Submitted:
05 November 2024
Posted:
06 November 2024
You are already at the latest version
Abstract
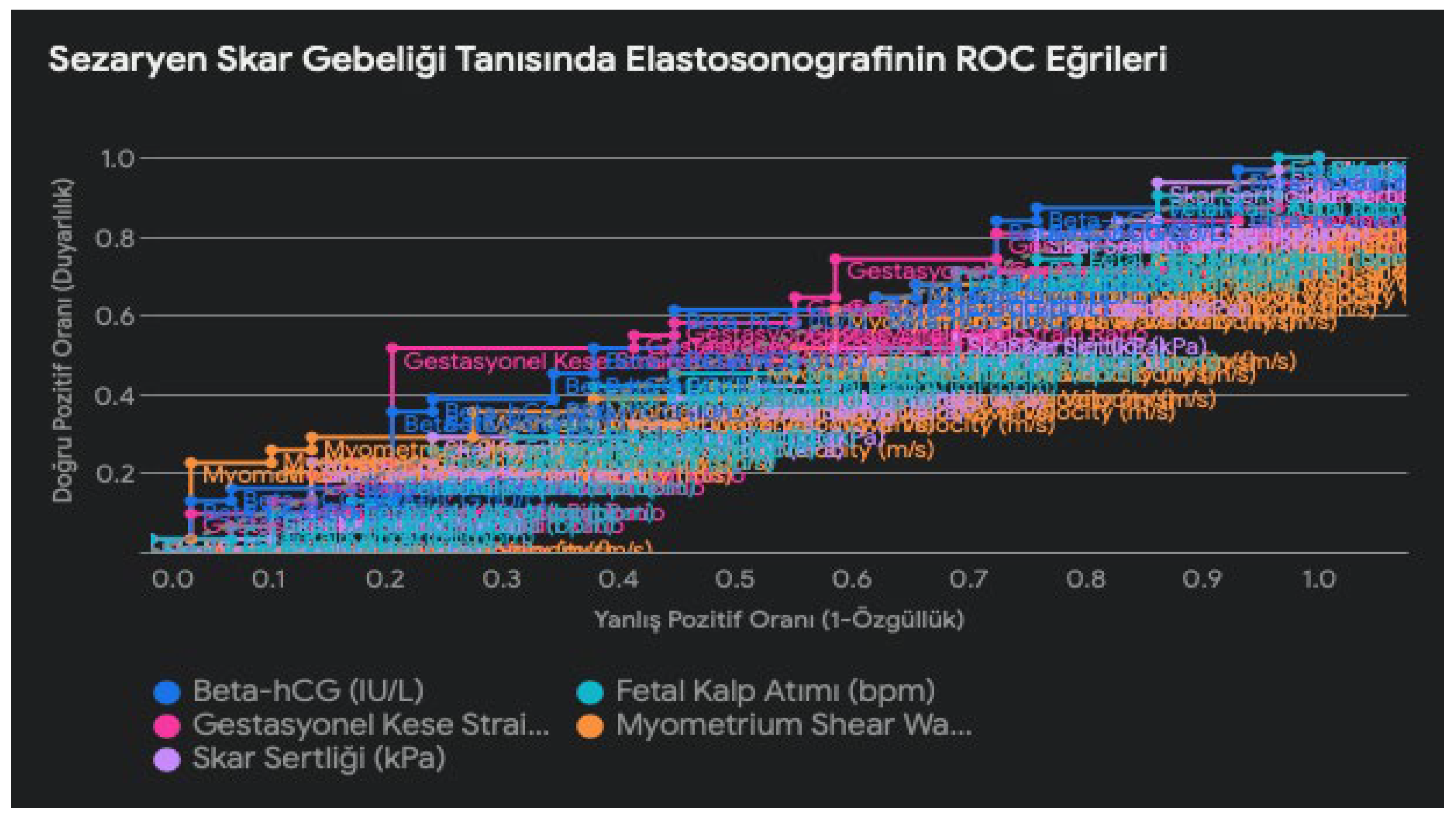
INTRODUCTION: The objective of this study is to assess the diagnostic accuracy, reliability, and efficacy of elastosonography in the diagnosis of cesarean scar pregnancy. To this end, the present study will compare the elastosonography findings in patients with cesarean scar pregnancy with those obtained through definitive diagnostic methods and investigate the diagnostic potential of elastosonography. MATERIAL AND METHOD: This prospective cohort study was conducted at Mardin Training and Research Hospital between October 2023 and January 2024. Patients with a cesarean scar pregnancy between six and twelve weeks of gestation were evaluated. The stiffness and elasticity of the scar tissue were assessed using elastosonography, and the diagnostic accuracy of this method was evaluated by comparing the results with those obtained through definitive diagnostic procedures. RESULTS: In this study, the demographic and clinical characteristics of 61 patients with cesarean scar pregnancy (CSP) were analyzed. The mean age of the patients was 32 years, the mean gestational age was 8.4 weeks, the mean BMI was 27.2, the mean parity was 1.9, and the mean number of previous cesarean sections was 1.3. While the elasticity of the scar tissue decreased with increasing gestational week, no significant correlation was found between age, BMI, parity, and number of previous cesarean sections and elastosonography findings. The gestational sac strain ratio, myometrial shear wave velocity, and scar stiffness, as measured by elastosonography, were found to be significant in the diagnosis of CSP. Conversely, the beta-hCG and fetal heart rate parameters did not contribute significantly to the diagnosis. CONCLUSION: In conclusion, the results of this study indicate that elastosonography has the potential to serve as a diagnostic tool for the identification of pregnancies in cases of cesarean section scar. The findings indicate that elastosonographic parameters, including the gestational sac tension ratio, myometrium shear wave velocity, and scar stiffness, may prove useful in diagnosing pregnancy in a cesarean scar. Further research is required to ascertain the full clinical utility of this technique. However, this study provides valuable information on the diagnostic accuracy and reliability of elastosonography in the evaluation of pregnancy in a cesarean scar.
Keywords:
Introduction
Material Ve Method
Study Design
Patient Selection
Inclusion Criteria
- Patients with a history of at least one previous cesarean section.
- Patients between 6-12 weeks of gestation.
- Patients with CSP findings on transvaginal ultrasonography (empty uterine cavity, closed internal os, gestational sac located between myometrium and bladder).
- Patients who can give written informed consent.
Exclusion Criteria
- Patients with a gestational week less than six or greater than 12.
- Patients who do not show signs of CSP on transvaginal ultrasonography.
- Patients with conditions that preclude elastosonography (e.g., extreme obesity, infection at the scar site).
- Patients who refused to participate in the study or were unable to give written informed consent.
- Patients lost to follow-up during the study.
- Patients with pregnancy complications (e.g., bleeding, uterine rupture).
- Patients with other serious health conditions (e.g., heart disease, renal failure).
Data Collection
Elastosonography
Outcome Measures
- The primary outcome measure was the diagnostic accuracy of elastosonography in the diagnosis of CSP.
- Secondary outcome measures were the relationship between strain rates measured by elastosonography and demographic characteristics and the variation of strain rates with gestational week.
Statistical Analysis
Results
Discussion
Looking into the Future: Artificial Intelligence and CSP Diagnosis
Limitations of the Study
References
- Timor-Tritsch, I.E.; Monteagudo, A.; Santos, R.; Tsymbal, T.; Pineda, G.; Arslan, A.A. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. Am. J. Obstet. Gynecol. 2012, 207, 44.e1–44.e13. [Google Scholar] [CrossRef] [PubMed]
- Rotas, M.A.; Haberman, S.; Levgur, M. Cesarean Scar Ectopic Pregnancies. Obstet. Gynecol. 2006, 107, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Women’s and Children’s Health. Caesarean section (NICE clinical guideliine 132). Royal College of Obstetricians and Gynaecologists (RCOG) Press: London, UK, 2011; 180–195.
- Vikhareva Osser, O.; Valentin, L. Clinical importance of appearance of cesarean hysterotomy scar at transvaginal ultrasonography in nonpregnant women. Obstet Gynecol. 2011, 117, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Timor-Tritsch IE, Monteagudo A, Cal`ı G, D’Antonio F, Agten AK. Cesarean Scar Pregnancy: Patient Counseling and Management. Obstet Gynecol Clin North Am 2019, 46, 813–828.
- Kaelin Agten A, Cali G, Monteagudo A, Oviedo J, Ramos J, Timor-Tritsch I. The clinical outcome of cesarean scar pregnancies implanted ‘‘on the scar’’ versus ‘‘in the niche’’. Am J Obstet Gynecol 2017; 216: 510.e1–6.
- Jurkovic D, Hillaby K, Woelfer B, Lawrence A, Salim R, Elson CJ. First trimester diagnosis and management of pregnancies implanted into the lower uterine segment Cesarean section scar. Ultrasound Obstet Gynecol. 2003; 21, 220–227.
- Timor-Tritsch, I.E.; Monteagudo, A.; Calì, G.; D’antonio, F.; Agten, A.K. Cesarean Scar Pregnancy. Obstet. Gynecol. Clin. North Am. 2019, 46, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Pegu, B.; Thiagaraju, C.; Nayak, D.; Subbaiah, M. Placenta accreta spectrum-a catastrophic situation in obstetrics. Obstet. Gynecol. Sci. 2021, 64, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Stănculescu, R.V.; Brătilă, E.; Socolov, D.G.; Russu, M.C.; Bauşic, V.; Chirculescu, R.; Coroleucă, C.A.; Pristavu, A.I.; Dragomir, R.E.; Papuc, P.; et al. Update on placenta accreta spectrum disorders by considering epidemiological factors, ultrasound diagnosis and pathological exam – literature review and authors’ experience. Romanian J. Morphol. Embryol. 2022, 63, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.S.-Y.; Chan, C.-P. The sonographic appearance and obstetric management of placenta accreta. Int. J. Women's Heal. 2012, 4, 587–594. [Google Scholar] [CrossRef] [PubMed]
- di Pasquo, E.; Kiener, A.J.O.; DallAsta, A.; Commare, A.; Angeli, L.; Frusca, T.; Ghi, T. Evaluation of the uterine scar stiffness in women with previous Cesarean section by ultrasound elastography: A cohort study. Clin. Imaging 2020, 64, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Cimsit, C.; Yoldemir, T.; Akpinar, I.N. Shear Wave Elastography in Placental Dysfunction. J. Ultrasound Med. 2015, 34, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Yang, M.; Wu, Q. Application of ultrasonography in the diagnosis and treatment of cesarean scar pregnancy. Clin. Chim. Acta 2018, 486, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Seliger, G.; Chaoui, K.; Lautenschläger, C.; Jenderka, K.-V.; Kunze, C.; Hiller, G.G.R.; Tchirikov, M. Ultrasound elastography of the lower uterine segment in women with a previous cesarean section: Comparison of in-/ex-vivo elastography versus tensile-stress-strain-rupture analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 225, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Varma, T.R. The value of ultrasonic B-scanning in diagnosis when bleeding is present in early pregnancy. Am. J. Obstet. Gynecol. 1972, 114, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Rizk, B.R.M.B.; Puscheck, E.E.; Abbasy, A.; Abuzeid, M.I.; Abuzeid, O.M.; Allahbadia, G.N.; Arora, S.; Awonuga, A.O.; Azmy, O.M.; Badawy, S.Z.A.; et al. Ultrasound diagnosis of cesarean scar ectopic pregnancy; Cambridge University Press (CUP): Cambridge, United Kingdom, 2014; pp. 172–176. [Google Scholar]
- Gonzalez, N.; Tulandi, T. Cesarean Scar Pregnancy: A Systematic Review. J. Minim. Invasive Gynecol. 2017, 24, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Liu, J.; Jing, Z.; Lin, L.; Li, X. Comparison of diagnostic accuracy of three-dimensional transvaginal ultrasound and magnetic resonance imaging in the diagnosis of scar pregnancy. Pak. J. Med Sci. 2022, 38, 1743–1747. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Ding, R.; Peng, L.; Liu, H.; Zhu, Y. Diagnostic performance of magnetic resonance imaging and ultrasonography on the detection of cesarean scar pregnancy. Medicine 2021, 100, e27532. [Google Scholar] [CrossRef] [PubMed]
- Alamo, L.; Vial, Y.; Denys, A.; Andreisek, G.; Meuwly, J.-Y.; Schmidt, S. MRI findings of complications related to previous uterine scars. Eur. J. Radiol. Open 2018, 5, 6–15. [Google Scholar] [CrossRef] [PubMed]

| n | Mean±SD | Min-Max (Median) | p | |
|---|---|---|---|---|
| Age (year) | 61 | 31.8 ± 5.1 | 30 (22-45) | > 0.05 |
| Gestational Week (weeks) | 61 | 8.4 ± 1.5 | 8 (6-12) | 0,003 |
| BMI (kg/m²) | 61 | 27.2 ± 3.8 | 26 (21-37) | > 0.05 |
| Parity | 61 | 1.9 ± 1.1 | 2 (1-5) | > 0.05 |
| Previous Number of Caesarean sections | 61 | 1.3 ± 0.5 | 1 (1-3) | > 0.05 |
| Parameter | Mean ± SD | P Value | Significance Level |
|---|---|---|---|
| Gestational Sac Strain Ratio | 2.5 ± 0.8 | 0,03 | p < 0.05 |
| Myometrium Shear Wave Velocity (m/s) | 3.2 ± 1.1 | 0,01 | p < 0.05 |
| Scar Hardness (kPa) | 85 ± 20 | <0,001 | p < 0.001 |
| Beta-hCG (IU/L) | 15000 ± 5000 | 0,25 | > 0.05 |
| Fetal Heart Rate (bpm) | 140 ± 15 | 0,1 | > 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



