
Submitted:
09 November 2024
Posted:
11 November 2024
You are already at the latest version
Abstract
Acute promyelocytic leukemia (APL) is characterized by abnormal promyelocytes and t(15;17)(q24;q21) PML::RARA. Rarely, patients may have cryptic or variant rearrangements. All-trans retinoic acid (ATRA)/arsenic trioxide (ATO) is largely curative provided that the diagnosis is established early. We present a case in which the diagnostic work-up suggested a diagnosis of APL; however, FISH, using the PML/RARA dual fusion and RARA breakapart probes, was negative. RT-PCR later revealed a cryptic fusion transcript. Optical genome mapping (OGM) confirmed the nature and orientation of the insertion of RARA into PML. This case underscores the importance of performing alternative testing in FISH-negative cases of APL.
Keywords:
Acute promyelocytic leukemia
; APL
; cryptic PML::RARA
; cryptic APL
Introduction
Acute promyelocytic leukemia (APL) is a subtype of acute myeloid leukemia (AML) which accounts for approximately 5-8% of all new AML diagnoses in young adults [1]. Patients present with features of coagulopathy and are at increased risk for disseminated intravascular coagulation (DIC) [1]. Morphologically, APL is characterized by abundant abnormal promyelocytes with a classic immunophenotype demonstrable by flow cytometry [1]. Per the WHO classification, the diagnosis of APL is rendered based on these microscopic findings in conjunction with t(15;17)(q24.1;q21.2). This rearrangement results in the fusion of the 5’ end of the promyelocytic leukemia (PML) gene (exons 1-3) on chromosome 15 with the 3’ end of the retinoic acid receptor alpha (RARA) gene (exons 3-9) on chromosome 17 [1,2,3]. The International Consensus Classification of Myeloid Neoplasms and Acute Leukemias (ICC) requires at least 10% blasts (or blast equivalents, i.e., abnormal promyelocytes) for diagnosis [2]. Morphologic subtypes of APL include the hypergranular (i.e., typical) and hypogranular (i.e., microgranular) forms (with a basophilic variant described in some studies) [2]. Notably, most APL subtypes, including cases with variant RARA translocations, demonstrate similar morphologies [2].
The t(15;17)(q24.1;q21.2) translocation can usually be identified by fluorescence in situ hybridization (FISH) using PML/RARA dual fusion or RARA breakapart probes or chromosomal Giemsa (G)-banding analysis. The reciprocal t(15;17) translocation is present in 90-95% of APL cases, and, depending on the location of the PML breakpoint, three PML::RARA fusion transcript isoforms can be produced: long (bcr1; intron 6), variant (bcr2; exon 6), and short (bcr3; intron 3), with the bcr1 and bcr3 isoforms being the most common [1,4,5]. Rarely, atypical isoforms can be also be detected [1]. The RARA breakpoint consistently occurs within intron 2 [4]. A subset of APL cases (~5-9%) [6] may show cryptic PML::RARA rearrangement with submicroscopic insertion of PML to RARA, or complex rearrangements involving other chromosomes. Other cases of APL (~1-2%) [7] may show variant RARA rearrangements [1,3,8,9,10,11,12,13]. Importantly, cases of APL with cryptic rearrangements may require alternative methods of detection [1].
Herein, we describe a case of cryptically rearranged APL. Fortunately, the patient had been initiated on all-trans retinoic acid (ATRA)/arsenic trioxide (ATO) early based on the morphological/immunophenotypic findings and demonstrated clinical improvement. These findings, in conjunction with those of our systematic literature review, highlight the importance of performing confirmatory testing in FISH-negative cases of suspected APL.
Materials and Methods
Pathological Examination
Standard Wright Giemsa peripheral blood smears were prepared.
Clinical Flow Cytometry Evaluation
Expression of cell surface markers was measured by flow cytometry (Navios, Beckman Coulter) using the ClearLLab 10C 10-color lymphoid and myeloid panels and analyzed using the Kaluza analysis software.
Chromosome G-Banding Karyotype Analysis
Cytogenetic analysis was performed using short-term bone marrow cultures per routine laboratory protocol. For microscopic analysis, metaphase chromosomes were stained using the trypsin-Giemsa technique [14]. For chromosome analysis, 20 cells were analyzed and two to five metaphases were karyotyped. Chromosomal abnormalities were defined according to ISCN (2020) [15].
Fluorescence In Situ Hybridization
Fluorescence in situ hybridization (FISH) was performed on 200 interphase nuclei using the AML panel probes (Abbott Molecular/Vysis, Inc.): LSI EGR1 (5q31) SO/D5S23, D5S721 SG, LSI D7S486 (7q31) SO/CEP 7 (D7Z1) SG, LSI RUNX1T1/RUNX1 Dual Color, Dual Fusion Translocation, LSI KMT2A Dual Color, Break Apart Rearrangement, LSI PML/RARA Dual Color, Dual Fusion Translocation, LSI CBFB Dual Color, Break Apart Rearrangement, LSI 13 (13q14) SG/LSI TP53 (17p13.1) SO, and LSI RARA Dual Color, Break Apart Rearrangement probes. Retrospective interphase FISH using the CytoCell (Oxford Gene Technology) PML/RARA dual color dual fusion probe set was performed, followed by confirmatory metaphase FISH using the CytoCell probe.
Mutational Analysis
FLT3 mutational analysis was performed using rapid multiplex PCR. Targeted DNA-based NGS was performed using the 34-gene Illumina TruSight Myeloid Panel.
Optical Genome Mapping
Optical Genome Mapping (OGM) was performed as described previously [16]. Briefly, ultra-high molecular weight DNA was isolated from the patient’s peripheral blood sample using the SP Blood and Cell Culture DNA Isolation Kit. The DLS DNA Labeling Kit was used to fluorescently label long molecules at specific CTTAAG motifs throughout the genome with the enzyme DLE-1 (Bionano Genomics). Labelled DNA was loaded onto a chip and imaged on the Saphyr instrument for the collection of 1500 Gb data with a molecule size of >150 kb. Data analysis was performed using the Bionano Access Software (BAS) Version 1.8.1 and Variant Intelligence Analysis (VIA) version 7.0
Systematic Literature Review
A systematic literature review was conducted through a targeted search (using the following search terms: “APL with cryptic translocation,” “APL with negative FISH,” “APML with negative FISH,” and “APL with RT-PCR”) for case reports and original articles published in English journals from 2013 – 2023 archived in PubMed.
Results
Case Description
A 36-year-old male presented with spontaneous ecchymosis, petechiae, and exertional dyspnea. Laboratory investigations revealed anemia (hemoglobin 11.2 g/dL), thrombocytopenia (platelets 10 THOU/µL), hypofibrinogenemia (70 mg/dL), prolonged prothrombin time (14.7 seconds)/international normalization ratio (INR) (1.3), and elevated D-dimer (26.20 µg/mL), concerning for DIC. Peripheral blood examination demonstrated pancytopenia. Scattered promyelocytes with bilobed nuclei, occasional Auer rods, and variable cytoplasmic granules were noted by microscopy, raising concern for APL (Figure 1A). Consistent with this preliminary diagnosis, flow cytometry evaluation revealed an abnormal cell population within the CD45-dim gate with high side scatter and co-expression of CD13, CD33, CD117, CD38, CD123, CD64, and cytoplasmic myeloperoxidase (MPO), while negative for all other markers tested (Figure 1B).
Stat FISH, however, was negative for the classical t(15;17) rearrangement (Figure 2).
Given the clinical concern for APL, rapid real-time polymerase chain reaction (RT-PCR) was performed, which detected a cryptic PML::RARA gene rearrangement (bcr3 transcript isoform). Despite negative FISH results, the patient had been started on all-trans retinoic acid (ATRA)/arsenic trioxide (ATO) therapy early based on the classical immunomorphology. Targeted DNA-based NGS subsequently revealed an oncogenic mutation in NRAS (c.35G>T, p.G12V) at a variant allele frequency (VAF) of 11%. Retrospective FISH using the CytoCell PML/RARA dual color dual fusion probe set revealed a fusion in 74% of interphase cells, suggestive of an insertion of the RARA gene into the PML gene (Figure 2B). Metaphase FISH also confirmed this aberration (Figure 2C). Further analysis using OGM revealed an insertion in the PML gene at intron 3 (bcr3 transcript) and missing molecules on 17q21.2 from exons 1 – 2 in the RARA gene with the breakpoint in intron 2 (Figure 3). Presently, the patient is in remission and undergoing consolidation therapy.
Literature Review
A total of 71 articles were retrieved, of which 29 articles were selected for further evaluation based on preliminary abstract review. Of these, 17 articles described single case reports of APL with cryptic PML::RARA rearrangements and are summarized in Table 1. The remaining reports are described below.
Discussion
While APL can be suspected based on clinical presentation and pathology evaluation [17], the definitive diagnosis requires the demonstration of the cytogenetic hallmark, t(15;17)(q24;q21) translocation by G-banding or targeted FISH. The chimeric PML::RARA oncoprotein, along with secondarily acquired genetic aberrations (e.g. mutations in FLT3 ITD, WT1, NRAS, or KRAS) [18,19], impair myeloid differentiation and drive leukemogenesis. We describe a case of APL that presented with signs of clinical coagulopathy. Although pathology evaluation in our patient suggested a diagnosis of APL, stat FISH and karyotype analysis were negative for t(15;17)(q24;q21). Concomitant RT-PCR revealed a cryptic PML::RARA gene fusion. Fortunately, the patient had been initiated on ATRA/ATO and demonstrated clinical improvement. Accordingly, we performed a systematic literature review to understand the prevalence, diagnosis, and prognosis of APL with cryptic PML::RARA translocations.
Several individual reports of APL with little-to-no cytogenetic evidence of t(15;17) but with nearly identical clinical presentations and morphologies have been reported in the literature, with RT-PCR later revealing a cryptic PML::RARA fusion (Table 1) [20,21,22]. In an institutional analysis over an 18.5-year timeframe, Gagnon et al found the majority of APL cases (87% [723/831]) to possess balanced PML::RARA translocations by chromosomal banding analysis and PML::RARA dual-color, dual-fusion FISH (Abbott) [6]. Of the remaining 13% of patients, only 0.7% (6/831) were found to harbor a cryptic PML::RARA gene fusion, confirmed by retrospective metaphase FISH in two cases [6]. Goldschmidt et al describe a case of APL with a cryptic PML::RARA gene rearrangement, in which subsequent metaphase FISH revealed an interstitial insertion of RARA into PML [23]. Burns et al present a similar case but with an insertion of PML into RARA.22 Interestingly, in a case of APL with a cryptic PML::RARA translocation, identified by RT-PCR, Koshy et al detected a 49-kilobase duplication of 15q24.1 by SNP microarray, which likely inserted into chromosome 19 or 20; they hypothesize that the RARA insert in this case was too small to detect using FISH or microarray [24]. Other methods of confirmation include sequencing (both Sanger and next-generation).
Likewise, atypical karyotypic findings are present in nearly 52% of cases of cryptically-rearranged APL [25]. Chromosomal aberrations reported in conjunction with cryptic PML::RARA rearrangements include trisomy 8 (most common) [4],4 trisomy 9 [23], i(5p) [23], complex karyotypes [26,27], and structural rearrangements involving chromosome 17 [3] (e.g., isochromosome 17q) [27,28,29,30]. Few studies suggest the presence of i(17q) in such cases to confer a worse prognosis, with short complete response durations and high rates of relapse [27]. Similarly, rearrangements involving chromosomes 3, 7, 9, 11, 17, and 22 have also been reported in association with cases of FISH-negative APL [31]. Of note, the presence of structural karyotypes does not seem to affect treatment response to ATRA/ATO [26].
Importantly, all patients with APL resulting from a cryptic t(15;17) achieved remission following treatment with ATRA/ATO [3,20,21]. Greenfield et al compared five patients with cryptically-rearranged APL to eight patients with APL resulting from the reciprocal t(15;17)(q24.1;q21.2) and found no significant difference in disease behavior or prognosis [32]. Furthermore, previous reports observed the bcr3 isoform to be more frequent in cases of cryptic PML::RARA-rearranged APL (61% of cases) [4], as was observed in our case. Although this isoform has been associated with leukocytosis and a poorer prognosis, further studies are needed to understand the association, if any [5,23,25].
Given the aggressive coagulopathy associated with APL (85% of cases) [4], it is imperative that cryptic PML::RARA translocations are identified early to initiate ATRA/ATO given the resistance of APL to standard induction chemotherapy regimens. FISH is an invaluable tool to detect the classical t(15;17) translocation with a resolution of nearly 200 kb; however, cryptic cases may be missed due to submicroscopic insertions unable to be visualized by fluorescent microscopy [33]. Although smaller custom FISH probes can be applied [33], alternative testing modalities, such as PCR, OGM, or sequencing, may be required to establish a diagnosis of APL [5,20,21,24,34,35]. Seldom, RT-PCR may also be negative in the case of an atypical PML::RARA rearrangement with a new breakpoint in PML that is not readily identifiable using routine primers [23]. Finally, both conventional cytogenetics and RT-PCR may fail to yield a positive result, such as cases with a submicroscopic deletion of 3’ RARA or cases with no RARA rearrangement [23,36,37].
Regardless, a high degree of clinical suspicion and prompt recognition are required in suspected cases of APL for immediate initiation of ATRA/ATO [4,38]. Although rare, cryptically-rearranged APL poses a diagnostic challenge and may require alternative, parallel testing modalities to establish the diagnosis [33,38].
Author Contributions
GVG wrote the manuscript with input from MUE. AGE, SA, BZ, and MAI provided edits. All authors reviewed and approved the final version of the manuscript.
Funding
This research received no funding.
Data Availability
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no potential conflicts of interest.
Patient Consent
Informed consent was not required for this study as no patient identifying information has been included.
References
- Alaggio R AC, Anagnostopoulos I, Attygalle AD, Araujo IBO, Berti E, Bhagat G, Borges AM, Boyer D, Calaminici M, Chadburn A, Chan JKC, Cheuk W, Chng WJ, Choi JK, Chuang SS, Coupland SE, Czader M, Dave SS, de Jong D, Du MQ, Elenitoba-Johnson KS, Ferry J, Geyer J, Gratzinger D, Guitart J, Gujral S, Harris M, Harrison CJ, Hartmann S, Hochhaus A, Jansen PM, Karube K, Kempf W, Khoury J, Kimura H, Klapper W, Kovach AE, Kumar S, Lazar AJ, Lazzi S, Leoncini L, Leung N, Leventaki V, Li XQ, Lim MS, Liu WP, Louissaint A, Jr., Marcogliese A, Medeiros LJ, Michal M, Miranda RN, Mitteldorf C, Montes-Moreno S, Morice W, Nardi V, Naresh KN, Natkunam Y, Ng SB, Oschlies I, Ott G, Parrens M, Pulitzer M, Rajkumar SV, Rawstron AC, Rech K, Rosenwald A, Said J, Sarkozy C, Sayed S, Saygin C, Schuh A, Sewell W, Siebert R, Sohani AR, Tooze R, Traverse-Glehen A, Vega F, Vergier B, Wechalekar AD, Wood B, Xerri L, Xiao W. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022;36:1720-48.
- Stone M, Lilley CM, Tang G, Loghavi S, Mirza KM. Phenotypic clues that predict underlying cytogenetic/genetic abnormalities in myeloid malignancies: A contemporary review. Cytopathology 2023;34(6):530-541. (In eng). [CrossRef]
- El-Hajj Ghaoui R, St Heaps L, Hung D, et al. A Paediatric Acute Promyelocytic Leukaemia Patient Harbouring a Cryptic PML-RARA Insertion due to a Complex Structural Chromosome 17 Rearrangement. Cytogenet Genome Res 2017;153(4):181-189. (In eng). [CrossRef]
- Rashidi A, Fisher SI. FISH-negative, cytogenetically cryptic acute promyelocytic leukemia. Blood Cancer J 2015;5(6):e320. (In eng). [CrossRef]
- Kim MJ, Cho SY, Kim MH, et al. FISH-negative cryptic PML-RARA rearrangement detected by long-distance polymerase chain reaction and sequencing analyses: a case study and review of the literature. Cancer Genet Cytogenet 2010;203(2):278-83. (In eng). [CrossRef]
- Gagnon MF, Berg HE, Meyer RG, et al. Typical, atypical and cryptic t(15;17)(q24;q21) (PML::RARA) observed in acute promyelocytic leukemia: A retrospective review of 831 patients with concurrent chromosome and PML::RARA dual-color dual-fusion FISH studies. Genes Chromosomes Cancer 2022;61(10):629-634. (In eng). [CrossRef]
- Singh MK, Parihar M, Arora N, Mishra DK, Bhave SJ, Chandy M. Diagnosis of variant RARA translocation using standard dual-color dual-fusion PML/RARA FISH probes: An illustrative report. Hematol Oncol Stem Cell Ther 2019;12(1):50-53. (In eng). [CrossRef]
- Catalano A, Dawson MA, Somana K, et al. The PRKAR1A gene is fused to RARA in a new variant acute promyelocytic leukemia. Blood 2007;110(12):4073-6. (In eng). [CrossRef]
- Osumi T, Watanabe A, Okamura K, et al. Acute promyelocytic leukemia with a cryptic insertion of RARA into TBL1XR1. Genes Chromosomes Cancer 2019;58(11):820-823. (In eng). [CrossRef]
- Pardo Gambarte L, Franganillo Suarez A, Cornago Navascues J, et al. ZBTB16-RARalpha-Positive Atypical Promyelocytic Leukemia: A Case Report. Medicina (Kaunas) 2022;58(4) (In eng). [CrossRef]
- Wang Y, Rui Y, Shen Y, et al. Myeloid Sarcoma Type of Acute Promyelocytic Leukemia With a Cryptic Insertion of RARA Into FIP1L1: The Clinical Utility of NGS and Bioinformatic Analyses. Front Oncol 2021;11:688203. (In eng). [CrossRef]
- Peterson JF, He RR, Nayer H, et al. Characterization of a rarely reported STAT5B/RARA gene fusion in a young adult with newly diagnosed acute promyelocytic leukemia with resistance to ATRA therapy. Cancer Genet 2019;237:51-54. (In eng). [CrossRef]
- Yao L, Wen L, Wang N, et al. Identification of novel recurrent STAT3-RARA fusions in acute promyelocytic leukemia lacking t(15;17)(q22;q12)/PML-RARA. Blood 2018;131(8):935-939. (In eng). [CrossRef]
- Seabright M. A rapid banding technique for human chromosomes. Lancet 1971;2(7731):971-2. (In eng). [CrossRef]
- An International System for Human Cytogenomic Nomenclature.: S.Karger AG., 2020.
- Pang AWC, Kosco K, Sahajpal NS, Sridhar A, Hauenstein J, Clifford B, Estabrook J, Chitsazan AD, Sahoo T, Iqbal A, Kolhe R, Raca G, Hastie AR, Chaubey A. Analytic Validation of Optical Genome Mapping in Hematological Malignancies. Biomedicines. 2023 Dec 9;11(12):3263. doi: 10.3390/biomedicines11123263. PMID: 38137484; PMCID: PMC10741484.
- Liu G, Liu L, Bartolo DD, Li KY, Li X. Acute Promyelocytic Leukemia with Rare Genetic Aberrations: A Report of Three Cases. Genes (Basel) 2022;14(1) (In eng). [CrossRef]
- Fasan A, Haferlach C, Perglerova K, Kern W, Haferlach T. Molecular landscape of acute promyelocytic leukemia at diagnosis and relapse. Haematologica 2017;102(6):e222-e224. (In eng). [CrossRef]
- Madan V, Shyamsunder P, Han L, et al. Comprehensive mutational analysis of primary and relapse acute promyelocytic leukemia. Leukemia 2016;30(8):1672-81. (In eng). [CrossRef]
- Blanco EM, Curry CV, Lu XY, et al. Cytogenetically cryptic and FISH-negative PML/RARA rearrangement in acute promyelocytic leukemia detected only by PCR: an exceedingly rare phenomenon. Cancer Genet 2014;207(1-2):48-9. (In eng). [CrossRef]
- Avgerinou G, Katsibardi K, Filippidou M, Tzanoudaki M, Papadhimitriou SI, Kattamis A. Cytogenetically cryptic and fish negative PML/RARA rearrangement in acute promyelocytic leukemia detected by RT-PCR. Leuk Lymphoma 2020;61(14):3526-3528. (In eng). [CrossRef]
- Burns TF, Loo EY, Bengtson EM, Bao L. Cytogenetically cryptic insertion of PML segment into RARA on chromosome 17q resulting PML-RARA fusion in acute promyelocytic leukemia. Ann Hematol 2019;98(1):211-213. (In eng). [CrossRef]
- Goldschmidt N, Yehuda-Gafni O, Abeliovich D, Slyusarevsky E, Rund D. Interstitial insertion of RARalpha gene into PML gene in a patient with acute promyelocytic leukemia (APL) lacking the classic t(15;17). Hematology 2010;15(5):332-7. (In eng). [CrossRef]
- Koshy J, Qian YW, Bhagwath G, Willis M, Kelley TW, Papenhausen P. Microarray, gene sequencing, and reverse transcriptase-polymerase chain reaction analyses of a cryptic PML-RARA translocation. Cancer Genet 2012;205(10):537-40. (In eng). [CrossRef]
- Karlin K, Bryke C, Dias A, Michaels P. Cytogenetically cryptic PML::RARA fusion in acute promyelocytic leukemia: Testing strategies in the modern era. Leuk Res Rep 2022;17:100320. (In eng). [CrossRef]
- Gu S, Zi J, Ma J, Ge Z. Cryptic t(15;17) acute promyelocytic leukemia with a karyotype of add(11)(p15) and t(13,20)- A case report with a literature review. Bosn J Basic Med Sci 2021;21(2):246-251. (In eng). [CrossRef]
- Tang Y, Wang Y, Hu L, et al. Acute promyelocytic leukemia with cryptic t(15;17) on isochromosome 17: a case report and review of literature. Int J Clin Exp Pathol 2015;8(11):15294-300. (In eng) (https://www.ncbi.nlm.nih.gov/pubmed/26823883).
- Shepshelovich D, Oniashvili N, Parnes D, et al. Acute promyelocytic leukemia with isochromosome 17q and cryptic PML-RARA successfully treated with all-trans retinoic acid and arsenic trioxide. Cancer Genet 2015;208(11):575-9. (In eng). [CrossRef]
- Cervera J, Montesinos P, Hernandez-Rivas JM, et al. Additional chromosome abnormalities in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and chemotherapy. Haematologica 2010;95(3):424-31. (In eng). [CrossRef]
- Kim M, Lim J, Kim Y, et al. The genetic characterization of acute promyelocytic leukemia with cryptic t(15;17) including a new recurrent additional cytogenetic abnormality i(17)(q10). Leukemia 2008;22(4):881-3. (In eng). [CrossRef]
- Mahmud W, Brown R, Buckingham L, Tira A, Katz DA. Cryptic partial insertion of the RARA gene into the PML gene without reciprocal RARA-PML fusion: a case report and review of literature. Acta Oncol 2020;59(12):1496-1499. (In eng). [CrossRef]
- Greenfield G, Michail O, Merron B, McGimpsey J, Catherwood M, McMullin MF. Acute promyelocytic leukaemia (APML) with cryptic PML-RARA fusion has a clinical course comparable to classical APML with t(15;17)(q24.1;q21.2) translocation. Br J Haematol 2019;186(1):155-157. (In eng). [CrossRef]
- Mohebnasab M, Li P, Hong B, et al. Cytogenetically Cryptic Acute Promyelocytic Leukemia: A Diagnostic Challenge. Int J Mol Sci 2023;24(17) (In eng). [CrossRef]
- Campbell LJ, Oei P, Brookwell R, et al. FISH detection of PML-RARA fusion in ins(15;17) acute promyelocytic leukaemia depends on probe size. Biomed Res Int 2013;2013:164501. (In eng). [CrossRef]
- Schultz MJ, Blackburn PR, Cogbill CH, et al. Characterization of a cryptic PML-RARA fusion by mate-pair sequencing in a case of acute promyelocytic leukemia with a normal karyotype and negative RARA FISH studies. Leuk Lymphoma 2020;61(4):975-978. (In eng). [CrossRef]
- Grimwade D, Biondi A, Mozziconacci MJ, et al. Characterization of acute promyelocytic leukemia cases lacking the classic t(15;17): results of the European Working Party. Groupe Francais de Cytogenetique Hematologique, Groupe de Francais d'Hematologie Cellulaire, UK Cancer Cytogenetics Group and BIOMED 1 European Community-Concerted Action "Molecular Cytogenetic Diagnosis in Haematological Malignancies". Blood 2000;96(4):1297-308. (In eng) (https://www.ncbi.nlm.nih.gov/pubmed/10942371).
- Han Y, Xue Y, Zhang J, Pan J, Wu Y, Bai S. Y-chromosome loss as the sole karyotypic anomaly with 3'RARalpha submicroscopic deletion in a case of M3r subtype of acute promyelocytic leukemia. Leuk Res 2009;33(10):1433-5. (In eng). [CrossRef]
- Singh J, Facey A, O'Malley F, Ryland GL, Blombery P, Gregory GP. Cryptic molecular lesion in acute promyelocytic leukemia with negative initial FISH. Leuk Lymphoma 2021;62(12):3060-3062. (In eng). [CrossRef]
Figure 1.
Peripheral Smear Findings. A. Morphologic examination revealed scattered abnormal promyelocytes with variable cytoplasmic granules and occasional Auer rods. B. An abnormal cell population (gray) with high SSC comprising 80% of total events is observed, co-expressing CD13, CD33, CD117 (not shown), CD38, CD123, CD64 and cytoplasmic-MPO, while negative for CD34, HLA-DR, and all other markers tested.
Figure 1.
Peripheral Smear Findings. A. Morphologic examination revealed scattered abnormal promyelocytes with variable cytoplasmic granules and occasional Auer rods. B. An abnormal cell population (gray) with high SSC comprising 80% of total events is observed, co-expressing CD13, CD33, CD117 (not shown), CD38, CD123, CD64 and cytoplasmic-MPO, while negative for CD34, HLA-DR, and all other markers tested.
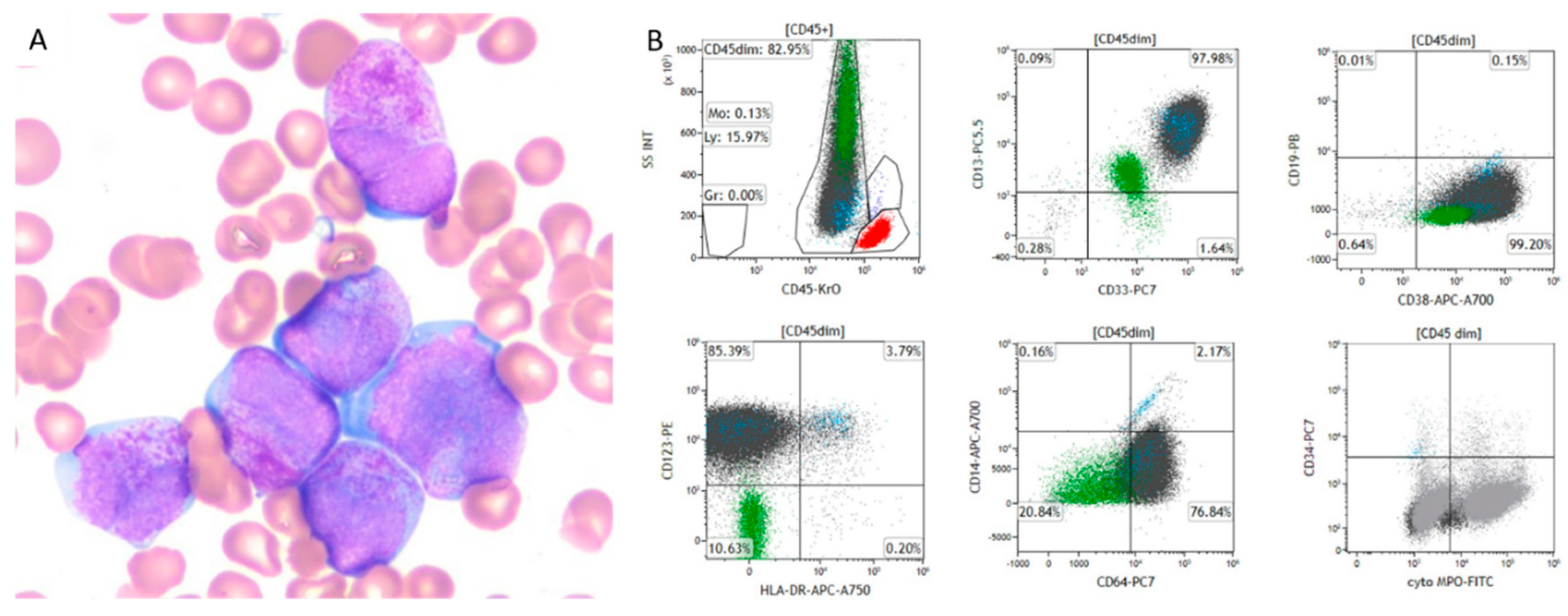
Figure 2.
A. Interphase FISH performed using the Vysis dual color dual fusion t(15;17) probe, showing normal signals for both PML (SpectrumOrange) and RARA (SpectrumGreen). B. Retrospective FISH using the CytoCell PML/RARA dual color dual fusion probe set, which targets smaller regions, revealed a fusion in 74% of interphase cells, suggestive of an insertion of the RARA gene into the PML gene. C. Metaphase FISH also confirmed this cryptic rearrangement.
Figure 2.
A. Interphase FISH performed using the Vysis dual color dual fusion t(15;17) probe, showing normal signals for both PML (SpectrumOrange) and RARA (SpectrumGreen). B. Retrospective FISH using the CytoCell PML/RARA dual color dual fusion probe set, which targets smaller regions, revealed a fusion in 74% of interphase cells, suggestive of an insertion of the RARA gene into the PML gene. C. Metaphase FISH also confirmed this cryptic rearrangement.
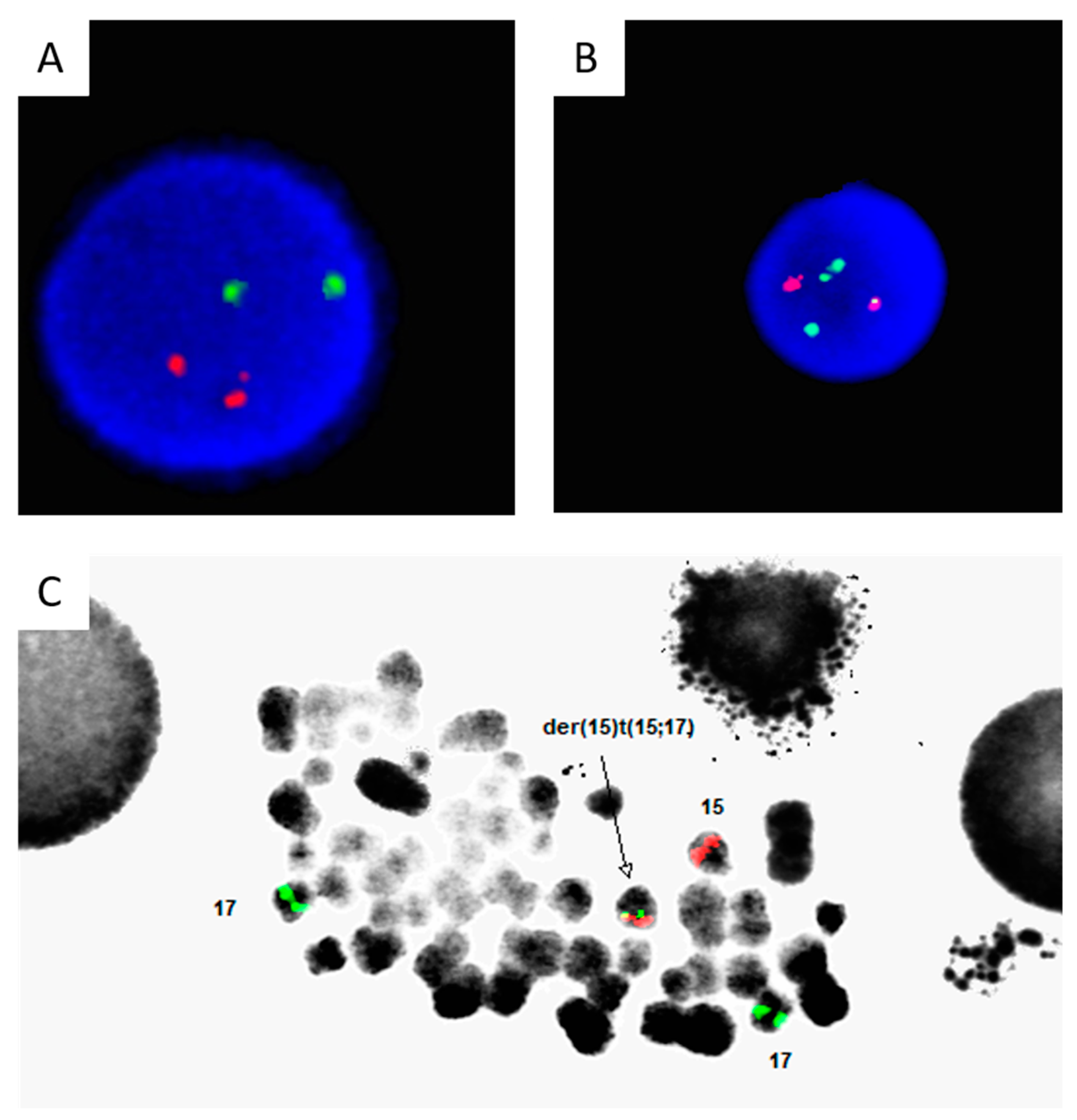
Figure 3.
Optical Genome Mapping Results. A. OGM analysis using the BAS software showed an insertion in the PML gene at breakpoints 73995446 and 74023755 marked in red. B. Further analysis using the VIA software confirmed the insertion in PML at intron 3 (bcr3 region). C. OGM analysis using the BAS software showed the missing alignment of molecules on the RARA gene highlighted using red. D. The low coverage of OGM molecules from exon 1 and 2 and the breakpoint in intron 2 of the RARA gene is highlighted in red, confirm the missing alignment of molecules. E. The possible S-isoform with type A translocation/fusion was constructed based on the available breakpoints and intron 3 involvement on the PML gene.
Figure 3.
Optical Genome Mapping Results. A. OGM analysis using the BAS software showed an insertion in the PML gene at breakpoints 73995446 and 74023755 marked in red. B. Further analysis using the VIA software confirmed the insertion in PML at intron 3 (bcr3 region). C. OGM analysis using the BAS software showed the missing alignment of molecules on the RARA gene highlighted using red. D. The low coverage of OGM molecules from exon 1 and 2 and the breakpoint in intron 2 of the RARA gene is highlighted in red, confirm the missing alignment of molecules. E. The possible S-isoform with type A translocation/fusion was constructed based on the available breakpoints and intron 3 involvement on the PML gene.
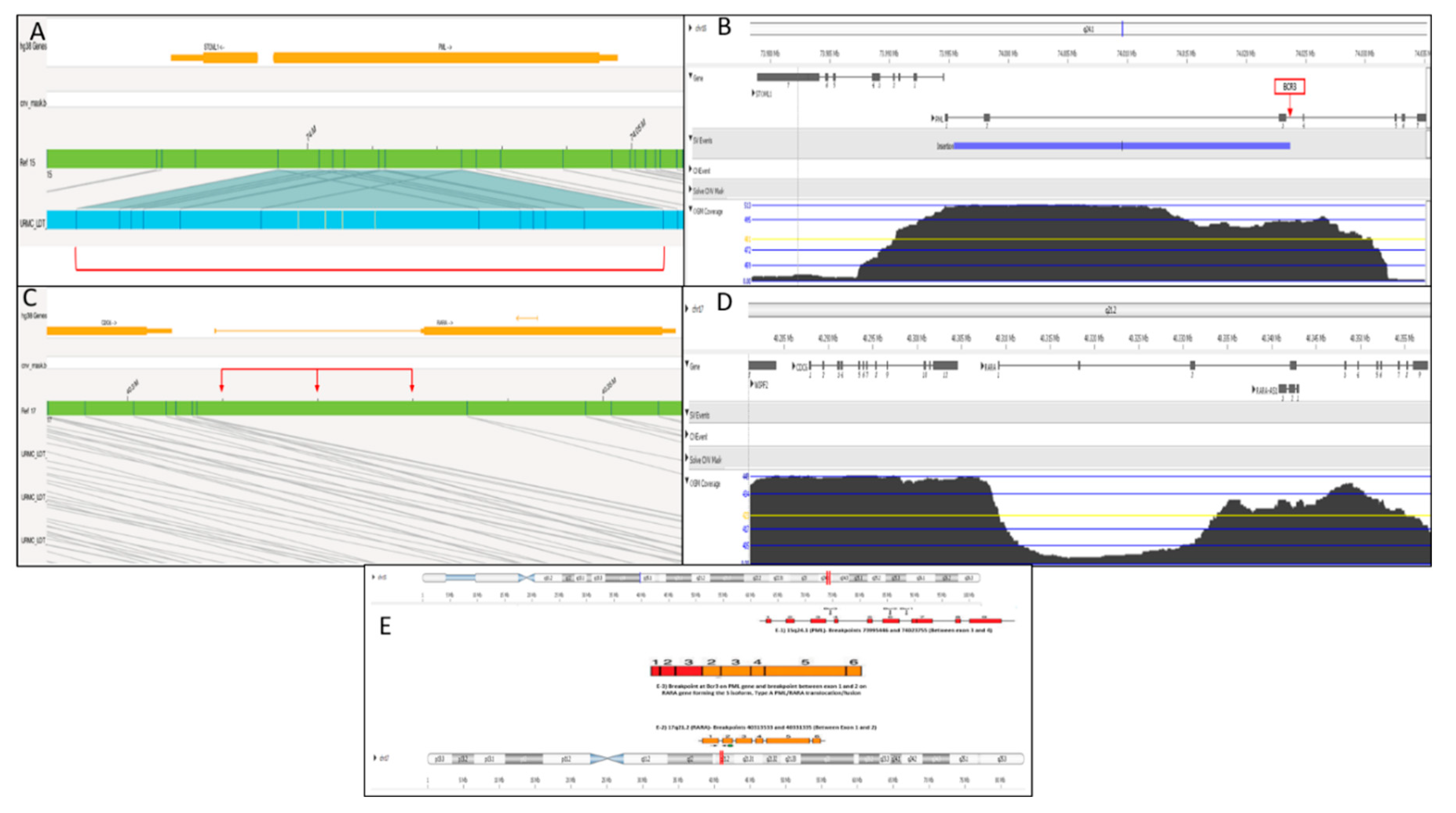

Table 1.
Previously reported single cases of APL with cryptic t(15;17).
| No. | Authors/ PMID |
Age/Sex | Clinical Presentation | Microscopic Findings | Flow Cytometry Expression | Karyotype Findings |
Interphase FISH | Mutational Analysis |
RT-PCR Results |
Confirmatory Testing |
| 1 | Avgerinou et al/ 32909480 |
12/F | Multiple ecchymoses | Leukocytosis Abnormal promyelocytes with bilobed nuclei and cytoplasmic granules Anemia thrombocytopenia |
MPO, CD34 CD123, CD64, CD33, CD117, CD9, HLA-DR and CD2, while negative for other markers | 46, XX | Abbott Molecular LSI PML/RARA dual-color dual-fusion translocation probe: Negative Cytocell (Cambridge, UK) positive for PML::RARA fusion |
FLT3-ITD | bcr3-PML/RARA transcript | Sanger sequencing: in-frame fusion of PML exon 3 and RARA exon 3 |
| 2 | Blanco et al/ 24561214 |
17/M | Gum bleeding, multiple ecchymoses, abdominal pain, and fever | Leukocytosis Abnormal promyelocytes with bilobed nuclei and cytoplasmic granules |
CD117, CD45 (dim), CD13, CD33, CD15 (weak), and CD64 while negative for HLA-DR, CD34, and other markers | 46, XY | Negative | FLT3-ITD | bcr1-PML/RARA transcript | Sequencing: in-frame fusion of PML exon 6 and RARA exon 3 |
| 3 | Burns et al/ 30030569 |
23/F | Epistaxis and easy bruising | Leukocytosis Abnormal myeloblasts/promyelocytes with ovoid nuclei and cytoplasmic granules (rare Auer rods) Anemia thrombocytopenia |
CD13, CD33 (partial), CD56 (partial, dim), CD64, and MPO, while negative for HLA-DR and CD34 | 46, XX,+8 | Abbott Molecular LSI PML/RARA dual-color dual-fusion translocation probe: Negative | Not mentioned | Cryptic PML::RARA fusion | Metaphase FISH: interstitial insertion of PML into the RARA gene |
| 4 | El-Hajj Ghaoui et al/ 29550828 |
8/M | Bruising and bleeding gums | Leukocytosis Blasts and abnormal promyelocytes with large irregularly folded or bi-lobed nuclei and abnormal granulation (rare Auer rods) Anemia thrombocytopenia |
CD13, CD33, CD117, CD123, and CD45, while negative for other markers | 46,XY,der(17)ins(17; 15) (q21;q24q24)?del(17)(p11.2)add(17)(q21) | MetaSystems, Germany dual colour dual fusion PML-RARA probe: single fusion signal and 2 copies of PML and RARA; second expected reciprocal fusion signal not present, and one each of the PML and RARA signals was of diminished intensity | FLT3-ITD | bcr3-PML/RARA transcript and a faint ∼ 350-bp product of unknown origin | Metaphase FISH (using RARA break-apart probe [Abbott Molecular, USA], 15q11.2 control locus [RP11-160D9 from Australasian Genome Research Facility, Melbourne, Australia], subtelomere clones for chromosome 15q [GS-154P1], 17p [cosmid 2111b1], and 17q [PAC GS-362K4], and NF1 within chromosome band 17q11.2): single fusion with diminished RARA signals on the derivative chromosome 17; i.e., der(17) 850K SNP chromosome microarray: no clinically relevant chromosome copy number abnormality across the tumor genome |
| 5 | Fan et al/ 24673420 |
61/F | Fatigue and easy bruising | Leukocytosis Blasts/promyelocytes 40% Anemia thrombocytopenia |
Dim CD45, CD13, CD33,CD117, variable CD34, and lacking HLA-DR | 46, XX, +8 (17/20 cells) | Peripheral blood: variant abnormal signal pattern with 1fusion (1F1O2G) in 52.5% of the nuclei Bone marrow: variant abnormal signal pattern with 1fusion (1F1O2G) in 42% of the nuclei |
Not mentioned | Cryptic PML::RARA fusion without reciprocal RARA-PML fusion transcripts in either the diagnostic or follow-up samples | Metaphase FISH: Non-reciprocaltranslocation with the fusion signal on chromosome 15 and absence of the fusion signal on chromosome 17 Metaphase FISH using whole chromosome paint: RARA(green) signal on chromosome15, without the corresponding PML (orange) signal on chromosome 17, demonstrating an insertion |
| 6 | Mai et al/ 32366568 |
17/M | Seizure (with recent history of nausea, blood-tinged vomiting, lethargy, and right-sided weakness) | Leukocytosis Blasts/promyelocytes 83% Anemia thrombocytopenia |
CD2 (partial), CD4 (partial), CD13, CD33, CD38, CD45, CD64, CD117 (partial), HLA-DR (small subset), and MPO (bright), while negative for other markers | 46, XY | Negative | Not mentioned | Cryptic PML::RARA fusion | Not performed |
| 7 | Zhang et al/ 31959056 |
66/M | Petechiae and bruises | Leukopenia Blasts/promyelocytes 68% (irregular nuclear shapes, misty nucleoli) Anemia thrombocytopenia |
CD34, CD7, CD13, CD33, CD117, CD38, HLA-DR and MPO, while negative for other markers | 46, XY | Negative | Biallelic CEBPA mutation | bcr2-PML/RARA transcript (nested RT-PCR) | Not performed |
| 8 | Gu et al/ 33052080 |
62/M | Pharyngalgia, fatigue, and gum bleeding | Anemia Leukopenia Hypercellular bone marrow with abnormal promyelocytes |
CD117, CD33, myeloperoxidase (MPO), CD13, CD58, CD38, and CD81 | 46,XY, add(11) (p15), and ?t(13;20)(q12;q11.2) |
Atypical PML::RARA fusion signal in 91% of nuclei | FLT3, WT1, and KRAS mutations | Major PML/RARα transcript harbored the three type breakpoints | Not performed |
| 9 | Kim et al/ 21156244 |
18/M | Hematuria and hematochezia | Leukocytosis Blasts/promyelocytes 84% Anemia thrombocytopenia |
CD13, CD33, CD45, and CD117 and negative for HLA-DR and CD34 | 46,XY | Negative | Not mentioned | Three PML::RARA fusion transcripts: bcr2, bcr1, and novel transcript (exon 4 of PML and exon 3 of RARA) | Long-distance DNA-PCR: rearrangement between PML (intron 6) and RARA (intron 2) |
| 10 | Goldschmidt et al/ 20863428 |
52/F | Bleeding tendency | Anemia Leukopenia Thrombocytopenia |
Strongly positive for CD33 and CD13 while negative for HLA-DR | 47,XX,zi(5)(p10)[20]/48,idem,z9[2]/46,XX[6] | Negative | Not mentioned | Bcr1-PML/RARa transcript | Metaphase FISH: interstitial insertion of RARa gene into PML gene (low signal retrospectively identified on interphase FISH) |
| 11 | Koshy et al/ 22982005 |
29/M |
Progressive fatigue Bruises |
Pancytopenia 26% abnormal promyelocytes |
Positive for CD117, CD33, and CD13 but negative for HLA-DR and CD34 | 46,XY | Negative with a small PML signal present on another chromosome (20% of cells) | Not mentioned | Positive for PML::RARA transcript | Sanger sequencing across the PML-RARA breakpoint demonstrated a BCR1-type fusion. Whole genome SNP microarray: intragenic duplication of PML on chromosome 15q24.1 (30% of cells). |
| 12 | Karlin et al/ 35572917 |
54/M |
DVT |
Pancytopenia 77% abnormal promyelocytes in the BM |
Positive for MPO and CD117 while negative for CD34 and HLA-DR | 46,XY | Negative | FLT3 p.D835Y variant | Bcr1-PML/RARA transcript | Not performed |
| 13 | Mahmud et al/ 32924730 |
68/F |
Dizziness Fatigue Acute on chronic PE |
Pancytopenia 70% abnormal promyelocytes/blasts |
Not mentioned | 46, XX | Two copies of chromosome 15, but absence of the reciprocal translocation on the two copies of chromosome 17 | Not mentioned | Positive for bcr3-PML::RARA transcript | Metaphase FISH: insertion of a RARA segment into chromosome 15 at the location of PML. Whole-genome sequencing: complex t(15;17) with a possible intrachromosomal rearrangement of chromosome 15. |
| 14 | Schultz et al/ 31809670 |
57/F |
Bruising Gingival bleeding |
Anemia Neutropenia Thrombocytopenia Abnormal promyelocytes/blasts |
Positive for CD13, CD33, CD34 (partial), CD117, MPO, and aberrant partial CD2 expression | 46, XX | Negative | Not mentioned | PML-RARA fusion in 53% of cells | Mate-pair sequencing: cryptic insertional translocation resulting in PML-RARA fusion with breakpoints located within intron 6 of PML and intron 2 of RARA. |
| 15 | Shepshelovich et al/ 26471811 |
53/F | Not mentioned | Not mentioned | Not mentioned | 46XX, iso(17)(q11) | Using the Cytocell probe: negative |
Not mentioned | Major PML−RARA transcript harbored the BCR-1 breakpoint. BCR-2 and BCR-3 were demonstrated as spliced variants. | FISH using the Vysis probe: several clones detected |
| 16 | Tang et al/ 26823883 |
21/M |
Melena Bleeding tendency |
Not mentioned | Not mentioned | Complex karyotype with isochromosome 17q | Two PML/RARA fusion signals | Not mentioned | Not mentioned | Not performed |
| 17 | Venci et al/ 28599418 |
73/F | Diagnosed incidentally (pre-operatively) | Anemia Thrombocytopenia Abnormal promyelocytes/blasts |
Positive for CD13, CD33, MPO, CD2 and CD9, while negative for other markers | 46,XX | Two fusion signals on the two copies of chromosome 15, but absence of the reciprocal on the two copies of chromosome 17 | Not mentioned | Bcr3/short form PML-RARA fusion transcript | Metaphase FISH: two PML/RARA fusion signals (one on each copy of chromosome 15, and two normal RARA signals on the two copies of chromosome 17), raising the possibility of uniparental isodisomy. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



