
Submitted:
08 November 2024
Posted:
08 November 2024
You are already at the latest version
Abstract
(1) Background: Literature to date has shown some contradictory findings regarding the associations between empathy and mental health. Thus, the Caring component of Positive Youth Development has been related to more mental health symptoms, while positive empathy seems to have a positive impact on psychological adjustment. The present study aimed to analyze the associations between Caring and positive empathy with youth depression and anxiety, as well as examining gender differences. (2) Methods: A cross-sectional study was carried out by administering an online self-report to a sample composed of 370 university students (67.2% women), aged 18-29 (M=21.29, SD = 3.61), enrolled across 10 universities in the Spanish region of Andalusia; (3) Results: Women reported higher levels of the caring dimension of PYD, more positive empathy, but more symptoms of depression and anxiety. Mediational analyses to explain the gender differences in mental health concluded that: a) women reported more depression and anxiety partly due to their higher scores in Caring, and b) despite women had more positive empathy than men, this mechanism was only protective against anxiety in the subsample of men; (4) Conclusions: The promotion of mental health in university context should include fostering adaptive empathetic skills.
Keywords:
caring
; empathy
; positive youth development
; depression
; anxiety
; gender
; emerging adults
; undergraduates
; mediation analyses
1. Introduction
The Positive Youth Development (PYD) model proposed a strength-based perspective of the transition to adulthood, in which positive outcomes appear when youth personal skills and contextual developmental assets are properly aligned [1,2]. A 5Cs model of PYD was presented by Lerner et al. [3], in which five thriving indicators, which are differentiated and expected to be related to better health and well-being in adolescent and youth samples [4,5,6,7]. These 5Cs are defined as: Confidence (an overall positive self-worth), Competence (positive self-efficacy in life domains such as academic or social), Connection (positive interpersonal relationships), Character (adequate internalization of the social rules and values), and Caring (feeling sympathy and empathy towards others). Evidence to date has determined that the 5Cs showed cross-lagged prospective associations with some positive outcomes across youth period. However, some paradoxical results have been observed concerning the dimension of Caring in PYD (as a thriving indicator) and some mental health results. In a longitudinal study with adolescents in the US, Geldhof et al. [8] pointed out a small positive correlation between Caring and depressive symptomatology. In this same line, Dvorsky et al. [9] reached the same conclusion with a sample of US undergraduates. They also observed positive associations between Caring, depression and emotional regulation difficulties.
Several studies have also confirmed these paradoxical findings in European samples. Thus, Holsen et al. [10] found, in Norwegian youth, that Caring was positively related with both anxiety and depressive symptoms. In Croatia, Novak et al. [11] found a protective role of PYD against adolescent mental distress, except for Caring, which was related to more depression, anxiety and stress. In this same line, Marin-Gutierrez et al. [12] demonstrated that Caring was positively correlated with perceived stress, while Confidence and Connection played a protective role in Chilean adolescents. In Slovenia, Pivec and Kozina [13] have reported that Caring was positive associated with anxiety and COVID-19 anxiety in a sample of adolescents. Some cross-national studies have also addressed this gap in literature. Kozina et al. [14] analyzed youth samples from Slovenia, Portugal and Spain, and showed that Connection and Confidence were protective factors against anxiety, while Caring presented a detrimental effect. In a study with samples from Spain and Croatia, Gomez-Baya et al. [15] explored the associations between the 5Cs of PYD and depression with data collected before COVID-19 pandemic. These authors concluded that more Confidence and more Connection were associated with less depressive symptoms, but more Caring was associated with more depressive symptoms. Finally, a study with undergraduates from Peru and Spain during the pandemic, conducted by Manrique-Millones et al. [16], showed negative effects by Competence, Confidence, Character and Connection on depressive symptoms, while Caring had a positive one in both samples. Other studies have reported the association between dispositional compassion and suicidal ideation [17] and with depressive symptoms in adolescent and youth samples [18].
Based on the preliminary findings in American samples, Geldhof et al. [19] argued about the importance of the interactions among the 5Cs. More than two decades ago, Schieman and Turner [20] found out that the association between empathy and distress was stronger among people who reported less education, lower self-esteem, and lower mastery. Thus, they posited that one component can sometimes be related to psychological maladjustment depending on the quality of the interactions between youth and their contexts. Those youth spending elevated and exhausting attention to others’ thoughts and feelings may have increased difficulties developing positive psychological adjustment. This kind of over-investment in others’ lives may lead to empathic stress when the boundaries between other people and themselves get blurred and they cannot cope with that situation. Thus, high scores in the Caring component of PYD may produce some exaggerated emotional hypersensitivity, instead of a way to provide useful prosocial and altruistic behavior. Adaptive help to others has been associated with positive mental health consequences [21]. Thus, some authors have pointed out the differential impact on mental health by empathy for positive and negative emotions. Andreychik and Migliaccio [22] concluded that empathizing with positive or negative emotions of others implied different patterns of social behavior and social emotion. In another study, Andreychik and Lewis [23] distinguished between positive and negative empathy examining the motivation to help others. They found that negative empathy is related to a motivation to help others to avoid negative emotions, contrary to positive empathy, which is associated with an other-oriented motivation to help others to approach positive emotions. Furthermore, Morelli et al. [24] reviewed the emerging study of positive empathy. They concluded that positive empathy has been associated with more prosocial behavior (i.e., spending on others, emotional support, and tangible assistance), well-being (i.e., positive affect and life satisfaction), and more social connection (i.e., closeness, trust and relationship satisfaction). Concerning the association with emotional problems, these authors argued that more evidence is still needed to more clearly understand how altered sensitivity to others’ positive emotions may contribute to clinical problems. Morrison et al. [25] concluded that individuals with social anxiety, compared to healthy controls, were less able to vicariously share others’ positive emotions. With regards to the link between positive empathy and prosocial behavior, Telle and Pfister [26] presented a model in which the perception of positive affect in others triggers vicarious positive emotion (positive empathy), which is associated with mood maintenance motive, which also triggers prosocial behavior, and in turn it causes genuine positive emotion.
Furthermore, several studies have found some gender differences in Caring, with women showing higher mean scores than men [27,28]. Conway et al. [29] found, in Ireland, higher scores in Caring among female adolescents, and Gomez-Baya et al. [30] found the same result in a sample of Spanish students from High school and university. Cross-cultural evidence has been documented concerning gender differences in caring morality, so that women showed more interpersonal sensitivity in Korea, China, Thailand and the USA [31]. Other studies have examined this tendency in gender differences along with its impact on related variables. In a 6-wave prospective study in the Netherlands, adolescent girls experienced an increase in prosocial behavior, what was predicted by higher scores in perspective taking and empathic concern [32]. Moreover, in US undergraduates, women were found to report more empathy as well as more emotional reactivity than men [33]. Rochat [34] indicated that sex and gender differences in the development of empathy throughout the lifespan are due to the joint interaction of social and neurobiological factors, including early socialization, brain's structural/functional variances, and genetics and hormonal factors. Furthermore, literature to date has well documented the emergence of gender differences in emotional problems since adolescence [35]. Gomez-Baya et al. [36] have shown that gender differences in anxiety may be partly due to the lower scores in positive identity and higher scores in positive values in women. Some psychosocial mediators have been proposed to explain gender differences in depression and anxiety across the life span [37], such as mastery, behavioral inhibition, rumination, and perceived interpersonal problems. In this line, stressful life events and emotional reactivity to these life events may explain gender differences in adolescents’ depression [38].
Given the mixed results regarding the Caring dimension in PYD and the consistent gender differences observed, further research is needed to deepen our understanding of empathy’s role in psychological wellbeing [19,39]. The present study aimed: a) to examine the gender differences in caring, positive empathy, depression and anxiety in Spanish emerging adults; b) to analyze the associations between caring and positive empathy with mental health outcomes; and c) to explore the mediational role of Caring and positive empathy in the gender differences in both depression and anxiety.
2. Materials and Methods
2.1. Participants and Data Collection Procedure
A cross-sectional study was carried out during Spring 2024, by administering an online self-report to a sample of undergraduates. The sample completed the questionnaire in around 30 minutes. Written consent was collected before participation and no reward was given. The study was performed following the principles of the Declaration of Helsinki and previously received the approval from the University of Huelva Ethic Board on January 10, 2019.
The participants were a sample of 370 university students (67.2% women, 31.4% men, and 1.4% non-binary), aged 18-29 (M=21.29, SD = 3.61), and enrolled at 10 universities in the Spanish region of Andalusia: University of Almeria, University of Cadiz, University of Cordoba, University of Granada, University of Huelva, University of Jaen, University of Malaga, University of Seville, University Pablo de Olavide (Seville), and Loyola University (Seville and Cordoba). Concerning habitat, most participants reported living in urban areas, such as cities over 300,000 inhabitants (38.4%) or in cities between 50,001-300,000 (31.1%). With regards to cohabitation, most of the students lived with their parents (49.5%) or flat mates (30.5%), and the 54.5% indicated that they did not have a couple. Around two thirds of the participants (65.6%) were not looking for a job now. Concerning the area of knowledge of the degree, 39.7% studied a degree in Law or Social Sciences, 29.6% studied Sciences/Engineering, 19.2% studied Arts and humanities, and 11.5% was enrolled in a degree of Health Sciences. Finally, regarding the academic year, half of the sample was enrolled in the first or second year, 42.6% in the 3rd one, and the 7.4% in the 4th or higher academic year.
2.2. Instrument
Caring dimension of Positive Youth Development. The Caring subscale included in the PYD short form created by Geldhof et al. [8] was administered. This overall questionnaire was adapted into Spanish by Gomez-Baya et al. [30] and demonstrated good factorial validity and excellent internal consistency. This subscale is composed of six items about sympathy and empathy for others, i.e., “When I see another person who is hurt or upset, I feel sorry for them” or “It bothers me when bad things happen to any person”. These items have a 5-point Likert-type scale which ranges from (1) “Not at all like me” to (5) “Very much like me”. Mean score was calculated and good internal consistency was observed (α = 0.79).
Positive empathy. The Dispositional Positive Empathy Scale, created by Sallquist et al. [40] and adapted to Spanish by Hess and Mesurado [41], was used. This scale is composed of seven items, e.g. “I feel happy for others who receive good news” or “I am happy when I see others succeed”. A 4-point Likert-type scale was presented, ranging from 1 = Never to 4 = Always. Notable internal consistency was detected (α = .84).
Depression. The Patient Health Questionnaire 9 (PHQ-9) [42,43] was administered to assess depressive symptoms. This questionnaire was introduced with the question “How often have you been bothered by the following over the past 2 weeks?” and presented nine items, representing depressive symptoms (e.g., “Little interest or pleasure in doing things” and “Feeling down, depressed, or hopeless”). The response options followed a 4-point Likert-type scale ranging from 0 = Not at all, to 3 = Nearly every day. Very good internal consistency was found (α = .84).
Anxiety. The Generalized Anxiety Disorder 7 (GAD-7) [44,45] was administered to assess anxiety symptoms. This questionnaire begins with the question “How often have you been bothered by the following over the past 2 weeks?” and described seven items, representing anxiety symptoms (e.g., “Feeling nervous, anxious or on edge” and “Not being able to stop or control worrying”). The response options followed a 4-point Likert-type scale ranging from 0 = Not at all, to 3 = Nearly every day. Excellent internal consistency was found (α = .91).
2.3. Data Analysis Design
First, descriptive statistics were presented for Caring, positive empathy, depression and anxiety, in the overall sample and by gender. T-tests were performed to examine gender differences in the study variables, and Cohen’s d was calculated. Second, Pearson zero-order bivariate correlations were conducted to examine the associations between variables in men and women subsamples. Third, two hierarchical regression analyses were separately conducted to explain depression and anxiety based on gender, age, caring and positive empathy. Standardized coefficients and R-squared were shown. These analyses were carried out with SPSS 21.0. Fourth, a multiple mediational model was tested to examine the mediation by caring and positive empathy in the effect by gender on both anxiety and depression. Indirect, direct and total effects were calculated. Standardized coefficients and confidence intervals were described in all the paths included. This analysis was tested with JASP 0.18.3.0.
3. Results
3.1. Gender Differences and Bivariate Correlations
Table 1 shows descriptive statistics in study variables in the overall sample and by gender. High scores were observed in both caring and positive empathy. Very high mean scores were also found in both depressive and anxiety symptoms, indicating mild depression and anxiety clinical levels, based on the cut off points of the respective instruments. Furthermore, significant gender differences in all the study variables were found, with higher mean scores in women. The greatest gender difference was observed in positive empathy, while the lowest one was found in depression. Concerning correlations, caring showed positive associations with depression and anxiety in women, and positive empathy had a negative association with anxiety in men. Positive correlations were observed between caring and positive empathy, and between depression and anxiety, in both women and men.
3.2. Regression and Mediational Analyses
Table 2 presents the results of two hierarchical regression analyses to explain symptoms of anxiety and depression based on demographics, positive empathy and Caring. The results indicated significant gender effects for both anxiety and depression. Caring had a positive effect on both mental health outcomes, while positive empathy had a negative effect only on anxiety. Higher explained variance was found concerning anxiety.
Table 3 described the results of the multiple mediation analysis of caring and positive empathy in the gender effect on both depression and anxiety. Figure 1 shows the standardized coefficients in the paths included in this mediational model. Results showed significant direct effects by gender on depression and anxiety after including the mediators. Moreover, significant indirect effects by gender through the mediator of caring were observed on both depression and anxiety. Thus, gender differences in both depression and anxiety were partly due to gender differences in caring. Higher scores in caring among women partly explained their higher scores in anxiety and depression. More caring was related to more symptoms of both depression and anxiety. Furthermore, positive empathy partially mediated the effect by gender on anxiety, but not on depression. Higher scores in positive empathy were protective against anxiety in men. Finally, positive covariances were observed between the mediators (i.e., caring and positive empathy) and between the outcomes (i.e., anxiety and depression). More explained variance was observed in anxiety, compared to depression.
4. Discussion
The present study had three aims. The first aim was to analyze the gender differences in caring, positive empathy, depression and anxiety in Spanish emerging adults. The results indicated that women presented more positive empathy, more caring, and more depressive and anxiety symptoms. These results are consistent with previous literature on gender differences in caring [29], empathy [34] and emotional distress [37]. The second aim was to calculate the associations between caring and positive empathy with depression and anxiety. The results indicated that more caring was related to more depression and anxiety in women, while more positive empathy was related to less anxiety in men. The relationship of caring with anxiety and depression in women is consistent with the works by Pivec and Kozina [13] and Manrique-Millones et al. [16]. The protective role of positive empathy is in line with the conclusions by Andreychik and Lewis [23] and Morelli et al. [24].
Finally, the third aim was to explore the mediational role of caring and positive empathy in the gender differences in both depression and anxiety. The results pointed out that: a) caring mediated gender differences in both depression and anxiety, while positive empathy mediated the gender differences in anxiety; b) higher caring was related to more depression and anxiety, while higher positive empathy was related to less anxiety. Women reported more depression and anxiety partly due to their higher scores in caring. Despite women had higher positive empathy than men, this mediator was only protective against anxiety in the men subsample. These results can be explained by the gendered socialization in which women are taught to be more expressive and sensitive, displaying more caring towards others [46], together with lower self-confidence, more rumination and a lower perception of their emotional skills [36,47,48]. Empathy can be protective for mental health in youth, as indicated Rieffe and De Rooji [49], but may increase emotional vulnerability when youth do not possess enough social support nor adequate emotional regulation skills [50]. Increased emotional reactivity in stressful life events may lead women to suffer more emotional problems when they do not possess adaptive coping styles [38]. In the case of empathy for others’ positive emotions, positive empathy has been associated with positive upward spirals characterized by more prosocial behavior, well-being and greater social connection. Thus, higher reactivity for others’ negative emotions in women may reduce the positive consequences derived from their higher level of positive empathy [51].
Some limitations should be acknowledged in these results. First, the cross-sectional study design limits the analysis to associations between variables, preventing any inference of causation. Longitudinal design is necessary to investigate the directionality of the relationships between empathy and mental health outcomes. Second, the use of self-report instruments introduces subjectivity, which may be affected by social desirability bias. Future research could provide evidence using objective measures and clinical diagnoses. Third, some variables should be controlled or included in the model to explain depression and anxiety. For example, emotion regulation strategies, neuroticism personality trait, resilience skills or perceived social support may have an important role in the empathy effect on stress generation. Fourth, a more comprehensive examination of empathy is recommended, separating cognitive and affective components [52], and other elements, such as interpersonal reactivity, perspective taking or empathic concern [53]. Fifth, future works should assess a representative sample of Spanish youth to generalize the conclusions. The present work assessed a convenient sample from 10 universities in Southern Spain.
Some implications for practice may be derived from the results of the present study. Interventions that promote adequate emotional regulation and coping styles to protect women from increased emotional reactivity in caring situations are specially needed to reduce their subsequent levels of anxiety and depression. As well, intervention to increase empathy in men in order to foster further contribution to others may be also necessary. PYD interventions should aim at promoting equal opportunities for male and female to develop in a healthy way [54]. The integration of PYD and empathy education programs may be recommended to jointly develop caring skills and well-being. Thus, empathy competency should be central in Higher Education curriculum [55], to train with evidence-based interventions the social and emotional skills needed for a healthy professional development. With undergraduate samples, some empathy education interventions were found effective in increasing empathy competency among medical students [56] and nursing students [57,58]. With an adolescent sample, a school-based social and emotional learning (SEL) program was found to be effective to activate social empathy in Ireland [59]. The practice of social and emotional skills, such as identifying emotions, perspective taking, problem solving, teamwork and goal setting, allows for building positive associations between empathy and PYD. From this SEL framework, Cullen et al. [60] argued the importance of faculty members’ instruction to provide these skills to their students, especially during the transition from High school to university. Also, counseling/well-being offices at universities may implement group sessions or workshops to work with the students [61]. The program Activate Empathy for Undergraduate College Students [62] was designed to teach empathy in students aged 18-25 with a 12-hour module (including topics such as the definition of empathy, conflict resolution, the psychology of empathy, listening skills, and mindfulness exercises) using Kolb’s model of experiential learning (i.e., including opportunities for abstract conceptualization, active experimentation, concrete experience, and reflective observation) [63]. This program underlined that the most effective components in this empathy education program were the ability to perceive typical emotions in a situation, the ability to respond appropriately to someone else’s emotions, the ability to understand emotions in an interaction, and the ability to separate one’s emotions from another’s emotions. Thus, this intervention showed an integration between empathy and emotional regulation skills to prevent distress in caring situations.
5. Conclusion
The present manuscript has provided some interesting contributions to the literature about empathy, mental health, and the examination of gender differences. First, this work showed that women reported more caring dimension of PYD, more positive empathy, but more symptoms of depression and anxiety. Second, the mediational analyses to explain the gender differences in mental health concluded that: a) women reported more depression and anxiety partly due to their higher scores in caring, and b) despite women had more positive empathy than men, this mechanism was only protective against anxiety in the subsample of men. These results underline the need to improve emotion regulation strategies to deal with stress while caring for others, and better social skills to build healthy social relationships. The promotion of mental health in the university context should integrate the development of empathic skills jointly with good opportunities to provide social contribution to the community.
Author Contributions
Conceptualization, D.G.-B., D.M.-M., E.L.-B., and A.J.G.; methodology, D.G.-B.; formal analysis, D.G.-B.; investigation, D.G.-B., D.M.-M., E.L.-B., and A.J.G.; data curation, D.G.-B.; writing—original draft preparation, D.G.-B., D.M.-M., E.L.-B., and A.J.G.; writing—review and editing, D.G.-B., D.M.-M., E.L.-B., and A.J.G.; supervision, D.M.-M. and A.J.G.; project administration, D.G.-B.; funding acquisition, D.G.-B. All authors have read and agreed to the published version of the manuscript.
Funding
This research and the APC were funded by Excellence Project of the Consejeria de Universidad, Investigacion e Innovacion of Junta de Andalucia (Spain), entitled Positive Youth Development in Andalusian University Students: Longitudinal Analysis of Gender Differences in Well-Being Trajectories, Health-Related Lifestyles and Social and Environmental Contribution, grant number PROYEXCEL_00303, awarded to D.G.-B.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of University of Huelva (protocol code UHU-1259711 and date of approval: 10 January 2019) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lewin-Bizan, S.; Bowers, E. P.; Lerner, R. M. One good thing leads to another: Cascades of positive youth development among American adolescents. Development and psychopathology 2010, 22(4), 759-770. [CrossRef]
- Dimitrova, R., & Wiium, N. Handbook of positive youth development: Advancing the next generation of research, policy and practice in global contexts (pp. 3-16). Springer International Publishing, 2021.
- Lerner, R. M.; Almerigi, J. B.; Theokas, C.; Lerner, J. V. Positive youth development a view of the issues. The journal of early adolescence 2005, 25(1), 10-16. [CrossRef]
- Bowers, E. P.; Li, Y.; Kiely, M. K.; Brittian, A.; Lerner, J. V.; Lerner, R. M. The five Cs model of positive youth development: A longitudinal analysis of confirmatory factor structure and measurement invariance. Journal of youth and adolescence 2010, 39, 720-735. [CrossRef]
- Domínguez Espinosa, A. D. C.; Wiium, N.; Jackman, D.; Ferrer-Wreder, L. Healthy lifestyle behaviors and the 5Cs of positive youth development in Mexico. Handbook of Positive Youth Development: Advancing Research, Policy, and Practice in Global Contexts 2021, 109-121.
- Gomez-Baya, D.; Gaspar de Matos, M.; Wiium, N. Positive youth development and subjective happiness: examining the mediating role of gratitude and optimism in Spanish emerging adults. Handbook of positive youth development: Advancing research, policy, and practice in global contexts 2021, 187-202.
- Milot Travers, A. S.; Mahalik, J. R. Positive youth development as a protective factor for adolescents at risk for depression and alcohol use. Applied Developmental Science 2021, 25(4), 322-331. [CrossRef]
- Geldhof, G. J.; Bowers, E. P.; Mueller, M. K.; Napolitano, C. M.; Callina, K. S.; Lerner, R. M. Longitudinal analysis of a very short measure of positive youth development. Journal of Youth and Adolescence 2014, 43, 933-949. [CrossRef]
- Dvorsky, M. R.; Kofler, M. J.; Burns, G. L.; Luebbe, A. M.; Garner, A. A.; Jarrett, M. A.; Becker, S. P. Factor structure and criterion validity of the five Cs model of positive youth development in a multi-university sample of college students. Journal of youth and adolescence 2019, 48, 537-553. [CrossRef]
- Holsen, I.; Geldhof, J.; Larsen, T.; Aardal, E. The five Cs of positive youth development in Norway: Assessment and associations with positive and negative outcomes. International Journal of Behavioral Development 2017, 41(5), 559-569.
- Novak, M.; Šutić, L.; Gačal, H.; Roviš, D.; Mihić, J.; Maglica, T. Structural model of 5Cs of positive youth development in Croatia: relations with mental distress and mental well-being. International journal of adolescence and youth 2023, 28(1), 2227253.
- Marín-Gutiérrez, M.; Caqueo-Urízar, A.; Castillo-Francino, J.; Escobar-Soler, C. The 5Cs of positive youth development: their impact on symptoms of depression, anxiety, stress, and emotional distress in Chilean adolescents. BMC psychology 2024, 12(1), 372.
- Pivec, T.; Kozina, A. Anxiety and COVID-19 anxiety in positive youth development: A latent profile analysis study. Journal of Youth and Adolescence 2023, 52(11), 2328-2343.
- Kozina, A.; Gomez-Baya, D.; Gaspar de Matos, M.; Tome, G.; Wiium, N. The association between the 5Cs and anxiety—insights from three countries: Portugal, Slovenia, and Spain. Frontiers in psychology 2021, 12, 668049.
- Gomez-Baya, D.; Babić Čikeš, A.; Hirnstein, M.; Kurtović, A.; Vrdoljak, G.; Wiium, N. Positive youth development and depression: An examination of gender differences in Croatia and Spain. Frontiers in psychology 2022, 12, 689354. [CrossRef]
- Manrique-Millones, D.; Gómez-Baya, D.; Wiium, N. The importance of the 5Cs of positive youth development to depressive symptoms: A cross-sectional study with university students from Peru and Spain. Behavioral Sciences 2023, 13(3), 280. [CrossRef]
- Jonsson, E.; Dennhag, I. Compassion in three perspectives: Associations with depression and suicidal ideation in a clinical adolescent sample. Scandinavian Journal of Child and Adolescent Psychiatry and Psychology 2023, 11(1), 120-127. [CrossRef]
- Saarinen, A.; Keltikangas-Järvinen, L.; Cloninger, C. R.; Veijola, J.; Elovainio, M.; Lehtimäki, T.; ... Hintsanen, M. The relationship of dispositional compassion for others with depressive symptoms over a 15-year prospective follow-up. Journal of Affective Disorders 2019, 250, 354-362. [CrossRef]
- Geldhof, G. J.; Larsen, T.; Urke, H.; Holsen, I.; Lewis, H.; Tyler, C. P. Indicators of positive youth development can be maladaptive: The example case of caring. Journal of Adolescence 2019, 71, 1-9.
- Schieman, S.; Turner, H. A. " When feeling other people's pain hurts": The influence of psychosocial resources on the association between self-reported empathy and depressive symptoms. Social Psychology Quarterly 2001, 376-389.
- Memmott-Elison, M. K.; Holmgren, H. G.; Padilla-Walker, L. M.; Hawkins, A. J. Associations between prosocial behavior, externalizing behaviors, and internalizing symptoms during adolescence: A meta-analysis. Journal of adolescence 2020, 80, 98-114.
- Andreychik, M. R.; Migliaccio, N. Empathizing with others’ pain versus empathizing with others’ joy: Examining the separability of positive and negative empathy and their relation to different types of social behaviors and social emotions. Basic and Applied Social Psychology 2015, 37(5), 274-291. [CrossRef]
- Andreychik, M. R.; Lewis, E. Will you help me to suffer less? How about to feel more joy? Positive and negative empathy are associated with different other-oriented motivations. Personality and Individual Differences 2017, 105, 139-149. [CrossRef]
- Morelli, S. A.; Lieberman, M. D.; Zaki, J. The emerging study of positive empathy. Social and Personality Psychology Compass 2015, 9(2), 57-68.
- Morrison, A. S.; Mateen, M. A.; Brozovich, F. A.; Zaki, J.; Goldin, P. R.; Heimberg, R. G.; Gross, J. J. Empathy for positive and negative emotions in social anxiety disorder. Behaviour research and therapy 2016, 87, 232-242. [CrossRef]
- Telle, N. T.; Pfister, H. R. Positive empathy and prosocial behavior: A neglected link. Emotion review 2016, 8(2), 154-163. [CrossRef]
- Tomé, G.; Gaspar de Matos, M.; Reis, M.; Gomez-Baya, D.; Coelhoso, F.; Wiium, N. Positive youth development and wellbeing: gender differences. Frontiers in Psychology 2021, 12, 641647.
- Wiium, N.; Wreder, L. F.; Chen, B. B.; Dimitrova, R. Gender and positive youth development. Zeitschrift für Psychologie 2019. [CrossRef]
- Conway, R. J.; Heary, C.; Hogan, M. J. An evaluation of the measurement properties of the five Cs model of positive youth development. Frontiers in psychology 2015, 6, 1941.
- Gomez-Baya, D.; Reis, M.; Gaspar de Matos, M. Positive youth development, thriving and social engagement: An analysis of gender differences in Spanish youth. Scandinavian journal of psychology 2019, 60(6), 559-568. [CrossRef]
- Stimpson, D.; Jensen, L.; Neff, W. Cross-cultural gender differences in preference for a caring morality. The Journal of Social Psychology 1992, 132(3), 317-322. [CrossRef]
- Van der Graaff, J.; Carlo, G.; Crocetti, E.; Koot, H. M.; Branje, S. Prosocial behavior in adolescence: Gender differences in development and links with empathy. Journal of youth and adolescence 2018, 47(5), 1086-1099. [CrossRef]
- Rueckert, L.; Branch, B.; Doan, T. Are gender differences in empathy due to differences in emotional reactivity? Psychology 2011, 2(6), 574.
- Rochat, M. J. Sex and gender differences in the development of empathy. Journal of neuroscience research 2023, 101(5), 718-729.
- Hankin, B. L.; Abramson, L. Y.; Moffitt, T. E.; Silva, P. A.; McGee, R.; Angell, K. E. Development of depression from preadolescence to young adulthood: emerging gender differences in a 10-year longitudinal study. Journal of abnormal psychology 1998, 107(1), 128.
- Gomez-Baya, D.; Salinas-Perez, J. A.; Sanchez-Lopez, A.; Paino-Quesada, S.; Mendoza-Berjano, R. The role of developmental assets in gender differences in anxiety in Spanish youth. Frontiers in Psychiatry 2022, 13, 810326. [CrossRef]
- Leach, L. S.; Christensen, H.; Mackinnon, A. J.; Windsor, T. D.; Butterworth, P. Gender differences in depression and anxiety across the adult lifespan: the role of psychosocial mediators. Social psychiatry and psychiatric epidemiology 2008, 43, 983-998. [CrossRef]
- Charbonneau, A. M.; Mezulis, A. H.; Hyde, J. S. Stress and emotional reactivity as explanations for gender differences in adolescents’ depressive symptoms. Journal of youth and adolescence 2009, 38, 1050-1058. [CrossRef]
- Yan, Z.; Zeng, X.; Su, J.; Zhang, X. The dark side of empathy: Meta-analysis evidence of the relationship between empathy and depression. PsyCh journal 2021, 10(5), 794-804.
- Sallquist, J.; Eisenberg, N.; Spinrad, T. L.; Eggum, N. D.; Gaertner, B. M. Assessment of preschoolers' positive empathy: concurrent and longitudinal relations with positive emotion, social competence, and sympathy. Journal of Positive Psychology 2009, 4(3), 223- 233.
- Hess, C.; Mesurado, B. Adaptación y validación de la Escala Disposicional de Empatía Positiva a población adolescente argentina. Acta Colombiana de Psicología 2023, 26(1), 27-44.
- Kroenke, K.; Spitzer, R. L.; Williams, J. B. The PHQ-9: validity of a brief depression severity measure. Journal of general internal medicine 2001, 16(9), 606-613.
- Muñoz-Navarro, R.; Cano-Vindel, A.; Medrano, L. A.; Schmitz, F.; Ruiz-Rodríguez, P.; Abellán-Maeso, C.; ... Hermosilla-Pasamar, A. M. Utility of the PHQ-9 to identify major depressive disorder in adult patients in Spanish primary care centres. BMC psychiatry 2017, 17, 1-9.
- Spitzer, R. L.; Kroenke, K.; Williams, J. B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of internal medicine 2006, 166(10), 1092-1097.
- García-Campayo, J.; Zamorano, E.; Ruiz, M. A.; Pardo, A.; Pérez-Páramo, M.; López-Gómez, V.; …Rejas, J. Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health and quality of life outcomes 2010, 8, 1-11.
- Silke, C.; Brady, B.; Boylan, C.; Dolan, P. Factors influencing the development of empathy and pro-social behaviour among adolescents: A systematic review. Children and Youth Services Review 2018, 94, 421-436. [CrossRef]
- Gomez-Baya, D.; Mendoza, R.; Paino, S.; Gillham, J. E. A two-year longitudinal study of gender differences in responses to positive affect and depressive symptoms during middle adolescence. Journal of Adolescence 2017, 56, 11-23. [CrossRef]
- Gómez-Baya, D.; Mendoza, R.; Paino, S.; Gaspar de Matos, M. Perceived emotional intelligence as a predictor of depressive symptoms during mid-adolescence: A two-year longitudinal study on gender differences. Personality and individual differences 2017, 104, 303-312. [CrossRef]
- Rieffe, C.; De Rooij, M. The longitudinal relationship between emotion awareness and internalising symptoms during late childhood. European child & adolescent psychiatry 2012, 21, 349-356.
- Zahn-Waxler, C.; Van Hulle, C. Empathy, guilt, and depression. Pathological altruism 2011, 321-344.
- Andreychik, M. R. Feeling your joy helps me to bear feeling your pain: Examining associations between empathy for others' positive versus negative emotions and burnout. Personality and Individual Differences 2019, 137, 147-156.
- Jolliffe, D.; Farrington, D. P. Development and validation of the Basic Empathy Scale. Journal of adolescence 2006, 29(4), 589-611.
- Stosic, M. D.; Fultz, A. A.; Brown, J. A.; Bernieri, F. J. What is your empathy scale not measuring? The convergent, discriminant, and predictive validity of five empathy scales. The Journal of Social Psychology 2022, 162(1), 7-25. [CrossRef]
- Gaspar de Matos, M.; Santos, T.; Reis, M.; Gómez-Baya, D.; Marques, A. Positive youth development in Portugal: a tool towards gender equity? ARC Journal of Pediatrics 2018, 4(1), 25-35.
- Van Winkle, L. J.; Schwartz, B. D.; Michels, N. A model to promote public health by adding evidence-based, empathy-enhancing programs to all undergraduate health-care curricula. Frontiers in Public Health 2017, 5, 339. [CrossRef]
- Buffel du Vaure, C.; Lemogne, C.; Bunge, L.; Catu-Pinault, A.; Hoertel, N.; Ghasarossian, C., ... Jaury, P. Promoting empathy among medical students: A two-site randomized controlled study. Journal of psychosomatic research 2017, 103, 102-107.
- Levett-Jones, T.; Cant, R.; Lapkin, S. A systematic review of the effectiveness of empathy education for undergraduate nursing students. Nurse education today 2019, 75, 80-94.
- Yang, C.; Zhu, Y. L.; Xia, B. Y.; Li, Y. W.; Zhang, J. The effect of structured empathy education on empathy competency of undergraduate nursing interns: A quasi-experimental study. Nurse education today 2020, 85, 104296. [CrossRef]
- Silke, C.; Davitt, E.; Flynn, N.; Shaw, A.; Brady, B.; Murray, C.; Dolan, P. Activating Social Empathy: An evaluation of a school-based social and emotional learning programme. Social and Emotional Learning: Research, Practice, and Policy 2024, 3, 100021.
- Cullen, J.; Bloemker, G.; Wyatt, J.; Walsh, M. Teaching a social and emotional learning curriculum: Transformative learning through the parallel process. International Journal of Higher Education 2017, 6(6), 163-169.
- Goodwin, J., Behan, L., Kelly, P., McCarthy, K., & Horgan, A. Help-seeking behaviors and mental well-being of first year undergraduate university students. Psychiatry research 2016, 246, 129-135. [CrossRef]
- Berardi, M. K. What are the most effective components of empathy education for undergraduate students to increase their empathy levels? The Pennsylvania State University, 2020.
- Kolb, D. A.; Boyatzis, R. E.; Mainemelis, C. Experiential learning theory: Previous research and new directions. In Perspectives on thinking, learning, and cognitive styles (pp. 227-247). Routledge, 2014.
Figure 1.
Multiple mediation model with standardized coefficients.
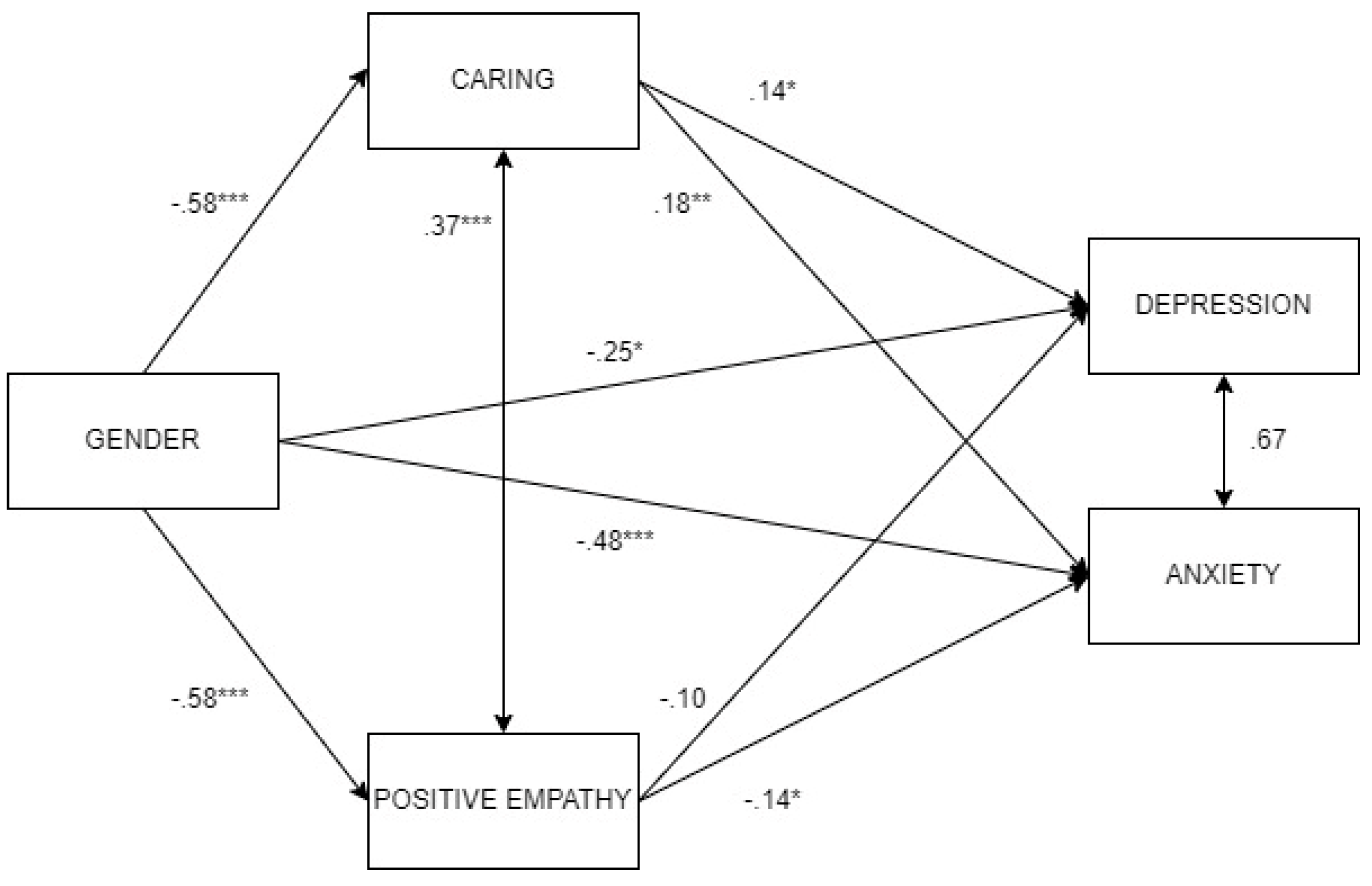

Table 1.
Descriptive statistics, gender differences and bivariate correlations.
| Overall M(SD) |
Women M(SD) | Men M(SD) |
t-test | Cohen’s d | 1 | 2 | 3 | 4 | |
| 1.Positive Empathy | 3.44(.50) | 3.54(.47) | 3.25(.50) | 5.38*** | .697 | (.84) | .35*** | -.09 | -.25** |
| 2.Caring | 4.17(.59) | 4.28(.53) | 3.94(.65) | 5.29*** | .596 | .43*** | (.79) | -.01 | -.01 |
| 3.Depression | 9.24(5.41) | 9.69(5.56) | 8.19(4.88) | 2.48* | .280 | -.02 | .16* | (.84) | .73*** |
| 4.Anxiety | 8.48(5.53) | 9.34(5.65) | 6.57(4.84) | 4.54*** | .512 | .01 | .19** | .71*** | (.91) |
Note. *** p <.001, ** p<.01, * p<.05. In the correlations section, women’s results are presented below the diagonal, and men’s results, over the diagonal.
Table 2.
Hierarchical regression analyses.
| Anxiety symptoms1 | Depressive symptoms2 | |||||
| F / R2 | β | t | F / R2 | β | t | |
| 7.66*** / .080 | 3.28* / .036 | |||||
| Gender | -.21*** | -3.92 | -.11* | -1.96 | ||
| Age | .05 | .97 | .06 | 1.19 | ||
| Caring | .17** | 2.90 | .14* | 2.29 | ||
| Positive empathy | -.12* | -2.02 | -.09 | -1.54 | ||
Note. *** p <.001, ** p<.01, * p<.05. 1 DW = 1.92; 2 DW = 2.00.
Table 3.
Multiple mediation model.
| Est | SE | Z | p | LLCI | ULCI | |
| Direct effects | ||||||
| G->Dep | -.25 | .12 | -2.11 | .035 | -.48 | -.02 |
| G->Anx | -.48 | .11 | -4.18 | <.001 | -.70 | -.25 |
| Indirect effects | ||||||
| G-> Ca->Dep | -.08 | .04 | -2.23 | .026 | -.16 | -.01 |
| G->Em->Dep | .06 | .04 | 1.61 | .109 | -.01 | .13 |
| G->Ca->Anx | -.10 | .04 | -2.72 | .006 | -.18 | -.03 |
| G-> Em->Anx | .08 | .04 | 2.22 | .026 | .01 | .15 |
| Total effects | ||||||
| G->Dep | -.27 | .11 | -2.44 | .015 | -.49 | -.05 |
| G->Anx | -.50 | .11 | -4.55 | <.001 | -.71 | -.28 |
| Residual covariances | ||||||
| Ca<->Em | .37 | .05 | 7.03 | <.001 | .27 | .47 |
| Dep<->Anx | .67 | .06 | 11.04 | <.001 | .55 | .79 |
| Path coefficients | ||||||
| Ca->Dep | .14 | .06 | 2.45 | .014 | .03 | .26 |
| Em->Dep | -.10 | .06 | -1.68 | .093 | -.21 | .02 |
| G->Dep | -.25 | .12 | -2.11 | .035 | -.48 | -.02 |
| Ca->Anx | .18 | .06 | 3.17 | .002 | .07 | .29 |
| Em->Anx | -.14 | .06 | -2.44 | .015 | -.25 | -.03 |
| G->Anx | -.48 | .11 | -4.18 | <.001 | -.70 | -.25 |
| G-> Ca | -.58 | .11 | -5.32 | <.001 | -.79 | -.36 |
| G->Em | -.58 | .11 | -5.36 | <.001 | -.79 | -.37 |
Note. Dep = Depression, Anx = Anxiety, Ca = Caring, Em = Positive empathy. R2 Dep = .034, R2 Anx = .084, R2 Ca = .072, R2 Em = .074.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



