
Submitted:
04 November 2024
Posted:
06 November 2024
You are already at the latest version
Abstract
Background: The clinical and laboratory features of patients with non-criteria obstetric antiphospholipid syndrome (NC-OAPS), as well as their pregnancy outcomes and ideal treatment are not clearly determined. The aim of this study is to describe the characteristics and outcomes of pregnancies in NC-OAPS and compare them with an obstetric APS (OAPS) cohort. Methods: Retrospective study conducted in a cohort of women referred to a high-risk obstetric unit of a tertiary hospital. Women that were classified as having OAPS or NC-OAPS were included and compared in terms of clinical and laboratory characteristics, management, and subsequent pregnancy outcomes. Results: We identified 107 women with 143 pregnancies, 91 with NC-OAPS and 16 with OAPS. There were no differences in demographic features between both groups. Women with NC-OAPS were more likely to have recurrent implantation failure and were predominantly positive for a single antiphospholipid antibody (aPL) subtype. Both groups were treated similarly (low dose aspirin plus low molecular weight heparin in 87.4% of NC-OAPS and 83.3% of OAPS, p>0.05). Live birth rate (82.4% and 75.0%, respectively, p>0.05) and adverse pregnancy outcomes (31.6% vs 37.5%, p>0.05) in subsequent pregnancies during follow-up were also similar between groups. Conclusions: This study revealed differences in the previous pregnancy morbidity and aPL profiles in women with NC-OAPS and OAPS, although the therapeutic approach and the outcomes of subsequent pregnancies were similar in both groups.
Keywords:
non-criteria obstetric antiphospholipid syndrome
; adverse pregnancy outcomes
; aspirin
; heparin
1. Introduction
Antiphospholipid syndrome (APS) is characterized by the presence of antiphospholipid antibodies (aPL) and clinical manifestations such as vascular thrombosis and pregnancy morbidity. For research purposes, APS classification criteria have been created and updated [1,2,3]. Currently, the most widely used are the Sydney criteria [2]. In daily clinical practice, particularly in the case of obstetric APS (OAPS), physicians are frequently faced with patients who do not meet these criteria. These cases are globally defined as non-criteria OAPS (NC-OAPS). In the literature, there are variations in the features included in this definition [4,5], and its management is controversial. The European Registry on Obstetric Antiphospholipid Syndrome (EUROAPS) cohort study, which compares 1000 women with diagnosis of OAPS and 640 with NC-OAPS, found clinical and laboratory disparities between patients of both groups, although fetal-maternal outcomes were similar when treatment was administered [5].
Adverse pregnancy outcomes (APO) such as sterility and recurrent implantation failure (RIF) are being investigated as related to aPL. The prevalence of positive aPL in infertile women was reported in 0-7.6%, according to the aPL subtype [6], and <5% in women with RIF [7]. Even though the low prevalence of aPL in these settings, a recent review found that the relative risk for the presence of any type of aPL was 3.06 in women with RIF compared to women having at least one successful in vitro fertilization (IVF) [8]. In contrast, a previous metanalysis of prospective studies found no significant correlations between aPL and IVF outcomes [9].
The types of aPL implicated in APO are also a matter of debate. Some studies reported lupus anticoagulant (LA) [10,11] or anti-β2glycoprotein I antibodies (aβ2GPI) [12] as strong predictors of APO, while others did not find association of aβ2GPI with fetal death or other APO [13,14]. Several studies have also suggested that low aPL titers have a similar clinical relevance in obstetric complications comparing to medium or high titers [15]. In patients with clinical criteria for OAPS but seronegative for conventional aPL, an effort has arisen in the last two decades to discover new aPL with clinical implications. Non-conventional aPL were reported in 68% of these patients [16]. Anti-phosphatidylserine/prothrombin antibodies (aPS/PT) IgG/IgM antibodies are amongst the best studied and many groups have showed their association with APO [16,17,18].
In women with OAPS, standard treatment consists of low dose aspirin (LDA) and low molecular weight heparin (LMWH) during pregnancy, which results in a rate of successful pregnancies up to 80–85% [17,19]. Whether women with NC-OAPS require treatment is controversial. Both EUROAPS and EUREKA studies suggested that patients with NC-OAPS benefited from treatment [5,20]. Some studies found that patients with aPS/PT also have a reduction of APO if they receive treatment during their pregnancy [16,17,18]. Furthermore, recent retrospective studies found that treatment with LDA plus LMWH +/- hydroxychloroquine (HCQ) improved IVF outcomes in patients with aPL, increasing the clinical pregnancy, implantation, and take-home baby rates [21,22]. Given the difficulty of performing randomized controlled trials in this field, there are no appropriately designed studies that could better evaluate treatment effectiveness. In alternative, potential valuable information may be achieved from real-world cohorts from dedicated centers.
The main objective of this study is to characterize the clinical and laboratory features, management and pregnancy outcomes of women with APO who do not meet Sydney clinical and/or laboratory APS criteria (NC-OAPS) in a monocentric real-world cohort. Secondary objectives are: a) to compare the cohort with a contemporaneous group of women with OAPS; b) and identify factors associated with APO in both groups.
2. Materials and Methods
2.1. Patients
Retrospective study of women referred to a high-risk obstetric unit of a tertiary hospital between 2010 and 2022, with APO and aPL positivity. This study was approved by the Institutional Review Board at the Hospital Clinic, Barcelona (protocol code HCB/2018/1221, approved on December 13, 2018), with a waiver of informed consent given the retrospective nature of the study. The study conformed to the principles of the Declaration of Helsinki.
2.2. Inclusion Criteria
Detailed in the flowchart of Figure 1:
- OAPS group: patients with obstetrical APS fulfilling the Sydney classification criteria [2].
- NC-OAPS group: patients with confirmed positive criteria aPL, but not meeting clinical Sydney criteria for OAPS (clinical NC-OAPS); or with clinical Sydney criteria and non-criteria aPL titers/subtypes (lab NC-OAPS); or with non-criteria obstetric morbidity associated with non-criteria aPL titers or subtypes (obstetric morbidity related to APS [OMAPS] subgroup).
The non-criteria clinical events included were the following: two pregnancy losses (PL) before 10 weeks, including at least one clinical PL; ≥3 non-consecutive PL; late placental vasculopathy (preeclampsia [PE]/eclampsia after 34 weeks or preterm birth after 34 weeks due to fetal growth restriction [FGR]); puerperal PE; placental abruption; RIF, defined as ≥3 embryo transfers of good quality without achieving a clinical pregnancy; and unexplained sterility.
The non-criteria laboratory features included were: low-medium aPL titers; one out-of-two positive aPL determinations; two positive aPL determinations, but less than 12 weeks apart; and negative classical aPL but positive aPS/PT.
2.3. Exclusion Criteria (Figure 1):
- APO due to anatomical, genetic, or infectious cause;
- thrombotic APS;
- patients not tested or only tested once for aPL at our laboratory;
- patients with no further pregnancies after evaluation at our Unit.
2.4. Recorded Information and Definitions
Medical records were reviewed retrospectively, and the following information was obtained:
- Demographic characteristics and previous medical history.
- aPL: LA, determined according to the guidelines of the International Society of Thrombosis and Haemostasis [23], and IgG and IgM isotypes of anticardiolipin (aCL) and aβ2GPI determined by enzyme-linked immunosorbent assay (ELISA) or by chemiluminescent immunoassay (CLIA). Samples were considered positive when ≥20 U/ml GPL/MPL or ≥20 chemiluminescent units (CU) (> 99th percentile). The defined ‘criteria titers’ were: IgG/IgM aCL >40 GPL/MPL by ELISA, IgG aCL >95 CU or IgM aCL >31 CU by CLIA (equivalent to ELISA antibody titers of 40 GPL/MPL units by ELISA, according to Lakos G et al. [24]), and aβ2GPI antibody results > 40 GPL/MPL or ≥ 20 CU. Results above the cut-off value but below these titers were categorized as ‘low-medium, non-criteria titers’. aPS/PT IgG and IgM antibodies were determined by ELISA and results at 99th percentile (≥ 30 U/ml) were considered positive, according to manufacturer’s instructions.
- Subsequent pregnancies, which were those conceived after medical evaluation at our Unit. For each subsequent pregnancy, the following data were collected: maternal age at delivery, treatment, and obstetric outcomes. The following relevant APO were defined and recorded:
- early PL: spontaneous PL before week 10 of gestation
- late PL: spontaneous PL of a morphologically normal fetus at or beyond week 10 of gestation
- PE or eclampsia during gestation or puerperium
- placental abruption
- FGR: estimated fetal weight below the 3rd percentile for a given gestational age, or below the 10th percentile associated with doppler abnormalities
- premature delivery (before 37 weeks of gestation) because of placental vasculopathy
- low birthweight (under 2500 grams)
- neonatal death before hospital discharge due to complications of prematurity and/or placental insufficiency.
- Additional outcomes, such as elective medical terminations, maternal thrombosis, hemorrhage or death, as well as embryo/fetal chromosomal analysis were also collected.
2.5. Statistical Analysis
Qualitative variables are expressed as absolute values or percentages. Their associations were evaluated using Chi-Square or Fisher’s exact tests, according to normal distribution. Continuous variables were expressed as means with standard deviation (SD), and t-tests were performed for their comparison. P values under 0.05 were considered significant. Statistical analyses were performed using SPSS version 20 (IBM SPSS Statistics 20).
3. Results
Among a total of 375 patients referred to the high-risk obstetric unit because of aPL positivity and/or previous APO, 107 women with 143 pregnancies (four multiple) were included in the analysis (Figure 1). Ninety-one patients (85.0%) were classified as having NC-OAPS, while 16 (15.0%) had OAPS.
3.1. Characteristics of Patients with NC-OAPS
Twenty-four women (26.4%) had an additional autoimmune disease, most frequently autoimmune thyroiditis (9.9%). Six patients (6.6%) had an inherited thrombophilia: heterozygous factor V Leiden (n=4), and heterozygous prothrombin gene mutation (n=2). Unexplained sterility was the most frequent previous pregnancy morbidity reported (36.3%), followed by two or ≥ 3 early PL (24.2% each). Concerning aPL profile, aCL was the most and LA the least common positive aPL (Table 1), and around 50% of patients had single aPL positivity.
3.2. Subsequent Pregnancies in Patients with NC-OAPS: Treatment and Outcomes
There were 119 subsequent pregnancies in the follow-up of patients with NC-OAPS. The combination of LDA and LMWH was the most common treatment regimen used (87.4%). Treatment was maintained until the end of pregnancy except in six, in which LMWH was stopped after the first trimester. Corticosteroids and HCQ were used in 14.3% and 19.3% of pregnancies, respectively, only in association with antithrombotic/anticoagulant treatment (Table 1).
Most pregnancies ended successfully with the delivery of live newborns (82.4%) (Table 1). Early PL occurred in 18 (15.1%), 9 (50%) of which with confirmed aneuploidy on chorionic villus biopsy, 3 (16.7%) with confirmed euploidy, and in 6 (33.3%) a chromosomal analysis was not performed. Late PL occurred twice in the same patient, on 12 and 13 gestational weeks, both with euploid chorionic villus biopsy results. PE occurred in 5.2% of women with NC-OAPS, all of them were non-severe and after 34 weeks of gestation (Table 1).
Regarding fetal and neonatal outcomes, low birthweight and FGR were the most common complications observed (11.5% and 9.0%, respectively) (Table 1). Preterm births occurred because of severe HELLP (hemolysis, elevated liver enzymes and low platelets) syndrome in one pregnancy and FGR in two.
3.3. Comparison Between NC-OAPS and OAPS Groups
No statistically significant differences were recorded between patients with NC-OAPS and women with OAPS in terms of ethnicity, cardiovascular risk factors and associated autoimmune diseases (Table 2). Considering all the previous pregnancy morbidity each patient experienced, late PL was the most frequent previous APO in the OAPS group (62.5%), contrasting with unexplained sterility in the NC-OAPS group (36.3%). History of a late PL was significantly more common in women with OAPS, whereas RIF was significantly more frequent in NC-OAPS. Positivity of aβ2GPI and LA was more frequent in the OAPS group, while the other aPL subtypes had comparable frequencies between groups. Triple or quadruple aPL positivity were more frequent in the OAPS group (Table 2 and Figure 2).
There were 24 subsequent pregnancies in patients with OAPS. Assisted reproduction techniques were used in 6 (25%) of patients with OAPS and 55 (46.6%) of those with NC-OAPS (p=0.070). Treatment with the combination of LDA and LMWH was used with similar frequencies in OAPS and NC-OAPS (83.3% versus 87.4%, p>0.05) (Table 3). Delivery of live newborns occurred in comparable percentages in pregnancies in OAPS (75.0%) and NC-OAPS (82.4%) groups, p>0.05 (Table 3). Considering all subsequent pregnancies per woman, after evaluation at our Unit, 100% of women with OAPS achieved the birth of at least one live newborn, a percentage similar to those with NC-OAPS (93.4%, p>0.05).
The occurrence of at least one APO per pregnancy was comparable between groups (37.5% in OAPS vs 31.6% in NC-OAPS, p>0.05). No significant differences were found between groups in terms of early or late PL, PE, preterm birth or low birthweight neonates (Table 3). The indications for caesarean section were predominantly obstetric in nature. In five cases, caesarean section was performed because of placental insufficiency: placental abruption (n=1, in a patient with NC-OAPS), PE (n=2, both in women with OAPS), FGR (n=2, in the NC-OAPS group). There were no maternal thrombosis nor maternal deaths in any group.
3.4. Risk Factors for Unexplained Pregnancy Loss
Since PL was the most frequent adverse event reported in the subsequent pregnancies of our entire cohort, we investigated potential risk factors associated with PL of unknown cause (those in which a chorion biopsy was not performed or with euploidy or inconclusive results, n=15). In a univariate analysis, we did not find significant differences between pregnancies that ended successfully and PL of unknown cause in terms of maternal body mass index (BMI) or age, aPL profile, adjusted Global Antiphospholipid Syndrome Score (aGAPSS) or treatment used (Table 4).
4. Discussion
This series reflects a real-world scenario of a specialized obstetric Unit in a third level hospital and shows that patients with NC-OAPS correspond to more than 80% of patients referred. The results of this study show an overall good pregnancy outcome for women with NC-OAPS when treatment is offered, comparable to patients with treated OAPS.
Our study found that a previous history of late PL was significantly more common in women with OAPS, whereas RIF was more common in NC-OAPS. These observations are in line with the results of the EUROAPS study, in which patients with OAPS had a higher number of early PL, late PL, stillbirth, early placental vasculopathy and prematurity than those with NC-OAPS, whereas women with NC-OAPS had higher rates of RIF and late placental events [5]. Placental vasculopathy was rare in our cohort, which could contribute to the lack of prevalence difference between NC-OAPS and OAPS groups. Furthermore, we found a high percentage of sterility in our cohort, a variable that was not included in the EUROAPS study. This may indicate that in routine clinical practice, patients with sterility are increasingly investigated for aPL presence and, if positive, referred for management. Nevertheless, there is a gap on literature respective to this issue and further research is required.
Patients with NC-OAPS are more likely to have single aPL positivity, in contrast with a higher number of positive aPL in OAPS patients. Patients in the EUROAPS study were similar to those of our cohort. In that study, patients with double or triple aPL positivity and patients with LA positivity alone had more frequently OAPS. Patients with aCL and aβ2GPI had more frequently NC-OAPS [5]. In our study, LA was also significantly more frequent in OAPS, but, contrarily to the EUROAPS study, aβ2GPI was also more common in OAPS, in part possibly because of the low thresholds used as criteria titers of this antibody when determined by CLIA in our study.
The optimal treatment in NC-OAPS patients is not defined. In our series, more than 80% of patients with NC-OAPS were treated with a combination of LDA and LMWH, a frequency similar to that of patients with OAPS. These results are aligned with those of a systematic review, aiming to compare treatment regimens in NC-OAPS versus OAPS [25]. The biologic mechanisms involved in the pathogenesis of aPL-associated obstetric morbidity may include not only thrombosis but also trophoblast dysfunction, decidual inflammation, complement activation, and implication of neutrophil extracellular traps [17]. For these reasons, apart from anti-thrombotic drugs and heparin, other treatments are commonly used, particularly in refractory OAPS [26], but their efficacy is yet to be clarified. We reported the adjuvant use of HCQ and corticosteroids in 8-20% of subjects, with the NC-OAPS group tending to receive more commonly these additional therapies. Other study reported a higher use of HCQ and steroids in NC-OAPS [27].
In subsequent pregnancies, our study found a similar prevalence of live births and APO between women with NC-OAPS and OAPS. Our results coincide partially with that of EUROAPS, as the percentages of treatment and rate of live births were also similar in both groups, but that study reported higher APO incidence (73.4% in NC-OAPS and 65.1% in OAPS) [5]. A metanalysis reported that five studies described an improvement of live births in both NC-APS and OAPS with treatment [25]. Several other studies of women with NC-OAPS, defined in a similar manner as in our study, suggested that they have similar pregnancy outcomes with standard treatment for OAPS [5,17,20,28,29,30]. On the whole, interpretation of results should be made with caution, as NC-OAPS definition varies among studies and most of study designs do not control the exposure to treatment.
An important focus of the scientific community in this area has been to identify prognostic factors for new obstetric complications and hopefully tailoring the management [31]. Research groups developed scores focusing on aPL to stratify the risk of patients carrying these antibodies, such as the GAPSS score [32], its variant aGAPSS score [33], and the EUREKA algorithm [20]. Few studies evaluated the prediction value of GAPSS/aGAPSS for pregnancy morbidity, and results are contradictory [34,35,36]. The authors of EUREKA algorithm found that the probability of developing APO in women with aPL was 64% with low titers and 68% with high titers, with a higher risk in those with LA and/or IgG antiβ2GPI positivity [20]. All women with low-titer aPL benefited from treatment with LDA+LMWH±HCQ, and its effectiveness was even greater for low-titer than for criteria aPL [20]. Nowadays, there is still no consensus about how to stratify the obstetric risk and tailor treatment, particularly in non-criteria subjects and after new obstetric events.
Recurrent early PL is the obstetric complication for which a diagnosis of APS is most often considered, and it was the most frequent subsequent APO observed in our study. However, the role of aPL in early PL is not always clearly defined, given the lack of discrimination in literature between biochemical and clinical losses, and incomplete evaluation for other causes of PL. Reflecting this last limitation, we reported that within the 23 early PL occurring in our entire cohort, only 13 had unknown cause, as the other 10 were associated with embryo aneuploidy. Not performing an embryonic/fetal chromosomal analysis could overestimate the magnitude of aPL effect in these events and eventually indicate a false therapeutic failure. In this sense, we searched for risk factors for PL of unknown cause, and found no correlation with maternal age, BMI, previous obstetric history, antibodies profile or used treatment. However, the low number of PL may affect the statistic power of this analysis.
Our study has limitations. It is retrospective, with inherent constraints in data collection and analysis, such as the variation of laboratory methods used to test for aPL along time, and unstandardized treatment regimens. One of the most important is that the aPL detection methods varied between and within patients. CLIA is the only method used at our laboratory since 2015. We acknowledge that this supposes a research limitation, as CLIA is not the standard method used to classify a patient with APS, and the correlation of values between the moderate-high thresholds of ELISA and CLIA is variable for different aPL subtypes and still requires validation. As there is ambiguity about the cut-off values for low-titers and criteria titers of aPL detected by CLIA, we tried to overcome this limitation by using the equivalent aCL criteria titers according to Lakos G et al. [24]. Nevertheless, for the aβ2GPI subtype, criteria levels were the in-house cut-off values. According to Vandevelde et al. [37], the use of these CLIA units would overestimate the number of patients with criteria aPL titers and eventually amplify the OAPS group, which is in fact the smaller group of our study. Another limitation of our study is the large difference of the size of the two cohorts analyzed, which may affect the validity of the comparison between them. The smaller size of the OAPS cohort at the same lapse of time may be attributed to several factors. On the one hand, patients are increasingly referred to the medical visit for APO not fulfilling the clinical APS criteria (for example, after two PL), and treatment is equally initiated, which potentially avoids another APO in the next pregnancy and the eventual classification of patients with OAPS. On another hand, we used strictly the Sidney criteria for attribution of the OAPS diagnosis. Since these are classification criteria, it is possible that in clinical practice many patients are diagnosed with and managed as OAPS without fulfilling them. Given the uncertainties of the impact of aPL in non-criteria pregnancy morbidity and of different aPL titers and subtypes, the classification criteria are increasingly restrictive regarding the clinical features included (according to ACR/EULAR 2023 criteria, only eight patients in this study would have been classified as OAPS), while physicians in daily clinical practice seem to take an opposite direction, assuming (and treating) the relevance of low or transitory aPL titers in otherwise unexplained pregnancy morbidity.
We consider that our study has several strengths. We included a cohort of women that represents the whole spectrum of patients with a clinical suspicion of aPL-associated pregnancy morbidity. Patients with thrombotic APS were excluded, providing a more homogenous group of patients only with unfavorable obstetric history. Finally, some of the PL observed were submitted to chromosomal analysis, revealing a not negligible number of aneuploidies. When feasible, the cytogenetic analysis of products of conception should be performed in all pregnancy losses to avoid erroneous tagging of aPL-related morbidity.
5. Conclusions
Patients with NC-OAPS represent an important and frequent, although incompletely known group in routine clinical practice. According to our results, patients with NC-OAPS may be treated similarly to those with OAPS. The outcome of subsequent pregnancies in treated patients is good and similar to treated patients with OAPS.
Author Contributions
Conceptualization, S.B. and G.E., N.B..; methodology, S.B.; formal analysis, S.B. and A.P.I.; writing—original draft preparation, S.B.; writing—review and editing, S.B., G.E., N.B., M.B., E.R.O., A.P.I., R.C., J.C.R. and D.T.; supervision, G.E.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Hospital Clinic, Barcelona (protocol code HCB/2018/1221, approved on December 13, 2018).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The dataset is available upon request from the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wilson, W.A.; Gharavi, A.E.; Koike, T.; Lockshin, M.D.; Branch, D.W.; Piette, J.C.; et al. International consensus statement on preliminary classification criteria for definite antiphospholipid syndrome: report of an international workshop. Arthritis Rheum 1999, 42, 1309–1311. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006, 4, 295–306. [Google Scholar] [CrossRef]
- Barbhaiya, M.; Zuily, S.; Naden, R.; Hendry, A.; Manneville, F.; Amigo, M.C.; et al. The 2023 ACR/EULAR Antiphospholipid Syndrome Classification Criteria. Arthritis Rheumatol 2023, 75, 1687–1702. [Google Scholar] [CrossRef]
- Pires da Rosa, G.; Bettencourt, P.; Rodriguez-Pinto, I.; Cervera, R.; Espinosa, G. "Non-criteria" antiphospholipid syndrome: A nomenclature proposal. Autoimmun Rev 2020, 19, 102689. [Google Scholar] [CrossRef]
- Alijotas-Reig, J.; Esteve-Valverde, E.; Ferrer-Oliveras, R.; Saez-Comet, L.; Lefkou, E.; Mekinian, A.; et al. Comparative study of obstetric antiphospholipid syndrome (OAPS) and non-criteria obstetric APS (NC-OAPS): report of 1640 cases from the EUROAPS registry. Rheumatology (Oxford) 2020, 59, 1306–1314. [Google Scholar] [CrossRef]
- Chighizola, C.B.; Raimondo, M.G.; Meroni, P.L. Does APS Impact Women's Fertility? Curr Rheumatol Rep 2017, 19, 33. [Google Scholar] [CrossRef]
- Vomstein, K.; Voss, P.; Molnar, K.; Ainsworth, A.; Daniel, V.; Strowitzki, T.; et al. Two of a kind? Immunological and clinical risk factors differ between recurrent implantation failure and recurrent miscarriage. J Reprod Immunol 2020, 141, 103166. [Google Scholar] [CrossRef]
- Papadimitriou, E.; Boutzios, G.; Mathioudakis, A.G.; Vlahos, N.F.; Vlachoyiannopoulos, P.; Mastorakos, G. Presence of antiphospholipid antibodies is associated with increased implantation failure following in vitro fertilization technique and embryo transfer: A systematic review and meta-analysis. PLoS One 2022, 17, e0260759. [Google Scholar] [CrossRef]
- Tan, X.F.; Xu, L.; Li, T.T.; Wu, Y.T.; Ma, W.W.; Ding, J.Y.; et al. Serum antiphospholipid antibody status may not be associated with the pregnancy outcomes of patients undergoing in vitro fertilization. Medicine (Baltimore) 2022, 101, e29146. [Google Scholar] [CrossRef]
- Lockshin, M.D.; Kim, M.; Laskin, C.A.; Guerra, M.; Branch, D.W.; Merrill, J.; et al. Prediction of adverse pregnancy outcome by the presence of lupus anticoagulant, but not anticardiolipin antibody, in patients with antiphospholipid antibodies. Arthritis Rheum 2012, 64, 2311–2318. [Google Scholar] [CrossRef]
- Yelnik, C.M.; Laskin, C.A.; Porter, T.F.; Branch, D.W.; Buyon, J.P.; Guerra, M.M.; et al. Lupus anticoagulant is the main predictor of adverse pregnancy outcomes in aPL-positive patients: validation of PROMISSE study results. Lupus Sci Med 2016, 3, e000131. [Google Scholar] [CrossRef] [PubMed]
- Saccone, G.; Berghella, V.; Maruotti, G.M.; Ghi, T.; Rizzo, G.; Simonazzi, G.; et al. Antiphospholipid antibody profile based obstetric outcomes of primary antiphospholipid syndrome: the PREGNANTS study. Am J Obstet Gynecol 2017, 216, 525 e1–525 e12. [Google Scholar] [CrossRef]
- Xu, J.; Chen, D.; Duan, X.; Li, L.; Tang, Y.; Peng, B. The association between antiphospholipid antibodies and late fetal loss: A systematic review and meta-analysis. Acta Obstet Gynecol Scand 2019, 98, 1523–1533. [Google Scholar] [CrossRef]
- Jiang, D.; Lim, W.; Crowther, M.; Garcia, D. A systematic review of the association between anti-beta-2 glycoprotein I antibodies and APS manifestations. Blood Adv 2021, 5, 3931–3936. [Google Scholar] [CrossRef] [PubMed]
- Meroni, P.L.; Borghi, M.O.; Grossi, C.; Chighizola, C.B.; Durigutto, P.; Tedesco, F. Obstetric and vascular antiphospholipid syndrome: same antibodies but different diseases? Nat Rev Rheumatol 2018, 14, 433–440. [Google Scholar] [CrossRef]
- Mekinian, A.; Bourrienne, M.C.; Carbillon, L.; Benbara, A.; Noemie, A.; Chollet-Martin, S.; et al. Non-conventional antiphospholipid antibodies in patients with clinical obstetrical APS: Prevalence and treatment efficacy in pregnancies. Semin Arthritis Rheum 2016, 46, 232–237. [Google Scholar] [CrossRef]
- Pleguezuelo, D.E.; Cabrera-Marante, O.; Abad, M.; Rodriguez-Frias, E.A.; Naranjo, L.; Vazquez, A.; et al. Anti-Phosphatidylserine/Prothrombin Antibodies in Healthy Women with Unexplained Recurrent Pregnancy Loss. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Mu, F.; Wang, M.; Zeng, X.; Liu, L.; Wang, F. Preconception Non-criteria Antiphospholipid Antibodies and Risk of Subsequent Early Pregnancy Loss: a Retrospective Study. Reprod Sci 2023. [Google Scholar] [CrossRef]
- Alijotas-Reig, J.; Esteve-Valverde, E.; Anunciacion-Llunell, A.; Marques-Soares, J.; Pardos-Gea, J.; Miro-Mur, F. Pathogenesis, Diagnosis and Management of Obstetric Antiphospholipid Syndrome: A Comprehensive Review. J Clin Med 2022, 11. [Google Scholar] [CrossRef]
- Pregnolato, F.; Gerosa, M.; Raimondo, M.G.; Comerio, C.; Bartoli, F.; Lonati, P.A.; et al. EUREKA algorithm predicts obstetric risk and response to treatment in women with different subsets of anti-phospholipid antibodies. Rheumatology (Oxford) 2021, 60, 1114–1124. [Google Scholar] [CrossRef]
- Wu, L.; Fang, X.; Lu, F.; Zhang, Y.; Wang, Y.; Kwak-Kim, J. Anticardiolipin and/or anti-beta2-glycoprotein-I antibodies are associated with adverse IVF outcomes. Front Immunol 2022, 13, 986893. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Song, Y.; Xia, X.; Wang, J.; Qian, Y.; Yuan, C.; et al. A retrospective study on IVF/ICSI outcomes in patients with persisted positive of anticardiolipin antibody: Effects of low-dose aspirin plus low molecular weight heparin adjuvant treatment. J Reprod Immunol 2022, 153, 103674. [Google Scholar] [CrossRef] [PubMed]
- Devreese, K.M.J.; de Groot, P.G.; de Laat, B.; Erkan, D.; Favaloro, E.J.; Mackie, I.; et al. Guidance from the Scientific and Standardization Committee for lupus anticoagulant/antiphospholipid antibodies of the International Society on Thrombosis and Haemostasis: Update of the guidelines for lupus anticoagulant detection and interpretation. J Thromb Haemost 2020, 18, 2828–2839. [Google Scholar] [CrossRef]
- Lakos, G.; Bentow, C.; Mahler, M. A Clinical Approach for Defining the Threshold between Low and Medium Anti-Cardiolipin Antibody Levels for QUANTA Flash Assays. Antibodies (Basel) 2016, 5. [Google Scholar] [CrossRef]
- Pires da Rosa, G.; Ferreira, E.; Sousa-Pinto, B.; Rodriguez-Pinto, I.; Brito, I.; Mota, A.; et al. Comparison of non-criteria antiphospholipid syndrome with definite antiphospholipid syndrome: A systematic review. Front Immunol 2022, 13, 967178. [Google Scholar] [CrossRef]
- Mekinian, A.; Alijotas-Reig, J.; Carrat, F.; Costedoat-Chalumeau, N.; Ruffatti, A.; Lazzaroni, M.G.; et al. Refractory obstetrical antiphospholipid syndrome: Features, treatment and outcome in a European multicenter retrospective study. Autoimmun Rev 2017, 16, 730–734. [Google Scholar] [CrossRef] [PubMed]
- Xi, F.; Cai, Y.; Lv, M.; Jiang, Y.; Zhou, F.; Chen, Y.; et al. Anticardiolipin Positivity Is Highly Associated With Intrauterine Growth Restriction in Women With Antiphospholipid Syndrome. Clin Appl Thromb Hemost 2020, 26, 1076029620974455. [Google Scholar] [CrossRef]
- Chen, J.; Yue, J.; Lu, Y.; Li, T.; Li, X.; Zhang, J.Y. Recurrent miscarriage and low-titer antiphospholipid antibodies. Clin Rheumatol 2024. [Google Scholar] [CrossRef]
- Martinez-Taboada, V.M.; Blanco-Olavarri, P.; Del Barrio-Longarela, S.; Riancho-Zarrabeitia, L.; Merino, A.; Comins-Boo, A.; et al. Non-Criteria Obstetric Antiphospholipid Syndrome: How Different Is from Sidney Criteria? A Single-Center Study. Biomedicines 2022, 10. [Google Scholar] [CrossRef]
- Li, X.; Deng, X.; Duan, H.; Zeng, L.; Zhou, J.; Liu, C.; et al. Clinical features associated with pregnancy outcomes in women with positive antiphospholipid antibodies and previous adverse pregnancy outcomes: a real-world prospective study. Clin Rheumatol 2021, 40, 193–204. [Google Scholar] [CrossRef]
- De Carolis, S.; Tabacco, S.; Rizzo, F.; Giannini, A.; Botta, A.; Salvi, S.; et al. Antiphospholipid syndrome: An update on risk factors for pregnancy outcome. Autoimmun Rev 2018, 17, 956–966. [Google Scholar] [CrossRef]
- Sciascia, S.; Sanna, G.; Murru, V.; Roccatello, D.; Khamashta, M.A.; Bertolaccini, M.L. The global anti-phospholipid syndrome score in primary APS. Rheumatology (Oxford) 2015, 54, 134–138. [Google Scholar] [CrossRef]
- Radin, M.; Schreiber, K.; Costanzo, P.; Cecchi, I.; Roccatello, D.; Baldovino, S.; et al. The adjusted Global AntiphosPholipid Syndrome Score (aGAPSS) for risk stratification in young APS patients with acute myocardial infarction. Int J Cardiol 2017, 240, 72–77. [Google Scholar] [CrossRef]
- Radin, M.; Cecchi, I.; Schreiber, K.; Rubini, E.; Roccatello, D.; Cuadrado, M.J.; et al. Pregnancy success rate and response to heparins and/or aspirin differ in women with antiphospholipid antibodies according to their Global AntiphosPholipid Syndrome Score. Semin Arthritis Rheum 2020, 50, 553–556. [Google Scholar] [CrossRef]
- Sciascia, S.; Radin, M.; Sanna, G.; Cecchi, I.; Roccatello, D.; Bertolaccini, M.L. Clinical utility of the global anti-phospholipid syndrome score for risk stratification: a pooled analysis. Rheumatology (Oxford) 2018, 57, 661–665. [Google Scholar] [CrossRef]
- Del Barrio-Longarela, S.; Martinez-Taboada, V.M.; Blanco-Olavarri, P.; Merino, A.; Riancho-Zarrabeitia, L.; Comins-Boo, A.; et al. Does Adjusted Global Antiphospholipid Syndrome Score (aGAPSS) Predict the Obstetric Outcome in Antiphospholipid Antibody Carriers? A Single-Center Study. Clin Rev Allergy Immunol 2022, 63, 297–310. [Google Scholar] [CrossRef]
- Vandevelde, A.; Chayoua, W.; de Laat, B.; Gris, J.C.; Moore, G.W.; Musial, J.; et al. Semiquantitative interpretation of anticardiolipin and antibeta2glycoprotein I antibodies measured with various analytical platforms: Communication from the ISTH SSC Subcommittee on Lupus Anticoagulant/Antiphospholipid Antibodies. J Thromb Haemost 2022, 20, 508–524. [Google Scholar] [CrossRef]
Figure 1.
Study flowchart. Selected patients with OAPS and NC-OAPS from an initial cohort of women with aPL and/or APO history. Abbreviations: aβ2GPI: anti-β2 glycoprotein-1 antibodies; aCL: anticardiolipin antibodies; aPL: antiphospholipid antibodies; APO: adverse pregnancy outcome; aPS/PT: anti-phosphatidylserine/prothrombin complex antibodies; FGR: fetal growth restriction; LA: lupus anticoagulant; NC-OAPS: non-criteria obstetric antiphospholipid syndrome; OAPS: obstetric antiphospholipid syndrome; OMAPS: obstetric morbidity related to APS; PE: preeclampsia.
Figure 1.
Study flowchart. Selected patients with OAPS and NC-OAPS from an initial cohort of women with aPL and/or APO history. Abbreviations: aβ2GPI: anti-β2 glycoprotein-1 antibodies; aCL: anticardiolipin antibodies; aPL: antiphospholipid antibodies; APO: adverse pregnancy outcome; aPS/PT: anti-phosphatidylserine/prothrombin complex antibodies; FGR: fetal growth restriction; LA: lupus anticoagulant; NC-OAPS: non-criteria obstetric antiphospholipid syndrome; OAPS: obstetric antiphospholipid syndrome; OMAPS: obstetric morbidity related to APS; PE: preeclampsia.
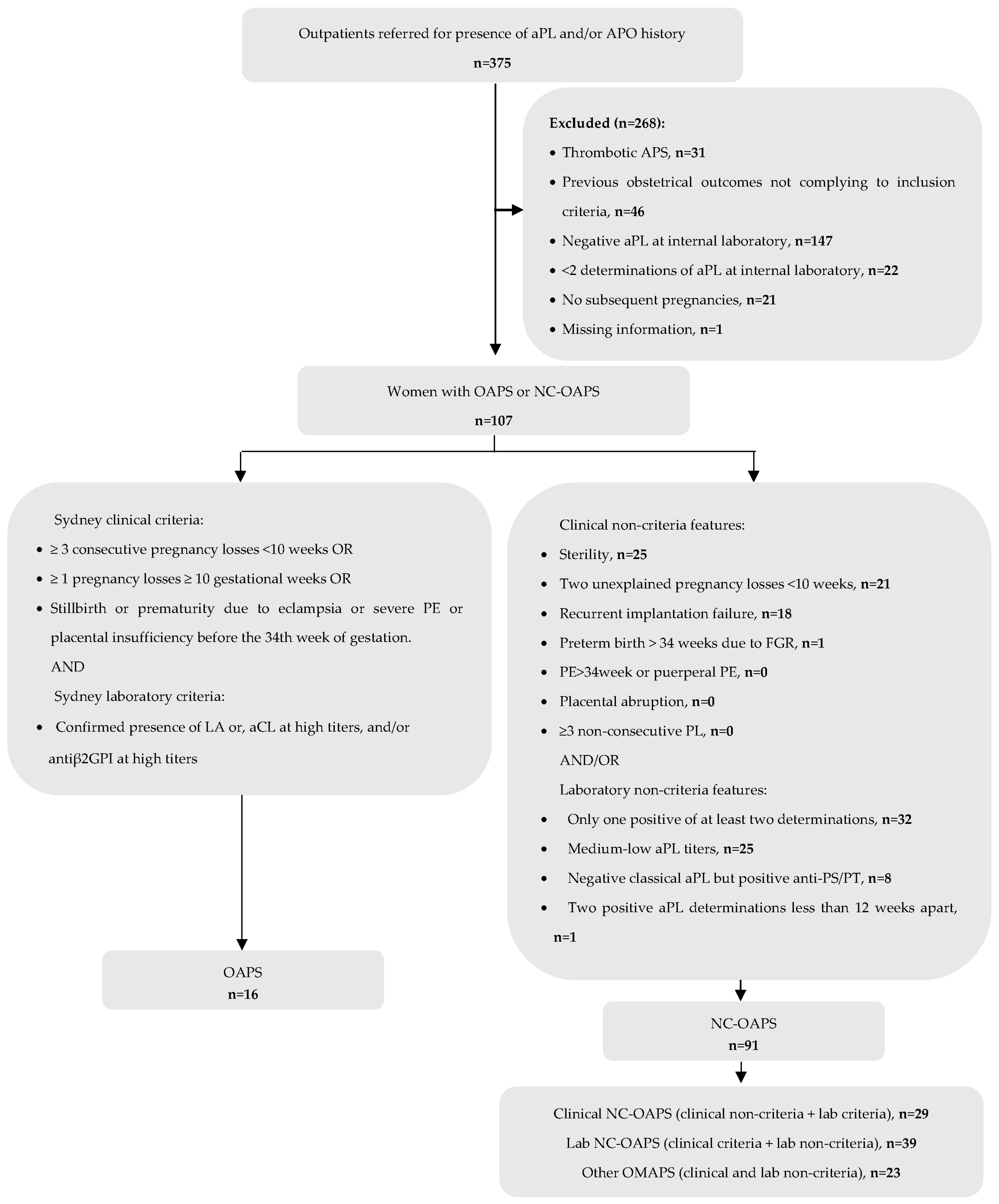
Figure 2.
Composition and distribution of aPL subtypes in OAPS and NC-OAPS groups. * p<0.05 for the comparison between percentages within OAPS and NC-OAPS.
Figure 2.
Composition and distribution of aPL subtypes in OAPS and NC-OAPS groups. * p<0.05 for the comparison between percentages within OAPS and NC-OAPS.
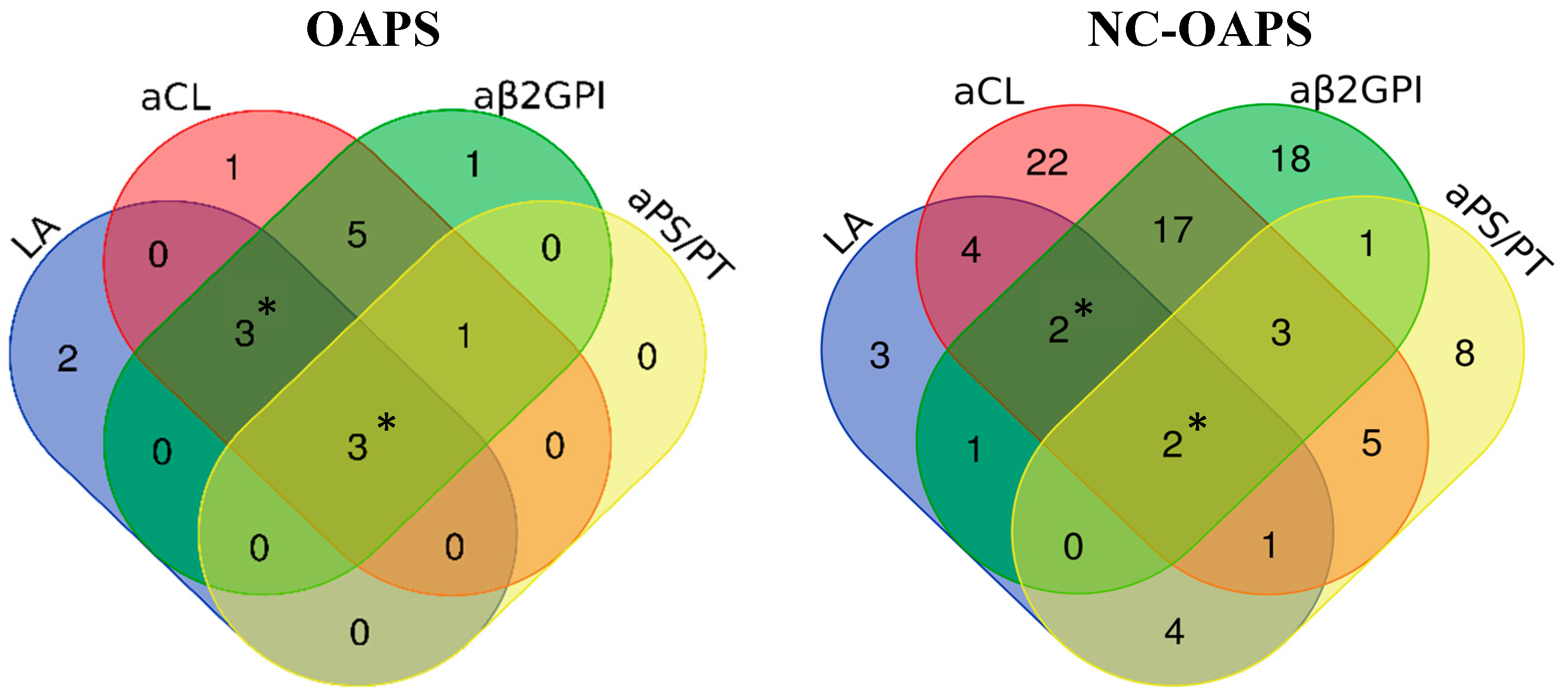

Table 1.
Demographic features, previous APO and aPL profile of patients with NC-OAPS.
| Demographic and clinical characteristics | NC-OAPS patients (n=91) |
|---|---|
| Ethnicity, n (%): | |
| Caucasian | 81 (89.0) |
| Hispanic/ South American | 5 (5.5) |
| Maghrebi | 1 (1.1) |
| Asian | 3 (3.3) |
| Black | 1 (1.1) |
| BMI, mean (S.D.)a | 24.73 (4.61) |
| Smoking habits, n (%)a | 18 (20.0) |
| Arterial hypertension, n (%) | 1 (1.1) |
| Diabetes mellitus, n (%) | 1 (1.1) |
| Dyslipidemia, n (%) | 1 (1.1) |
| Presence of other autoimmune diseases, n (%): | 24 (26.4) |
| Autoimmune thyroiditis | 9 (9.8) |
| Systemic lupus erythematosus | 3 (3.3) |
| Rheumatoid arthritis | 2 (2.2) |
| Psoriasis | 2 (2.2) |
| Cutaneous lupus | 1 (1.1) |
| Systemic sclerosis | 1 (1.1) |
| Sjögren's syndrome | 1 (1.1) |
| Undifferentiated connective tissue disease | 1 (1.1) |
| Seronegative spondyloarthropathy | 1 (1.1) |
| Immune thrombocytopenic purpura | 1 (1.1) |
| IgA vasculitis | 1 (1.1) |
| Multiple sclerosis | 1 (1.1) |
| Inherited thrombophilia, n (%) | 6 (6.6) |
| Previous APO | |
| 2 early pregnancy losses, n (%) | 22 (24.2) |
| ≥3 early pregnancy losses, n (%) | 22 (24.2) |
| ≥1 late pregnancy loss, n (%) | 16 (17.6) |
| Neonatal death (because of FGR/PE/prematurity), n (%) | 2 (2.2) |
| Preterm birth <34 weeks because of FGR, n (%) | 3 (3.3) |
| Preterm birth >34 weeks because of FGR, n (%) | 2 (2.2) |
| PE/eclampsia <34 weeks, n (%) | 2 (2.2) |
| PE/eclampsia >34 weeks, n (%) | 1 (1.1) |
| Placental abruption, n (%) | 2 (2.2) |
| Recurrent implantation failure, n (%) | 20 (22.0) |
| Unexplained sterility, n (%) | 30 (36.3) |
| Antiphospholipid antibodies subtypes | |
| Lupus anticoagulant, n (%) | 17 (18.7) |
| aCL IgM and/or IgG autoantibodies, n (%) | 56 (61.5) |
| aβ2GPI IgM and/or IgG autoantibodies, n (%) | 44 (48.4) |
| aPS/PT IgM and/or IgG autoantibodies, n (%)b | 24 (51.1) |
| Treatment | Subsequent pregnancies (n=119) |
| No treatment, n (%) | 1 (0.8) |
| LDA alone, n (%) | 12 (10.1) |
| LMWH alone, n (%) | 2 (1.7) |
| LDA plus LMWH, n (%) | 104 (87.4) |
| Hydroxychloroquine, n (%) | 23 (19.3) |
| Corticosteroids, n (%) | 17 (14.3) |
| Obstetric and maternal outcomes | |
| Live births, n (%) | 98 (82.4) |
| Pregnancy loss <10w, n (%) | 18 (15.1) |
| Pregnancy loss 10-24w, n (%) | 2 (1.7) |
| Pregnancy loss >24w, n (%) | 0 (0) |
| Preeclampsia, n (%)c | 5 (5.2) |
| HELLP syndrome, n (%)c | 1 (1.0) |
| Placental abruption, n (%)c | 1 (1.0) |
| Fetal and neonatal outcomes | Neonates (n=101) |
| FGR, n (%)c | 9 (9.0) |
| Preterm birth related to PE/HELLP/FGR, n (%)c | 3 (3.0) |
| Low birthweight, n (%)c | 11 (11.5) |
| Neonatal death, n (%) | 1 (1.0) |
Abbreviations: aβ2GPI: anti-β2 glycoprotein-1 antibodies; aCL: anticardiolipin antibodies; aPS/PT: anti-phosphatidylserine/prothrombin complex antibodies; BMI: body mass index; FGR: fetal growth restriction; HELLP: Hemolysis, Elevated Liver enzymes and Low Platelets; LDA: low-dose aspirin; LMWH: low molecular weight heparin; NC-OAPS: non-criteria obstetric antiphospholipid syndrome; PE: preeclampsia; w: weeks. a BMI data were available in 85 patients and smoking habits in 90 patients. b aPS/PT determined in 47 patients (missing in 44). c Data for preeclampsia, HELLP, placental abruption are missing for two women; FGR and preterm birth are missing in one neonate, and low birthweight is missing for five neonates.
Table 2.
Comparison of demographic, obstetric history and aPL profiles in women with OAPS and women with NC-OAPS.
Table 2.
Comparison of demographic, obstetric history and aPL profiles in women with OAPS and women with NC-OAPS.
| OAPS (n=16) |
NC-OAPS (91) |
p value | |
|---|---|---|---|
| Demographic and clinical characteristics | |||
| Ethnicity, n (%) | 0.201 | ||
| Caucasian | 12 (75.0%) | 81 (89.0%) | |
| Hispanic/ | 2 (12.5%) | 5 (5.5%) | |
| South American | |||
| Maghrebi | 1 (6.2%) | 1 (1.1%) | |
| Asian | 1 (6.2%) | 3 (3.3%) | |
| Black | 0 (0%) | 1 (1.1%) | |
| BMI, mean (S.D.)* | 25.03 (6.10) | 24.73 (4.61) | 0.830 |
| Smoker, n (%)** | 1 (6.7) | 18 (20.0) | 0.296 |
| Arterial hypertension, n (%) | 2 (12.5) | 1 (1.1) | 0.058 |
| Diabetes mellitus, n (%) | 0 (0) | 1 (1.1) | 1.000 |
| Dyslipidemia, n (%) | 0 (0) | 1 (1.1) | 1.000 |
| Presence of other autoimmune diseases, n (%) | 4 (25.0) | 24 (26.4) | 1.000 |
| Inherited thrombophilia, n (%) | 0 (0) | 6 (6.6) | 0.588 |
| Age at first subsequent pregnancy, years, mean (S.D.) | 36.81 (6.41) | 36.86 (3.94) | 0.979 |
| Subsequent pregnancies per patient, mean (S.D.) | 1.5 (0.82) | 1.31 (0.59) | 0.261 |
| Previous obstetric history | |||
| Live births before study, n (%) | 7 (43.8) | 18 (19.8) | 0.053 |
| 2 early pregnancy losses, n (%) | 1 (6.2) | 22 (24.2) | 0.184 |
| ≥3 early pregnancy losses, n (%) | 3 (18.8) | 22 (24.2) | 0.758 |
| ≥1 late pregnancy loss, n (%) | 10 (62.5) | 16 (17.6) | 0.000 |
| Neonatal death (because of FGR/PE/prematurity), n (%) | 2 (12.5) | 2 (2.2) | 0.105 |
| Previous preterm birth <34 weeks because of FGR, n (%) | 1 (6.2) | 3 (3.3) | 0.482 |
| Previous preterm birth >34 weeks because of FGR, n (%) | 0 (0) | 2 (2.2) | 1.000 |
| PE/eclampsia <34 weeks, n (%) | 2 (12.5) | 2 (2.2) | 0.105 |
| PE/eclampsia >34 weeks, n (%) | 1 (6.2) | 1 (1.1) | 0.278 |
| Placental abruption, n (%) | 0 (0) | 2 (2.2) | 1.000 |
| Recurrent implantation failure, n (%) | 0 (0) | 20 (22.0) | 0.038 |
| Unexplained sterility, n (%) | 2 (12.5) | 30 (36.3) | 0.062 |
| aPL profile | |||
| Subtypes of aPL | |||
| Lupus anticoagulant, n (%) | 8 (50.0) | 17 (18.7) | 0.011 |
| aCL autoantibodies, n (%) | 13 (81.2) | 56 (61.5) | 0.129 |
| IgM | 3 (23.1) | 14 (25.0) | 1.000 |
| IgG | 8 (61.5) | 37 (66.1) | 0.756 |
| IgM+IgG | 2 (15.4) | 5 (8.9) | 0.609 |
| aβ2GPI autoantibodies, n (%)* | 13 (86.7) | 44 (48.4) | 0.006 |
| IgM | 3 (23.1) | 17 (38.6) | 0.346 |
| IgG | 7 (53.8) | 24 (54.5) | 0.965 |
| IgM+IgG | 3 (23.1) | 3 (6.8) | 0.125 |
| aPS/PT autoantibodies, n (%)** | 4 (50.0) | 24 (51.1) | 1.000 |
| IgM | 3 (75.0) | 20 (85.7) | 1.000 |
| IgG | 0 (0) | 1 (4.2) | 1.000 |
| IgM+IgG | 1 (25.0) | 3 (12.5) | 0.481 |
| Number of positive aPL tests | |||
| In patients with aPS/PT determination (n=55): | |||
| Single positive, n (%) | 2 (25.0) | 27 (57.4) | 0.131 |
| Double positive, n (%) | 2 (25.0) | 14 (29.8) | 1.000 |
| Triple positive, n (%) | 1 (12.5) | 4 (8.5) | 0.559 |
| Four positive, n (%) | 3 (37.5) | 2 (4.3) | 0.018 |
| In patients without aPS/PT determination (n=52): | |||
| Single positive, n (%) | 2 (25.0) | 24 (54.5) | 0.248 |
| Double positive, n (%) | 3 (37.5) | 18 (40.9) | 1.000 |
| Triple positive, n (%) | 3 (37.5) | 2 (4.5) | 0.022 |
| aGAPSS *, n (%) |
0.003 |
||
| ≤5 | 4 (26.7) | 61 (67.0) | |
| >5 | 11 (73.3) | 30 (33.3) |
Abbreviations: BMI: body mass index; aβ2GPI: anti-β2 glycoprotein-1 antibodies; aCL: anticardiolipin antibodies; aGAPSS: adjusted Global APS score; aPL: antiphospholipid antibodies; aPS/PT: anti-phosphatidylserine/prothrombin complex antibodies; FGR: fetal growth restriction; NC-OAPS: non-criteria obstetric antiphospholipid syndrome; OAPS: obstetric antiphospholipid syndrome; PE: preeclampsia. * aβ2GPI and aGAPSS was determined in 106 patients (missing data in one with OAPS). ** aPS/PT was determined in 55 patients (missing in 8 patients with OAPS and 44 with NC-OAPS).
Table 3.
Obstetric, maternal, and fetal/neonatal outcomes among subsequent pregnancies in women with OAPS and women with NC-OAPS.
Table 3.
Obstetric, maternal, and fetal/neonatal outcomes among subsequent pregnancies in women with OAPS and women with NC-OAPS.
| OAPS n=24 |
NC-OAPS n=119 |
p value |
|
|---|---|---|---|
| Treatment regimen | |||
| No treatment, n (%) | 0 (0) | 1 (0.8) | 1.000 |
| LDA alone, n (%) | 3 (12.5) | 12 (10.1) | 0.718 |
| LMWH alone, n (%) | 1 (4.2) | 2 (1.7) | 0.426 |
| LDA plus LMWH, n (%) | 20 (83.3) | 104 (87.4) | 0.527 |
| Additional treatments | |||
| Hydroxychloroquine, n (%) | 2 (8.3) | 23 (19.3) | 0.250 |
| Corticosteroids, n (%) | 2 (8.3) | 17 (14.3) | 0.741 |
| ART, n (%) | 6 (25.0) | 55 (46.6%) | 0.070 |
| Treatment doses | |||
| Aspirin 100mg, n (%) | 15 (62.5) | 103 (86.6) | 0.015 |
| Aspirin 150mg, n (%) | 8 (33.3) | 13 (10.1) | 0.009 |
| Prophylactic doses LMWH, n (%) | 15 (62.5) | 92 (77.3) | 0.127 |
| Intermediate doses LMWH, n (%) | 6 (25.0) | 10 (8.4) | 0.030 |
| Therapeutic doses LMWH, n (%) | 0 (0) | 4 (3.4) | 1.000 |
| Corticosteroids ≥10mg/day, n (%) | 1 (4.2) | 13 (10.9) | 0.465 |
| Final pregnancy outcome | |||
| Live births, n (%) | 18 (75.0) | 98 (82.4) | 0.400 |
| Elective medical termination, n (%) | 1 (4.2) | 1 (0.8) | 0.308 |
| Pregnancy loss <10w, n (%) | 5 (20.8) | 18 (15.1) | 0.543 |
| Pregnancy loss 10-24w, n (%) | 0 (0) | 2 (1.7) | 1.000 |
| Pregnancy loss >24w, n (%) | 0 (0) | 0 (0) | NA |
| Obstetric and maternal outcomes | |||
| Deliveries, n | 18 | 98 | |
| Cesarian section, n (%)a | 5 (29.4) | 51 (53.1) | 0.071 |
| Preeclampsia, n (%)b | 3 (16.7) | 5 (5.2) | 0.111 |
| HELLP, n (%)b | 0 (0) | 1 (1.0) | 1.000 |
| Placental abruption, n (%)b | 0 (0) | 1 (1.0) | 1.000 |
| Maternal death, n (%) | 0 (0) | 0 (0) | NA |
| Maternal thrombosis, n (%) | 0 (0) | 0 (0) | NA |
| Postpartum hemorrhage | 0 (0) | 4 (4.6) | 1.000 |
| Fetal and neonatal outcomes | |||
| Neonates, n | n=18 | n=101* | |
| Gestational Age (weeks), mean (SD) | 38.6 (1.88) | 38.791 (2.00) | 0.653 |
| FGR, n (%)c | 0 (0) | 9 (9.0) | 0.351 |
| Preterm birth related to PE/HELLP/FGR, n (%)c | 1 (5.6) | 3 (3.0) | 0.489 |
| <28 weeks | 0 | 1 | |
| 32-33.6 weeks | 1 | 0 | |
| 34-<37 weeks | 0 | 2 | |
| Birthweight (gr), mean (SD) | 3146 (506) | 3050 (550) | 0.491 |
| Low birthweight, n (%)c | 2 (11.1) | 11 (11.5) | 1.000 |
| Neonatal death, n (%) | 0 (0) | 1 (1.0) | 1.000 |
Abbreviations: FGR: fetal growth restriction; HELLP: Hemolysis, Elevated Liver enzymes and Low Platelets; HCQ: Hydroxychloroquine; LDA: low-dose aspirin; LMWH: low molecular weight heparin; NC-OAPS: non-criteria obstetric antiphospholipid syndrome; OAPS: obstetric antiphospholipid syndrome; PE: preeclampsia; w: weeks. a Information for mode of delivery is missing in one woman in OAPS group and two women in the NC-OAPS group. b Data for preeclampsia, HELLP, and placental abruption are missing for two women in the NC-OAPS group. c Information for FGR and preterm birth is missing in one and for low birthweight is missing for five neonates in the NC-OAPS group. *Four twin pregnancies, one of which with loss of one fetus.
Table 4.
Comparison of maternal clinical and laboratory features and treatment regimen in pregnancies resulting in live births and pregnancy losses of unknown cause.
Table 4.
Comparison of maternal clinical and laboratory features and treatment regimen in pregnancies resulting in live births and pregnancy losses of unknown cause.
| PL of unknown cause (n=15) | Live birth (n=116) |
p value | |
|---|---|---|---|
| Demographics and previous obstetric history | |||
| BMI, Kg/m2 | 0.416 | ||
| < 25 | 10 (71.4) | 65 (60.2) | |
| ≥ 25 | 4 (28.6) | 43 (39.8) | |
| Associated autoimmune disease, n (%) | 5 (33.3) | 30 (25.9) | 0.544 |
| Live births before study, n (%) | 4 (26.7) | 26 (22.4) | 0.747 |
| Live births before study if at least one previous pregnancy, n (%) | 4 (28.6) | 26 (26.8) | 1.000 |
| ≥ 4 previous PL | 3 (20) | 10 (8.6) | 0.171 |
| Age at subsequent pregnancy, years, n (%) | 0.385 | ||
| < 35 | 3 (20.0) | 39 (33.6) | |
| ≥ 35 | 12 (80.0) | 77 (66.4) | |
| Diagnosis, n (%) | 0.280 | ||
| OAPS | 4 (26.7) | 18 (15.5) | |
| NC-OAPS | 11 (73.3) | 98 (84.5) | |
| aGAPSS *, n (%) | 0.082 | ||
| ≤ 5 | 12 (80) | 65 (56.5) | |
| > 5 | 3 (20) | 50 (43.5) | |
| Laboratory features | |||
| Subtypes of aPL, n (%) | |||
| LA | 4 (26.7) | 29 (25.0) | 1.000 |
| aCL | 10 (66.7) | 76 (65.5) | 1.000 |
| aβ2GPI * | 5 (33.3) | 67 (58.3) | 0.068 |
| aPS/PT ** | 8 (72.7) | 28 (49.1) | 0.151 |
| Number of positive aPL tests | |||
| If aPS/PT not determined (n=63), n (%) | |||
| Single positive | 3 (75.0) | 28 (47.5) | 0.355 |
| Double positive | 1 (25.0) | 25 (43.1) | 0.633 |
| Triple positive | 0 (0) | 6 (10.2) | 1.000 |
| If aPS/PT determined (n=68), n (%) | |||
| Single positive | 4 (36.4) | 29 (50.9) | 0.378 |
| Double positive | 5 (45.5) | 16 (28.1) | 0.295 |
| Triple positive | 0 (0) | 5 (8.8) | 0.583 |
| Quadruple positive | 2 (18.2) | 7 (12.3) | 0.631 |
| Treatment regimen | |||
| LDA plus LMWH, n (%) | 12 (80.0) | 103 (88.8) | 0.395 |
| LDA alone, n (%) | 3 (20.0) | 9 (7.8) | 0.142 |
| Hydroxychloroquine, n (%) | 2 (13.3) | 19 (16.4) | 1.000 |
| Corticosteroids, n (%) | 2 (13.3) | 15 (12.9) | 1.000 |
| ART, n (%) | 6 (40.0) | 53 (46.1) | 0.656 |
Abbreviations: aβ2GPI: anti-β2 glycoprotein-1 antibodies; aCL: anticardiolipin antibodies; aGAPSS: adjusted Global APS score; aPL: antiphospholipid antibodies; aPS/PT: anti-phosphatidylserine/prothrombin complex antibodies; ART: assisted reproductive technologies; BMI: body mass index; LA: lupus anticoagulant; LDA: low-dose aspirin; LMWH: low molecular weight heparin; NC-OAPS: non-criteria obstetric antiphospholipid syndrome; OAPS: obstetric antiphospholipid syndrome; PL: pregnancy loss. * aβ2GPI and aGAPSS determined in 130 pregnancies. ** aPS/PT determined in 68 pregnancies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



