
Submitted:
01 November 2024
Posted:
05 November 2024
You are already at the latest version
Abstract
Background: In the UK pharmacy professionals (pharmacists and pharmacy technicians) contribute to the delivery of local and national public or population health interventions. Existing literature predominantly focuses on micro-level activities, primarily in community pharmacies typically delivering public health interventions to individuals. Despite their sizeable daily interaction, there is little-known evidence on pharmacy professionals’ (PPs) involvement at meso and macro levels nor to what extent pharmacy professionals have specialist/advanced roles within public health practice. This mixed method study presents recommendations for future action. The study explored pharmacy professionals’ specialist/advanced roles within public health as well as their opportunities and barriers to career development. Method: The study included two surveys (for pharmacy professionals and public health professionals (PhPs)), a call for evidence and two workshops to develop recommendations. Pharmacy professionals (n=128) and public health professionals (n= 54) across the UK participated in the survey. Results: The majority of PP respondents were females (70%); pharmacists (85%), working in primary (33%) or secondary (25%) care settings, mainly based in England (75%), most (63%) lacked formal public health qualifications, although they were involved in a diverse range of public health interventions. The PhPs were mostly females (67%), practicing in England (58%). Both professional groups identified opportunities and barriers to pharmacy professionals' involvement in public health. Almost half or the PhP respondents (44%) stated that they had a pharmacy professional working as part of their current public health teams. Eighty-seven per cent of PhP respondents (45/52) agreed that having pharmacists or pharmacy technicians specialising in public health would be beneficial or very beneficial. Most documents, reports, case histories provided through the call for evidence were unpublished. The workshops generated 94 recommendations, highlighting collaboration and the need to acknowledge pharmacy professionals' contributions to public health. Conclusion: The recommendations for action had three main themes: national strategic approach and commissioning, workforce development and further pharmaceutical public health evidence reviews research.
Keywords:
pharmacy
; pharmacoequity
; health inequalities
; Emergency Preparedness Resilience and Response
; community pharmacy
; policy
1. Introduction
Pharmacy professionals (pharmacists and pharmacy technicians) have an increasing role in improving the health and wellbeing of populations and communities. Currently, pharmacy colleagues work across the three core domains of public health practice [1]: health improvement, health protection and healthcare public health (Box 1), informing population care beyond individual health outcomes (Figure 1). Pharmaceutical Public Health (PPH) was first defined in the literature in 2000 as “the application of pharmaceutical knowledge, skills and resources to the science and art of preventing disease, prolonging life, promoting, protecting, and improving health for all through organised efforts of society” [2]. At the time, Walker recognized that “Pharmaceutical Public Health is a real value-added role that the profession has, to date, chosen not to exploit” [2].
Walker’s observation is reflected in the relatively narrow focus of the literature on PPH. Mulvale and colleagues organized contextual factors as an interrelated set of policy (macro), organizational (meso), team (micro) and individual factors [3]. Over the years, the available literature on the pharmacy professions public health function has predominantly focused on the contribution of community pharmacy and pharmacists’ delivering public health interventions to individuals, through micro-level activities such as health promotion, secondary prevention measures through medicines management and prescribing advice, rather than on population health or broader public health interventions more broadly [4]. Community pharmacies are frequently located in some of the most deprived and challenging communities, providing daily contact for individuals seeking ad hoc and unplanned health advice alongside collection of prescribed medicines or purchasing over the counter health related products [5,6]. In England, there are over 1.2 million daily health-related visits to community pharmacies. This presents an important opportunity to support behavioural change at an individual micro level. However there are also opportunities for community pharmacy teams as well as pharmacy professionals across all sectors to address wider societal aspects of public health at meso and macro levels [3,5,6].
An evidence gap currently exists that describes the involvement of pharmacy professionals working at the meso and macro levels. The meso level involves partnership working and involvement in community support networks (group/institution level); the macro level, involves influencing and working within local, regional and national governments on complex agendas such as tackling health inequalities and implementing health policies (Figure 2). Involvement at these broader levels requires advanced public health skills in addition to pharmacy specialty skills.
In the UK, key population health policies include the following: in England the NHS Long term plan, including the development of integrated care systems (ICSs) and integrated care boards (ICBs) and primary care networks (PCNs); in Scotland the Public Health Priorities for (2018); in Northern Ireland ‘Making Life Better—a whole system framework for public health (2013-23) and in Wales A Healthier Wales: Long Term Plan for Health and Social Care [7,8,9,10]. These policies have the clear aim to improve the health and wellbeing of the UK population by bringing together multi professional groups, including pharmacy professionals, to coordinate care better.
Box 1. Definitions of public health, domains of public health and population health.
Public Health is defined as “the art and science of preventing disease, prolonging life and promoting health through the organized efforts of society”
Health protection is the protection of individuals, groups and populations through the effective collaboration of experts in identifying, preventing and mitigating the impacts of infectious diseases and of environmental, chemical and radiological threats.
Healthcare public health is concerned with the application of population sciences to the design, organisation, and delivery of healthcare services, with the ultimate aim of improving population health.
Health improvement is concerned with assessment of population health needs, and commissioning and evaluating health programmes and initiatives to promote healthy behaviours. These include improving nutrition, physical activity, sexual health, substance use, disease prevention, and the importance of vaccinations.
Population health is an approach aimed at improving the health of an entire population. It is about improving the physical and mental health outcomes and wellbeing of people, whilst reducing health inequalities within and across a defined population. It includes action to reduce the occurrence of ill-health, including addressing wider determinants of health, and requires working with communities and partner agencies.
This evidence review (commissioned by the UK Chief Pharmaceutical Officers in 2020,) aimed to address the UK national policy direction publications [7,8,9,10] and pharmacy professionals’ specialist public health contributions. It aimed to assess the barriers and opportunities to contributions at meso and macro levels of public health, and to mak recommendations for future action. The overall aim was to provide evidence as part of the national policy directions on the PPs role in population and public health.
2. Methods
2.1. Survey of Pharmacy and Public Health Professionals—Overview and Data Analysis
Two independent cross-sectional electronic surveys were developed, piloted, and deployed to pharmacy and public health specialists via email and social media cascades. The surveys explored the extent to which pharmacy professionals are involved in public health roles, including barriers and opportunities encountered.
A combination of purposive and convenience sampling was employed to identify pharmacy and public health professionals in all of the four UK nations (England, Scotland, Wales and Northern Ireland).
The surveys (Supplementary Material 1 and 2) were developed by pharmacist researchers with experience and advanced skills in public health and a public health professional (authors—DAO, UO, EW, CN, RO, MB, AE, CP, CG), after an extensive literature review and regular meetings to assess the survey questions. The surveys were pilot-tested and reviewed by the study researchers and independent researchers. The surveys were revised following feedback from reviewers. Independent researchers outside the core project team researchers and convenience sampling of participants with similar demographics to intended participants (8 pharmacists and 14 public health professionals) were asked to pilot test the survey to ensure clarity; revisions were made based on feedback.
The links to the surveys were disseminated via social media platforms (including LinkedIn, Twitter (X), and WhatsApp), also via email to universities with public health courses and public health offices at acute trusts; in addition they were disseminated via telephone calls and directed contact to professional colleagues. The survey for public health professionals was also disseminated by the Faculty of Public Health and the Association of Directors of Public Health through email and newsletter cascade routes.
The questions comprised mainly closed-ended multiple choice questions, alongside questions that allowed for open-ended responses inviting additional insights. Respondents were asked to append links to previously published relevant work. Data responses were collected anonymously, although survey respondents could voluntarily provide their name and email address via a separate link at the end of the survey, with personal information disaggregated from their survey responses. This allowed these individuals the opportunity to join a network of pharmacists with interest and experience in public and population health.
Survey data was imported into Microsoft Excel for analysis. The response rate was not calculated since information was not available on the number of unique individuals who viewed or initiated the survey. Descriptive statistics were used to summarise the quantitative data collected. Missing data was excluded from analysis. Open-ended free text responses were analysed using inductive content analysis.
All data were stored securely in line with the General Data Protection Regulation 2016/679.
2.1.1. Survey of Pharmacy Professionals
The intended audience for the pharmacy survey were pharmacy professionals (pharmacists and pharmacy technicians) across all four UK nations. The survey included 32 questions and remained open for responses over a 4-week period (25th June 2021 till 27th July 2021).
The objectives of the pharmacy professionals survey were to:
- ▪
- Explore the number of pharmacy professionals who have experience in leading public/population health projects or have completed/are undertaking additional public/population health training.
- ▪
- Explore the context in which pharmacists are currently involved in public/population health related roles (excluding nationally commissioned public health services through community pharmacy),
- ▪
- Understand the drivers and barriers associated with pharmacists undertaking public/population health roles.
The pharmacy professional survey elicited participant demographics, public/population health qualifications and public/population professional experience, including barriers and facilitators to undertaking advanced public/population health roles, and public health projects they had been involved in. In addition, participants were asked how the projects were disseminated. The survey included a comment box to provide further details about the projects and how to access the published information about the projects.
2.1.2. Survey of Public Health Professionals
The intended audience for the public health professionals survey were public health specialists, registrars and public health practitioners. The survey included 35 questions and remained open for responses over a 6-week period (15th September till 27th October 2021). All participation was voluntary.
The objectives were to seek the views of public health professionals on:
- The potential functions of public health that can benefit from pharmacists’ unique expertise including access to care, prevention services as well as pharmacotherapy, pharmacoepidemiology and economics,
- The contributions of pharmacy professionals to public/population health (in addition to traditionally/nationally commissioned community pharmacy services) that they were aware of in the four UK nations.
The public health professional survey elicited participant demographics, their experience of working with pharmacy professionals, examples of how correct and efficient use of medicines currently or previously had arisen as an area of challenge or consideration. The survey also requested their perceptions of the benefits, barriers and opportunities of pharmacists/pharmacy technicians specialising in public health and areas of public/population health they felt would benefit having individuals with pharmacy backgrounds working directly as part of the public health team.
The conduct and reporting of the study adhered to the Consensus-Based Checklist for Reporting of Survey Studies (CROSS). The completed CROSS checklist is available as supplementary information
2.2. Call for Evidence
A call for evidence questionnaire (Supplementary Material 3) was sent by the Project Lead (DAO) on 25 June 2021 via email to key stakeholders who held senior pharmacy related positions in the UK for further cascade. The questionnaire was designed to identify any published or unpublished reports, documents, or case histories related to PPH. In addition, they were asked to give examples of pharmacists in the UK who have received public health training or had experience working at a strategic level and influencing population health in UK. To optimise responses, additional reminders were sent and an extension until 16 July was sent out on 5th July 2021 (initial deadline).
The evidence received from published or unpublished reports, documents or case histories was collated via the questionnaire and was used to classify all findings under one of 8 topic headings:
- National Strategic Approach
- Expanding Service Delivery within Community Pharmacy
- Expanding Service Delivery beyond Community Pharmacy
- Embedding Optimisation of Medicines at a Population Health Level
- Emergency Preparedness, Resilience and Response
- Integration of Pharmacy to Better Support Public Health Protection & Improvement Goals
- Public Health Skills and Training
- Mitigating Health Inequalities
Findings were shared via two workshops, each with a selected group of stakeholders, to promote discussion and help clarify questionnaire responses.
2.3. Workshops
Two workshops were held with key stakeholders on 16 July 2021 and 02 September 2021. The first workshop included the participation of key stakeholders in a presentation and discussion regarding the mixed method review, a literature review, key findings and interim survey and call for evidence findings.
Ahead of the second workshop, a slide set summary of the literature review and interim results of the two surveys and call for evidence were sent to invitees, with a request via a Slido tool to recommend how to steer national changes to improve pharmacy professionals’ contribution to public health across the four UK nations, in addition to what already existed as commissioned community pharmacy services. These recommendations were further discussed at the workshop (Supplementary box 1 includes the workshop agenda) and each participant was asked to share which one recommendation they deemed most important regarding the involvement of pharmacy professionals in PPH.
2.4. Ethics Approval and Consent
Ethical approval was not required according to the NHS Health Research Authority tool, the surveys aimed to evaluate through exploration specialist contributions of pharmacy professionals to national policies/direction on public health. Consent was sought from all participants and anonymity of contributions provided.
3. Results
3.1. Survey of Pharmacy and Public Health Professionals
3.1.1. Survey of Pharmacy Professionals
3.1.1.1. Demographics
A total of 128 pharmacy professionals (85% pharmacists) responded from the four UK nations (n=96 (England), n=13 (Scotland), n=9 (Wales), n=9 (Northern Ireland) and n=1 (stated Great Britain)) (Table 1). Respondents were predominantly female (70%; 90/128); 27% (35/128) were male and 3% (3/128) preferred not to say. Most were of white British background (48%; 62/128), 14% (19/128) were Asian or Asian British, 12% (14/128) were Black or Black British. Within England, most respondents worked in the South East (20%; 20/96)), while 19% (18/96), 17% (17/96) and 11% (11/96) worked in Midlands, London and North East and Yorkshire respectively. Regions that were represented in lower proportions included the Southwest, North West and East of England.
Respondents worked in a range of sectors including primary care, secondary care, health boards, public health bodies, community pharmacies, local authority and health and justice settings (Figure 3). Many respondents (33%; 43/128) worked in the primary care setting and 25% (33/128) in the secondary care setting. Thirteen per cent (16/128) stated they worked across both the community setting and public health bodies. Eighty-five per cent (109/128) of survey respondents stated their role was a pharmacist, while 15% (19/128) stated pharmacy technician. No trainees (pharmacists or pharmacy technicians) responded to the survey.
3.1.1.2. Public Health Qualifications and Motivation
Most of the respondents (63%, 80/128) had no formal public health qualification, 27% (34/128) had formal public health qualification, and the remaining 10% (14/128) had a qualification in progress. For those who held a public health qualification, the year of qualification ranged from one to 49 years ago. One respondent was a Fellow of the Faculty of Public Health and another was a member of the Royal Society of Public Health. In response to the question “How long have you been using your public health qualification or skills within role(s)?”, over half (55.2%, 16/29) answered they had been using their public health qualifications or skills within their roles for five or more years, 20.7% (6/29) had not used their qualification nor skills, and 13.8% (4/29) and 10.3% (3/29) had used their qualifications or skills for three to four years and one to two years respectively.
The public health education modules most often completed by pharmacy professionals (most commonly as part of a Masters in Public Health course) were health improvement/promotion (12%, 15/128), epidemiology (12%, 15/128), health policy (11%, 14/128), infectious and tropical diseases (10%, 13/128), health services (10%, 13/128), global health/global health policy (110%, 3/128), health systems (10%, 13/128), health economics (0.1%, 2/128), climate change (0.1%, 1/128) and community pharmaceutical public health (0.1%, 1/128).
When respondents were asked what best described their motivation for undertaking an additional public/ population health qualification(s), 31% (17/55) selected an ambition to work in public health as a pharmacy professional, 29% (16/55) selected ambition to work in public health as an alternative career to pharmacy. About a third 27% (15/55) also selected that it was completed for general interest, seven per cent (4/55) and 4% (4/55) of the respondents stated that their motivation was based on recommendations received and qualification required for their roles, respectively, while 2% (1/55) of respondents did not identify a specific motivation.
3.1.1.3. Public Health Experience
Within public health, pharmacy professionals were involved in various non-COVID-19 related public health areas as shown by Figure 4. Over 70% of respondents were involved in antimicrobial stewardship activities to tackle antimicrobial resistance, managing long term conditions, health improvement and data analysis/statistics before and since the COVID-19 pandemic. The proportion of respondents that were engaged in the development of Pharmaceutical Need Assessments** was 31% (21/68) before, and 4% (3/68) since the pandemic and for health inequalities this was 16% (9/57) pre and 10% (6/57) since the pandemic.
Pharmacy professionals respondents had conducted diverse public health projects. Forty per cent (69/174) of pharmacy professionals had not shared project findings beyond their organisation;18% (32/174) had their project findings disseminated during conference presentations and abstracts, 16% (28/174) via guidance, protocols or Patient Group Directions (PGDs) and 11% (20/174) as peer review publications. Eight per cent (13/174) and 7% (12/174) of respondents had their findings published in non peer-reviewed publications or as blogs and online reports respectively.
3.1.1.4. Barriers and Opportunities
Most respondents to the question on barriers (71%; 89/126) believed there are barriers for pharmacy professionals to engage in public and population health, 23% (29/126) of the respondents believed there might be barriers for pharmacy professionals to public and population health engagement and only 6% (8/126) did not believe barriers exist for pharmacy professionals to get involved in public and population health.
Eight key themes were identified from the barriers provided by respondents (Table 2). The highest number of comments mentioned as a barrier to PPH related to limited career opportunities or no defined career pathway.
Most respondents (80%; 102/127) believed opportunities exist for pharmacy professionals to engage in public and population health. Six themes were identified as opportunities for pharmacy professionals to engage in public or population health (Table 3). The most popular theme was that pharmacy professionals are well placed to make a public health impact.
There were specific barriers and opportunities highlighted by pharmacy technician respondents (Supplementary Box 2 and 3). The main barrier reported by pharmacy technicians was an underuse of skills. Technicians also remarked on a lack of professional accreditation which resulted in a gap in service provision.
3.2. Survey of Public Health Professionals
A total of 54 public health professionals participated in the survey; 67% (36/54) were female, 30% (16/54) male and 3% (2/54) preferred not to say (Table 4). Most respondents (59%, 32/54) were practising in England, 28 (15/54) in Scotland and 13% (7/54) in Wales. Participants worked in a range of roles, 19% (10/54) were public health consultants, 9% (5/54) directors of public health, 11% (6/54) public health registrar ST4-5 and 13% (7/54) public health registrar ST1-3.
Almost half of the public health participants (44.4%, 24/54) reported they had pharmacy professionals as part of their current public health team. Fifty-two per cent (27/52) stated that they were aware of a pharmacy professional who was also a public health professional; example of roles included public health partnerships and improvement leads, chief pharmacist for Public Health Scotland, pharmacists guiding the analysis of national prescribing data and production of official statistics and ad hoc reports, lead antimicrobial resistance pharmacists.
Twenty-one per cent (10/54) of respondents agreed that their organisation would be willing to provide a placement to a funded pharmacy professional to undertake a secondment or fellowship in public health, whereas 12.8% (6/54) of respondents did not agree to provide a placement. A third (34%; 16/54) of respondents stated that their organization may possibly provide a placement.
Over half of respondents (54%; 27/54) stated the challenge of ensuring efficient medicine use in patient cohorts for the 12 months prior to the COVID-19 pandemic.
In England, more than half of the respondents (57%) stated that their public health teams had contributed to a pharmaceutical needs assessment (PNA) in the previous 5 years. Of which, 47% stated that a pharmacy professional was part of the public health team and 40% did not know. In Scotland, Wales and Northern Ireland, the survey captured the involvement of pharmacy professionals in the public health reports or delivery strategies, with a variable response across nations in the engagement of pharmacy professionals in reports.
Respondents were also asked what level of experience or qualification was required for a pharmacy professional who wants to focus on medicines or pharmacy-related public health activities. Almost half (43%; 13/29) specified a Masters in Public Health, two specified credentials at a consultant level by a public health or pharmacy professional body (Box 2).
Box 2. Examples of comments on level of experience or qualification required for a pharmacy professional who wants to focus on medicines or pharmacy-related public health activities.
“Bachelors degree standard public health qualification or masters modules in public health pertaining to determinants of health, inequalities, health economics (not necessarily the whole masters but perhaps a certain count of credits across key modules)”
“I think this would depend on what they were being asked to do however probably working towards masters in public health.”
“MPH and working toward UKPHR if not on formal training scheme.”
“MSc Pharmacy and MPH as minimum also at Royal Pharmaceutical Society consultant pharmacist ready status.”
Postgraduate qualification incorporating at least one module on public health or a public health related area. There are certain vocational aspects in healthcare where things can be learned on the job e.g., clinical practice, however in public health you need to know fundamentals and these are best taught in an academic context.
3.2.1. Benefits and Barriers to Specialist Roles for Pharmacists in Public Health
Eighty-seven per cent of public health professional respondents (45/52) agreed that having pharmacists or pharmacy technicians specialising in public health would be beneficial (37%) or very beneficial (50%), 13% agreed that it would be somewhat beneficial (Table 5 and Box 3). Respondents selected several areas of public health where they believed direct benefits would be realised and achieved by having direct involvement of pharmacy professionals. There were 15 areas that over a third of respondents selected as their top five areas (Figure 5), the top one being antimicrobial resistance/stewardship.
Example quotes from respondents are provided in Box 3.
Box 3. Examples of quotes from respondents on benefits of having pharmacy professionals as part of public health teams.
“Pharmacy professionals’ knowledge of medicines and medicines use is second to none. This knowledge could be utilized to analyse medicines use data and the development of public health strategies and campaigns. There are several areas within public health where the expertise of a pharmacy professional would be beneficial including vaccination, antimicrobial stewardship, smoking cessation, weight loss management and substance misuse. Within health institutions multi-disciplinary working is fully embedded and the role of the pharmacy professional is appreciated but the same system of working has not been established within public health.”
“They can bring knowledge of pharmacoeconomic, understanding of how pharmacy services are delivered in the community to the wider population, an independent prescriber would have the authority to help deliver health protection interventions e.g., managing outbreaks”
“Pharmacies are ideally placed to provide local people with information to support behaviour change and start them on their journey to improved H&WB. Health campaigns are promote via pharmacy a lot, this model could be used to support behaviour change through e.g., increased physical activity, signposting, raising the issue of PA or Healthy Weight, greenspace access etc”
Sixty per cent of respondents (30/50) believed there are barriers for pharmacy professionals to get involved in public or population health, while 26% (13/50) believed that there are no barriers for pharmacy professionals. Very few participants (4%;2/50) were unsure. (Table 6).
3.2.2. Call for Evidence
Forty-five stakeholders responded to the call for evidence. Sixty-nine per cent (n=31) were from England, 18% (n=80) from Northern Ireland, 9% (n=4) from Scotland and 4% (n=2) from Wales.
Most documents, reports and case histories identified were unpublished, and the case histories varied in detail. The number of papers identified by the respondents across each of the eight topic headings are illustrated in Figure 6. The majority of papers (n=21) related to expanding service beyond community pharmacy (CP), followed by expanding service delivery within CP (n=12). Fewer papers were identified for public health skills training (n=7), embedding optimisation of medicines at population level (n=8) and mitigating health inequalities (n=9).
3.3. Workshops to Generate Recommendations
The first workshop was attended by 12 people and the second workshop by 42 people. Seven attendees from the first workshop also attended the second workshop. From these two workshops, 94 recommendations were proposed and grouped under 8 themes (Table 7). For the full list of recommendations see Supplementary Material 4.
4. Discussion
The findings from this exploratory evidence review showcase the scope of existing PPH and further opportunities for pharmacy professionals to make substantial contributions in the public health landscape. In Griffiths et al., the importance of a varied skill mix within public health was highlighted, stating that “different levels of skill and a wide range of contributions are needed if public health programmes are to make the most impact” [11]. The WHO-ASPHER Competency Framework for the Public Health Workforce in the European Region stands as a cornerstone and valuable resource that offers comprehensive insights into skill mix for competent public health teams. Through their training, pharmacy professionals possess skills that align with all ten of the competency categories outlined by the WHO ASPHER framework [12]. Additionally, collaborative public health efforts between healthcare professionals are highlighted within the UK Faculty of Public Health Functions and Standards of a Public Health System [28] and the Royal Society of Public Health’s Unlocking the Potential of the Wider Public Health Workforce report [29].
The majority of pharmacy professionals surveyed do not hold a formal qualification in public health, and cited inadequate public health knowledge as a substantial barrier to further PPH involvement. Concurrently, the public health professionals surveyed stated that they would expect qualifications to be available for pharmacy professionals, such as public health Masters courses or postgraduate modules in public health related areas (e.g., health economics, health inequalities). As a result, the clear need for dedicated PPH training and system wide leadership is required to fully unlock the involvement of pharmacy professionals for population level benefits.
The barriers and opportunities identified in this study can be categorised as macro-, meso- or micro-level factors, as per an established socio-institutional framework previously used to examine how healthcare professionals expand scope of practice [13]. This framework helps recognise the opportunities that decision-makers have at each level to encourage more effective collaboration in interprofessional care teams [15]. Macro factors include professional regulation, education, funding, and provider payment schemes [17–23]. Meso factors include organisational structure, rewards, and information systems. Micro factors include processes based on mutual trust, and power-sharing that reflects knowledge and experience rather than titles [24,25,26]. and individual factors such as maturity in one’s profession and attitudes toward collaborative practices [27]. The delicate interactions between factors at all three levels shed light on the interconnectedness which is crucial for shaping and enabling collaborative practices within the ever-evolving public health landscape.
From our study, macro-level barriers as well as lack of pharmacy representation in public health domains coincide with the recent change in the UK healthcare landscape, policies such as the NHS Long Term Plan for England and the impact of the COVID-19 pandemic. In the wake of the pandemic, there are clear opportunities within the field of PPH.
Analysing the meso-level barriers and opportunities, the focus was on issues within local institutions and the wider community. Meso-level barriers identified by pharmacy professionals included organisational and structural barriers, a deficit in training and support, inadequate professional recognition and limited time and/or financial resources for pharmacy professionals to develop more advanced skills in public health. Meso-level opportunities were identified by at least half of the public health professional survey respondents, who had either previously or presently encountered pharmacy professionals working as members of public health teams or organisations. Additionally, over a third of respondents acknowledged 15 public health areas where pharmacy professionals could directly add value through the strategic position of pharmacy professionals in the community and good public health perception.
The micro-level barriers of day-to-day practice emphasised the limited career prospects and absence of defined career pathways for pharmacy professionals within the public health sector. This perceived lack of job opportunities also emphasizes the broader issue of scarce recognition of core knowledge, skills and qualifications pharmacy professionals bring to the public health sector.
The eight main themes identified from the proposed recommendations, outline the potential multifaceted nature of pharmacy professionals’ roles within the public health setting. Recently Todd and Ashiru-Oredope proposed that the definition of pharmaceutical public health is updated to include health inequalities. Suggesting the following definition: ‘the application of pharmaceutical knowledge, skills and resources to the science and art of preventing disease, prolonging life, promoting, protecting, improving health and reducing health inequalities for all through organized efforts of society’ [30]. A knowledge of the barriers and opportunities that pharmacy professionals face in public health can serve to advance and optimise their contributions in all themed areas.
Consensus from the emerging themes of both the surveys and rapid review findings highlighted the contribution pharmacy professionals can make to public health at all levels. There appears to be strong support from public health professionals regarding the impact and benefits of working in partnership with pharmacy professionals with advanced public health knowledge and skills, either directly or as part of a multidisciplinary public health team. As the health and care sector face intense challenges exacerbated by a declining labour pool, innovative and diverse roles within both the public health and pharmacy sectors can serve to unlock hidden potential [14].
Further grouping the eight themes, hidden potential can be focused on the macro-level of national strategic approach and commissioning, the meso-level pertaining to training and workforce development and the micro-level of individual development and involvement in research. Recent scoping reviews have proposed pharmaceutical public health competences for pharmacists [31,32]. There is currently a gap in the literature for pharmacy technicians. Recent qualitative study including pharmacists from Australia, United Kingdom, Canada and the United States of America, and Australia concluded that development strategies are required to be more effective in integrating public health approaches into pharmacy professional practice and for them to be recognised for their public health-related roles [33].
One of the main limitations of the study was the low response. However, the consensus from the themes emerging from both surveys’ findings highlighted the significant contribution pharmacy professionals make to the public health despite the barriers. Future qualitative studies should be considered to investigate and identify how to best resource advanced PPH resources.
4.1. Recommendations for Action
Using the findings of this mixed-methods exploratory study (surveys, call for evidence, workshops), overall recommendations for action to advance the public health skills of pharmacy professionals are grouped as follows:
National Strategic Approach and Commissioning
- Clearer regional and national leadership is required, defining standards and career pathways for pharmacy professionals in public health, with a robust competency framework and accreditation.
- Review of relevant regulations such as the Pharmaceutical Needs Assessment (PNA) regulations in UK would ensure that the emerging role of pharmacy professionals in public health is highlighted, and that data is formally collected as part of the PNA process.
- Setting priorities for public health contributions from pharmacy professionals in areas with limited pharmacy input, such as in emergency preparedness and planning, health protection, medicines surveillance and interventions, integration of primary, secondary and tertiary care, and health inequalities—the latter particularly in areas with a high population of underserved communities.
Workforce Development
- Defining a PPH career pathway will allow pharmacy professionals to remain within the profession whilst contributing or leading on public health matters, including at strategic levels. Within undergraduate and postgraduate programmes, public health competencies can be embedded within the curricula, such as undergraduate foundation modules or public health components in clinical and prescribing courses.
- Promoting specialism in PPH, for example in the UK through the Royal Pharmaceutical Society’s consultant credentialing and/or joint recognition or registration with the General Pharmaceutical Council and Faculty of Public Health (or UKPHR) would be a strong step to validating pharmacy professionals pursuing this avenue. For pharmacy technicians and pharmacy support staff, embedding PPH within their respective training courses would highlight the importance of pharmacy involvement in this area.
- Training programme for pharmacy professionals should include options to undertake public health activities, including health policy, wider determinants of health and financial drivers of population health. Constructing an effective professional development network will provide peer support and continual workforce development.
Evidence Development and Research
- Promoting the sharing of good PPH practice models and increasing the dissemination and adoption of research, audits and project findings by individuals will strengthen the PPH community. For high quality research, creating funding mechanisms for PPH with in turn promote involvement and collaboration in public health spheres.
5. Conclusions
This study highlights the multifaceted nature of pharmacy professionals’ roles within public health. The involvement of pharmacy professionals in public health aligns with global competency frameworks and public health standards. Barriers and opportunities to PPH involvement were analysed and categorised through a socio-institutional lens, spanning macro to micro-level factors. Recommendations to advance pharmacy professional involvement in PPH include their involvement with national strategic approach and commissioning, workforce development and further pharmaceutical public health evidence reviews and research.
Against the backdrop of an ever-changing healthcare landscape, shaping a transformative future for PPH must recognise, address, and leverage the interwoven factors at macro-, meso- and micro-level to identify innovative solutions that will unlock the full hidden potential of pharmacy professionals within public health and pharmacy sectors. Future qualitative studies should investigate and identify how to best utilise advanced PPH resources for the benefit of populations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Diane Ashiru-Oredope; Data curation, Diane Ashiru-Oredope, Eleanor J Harvey, Emma Wright, Uju Okereke and Cecilia Pyper; Formal analysis, Diane Ashiru-Oredope, Roeann Osman, Adeola H Ayeni, Eleanor J Harvey and Cecilia Pyper; Funding acquisition, Diane Ashiru-Oredope; Investigation, Diane Ashiru-Oredope; Methodology, Diane Ashiru-Oredope, Roeann Osman, Eleanor J Harvey, Emma Wright, Christina Narh, Uju Okereke, Tasmin Harrison, Christopher Garland, Cecilia Pyper, Andrew Evans and Marion Bennie; Project administration, Diane Ashiru-Oredope; Supervision, Andrew Evans and Marion Bennie; Validation, Christopher Garland, Andrew Evans and Marion Bennie; Writing—original draft, Diane Ashiru-Oredope, Adeola H Ayeni, Christina Narh and Cecilia Pyper; Writing—review & editing, Diane Ashiru-Oredope, Roeann Osman, Adeola H Ayeni, Eleanor J Harvey, Maria Nasim, Emma Wright, Christina Narh, Uju Okereke, Tasmin Harrison, Christopher Garland, Cecilia Pyper, Andrew Evans and Marion Bennie.
Funding
This project was funded in 2020 by the Chief Pharmaceutical Officer, NHS England on behalf of the Chief Pharmaceutical Officers across all four UK nations.
Institutional Review Board Statement
Ethical approval was not required for the studies involving humans because according to the NHS Health Research Authority tool, the surveys aimed to evaluate through exploration specialist contributions of pharmacy professionals to public health. Consent was sought from all participants and anonymity of contributions provided. . The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
Contributors to the development of the scope, workshops, discussions and recommendations: Ade Williams, Alison Hemsworth, Andrew Evans, Andrew Radley, Angela Kam, Angela Timoney, Anne Everden, Anisha Soni, Barry Melia, Brian McKenna, Catherine Duggan, Catherine Goudy, Cecilia Pyper, Christina Narh, Christopher Garland, Clair Huckerby, David Onuoha, Diane Ashiru- Oredope, Duncan Jenkins, Eleanor Harvey, Elizabeth Beech, Elizabeth (Beth) Ward, Emma McClay, Glenda Fleming, Gul Root, Hazel Marsden, Helen Creighton, Jackie Lamberty, Joanne Coleman, Joanne Linton, Joe Bush, Kate Lees, Kieran Hand, Kweku Bimpong, Mar Estupinan, Marian Salek, Marion Bennie, Matthew Dolan, Michelle O’Prey, Natalie Dean, Natasha Callender, Nicholas Reid, Nick Haddington, Richard Cattell, Richard Seal, Roeann Osman, Shane Williams, Sharon Pfleger, Stephen Brown, Stephen Doherty, Steve Maddern, Sue White, Trevor Beswick, Uju Okereke, Wasim Baqir, Ian Heslop, Adam Todd. Contributors of Case histories and call for evidence: Alifia Chakera, Alison Freemantle, Andrew Evans, Andrew Smith, Beth Ward, Brendan Moore, Brian MacKenna, Cairine Gormley, Caitlin Nelson, Catherine Tucker, Catherine Watkinson, Christopher Garland, Claire Jones, Clair Huckerby, Donna Seaton, Diane Ashiru-Oredope, Duncan Jenkins. Elizabeth Beech, Emma McClay, Ewan Maule, Fazal Rahman, Glenda Fleming, Graeme Hood, Gul Root, Hayley Berry, Heidi Wright, Hels Bennett, Hilary Millar, Julia Parascandolo, Kerry Street, Marcus Rattray, Marion Bennie, Michael Ogilby, Michelle Roberts, Natasha Callender, Nik Reid, Rosemary Allgeier, Rosie Taylor, Samrina Bhatti, Sarah Marshall, Shirley Walker, Sonal Mehta, Stephen Slaine, Suzanne O’Sullivan, Una Convery, Wasim Baqir, Yeyenta Osasu. Faculty of Public Health and Association of Directors of Public Health are acknowledged for their support in cascading the survey to public health professionals. In addition, FPH’s Health Protection, Health Services, Health Improvement and Academic & Research Committees and UK People in Health Group are acknowledged for their feedback on the findings presented at their committee meetings between March and July 2022 (Supplementary box 2). This manuscript is significantly expanded versions of abstracts and posters presented at the Royal Pharmaceutical Society Conference November 2022 and Public Health Science: A National Conference November 2023 [34,35]
Conflicts of Interest
The authors declare no conflicts of interest The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- John Coggon, What Is Public Health? (London: Faculty of Public Health, 2023. https://www.fph.org.uk/what-is-public-health/.
- Walker, R. Pharmaceutical public health: the end of pharmaceutical care? Pharm J 2000;264:340–1.
- Mulvale, G., Embrett, M. & Razavi, S.D. ‘Gearing Up’ to improve interprofessional collaboration in primary care: a systematic review and conceptual framework. BMC Fam Pract 17, 83 (2016). [CrossRef]
- Stokes G, Rees R, Khatwa M, Stansfield C, Burchett H, Dickson K, Brunton G, Thomas J. Public health service provision by community pharmacies: a systematic map of evidence. https://eppi.ioe.ac.uk/cms/Default.aspx?tabid=3753 (accessed 28 October 2024).
- Root G, Varney J. Pharmacy: a way forward for public health. Opportunities for action through pharmacy for public health. Public Health England: London, UK. 2017:1-53.
- Todd A, Copeland A, Husband A, Kasim A, Bambra C. The positive pharmacy care law: an area-level analysis of the relationship between community pharmacy distribution, urbanity and social deprivation in England. BMJ Open. 2014 Aug 12;4(8): e005764. [CrossRef]
- National Health Service. The NHS long term plan London NHS; 2019 https://www.longtermplan.nhs.uk/publication/nhs-long-term-plan/ (Accessed 6 Oct 2023).
- Scottish Government. Scotland’s public health priorities. 2018 https://www.gov.scot/publications/scotlands-public-health-priorities/ (Accessed 6 Oct 2023).
- Department of Health, Northern Ireland. Making Life Better—a whole system framework for public health. 2014 https://www.health-ni.gov.uk/publications/making-life-better-strategy-and-reports (Accessed 6 Oct 2023).
- Welsh Government. A Healthier Wales: Long Term Plan for Health and Social Care (Wales). 2021 https://www.gov.wales/healthier-wales-long-term-plan-health-and-social-care (Accessed 6 Oct 2023).
- Griffiths S, Jewell T, Donnelly P. Public health in practice: the three domains of public health. Public health. 2005 Oct 1;119(10):907-13. [CrossRef]
- World Health Organization. WHO-ASPHER competency framework for the public health workforce in the European region. World Health Organization. Regional Office for Europe; 2020. https://iris.who.int/handle/10665/347866 (accessed 06 Oct 2024).
- Mulvale G, Embrett M, Razavi SD. ‘Gearing Up’to improve interprofessional collaboration in primary care: a systematic review and conceptual framework. BMC family practice. 2016 Dec;17(1):1-3.
- McConkey R. The Health Foundation-Technical annexes A–G: NHS workforce projections 2022. https://www.health.org.uk/publications/nhs-workforce-projections-2022 (accessed 28 October 2024).
- Zwarenstein M, Goldman J, Reeves S. Interprofessional collaboration: Effects of Practice-based Interventions on Professional Practice and Healthcare Outcomes. Cochrane Database Syst Rev. 2009;3:CD000072.
- Petrelli F, Francesco T, Scuri S, Cuc NT, Grappasonni I. The pharmacist’s role in health information, vaccination and health promotion. Annali Di Igiene Medicina Preventiva E Di Comunità. 2019;31(4):309-15.
- Thomson K, Hillier-Brown F, Walton N, Bilaj M, Bambra C, Todd A. The effects of community pharmacy-delivered public health interventions on population health and health inequalities: a review of reviews. Preventive Medicine. 2019 Jul 1;124:98-109. [CrossRef]
- Mossialos E, Courtin E, Naci H, Benrimoj S, Bouvy M, Farris K, Noyce P, Sketris I. From “retailers” to health care providers: Transforming the role of community pharmacists in chronic disease management. Health Policy. 2015 May;119(5):628-39. [CrossRef]
- Garber J, Downing D. Perceptions, Policy, and Partnerships: How Pharmacists Can Be Leaders in Reducing Overprescribing. Sr Care Pharm. 2021 Mar 1;36(3):130-135.
- Maidment I, Young E, MacPhee M, Booth A, Zaman H, Breen J, Hilton A, Kelly T, Wong G. Rapid realist review of the role of community pharmacy in the public health response to COVID-19. BMJ Open. 2021 Jun 16;11(6): e050043. [CrossRef]
- Aruru M, Truong HA, Clark S. Pharmacy Emergency Preparedness and Response (PEPR): a proposed framework for expanding pharmacy professionals’ roles and contributions to emergency preparedness and response during the COVID-19 pandemic and beyond. Res Social Adm Pharm. 2021 Jan;17(1):1967-1977. [CrossRef]
- Noe B, Smith A. Development of a community pharmacy disaster preparedness manual. J Am Pharm Assoc (2003). 2013 Jul-Aug;53(4):432-7. [CrossRef]
- Anderson C, Blenkinsopp A, Armstrong M. The contribution of community pharmacy to improving the public’s health: summary report of the literature review 1990–2007.
- Strand MA, DiPietro Mager NA, Hall L, Martin SL, Sarpong DF. Pharmacy Contributions to Improved Population Health: Expanding the Public Health Roundtable. Prev Chronic Dis. 2020 Sep 24;17:E113. [CrossRef]
- Strand MA, Tellers J, Patterson A, Ross A, Palombi L. The achievement of public health services in pharmacy practice: A literature review. Res Social Adm Pharm. 2016 Mar-Apr;12(2):247-56. [CrossRef]
- Power A; NHS Education for Scotland Pharmacy Team. Scotland: a changing prescription for pharmacy. Educ PrimCare. 2017 Sep;28(5):255-257.
- Xyrichis A, Lowton K. What fosters or prevents interprofessional teamworking in primary and community care? A literature review. IJNS. 2008 Jan 1;45(1):140-53. [CrossRef]
- Faculty of Public Health. Functions and Standards of a Public Health System. 2021. https://www.fph.org.uk/professional-development/good-public-health-practice/ (accessed 06 October 2023).
- Roberts W, Satherley P, Starkey I, et al. The unusual suspects: unlocking the potential of the wider public health workforce [Online]. 2024. Available at: https://www.rsph.org.uk/our-work/policy/wider-public-health-workforce/unusual-suspects-unlocking-potential-wider-public-health-workforce-report.html#:~:text=%22This%20new%20RSPH%20report%20makes,healthier%20and%20more%20prosperous%20future.%22 (accessed 06 October 2023).
- Adam Todd, Diane Ashiru-Oredope, Building on the success of pharmaceutical public health: is it time to focus on health inequalities?, IJPP, 32 (5): 337–339,. [CrossRef]
- Warren, R., Young, L., Carlisle, K., Heslop, I. ., & Glass, B. (2021). REVIEW: Public health competencies for pharmacists: A scoping review. Pharm Ed, 21, p. 731–758. [CrossRef]
- Auimekhakul T, Suttajit S, Suwannaprom P. Pharmaceutical public health competencies for Thai pharmacists: A scoping review with expert consultation. Explor Res Clin Soc Pharm. 2024 Apr 22;14:100444. [CrossRef] [PubMed] [PubMed Central]
- Warren R, Young L, Carlisle K, Heslop I, Glass B. A systems approach to the perceptions of the integration of public health into pharmacy practice: A qualitative study. Explor Res Clin Soc Pharm. 2023 May 9;10:100279. [CrossRef] [PubMed] [PubMed Central]
- D Ashiru-Oredope, T Harrison, E Wright, R Osman, C Narh, U Okereke, E Harvey, M Bennie, C Garland, A Evans, C Pyper, Barriers and facilitators to pharmacy professionals’ specialist public health roles: a mixed methods UK-wide pharmaceutical public health evidence review, International Journal of Pharmacy Practice, Volume 30, Issue Supplement_2, December 2022, Pages ii2–ii3.
- Ashiru-Oredope D, Osman R, Narh C, Okereke U, Harvey EJ, Garland C, Pyper C, Bennie M, Evans A. Public health qualifications, motivation, and experience of pharmacy professionals: exploratory cross-sectional surveys of pharmacy and public health professionals. Lancet. 2023 Nov;402 Suppl 1:S24. [CrossRef] [PubMed]
Figure 1.
Domains of public health (reproduced with permission from Ashiru-Oredope, Population and public health. Pharmacy Magazine. https://www.pharmacymagazine.co.uk/cpd-modules/population-and-public-health.
Figure 1.
Domains of public health (reproduced with permission from Ashiru-Oredope, Population and public health. Pharmacy Magazine. https://www.pharmacymagazine.co.uk/cpd-modules/population-and-public-health.
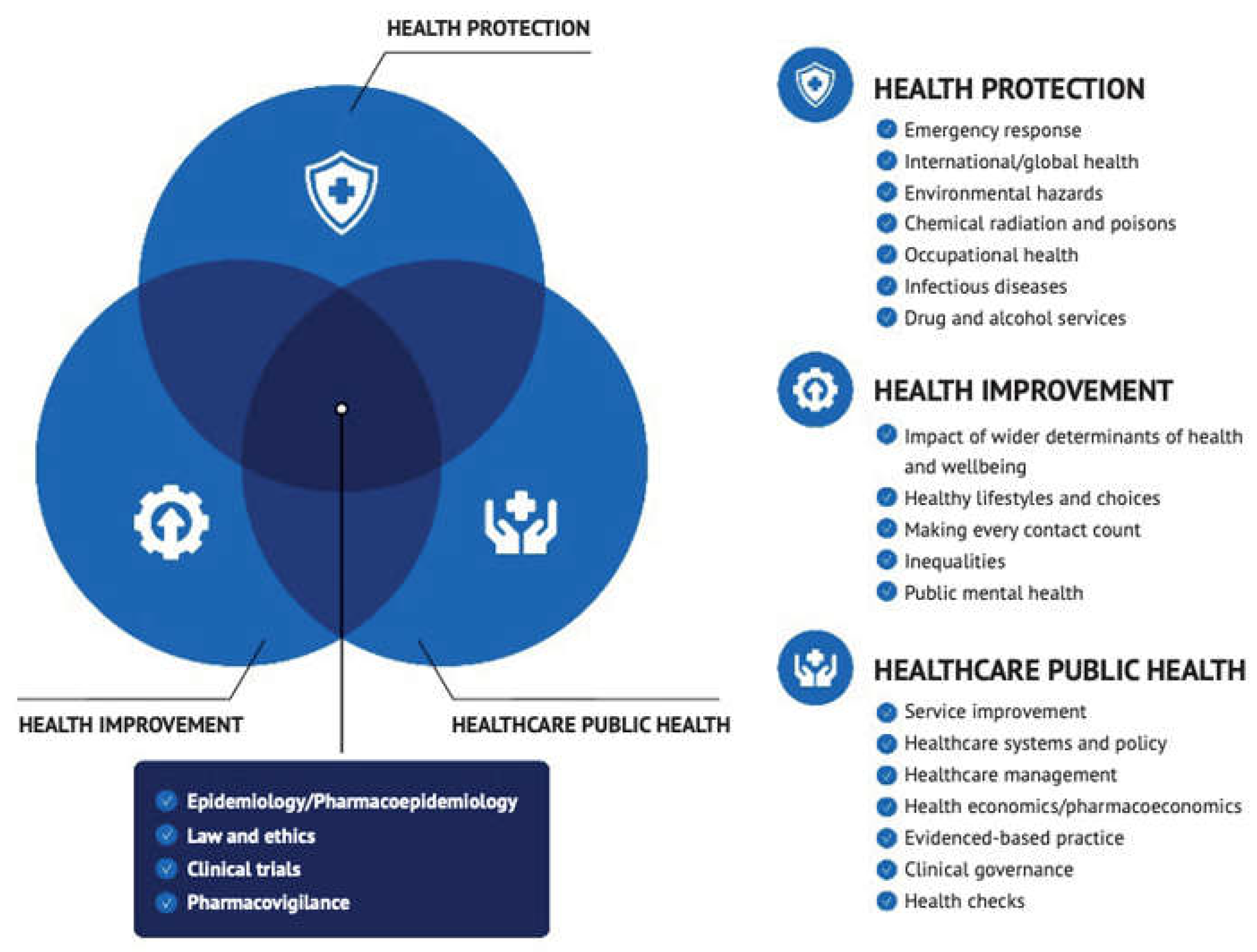
Figure 2.
micro-meso and macro level public health activities of pharmacy professionals.
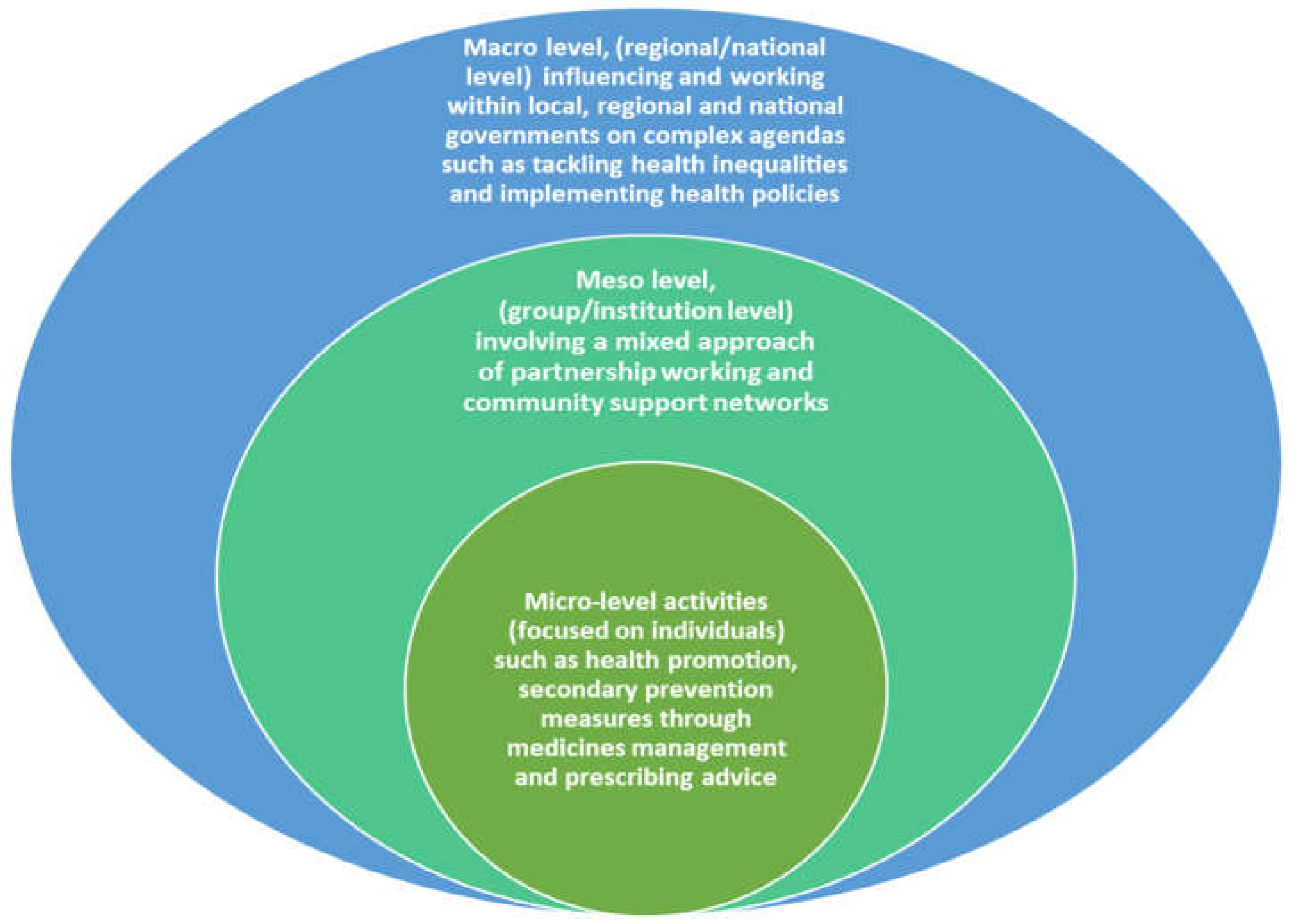
Figure 3.
sectors pharmacy respondents work in.
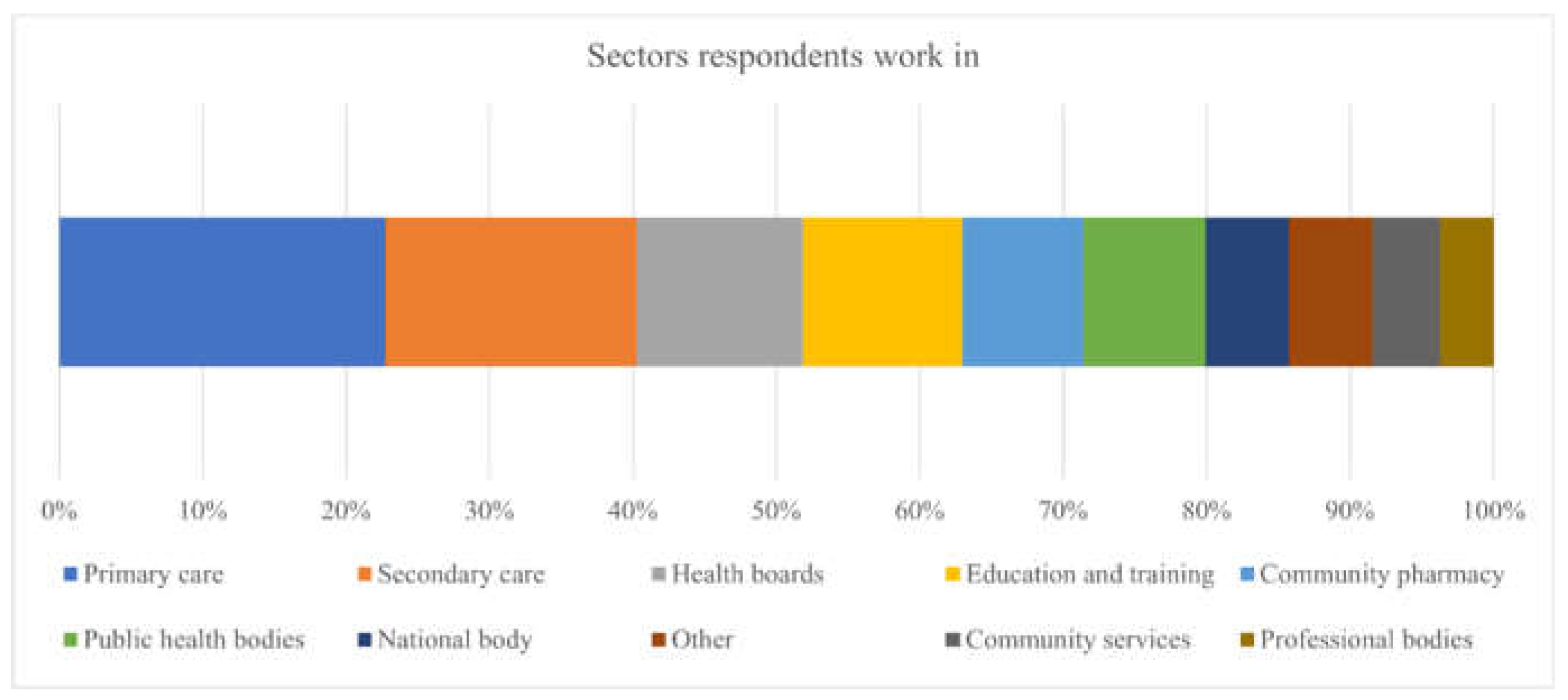
Figure 4.
Public/population health areas (non-Covid) that best describes the work pharmacy professionals were involved in or leading on. ** “Section 128A of the National Health Service Act 2006 (NHS Act 2006) requires each health and wellbeing board to assess the need for pharmaceutical services in its area and to publish a statement of its assessment. Termed a ‘pharmaceutical needs assessment’”.
Figure 4.
Public/population health areas (non-Covid) that best describes the work pharmacy professionals were involved in or leading on. ** “Section 128A of the National Health Service Act 2006 (NHS Act 2006) requires each health and wellbeing board to assess the need for pharmaceutical services in its area and to publish a statement of its assessment. Termed a ‘pharmaceutical needs assessment’”.
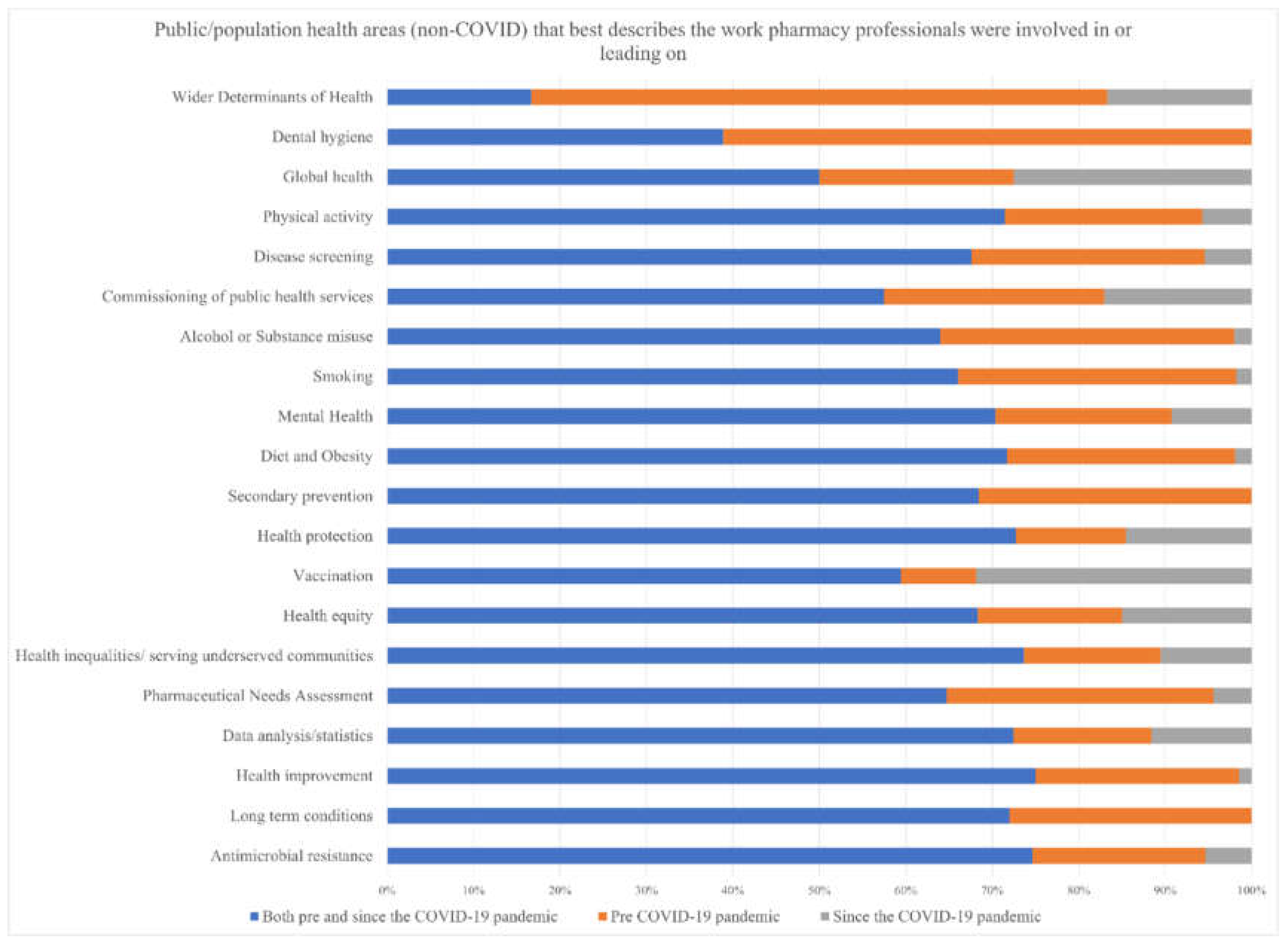
Figure 5.
Areas of public health* that benefit would be achieved by having pharmacy professionals working directly as part of the public health team. *Faculty of Public Health, Functions and Standards of a Public Health System. The document draws together a range of different papers that the Faculty of Public Health has produced in recent years to describe the essential functions of a public health system, and the standards and contribution of the specialist public health workforce that are crucial to a robust UK public health structure. https://www.fph.org.uk/professional-development/good-public-health-practice/ https://www.fph.org.uk/media/3031/fph_systems_and_function-final-v2.pdf
Figure 5.
Areas of public health* that benefit would be achieved by having pharmacy professionals working directly as part of the public health team. *Faculty of Public Health, Functions and Standards of a Public Health System. The document draws together a range of different papers that the Faculty of Public Health has produced in recent years to describe the essential functions of a public health system, and the standards and contribution of the specialist public health workforce that are crucial to a robust UK public health structure. https://www.fph.org.uk/professional-development/good-public-health-practice/ https://www.fph.org.uk/media/3031/fph_systems_and_function-final-v2.pdf
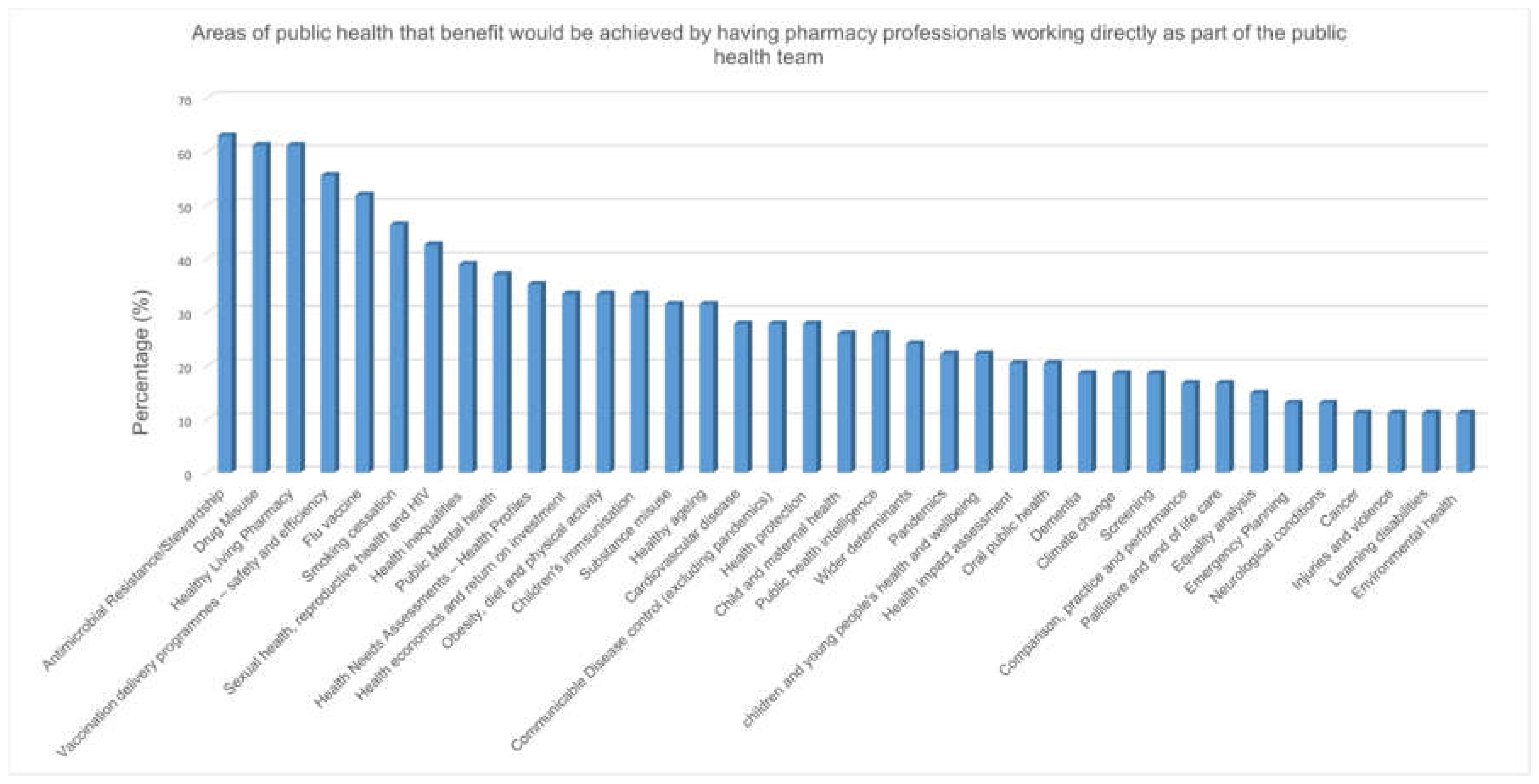
Figure 6.
Number of documents, reports and case histories identified and aligned with 8 themes.
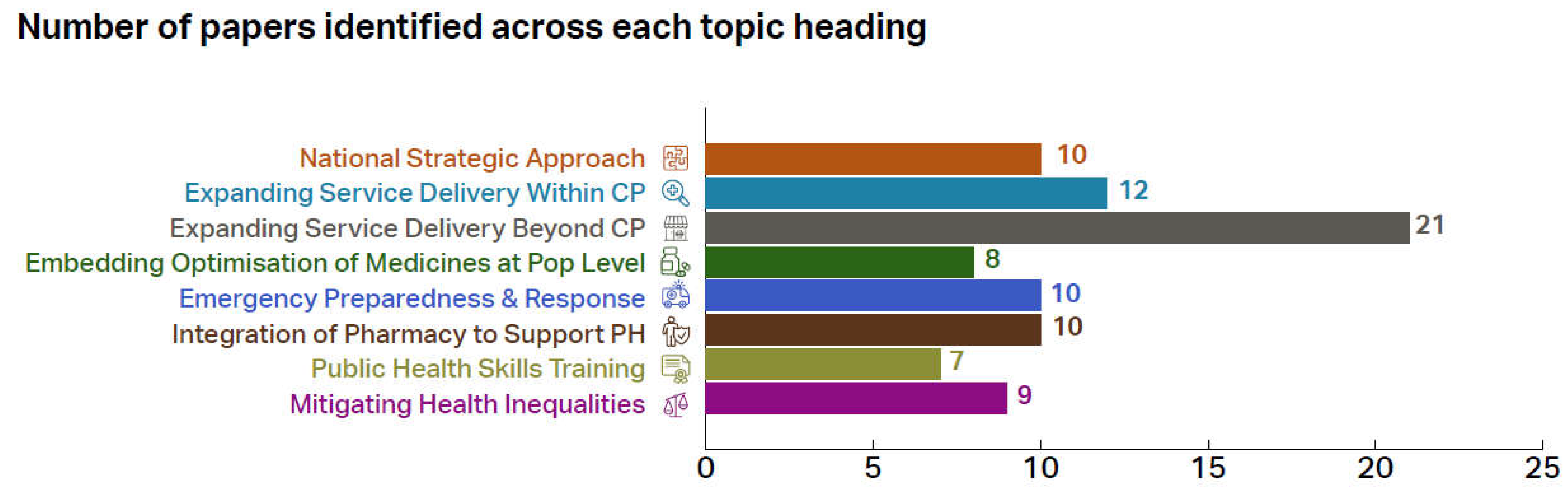

Table 1.
Demographic characteristics of pharmacy professionals survey participants.
| Demographic | Frequency (%) |
|---|---|
| Gender identity | |
| Female (including trans women) | 90 (70) |
| Male (including trans men) | 35 (27) |
| Prefer not to say | 3 (3) |
| Ethnic group or background | |
| White—British | 62 (48) |
| Asian or Asian British—Indian | 13 (10) |
| White—Irish | 12 (9) |
| Black or Black British—African | 11 (9) |
| White—Any other White background | 8 (6) |
| Prefer not to say | 5 (4) |
| Asian or Asian British—Any other Asian | 3 (2) |
| Asian or Asian British—Pakistani | 3 (2) |
| Mixed—Any other mixed background | 3 (2) |
| Other Ethnic Groups—Chinese | 3 (2) |
| Black or Black British—Caribbean | 2 (2) |
| Black or Black British—Any other Bla | 1 (1) |
| Mixed—White and Asian | 1 (1) |
| Not stated | 1 (1) |
| Country of work | |
| England region | 96 (75) |
| South East | 20 (21) |
| Midlands | 18 (19) |
| London | 17 (18) |
| North East and Yorkshire | 11 (11) |
| National | 9 (9) |
| East of England | 8 (8) |
| North West | 7 (7) |
| South West | 6 (6) |
| Scotland | 13 (10) |
| Northern Ireland | 9 (7) |
| Wales | 9 (7) |
| GB | 1 (0.1) |
| Total | 128 (100) |
Table 2.
Barrier themes and sample quotes.
| Themes | Number | Sample quotes |
| Limited career opportunities/ no defined career pathway | 39 (19.7%) |
No clear career pathway, very few boards have pharmacy public health posts. There is a lack of job opportunities for pharmacy professionals within public health teams themselves as there is a lack of recognition of the core knowledge and qualification that pharmacy professionals possess. There is also a lack of clarity with regards to professional management of the pharmacy professional within public health. Not a traditional role. Used to be common placed for a PH pharmacists in boards but sadly no longer the case |
| Poor professional recognition | 34 (17%) |
Not always seen as public health champions the profession is often overlooked as a solution, The barriers for pharmacist to be involved in public and population health are: 1. lack of awareness in public health of what pharmacists can bring to the table. 2. lack of awareness in the pharmacy community of the role that pharmacists can play in public health at a policy and strategy level. I suspect many pharmacists will not be aware of needs assessments other than that for community pharmacies. There appears to not be a good understanding from other healthcare professionals and the general public of the impact pharmacy professionals could have given the opportunity Pharmacist are not seeing as a profession that can contribute to public health |
|
Limited resources (time or financial) |
32 (16%) |
capacity- pharmacists workload, less protected time for research/QI, under-resourced profession in multiple sectors Busy on daily task. No time to put aside to capture data to understand impact of our daily work on public health. No time to design audits. Prohibitive costs associated with studying a Master’s course and lack of sponsorships for experienced healthcare professionals from high income countries. capacity, resources and whether it is seen as economically viable |
| Lack of training and support | 30 (15%) |
lack of pharmacy specific formal training that can easily be accessed. to progress in public health as a pharmacist means moving away from being a pharmacist to become a public health specialist/consultant. Pharmacy technicians for example are only required to ‘know’ about public health issues and not to be able to demonstrate how they can tackle them. |
| Inadequate Public Health knowledge |
21 (11%) |
Lack of understanding of the difference between individual and population health and how inadvertent actions to do better for every individual may actually widen inequality. No undergraduate training in epidemiology and/or data science. Pharmacy degree doesn’t set people up very well for research. There’s too much focus on completing clinical diploma post-reg for people to consider a career in PH I feel that a lot of pharmacists don’t consider aspects of what they are already doing as public health. Having this broader understanding may change the way they think about delivery of certain services and care. Public health not a core part of the pharmacy degree (that I am aware of) Training on Health promotion and changing health behaviours would be helpful for all pharmacists. There are vast opportunities for pharmacy professionals to be involved in public health but the initial education of neither profession enables a natural progression towards that. |
| Organisational and structural barriers | 19 (10%) |
workload and staffing structures & wider corporate agenda (large multiples) for Community pharmacy For popoulation health lack of understanding within pharmacy senior leadership in practice settings, lack of education and training in this area (prior experience and access to), no pharmacy network Generally work gets focused on medication management leave less scope for work on wider determinants and other aspects of healthcare public health like screening, Health Impact assessment, health promotion programmes though options are increasing.More likely to have a public health component to work rather than have it as a primary focus |
| Not capitalizing on available opportunities | 12 (6%) |
Just about not being aware of what the role entails and having experience in publishing research and drafting proposals/business cases. Not knowing the opportunities available Pharmacy professionals advocating for traditional roles |
| Poor representation in public health domains | 11 (6%) |
Pharmacists are not actively targeted for our experiences to work for PH. There aren’t many pharmacists directly employed by LAs—I don’t know why this is. Provide a service then take it away and see what happens—back to the “proving one’s worth” in a political organisation maybe? In some arenas there are perceptions that all avenues are covered. It’s only when pharmacists/technicians become involved that new solutions or alternative ways of working are exposed. |
Table 3.
Opportunity themes and sample quotes.
| Themes | Number | • Sample quotes |
| A range of Public Health areas pharmacy professionals can get involved in | 44 |
There are many opportunities for community pharmacy professionals to be involved in public health interventions depending on capacity, training and commissioning of services e.g., smoking cessation, sexual health, vaccination, substance misuse services, infection prevention and testing/treating and contributing to pathways for overweight and obesity. There are also opportunities for pharmacists employed by health boards to be involved in population health e.g., prescribing /medicines management initiatives. The All Wales Therapeutics and Toxicology Centre has various working groups in which pharmacists can be involved in strategic medicines management/pharmaceutical public health which in some instances links to other sources of data to provide a broader perspective . Infectious disease screening and treatment in addition/association to the work commonly done by nurses, e.g., TB. Hepatitis CBRNE and disaster preparedness. Pharmacists long overlooked. Their expertise lends itself to this. Mass vaccination programs Work with diseases of global importance, e.g., haemorrhagic fevers Polypharmacy and de-prescribing • Some local authorities are lacking clinically trained staff. I have found that pharmaceutical expertise embedded within and available to support the local authority public health, and wider LA teams is crucial to enable the appropriate/correct collaboration which is needed for commissioning/transformational change/medicines optimisation. Without this, going forward our community pharmacies may not be considered locally or become recognised as place-based assets to reach their full potential to improve health prevention and chronic disease management as part of the NHS Long Term Plan. • Significant need and opportunity for pharmaceutical public health skills to be deployed at system and place level to support commissioning of medicines and pharmacy services |
| Qualification, knowledge and skills | 26 | • Pharmacy technicians are highly trained, knowledgeable and experienced in providing direct patient care, liaising professionally with other healthcare professionals and are experts in medicines supply and storage • A lot of what Pharmacy professionals do in primary care is on a population basis and has an immediate link with public health. For example from producing a local guideline to seeing its implementation in practice affects the health of our population. • We have a unique perspective on health related to medication. This can be valuable in many different areas • Based at the heart of local communities community pharmacy professionals are most likely to see the patient first in respect of public health issues especially when related to self care and yet they are not always the first choice for commissioners. The sector cannot play its role in integrated care if is not included at the right tables. Seats at the right tables need to be made available to pharmacists and pharmacy technicians (as opposed to the contractor) so that both professions can maximise their usefulness in this arena. |
| Strategic position in the community | 18 | • Very important area—pharmacies are embedded in the heart of our communities, see our population more than any other health professional • Pharmacy professionals is widely accessible by the general public and key to deliver any public health messages • Community pharmacists in particular have an opportunity to engage with the public on PH issues. General Practice and hospital pharmacists also have opportunities to engage with patients during discussion of medication issues. • I believe pharmacists are well placed to be involved in public / population health. They have insights into their local areas and communities. They approach health with a hollistic approach whilst still maintaining the traditional clinical role. Thay are more accessible than most other health care professionals and have greater insight into reasoning for lifestyle choices and behaviours, such as addiction, obesity, etc. • As accessible healthcare professionals, we have increasing opportunities to identify risk and take a proactive approach to improving the health of populations and individuals. • Pharmacists/ technicians are easily accessible on the high street without an appointment to provide advice/ support/ signposting. Lots of opportunity for brief advice in both community and also primary care pharmacy when undertaking medication optimisation/ medication reviews. |
| Recent changing health landscape (health policy e.g., long-term plan) | 4 | • The long term plan has increased the opportunity available for pharmacy professionals. • There is large overlap between public/ population health and pharmacy practice and pharmacists I think have a particular role in pharmaceutical public health. |
| COVID | 3 | • My colleagues were directly involved with the covid vaccinations • Most definitely- involvement in recent Covid vaccination for example. • Pharmacists played a central role in the excellent vaccine rollout in the UK, manufacturing of alcohol rubs, in providing advice on the administration and sourcing of medication to be used in COVID19. We are analytical, excellent communicators, efficient and brilliant decision makers. There are many opportunities for us to demonstrate this at a global, regional and national level. |
| Good public perception | 2 | • The public and healthcare professionals trust our judgement and knowledge, so now is the perfect time to showcase our skills in public/ population health. • trusted professional, expert in medicines, access to patients, |
Table 4.
Demographic characteristics of public health professional survey participants.
| Category | Subcategory | Frequency (%) |
|---|---|---|
| Job Role of Respondent n=54 | Public health consultant | 10 (18.5%) |
| Public health Registrar ST1-3 | 7 (13.0%) | |
| Public health Registrar ST4-5 | 6 (11.1%) | |
| Public health practitioner | 5 (9.3%) | |
| Director of Public health | 5 (9.3%) | |
| Others | 4 (7.4%) | |
| Strategist | 2 (3.4%) | |
| Public Health pharmacist | 1 (1.9%) | |
| Principal public health practitioner | 1 (1.9%) | |
| Public health academic | 1 (1.9%) | |
| Allied health practitioner | 1 (1.9%) | |
| Area of Specialty n=51 | General | 13 (24.1%) |
| Health Improvement | 11 (20.4%) | |
| Health Protection | 10 (18.5%) | |
| Healthcare Public Health | 10 (18.5%) | |
| Commission | 3 (5.6%) | |
| Screening | 2 (3.7%) | |
| Sexual Health | 1 (1.9%) | |
| Substance abuse | 1 (1.9%) | |
| Gender n=54 | Female | 36 (66.7%) |
| Male | 16 (29.6%) | |
| Prefer not to say | 2 (3.7%) | |
| Location of practice (Country) n=54 | England | 32(59.3%) |
| Scotland | 15(27.8%) | |
| Wales | 7(13.0%) | |
| Location of practice (Region) n=22 | Midlands | 7 (22.0%) |
| South West | 6 (19.0%) | |
| South East | 5 (16.0%) | |
| North East and Yorkshire | 4 (13.0%) | |
| North West | 4 (13.0%) | |
| London | 4 (13.0%) | |
| National | 2(6.0%) | |
| East of England | 0 | |
| Description of main area(s) of work n=31 | Local Authority council | 14 (43.8) |
| Public Health England—regional/ local | 7 (21.9%) | |
| Public Health England—national | 2 (6.2%) | |
| Acute national health service (NHS) trust | 1 (3.1%) | |
| Health boards or trusts | 1 (3.1%) | |
| Clinical Commissioning Group (CCG) | 1 (3.1%) | |
| University | 1 (3.1%) | |
| Professional body– regional/ local | 1 (3.1%) | |
| Military | 1 (3.1%) | |
| Mental Health trust | 1 (3.1%) | |
| Primary care Network | 1 (3.1%) |
Table 5.
Benefits, barriers and placement opportunities for pharmacy professionals in public health teams.
Table 5.
Benefits, barriers and placement opportunities for pharmacy professionals in public health teams.
| Benefit of having pharmacy professional specialise in public health n=52 | Very Beneficial | Beneficial | Somewhat Beneficial |
| 26(50.0) | 19(26.5) | 7(13.5) | |
| Barriers for pharmacy professional to get involved in population health n=50 | Yes | No | Not sure |
| 30(60.0) | 13(26.0) | 1(2.0) | |
| Organization provide placement to funded pharmacy professional for fellowship in public health n=32 | Yes | No | Maybe |
| 10(21.3) | 6(12.8) | 16(34.0) | |
| Local Authority inclusion of medicine service as part of MOU with CCG n=19 | Yes | No | Not sure |
| 1(3.3) | 4(13.3) | 14(46.7) |
Table 6.
Barriers highlighted by public health professionals.
| Themes | Number | Sample quotes |
| Organisational and structural barriers | 13 |
“time, staff turnover, recovery from COVID pandemic” “Reluctance to change status quo from senior management and policy down to front-line. Fear of additional workloads in already stretched services (although social prescription and signposting goal would be to reduce reliance), lack of undertanding (not enough data locally or nationally) on the long-term benefits of an increased focus and increase in funding towards social prescription.” “It seems form my experience of working with pharmacies that they are quite pressured for time and there is a high turn over of counter staff sometime as well as a turn over of commercial owners” gaining of agreement for pharmacists to be willing to do more public health focused work as it could be seem as detracting from their ‘core business’. |
| Lack of training and support | 6 |
There will be barriers including limitations to what pharmacists are able to do in their working day, what training they would need to undertake public health work, To be blunt I have been working in XXXXXX for x years and nobody ever suggested I take formal training in this area. People work in silos and as long as you are ticking the boxes, they leave you alone. I feel any senior professional joining a public health organisation without public health training needs to obtain it, fast! |
| Limited career opportunities/ no defined career pathway | 9 |
, not many role models or possibly job opportunities, may need to carve out a niche for themselves potentially difficult to maintain professional practice whilst working in PH there is no defined formal route into public health. Some pharmacists can go via Specialty Registrar, and others have used the Defined specialist route (recently refined). The public health role and opportunity for pharmacists need to be integrated into Learning and Academic organisations to get early buy in There is a lack of job opportunities for pharmacy professionals within public health teams themselves as there is a lack of recognition of the core knowledge and qualification that pharmacy professionals possess. Pharmacy professionals may also lack clarity/confidence in moving to a new area of work especially if they feel that they will need to undertake a new qualification to enable them to work within public health. There is also a lack of clarity with regards to professional management of the pharmacy professional within public health. Not a traditional role. Used to be common placed for a PH pharmacists in boards but sadly no longer the case |
| Poor professional recognition | 10 | |
| Inadequate PH knowledge | 2 |
In general our pharmacy colleagues are not PH trained. They are therefore clearly expert in medicines issues, but don’t have wider skills in population health approaches and epidemiology. Collaborative working with PH specialists and others overcomes this to a large extent, but some training in PH for at least some of our pharmacists would be helpful. Not covered extensively at undergraduate level. Role of pharmacists in public health very variable and topic specific. Pharmaceutical public health not seem by PH fraternity or professional body as a discipline. No formal training to skill pharmacists up in this area broadly. Community pharmacy contract not remunerated for this work |
| Limited resources (time and/or financial) | 11 |
Cant think of any specific barriers although availability of pharmacists in the SW is already a challenge and exacerbating that would be a concern capacity, resources and whether it is seen as economically viable Unlikely to be a full time rule so hard to find match an interested person to a small number of hours e.g., 1 day a week. Entry level of public health professional does not support pharmacy pay grades |
| Not capitalising on available opportunities | 4 |
The importance of public health implications of medicines largely unexplored Expectations around what can be achieved with medicines are often limited to cost savings in commissioning. Wider work on reducing medication, working with community teams to ensure medication cocktails are well suited to patients will be more important as more co-morbidities in population. This work isn’t generally considered public health but it is- making sure system works together is very important. |
| Poor representation in PH domains | 3 |
Lack of understanding of wider benefits to self, profession, community and other HC professionals I think we don’t always understand each other’s areas of work and the ‘business’ side of pharmacy means certain work takes preference , like primary care. |
Table 7.
Recommendation themes and examples of statements from workshop participants.
| Themes | Number of recommendations per theme | Examples of individual recommendation |
|---|---|---|
| Public Health Skills and Training: Define PPH career pathway to allow pharmacy professionals to remain within the profession but contribute/lead on PH |
32 | Develop a career development pathway that does not require pharmacy professionals to work outside the speciality to be recognised as qualified public health professionals. |
| National Strategic Approach: Define national standards and career pathway for pharmacy professionals in Public Health (PH) |
31 | Define national standards for population health knowledge to support consistency across all localities of Great Britain and support capability for roll out of national services. |
| Other Commissioning: All ICSs should have PPH representation |
13 | Increase involvement of pharmacy in the commissioning process. |
| Expanding Service Delivery beyond Community Pharmacy: Integrate Pharmaceutical PH (PPH) teams within a variety of care sectors | 10 | Bring elements of public health into pharmacist practice. |
| Integration of Pharmacy to Better Support PH Protection & Improvement Goals | 3 | Involve pharmacy in leading public health services, e.g., National Centre for Smoking Cessation and Training practitioners. |
| Mitigating Health Inequalities: Involve PPH as part of Integrated Care Systems (ICS) health inequalities agenda |
3 | Each ICS health inequalities agenda to produce a review of what pharmacy can do to make a difference. |
| Embedding Optimisation of Medicines at a Population Health Level: Include PPH within medicines optimisation at a population level |
1 | Improve the integration / joint working between ICS / LA / PHE to address use of medicines for population health management—as currently addressed at individual sector level but not at strategic level. |
| Emergency Preparedness, Resilience and Response | 1 | Learn from the COVID-19 pandemic experience, particularly regarding the role of specialist pharmacy services and specialist pharmacists working across PHE, NHSEI and CCG’s and how they should be included as part of EPRR future planning processes. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



