Submitted:
29 October 2024
Posted:
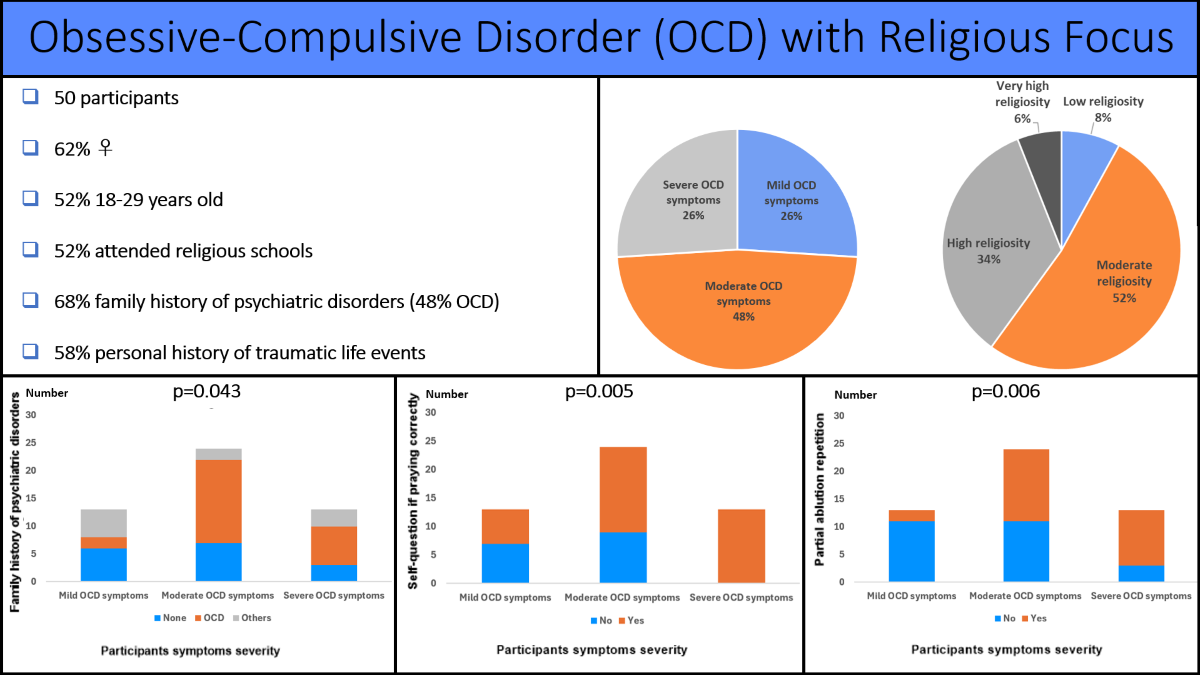
30 October 2024
You are already at the latest version
Abstract
(1) Background: Obsessive-Compulsive Disorder (OCD) is a psychiatric disorder with poorly detailed subtypes/dimensions, such as religious OCD (ROCD). To date, little is known about ROCD characteristics. This work aimed to describe the sociodemographic and clinical characteristics, as well as the religiosity and spirituality among Lebanese Muslim citizens diagnosed with OCD and exhibiting religious symptoms. (2) Methods: Outpatients were enrolled according to the following inclusion criteria: 18 years of age or above, diagnosis of OCD, presence of religious symptoms, and ability to read and understand the questionnaire. Exclusion criteria were as follows: other psychiatric disorders, and cognitive or physical impairments preventing participation. They filled in a questionnaire including the 25-item Arabic Scale of Obsessions and Compulsions (10 questions addressing obsessions, 10 questions addressing compulsions and five filler items, all of which rated on a 4–point Likert scale; higher total scores indicating increasing severity), the 26-item Spiritual Involvement and Beliefs Scale (rated on a 5-point Likert scale; higher scores indicating higher spirituality), and questions assessing the sociodemographic, clinical, and religiosity variables. (3) Results: Fifty adults (62% females, 52% aged between 18-29 years) completed the study. They had mild (26%), moderate (48%) and severe (26%) OCD symptoms. The majority had a family history of psychiatric disorders (48% OCD) and reported traumatic life events (58%). The majority attended religious school at least at one point in their life and described moderate to very high degree of self-religiosity and parental religiosity. Group comparisons (patients with mild vs. moderate vs. severe OCD symptoms) showed significant differences with regards to family history of psychiatric disorders (p=0.043), frequency of self-questioning if praying correctly (p=0.005), higher rating of partial ablution repetition (p=0.006), and frequency of partial ablution repetitions (p=0.041). No significant groups differences were noted with regards to sociodemographic or spirituality outcomes (4) Conclusion: Some religiosity variables (thoughts and practices) seem to be associated with OCD severity. The current results support the need for further research pertaining to ROCD.
Keywords:
obsessive-compulsive disorder
; religiosity
; religious obsessions
; spirituality
1. Introduction
Obsessive-Compulsive Disorder (OCD) is a heterogeneous psychiatric disorder with a lifetime prevalence of 1-3% [1,2,3]. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM), 5th edition – text revision (DSM-5-TR), OCD belongs to the diagnostic category entitled “Obsessive-compulsive and related disorders” with variable clinical presentations [4,5]. As its name implies, OCD is characterized by the presence of obsessions (e.g., recurrent intrusive unwanted thoughts, images, urges) and/or compulsions (repetitive mental acts or behaviors) aimed to neutralize the obsessions and relieve anxiety.
OCD could lead to many burdens impacting both the social and personal aspects of patients’ lives. At the demographic level, researchers have found that OCD is more common in females compared to male patients, with an onset of presentation at around 18-29 years of age [5]. While the prevalence of OCD in Lebanese society is not well established, a national epidemiologic survey evaluated the 12-month prevalence of mental disorders in Lebanon and showed a high prevalence of anxiety disorders (11.2%) [6]. In this survey, OCD was considered among the anxiety disorders (according to the 4th edition of DSM) and its 12-month prevalence was 0.1% [6].
OCD could manifest in a heterogeneous manner, and many subtypes/symptoms’ dimensions of OCD have been suggested. When classifying the subtypes/dimensions based on the focus of compulsions and obsessions, examples could include harm OCD, sexual orientation OCD, pedophilia OCD, relationship OCD, contamination/washing OCD, doubts/checking OCD, symmetry/ordering/arrangement OCD, and religious OCD (ROCD) [7]. When referring to factor analysis-based studies, a multidimensional model of OCD has been proposed, constituted of four or five factors as follows: contamination/cleaning, harmful thoughts, forbidden thoughts (including religious obsessions/rituals), symmetry/ordering/repeating/counting, and hoarding (the latter being considered a separate diagnostic entity in the most recent DSM revision) [8].
When evaluating OCD, it is important to take into consideration the comorbidities and differential diagnoses. For instance, OCD can coexist with a psychotic disorder. However, when setting the diagnosis of OCD according to DSM-5-TR, OCD symptoms per se should not be better explained by another psychiatric disorder like schizophrenia spectrum and other psychotic disorders (criterion D, in the DSM-5-TR) [5]. Differentiating OCD from psychotic symptoms could constitute sometimes a clinical challenge. Here, the absence of thought-insertion or delusional preoccupations could help, for example, distinguishing ROCD symptoms from delusional symptoms with religious themes [9].
Different OCD dimensions or subtypes might have distinct underlying mechanisms and might respond differently to treatments [2,10]. For instance, religious (as well as sexual and aggressive) symptoms are associated with a higher risk of delaying or not starting a treatment, possibly due to important perceived immorality and shame, both of which are related to the heightened response of the amygdala [10].
Neuroimaging studies have linked OCD with pathological findings involving a cortico-basal ganglia-thalamo-cortical loop (e.g., prefrontal-orbitofrontal regions, basal ganglia, and thalami, as well as cerebellar, insular, anterior cingular, temporal, parietal, and occipital areas) [11].
OCD management includes psychotherapies (i.e., cognitive behavioral therapies (CBT) - namely exposure and response prevention- as well as pharmacological treatments (i.e., selective serotonin reuptake inhibitor (SSRI)) [2] administered in monotherapy or combination. Despite the latter, patients may have a partial or lack of response, situations that are managed by other strategies (e.g., switching the antidepressants to another SSRI/clomipramine, augmentation therapy with antipsychotics, surgical interventions such as deep brain stimulation in severe and pharmaco-resistant cases, or alternative interventions that are gaining a growing interest such as noninvasive brain stimulation) [1,2].
ROCD, or scrupulosity, is an OCD with a religious theme involving intrusive blasphemous thoughts, repeating prayers, excessive morality, repetitively asking for reassurance, and unnecessary cleaning habits [12,13]. Data on this matter are scarce and sometimes inconsistent. In their research, Himle et al. noted that most of these rituals are performed by the patient to seek forgiveness and atonement for sinful thoughts or actions [12]. While this entity is poorly studied and incompletely elucidated, many studies have investigated potential factors that could increase the risk of experiencing religious obsessions and intrusive thoughts.
OCD seems to occur in a similar frequency across cultures/religions [6], although some studies have reported different findings [14]. For instance, greater risk for OCD and higher symptoms severity among Catholics were suggested by some authors, while other authors have described more obsessive-compulsive symptoms reporting in Muslim patients compared to Christian individuals (for reviews see [14]).
However, religion might affect the content of symptoms [14]. In other words, OCD symptoms may differ across different religions due to differences in doctrines and rituals performed [6]. For instance, a practicing Muslim prays five times a day and, performs a cleaning ritual that involves washing certain body parts (i.e., partial ablution) for a predetermined number of times before the prayers, and practices fasting during the holy month of Ramadan [15]. Such religious practices and rituals constitute important issues in Islam and are performed in conformity with strict religious rules [15]. In addition, doubts about religious practices could be perceived as a test of faithfulness (evil temptations) and they are accepted [16]. Moreover, it was found that Catholic individuals are more prone to develop ritualistic ROCD while Protestants are expected to manifest ROCD with intrusive negative thoughts related to faith [12]. Furthermore, in the Jewish community, OCD manifestation seem to be also shaped by the Jewish scriptures [17]. In other words, the pattern of thoughts or actions would be associated with their religious rite sand rules.
Besides religion, religiosity might also be associated with the severity of manifestations albeit the availability of inconsistent findings [14]. For instance, while no correlation between religiosity and OCD symptoms severity was reported by some authors, others have documented more obsessive thoughts and checking with higher religiosity rating (for reviews see [14]).
There are no clear diagnostic criteria and risk factors listed for ROCD in the literature, and studies conducted thus far have sometimes linked the degree of religiosity to the occurrence of religious obsessions, with no data on the role of sociodemographic variables or past personal/family history of psychiatric illnesses on the development of religious obsessions [18].
Lebanon, a Middle Eastern country, is known for the diverse religious sects encountered within its population, with Islam and Christianity being the two major groups. Moreover, religion is deeply enrooted in Lebanese culture, societal organization, educational system, and political structure [19,20]. As such, one can appreciate the impact that religion has on Lebanese citizens’ decision-making in daily life errands and on their personal lives. This relationship might affect citizens with pre-existing OCD by increasing their intrusive thoughts and compulsive behaviors, gearing them toward religious topics, and leaving them with great distress regarding their religious thoughts and rituals. It is also worth mentioning that Lebanon has faced periods of crisis and conflicts, leading to increased stressors and traumatic life events for its population, both of which can predispose individuals to a variety of psychiatric disorders.
The current work addresses religious OCD symptoms, particularly among Lebanese Muslim citizens who were previously diagnosed with OCD. It aims to characterize this clinical population in terms of sociodemographic and clinical characteristics, as well as religiosity and spirituality. It also aims to assess the relationship between the latter features and OCD symptoms’ severity.
With the scarcity of data available on this topic and with the Lebanese population being known for the prevalence of its religiosity and spirituality, making it an adequate target population for studying ROCD, the current study aims to address this gap in the literature and pave the way for future comparative studies to be done to establish risk factors and diagnostic criteria for this poorly studied and underreported entity.
2. Materials and Methods
This is a prospective cross-sectional study in adult patients with ROCD.
2.1. Participants
The participants for this study were recruited through an online survey platform. Inclusion criteria were as follows: outpatient adults aged 18 years and above, having a clinical diagnosis of OCD according to the DSM-5-TR diagnostic criteria [5], having religious symptoms, and being able to read and understand the questionnaire.
Exclusion criteria were the presence of other psychiatric disorders, or the presence of cognitive or physical impairments preventing participation.
A list of patients with ROCD from the clinical database was prepared. The list was numbered, and the names were masked. Among these patients, 50 patients were selected using an online randomizer application (randomizer.org) which generated a dataset of 50 unique numbers. Afterwards, patients were contacted accordingly. All participants provided informed consent before engaging in the survey.
2.2. Survey Instrument
The survey instrument was developed for this research project and was created using an online survey platform, facilitating easy distribution and collection of responses.
The survey contains multiple sections designed to gather information on participants' sociodemographic and clinical characteristics related to the topic as follows: age, sex, relationship status, childhood, and current residence areas, religious vs. nonreligious school, educational level, socioeconomic status, age of diagnosis, pharmacological or psychological interventions, obsessive and compulsive symptoms, family history of psychiatric disorders.
The severity of the participants’ OCD was assessed using the Arabic Scale of Obsession Compulsion (ASOC) developed by Abdel-Khalek [20,21,22]. ASOC originally consisted of 32 items answered in a yes/no format. The revised version used here consists of 25 items: 10 items addressing obsessions, 10 items addressing compulsions, and five filler items to control response bias without being included in the total scores (items #1, #5, #12, #17 and #20). Items are scored on a 4-point Lickert scale (no, some, much and always). ASOC scores could range from 20 to 80, indicating mild (20-39), moderate (40-59) or severe (60-80) symptomatology [21,22,23,24]. ASOC is validated in the Arabic Language and has good psychometric properties (high internal consistency: αCronbach= 0.897) [20,22].
Spirituality was assessed using the Spiritual Involvement and Beliefs Scale (SIBS) developed by Hatch and colleagues [25]. The scale involves 26 questions rated on a 5-point scale (strongly agree, agree, neutral, disagree, and strongly disagree) assessing internal beliefs, external practices, personal applications (e.g., practicing humility and forgiveness toward others), and existential and meditative beliefs. Scores vary between 26 and 130, with high scores implying high spirituality [25]. SIBS is validated in the Arabic Language and has good psychometric properties (αCronbach= 0.76) [26].
The patients’ degree of religiosity was assessed by a questionnaire designed to assess the practice, frequency, and location preference of praying, fasting, partial ablution (washing body parts), and full ablution. The questionnaire also implied questions assessing whether praying/fasting was considered to be done correctly or accepted by God, and if there are blasphemous thoughts, skeptical thoughts regarding the holy book or prophetic hadiths, or experiencing intrusive thoughts related to ritual impurities (body secretions, blood, flatulence, animals’ secretions, or shaking hands with a stranger of the opposite sex). The participants were also asked to report the frequency of visiting religious places and to assess their parents as well as their own degree of religiosity.
2.3. Data Collection Procedure
To collect data, the online survey link was distributed to participants through their Psychiatrists/Psychotherapists. The survey remained accessible for two weeks, allowing participants ample time to complete it. Upon clicking the survey link, participants were directed to a secure online survey platform where they encountered the survey questions. It was a self-administered survey, offering participants the flexibility to complete it at their convenience. To ensure the data's quality and reliability, participants were required to answer all mandatory questions before submitting the survey.
2.4. Ethical Considerations
Our study adhered to ethical guidelines following IRB approval from the Lebanese American University IRB Office. Participants' confidentiality and anonymity were strictly maintained throughout the data collection process, collecting no personal identifying information. All collected data were securely stored and accessed only by our research team. As stated above, this study has been reviewed and approved by the LAU IRB under the following tracking number “LAUMCRH.NM1.17/Oct/2022”.
2.5. Data Analysis
Upon completing the data collection phase, survey responses were exported from the online platform into statistical analysis software for further analysis. Data were analyzed using the GraphPad Prism 10.2. First, descriptive statistics were used to present the participants' sociodemographic, clinical, religiosity, and spirituality data.
A bivariate analysis was performed to understand the relationship between ASOC and all the sociodemographic and clinical characteristics from the other side. Participants were classified into three groups according to mild, moderate, and severe ASOC scores. The relationship of ASOC with quantitative data was performed using the Kruskal-Wallis test (since data did not follow a normal distribution according to the Shapiro–Wilk test) and with qualitative data using Fisher’s exact test.
In addition, a subgroup analysis was performed using the Kruskal-Wallis (in case of three or more categories) or Mann-Whitney test (in case of two categories) to compare the ASOC scores across the different categories of the sociodemographic, clinical and religiosity variables. A correlation analysis was also employed using Spearman’s test to assess the relation between ASOC and SIBS scores.
Quantitative variables were expressed as mean ± SD, and qualitative variables as number or percentage. P values were based on 2-tailed tests, with values <0.05 considered statistically significant.
3. Results
3.1. Descriptive Statistics
Overall, 50 eligible responses were collected from the online survey. Out of these, 19 (38%) were males, and 31 (62%) were females. Among them, 26 (52%) were aged between 18-29 years old, 23 (46%) were between 30-49 years old, and only one respondent was between 50-64 years old. 82% of participants lived outside the capital during their childhood, and 80% resided outside the capital at the time of the study. In terms of education, 72% of respondents completed a higher university degree. Regarding socioeconomic status (SES), 46% of the participants earn between 2-5 million Lebanese pounds per month, classified as low SES given the country ongoing economic inflation.
Concerning marital status, 48% of them were married and 46% were never married. Regarding the type of school attended, 52% attended religious schools [exclusively (24%) or at one point in their life (28%)], while 48% reported attending a non-religious school.
Most participants were diagnosed with OCD after the age of 18 years (44% between 18-25 years old, 30% after 25 years old) by a mental health specialist. Among them, 54% are not taking any medication and have not considered attending or have attended any psychotherapy sessions. Moreover, a positive family history of psychiatric disorders was common among participants, consisting of OCD (48%), depression (10%), generalized anxiety disorder (6%), or other disorders (4%). 58% reported having experienced traumatic life events.
All participants practice praying, with the majority doing so daily or weekly (86%). When asked about obsessions related to prayer, 68% reported questioning whether they were praying correctly, and 70% questioned whether their prayers were accepted by God. However, only 44% reported repeating the prayer one (14%), two (22%), or three and more (8%) times to calm obsessive thoughts. Similarly, all participants reported practicing partial ablution, with 50% repeating it one (14%), two (20%), or three times and more (16%). Moreover, most participants (98%) practiced full ablution, with 38% repeating it one (20%), two (6%), or three times and more (12%).
Concerning fasting rituals, 94% reported practicing them during the holy month of Ramadan only (54%), intermittently during the year on special occasions (14%), or 1-6 months per year (26%). A subset of respondents reported questioning whether the fasting was done correctly (36%) or accepted by God (38%), prompting them to repeat their fast (20%). Additionally, 72% reported experiencing intrusive thoughts related to ritual impurities. 48% reported experiencing them multiple times per day, prompting them to act upon the thoughts sometimes or every time in 68% of the cases.
When asked about blasphemous thoughts or skeptical thoughts regarding holy books, religious scripts, or prophetic sayings, most respondents denied experiencing any.
Participants were asked about their parents as well as their own degree of religiosity. The majority reported moderate (46%), high (30%), or very high (8%) degree of religiosity in their parents, as well as a moderate (52%), high (34%), or very high (6%) degree of religiosity in themselves. The majority of the respondents (82%) reported visiting religious places. ASOC score was 49.82 ± 12.37, and SIBS score was 81.80 ± 8.85.
3.2. Bivariate Analysis
Data were compared among participants with mild (26%), moderate (48%), and severe symptoms (26%) (i.e., according to ASOC). No significant differences were observed among the three groups with regard to sociodemographic variables.
Concerning clinical variables, significant group differences were observed with regards to family history of psychiatric disorders (p=0.043).
Significant differences were also observed regarding some religiosity variables, namely the frequency of self-questioning if praying correctly (p=0.005), the repetition of partial ablution occurrence (p=0.006) and frequency (p=0.041). No group differences were observed with regard to spirituality (SIBS) outcomes. Results are summarized in Table 1. Significant findings are presented in Figure 1.
Subgroup analysis considering ASOC scores as a continuous variable and comparing it among the different categories of each qualitative variable (socio-demographic, clinical and religiosity variables) yielded significantly higher ASOC scores among patients who questioned themselves if praying correctly compared to those who did not (52.91±12.68 vs. 43.25±8.85, respectively; U=390.000; p=0.014), and among patients who repeated partial ablution compared to those who did not (53.68±11.75 vs. 45.96±11.97, respectively; U=425.500; p=0.028). No other significant results were observed. Data are summarized in Table 2.
Finally, no significant correlation was found between ASOC and SIBS scores (ρ=0.121, p=0.402).
4. Discussion
In this study, we described the sociodemographic characteristics, clinical variables, religiosity, and spirituality among patients diagnosed with OCD exhibiting ROCD symptoms and we assessed the relationship between these variables and OCD symptoms severity.
4.1. Sociodemographic and Clinical Characteristics
The study comprised a sample of 50 participants, with a higher representation of females compared to males, as observed in a previous study performed in Morocco [18]. Most of them were aged between 18-29 years, followed by the 30-49 years age group, and a smaller proportion from the 50-64 years age group. They were mostly diagnosed after 18 years of age. These findings align with the literature where, despite mixed findings, OCD seems to be more frequent among adult females while it seems to be more common in male children [27]. Females seem to have an older age of onset compared to males [28]. Group comparison showed no significant sex differences according to OCD symptoms severity, in line with some previous findings on this matter [28]. Conversely, in terms of ROCD, some studies suggest ROCD symptoms to be more frequent in males compared to females [29].
Most of the cohort attended religious schools at least at one point in their life and described a certain degree of parents’ religiosity. Limited data are available regarding the relationship between OCD manifestation and cultural or educational background [14]. With some exceptions, the available data suggest a higher frequency of religious themes in Middle Eastern countries compared to occidental and fast-east countries [17]. Culture might not only shape OCD symptoms (obsessions content, compulsions expression), but it might also impact symptom interpretation by the patients, as well as symptom management [17,30]. These merits further assessment.
Significant group differences were observed regarding family history of psychiatric disorders and 68% had a positive family history of psychiatric disorders (most frequently OCD). However, statistical significance was not reached in subgroup analysis, a finding that could be attributed to the small sample size. A high risk of OCD in first-degree relatives was previously reported [31,32]. For instance, a risk of ~23% (odds ratios: 11-32) was reported in controlled family studies [31]. Moreover, in a nationwide study including 23 258 175 participants with OCD and 89 500 first-degree relatives, a high relative risk of OCD was observed among first-degree relatives (relative risk: 8.11) [32].
More than half of the participants reported traumatic life events. Some evidence suggests a relationship between traumatic life events and OCD [33,34,35]. In previous works, traumatic life events were reported by 54-60.8% of patients with OCD [33,34]. Some authors suggest that experiencing traumatic incidents is common in late-onset OCD compared to early-onset genetic OCD [35]. In addition, in a large meta-analysis involving 24 articles (4 557 participants), a significant association was observed between traumatic life events and OCD symptom severity [36]. Interestingly, this relationship was found to be stronger in females than in males, and the association concerns the severity of compulsions but not obsessions [36].
4.2. Religiosity and Spirituality
In this work, most participants reported a certain degree of religiosity (moderate to very high). Additionally, a significant proportion reported regular visits to religious places. Religious practices were also prevalent, with almost all participants reporting engagement in daily or weekly prayer (86%), practicing ablution (98%), and fasting rituals (94%) during Ramadan or other occasions. This demonstrates the importance of religious practices in their lives.
Obsessions related to religious practices were also assessed. A significant proportion of participants reported questioning the correctness of their prayers (68%) and whether their prayers were accepted by God (70%). A subset of patients (44%) reported engaging in repetitive prayer to alleviate obsessive thoughts. Regarding ritual impurities, most participants (72%) reported experiencing intrusive thoughts related to specific ritual impurities, leading them to perform compulsive actions.
When comparing patients according to their OCD symptoms severity, significant group differences were observed regarding the frequency of self-questioning if praying correctly, the occurrence of partial ablution repetition as well as the frequent of this practice. In addition, the subgroup analysis revealed significantly higher ASOC scores among patients who questioned themselves if praying correctly and repeated partial ablution compared to those who did not.
Such results are consistent with those of previous studies. In one study from Morocco, self-questioning if praying correctly was the most common religious obsession affecting 47% of patients [18]. In another work from Saudi Arabia, half of the obsessions concerned prayers and the associated washing rituals [37].
In fact, no causality link seems to exist between religiosity/spirituality and OCD occurrence. However, in religious individuals, the symptoms would manifest with religious themes [38]. Particularly, the symptoms’ expression may be related to the religion in question, such as self-questioning if praying correctly or repeating washing rituals in the case of Muslims.
In addition, as found in the present work, a relationship seems to exist between the degree of religiosity/spirituality and the intensity of symptoms [16,30,39]. For instance, in a group of Muslim and Christian subjects from Turkey and Canada, Yorulmaz and colleagues have found an association between religiosity ratings (based on the Religiousness Screening Questionnaire) and the frequency of obsessive thoughts and checking (evaluated by means of the Obsessive-Compulsive Beliefs Questionnaire) [16]. In another work by Rakesh and colleagues involving patients with OCD from India, a significant correlation was found between religiosity (Belief into Action Scale) and OCD symptoms severity (Yale-Brown Obsessive Compulsive Scale) [39].
In some works, this relationship between religiosity and OCD symptoms severity seems to be moderated by some variables such as disgust sensitivity or thought-action fusion [40,41]. The latter consists of maladaptive cognitions about the link between mental events and behaviors (believing that thoughts are morally equivalent to action) which could be fueled by the teaching that may underlie some religious doctrines [40,41]. Thought-action fusion might induce thought suppression which could subsequently promote the symptoms [42].
4.3. Limitations and Implications
It is important to consider the limitations of the study. The sample size was relatively small and not representative of the entire Lebanese population. The study relied on self-reported measures, which can be subject to recall bias or social desirability bias. Additionally, the study did not include a control group which could have helped further understanding the significance of the reported patients’ data in comparison with nonclinical individuals sharing similar cultural and religious backgrounds and practicing, for instance, fasting rituals and ablutions. Moreover, the study focused on one religious group (Muslims), limiting the generalizability of the results to other religions. Furthermore, the study assessed the current pharmacological status of patients as well as the current or past management with psychotherapies, but it did not collect in detail the therapeutics of the prior months (treatment type, dosage, initiation date). Although no group differences with regard to the treatment status (subgroup analysis results), the existence of prior therapeutic interventions could mitigate the severity and manifestation of key ROCD symptoms and might modify the results.
Despite these limitations, the study provides valuable preliminary findings that shed light on the demographic characteristics, mental health symptoms, religious practices, and religious obsessions among a specific group of Lebanese individuals. These findings may contribute to the understanding of the intersection between religiosity and mental health and inform future research and interventions in this domain. Further studies with larger and more diverse samples are necessary to validate and expand upon these initial findings.
5. Conclusions
The main finding of this work is a significant association between OCD symptoms severity and some religiosity variables, namely self-questioning if praying correctly and partial ablution repetition. This study provides insights into the characteristics of patients exhibiting ROCD. The findings show that religious practices are significant in their lives, and religious obsessions are not uncommon. Although the study has limitations, it opens the door for further research in this under-explored area of mental health. Mental health professionals should be aware of religious obsessions as a potential aspect of OCD symptomatology, approaching it with cultural sensitivity. Understanding the interplay between religiosity and OCD could lead to better mental health care. Further research is needed on this matter.
Supplementary Materials
None.
Author Contributions
Conceptualization, Wissam Al Rida Ayoub and Ronza Abdel Rassoul; Data curation, Jana Dib El Jalbout; Formal analysis, Samar Ayache and Moussa Chalah; Investigation, Wissam Al Rida Ayoub and Nancy Maalouf; Methodology, Wissam Al Rida Ayoub, Samar Ayache, Moussa Chalah and Ronza Abdel Rassoul; Project administration, Ronza Abdel Rassoul; Software, Jana Dib El Jalbout; Supervision, Moussa Chalah and Ronza Abdel Rassoul; Visualization, Jana Dib El Jalbout; Writing – original draft, Wissam Al Rida Ayoub, Jana Dib El Jalbout, Nancy Maalouf and Ronza Abdel Rassoul; Writing – review & editing, Samar Ayache and Moussa Chalah.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Lebanese American University Medical Center – Rizk Hospital (tracking number: “LAUMCRH.NM1.17/Oct/2022”).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data can be made available by the corresponding author upon reasonable requests.
Acknowledgments
The authors would like to thank the study participants for taking part of this work and the reviewers who help improving the quality of this article.
Conflicts of Interest
S.S.A. declares having received compensation from Exoneural Network AB, Sweden and Ottobock, France. M.A.C. declares having received compensation from Janssen Global Services LLC, Exoneural Network AB, Sweden, and Ottobock, France. The remaining authors declare no conflicts of interest.
References
- Hirschtritt, M.E.; Bloch, M.H.; Mathews, C.A. Obsessive-Compulsive Disorder: Advances in Diagnosis and Treatment. JAMA. 2017, 317, 1358–1367. [Google Scholar] [CrossRef] [PubMed]
- Chalah, M.A.; Ayache, S.S. Could Transcranial Direct Current Stimulation Join the Therapeutic Armamentarium in Obsessive-Compulsive Disorder? Brain Sci. 2020, 10, 125. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Costa, D.L.C.; Lochner, C.; Miguel, E.C.; Reddy, Y.C.J.; Shavitt, R.G; et al. Obsessive–compulsive disorder. Vol. 5, Nature Reviews Disease Primers; Nature Publishing Group, 2019. [Google Scholar]
- Brock, H.; Hany, M. Obsessive-Compulsive Disorder. 2023 May 29. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 29 May 2024. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed., text rev.), 2022.
- Karam, E.G.; Mneimneh, Z.N.; Karam, A.N.; Fayyad, J.A.; Nasser, S.C.; Chatterji, S.; et al. Prevalence and treatment of mental disorders in Lebanon: a national epidemiological survey. Lancet. 2006, 367, 1000–6. [Google Scholar] [CrossRef]
- Ramezani, Z.; Rahimi, C.; Mohammadi, N. Birth Order and Sibling Gender Ratio of a Clinical Sample Predicting Obsessive Compulsive Disorder Subtypes Using Cognitive Factors. Iranian J Psychiatry. Iran J Psychiatry. 2016, 11, 75–81. [Google Scholar]
- Stein, D.J.; Costa, D.L.C.; Lochner, C.; Miguel, E.C.; Reddy, Y.C.J.; Shavitt, R.G.; et al. Obsessive-compulsive disorder. Nat Rev Dis Primers. 2019, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Palermo, S.; Marazziti, D.; Baroni, S.; Barberi, F.M.; Mucci, F. The Relationships Between Obsessive-Compulsive Disorder and Psychosis: An Unresolved Issue. Clin Neuropsychiatry. 2020, 17, 149–157. [Google Scholar]
- Thorsen, A.L.; Kvale, G.; Hansen, B.; van den Heuvel, O.A. Symptom dimensions in obsessive-compulsive disorder as predictors of neurobiology and treatment response. Curr. Treat. Options Psychiatry. 2018, 5, 182–194. [Google Scholar] [CrossRef]
- Brennan, B.P.; Wang, D.; Li, M.; Perriello, C.; Ren, J.; Elias, J.A.; et al. Use of an Individual-Level Approach to Identify Cortical Connectivity Biomarkers in Obsessive-Compulsive Disorder. Boil. Psychiatry Cogn. Neurosci. Neuroimaging. 2019, 4, 27–38. [Google Scholar] [CrossRef]
- Himle, J.A.; Chatters, L.M.; Taylor, R.J.; Nguyen, A. The relationship between obsessive-compulsive disorder and religious faith: Clinical characteristics and implications for treatment. Psycholog Relig Spiritual. 2011, 3, 241–258. [Google Scholar] [CrossRef]
- Greenberg, D.; Huppert, J.D. Scrupulosity: a unique subtype of obsessive-compulsive disorder. Curr Psychiatry Rep. 2010, 12, 282–9. [Google Scholar] [CrossRef]
- Nicolini, H.; Salin-Pascual, R.; Cabrera, B.; Lanzagorta, N. Influence of Culture in Obsessive-compulsive Disorder and Its Treatment. Curr Psychiatry Rev. 2017, 13, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Besiroglu, L.; Karaca, S.; Keskin, I. Scrupulosity and obsessive compulsive disorder: the cognitive perspective in Islamic sources. J Relig Health. 2014, 53, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Yorulmaz, O.; Gençöz, T.; Woody, S. OCD cognitions and symptoms in different religious contexts. J Anxiety Disord. 2009, 23, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Vinker, M.; Jaworowski, S.; Mergui, J. [Obsessive compulsive disorder (OCD) in the ultra-orthodox community--cultural aspects of diagnosis and treatment]. Harefuah. 2014, 153, 463–466, 498, 497. [Google Scholar] [PubMed]
- Khoubila, A.; Kadri, N. [Religious obsessions and religiosity]. Can J Psychiatry. 2010, 55, 458–63. [Google Scholar] [CrossRef]
- Badaan, V.; Richa, R.; Jost, J.T. Ideological justification of the sectarian political system in Lebanon. Curr Opin Psychol. 2020, 32, 138–145. [Google Scholar] [CrossRef]
- Baytiyeh, H. Has the Educational System in Lebanon Contributed to the Growing Sectarian Divisions? Educ. Urban Soc. 2017, 49, 546–559. [Google Scholar] [CrossRef]
- Abdel-Khalek, A.M. The development and validation of the Arabic Obsessive Compulsive Scale. Eur J Psychol Assess. 1998, 14, 146–158. [Google Scholar] [CrossRef]
- Abdel-Khalek, A.M. Manual of the Arabic Scale of Obsession-compulsion; The Anglo-Egyptian Bookshop: Cairo, 1992. [Google Scholar]
- Abdel-Khalek, A.M. (2018). The construction and validation of the revised Arabic Scale of Obsession-Compulsion (ASOC). Online J Neurol Brain Disord. 2018, 1, 1–7. [Google Scholar]
- Metwally Elsayed, M.; Ahmed Ghazi, G. Fear of covid-19 pandemic, obsessive-compulsive traits and sleep quality among first academic year nursing students, Alexandria University, Egypt. Egypt. J. Health Care. 2021, 12, 224–241. [Google Scholar] [CrossRef]
- Hatch, R. L.; Burg, M. A.; Naberhaus, D.S.; Hellmich, L.K. The Spiritual Involvement and Beliefs Scale. Development and testing of a new instrument. J Fam Pract. 1998, 46, 476–86. [Google Scholar] [PubMed]
- Musa, A.S. Psychometric Evaluation of an Arabic Version of the Spiritual Involvement and Beliefs Scale in Jordanian Muslim College Nursing Students. J. Educ. Pract. 2015, 6, 64–73. [Google Scholar]
- Mathes, B. M.; Morabito, D. M.; Schmidt, N.B. Epidemiological and Clinical Gender Differences in OCD. Curr. Psychiatry Rep. 2019, 21, 36. [Google Scholar] [CrossRef] [PubMed]
- Benatti, B.; Girone, N.; Celebre, L.; Vismara, M.; Hollander, E.; Fineberg, N. A.; et al. The role of gender in a large international OCD sample: A Report from the International College of Obsessive-Compulsive Spectrum Disorders (ICOCS) Network. Compr Psychiatry. 2022, 116, 152315. [Google Scholar] [CrossRef] [PubMed]
- Mathis, M.A.; Alvarenga, P.D.; Funaro, G.; Torresan, R.C.; Moraes, I.; Torres, A. R.; et al. Gender differences in obsessive-compulsive disorder: a literature review. Braz J Psychiatry, 2011, 33, 390–399. [Google Scholar] [CrossRef]
- Hassan, W.; El Hayek, S.; de Filippis, R.; Eid, M.; Hassan, S.; Shalbafan, M. Variations in obsessive compulsive disorder symptomatology across cultural dimensions. Front Psychiatry. 2024, 15, 1329748. [Google Scholar] [CrossRef]
- Balachander, S.; Meier, S.; Matthiesen, M.; Ali, F.; Kannampuzha, A.J.; Bhattacharya, M.; et al. Are There Familial Patterns of Symptom Dimensions in Obsessive-Compulsive Disorder? Frontiers Psychiatry. 2021, 12, 651196. [Google Scholar] [CrossRef]
- Huang, M.H.; Cheng, C.M.; Tsai, S.J.; Bai, Y.M.; Li, C.T.; Lin, W.C.; et al. Familial coaggregation of major psychiatric disorders among first-degree relatives of patients with obsessive-compulsive disorder: a nationwide study. Psychol Med. 2021, 51, 680–687. [Google Scholar] [CrossRef]
- Cromer, K.R.; Schmidt, N. B.; Murphy, D.L. An investigation of traumatic life events and obsessive-compulsive disorder. Behav Res Ther. 2007, 45, 1683–1691. [Google Scholar] [CrossRef]
- Rosso, G.; Albert, U.; Asinari, G.F.; Bogetto, F.; Maina, G. Stressful life events and obsessive-compulsive disorder: clinical features and symptom dimensions. Psychiatry Res. 2012, 197, 259–64. [Google Scholar] [CrossRef]
- Murayama, K.; Nakao, T.; Ohno, A.; Tsuruta, S.; Tomiyama, H.; Hasuzawa, S.; et al. Impacts of Stressful Life Events and Traumatic Experiences on Onset of Obsessive-Compulsive Disorder. Frontiers Psychiatry. 2020, 11, 561266. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.L.; Brock, R.L. The effect of trauma on the severity of obsessive-compulsive spectrum symptoms: A meta-analysis. J Anxiety Disord. 2017, 47, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Mahgoub, O.M.; Abdel-Hafeiz, H.B. Pattern of obsessive-compulsive disorder in Eastern Saudi Arabia. Br J Psychiatry. 1991, 158, 840–842. [Google Scholar] [CrossRef] [PubMed]
- Abramowitz, J.S.; Buchholz, J.L. Chapter 4 - Spirituality/religion and obsessive–compulsive-related disorders. Handbook of Spirituality, Religion, and Mental Health (Second Edition). 2020, 61-78.
- Rakesh, K.; Arvind, S.; Dutt, B.P.; Mamta, B.; Bhavneesh, S.; Kavita, M.; et al. The Role of Religiosity and Guilt in Symptomatology and Outcome of Obsessive Compulsive Disorder. Psychopharmacol Bull. 2021, 51, 38–49. [Google Scholar]
- Inozu, M.; Ulukut, F.O.; Ergun, G.; Alcolado, G.M. The mediating role of disgust sensitivity and thought-action fusion between religiosity and obsessive compulsive symptoms. Int J Psychol. 2014, 49, 334–41. [Google Scholar] [CrossRef]
- Williams, A.D.; Lau, G.; Grisham, J.R. Thought-action fusion as a mediator of religiosity and obsessive-compulsive symptoms. J Behav Ther Exp Psychiatry. 2013, 44, 207–12. [Google Scholar] [CrossRef]
- Rassin, E.; Muris, P.; Schmidt, H.; Merckelbach, H. Relationships between thought-action fusion, thought suppression and obsessive-compulsive symptoms: a structural equation modeling approach. Behav Res Ther. 2000, 38, 889–97. [Google Scholar] [CrossRef]
Figure 1.
Significant group differences with regards to clinical and religiosity variables among participants with obsessive-compulsive disorder (OCD).
Figure 1.
Significant group differences with regards to clinical and religiosity variables among participants with obsessive-compulsive disorder (OCD).
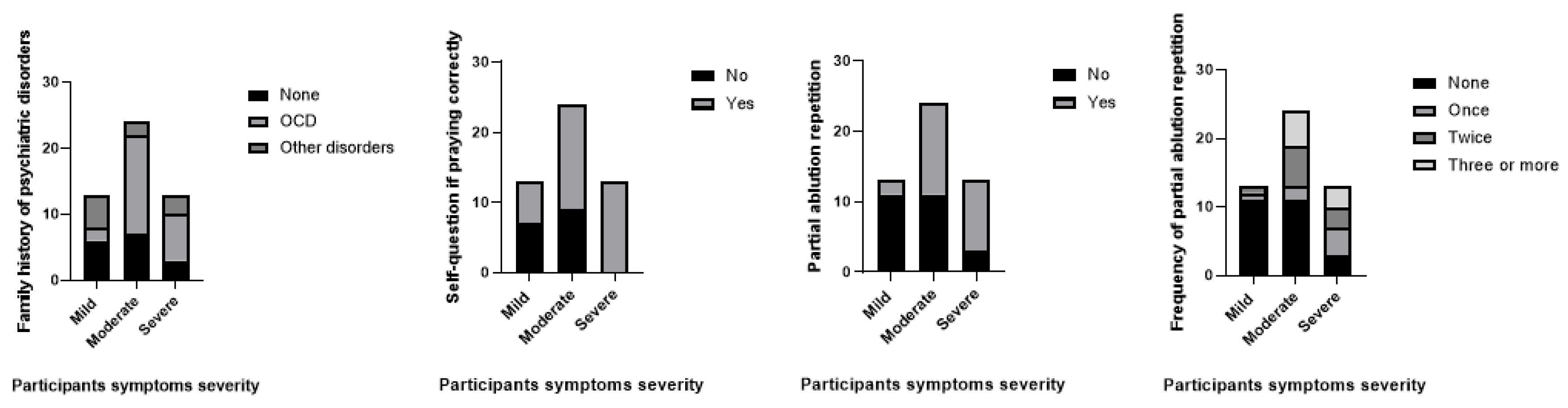

Table 1.
Comparison of Sociodemographic, clinical, religiosity, and spirituality variables among patients with mild, moderate, and severe obsessive-compulsive symptoms. Data are presented in terms of the number of participants, except for SIBS scores which are presented as mean ± SD. USD: United States Dollar.
Table 1.
Comparison of Sociodemographic, clinical, religiosity, and spirituality variables among patients with mild, moderate, and severe obsessive-compulsive symptoms. Data are presented in terms of the number of participants, except for SIBS scores which are presented as mean ± SD. USD: United States Dollar.
| Mild (n=13) | Moderate (n=24) | Severe (n=13) | P value | |
|---|---|---|---|---|
|
Age 18-29 years 30-49 years ≥50 years |
5 7 1 |
13 11 0 |
8 5 0 |
0.489 |
|
Sex Females Males |
5 8 |
17 7 |
9 4 |
0.162 |
|
Educational level Middle school High school University degree |
1 2 10 |
1 9 14 |
1 0 12 |
0.057 |
|
Relationship status Single Married Divorced |
6 6 1 |
13 10 1 |
4 8 1 |
0.713 |
|
Area of living (childhood) Outside the capital Within the capital |
10 3 |
20 4 |
11 2 |
0.897 |
|
Area of living (current) Outside the capital Within the capital |
10 3 |
19 5 |
11 2 |
>0.999 |
|
Monthly living income (Lebanese pounds and equal rates in USD) <2 millions (~22 USD) Between 2 & 5 millions (~22-56 USD) Between 5 & 10 millions (56 –112 USD) Between 10 & 20 millions (112-224 USD) >20 millions (>224 USD) |
0 3 4 2 4 |
3 14 2 3 2 |
2 6 1 2 2 |
0.240 |
|
Attended school Religious Non-religious Both |
3 6 4 |
5 13 6 |
4 5 4 |
0.913 |
|
Parents’ relationship status Married Divorced Widowed |
12 0 1 |
18 4 2 |
11 1 1 |
0.650 |
|
Traumatic life events No Yes |
7 6 |
9 15 |
5 8 |
0.662 |
|
Age of diagnosis Before 12 years 12-18 years 18-25 years >25 years |
2 0 6 5 |
1 8 9 6 |
1 1 7 4 |
0.184 |
|
Family history of psychiatric illness None OCD Others |
6 2 5 |
7 15 2 |
3 7 3 |
0.043 |
|
Current OCD medications Untreated Treated |
7 6 |
10 14 |
10 3 |
0.119 |
|
Current or past psychotherapy None Past Current |
9 1 3 |
12 7 5 |
6 5 2 |
0.482 |
|
Praying frequency Rarely Irregularly Daily or weekly |
0 1 12 |
1 2 21 |
0 3 10 |
0.702 |
|
Self-question if praying correctly No Yes |
7 6 |
9 15 |
0 13 |
0.005 |
|
Self-question if prayers are accepted by God No Yes |
4 9 |
10 14 |
1 12 |
0.111 |
|
Frequency of prayers repetition if questioning None Once Twice Three of more |
9 1 1 2 |
14 2 6 2 |
5 5 3 0 |
0.162 |
|
Praying location No preference As long as the setting is available Home only Home & praying place |
7 1 3 2 |
16 1 4 3 |
6 2 2 3 |
0.830 |
|
Frequency of partial ablution Daily 3-5/day More than 5/day |
12 1 |
18 6 |
12 1 |
0.404 |
|
Partial ablution repetition No Yes |
11 2 |
11 13 |
3 10 |
0.006 |
|
Frequency of partial ablution repetition None Once Twice Three or more |
11 1 1 0 |
11 2 6 5 |
3 4 3 3 |
0.041 |
|
Partial ablution location No preference Home only Home & praying place |
6 5 2 |
15 9 0 |
4 5 4 |
0.058 |
|
Full ablution repetition No Yes |
10 3 |
16 8 |
5 8 |
0.123 |
|
Frequency of full ablution repetition None Once Twice Three of more |
10 2 1 0 |
16 4 2 2 |
5 4 0 4 |
0.166 |
|
Frequency of fasting practice None During the holy month 1-6 months per year Throughout the year during religious ceremony |
0 10 3 0 |
3 11 5 5 |
0 6 5 2 |
0.252 |
|
Self-question if fasting correctly No Yes |
10 3 |
16 8 |
6 7 |
0.282 |
|
Self-question if fasting accepted by God No Yes |
9 4 |
15 9 |
7 6 |
0.703 |
|
Frequency of fasting repetition None Rarely Sometimes |
10 2 1 |
21 1 2 |
9 1 3 |
0.495 |
|
Frequency of suspecting intrusive thoughts related to ritual impurity None Sometimes > once per month > once per week > once per day |
6 1 0 3 3 |
6 3 1 2 12 |
2 1 0 1 9 |
0.365 |
|
Frequency of attempts to correct suspected ritual impurities None Rarely Sometimes Every time |
6 1 1 5 |
6 1 4 13 |
2 0 1 10 |
0.445 |
|
Blasphemous thoughts No Yes |
10 3 |
13 11 |
8 5 |
0.459 |
|
Skeptical thoughts regarding the holy book No Yes |
11 2 |
19 5 |
11 2 |
>0.999 |
|
Skeptical thoughts regarding religious scripts or prophetic Hadiths No Yes |
8 5 |
16 8 |
9 4 |
>0.999 |
|
Perceived parents’ religiosity No Practice Low moderate High Very high |
0 2 7 3 1 |
0 5 11 5 3 |
1 0 5 7 0 |
0.221 |
|
Perceived self-religiosity Low moderate High Very high |
0 8 5 0 |
4 12 8 0 |
0 6 4 3 |
0.104 |
|
Frequency of visiting religious places/centers None Rarely Religious occasions Sometimes Weekly Daily |
2 2 3 2 3 1 |
6 1 3 6 7 1 |
1 1 4 2 4 1 |
0.864 |
| SIBS scores | 78.54±10.65 |
83.38±6.03 |
82.15±10.96 |
0.277 |
Table 2.
Subgroup analysis comparing obsessive-compulsive symptoms scores (ASOC) among the different categories of the sociodemographic, clinical, religiosity variables. Bolded p values are statistically significant (<0.05).
Table 2.
Subgroup analysis comparing obsessive-compulsive symptoms scores (ASOC) among the different categories of the sociodemographic, clinical, religiosity variables. Bolded p values are statistically significant (<0.05).
| Mann-Whitney or Kruskal Wallis test statistics | P value | |
|---|---|---|
| Age | H=3.044 | 0.218 |
| Sex | U=232.000 | 0.211 |
| Educational level | H=2.845 | 0.416 |
| Relationship status | H=0.248 | 0.884 |
| Area of living (childhood) | U=180.500 | 0.921 |
| Area of living (current) | U=193.000 | 0.877 |
| Monthly living income (Lebanese pounds) | H=4.266 | 0.371 |
| Attended school | H=0.915 | 0.633 |
| Parents’ relationship status | H=0.120 | 0.942 |
| Traumatic life events | U=365.500 | 0.230 |
| Age of diagnosis | H=0.611 | 0.894 |
| Family history of psychiatric illness | H=4.419 | 0.110 |
| Current OCD medications | U=248.00 | 0.223 |
| Current or past psychotherapy | H=1.665 | 0.435 |
| Praying frequency | H=1.386 | 0.500 |
| Self-question if praying correctly | U=390.000 | 0.014 |
| Self-question if prayers are accepted by God | U=300.000 | 0.427 |
| Frequency of prayers repetition if questioning | H=3.552 | 0.314 |
| Praying location | H=1.506 | 0.681 |
| Frequency of partial ablution | U=189.000 | 0.594 |
| Partial ablution repetition | U=425.500 | 0.028 |
| Frequency of partial ablution repetition | H=6.785 | 0.079 |
| Partial ablution location | H=0.600 | 0.741 |
| Full ablution repetition | U=13.000 | 0.560 |
| Frequency of full ablution repetition | H=6.832 | 0.077 |
| Frequency of fasting practice | H=1.120 | 0.772 |
| Self-question if fasting correctly | U=368.500 | 0.103 |
| Self-question if fasting accepted by God | U=342.000 | 0.342 |
| Frequency of fasting repetition | H=1.038 | 0.595 |
| Frequency of suspecting intrusive thoughts related to ritual impurity | H=3.653 | 0.455 |
| Frequency of attempts to correct suspected ritual impurities | H=1.933 | 0.586 |
| Blasphemous thoughts | U=338.500 | 0.379 |
| Skeptical thoughts regarding the holy book | U=209.500 | 0.534 |
| Skeptical thoughts regarding religious scripts or prophetic Hadiths | U=289.500 | 0.854 |
| Perceived parents’ religiosity | H=7.912 | 0.095 |
| Perceived self-religiosity | H=3.146 | 0.370 |
| Frequency of visiting religious places/centers | H=1.533 | 0.199 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



