Submitted:
10 November 2024
Posted:
11 November 2024
You are already at the latest version
Abstract
Background/Objectives: The prognosis of acute lymphoblastic leukemia has changed radically since the incorporation of innovative therapies such as immunotherapy, tyrosine kinase blockers, and CAR-T-based therapy. In lymphoblastic leukemia, both the expression and different types of polymorphisms in resistance proteins (ABCB1), have been associated with greater resistance to drugs from cell lines to clinical different scenarios. Although measurable residual disease is the best tool for monitoring acute lymphoblastic leukemia´s treatment, its association with the ABCB1 gene is still unknown. Aims: to describe the association of the expression of the ABCB1 resistance gene with measurable residual disease. Methods: Prospective cohort where 37 patients with de novo diagnosis of Acute Lymphoblastic Leukemia were admitted to the Hospital General de México “Dr. Eduardo Liceaga” between 2022 and 2024. Results: A total of 57 patients who began chemotherapy-based treatment were studied, the majority were male (n=30, 52.6%), with a mean age of 32 years (range 18 to 71 years). When analyzing the expression of the ABCB1 drug resistance gene, 35.1% (n=20) were considered to have low expression, 40.4% (n=23) overexpressed the gene and 24.6% (n=14) showed absent expression. Association was not identified between MRD positivity with the Philadelphia chromosome (p=0.171, 95% CI) or the ABCB1 group considered high risk (high or absent expression) (p=0.538, 95% CI). Conclusions: In conclusion, identifying drug-resistance genes remains useful for acute leukemias while the treatment remains chemotherapy-based. Nevertheless, in an age of personalized medicine, the determination of MRD is the main prognosis factor that could predict a failure in therapy.
Keywords:
ABCB1 gene
; Acute Lymphoblastic Leukemia
; Measurable Residual Disease
; Adults
1. Introduction
The prognosis of acute lymphoblastic leukemia has changed radically since the incorporation of innovative therapies such as immunotherapy (monoclonal, bi-specific antibodies), tyrosine kinase blockers, and, more recently, the introduction of CAR-T-based therapy [1,2]; despite this, most patients continue to be treated through chemotherapy, especially during a bone marrow relapse. The sum of different factors, both clinical (age, leukocyte count) and molecular (Philadelphia chromosome, Ph+ like leukemia or abnormalities in KMT2A), increase the risk of relapse, especially in adolescents and adults [3,4,5].
One of the most important abnormalities within the resistance mechanisms is related to the expression of drug-resistance genes belonging to the ABC (ATP binding cassette) family that encode the expression of different efflux pumps in cell membranes [6]. P-glycoprotein (P-gp or MRP1) is a member of this family that, along with the ABCG2 gene (known as BCRP), and its expression is variable in different tissues (placenta, kidney, blood-brain barrier), as well as in neoplastic cells, causing the expulsion of different substrates, including different types of chemotherapy [7,8,9]. In lymphoblastic leukemia, both the expression and the different types of polymorphisms in resistance proteins (ABCB1 or MDR1, ABCC1 or MRP1), have been associated with greater resistance to drugs (steroids, vincristine, doxorubicin) from cell lines to clinical different scenarios [10,11,12,13]. In our center, it was identified that high expression levels (4.5 times) were related to higher mortality and a higher risk of induction failure [14,15].
These factors are analyzed at diagnosis and have been displaced by the identification of measurable residual disease detected at different treatment stages [16]. Its detection can be carried out through both molecular techniques (Next-generation sequencing) and multiparametric flow cytometry, which, being negative (ERM negative <0.01% cells (for example, ≥104), allows adaptation of treatment regimens to reduce toxicity [17,18]. The persistence of residual disease translates as resistance to different combinations of drugs, among which are those mediated by p-glycoprotein. Although measurable residual disease is the best tool for monitoring the treatment of acute lymphoblastic leukemia, its association with the different drug-resistance genes is still unknown. This study aims to describe the association of the expression of the ABCB1 resistance gene with measurable residual disease.
2. Materials and Methods
Patients with de novo diagnosis of Acute Lymphoblastic Leukemia who were admitted to the Hospital General de México “Dr. Eduardo Liceaga” between 2022 and 2024 were included. The diagnosis of Acute lymphoblastic Leukemia was corroborated by morphological analysis and flow cytometry. The exclusion criteria were: (1) neutropenia, infections, and bleeding at admission; (2); alterations of heart function; (3) bone marrow or central nervous system relapse; or (4) referral from another hospital and who were treated at our service.
All individuals began induction treatment based on the CALGB10403 scheme when the patients were considered to belong to the AYA group (Adolescents and Young Adults), and the rest were treated with a HyperCVAD; central nervous system prophylaxis was performed through intrathecal chemotherapy with Methotrexate and Cytarabine (19,20). The response to induction treatment was carried out through morphological analysis, and it was considered refractory if there were >5% blasts after induction. After induction on day 45 of treatment, measurable residual disease in bone marrow was determined through flow cytometry, with a value greater than 0.01% considered positive. A bone marrow blast value greater than 5% at any time during treatment was considered a relapse. The selection of the relapse scheme was to the consideration of the medical staff and available resources.
The real-time polymerase chain reaction (RQ-PCR) test based on specific oligonucleotides determined the Philadelphia chromosome. Samples were obtained from bone marrow or peripheral blood.
This prospective study was carried out following the Helsinki Declaration and approved by the Biosecurity, Ethics, and Research Committee of Hospital General de México “Dr. Eduardo Liceaga,” under the protocol number HGM/DI/08/204/04/17. This study completed the CONSORT 2010 checklist for Randomized Trials.
2.1. Expression levels of ABCB1 gene
From each patient, mononuclear cells were obtained by Lymphoprep (Axis-Shield, Oslo, Norway) from anticoagulated blood with EDTA (Vacutainer tubes, BD Diagnostics Franklin Lakes, New Jersey) before chemotherapy treatment, homogenized in TRIzol (Invitrogen, Life Technologies Carlsbad, CA) for total RNA extraction according to the manufacturer’s protocol. For cDNA synthesis, 2000 ng of RNA was reverse transcribed according to the manufacturer’s protocol (PROMEGA, Madison WI, USA).
To determine the relative expression levels of the ABCB1 transcript, RT-qPCR was performed in triplicate on Step One ™ Applied Biosystems equipment, using 100 ng of cDNA, and specific hydrolysis probes for ABCB1 (Hs04992772_s1), and endogenous control GUSB (Hs00939627_m1), using K562 hematological cell line (CCL-243™, ATCC) as reference sample. Expression levels were obtained with the 2-ΔΔCt method. The ABCB1 expression levels were categorized as previously described [15].
2.2. Minimal residual Disease (MRD)
After induction, Minimal Residual Disease (MRD) testing was performed to evaluate the clearance of blast cells in the bone marrow (BM). For MRD determination, 5 mL of heparin-anticoagulated BM was obtained for multiparametric flow cytometry immunophenotype analysis. A minimum of 1x106 events were analyzed for blast detection (CD45dim/CD34/CD10/CD19/CD22) into the cellular population (granulocytes, monocytes, and lymphocytes). The absence of blast cells determined an MDR negative test, and a blast/total event ratio (%) obtained an MDR positive result.
3. Results
3.1. General characteristics of the patients
A total of 57 patients who began chemotherapy-based treatment were studied, the majority were male (n=30, 52.6%), with a mean age of 32 years (range 18 to 71 years). 93% (n=53) corresponded to B precursor leukemia, 7% (n=4) to T precursor leukemia, 5.3% (n=3) had infiltration into the central nervous system at diagnosis and 15.8% (n =9) corresponded to a positive ALL-Philadelphia. The average leukocyte count at diagnosis was 69 x 103/µl (0.2- 362 x 103/µl), of which 49% (n=28) showed counts greater than 30 x 103/µl at diagnosis. When combining the risk factors, 75.4% (n=43) were classified as high risk while 24.6% (n=14) were classified as usual risk. (Table 1)
3.2. Clinical response and follow-up.
The percentage of complete remissions was 64.9% (n=37), 15.8% (n=9) died in the induction stage and 19.3% (n=11) were considered refractory. In individuals at usual risk, the percentage of complete remissions was higher (71.4% v 62.8%), being lower in individuals over 35 years of age (57.1%) and with the presence of the Philadelphia chromosome (55.6%). The mean follow-up was 352 days (range 284-420, 95% CI), with a mortality rate of 47.4% (n=27). During follow-up, 19.3% (n=11) presented bone marrow relapse, with the highest being in the high-risk group (20.9%) and in cases with Ph+-ALL (n=3, 33.3%).
3.3. Expression of the drug resistance gene ABCB1
When analyzing the expression of the ABCB1 drug resistance gene, 35.1% (n=20) were considered to have low expression, 40.4% (n=23) overexpressed the gene and 24.6% (n=14) showed absent expression. When combining risk expression levels (overexpression or absent expression), no significant differences were found in patients with leukocyte counts greater than 30 x 103/µl (48.6% vs 51.4%, p=0.571, 95% CI) or the type of risk (71.4% vs 62.8%, p=0.402, 95% CI). According to the response to treatment, 62.2% (n=23) of the cases that integrated complete remission (CR) had a high or absent expression, while refractory cases showed a higher percentage (72.7%, n=8) of abnormalities in gene expression. Likewise, patients with bone marrow relapse showed a higher percentage of risk expression (63.6%), but this difference was not significant (p=0.591, 95% CI). When analyzing the follow-up, both cases with absent expression or high expression showed lower survival, but without being significant in the long term (Log-Rank 0.350).
3.4. Measurable Residual Disease (MRD)
The determination of measurable residual disease was carried out by flow cytometry on day 45 of treatment, the presence of a positive MRD at the end of induction was recorded in 66.7% (n=32), when evaluating the positivity of the MRD with variables such as risk, age or leukocyte count (p=0.356, p=0.366, p=0.179 respectively) no significant association was identified. Regarding molecular abnormalities, an association was not identified between MRD positivity with the Philadelphia chromosome (p=0.171, 95% CI) or the ABCB1 group considered high risk (high or absent expression) (p=0.538, 95% CI). When individually analyzing the positivity of the MRD with the different expression levels of the ABCB1 gene, most of the individuals with absent expression showed a positive MRD (n=10 of 12 individuals, 83.3%), while the behavior of positivity in individuals with low or high expression was similar (64.7% and 57.9% respectively). When analyzing the association between absent expressions individually, no other association was identified (p=0.144, 95%CI). Regarding survival, the presence of a negative MRD was associated with a favorable prognosis (Log-Rank 0.048).
3.5. Factors associated with survival.
Overall survival at 600 days of follow-up was 56%, with the median survival reaching 641 days (428-640 days, 95% CI). Variables such as clinical risk at diagnosis (log Rank 0.699), age over 35 years (log Rank 0.242), or leukocyte count over 30 x 103/mcl (Log Rank 0.824) did not show an impact on survival. According to the molecular alterations, the expression of the Philadelphia chromosome was associated with greater survival (Log Rank 0.076) due to the combination with second-generation tyrosine kinase inhibitors, while low expression of the ABCB1 gene showed better behavior, but without showing a significant difference (Log Rank 0.350). In contrast to the different variables, positive measurable residual disease behaved as a risk factor for overall survival, since its negativity was associated (negative MRD) with better survival (p=0.048, 95% CI). The survival curves according to the MRD and the expression of the ABCB1 resistance gene are presented in Figure 1 and Figure 2.
When analyzing the different variables that impacted the response, no clinical variable was identified that significantly impacted the possibility of achieving a negative MRD, while, for overall and disease-free survival, the positivity of an MRD behaved as a risk factor (RR). The relative risk of the different variables on overall survival is presented in Figure 3.
When analyzing the behavior of the different expression patterns, both its overexpression and its absence did not impact the percentage of relapses or the presence of a positive MRD, particularly in individuals who had a risk expression of the ABCB1 gene, the presence of a negative measurable residual disease significantly improved the prognosis in this risk group (Figure 4).
4. Discussion
This study explores the relation between the positivity of measurable residual disease (MRD) and the different expression levels of the ABCB1 drug resistance gene [23]. ABCB1 codifies the P-glycoprotein, a transmembrane protein involved in the expulsion of various substrates, including chemotherapy agents.
Although the phenotype multi-drug resistance (MDR) is not sufficient to induce resistance on its own, it requires changes in the microenvironment and other mechanisms, like those mediated by extracellular vesicles [24]. Strategies to inhibit the P-glycoprotein have been explored, like the use of medications like verapamil, cyclosporine, elacridar, laniquidar, zosuquidar, or the use of liposome-encapsulated drugs designed to avoid this resistance mechanism [25,26].
In acute lymphoblastic leukemia (ALL), both the expression as well as certain polymorphisms (rs1045642 genotype (3435 C>T)) of the ABCB1 gene affect the response to essential medications like methotrexate, vincristine, and 6-mercaptopurine, increasing the toxicity and reducing its efficiency [27,28,29]. Our group had previously identified that both the overexpression as well as the absence of expression of the ABCB1 gene have an impact on the prognosis, suggesting that drugs like metformin might be useful for this specific group of patients [15,30].
The resistance, evidenced by the persistence of residual cells, can be identified through various techniques, each with different sensitivities, but all maintaining a limit of detection (≥10−4). Although some techniques can have limitations due to cost or access, most agree that the persistence of the disease is related to a relapse, especially in the first few months of treatment [31].
Since the positivity of the MDR is the main factor associated with the failure of the treatment, our study is centered on identifying its association with the treatment-resistant gene. While the behavior analysis of the gene expression did not present a statistical impact, a higher rate of changes in the gene in refractory or relapse patients was observed, albeit without a clear association with the positivity in MRD.
On an individual level, the positivity in MRD had an impact in the prognosis, consolidating itself as the main factor of risk associated with it. In conclusion, despite the alterations detected at diagnosis, both clinical and biological, the MRD remains the main prognosis factor. This indicates that the intensification of the treatment to prevent relapses might be necessary, even in patients with a favorable initial prognosis.
The lack of relevant association between the resistance gene and the MRD could be attributed to the resistance being measured not only by mechanisms related to the P-glycoprotein, but also involves transporters such as ABCG2, exportin-mediated nuclear mechanisms (XPO), and enzymes like paraoxonase 2 (PON2) [32,33,34,35]. Another resistance mechanism is associated with the expression of antiapoptotic proteins like Bcl-2, similar to acute myeloid leukemia, where the lymphoblasts can express this protein and be susceptible to drugs like Venetoclax [36].
It is important to consider that several medications can be substrates of these efflux pumps and act with an antagonistic effect. The correlation of in vitro results can help personalize the treatment [37,38]. Lastly, with the introduction of new strategies based on monoclonal antibodies, the resistance mechanism through efflux proteins will be replaced by new mechanisms regulated by the microenvironment or by the adjustment of expression of different types of receptors [39,40].
In conclusion, identifying drug-resistance genes remains useful for acute leukemias while the treatment remains chemotherapy-based. Nevertheless, in an age of personalized medicine, the determination of MRD is the main prognosis factor that could predict a failure in therapy
Author Contributions
Conceptualization, Christian Ramos Peñafiel and Adán Gallardo Rodriguez; Data curation, Daniela Pérez Sámano, Rafael Cerón-Maldonado and Adán Gallardo Rodriguez; Formal analysis, Daniela Pérez Sámano and Adán Gallardo Rodriguez; Funding acquisition, Christian Ramos Peñafiel, Adolfo Martínez Tovar and Irma Olarte Carrillo; Investigation, Christian Ramos Peñafiel and Adán Gallardo Rodriguez; Methodology, Christian Ramos Peñafiel, Rafael Cerón-Maldonado and Adán Gallardo Rodriguez; Project administration, Christian Ramos Peñafiel and Adolfo Martínez Tovar; Resources, Adolfo Martínez Tovar and Irma Olarte Carrillo; Software, Rafael Cerón-Maldonado and Adán Gallardo Rodriguez; Supervision, Christian Ramos Peñafiel and Carlos Martínez Murillo; Validation, Christian Ramos Peñafiel, Adolfo Martínez Tovar, Carlos Martínez Murillo and Irma Olarte Carrillo; Visualization, Christian Ramos Peñafiel and Adolfo Martínez Tovar; Writing – original draft, Adán Gallardo Rodriguez; Writing – review & editing, Christian Ramos Peñafiel, Adolfo Martínez Tovar, Carlos Martínez Murillo and Irma Olarte Carrillo. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted following the Helsinki Declaration and approved by the Biosecurity, Ethics and Research Committee of “Hospital General de México “Dr. Eduardo Liceaga,” under the protocol number (HGM/DI/08/204/04/17). This study completed the CONSORT 2010 checklist for Randomized Trials.
Informed Consent Statement
Not applicable.
Data Availability Statement
Due to privacy and confidentiality restrictions, the data presented in this study is available on request from the corresponding author. The data are not publicly available due to the confidentiality restrictions of the Biosecurity, Ethics, and Research Committee of Hospital General de México “Dr. Eduardo Liceaga”
Conflicts of Interest
The authors declare no conflict of interest
References
- Samra B, Jabbour E, Ravandi F, Kantarjian H, Short NJ. Evolving therapy of adult acute lymphoblastic leukemia: state-of-the-art treatment and future directions. J Hematol Oncol [Internet]. 2020, 13, 70. [Google Scholar] [CrossRef] [PubMed]
- Kegyes D, Jitaru C, Ghiaur G, Ciurea S, Hoelzer D, Tomuleasa C, et al. Switching from salvage chemotherapy to immunotherapy in adult B-cell acute lymphoblastic leukemia. Blood Rev [Internet]. 2023, 59, 101042. [Google Scholar] [CrossRef] [PubMed]
- Aberuyi N, Rahgozar S, Ghodousi ES, Ghaedi K. Drug resistance biomarkers and their clinical applications in childhood acute lymphoblastic leukemia. Front Oncol [Internet]. 2019, 9, 1496. [Google Scholar] [CrossRef]
- Ribera J-M. Philadelphia chromosome-like acute lymphoblastic leukemia. Still a pending matter. Haematologica [Internet]. 2021, 106, 1514–1516. [Google Scholar] [CrossRef]
- Chiaretti S, Messina M, Della Starza I, Piciocchi A, Cafforio L, Cavalli M, et al. Philadelphia-like acute lymphoblastic leukemia is associated with minimal residual disease persistence and poor outcome. First report of the minimal residual disease-oriented GIMEMA LAL1913. Haematologica [Internet]. 2021, 106, 1559–1568. [Google Scholar] [CrossRef]
- Lage, H. MDR1/P-glycoprotein (ABCB1) as target for RNA interference-mediated reversal of multidrug resistance. Curr Drug Targets [Internet]. 2006, 7, 813–821. [Google Scholar] [CrossRef]
- Lage, H. Gene therapeutic approaches to overcome ABCB1-mediated drug resistance. Recent Results Cancer Res [Internet]. 2016, 209, 87–94. [Google Scholar] [CrossRef]
- Xiao H, Zheng Y, Ma L, Tian L, Sun Q. Clinically-relevant ABC transporter for anti-cancer drug resistance. Front Pharmacol [Internet]. 2021, 12, 648407. [Google Scholar] [CrossRef]
- Dhakne P, Pillai M, Mishra S, Chatterjee B, Tekade RK, Sengupta P. Refinement of safety and efficacy of anti-cancer chemotherapeutics by tailoring their site-specific intracellular bioavailability through transporter modulation. Biochim Biophys Acta Rev Cancer [Internet]. 2023, 1878, 188906. [Google Scholar] [CrossRef]
- Dallavalle S, Dobričić V, Lazzarato L, Gazzano E, Machuqueiro M, Pajeva I, et al. Improvement of conventional anti-cancer drugs as new tools against multidrug resistant tumors. Drug Resist Updat [Internet]. 2020, 50, 100682. [Google Scholar] [CrossRef]
- Winter SS, Ricci J, Luo L, Lovato DM, Khawaja HM, Serna-Gallegos T, et al. ATP Binding Cassette C1 (ABCC1/MRP1)-mediated drug efflux contributes to disease progression in T-lineage acute lymphoblastic leukemia. Health [Internet]. 2013, 5, 41–50. [Google Scholar] [CrossRef]
- Gasic V, Zukic B, Stankovic B, Janic D, Dokmanovic L, Lazic J, et al. Pharmacogenomic markers of glucocorticoid response in the initial phase of remission induction therapy in childhood acute lymphoblastic leukemia. Radiol Oncol [Internet]. 2018, 52, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Chauhan PS, Bhushan B, Singh LC, Mishra AK, Saluja S, Mittal V, et al. Expression of genes related to multiple drug resistance and apoptosis in acute leukemia: response to induction chemotherapy. Exp Mol Pathol [Internet]. 2012, 92, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Kourti M, Vavatsi N, Gombakis N, Sidi V, Tzimagiorgis G, Papageorgiou T, et al. Expression of multidrug resistance 1 (MDR1), multidrug resistance-related protein 1 (MRP1), lung resistance protein (LRP), and breast cancer resistance protein (BCRP) genes and clinical outcome in childhood acute lymphoblastic leukemia. Int J Hematol [Internet]. 2007, 86, 166–173. [Google Scholar] [CrossRef]
- Olarte Carrillo I, Ramos Peñafiel C, Miranda Peralta E, Rozen Fuller E, Kassack Ipiña JJ, Centeno Cruz F, et al. Clinical significance of the ABCB1 and ABCG2 gene expression levels in acute lymphoblastic leukemia. Hematology [Internet]. 2017, 22, 286–291. [Google Scholar] [CrossRef]
- Ramos-Peñafiel C, Olarte-Carrillo I, Maldonado RC, de la Cruz Rosas A, Collazo-Jaloma J, Martínez-Tovar A. Association of three factors (ABCB1 gene expression, steroid response, early response at day + 8) on the response to induction in patients with acute lymphoblastic leukemia. Ann Hematol [Internet]. 2020, 99, 2629–2637. [Google Scholar] [CrossRef]
- Bassan R, Intermesoli T, Scattolin A, Viero P, Maino E, Sancetta R, et al. Minimal residual disease assessment and risk-based therapy in acute lymphoblastic leukemia. Clin Lymphoma Myeloma Leuk [Internet]. Available online. [CrossRef]
- Kruse A, Abdel-Azim N, Kim HN, Ruan Y, Phan V, Ogana H, et al. Minimal residual disease detection in acute lymphoblastic leukemia. Int J Mol Sci [Internet]. 2020, 21, 1054. [Google Scholar] [CrossRef]
- Correia RP, Bento LC, de Sousa FA, Barroso R de S, Campregher PV, Bacal NS. How I investigate minimal residual disease in acute lymphoblastic leukemia. Int J Lab Hematol [Internet]. 2021, 43, 354–363. [Google Scholar] [CrossRef]
- Rausch CR, Jabbour EJ, Kantarjian HM, Kadia TM. Optimizing the use of the hyperCVAD regimen: Clinical vignettes and practical management. Cancer [Internet]. 2020, 126, 1152–1160. [Google Scholar] [CrossRef]
- Stock W, Luger SM, Advani AS, Yin J, Harvey RC, Mullighan CG, et al. A pediatric regimen for older adolescents and young adults with acute lymphoblastic leukemia: results of CALGB 10403. Blood [Internet]. 2019, 133, 1548–1559. [Google Scholar] [CrossRef]
- Mohammad IS, He W, Yin L. Understanding of human ATP binding cassette superfamily and novel multidrug resistance modulators to overcome MDR. Biomed Pharmacother [Internet]. 2018, 100, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Assaraf YG, Brozovic A, Gonçalves AC, Jurkovicova D, Linē A, Machuqueiro M, et al. The multi-factorial nature of clinical multidrug resistance in cancer. Drug Resist Updat [Internet]. 2019, 46, 100645. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Mayea Y, Mir C, Masson F, Paciucci R, LLeonart ME. Insights into new mechanisms and models of cancer stem cell multidrug resistance. Semin Cancer Biol [Internet]. 2020, 60, 166–180. [Google Scholar] [CrossRef] [PubMed]
- Bugde P, Biswas R, Merien F, Lu J, Liu D-X, Chen M, et al. The therapeutic potential of targeting ABC transporters to combat multi-drug resistance. Expert Opin Ther Targets [Internet]. 2017, 21, 511–530. [Google Scholar] [CrossRef]
- Mayer LD, Tardi P, Louie AC. CPX-351: a nanoscale liposomal co-formulation of daunorubicin and cytarabine with unique biodistribution and tumor cell uptake properties. Int J Nanomedicine [Internet]. 2019, 14, 3819–3830. [Google Scholar] [CrossRef]
- Hu Y-H, Zhou L, Wang S-S, Jing X, Guo H-L, Sun F, et al. Methotrexate disposition in pediatric patients with acute lymphoblastic leukemia: What have we learnt from the genetic variants of drug transporters. Curr Pharm Des [Internet]. 2019, 25, 627–634. [Google Scholar] [CrossRef]
- Gervasini G, de Murillo SG, Jiménez M, de la Maya MD, Vagace JM. Effect of polymorphisms in transporter genes on dosing, efficacy and toxicity of maintenance therapy in children with acute lymphoblastic leukemia. Gene [Internet]. 2017, 628, 72–77. [Google Scholar] [CrossRef]
- Ramírez-Pacheco A, Moreno-Guerrero S, Alamillo I, Medina-Sanson A, Lopez B, Moreno-Galván M. Mexican childhood acute lymphoblastic leukemia: A pilot study of the MDR1 and MTHFR gene polymorphisms and their associations with clinical outcomes. Genet Test Mol Biomarkers [Internet]. 2016, 20, 597–602. [Google Scholar] [CrossRef]
- Ramos-Peñafiel C, Olarte-Carrillo I, Cerón-Maldonado R, Rozen-Fuller E, Kassack-Ipiña JJ, Meléndez-Mier G, et al. Effect of metformin on the survival of patients with ALL who express high levels of the ABCB1 drug resistance gene. J Transl Med [Internet]. 2018, 16, 245. [Google Scholar] [CrossRef]
- Della Starza I, De Novi LA, Elia L, Bellomarino V, Beldinanzi M, Soscia R, et al. Optimizing molecular minimal residual disease analysis in adult acute lymphoblastic leukemia. Cancers (Basel) [Internet]. 2023, 15, 374. [Google Scholar] [CrossRef]
- Allegra A, Innao V, Allegra AG, Leanza R, Musolino C. Selective inhibitors of nuclear export in the treatment of hematologic malignancies. Clin Lymphoma Myeloma Leuk [Internet]. 2019, 19, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Azmi AS, Uddin MH, Mohammad RM. The nuclear export protein XPO1 - from biology to targeted therapy. Nat Rev Clin Oncol [Internet]. 2021, 18, 152–169. [Google Scholar] [CrossRef] [PubMed]
- Tomiyasu H, Watanabe M, Sugita K, Goto-Koshino Y, Fujino Y, Ohno K, et al. Regulations of ABCB1 and ABCG2 expression through MAPK pathways in acute lymphoblastic leukemia cell lines. Anticancer Res. 2013, 33, 5317–5323. [Google Scholar]
- Hui P-Y, Chen Y-H, Qin J, Jiang X-H. PON2 blockade overcomes dexamethasone resistance in acute lymphoblastic leukemia. Hematology [Internet]. 2022, 27, 32–42. [Google Scholar] [CrossRef]
- Aumann S, Shaulov A, Haran A, Gross Even-Zohar N, Vainstein V, Nachmias B. The emerging role of venetoclax-based treatments in acute lymphoblastic leukemia. Int J Mol Sci [Internet]. 2022, 23, 10957. [Google Scholar] [CrossRef]
- de Moraes ACR, Maranho CK, Rauber GS, Santos-Silva MC. Importance of detecting multidrug resistance proteins in acute leukemia prognosis and therapy: Multidrug resistance proteins in acute leukemia. J Clin Lab Anal [Internet]. 2013, 27, 62–71. [Google Scholar] [CrossRef]
- Kolesnikova M, Sen’kova A, Tairova S, Ovchinnikov V, Pospelova T, Zenkova M. Clinical and prognostic significance of cell sensitivity to chemotherapy detected in vitro on treatment response and survival of leukemia patients. J Pers Med [Internet]. 2019, 9, 24. [Google Scholar] [CrossRef]
- Jędraszek K, Malczewska M, Parysek-Wójcik K, Lejman M. Resistance mechanisms in pediatric B-cell acute lymphoblastic leukemia. Int J Mol Sci [Internet]. 2022, 23, 3067. [Google Scholar] [CrossRef]
- Locatelli F, Shah B, Thomas T, Velasco K, Adedokun B, Aldoss I, et al. Incidence of CD19-negative relapse after CD19-targeted immunotherapy in R/R BCP acute lymphoblastic leukemia: a review. Leuk Lymphoma [Internet]. 2023, 64, 1615–1633. [Google Scholar] [CrossRef]
Figure 1.
Overall Survival Kaplan-Meier graph of patients with negative MRD versus positive MRD.
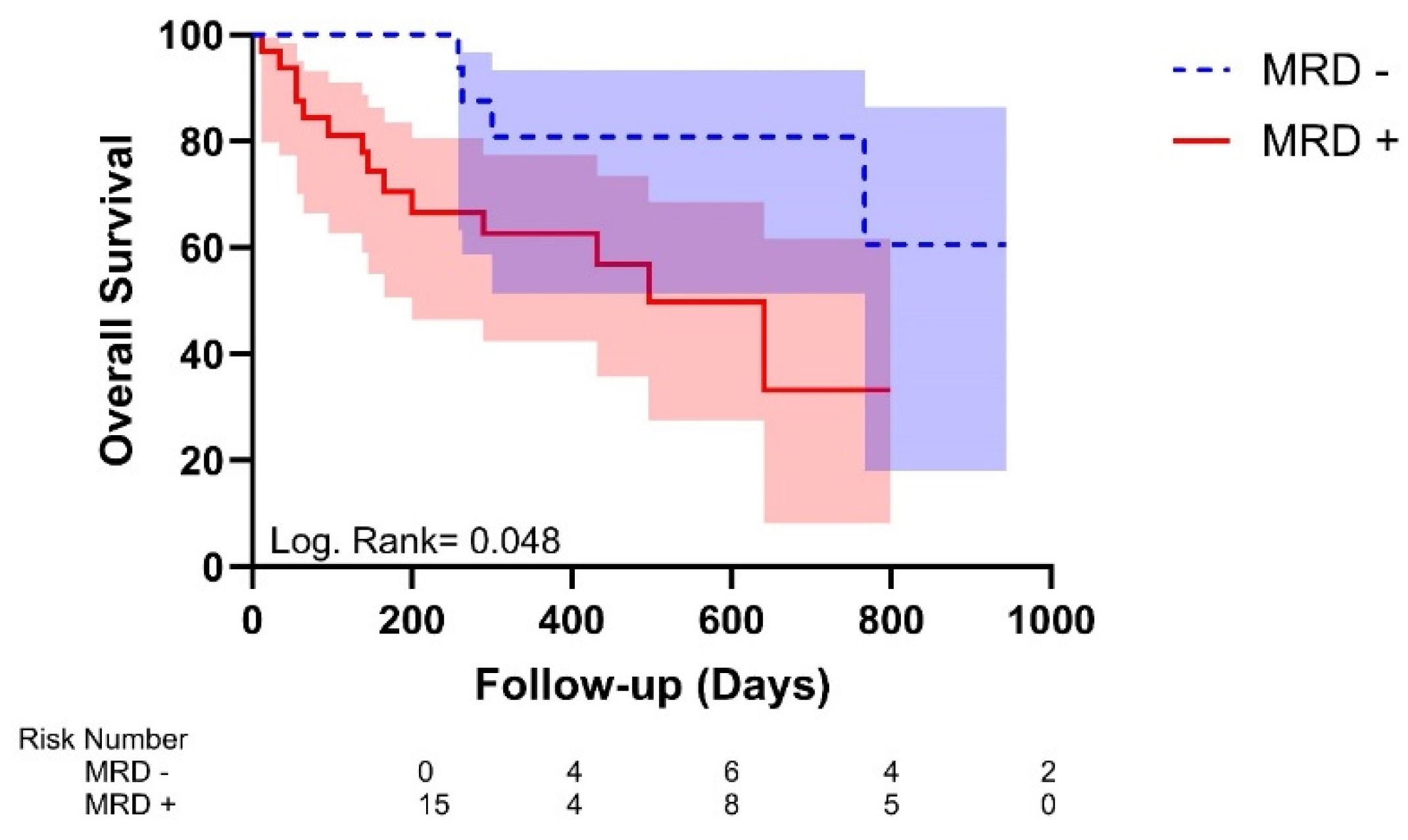
Figure 2.
Overall Survival Kaplan-Meier graph of patients with different ABCB1 gene expressions.
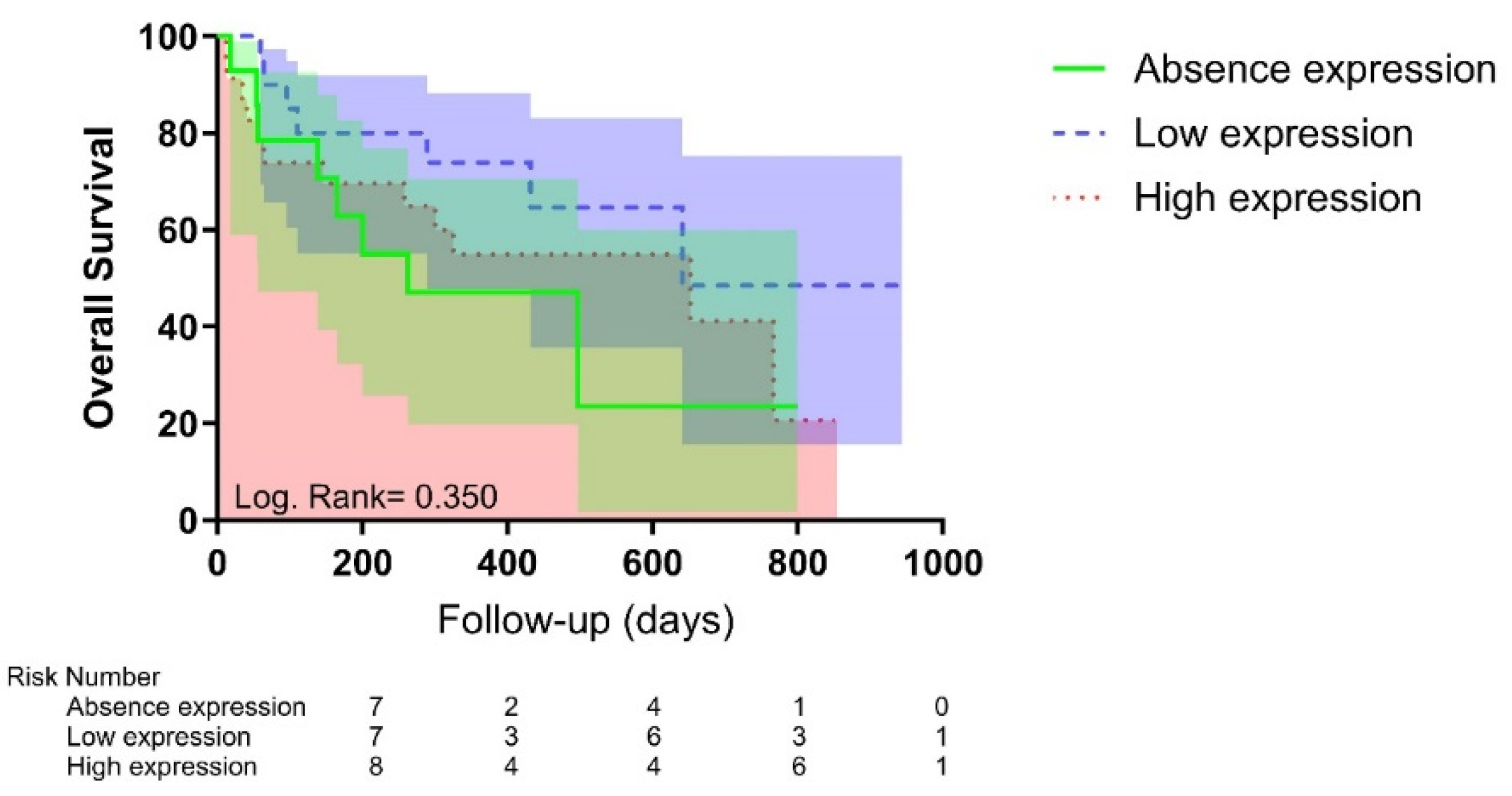
Figure 3.
Relative Risk of principal outcomes for overall survival.
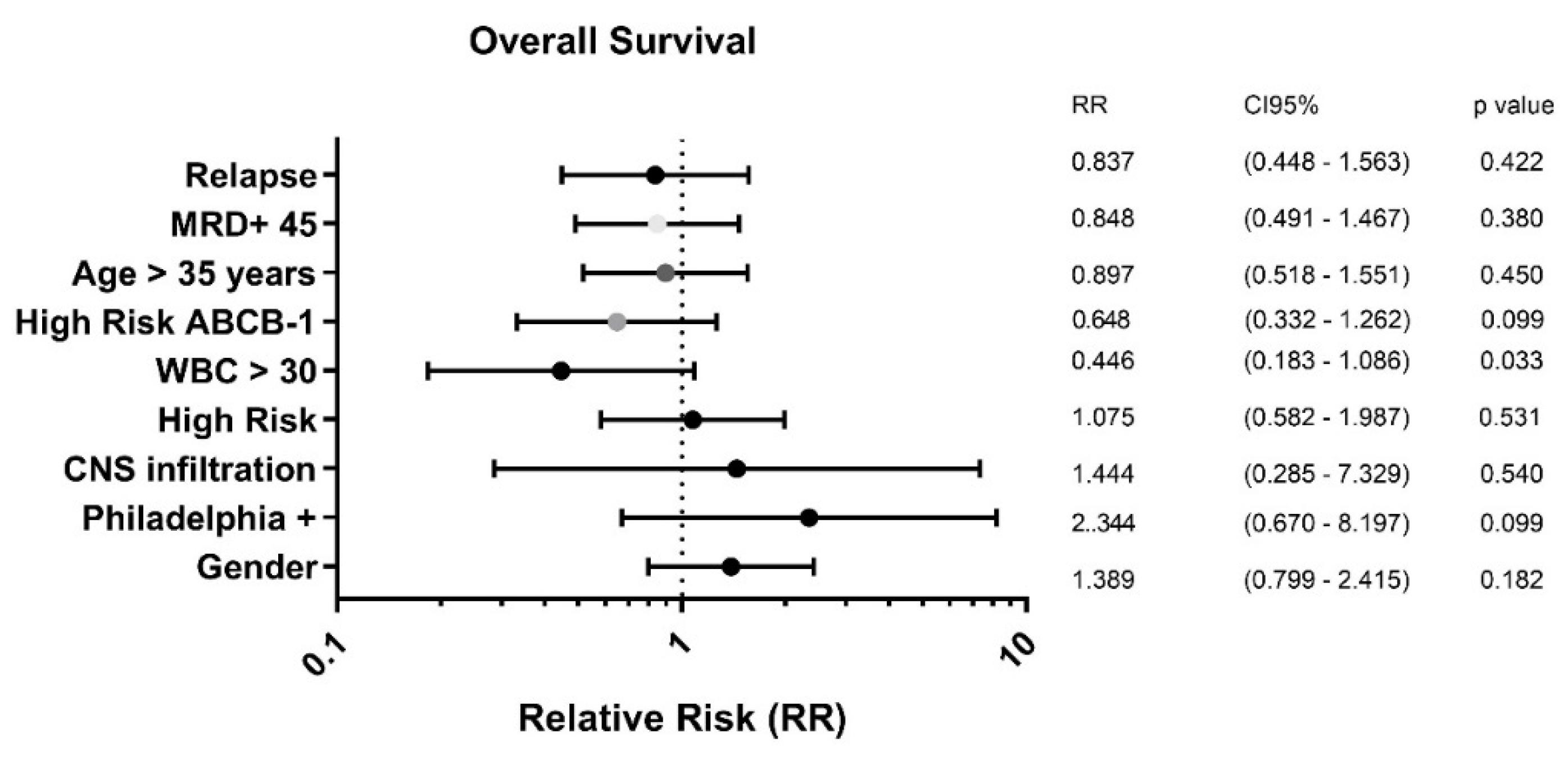
Figure 4.
Overall Survival Kaplan Meier graph of positive and negative MRD in patients with ABCB1 High Risk.
Figure 4.
Overall Survival Kaplan Meier graph of positive and negative MRD in patients with ABCB1 High Risk.
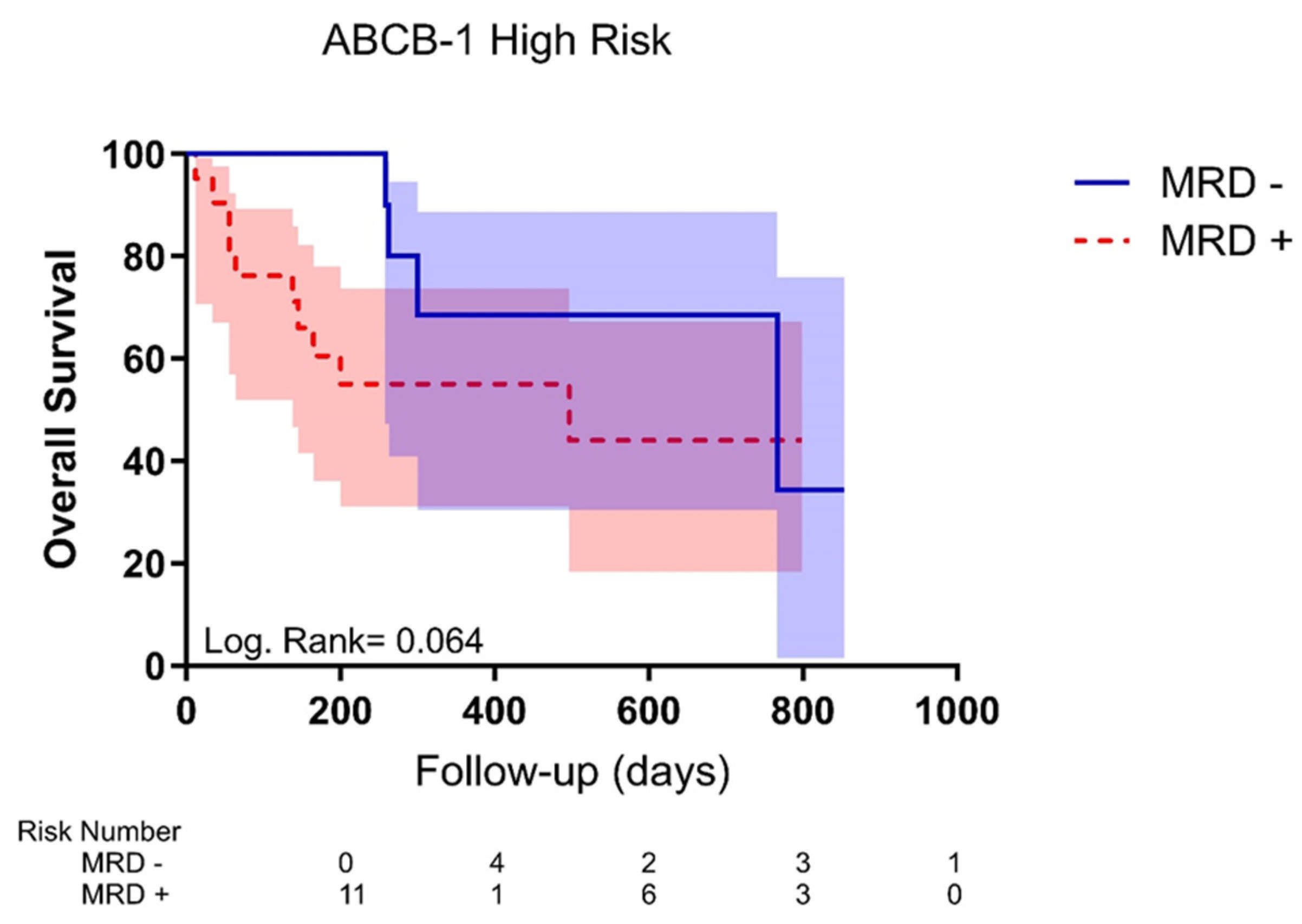
Figure 5.
Relative Risk of principal outcomes for positivity of MRD.
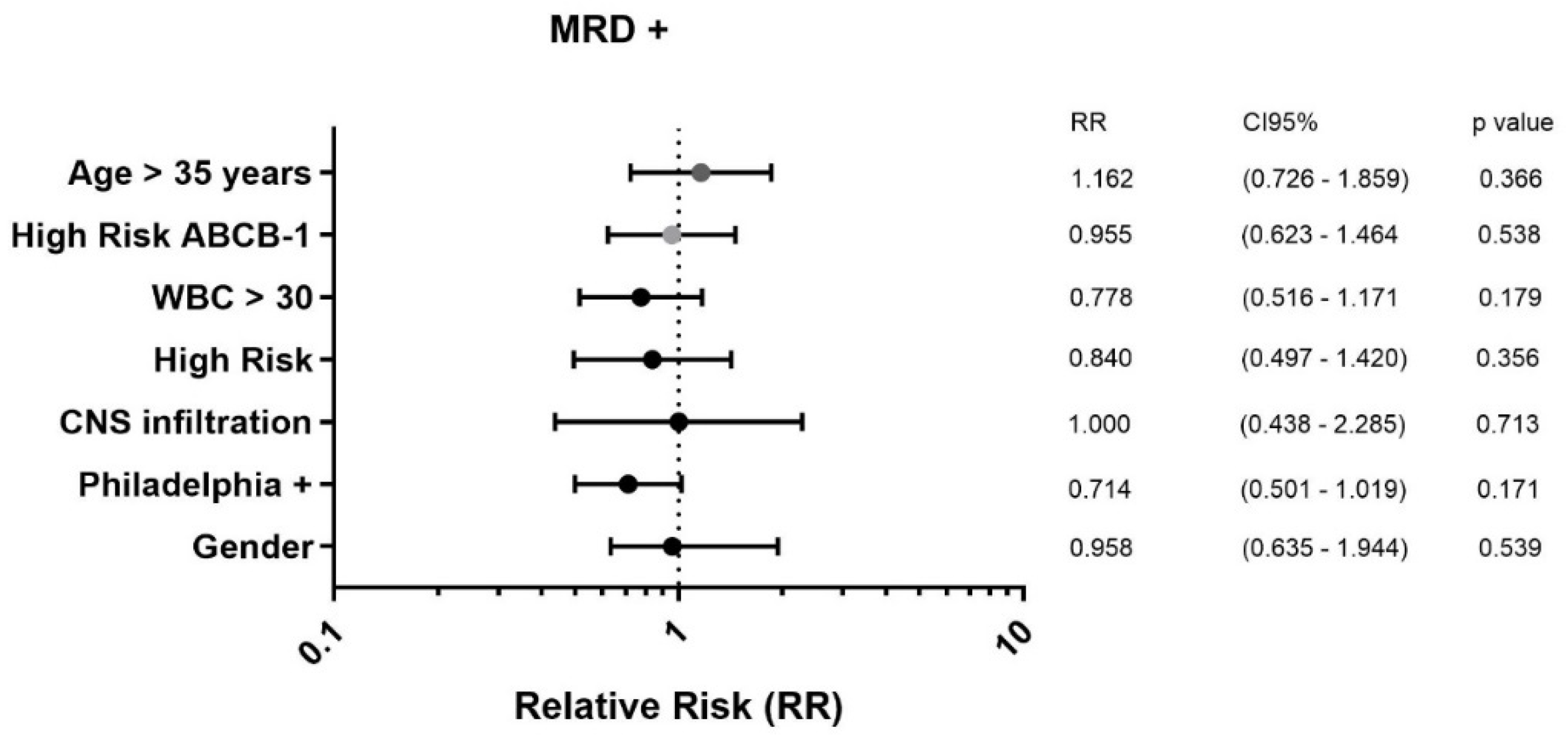
Figure 6.
Relative Risk of principal outcomes for relapse.
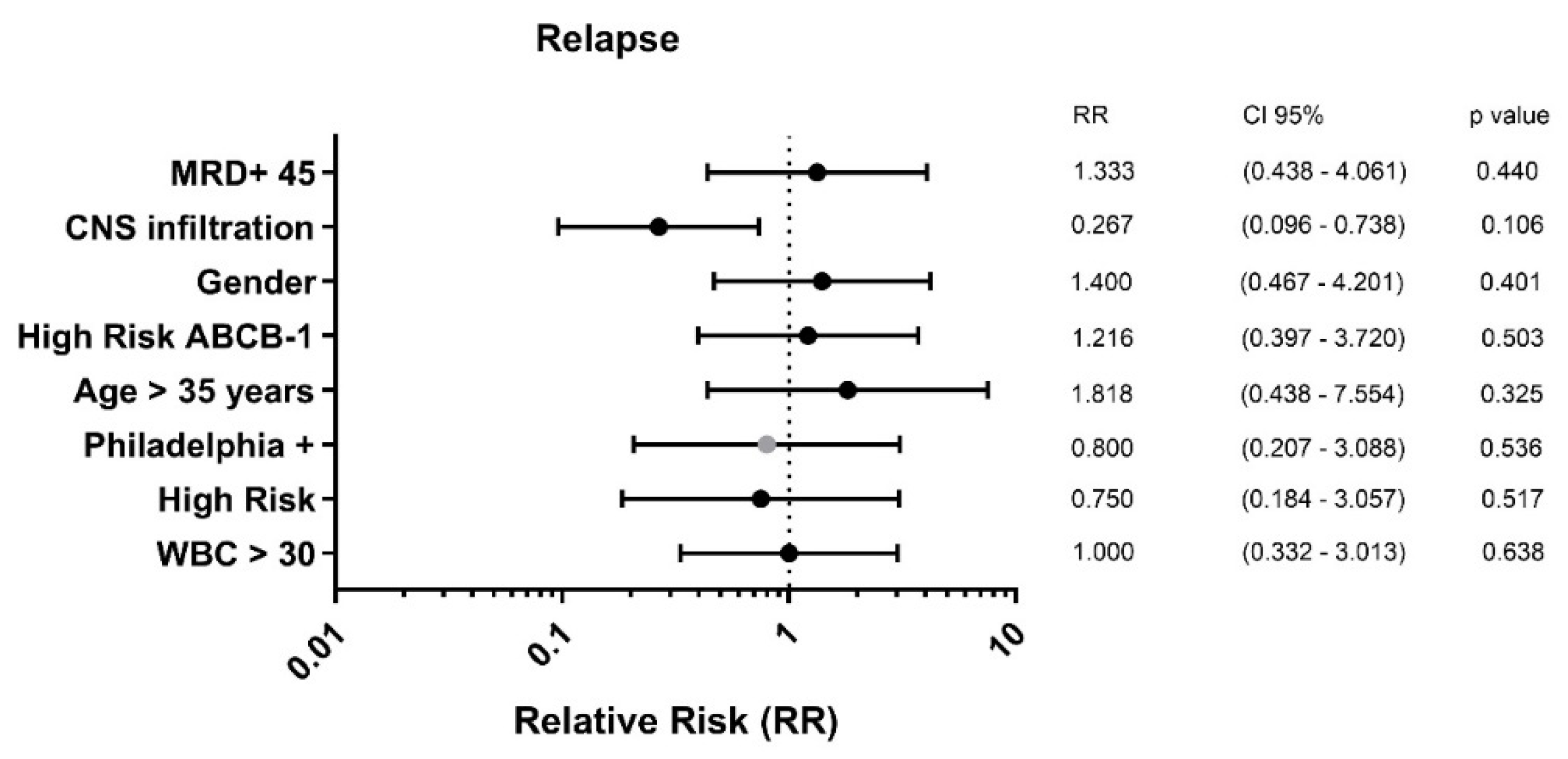

Table 1.
Demographic Characteristics of the study population.
| ABCB1 (No expression) n=34 |
ABCB1 (High expression) n=23 |
p-value | |
|---|---|---|---|
| Age (Years) | 29.50 (18.00 – 71.00) | 31.00 (18.00 – 57.00) | 0.913 |
| Gender (M:F) | 19 (55.9%) 15 (44.1%) |
11 (47.8%) 12 (52.2%) |
0.372 |
| WBC (x103) | 29.95 (0.20 – 348.00) | 24.00 (1.20 – 362.00) | 0.913 |
| Overall survival (days) | 351.50 (18.00 – 944.00) | 325.00 (12.00 – 854.00) | 0.913 |
| Disease-Free Survival (days) | 237.50 (18.00 – 820.00) | 300.00 (12.00 – 740.00 | 0.913 |
|
Philadelphia gene Absence Presence |
29 (85.3%) 5 (14.7%) |
19 (82.6%) 4 (17.4%) |
0.532 |
|
Immunophenotype Lymphocytes B Lymphocytes T |
33 (97.1%) 1 (2.9%) |
20 (87.0%) 3 (13.0%) |
0.175 |
|
CNS Negative Positive |
32 (94.1%) 2 (5.9%) |
22 (95.7%) 1 (4.3%) |
0.645 |
|
Risk Normal High |
7 (20.6%) 27 (79.4%) |
7 (30.4%) 16 (69.6%) |
0.295 |
|
MRD Negative Positive |
8 (23.5%) 26 (76.5%) |
8 (34.8%) 15 (65.2%) |
0.264 |
|
Survival Live Death |
19 (55.9%) 15 (44.1%) |
11 (47.8%) 12 (52.2%) |
0.372 |
|
Relapse Absence Presence |
27 (79.4%) 7 (20.6%) |
19 (82.6%) 4 (17.4%) |
0.522 |
|
WBC >30 Absence Presence |
17 (50.0%) 17 (50.0%) |
12 (52.2%) 11 (47.8%) |
0.543 |
|
Risk age < 35 years > 35 years |
21 (61.8%) 13 (38.25) |
15 (65.2%) 8 (34.8%) |
0.508 |
M: Male; F: Female; WBC: White Blood Cells Count; CNS: Central Nervous system invasion; MRD: Minimal Residual Disease. Values are expressed as median (ranges) for quantitative variables and absolute values (%) for qualitative variables. Wilcoxon Test was used to compare medians of quantitative non parametric variables for independent groups, and Chi2 was used for categorical variables. A p value <0.05 was considered as statistical significance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



