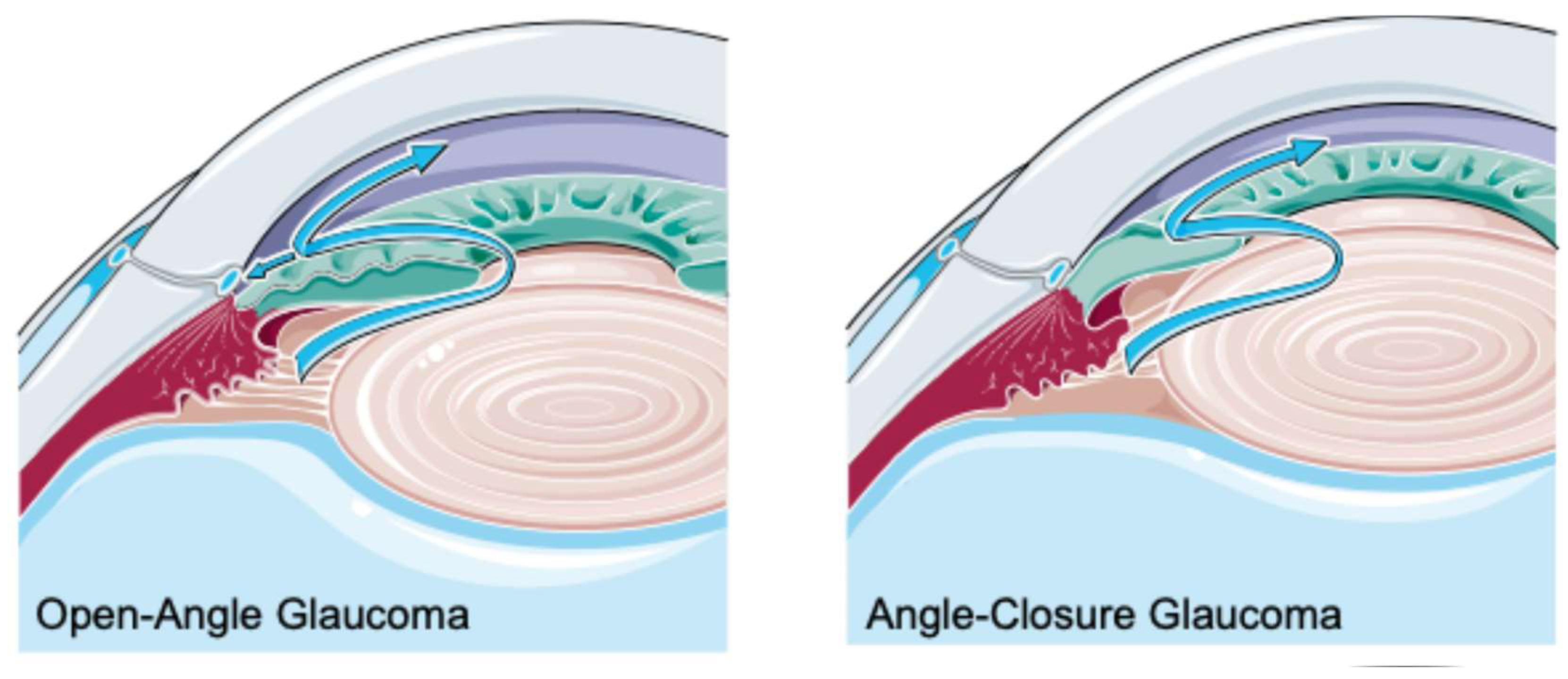
Figure 3.
(a) - Chronic glaucoma in a dog showing conjunctival and episcleral congestion, corneal oedema, neovascularization and multiple corneal Haab’s striae corresponding to breaks in the Descemet membrane. You can also identify a ruptured iris cyst adherent to the corneal endothelium in the center of the cornea and a moderately dilated pupil where you can see a posterior subluxated lens; (b) - Chronic glaucoma in a dog showing corneal oedema, neopigmentation near the limbus, neovascularization and multiple corneal Haab´s striae. Through the completely dilated pupil it is possible to see the fundus, showing marked retinal atrophy with complete retinal vascular attenuation, tapetal hyperreflectivity and optic disk atrophy and cupping.
Figure 3.
(a) - Chronic glaucoma in a dog showing conjunctival and episcleral congestion, corneal oedema, neovascularization and multiple corneal Haab’s striae corresponding to breaks in the Descemet membrane. You can also identify a ruptured iris cyst adherent to the corneal endothelium in the center of the cornea and a moderately dilated pupil where you can see a posterior subluxated lens; (b) - Chronic glaucoma in a dog showing corneal oedema, neopigmentation near the limbus, neovascularization and multiple corneal Haab´s striae. Through the completely dilated pupil it is possible to see the fundus, showing marked retinal atrophy with complete retinal vascular attenuation, tapetal hyperreflectivity and optic disk atrophy and cupping.
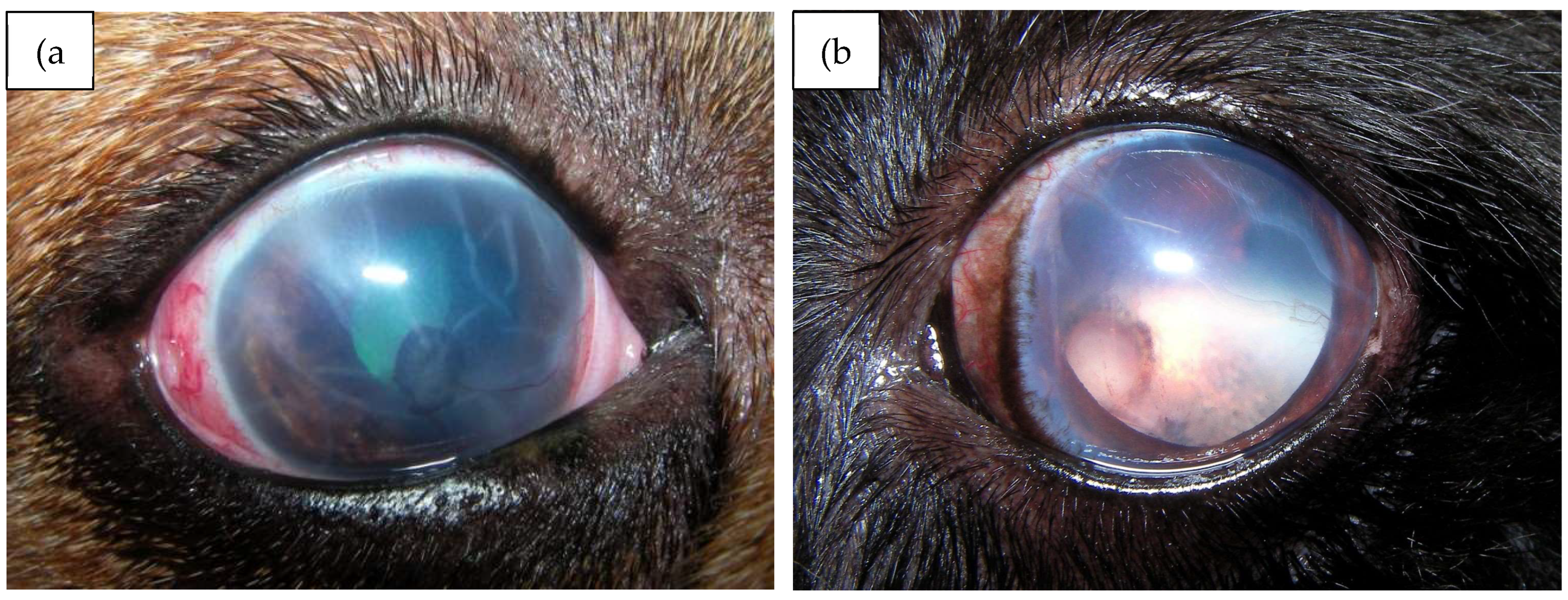
Figure 4.
UC-MSCs in culture showing a typical fibroblastic-like morphology; (a) - Magnification: 100x; (b) - Magnification: 600x).
Figure 4.
UC-MSCs in culture showing a typical fibroblastic-like morphology; (a) - Magnification: 100x; (b) - Magnification: 600x).
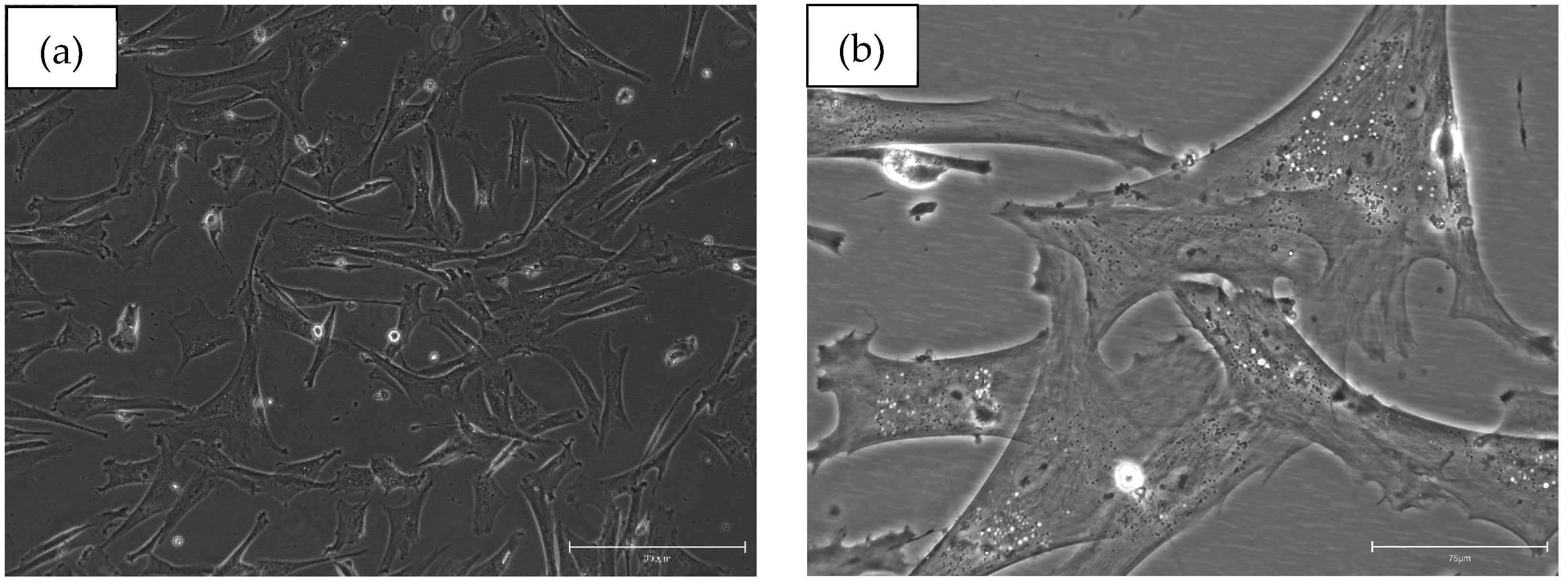

Table 1.
Overview of clinical trials investigating stem cell-based therapies and other therapeutic options for glaucoma treatment.
Table 1.
Overview of clinical trials investigating stem cell-based therapies and other therapeutic options for glaucoma treatment.
| Study public title | NCT number, location and date | Eye conditions | Treatment | Status | Sample size/target | Results |
|---|---|---|---|---|---|---|
| Safety of Cultured Allogeneic Adult Umbilical Cord Derived Mesenchymal Stem Cells for Eye Diseases | NCT05147701 Antigua, Barbuda, Argentina (2022-2026) |
Macular Degeneration Optic Atrophy Retinitis Pigmentosa Eye Diseases Traumatic Optic Neuropathy Diabetic Retinopathy Glaucoma |
AlloRx (cultured allogeneic adult umbilical cord derived MSCs, intravenous and sub-tenon delivery, total dose of 100 million cells) |
Recruiting | 20 | [139,140,141] |
| Stem Cell Ophthalmology Treatment Study II (SCOTS2) | NCT03011541 United States, United Arab Emirates (2016-2026) |
Age-Related Macular Degeneration Glaucoma Retinopathy Hereditary Optic Neuropathy Macular Degeneration Blindness (…) |
Arm 1 (Autologous bone marrow derived stem cells provided retrobulbar, subtenon and intravenous for one or both eyes) |
Recruiting | 500 | [142,143,144,145,146,147,148,149,150,151,152] |
| Intravitreal Mesenchymal Stem Cell Transplantation in Advanced Glaucoma. | NCT02330978 Brazil (2014-2019) |
Retinal degeneration POAG |
Intravitreal transplantation of autologous bone-marrow mesenchymal stem cells (BM-MSCs) | Completed | 2 | [153] |
| Stem Cell Ophthalmology Treatment Study (SCOTS) | NCT01920867 United States, United Arab Emirates (2013-2019) |
Macular Degeneration Hereditary Retinal Dystrophy Optic Nerve Disease Glaucoma Retinal Disease |
Intraocular, retrobulbar, intravenous, subtenon, intravitreal transplantation of autologous BM-MSCs | Unknown | 300 | [154,155,156,157,158] |
| Platelet-rich Fibrin (PRF) Membrane in Ophthalmic Diseases | NCT06200727 China (2023-2025) |
Platelet-rich Fibrin Macular Holes Pterygium Glaucoma |
Autologous PRF membrane grafting/ amniotic membrane to cover the exposed sclera after trabeculectomy for glaucoma. |
Active, not recruiting |
170 | [159,160] |
| Effectiveness and Safety of Adipose-Derived Regenerative Cells for Treatment of Glaucomatous Neurodegeneration | NCT02144103 Moscow, Russian federations (2014-2019) |
Retinal degeneration POAG |
ADRC injection: liposuction to isolate adipose-derived regenerative cells (ADRC). The concentrated ADRCs will then be injected into the subtenon space of the patient’s eye. |
Unknown | 16 | No results reported yet |
| Efficacy of NSAID vs. Steroid-NSAID Combo Post-Selective Laser Trabeculoplasty: Phase 4, Single-Center RCT (CES-NSLT) | NCT06498440 Canada (2024-2025) |
Open Angle Glaucoma Ocular Hypertension Postoperative Inflammation |
Ketorolac 0.5% eye drops; Ketorolac 0.5% and Fluorometholone 0.1% eye drops |
Not yet recruiting |
126 | No results reported yet |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



