Submitted:
10 November 2024
Posted:
11 November 2024
You are already at the latest version
Abstract
The interplay between metabolic dysfunction-associated steatotic liver disease (MASLD) and heart failure (HF) reveals a significant and complex relationship marked by shared metabolic, inflammatory, and fibrotic pathways. This review explores their combined epidemiology, pathophysiology, and clinical implications, emphasizing the need for integrative management approaches. MASLD, which encompasses a range of liver conditions from benign steatosis to advanced fibrosis and hepatocellular carcinoma, is tightly linked with metabolic syndrome, while HF represents the culmination of systemic and cardiovascular stresses often exacerbated by comorbid conditions like diabetes and hypertension. Their mutual pathophysiology involves disruptions in lipid metabolism, systemic inflammation, insulin resistance, and fibrosis, with MASLD-associated inflammatory markers accelerating HF progression and vice versa. Epidemiological studies underscore MASLD’s association with elevated cardiovascular risk, particularly HF, which persists even after adjusting for traditional risk factors. This narrative review underscores the urgent need for early diagnosis, risk factor management, and novel therapeutic targets to mitigate the escalating burden of MASLD and HF on global health, especially within aging populations increasingly affected by metabolic disorders.
Keywords:
NAFLD
; fluid retention
; Ejection Fraction
; inflammation
Background
Metabolic dysfunction-associated steatotic liver disease (MASLD), previously known as non-alcoholic fatty liver disease (NAFLD), is a global public health concern, characterized by the accumulation of excess fat in the liver[1]. MASLD includes a range of conditions, from simple steatosis to more severe metabolic dysfunction-associated steatohepatitis (MASH), which can lead to fibrosis, cirrhosis, and hepatocellular carcinoma[2,3]. The disease is strongly associated with metabolic risk factors, such as obesity, type 2 diabetes mellitus, dyslipidemia, and hypertension, and is considered a hepatic manifestation of metabolic syndrome[4].
Heart failure (HF) is a prevalent, multifaceted syndrome whose epidemiology and pathophysiology reflect a broad interplay of cardiovascular, metabolic, and systemic factors[5,6]. As HF rates rise globally, especially within aging and metabolically challenged populations[5,7], understanding these underlying mechanisms is essential for developing effective, targeted therapies that can mitigate disease progression and reduce the substantial healthcare burden of HF.
This manuscript briefly reviews the MASLD and HF interplay, their combined pathophysiology, and their clinical aspects.
Metabolic Dysfunction-Associated Steatotic Liver Disease
The prevalence of MASLD has increased dramatically over recent decades. Currently, MASLD affects about 38% of the global adult population[8], with particularly high rates in North America, South America, the Middle East, and parts of Asia[8,9,10]. This rise reflects the increasing prevalence of obesity and metabolic syndrome in these regions[10]. For instance, the United States is projected to see over 100 million cases of MASLD by 2030, driven largely by lifestyle factors such as high-calorie diets and sedentary behavior[11].
Epidemiological studies highlight a particularly concerning trend. MASLD and MASH are no longer diseases primarily affecting middle-aged and older adults [8,12,13]. Increasing rates are now reported in adolescents and young adults, likely due to early onset of obesity and metabolic syndrome, which can lead to liver disease progression at a younger age[14]. With a global prevalence of 7-14% in epidemiological studies in adolescents and young adults, in the U.S., it is estimated that about 5.8% of children and adolescents have MASLD[8,14], underscoring the urgent need for preventive measures across all age groups.
Risk factors such as obesity and diabetes mellitus not only increase MASLD risk but also drive its progression to MASH[15]. MASH has been found in 63% of patients with MASLD undergoing liver biopsy in an Asian multi-center study, which is more likely to lead to advanced fibrosis and other severe liver complications[4]. The presence of MASH was not associated with a higher incidence of atherosclerotic cardiovascular events, although a trend was apparent[16]. However, another study showed that among those with MASH, the prevalence of cardiovascular diseases, including heart failure, coronary artery disease, and stroke, is markedly higher compared to those without liver disease or with less severe forms of MASLD[17]. This interrelationship complicates disease management, as patients with both MASLD/MASH and cardiovascular disease (CVD) require a more intensive and nuanced approach to managing metabolic and liver health.
Ethnic and racial disparities further complicate the MASLD epidemiology[18]. Hispanic individuals, for example, have disproportionately higher MASLD rates, partly due to genetic predispositions that affect fat metabolism in the liver[19]. Meanwhile, African American populations show relatively lower MASLD prevalence but may present with more advanced fibrosis at diagnosis[20,21]. This variability underscores the need for tailored diagnostic and treatment approaches based on demographic factors.
Screening and diagnosing MASLD, particularly MASH, present challenges due to the disease’s asymptomatic nature in early stages. Imaging techniques, like ultrasound and elastography, are frequently used, yet liver biopsy remains the gold standard for MASH diagnosis, especially to assess fibrosis stages [22,23,24]. However, biopsy is invasive and costly, limiting its feasibility for large-scale screening. As a result, MASLD often remains undiagnosed until complications arise, highlighting a need for accessible and non-invasive diagnostic alternatives[24].
MASLD’s epidemiology reflects complex interactions among metabolic, genetic, and lifestyle factors, resulting in a high prevalence and substantial health burden. With MASLD projected to rise further due to global trends in obesity and metabolic syndrome, a comprehensive approach—including public health initiatives targeting lifestyle factors and improved screening methods—is essential to manage and mitigate this growing epidemic[8,25,26].
Heart Failure
HF is a complex clinical syndrome marked by the heart’s inability to pump blood effectively to meet the body’s needs, either due to weakened heart muscles (systolic dysfunction) or stiffened ventricles (diastolic dysfunction)[27,28]. HF represents the final stage of numerous cardiovascular diseases and is often categorized by the ejection fraction (EF) metric, which assesses the percentage of blood the left ventricle pumps out with each contraction[29]. Based on EF, HF can be classified as heart failure with reduced ejection fraction (HFrEF), preserved ejection fraction (HFpEF), or mildly reduced ejection fraction (HFmrEF)[29,30].
The global prevalence of HF is significant, affecting over 64 million people worldwide, with rates steadily increasing due to aging populations, better survival from other cardiovascular conditions, and rising levels of risk factors like hypertension, diabetes mellitus, and obesity[31,32]. In the United States alone, over 6 million adults are affected, and this number is projected to increase substantially over the coming decades[33,34]. Epidemiologically, HF is most common in individuals over 65 years of age[35,36], with men generally experiencing a higher incidence of HFrEF[37], and women more commonly affected by HFpEF, especially among those with diabetes mellitus or hypertension[35,38,39].
The incidence of HF varies widely by geography, socioeconomic factors, and ethnicity, with higher prevalence noted in African American and Hispanic populations. This discrepancy is likely due to a combination of genetic predispositions and greater prevalence of risk factors, including hypertension and metabolic syndrome[5,40]. Racial and ethnic disparities in healthcare access and quality further contribute to the increased HF burden within these populations[5]. Similarly, HF is a leading cause of hospitalization and readmission in older adults, posing a significant burden on healthcare systems worldwide[41,42]. In the U.S., HF accounts for over 1 million hospitalizations annually, with costs estimated to reach $70 billion by 2030, underscoring the pressing need for effective prevention and management strategies[33].
The pathophysiology of HF involves complex interactions among myocardial injury, neurohormonal activation, and systemic inflammation[27,43]. These processes vary depending on HF subtype but commonly result in a progressive decline in cardiac function. In HFrEF, myocardial infarction, chronic ischemic damage, or dilated cardiomyopathy often causes weakening of the heart muscle, impairing its ability to contract forcefully. This leads to reduced cardiac output, which activates compensatory mechanisms like the renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system. Although initially beneficial, chronic neurohormonal activation promotes fluid retention, vasoconstriction, and further cardiac remodeling, ultimately exacerbating HF[44,45].
HFpEF, on the other hand, is primarily associated with impaired ventricular relaxation rather than contractile function, often resulting from stiffening of the myocardium due to conditions like hypertension, left ventricular hypertrophy, or metabolic comorbidities such as obesity and diabetes mellitus. This leads to increased diastolic pressures and difficulty in filling the left ventricle during diastole, causing symptoms despite a preserved EF. Chronic systemic inflammation is a key feature in HFpEF pathophysiology, often driven by comorbidities, which in turn contribute to vascular stiffness, microvascular dysfunction, and myocardial fibrosis[46,47,48].
Emerging research highlights metabolic and inflammatory pathways as significant contributors to HF, especially HFpEF[49]. These mechanisms are increasingly relevant given the high prevalence of metabolic conditions such as MASLD among HF patients. The relationship between HF and comorbidities like MASLD points to the importance of a comprehensive, multi-system approach to HF management, addressing not only cardiovascular health but also metabolic and inflammatory conditions that influence HF progression[16,50,51].
Metabolic Dysfunction-Associated Steatotic Liver Disease and Heart Failure Pathophysiology
The pathophysiological link between HF and MASLD centers on shared metabolic, inflammatory, and fibrotic pathways that intensify both conditions[51]. Central to this link is the role of metabolic syndrome and chronic low-grade inflammation, both of which foster cardiovascular and hepatic complications through cellular and molecular mechanisms that reinforce disease progression[52,53]. As MASLD often coexists with metabolic risk factors such as insulin resistance, dyslipidemia, and hypertension, it predisposes patients to increased cardiovascular strain, contributing directly to HF development and worsening its prognosis [50,54,55].
At the cellular level, HF and MASLD share disruptions in lipid metabolism that lead to toxic lipid accumulation and lipotoxicity in both cardiac and hepatic tissues[51,56]. Shin et al. [57], Svobodová et al. [58], and Zhao et al. [59] emphasize that in MASLD, hepatic steatosis results in the buildup of free fatty acids (FFAs) and toxic lipid intermediates, which impair mitochondrial function and induce oxidative stress. These alterations stimulate reactive oxygen species (ROS) production and subsequent inflammatory cytokine release, particularly interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), creating a chronic inflammatory state[60]. Similarly, in HF, lipotoxicity impairs cardiomyocyte function, leading to mitochondrial dysfunction and oxidative stress that weaken cardiac output[61,62]. This shared pathway of lipotoxicity exacerbates both hepatic and myocardial injury, establishing a cyclical progression where HF promotes MASLD and vice versa.
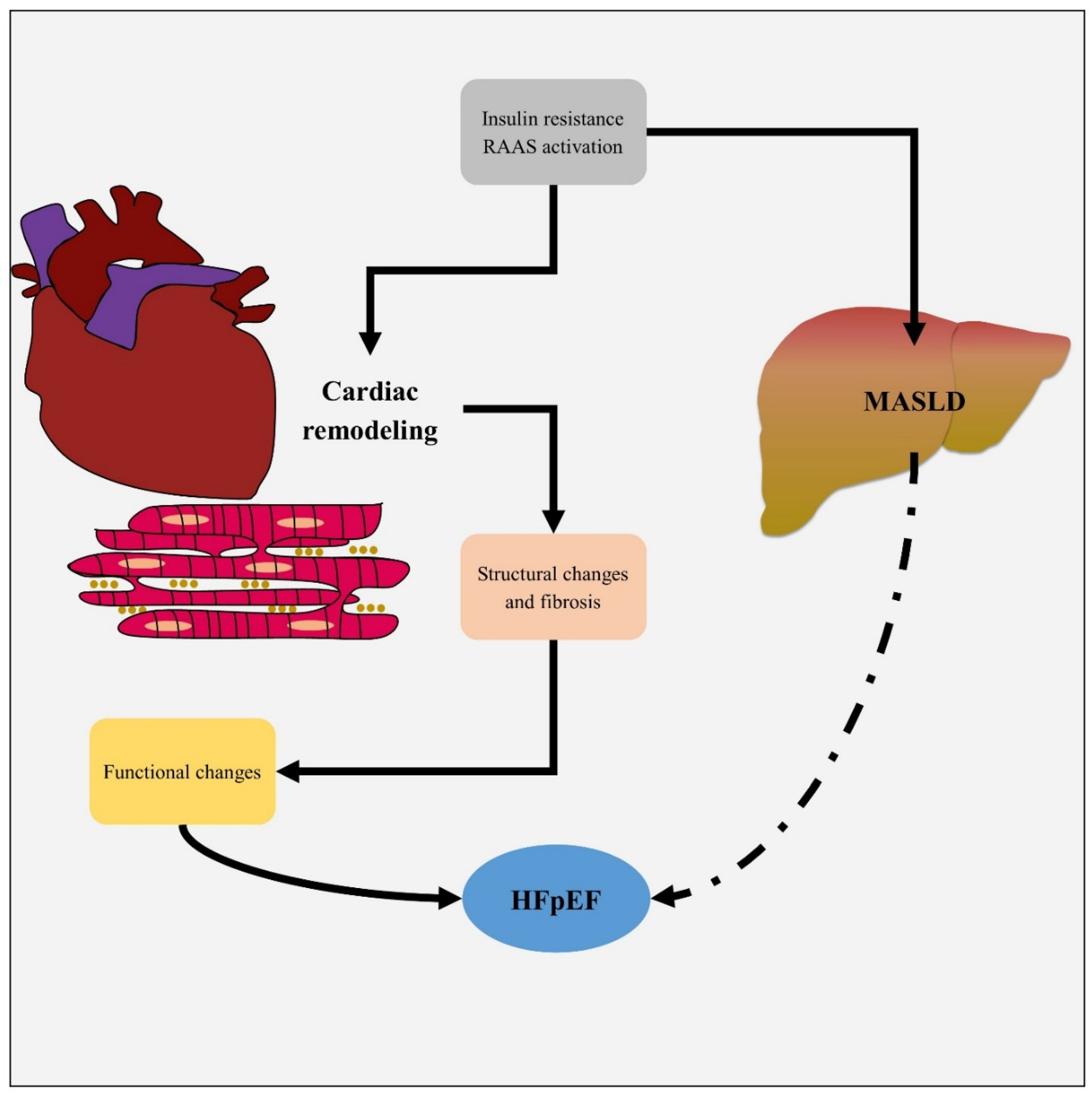
Molecular signaling pathways involved in insulin resistance also play a significant role in linking MASLD to HF[16,56]. Insulin resistance, frequently observed in MASLD, reduces glucose uptake and promotes FFA mobilization, contributing to lipid overload in the liver and heart[63]. It had been reported that impaired insulin signaling enhances the activation of the RAAS and sympathetic nervous system, further elevating blood pressure and cardiac workload, which are deleterious in HF[64,65]. This continuous RAAS activation contributes to vasoconstriction, sodium retention, and cardiac remodeling, worsening HF while simultaneously promoting MASLD progression through vascular and systemic inflammatory pathways (Figure 1) [66,67,68].
Fibrosis is a critical aspect of both MASLD and HF pathophysiology, with the progression of fibrosis in one organ often influencing the other. In the liver, Kupffer cells and hepatic stellate cells respond to inflammatory signals by producing collagen and extracellular matrix proteins, leading to liver fibrosis[69]. This fibrotic process is paralleled in HF, where inflammatory cell infiltration and fibroblast activation lead to cardiac fibrosis[70,71]. Over time, this fibrosis impairs the structural integrity and function of both organs, with liver stiffness often correlating with reduced cardiac output in HF patients[72,73]. Notably, patients with advanced MASLD and fibrosis show a 1.5-fold increase in HF risk, underscoring the impact of fibrosis in linking these two conditions[74,75].
Chronic systemic inflammation bridges MASLD and HF[76,77], as myocardial injury accelerates the progression of MASH by triggering immunoinflammatory response [78]. Van Wagner et al. demonstrate that cytokines such as IL-1β and TNF-α, released from the liver in MASLD, contribute to endothelial dysfunction and increased vascular permeability, worsening cardiac hemodynamics[79,80]. The persistence of this inflammatory state exacerbates HF pathogenesis, driving adverse cardiac remodeling and fibrosis. This mutual inflammatory feedback between MASLD and HF presents a major challenge, as it perpetuates a cycle of systemic inflammation and tissue damage across both organs.
Therefore, the shared pathophysiology of HF and MASLD involves overlapping mechanisms of lipotoxicity, insulin resistance, fibrosis, systemic inflammation, and mitochondrial dysfunction. The interdependent cellular and molecular interactions between these pathways foster disease progression in both organs, highlighting the need for a comprehensive approach to manage HF in patients with MASLD. Addressing these common mechanisms offers potential for novel therapeutic targets that could mitigate the progression of both HF and MASLD, improving outcomes for this high-risk population.
Metabolic Dysfunction-Associated Steatotic Liver Disease and Heart Failure Association
The connection between liver diseases and heart failure is widely recognized. Heart failure can result in congestive hepatopathy, while severe liver disease can lead to cirrhotic cardiomyopathy. Recent studies, however, suggest a link between heart failure and early-stage liver conditions, such as noncirrhotic MASLD. Additionally, growing evidence indicates a possible association between MASLD and heart failure with preserved ejection fraction[16].
The association between MASLD and cardiovascular diseases, particularly heart failure, reveals a complex interplay that suggests a risk amplified by shared risk factors such as type 2 diabetes mellitus, hypertension, and obesity[16,50,51]. Studies demonstrate that MASLD, especially in its severe form known as MASH, increases CVD prevalence and mortality compared to other liver diseases and general populations, although some findings vary based on sample characteristics, cardiovascular endpoints, and confounding factors[17,81].
It is likely that cardiometabolic risk factors play a greater role in the development of CVD than MASH, which could explain the similar risks of CV events found in many of these studies, especially those comparing populations with MASH vs. MASLD[81] while other study showed that MASH was associated with a higher prevalence of coronary artery disease (CAD)[81]. However, one analysis showed a heightened prevalence of CAD in MASH patients undergoing liver transplantation compared to those with hepatitis C or alcoholic cirrhosis, with CAD present in 52.8% of MASH cases versus 20.0% in alcoholic cirrhosis patients[82]. The risk for three-vessel disease in MASH patients was also significantly greater, suggesting an advanced atherosclerotic burden within this population. Odds ratios for significant CAD in MASH patients undergoing transplant evaluations reached 3.12 (95% CI: 1.33–5.32), underscoring an elevated cardiovascular risk that may necessitate more aggressive intervention strategies[81].
In a robust study, Simon et al. [83] used liver biopsy as a gold standard, matching 10,422 MASLD patients with 46,517 controls. They found MASLD significantly linked to heart failure, with a hazard ratio (HR) of 1.75 (95% CI: 1.63, 1.87). This risk rose with liver disease severity, independent of common cardiometabolic factors.
Several studies underscore a disproportionately high incidence of CVD-related comorbidities in MASLD and MASH populations. In one study, the baseline prevalence of CVD among liver transplant patients with MASH reached 37.7%, significantly exceeding the 17.0% observed in non-MASH cases (p < 0.001). Similarly, hypertension and diabetes mellitus were markedly higher in MASH cohorts, with nearly two-thirds of patients meeting obesity criteria, emphasizing the metabolic overlap that likely fuels cardiovascular risk escalation. In contrast, non-MASH liver transplant patients demonstrated only a 30% prevalence of diabetes mellitus and a 15.6% rate of hypertension, underscoring the metabolic syndrome’s intensification in MASH cases[81,84].
Heart failure emerges as a particularly concerning outcome among patients with MASLD, as this cohort consistently experiences an elevated risk for heart failure independent of traditional cardiovascular risks. MASLD patients are estimated to face a 1.5-fold greater likelihood of developing heart failure compared to non-MASLD populations, and this association persists even after adjusting for diabetes mellitus, hypertension, and obesity, suggesting an intrinsic risk element within MASLD pathology[17,74,75]. Importantly, data also reveal that liver disease severity correlates with heart failure risks, with individuals experiencing advanced fibrosis or cirrhosis exhibiting higher incidences of HFpEF, a common and challenging heart failure subtype associated with MASLD[51].
A retrospective cohort study on 98,685 participants showed that participants with MASLD had an increased risk of HF compared with non-MASLD individuals (HR: 1.40, 95% CI: 1.30–1.50)[85].
Nonetheless, conflicting results exist concerning cardiovascular outcomes in MASLD patients post-transplant. For instance, in one cohort study of liver transplant recipients, cardiovascular event rates did not significantly differ between patients with MASH versus those with alcoholic cirrhosis within one year post-transplant. Despite MASH patients’ higher comorbidity rates, the cardiovascular event incidence remained relatively balanced, possibly due to the pre-transplant cardiovascular evaluation processes that select only patients with manageable cardiac conditions. These findings suggest that MASLD’s cardiovascular impact may be moderated in clinical settings where risk is carefully managed, though it does not eliminate MASLD’s intrinsic association with cardiovascular deterioration[81].
Examining mortality outcomes also yields nuanced insights into MASLD’s cardiovascular impacts. In studies comparing MASH to other etiologies, one-year mortality due to cardiovascular complications was higher in MASH than in hepatitis C virus (HCV) and alcohol-related cirrhosis cases, with hazard ratios of 1.30 and 1.34, respectively. Cardiovascular deaths were significantly more common within the MASH group, often concentrated within the first months post-transplant, possibly reflecting MASH’s pronounced cardiovascular burden even amid other high-risk liver conditions[81,86].
Interestingly, despite MASLD’s established cardiovascular associations, some studies suggest a protective element in specific contexts. In a cohort comparing MASLD versus HCV-positive and HCV-negative groups, MASLD patients had a lower cardiovascular mortality rate (HR 0.65) than HCV-positive individuals. This inverse association’s etiology is unclear, although it may involve differences in systemic inflammatory profiles or complications unique to HCV. Additionally, MASLD patients’ cardiovascular event prevalence varies by demographic factors, such as age and sex, further complicating an overarching assessment of MASLD’s cardiac outcomes[81].
Conclusion
In conclusion, MASLD, especially in its MASH form, poses a substantial cardiovascular risk, accentuating the prevalence of heart failure and ischemic conditions. However, the presence of comorbidities like diabetes mellitus and obesity often obscures whether MASLD itself directly escalates cardiovascular risks or serves as a proxy marker for metabolic dysfunction. The disproportionate occurrence of heart failure among MASLD patients suggests an independent risk element, though clinical outcomes often depend on broader metabolic health and disease severity. For patients with advanced liver involvement, aggressive management of cardiometabolic factors may mitigate MASLD’s cardiovascular impacts, supporting preventive strategies to reduce mortality.
Authors’ Contributions
MS: Reviewing the literature, Methodology, Investigation, Conceptualization, Data curation, Formal analysis, Writing – the original draft, review & and editing, Designing the Figure.
Funding
None
Acknowledgments
Special thanks to Dr. Seyed-Mohamad-Sadegh Mirahmadi and Dr. Reza Azarbad.
Conflict of Interest
The author declare that they have no conflict of interest.
References
- Lekakis V, Papatheodoridis GV. Natural history of metabolic dysfunction-associated steatotic liver disease. European Journal of Internal Medicine 2024, 122, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Corrao S, Calvo L, Granà W, Scibetta S, Mirarchi L, Amodeo S, et al. Metabolic dysfunction-associated steatotic liver disease: A pathophysiology and clinical framework to face the present and the future. Nutrition, Metabolism and Cardiovascular Diseases 2024.
- El-Kassas M, Othman HA, Elbadry M, Alswat K, Yilmaz Y. Risk Stratification of Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease: Steatohepatitis, Fibrosis, and Hepatocellular Carcinoma. Journal of Clinical and Experimental Hepatology 2024, 102415.
- Chan W-K, Chuah K-H, Rajaram RB, Lim L-L, Ratnasingam J, Vethakkan SR. Metabolic dysfunction-associated steatotic liver disease (MASLD): a state-of-the-art review. Journal of Obesity & Metabolic Syndrome 2023, 32, 197. [Google Scholar]
- Khan MS, Shahid I, Bennis A, Rakisheva A, Metra M, Butler J. Global epidemiology of heart failure. Global epidemiology of heart failure. Nature Reviews Cardiology. 2024, 1–18. [Google Scholar]
- Doehner W, Frenneaux M, Anker SD. Metabolic impairment in heart failure: the myocardial and systemic perspective. Journal of the American College of Cardiology 2014, 64, 1388–1400. [Google Scholar] [CrossRef]
- Liu Z, Li Z, Li X, Yan Y, Liu J, Wang J, et al. Global trends in heart failure from 1990 to 2019, An age-period-cohort analysis from the Global Burden of Disease study. ESC Heart Failure. 2024.
- Younossi ZM, Kalligeros M, Henry L. Epidemiology of Metabolic Dysfunction Associated Steatotic Liver Disease. Clinical and Molecular Hepatology 2024. [Google Scholar]
- Younossi ZM, Golabi P, Paik J, Owrangi S, Yilmaz Y, El-Kassas M, et al. Prevalence of metabolic dysfunction-associated steatotic liver disease in the Middle East and North Africa. Liver International 2024, 44, 1061–1070. [Google Scholar] [CrossRef]
- Miao L, Targher G, Byrne CD, Cao Y-Y, Zheng M-H. Current status and future trends of the global burden of MASLD. Trends in Endocrinology & Metabolism 2024.
- Manikat R, Ahmed A, Kim D. Current epidemiology of chronic liver disease. Gastroenterology Report 2024, 12, goae069. [Google Scholar]
- He Q-J, Li Y-F, Zhao L-T, Lin C-T, Yu C-Y, Wang D. Recent advances in age-related metabolic dysfunction-associated steatotic liver disease. World Journal of Gastroenterology 2024, 30, 652. [Google Scholar] [CrossRef] [PubMed]
- Kim Y, Charlton M, Rezvani G, Saal GB. S1826 Prevalence of Metabolic-Associated Steatohepatitis (MASH) and Advanced Fibrosis in At-Risk Pediatric Populations. Official journal of the American College of Gastroenterology| ACG 2024, 119, S1316–S7.
- Shen T-H, Wu C-H, Lee Y-W, Chang C-C. Prevalence, trends, and characteristics of metabolic dysfunction-associated steatotic liver disease among the US population aged 12–79 years. European Journal of Gastroenterology & Hepatology 2024, 36, 636–645. [Google Scholar]
- Gancheva S, Roden M, Castera L. Diabetes as a risk factor for MASH progression. Diabetes Research and Clinical Practice 2024, 111846. [Google Scholar]
- Driessen S, Francque SM, Anker SD, Cabezas MC, Grobbee DE, Tushuizen ME, et al. Metabolic dysfunction associated steatotic liver disease and the heart. Hepatology 2023, 10, 1097. [Google Scholar]
- Targher G, Byrne CD, Tilg H. MASLD: a systemic metabolic disorder with cardiovascular and malignant complications. Gut 2024, 73, 691–702. [Google Scholar]
- Gulati R, Moylan CA, Wilder J, Wegermann K. Racial and ethnic disparities in metabolic dysfunction-associated steatotic liver disease. Metabolism and Target Organ Damage 2024, 4, N/A–N/A. [Google Scholar]
- Kardashian A, Serper M, Terrault N, Nephew LD. Health disparities in chronic liver disease. Hepatology 2023, 77, 1382–1403. [Google Scholar] [CrossRef]
- Díaz LA, Lazarus JV, Fuentes-López E, Idalsoaga F, Ayares G, Desaleng H, et al. Disparities in steatosis prevalence in the United States by Race or Ethnicity according to the 2023 criteria. Communications Medicine 2024, 4, 219. [Google Scholar] [CrossRef]
- Saini A, Rutledge B, Damughatla AR, Rasheed M, Naylor P, Mutchnick M. Manifestation and Progression of Metabolic Dysfunction-Associated Steatotic Liver Disease in a Predominately African American Population at a Multi-Specialty Healthcare Organization. Healthcare 2024, 1478.
- Sotoudeheian, M. Galectin-3 and Severity of Liver Fibrosis in Metabolic Dysfunction-Associated Fatty Liver Disease. Protein and Peptide Letters 2024, 31, 290–304. [Google Scholar] [CrossRef] [PubMed]
- Mokhtare M, Abdi A, Sadeghian AM, Sotoudeheian M, Namazi A, Sikaroudi MK. Investigation about the correlation between the severity of metabolic-associated fatty liver disease and adherence to the Mediterranean diet. Clinical Nutrition ESPEN 2023, 58, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Mohammadjavad, S. Agile 3+ and Metabolic Dysfunction-Associated Fatty Liver Disease: Detecting Advanced Fibrosis based on Reported Liver Stiffness Measurement in FibroScan and Laboratory Findings. The International Journal of Gastroenterology and Hepatology Diseases 2024, 3, 43–54. [Google Scholar]
- Lee EC, Anand VV, Razavi AC, Alebna PL, Muthiah MD, Siddiqui MS, et al. The global epidemic of metabolic fatty liver disease. Current Cardiology Reports 2024, 26, 199–210. [Google Scholar] [CrossRef] [PubMed]
- El-Kassas M, Awad A, Elbadry M, Arab JP. Tailored Model of Care for Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease. Seminars in Liver Disease: Thieme Medical Publishers, Inc.; 2024.
- Sotoudeheian M, Hoseini S. Understanding the Pathophysiology of Heart Failure with Mid-Range Ejection Fraction: A Comprehensive Narrative Review. 2023.
- Sotoudeheian MJ, Mirahmadi S-M-S, Pirhayati M, Azarbad R, Nematollahi S, Taghizadeh M, et al. Understanding the Role of Galectin-1 in Heart Failure: A Comprehensive Narrative Review. Current Cardiology Reviews 2024, 20, 82–90. [Google Scholar]
- Murphy SP, Ibrahim NE, Januzzi JL. Heart failure with reduced ejection fraction: a review. Jama 2020, 324, 488–504. [Google Scholar] [CrossRef]
- Severino P, Maestrini V, Mariani MV, Birtolo LI, Scarpati R, Mancone M, et al. Structural and myocardial dysfunction in heart failure beyond ejection fraction. Heart failure reviews 2020, 25, 9–17. [Google Scholar] [CrossRef]
- Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GM, Coats AJ. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovascular research 2022, 118, 3272–3287. [Google Scholar]
- Triposkiadis F, Xanthopoulos A, Parissis J, Butler J, Farmakis D. Pathogenesis of chronic heart failure: cardiovascular aging, risk factors, comorbidities, and disease modifiers. Heart failure reviews 2022, 27, 337–344. [Google Scholar] [CrossRef]
- Heidenreich PA, Fonarow GC, Opsha Y, Sandhu AT, Sweitzer NK, Warraich HJ, et al. Economic issues in heart failure in the United States. Journal of cardiac failure 2022, 28, 453–466. [Google Scholar] [CrossRef]
- Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nature Reviews Cardiology 2016, 13, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure. European journal of heart failure 2020, 22, 1342–1356. [Google Scholar] [CrossRef] [PubMed]
- Dharmarajan K, Rich MW. Epidemiology, pathophysiology, and prognosis of heart failure in older adults. Heart failure clinics 2017, 13, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nature Reviews Cardiology 2017, 14, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Shi K, Yang M-X, Huang S, Yan W-F, Qian W-L, Li Y, et al. Effect of diabetes mellitus on the development of left ventricular contractile dysfunction in women with heart failure and preserved ejection fraction. Cardiovascular diabetology 2021, 20, 1–10. [Google Scholar]
- Tadic M, Cuspidi C, Plein S, Belyavskiy E, Heinzel F, Galderisi M. Sex and heart failure with preserved ejection fraction: from pathophysiology to clinical studies. Journal of clinical medicine 2019, 8, 792. [Google Scholar] [CrossRef]
- Roger, VL. Epidemiology of heart failure: a contemporary perspective. Circulation research 2021, 128, 1421–1434. [Google Scholar] [CrossRef]
- Kilgore M, Patel HK, Kielhorn A, Maya JF, Sharma P. Economic burden of hospitalizations of Medicare beneficiaries with heart failure. Risk management and healthcare policy 2017, 63–70. [Google Scholar]
- Arora S, Patel P, Lahewala S, Patel N, Patel NJ, Thakore K, et al. Etiologies, trends, and predictors of 30-day readmission in patients with heart failure. The American journal of cardiology 2017, 119, 760–769. [Google Scholar] [CrossRef]
- Grosman-Rimon L, Billia F, Wright E, Carasso S, Elbaz-Greener G, Kachel E, et al. Neurohormones, inflammatory mediators, and cardiovascular injury in the setting of heart failure. Heart Failure Reviews 2020, 25, 685–701. [Google Scholar] [CrossRef]
- Chaudhry R, Mahmood A, Ullah I, Urra EP, Masmoum MD, Atif A, et al. Heart Failure: Causes, Symptoms, and Management Strategies. Journal of Advances in Medicine and Medical Research 2024, 36, 335–345. [Google Scholar] [CrossRef]
- Ge Z, Li A, McNamara J, Dos Remedios C, Lal S. Pathogenesis and pathophysiology of heart failure with reduced ejection fraction: translation to human studies. Heart failure reviews 2019, 24, 743–758. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, BA. The pathophysiology of heart failure with preserved ejection fraction. Nature Reviews Cardiology 2014, 11, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Gevaert AB, Boen JR, Segers VF, Van Craenenbroeck EM. Heart failure with preserved ejection fraction: a review of cardiac and noncardiac pathophysiology. Frontiers in physiology 2019, 10, 638. [Google Scholar] [CrossRef] [PubMed]
- Fayyaz AU, Eltony M, Prokop LJ, Koepp KE, Borlaug BA, Dasari S, et al. Pathophysiological insights into HFpEF from studies of human cardiac tissue. Nature Reviews Cardiology 2024, 1–15. [Google Scholar]
- Schiattarella GG, Rodolico D, Hill JA. Metabolic inflammation in heart failure with preserved ejection fraction. Cardiovascular research 2021, 117, 423–434. [Google Scholar] [CrossRef]
- Sandireddy R, Sakthivel S, Gupta P, Behari J, Tripathi M, Singh BK. Systemic impacts of metabolic dysfunction-associated steatotic liver disease (MASLD) and metabolic dysfunction-associated steatohepatitis (MASH) on heart, muscle, and kidney related diseases. Frontiers in Cell and Developmental Biology 2024, 12, 1433857. [Google Scholar]
- Leite AR, Dias J, Godinho T, Correia-Chaves J, Borges-Canha M, Lourenço IM, et al. Metabolic Dysfunction-associated Steatotic Liver Disease and Heart Failure with Preserved Ejection Fraction: a bidirectional relationship with clinical and therapeutic implications. Endocrinology Insights 2024, 1–17.
- Lopez-Candales A, Burgos PMH, Hernandez-Suarez DF, Harris D. Linking chronic inflammation with cardiovascular disease: from normal aging to the metabolic syndrome. Journal of nature and science 2017, 3.
- Gehrke N, Schattenberg JM. Metabolic inflammation—a role for hepatic inflammatory pathways as drivers of comorbidities in nonalcoholic fatty liver disease? Gastroenterology 2020, 158, 1929–1947.e6.
- Ferenc K, Jarmakiewicz-Czaja S, Sokal-Dembowska A, Stasik K, Filip R. Common Denominator of MASLD and Some Non-Communicable Diseases. Current Issues in Molecular Biology 2024, 46, 6690–6709. [Google Scholar] [CrossRef] [PubMed]
- Jamalinia M, Lonardo A. determinants and assessment of cardiovascular risk in steatotic liver disease owing to metabolic dysfunction-addressing the challenge. Metabolism and Target Organ Damage 2024, 4, N/A-N/A.
- Yanai H, Adachi H, Hakoshima M, Iida S, Katsuyama H. Metabolic-Dysfunction-Associated Steatotic Liver Disease—Its Pathophysiology, Association with Atherosclerosis and Cardiovascular Disease, and Treatments. International journal of molecular sciences 2023, 24, 15473. [Google Scholar] [CrossRef] [PubMed]
- Shin S, Kim J, Lee JY, Kim J, Oh C-M. Mitochondrial quality control: its role in metabolic dysfunction-associated steatotic liver disease (MASLD). Journal of Obesity & Metabolic Syndrome 2023, 32, 289.
- Svobodová G, Horní M, Velecká E, Boušová I. Metabolic dysfunction-associated steatotic liver disease-induced changes in the antioxidant system: a review. Archives of Toxicology 2024, 1–22.
- Zhao Y, Zhou Y, Wang D, Huang Z, Xiao X, Zheng Q, et al. Mitochondrial Dysfunction in Metabolic Dysfunction Fatty Liver Disease (MAFLD). International Journal of Molecular Sciences 2023, 24, 17514. [Google Scholar] [CrossRef]
- Ma Y, Wang J, Xiao W, Fan X. A review of MASLD-related hepatocellular carcinoma: progress in pathogenesis, early detection, and therapeutic interventions. Frontiers in Medicine 2024, 11, 1410668. [Google Scholar] [CrossRef]
- He Y, Huang W, Zhang C, Chen L, Xu R, Li N, et al. Energy metabolism disorders and potential therapeutic drugs in heart failure. Acta Pharmaceutica Sinica B 2021, 11, 1098–1116. [Google Scholar] [CrossRef]
- Ramaccini D, Montoya-Uribe V, Aan FJ, Modesti L, Potes Y, Wieckowski MR, et al. Mitochondrial function and dysfunction in dilated cardiomyopathy. Frontiers in cell and developmental biology 2021, 8, 624216. [Google Scholar]
- Bansal SK, Bansal MB. Pathogenesis of MASLD and MASH–role of insulin resistance and lipotoxicity. Alimentary Pharmacology & Therapeutics 2024, 59, S10–S22. [Google Scholar]
- Meagher P, Adam M, Civitarese R, Bugyei-Twum A, Connelly KA. Heart failure with preserved ejection fraction in diabetes: mechanisms and management. Canadian Journal of Cardiology 2018, 34, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Caturano A, Vetrano E, Galiero R, Sardu C, Rinaldi L, Russo V, et al. Advances in the Insulin–Heart Axis: Current Therapies and Future Directions. International Journal of Molecular Sciences 2024, 25, 10173. [Google Scholar] [CrossRef] [PubMed]
- Varghese TP, Tazneem B. Unraveling the complex pathophysiology of heart failure: insights into the role of renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system (SNS). Current Problems in Cardiology 2024, 49, 102411. [Google Scholar] [CrossRef] [PubMed]
- Manolis AA, Manolis TA, Manolis AS. Neurohumoral activation in heart failure. International Journal of Molecular Sciences 2023, 24, 15472. [Google Scholar] [CrossRef] [PubMed]
- McGrath MS, Wentworth BJ. The Renin–Angiotensin System in Liver Disease. International Journal of Molecular Sciences 2024, 25, 5807. [Google Scholar] [CrossRef]
- Akkız H, Gieseler RK, Canbay A. Liver fibrosis: From basic science towards clinical progress, focusing on the central role of hepatic stellate cells. International Journal of Molecular Sciences 2024, 25, 7873. [Google Scholar] [CrossRef]
- Hara A, Tallquist MD. Fibroblast and immune cell cross-talk in cardiac fibrosis. Current Cardiology Reports 2023, 25, 485–493. [Google Scholar] [CrossRef]
- Amrute JM, Luo X, Penna V, Bredemeyer A, Yamawaki T, Yang S, et al. Targeting immune-fibroblast crosstalk in myocardial infarction and cardiac fibrosis. Research square. 2023.
- Boeckmans J, Sandrin L, Knackstedt C, Schattenberg JM. Liver stiffness as a cornerstone in heart disease risk assessment. Liver International 2024, 44, 344–356. [Google Scholar] [CrossRef]
- Macerola N, Riccardi L, Di Stasio E, Montalto M, Gasbarrini A, Pompili M, et al. Prognostic value of liver stiffness in patients hospitalized for acute decompensated heart failure: a meta-analysis. Journal of Ultrasound. 2024, 1–7.
- Mantovani A, Petracca G, Csermely A, Beatrice G, Bonapace S, Rossi A, et al. Non-alcoholic fatty liver disease and risk of new-onset heart failure: an updated meta-analysis of about 11 million individuals. Gut 2023, 72, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Inciardi RM, Mantovani A, Targher G. Non-alcoholic fatty liver disease as an emerging risk factor for heart failure. Current Heart Failure Reports 2023, 20, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Petrescu M, Vlaicu SI, Ciumărnean L, Milaciu MV, Mărginean C, Florea M, et al. Chronic inflammation—A link between nonalcoholic fatty liver disease (NAFLD) and dysfunctional adipose tissue. Medicina 2022, 58, 641. [Google Scholar] [CrossRef] [PubMed]
- Chen L-z, Jing X-b, Wu C-f, Zeng Y-c, Xie Y-c, Wang M-q, et al. Nonalcoholic fatty liver disease-associated liver fibrosis is linked with the severity of coronary artery disease mediated by systemic inflammation. Disease Markers 2021, 2021, 6591784. [Google Scholar]
- Xie W, Gan J, Zhou X, Tian H, Pan X, Liu W, et al. Myocardial infarction accelerates the progression of MASH by triggering immunoinflammatory response and induction of periosti. Cell metabolism 2024, 36, 1269–1286. [Google Scholar] [CrossRef]
- Nasiri-Ansari N, Androutsakos T, Flessa C-M, Kyrou I, Siasos G, Randeva HS, et al. Endothelial cell dysfunction and nonalcoholic fatty liver disease (NAFLD): A concise review. Cells 2022, 11, 2511. [Google Scholar] [CrossRef]
- Garbuzenko, DV. Pathophysiological mechanisms of cardiovascular disorders in non-alcoholic fatty liver disease. Gastroenterology and Hepatology from Bed to Bench 2022, 15, 194. [Google Scholar]
- Sanyal AJ, Husain M, Diab C, Mangla KK, Shoeb A, Lingvay I, et al. Cardiovascular disease in patients with metabolic dysfunction-associated steatohepatitis compared with metabolic dysfunction-associated steatotic liver disease and other liver diseases: A systematic review. American Heart Journal Plus: Cardiology Research and Practice. 2024, 100386.
- Patel SS, Nabi E, Guzman L, Abbate A, Bhati C, Stravitz RT, et al. Coronary artery disease in decompensated patients undergoing liver transplantation evaluation. Liver transplantation 2018, 24, 333–342. [Google Scholar] [CrossRef]
- Simon TG, Roelstraete B, Hagström H, Sundström J, Ludvigsson JF. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: results from a nationwide histology cohort. Gut 2022, 71, 1867–1875. [Google Scholar] [CrossRef]
- VanWagner LB, Lapin B, Skaro AI, Lloyd-Jones DM, Rinella ME. Impact of renal impairment on cardiovascular disease mortality after liver transplantation for nonalcoholic steatohepatitis cirrhosis. Liver International 2015, 35, 2575–2583. [Google Scholar] [CrossRef] [PubMed]
- Wei Z, Huang Z, Song Z, Zhao W, Zhao D, Tan Y, et al. Metabolic Dysfunction-associated fatty liver disease and incident heart failure risk: the Kailuan cohort study. Diabetology & Metabolic Syndrome 2023, 15, 137. [Google Scholar]
- Nagai S, Collins K, Chau LC, Safwan M, Rizzari M, Yoshida A, et al. Increased risk of death in first year after liver transplantation among patients with nonalcoholic steatohepatitis vs liver disease of other etiologies. Clinical gastroenterology and hepatology 2019, 17, 2759–2768.e5. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Cardiac remodeling and MASLD share pathophysiological drivers leading to HFpEF. Structural changes cause functional alterations in the heart, while hepatic flow obstruction impacts preload reserve.
Figure 1.
Cardiac remodeling and MASLD share pathophysiological drivers leading to HFpEF. Structural changes cause functional alterations in the heart, while hepatic flow obstruction impacts preload reserve.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



