
Submitted:
01 November 2024
Posted:
01 November 2024
You are already at the latest version
Abstract
Background/Objectives: Telenutrition has been reported to enable dietitians to support outpa-tients remotely in an accessible and most convenient state. The literature has also proved that both telemonitoring and health coaching are effective approaches for a greater impact on weight loss and client’s compliance to the diet. The purpose of the present study is to assess the impact of a Telenutrition Weight Loss Program supported with telemonitoring and health coaching on weight reduction.; Methods: A pilot randomized controlled trial was conducted among 50 overweight and obese adults. The control group (n=25) have received a hypocaloric and tailored diet via telenutrition. Intervention group (n=25) have also received hypocaloric and tailored diet via telenutrition but supported with weekly telemonitoring and monthly health coaching; Results: Participants who joined the intervention group had a reduction in weight, BMI, fat%, visceral fat, and WC. Whereas participants in the control group only had a reduction in WC after a period of 3 months. In comparison between the groups, a greater reduction in weight, BMI, fat % and visceral fat was seen in the intervention group. Furthermore, muscle % after a period of 3 months was sig-nificantly higher in the intervention group. At 6 months follow-up, the intervention group still showed promising results, but it was not significant; Conclusions: Our data indicate that all three approaches telenutrition, telemonitoring and health coaching when combined provides an integrative personalized approach, which may have a significant impact on weight loss in obese and overweight individuals.
Keywords:
Obesity
; weight loss
; telenutrition
; telemonitoring
; health coaching
1. Introduction
The healthcare landscape is perpetually evolving, marked by a relentless pursuit of innovative solutions to address the multifaceted challenges encountered by individuals battling chronic conditions and improving their lifestyle via telemedicine [1] Within this context, the convergence of telecare interventions and the management of chronic diseases, such as obesity and diabetes has emerged as a focal point of exploration and advancement seen with telemonitoring [2]. Yet, dietetic practice has been shifting to some extent towards incorporating online consultations rather than traditional in-person consultations, as virtual care has been emerging as a promising strategy for promoting health and well-being in the dynamic landscape of today’s life [3]. In 2019, “Telenutrition” has been defined by The Academy of Nutrition and Dietetics as “the interactive use by an RDN of electronic information and telecommunications technologies to implement the Nutrition Care Process with individuals at another location and following state laws” [4]. This modern approach not only addresses nutritional concerns but also impacts various facets of health, including weight management in obesity [5,6]. Obesity is defined by the World Health Organization (WHO) as a global epidemic chronic disease, which resulted in more than 5 million deaths yearly around the world; The WHO identified combating this public crisis as one of the 2025 global nutrition targets (for children under 5) and one of the Targets for Noncommunicable Diseases (NCDs) reduction for adolescents and adults [7]. Different methods, including various treatments such as dietary changes, physical activity, behavioral therapy, medications, surgery, or a combination of these approaches, can be accessible for both clinical and community groups via telenutrition [4]. However, challenges exist in their availability, costs, adherence to treatment, and their effectiveness over the long term [8]. The expense of these approaches is a significant issue within continuous care settings, posing obstacles to public health strategies [9] . Sustaining weight loss is the primary difficulty in addressing obesity, as most individuals regain around one-third of lost weight within a year [10]. Telenutrition is believed to provide better healthcare outcomes for patients than traditional care, and reduces geographic barriers related to the management of their health. Electronic devices used for tele-based monitoring include video conferencing, software, websites, email, mobile phones, and Bluetooth telecommunications resources [11,12]. Telehealth is used as sustainable and economical strategies capable of reaching large groups of obese individuals, thoroughly assessed concerning adherence and the sustained adoption of healthy behaviors over time at minimal expenses in TECNOB study (Technology for Obesity) [5]. Additionally, telemonitoring has also been seen to support women with gestational diabetes mellitus in managing weight gain [13].
Previous studies have demonstrated the effectiveness of telenutrition in weight management in comparison with traditional dietetic consultations [6,14,15,16]. Other studies have shown that telemonitoring [2,13,17] and health coaching [18,19], have also supported patients to lose weight. Such approaches are rapidly emerging and need further investigation to reach an ideal model of telenutrition that promotes sustainable weight loss and patient compliance to long term healthy habits and lifestyle behaviors. In the present study we aimed to confirm the impact of virtual health care and expand our investigation to a comparison between the effect of home telenutrition combined with telemonitoring and personalized health coaching on weight loss vs. home telenutrition only. Furthermore, we also assessed the biochemical tests related to health and diet to be able to evaluate the effectiveness of the intervention on health status.
2. Materials and Methods
2.1. Participants
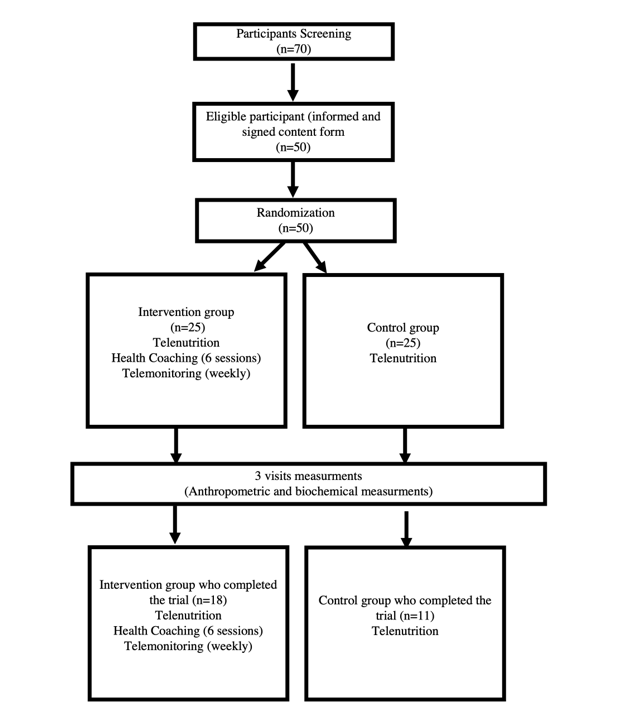
The study participants consisted of adults from both genders, aged 20-50 years who met the following criteria: (1) Obese or overweight based on the World Health Organization (WHO) criteria BMI over and equal 25 for overweight participants and BMI over and equal 30 kg/m2 for obese participants. (2) Informed and signed consent form. Participants were excluded for the following reasons: (1) not capable of understanding or not familiar with using online applications required for the study. (2) pregnant or lactating women. (3) history of chronic diseases such as diabetes or cardiovascular diseases or thyroid dysfunction or any other endocrine abnormality. (4) Participation in any other weight loss programs or using medication to lose weight for the past 3 months. (5) not being available for the whole 6 months trial duration. Sample size calculations using a significance level of 5 %, and power of 80%, and a dropout rate of 25%, indicated that to detect a significant change in weight loss between intervention (3.7 kg/2.5 SD) and control group of (1.6kg/2.5SD) , a minimum of thirty-five participants were required [18]. Intervention group (n=18) had 7 participants dropping out from the study. A total of 70 50 participants were eligible for the study. Followed by randomization and dividing the participants into two groups. Control group received a hypocaloric and tailored diet via telenutrition by registered dietitians RD. the control group (n 11) had 14 participants dropping out from the study before completing a 3months duration of the trial which is demonstrated in Figure 1.
2.2. Study Design
A pilot randomized control and intervention study was conducted in Jeddah, Saudi Arabia between January 2022 – August 2023. The Research Ethics Committee (REC) at the Unit of Biomedical Ethics, Faculty of Medicine at King Abdul-Aziz University approved the study protocol (HA-02-j-008). The study was designed as a two-arm randomized controlled trial, where participants were randomly divided into two groups: Intervention group joined received a hypocaloric and tailored diet via telenutrition by registered dietitians RD and supported with weekly monitoring and health coaching sessions delivered by a certified integrative nutrition health coach.
2.3. Program Description
Participants were recruited through the university and research center online platforms, by sharing advertisement flyers that describes the study purpose and contact details of research assistants. All participants were screened for eligibility by a family doctor, followed by an informed consent form to be signed once eligible to the study. All eligible participants were scheduled to attend 3 physical visits through the 6-month duration of the study to collect specific measurements at baseline, after 3month, and after 6months (anthropometric measurements and biochemical analysis). At the end of each visit participants from both groups were invited to join an online education talk about nutrition and health. Regarding the intervention group, each participant has received a bag containing “self-recording devices”, such as a weight balance, blood pressure analyzer and an armband measuring daily steps to be recorded during the weekly telemonitoring. Telemonitoring was carried via what’s ap texting to gather the following health information, which included (body weight, blood pressure, steps, and circle of life information) [13]. In addition, at end of each month, participants from the intervention group were invited to join to one on one and/or group coaching sessions delivered by an integrative nutrition health coach to use information gathered via telemonitoring and support participants on their circle of life such as, which include spirituality, creativity, finances, career, education, health, physical activity, home cooking, home environment, relationships, social life, and joy [20]. Health coaching aim was to tackle factors associated with their eating habits and behavior to support weight loss. Research assistants ensured that all participants downloaded the business what’s ap application and zoom conference call software for both telemonitoring and health coaching.
2.4. Anthropometric Measurements and Blood Biochemical Measures
Anthropometric measures, including systolic and diastolic blood pressure, weight, waist, BMI, and body fat percentage (body composition analyzer;), were recorded during each visit using standardized equipment and techniques. Samples were collected from the Food, Nutrition and lifestyle unit and sent to ROYA first vision laboratories in King Fahd Center for Medical Research to carry several tests which include; CBC, Alanine aminotransferase, Aspartate Aminotransferase, albumin serum, alkaline phosphatase, gamma-glumly Transferases, Direct Bilirubin, Total Bilirubin, HbA1C, Vitamin D , total cholesterol, Low Dentistry Lipoprotein, High Density Lipoprotein, Triglycerides, Thyroid Stimulating Hormones, Ferritin, C-Reactive Protein, and Total Protein. Results obtained were determined to be appropriate according to the quality control values given in a specific range by the manufacturers (https://royakau.com/en/).
2.5. Statistical Analysis
Data was analyzed using SPSS program version 26.0. Continuous data was reported as mean and SD. Categorical variables were reported as frequency and percentages (%). Between-group differences in anthropometric were examined at all time-points using independent t-test. A completers analysis was performed for any time-points (n=29 at 3 months, n=25 at 6 months). Chi-square test was used for categorical variables. A <0.05 value (two-sided test) was accepted as statistically significant.
3. Results
3.1. Participants Characteristics
A total of 29 participants (18 and 11 in the intervention and control arms, respectively) have completed the 3-months visit, and a total of 25 participants (16 and 9 in the intervention and control arms, respectively) have completed the 6-month visit. Both arms were balanced as baseline characteristics of participants were not significantly different between the two study groups as shown in Table 1.
3.2. Clinical and Biochemical Measurements at All Time-Points
Biochemical and clinical data for the two arms collected at baseline, 3 months, and 6 months are presented in Table 2. There were no significant differences in systolic and diastolic BP changes at 3 and 6 months between the Intervention and control groups. However, at 3 months, intervention group had a significantly lower TG level compared with the control group (0.97 (SD=0.35) and 1.38 (SD=0.67) respectively, p= 0.043; Table 2)). At 6 months, LDL and TG levels were significantly lower in the intervention group (LDL: 3.49 (SD=0.59) and 4.17 (SD=0.85) respectively, p = 0.034; TG: 0.99 (SD=0.52) and 1.47 (SD=0.4) respectively, p = 0.034; Table 2).
3.3. Changes in Anthropometric and Body Composition Measurements from Baseline at 3 and 6 Months
There were no significant differences between groups in anthropometric measurements at discharge and at 3-month follow-up. However, at 3 months, the intervention group experienced a significant reduction in weight, decreasing by an average of 3.93 kg (SD = 4.58), compared to a modest reduction of 0.19 kg (SD = 2.50) in the control group (p = 0.02, Table 3). The percentage change further emphasized this difference, with a -4.06% change in the intervention group versus -0.48% in the control group (p = 0.022; Table 4). However, at 6 months, while the intervention group continued to show a greater reduction in weight (-3.11 kg, SD = 6.02) and percentage change (-3.46%) compared to the control group (-1.02 kg, SD = 2.69; -1.17% change), these differences were not statistically significant between groups (Table 3 and Table 4). Similar trends were observed in BMI reductions. At 3 months, the intervention group demonstrated a notable decrease in BMI (-1.46, SD = 1.66) compared to the control group (-0.14, SD = 1.01 (p = 0.025; Table 4). The percentage change in BMI also reflected significant differences (-4.35% vs. -0.63%, p = 0.024; Table 4). By 6 months, the reductions in BMI persisted in both groups, but the differences were not statistically significant (p = 0.44 and p = 0.324 for absolute and percentage changes, respectively; Table 3 and Table 4).In terms of fat percentage, the intervention group showed a significant reduction at 3 months (-2.94%, SD = 2.80) compared to the control group (-0.89%, SD = 1.77), (p = 0.048; Table 3). However, by 6 months, the reduction in fat percentage was not significantly different between groups (Table 3). Conversely, muscle percentage tended to have a significant increase in the intervention group at 3 months (1.68%, SD = 1.77) compared to the control group (0.56%, SD = 1.05), (p = 0.051; Table 4) and showed no significant difference at 6 months (p = 0.866).Reductions in visceral fat at 3 months were more pronounced in the intervention group (-0.94 g, SD = 1.39) compared to the control group (-0.09 g, SD = 0.70) (p = 0.048, Table 3). However, these differences did not persist at 6 months (p = 0.295). Waist circumference (WC) changes did not show significant differences at both time points, although both groups experienced reductions.
The analysis of weight change at three months, stratified by BMI level and gender, significant interactions between gender, BMI level, and the effectiveness of intervention group versus control group. The weight reduction observed in participants with a lower BMI (<30) was -1.86 kg (SD = 2.19) for the intervention arm and -1.27 kg (SD = 1.51) for the control arm, with the difference not reaching statistical significance (p = 0.686; Table 5). However, for participants with a higher BMI (≥30), the intervention group experienced a more pronounced weight reduction of -5.25 kg (SD = 5.28) compared to a slight weight gain of 0.21 kg (SD = 2.75) in the control group, with the difference being statistically significant (p = 0.017; Table 5).Men in the intervention group had a significant weight loss of -7.8 kg (SD = 5.44), markedly greater than the -0.4 kg (SD = 2.04) observed in the control group, with a significant difference (p = 0.035; Table 5). Additionally, the weight loss in men under intervention was significantly greater compared to women within the same intervention arm (p < 0.05; Table 5). Women had a weight reduction of -2.44 kg (SD = 3.34) in the intervention group and a negligible weight change of 0.06 kg (SD = 3.2) in the control group, with no significant difference between interventions.
4. Discussion
Home telemonitoring has shown effective results in patients with various chronic illnesses, such as diabetes and hypertension [21,22,23,24], as well as improving outcomes in management of obstetrics cases and complicated pregnancies [25]. The present study provides evidence that a telemonitoring approach may be effective for obesity management and weight reduction; Following 3 months of the intervention, participants in the present study who were receiving both telemonitoring and health coaching have experienced a reduction in weight, BMI, fat%, visceral fat, and WC. These participants also showed an increase in muscle % after following the intervention for 3 months. On the other hand, participants in the control group only exhibited a reduction in WC after a period of 3 months. Comparing the intervention group to the control group, the decrease in weight, BMI, fat % and visceral fat was significantly greater. Furthermore, participants in the intervention group showed a greater increase in muscle % after a period of 3 months compared to participants in the control group. 6 months follow-up, although participants in the intervention group also showed a greater reduction in weight, BMI, fat%, visceral fat, and WC as well as greater increase in muscle %, compared to participants in the control group, none of these differences were statistically significant. According to results of previous research that was followed in the current study, telemedical coaching contronutes significanlt in weight loss in overweight employees [18]. Yet, our findings gives a detailed analysis of body weight compostion which has been altered significanly among particioants in the intervention group. In agreement with our findins, a retrospective study have looked at the impact of health coaching on both weight loss and weight loss percentages, where data confimrs that there is a strong association with losing at least -5% of weight loss were and attending five or more health coaching sessions [26]. Furthermore intervention trials have shown strong inlfuence of health coaching on weight loss outcomes [27]. One of the main effective roles of health coaches is to follow up with telemonitoring data, which has an impact on their health and wellbeing, such as stress [28], sleep [29] and physical inactivity [30]. In the current study, participants got coached to set specific goals to support their commitments to their hypocaloric diets, which is defined as “integrative nutrition”.
To our knowledge, the present study is the first in Saudi Arabia assessing the effectiveness of a telemonitoring that incorporated personalized nutritional counseling and health coaching for weight management among overweight and obese individuals. A previous study conducted among obstructive sleep apnea patients in Japan, found that enhancing continuous positive airway pressure (CPAP) telemonitoring with electronic scales, BP monitors, and pedometers led to greater body weight reductions [31]. On the contrary, a randomized controlled trial involving pregnant females found that a self-directed, telemonitoring intervention, did not result in less excessive weight gain during pregnancy[32]. Although there are conflicting findings regarding the effectiveness of telemonitoring and internet-based intervention on weight reduction [32,33] , where discrepancies may be due to components of the intervention and whether or not it includes coaching sessions or personalized counseling with professionals. The present study included one-on-one online coaching sessions delivered by an integrative nutrition health coach to reflect on monitored weekly health measurements, which has been seen to be effective when combined with telemonitoring in the intervention group in improving weight and body composition outcomes among obese patients. This is in line with a previous study which also incorporated weekly coaching sessions into its telemonitoring intervention and found this approach to be related to greater weight loss among overweight employees [18].
The diminished significance in differences between the two groups might be explained by lack of adherence to lifestyle changes among participants as previously observed at 6 months during weight loss programs [34]. Additionally, metabolic adaptations that occur following a period of weight reduction may have contributed to weight loss plateau at 6 months [35]. According to results from our stratified analysis, participants who had a BMI ≥ 30 kg/m2 lost more weight when supported with telemonitoring and health coaching compared to participants who had a BMI < 30 kg/m2. Previous research also found that higher BMI categories were associated with greater reduction in body weight [33]. The higher weight loss among obese vs. overweight individuals might be due to higher energy expenditure [36]. Additionally, our findings showed that the telemonitoring and health coaching impacts yielded greater weight loss among men compared to women, which is consistent with findings from previous weight loss interventions [37]. This difference between men and women might be explained by the possibility that only highly motivated men participated in the study, as the majority of participants were women (62.1%), which is similar to what has been observed in previous research [38] Assessing motivation and readiness to change prior to the intervention might be an important step for interpreting findings in future studies. Our findings therefore highlight the importance of considering both BMI and gender when evaluating the impact of weight loss interventions, indicating that telemonitoring could offer a tailored approach to support significant weight loss in more obese individuals and particularly in males. In accordance with previous findings [39], analysis of our biochemical data showed that the telemonitoring and health coaching approach had a positive effect on blood lipids profile; Participants in the intervention group had a significantly lower blood triglycerides level compared to participants in the control group at 3 months follow-up. Additionally, participants in the intervention group had significantly lower triglycerides and LDL levels at 6 months follow-up compared to participants in the control group.
5. Conclusions
The current study is considered a preliminary one demonstrating a personalized approach for weight management programs. Data successfully confirmed significant reduction in BMI, fat%, visceral fat, and WC and an increase in % of muscles among participants joining the intervention group in comparison with the control group. An additional strength of this study design is the weekly monitoring, which help in reducing errors and dropouts in the intervention group. In addition to health coaching which has a strong impact on human health. The research team consisted of various health professionals such as the family medicine doctor, clinical dietitian, and integrative nutrition health coaches to support volunteers’ health status and weight management. Yet, baseline and follow-up assessments as well as nutrition counseling sessions were conducted by the same research group members, and blinding was therefore not feasible. More measures must be applied in future work as seen in previous study protocols[40], where adding the WHO Quality-of-Life form and the End of Project Evaluation Survey may be useful to understand why the intervention group have significant promising results when compared to the control groups. The WHO QOL measures reflected by its four domains: physical, psychological, social and environment and the End of Project Evaluation survey looks at the volunteer’s commitment, motivation, enjoyment level and challenges after being weekly monitored and coached by the integrative nutrition health coaches. Thus, it is important to evaluate the reasons behind dropping out of the study as the telemonitoring and health coaching approach is original, especially in the Saudi community and that may be achieved by using semi-structured interview-based questionnaire [41]. Another trial should be proposed with a longer period of intervention (12 months) which was seen in previous trails [18] , where targets can be achieved when set on a longer period of time [42], as for volunteers in the current study , the short duration of 3 and 6 months may not have been long enough to reflect sustainability of changes in weight and body composition.
Author Contributions
Conceptualization, Noura Eid and Ebtisam Al-ofi ; Data curation, Sumia Enani; Formal analysis, Sumia Enani; Funding acquisition, Noura Eid, Ebtisam Al-ofi , Sumia Enani, Rana Mosli, Raneem Saqr, Karimah Qutah and Sara Eid; Investigation, Ebtisam Al-ofi , Karimah Qutah and Sara Eid; Methodology, Noura Eid, Sumia Enani, Raneem Saqr and Sara Eid; Project administration, Noura Eid; Resources, Rana Mosli and Karimah Qutah; Software, Raneem Saqr; Supervision, Noura Eid; Validation, Rana Mosli and Raneem Saqr; Visualization, Rana Mosli; Writing – original draft, Noura Eid; Writing – review & editing, Noura Eid, Ebtisam Al-ofi , Sumia Enani, Rana Mosli, Raneem Saqr, Karimah Qutah and Sara Eid. All authors have read and agreed to the published version of the manuscript.
Funding
This research is funded by the Institutional Fund Projects under grant no. IFPRC-206-141-2020.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of The Research Ethics Committee (REC) at the Unit of Biomedical Ethics, Faculty of Medicine at King Abdul-Aziz University, Jeddah, Saudi Arabia (HA-02-j-008).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author: ooaeid2@kau.edu.sa.
Acknowledgments
The authors gratefully acknowledge the support of Institutional Fund Projects by the Ministry of Education and King Abdul Aziz University in Jeddah, Saudi Arabia.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wang, Y.; Min, J.; Khuri, J.; Xue, H.; Xie, B.; Kaminsky, L.A.; L, J.C. Effectiveness of Mobile Health Interventions on Diabetes and Obesity Treatment and Management: Systematic Review of Systematic Reviews. JMIR Mhealth Uhealth. 2020, 8, e15400. [Google Scholar] [CrossRef] [PubMed]
- Luley, C.; Blaik, A.; Götz, A.; Kicherer, F.; Kropf, S.; Isermann, B.; Stumm, G.; Westphal, S. Weight loss by telemonitoring of nutrition and physical activity in patients with metabolic syndrome for 1 year. J Am Coll Nutr. 2014, 33, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Bookari, K.; Arrish, J.; Alkhalaf, M.M.; Alharbi, M.H.; Zaher, S.; Alotaibi, H.M.; Tayyem, R.; Al-Awwad, N.; Qasrawi, R.; Allehdan, S.; et al. Perspectives and practices of dietitians with regards to social/mass media use during the transitions from face-to-face to telenutrition in the time of COVID-19: A cross-sectional survey in 10 Arab countries. Front Public Health. 2023, 11, 1151648. [Google Scholar] [CrossRef] [PubMed]
- Gnagnarella, P.; Ferro, Y.; Monge, T.; Troiano, E.; Montalcini, T.; Pujia, A.; Mazza, E. Telenutrition: Changes in Professional Practice and in the Nutritional Assessments of Italian Dietitian Nutritionists in the COVID-19 Era. Nutrients. 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Castelnuovo, G.; Manzoni, G.M.; Cuzziol, P.; Cesa, G.L.; Tuzzi, C.; Villa, V.; Liuzzi, A.; Petroni, M.L.; Molinari, E. TECNOB: study design of a randomized controlled trial of a multidisciplinary telecare intervention for obese patients with type-2 diabetes. BMC Public Health. 2010, 10, 204. [Google Scholar] [CrossRef]
- Castelnuovo, G.; Manzoni, G.M.; Cuzziol, P.; Cesa, G.L.; Corti, S.; Tuzzi, C.; Villa, V.; Liuzzi, A.; Petroni, M.L.; Molinari, E. TECNOB Study: Ad Interim Results of a Randomized Controlled Trial of a Multidisciplinary Telecare Intervention for Obese Patients with Type-2 Diabetes. Clin Pract Epidemiol Ment Health. 2011, 7, 44–50. [Google Scholar] [CrossRef]
- Eastern Mediterranean Region intercountry dialogue on the WHO Acceleration Plan to STOP Obesity. East Mediterr Health J. 2023, 29, 491. [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R. Telemedicine for healthcare: Capabilities, features, barriers, and applications. Sens Int. 2021, 2, 100117. [Google Scholar] [CrossRef]
- Weinstein, P.K. A review of weight loss programs delivered via the Internet. J Cardiovasc Nurs. 2006, 21, 251–258; quiz 259–260. [Google Scholar] [CrossRef]
- Hill, J.O.; Thompson, H.; Wyatt, H. Weight maintenance: what’s missing? J Am Diet Assoc. 2005, 105, S63–S66. [Google Scholar] [CrossRef]
- Wing, R.R.; Tate, D.F.; Gorin, A.A.; Raynor, H.A.; Fava, J.L. A self-regulation program for maintenance of weight loss. N Engl J Med. 2006, 355, 1563–1571. [Google Scholar] [CrossRef]
- Barbosa, W.; Zhou, K.; Waddell, E.; Myers, T.; Dorsey, E.R. Improving Access to Care: Telemedicine Across Medical Domains. Annu Rev Public Health. 2021, 42, 463–481. [Google Scholar] [CrossRef] [PubMed]
- Al-Ofi, E.A.; Mosli, H.H.; Ghamri, K.A.; Ghazali, S.M. Management of postprandial hyperglycaemia and weight gain in women with gestational diabetes mellitus using a novel telemonitoring system. J Int Med Res. 2019, 47, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Santana, F.B.; Oliveira, N.S.; Costa, M.G.O.; Andrade, A.C.S.C.; Costa, M.L.; Teles, A.C.S.J.; Mendes-Netto, R.S. Impact of telenutrition protocols in a web-based nutrition counseling program on adult dietary practices: Randomized controlled pilto study. Patient Educ Couns 2024, 118, 108005. [Google Scholar] [CrossRef]
- Ventura Marra, M.; Lilly, C.L.; Nelson, K.R.; Woofter, D.R.; Malone, J. A pilot randomized controlled trial of a telenutrition weight loss intervention in middle-aged and older men with multiple risk factors for cardiovascular disease. Nutrients. 2019, 11, 229. [Google Scholar] [CrossRef] [PubMed]
- Kuzmar, I.E.; Cortés-Castell, E.; Rizo, M. Effectiveness of telenutrition in a women’s weight loss program. PeerJ. 2015, 3, e748. [Google Scholar] [CrossRef] [PubMed]
- Ezgi, M.a.K., C. Investigating the Weight Loss Success of Clients Participated in Different Telenutrition Intervention Groups: A Cross-Sectional Design. Turkiye Klinikleri Journal of Health Sciences. 2022, 7.
- Kempf, K.; Röhling, M.; Martin, S.; Schneider, M. Telemedical coaching for weight loss in overweight employees: a three-armed randomised controlled trial. BMJ Open. 2019, 9, e022242. [Google Scholar] [CrossRef]
- Conn, S.; Curtain, S. Health coaching as a lifestyle medicine process in primary care. Aust J Gen Pract. 2019, 48, 677–680. [Google Scholar] [CrossRef]
- Rosenthal, J. Integrative Nutrition: Feed Your Hunger for Health and Happiness. 3rd ed. 2014: Integrative Nutrition Publishing.
- Nicolucci, A.; Cercone, S.; Chiriatti, A.; Muscas, F.; Gensini, G. A Randomized Trial on Home Telemonitoring for the Management of Metabolic and Cardiovascular Risk in Patients with Type 2 Diabetes. Diabetes Technol Ther. 2015, 17, 563–570. [Google Scholar] [CrossRef]
- Davis, T.C.; Hoover, K.W.; Keller, S.; Replogle, W.H. Mississippi Diabetes Telehealth Network: A Collaborative Approach to Chronic Care Management. Telemed J E Health. 2020, 26, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.; Woods, J.; Zhang, Y.; Chandra, S.; Summers, R.L.; Jones, D.W. Home Blood Pressure Telemonitoring With Remote Hypertension Management in a Rural and Low-Income Population. Hypertension. 2021, 78, 1927–1929. [Google Scholar] [CrossRef] [PubMed]
- Michaud, T.L.; Ern, J.; Scoggins, D.; Su, D. Assessing the Impact of Telemonitoring-Facilitated Lifestyle Modifications on Diabetes Outcomes: A Systematic Review and Meta-Analysis. Telemed J E Health. 2021, 27, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Bekker, M.N.; Koster, M.P.H.; Keusters, W.R.; Ganzevoort, W.; de Haan-Jebbink, J.M.; Deurloo, K.L.; Seeber, L.; van der Ham, D.P.; Zuithoff, N.P.A.; Frederix, G.W.J.; et al. Home telemonitoring versus hospital care in complicated pregnancies in the Netherlands: a randomised, controlled non-inferiority trial (HoTeL). Lancet Digit Health. 2023, 5, e116–e124. [Google Scholar] [CrossRef] [PubMed]
- Aldhamin, R.A.; Al-Ghareeb, G.; Al Saif, A.; Al-Ahmed, Z. Health Coaching for Weight Loss Among Overweight and Obese Individuals in Saudi Arabia: A Retrospective Analysis. Cureus. 2023, 15, e41658. [Google Scholar] [CrossRef]
- Johnson, K.E.; Alencar, M.K.; Coakley, K.E.; Swift, D.L.; Cole, N.H.; Mermier, C.M.; Kravitz, L.; Amorim, F.T.; Gibson, A.L. Telemedicine-Based Health Coaching Is Effective for Inducing Weight Loss and Improving Metabolic Markers. Telemed J E Health. 2019, 25, 85–92. [Google Scholar] [CrossRef]
- van der Valk, E.S.; Savas, M.; van Rossum, E.F.C. Stress and Obesity: Are There More Susceptible Individuals? Curr Obes Rep. 2018, 7, 193–203. [Google Scholar] [CrossRef]
- Ghrouz, A.K.; Noohu, M.M.; Dilshad Manzar, M.; Warren Spence, D.; BaHammam, A.S.; Pandi-Perumal, S.R. Physical activity and sleep quality in relation to mental health among college students. Sleep Breath. 2019, 23, 627–634. [Google Scholar] [CrossRef]
- AlMarzooqi, M.A.; Saller, F. Physical Activity Counseling in Saudi Arabia: A Systematic Review of Content, Outcomes, and Barriers. Int J Environ Res Public Health. 2022, 19. [Google Scholar] [CrossRef]
- Murase, K.; Minami, T.; Hamada, S.; Gozal, D.; Takahashi, N.; Nakatsuka, Y.; Takeyama, H.; Tanizawa, K.; Endo, D.; Akahoshi, T.; et al. Multimodal Telemonitoring for Weight Reduction in Patients With Sleep Apnea: A Randomized Controlled Trial. Chest. 2022, 162, 1373–1383. [Google Scholar] [CrossRef]
- Olson, C.M.; Groth, S.W.; Graham, M.L.; Reschke, J.E.; Strawderman, M.S.; Fernandez, I.D. The effectiveness of an online intervention in preventing excessive gestational weight gain: the e-moms roc randomized controlled trial. BMC Pregnancy Childbirth. 2018, 18, 148. [Google Scholar] [CrossRef] [PubMed]
- Alencar, M.K.; Johnson, K.; Mullur, R.; Gray, V.; Gutierrez, E.; Korosteleva, O. The efficacy of a telemedicine-based weight loss program with video conference health coaching support. J Telemed Telecare. 2019, 25, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.M.; Martin, C.K.; Redman, L.M.; Heymsfield, S.B.; Lettieri, S.; Levine, J.A.; Bouchard, C.; Schoeller, D.A. Effect of dietary adherence on the body weight plateau: a mathematical model incorporating intermittent compliance with energy intake prescription. Am J Clin Nutr. 2014, 100, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Drapeau, V.; Hetherington, M.; Lemieux, S.; Provencher, V.; Tremblay, A. Psychobiological effects observed in obese men experiencing body weight loss plateau. Depress Anxiety. 2007, 24, 518–521. [Google Scholar] [CrossRef] [PubMed]
- National Research Council Committee on, D.; Health, in Diet and Health: Implications for Reducing Chronic Disease Risk. 1989, National Academies Press (US) Washington (DC).
- Flodgren, G.; Rachas, A.; Farmer, A.J.; Inzitari, M.; Shepperd, S. Interactive telemedicine: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2015, 2015, Cd002098. [Google Scholar] [CrossRef]
- Rogers, J.L.; Haring, O.M.; Wortman, P.M.; Watson, R.A.; Goetz, J.P. Medical information systems: assessing impact in the areas of hypertension, obesity and renal disease. Med Care. 1982, 20, 63–74. [Google Scholar] [CrossRef]
- Jin, K.; Khonsari, S.; Gallagher, R.; Gallagher, P.; Clark, A.M.; Freedman, B.; Briffa, T.; Bauman, A.; Redfern, J.; Neubeck, L. Telehealth interventions for the secondary prevention of coronary heart disease: A systematic review and meta-analysis. Eur J Cardiovasc Nurs. 2019, 18, 260–271. [Google Scholar] [CrossRef]
- Bayes, J.; Schloss, J.; Sibbritt, D. A randomised controlled trial assessing the effect of a Mediterranean diet on the symptoms of depression in young men (the ‘AMMEND’ study): a study protocol. Br J Nutr. 2021, 126, 730–737. [Google Scholar] [CrossRef]
- Bazrafkan, L.; Choobineh, M.A.; Shojaei, M.; Bozorgi, A.; Sharifi, M.H. How do overweight people dropout of a weight loss diet? A qualitative study. BMC nutrition. 2021, 7, 1–9. [Google Scholar]
- Avery, A.; Langley-Evans, S.C.; Harrington, M.; Swift, J.A. Setting targets leads to greater long-term weight losses and ‘unrealistic’ targets increase the effect in a large community-based commercial weight management group. J Hum Nutr Diet. 2016, 29, 687–696. [Google Scholar] [CrossRef]
Figure 1.
Participant Flow Diagram.
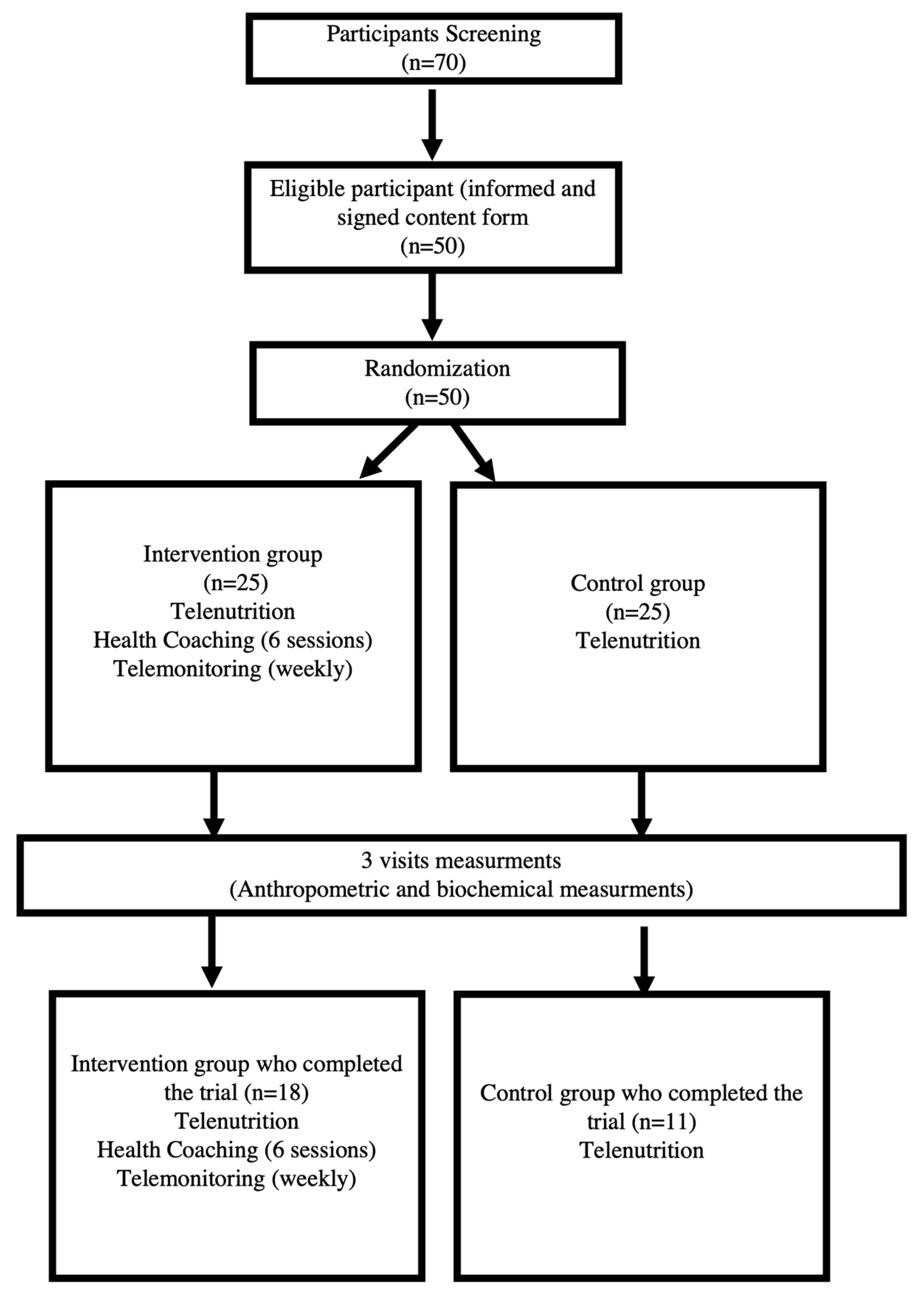

Table 1.
Baseline characteristics of participants.
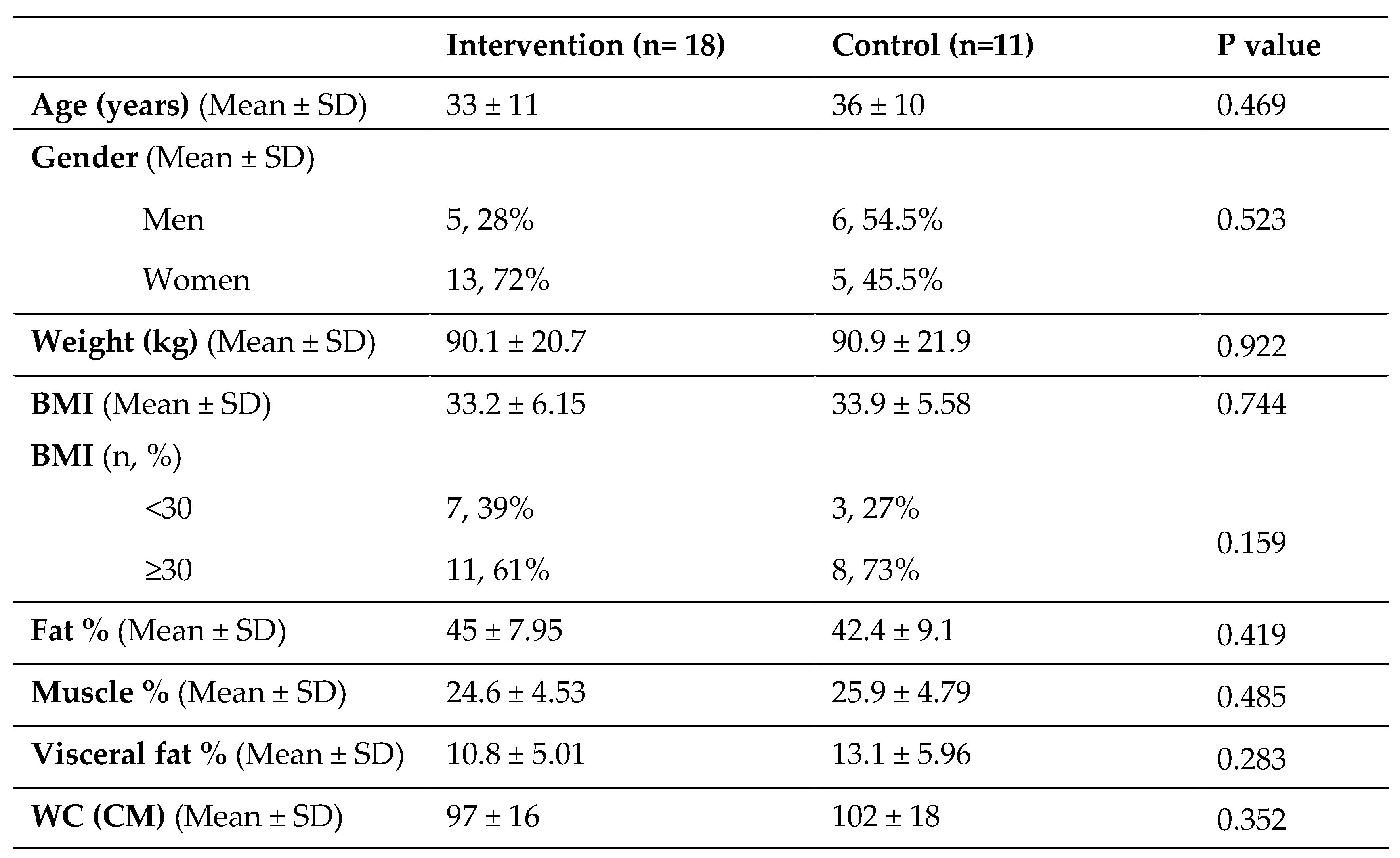
Table 2.
Clinical and biochemical measurements at all time-points.
| Variable/timepoint | Group | n | Mean | SD | P-value |
|---|---|---|---|---|---|
| Systolic BP | |||||
| Baseline | Intervention | 18 | 131.4 | 16.9 | 0.868 |
| Control | 11 | 132.5 | 16.2 | ||
| 3 months | Intervention | 18 | 119.0 | 10.4 | 0.463 |
| Control | 11 | 122.6 | 15.3 | ||
| 6 months | Intervention | 16 | 126.0 | 16.1 | 0.961 |
| Control | 9 | 126.3 | 16.2 | ||
| Diastolic BP | |||||
| Baseline | Intervention | 18 | 77.8 | 13.8 | 0.026 |
| Control | 11 | 89.0 | 9.8 | ||
| 3 months | Intervention | 18 | 75.1 | 7.3 | 0.304 |
| Control | 11 | 78.4 | 9.7 | ||
| 6 months | Intervention | 16 | 81.3 | 9.7 | 0.939 |
| Control | 9 | 81.6 | 9.2 | ||
| Cholesterol (mmol/L) | |||||
| Baseline | Intervention | 18 | 5.23 | 0.73 | 0.207 |
| Control | 11 | 5.67 | 1.11 | ||
| 3 months | Intervention | 18 | 4.68 | 0.94 | 0.16 |
| Control | 11 | 5.27 | 1.25 | ||
| 6 months | Intervention | 16 | 4.94 | 0.68 | 0.052 |
| Control | 9 | 5.61 | 0.82 | ||
| HDL (mmol/L) | |||||
| Baseline | Intervention | 18 | 1.35 | 0.25 | 0.958 |
| Control | 11 | 1.35 | 0.19 | ||
| 3 months | Intervention | 18 | 1.14 | 0.20 | 0.509 |
| Control | 11 | 1.09 | 0.18 | ||
| 6 months | Intervention | 16 | 1.14 | 0.22 | 0.421 |
| Control | 9 | 1.06 | 0.19 | ||
| LDL (mmol/L) | |||||
| Baseline | Intervention | 18 | 4.59 | 0.77 | 0.477 |
| Control | 11 | 4.90 | 1.54 | ||
| 3 months | Intervention | 18 | 3.47 | 1.03 | 0.243 |
| Control | 11 | 3.98 | 1.24 | ||
| 6 months | Intervention* | 16 | 3.49 | 0.59 | 0.034 |
| Control | 9 | 4.17 | 0.85 | ||
| TG (mmol/L) | |||||
| Baseline | Intervention | 18 | 1.05 | 0.47 | 0.431 |
| Control | 11 | 1.19 | 0.40 | ||
| 3 months | Intervention* | 18 | 0.97 | 0.35 | 0.043 |
| Control | 11 | 1.38 | 0.67 | ||
| 6 months | Intervention* | 16 | 0.99 | 0.52 | 0.037 |
| Control | 9 | 1.47 | 0.40 | ||
| Control | 11 | 7.79 | 12.73 | ||
| 6 months | Intervention | 16 | 4.36 | 4.93 | 0.115 |
| Control | 9 | 8.11 | 5.73 | ||
a P-values are for intervention vs. control. * Denotes significantly different than control group within the same timepoint (P <0.05)
Table 3.
Change of anthropometric measurements from baseline at 3 and 6 months.
| Variable/timepoint | Group | n | Mean | SD | P-valuea |
|---|---|---|---|---|---|
| Weight (kg) | |||||
| Δ at 3 months | Intervention | 18* | -3.93 | 4.58 | 0.02 |
| Control | 11 | -0.19 | 2.50 | ||
| Δ at 6 months | Intervention | 16 | -3.11 | 6.02 | 0.337 |
| Control | 9 | -1.02 | 2.69 | ||
| BMI | |||||
| Δ at 3 months | Intervention | 18* | -1.46 | 1.66 | 0.025 |
| Control | 11 | -0.14 | 1.01 | ||
| Δ at 6 months | Intervention | 16 | -1.18 | 2.35 | 0.44 |
| Control | 9 | -0.51 | 1.09 | ||
| Fat % | |||||
| Δ at 3 months | Intervention | 18* | -2.94 | 2.80 | 0.048 |
| Control | 11 | -0.89 | 1.77 | ||
| Δ at 6 months | Intervention | 16 | -1.64 | 3.12 | 0.306 |
| Control | 9 | -0.46 | 1.76 | ||
| Muscle % | |||||
| Δ at 3 months | Intervention | 16 | 1.68 | 1.77 | 0.051 |
| Control | 11 | 0.56 | 1.05 | ||
| Δ at 6 months | Intervention | 15 | 0.46 | 2.89 | 0.866 |
| Control | 9 | 0.29 | 0.93 | ||
| Visceral Fat (g) | |||||
| Δ at 3 months | Intervention | 16* | -0.94 | 1.39 | 0.048 |
| Control | 11 | -0.09 | 0.70 | ||
| Δ at 6 months | Intervention | 15 | -0.80 | 1.52 | 0.295 |
| Control | 9 | -0.22 | 0.67 | ||
| WC (CM) | |||||
| Δ at 3 months | Intervention | 18 | -5.69 | 4.47 | 0.207 |
| Control | 11 | -3.68 | 3.26 | ||
| Δ at 6 months | Intervention | 16 | -4.72 | 7.30 | 0.959 |
| Control | 9 | -4.56 | 7.73 |
a P-values are for intervention vs. control from baseline at 3 and 6 months. * Denotes significantly different than control group within the same timepoint (P <0.05).
Table 4.
Percentage of anthropometric measurements change from baseline at 3 and 6 months.
| Variable/timepoint | Group | n | Mean | SD | P-valuea |
|---|---|---|---|---|---|
| Weight (kg) | |||||
| Δ% at 3 months | Intervention | 18* | -4.06 | 4.26 | 0.022 |
| Control | 11 | -0.48 | 3.00 | ||
| Δ% at 6 months | Intervention | 16 | -3.46 | 6.49 | 0.332 |
| Control | 9 | -1.17 | 3.14 | ||
| BMI | |||||
| Δ% at 3 months | Intervention | 18* | -4.35 | 4.56 | 0.024 |
| Control | 11 | -0.63 | 3.03 | ||
| Δ% at 6 months | Intervention | 16 | -3.84 | 6.60 | 0.324 |
| Control | 9 | -1.46 | 3.25 | ||
| Fat % | |||||
| Δ% at 3 months | Intervention | 18 | -6.73 | 6.51 | 0.075 |
| Control | 11 | -2.56 | 4.66 | ||
| Δ% at 6 months | Intervention | 16 | -4.33 | 9.24 | 0.312 |
| Control | 9 | -0.96 | 3.93 | ||
| Muscle % | |||||
| Δ% at 3 months | Intervention | 16* | 7.08 | 7.87 | 0.033 |
| Control | 11 | 1.90 | 3.91 | ||
| Δ% at 6 months | Intervention | 15 | 1.61 | 11.35 | 0.929 |
| Control | 9 | 1.26 | 3.97 | ||
| Visceral Fat (g) | |||||
| Δ% at 3 months | Intervention | 16 | -7.20 | 9.50 | 0.061 |
| Control | 11 | -1.52 | 5.46 | ||
| Δ% at 6 months | Intervention | 15 | -6.02 | 13.18 | 0.376 |
| Control | 9 | -1.75 | 6.41 | ||
| WC (CM) | |||||
| Δ% at 3 months | Intervention | 18 | -5.69 | 4.13 | 0.149 |
| Control | 11 | -3.57 | 2.92 | ||
| Δ% at 6 months | Intervention | 16 | -4.59 | 6.64 | 0.876 |
| Control | 9 | -4.15 | 6.82 |
a P-values are for intervention vs. control from baseline at 3 and 6 months. * Denotes significantly different than control group within the same timepoint (P <0.05).
Table 5.
Three-month weight change (kg) in each arm stratified by BMI level and gender.
| Intervention | Control | P-value a | |
|---|---|---|---|
| BMI | |||
| <30 (34.5%) | -1.86 (2.19) | -1.27 (1.51) | 0.686 |
| ≥30 (65.5%) | -5.25 (5.28) | 0.21 (2.75) | 0.017 |
| Gender | |||
| Male (37.9%) | -7.8 (5.44)* | -0.4 (2.04) | 0.035 |
| Female (62.1%) | -2.44 (3.34) | 0.06 (3.2) | 0.171 |
a P-values are for intervention vs. control in stratified groups. * Denotes significantly different than female within the same intervention arm (P <0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



